linfoma de hodgkin - comanes.orgcomanes.org/reunionacademica_2017/hodgkin_lymphoma_takeda.pdf ·...
TRANSCRIPT
HODGKIN LYMPHOMA
DR. ALEJANDRA ZARATE OSORNOHOSPITAL ESPAÑOL DE MEXICO

HODGKIN LYMPHOMA CLASSIFICATION
Lukes & Butler Rye WHO-2016Linphocyticand/or histiocyticNodular & diffuse
Lymphocytepredominance
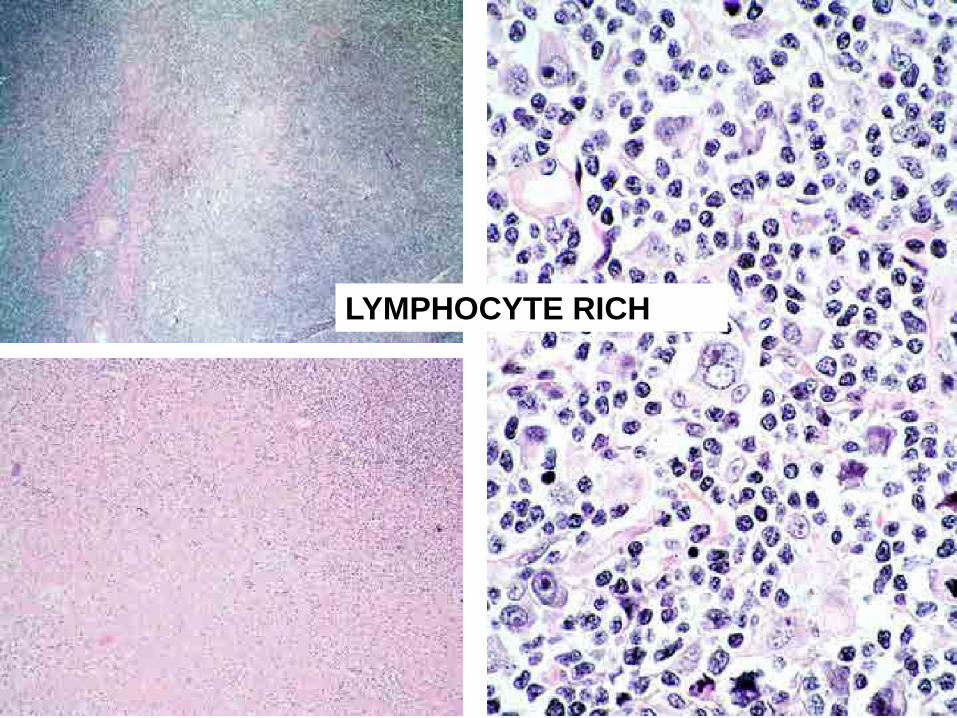
NodularLymphocytePredominancecHL: lymphocyterich
Nodular Sclerosis
Nodular Sclerosis
cHL: Nodular Sclerosis
Mixed Cellularity Mixed Cellularity cHL: MixedCellularity
Diffuse FibrosisReticular
LymphocyteDepletion
cHL: LymphocyteDepletion
HODGKIN LYMPHOMA• 15% of all the lymphomas• México: 15%• Incidence: stable• Hodgkin’s disease Hodgkin
Lymphoma• B-cell origin• Classification based on the original Lukes
&Butler classification
DIAGNOSTIC CRITERIA• There have been changes• Purely histological to histological and
immunophenotypic
– Reclassification of the disease– Change on the frequency of the subtypes – Changes on the criteria for the HL
diagnosis
IMMUNOPHENOTYPE
• RS cells RS + appropriate milieu HL
• Inmunophenotype– NLP HL LP cell– cHL, NS: Lacunar cell– cHL, MC: RS+ mononuclear cells– cHL, LD RS+ anaplastic cells
ImmunophenotypeSmall biopsies
• RS cells are not necessary for the diagnosis
• Enough number of mononuclear cells with the appropriate immunophenotype
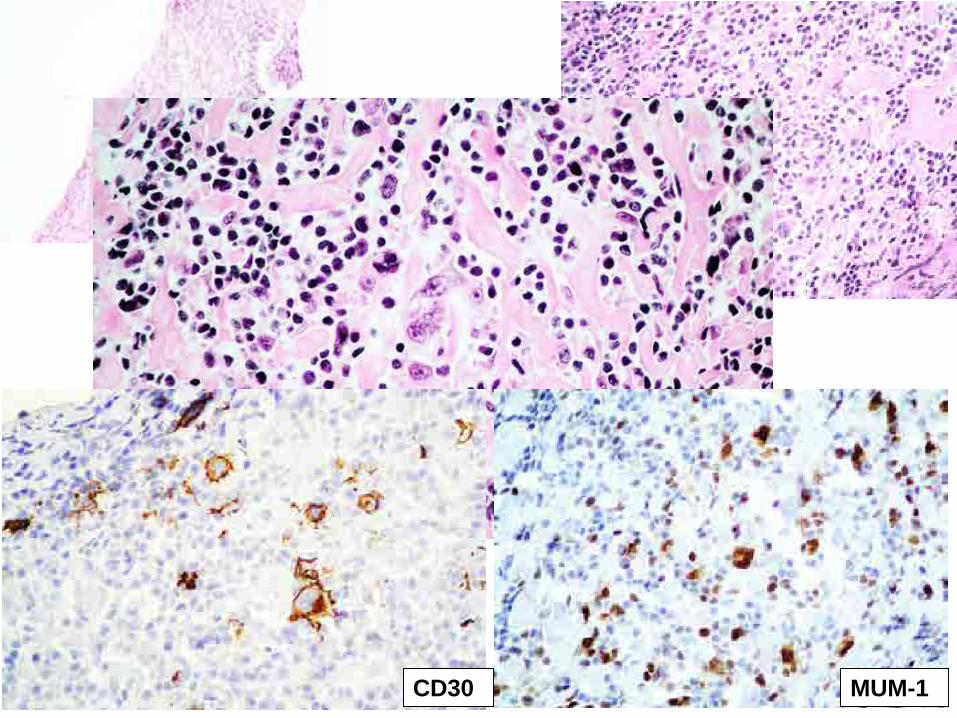
CD30 MUM-1
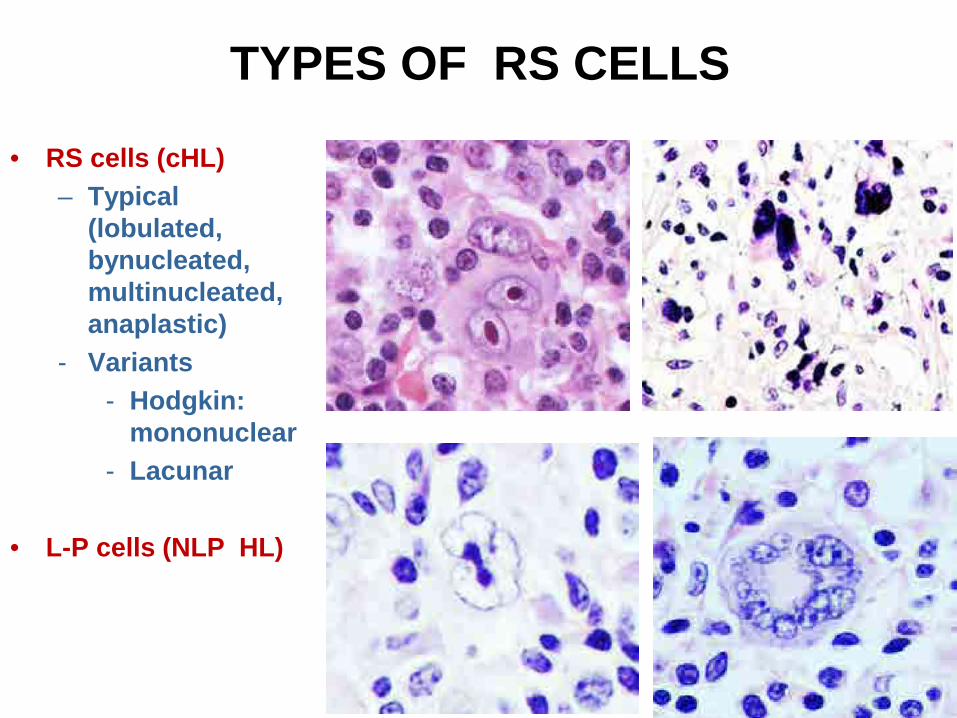
TYPES OF RS CELLS
• RS cells (cHL)– Typical
(lobulated, bynucleated, multinucleated, anaplastic)
- Variants- Hodgkin:
mononuclear- Lacunar
• L-P cells (NLP HL)
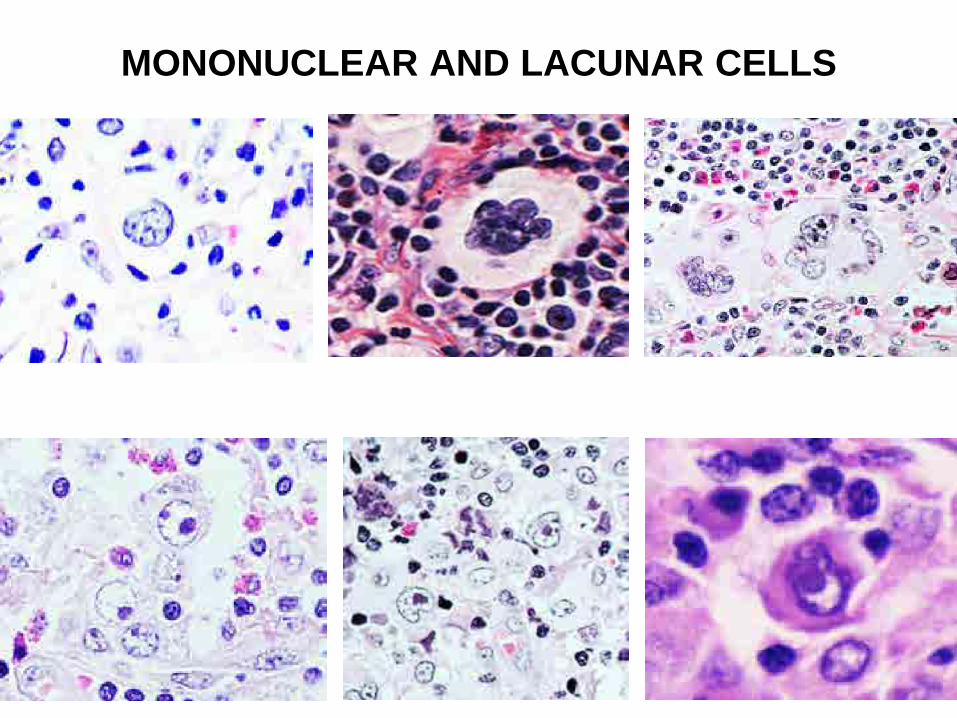
MONONUCLEAR AND LACUNAR CELLS
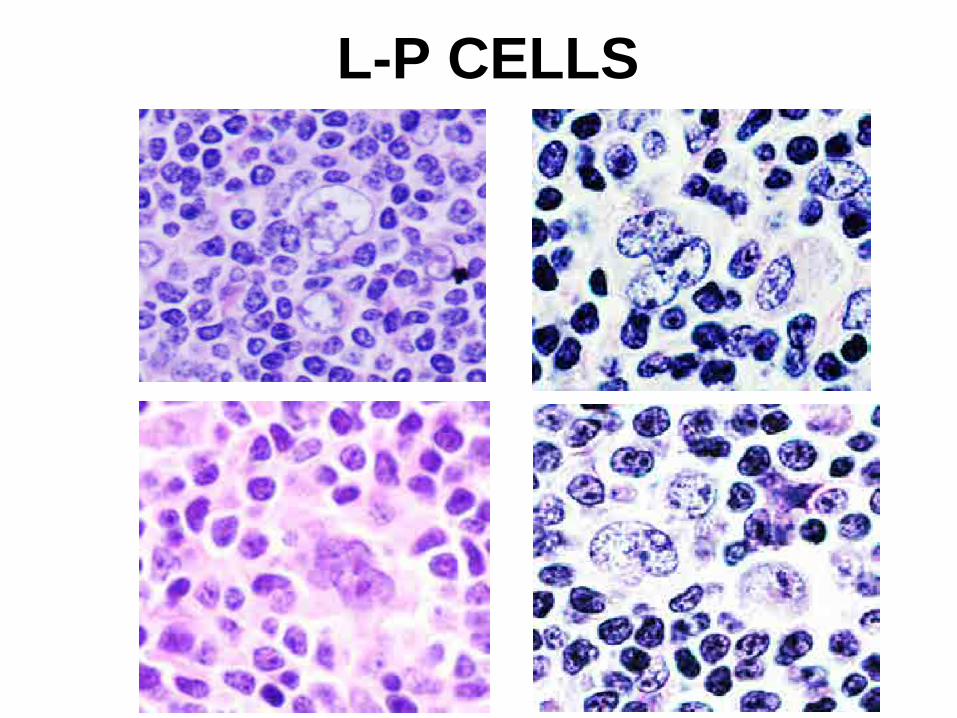
L-P CELLS
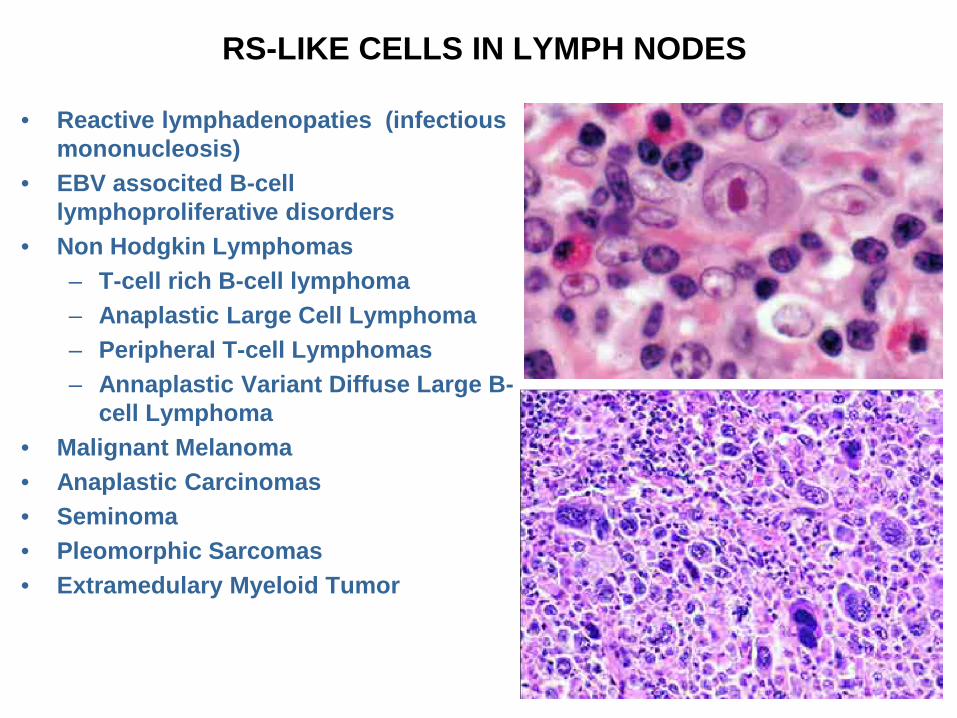
RS-LIKE CELLS IN LYMPH NODES
• Reactive lymphadenopaties (infectious mononucleosis)
• EBV associted B-cell lymphoproliferative disorders
• Non Hodgkin Lymphomas– T-cell rich B-cell lymphoma– Anaplastic Large Cell Lymphoma– Peripheral T-cell Lymphomas – Annaplastic Variant Diffuse Large B-
cell Lymphoma• Malignant Melanoma• Anaplastic Carcinomas • Seminoma• Pleomorphic Sarcomas • Extramedulary Myeloid Tumor
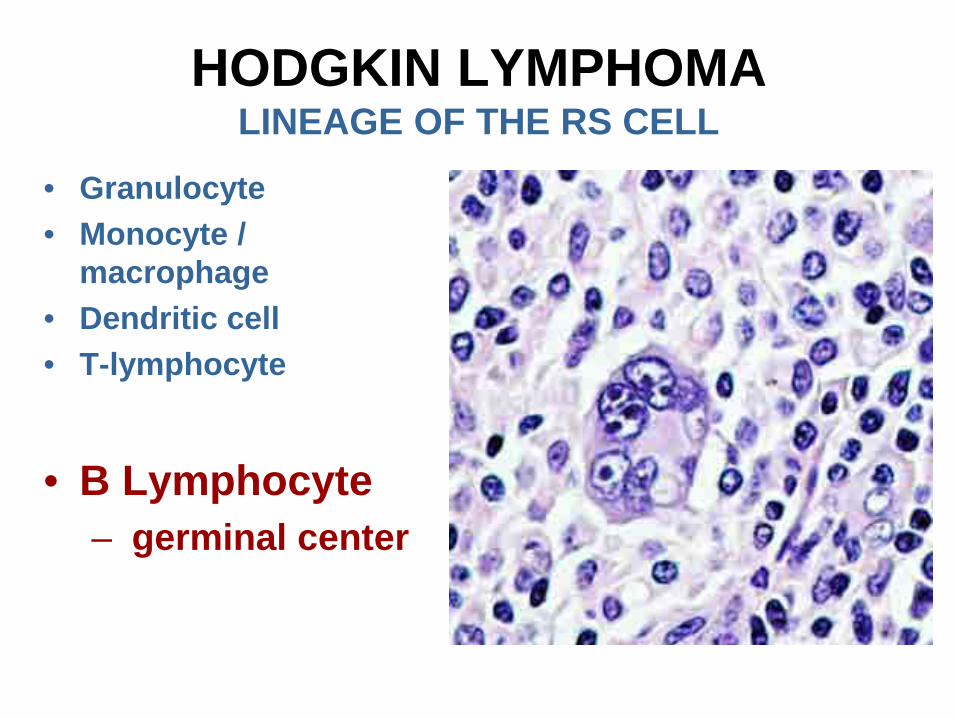
HODGKIN LYMPHOMALINEAGE OF THE RS CELL
• Granulocyte• Monocyte /
macrophage• Dendritic cell• T-lymphocyte
• B Lymphocyte– germinal center
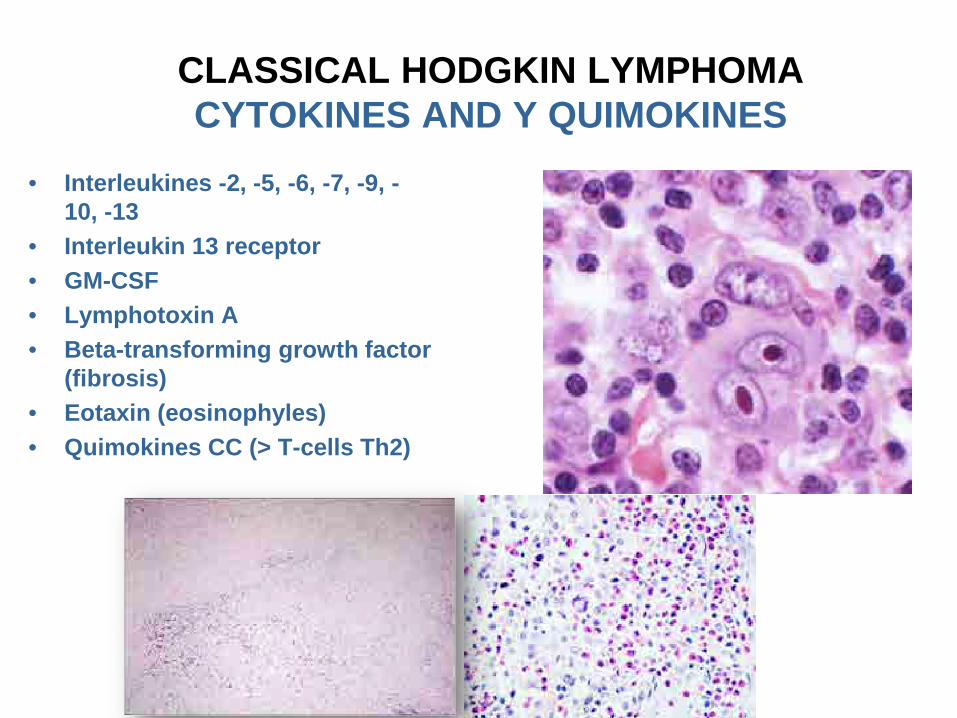
CLASSICAL HODGKIN LYMPHOMACYTOKINES AND Y QUIMOKINES
• Interleukines -2, -5, -6, -7, -9, -10, -13
• Interleukin 13 receptor• GM-CSF• Lymphotoxin A• Beta-transforming growth factor
(fibrosis)• Eotaxin (eosinophyles)• Quimokines CC (> T-cells Th2)
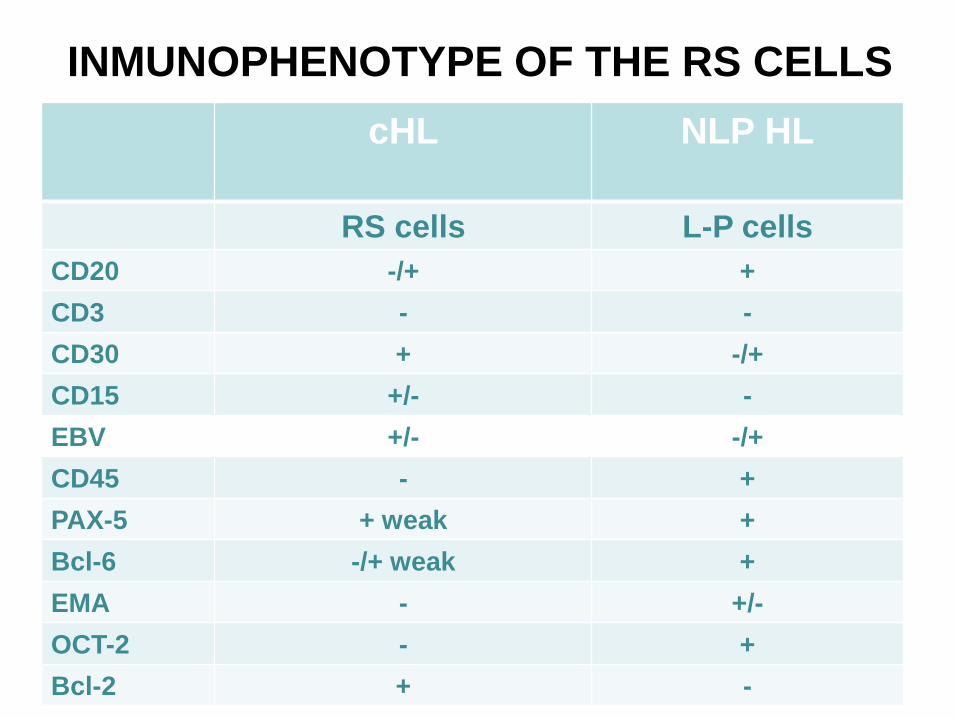
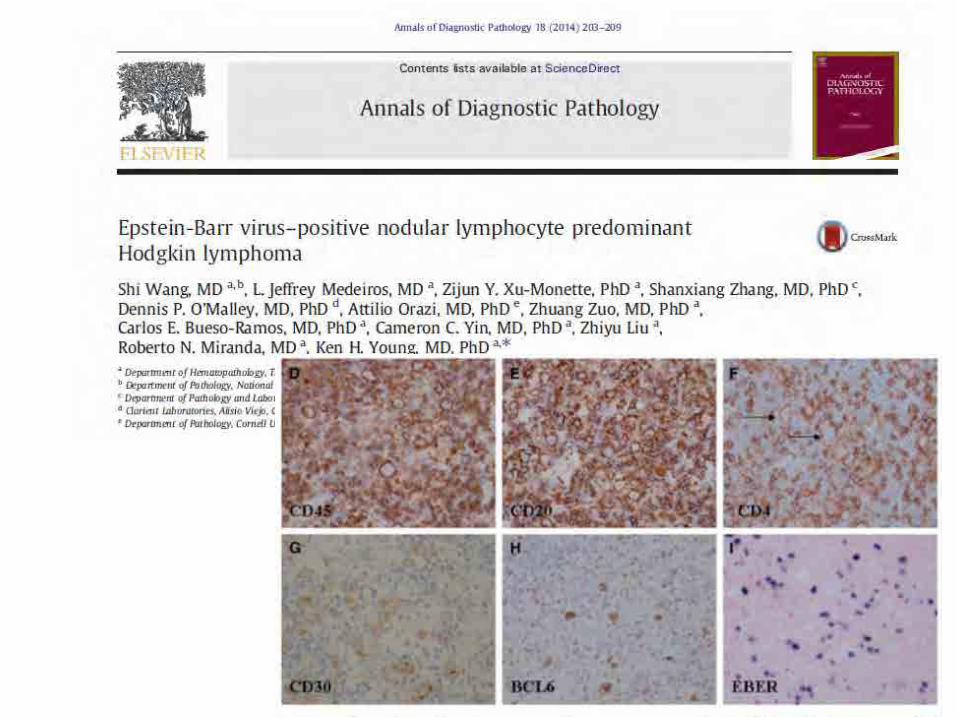
INMUNOPHENOTYPE OF THE RS CELLScHL NLP HL
RS cells L-P cellsCD20 -/+ +CD3 - -CD30 + -/+CD15 +/- -EBV +/- -/+CD45 - +PAX-5 + weak +Bcl-6 -/+ weak +EMA - +/-OCT-2 - +Bcl-2 + -
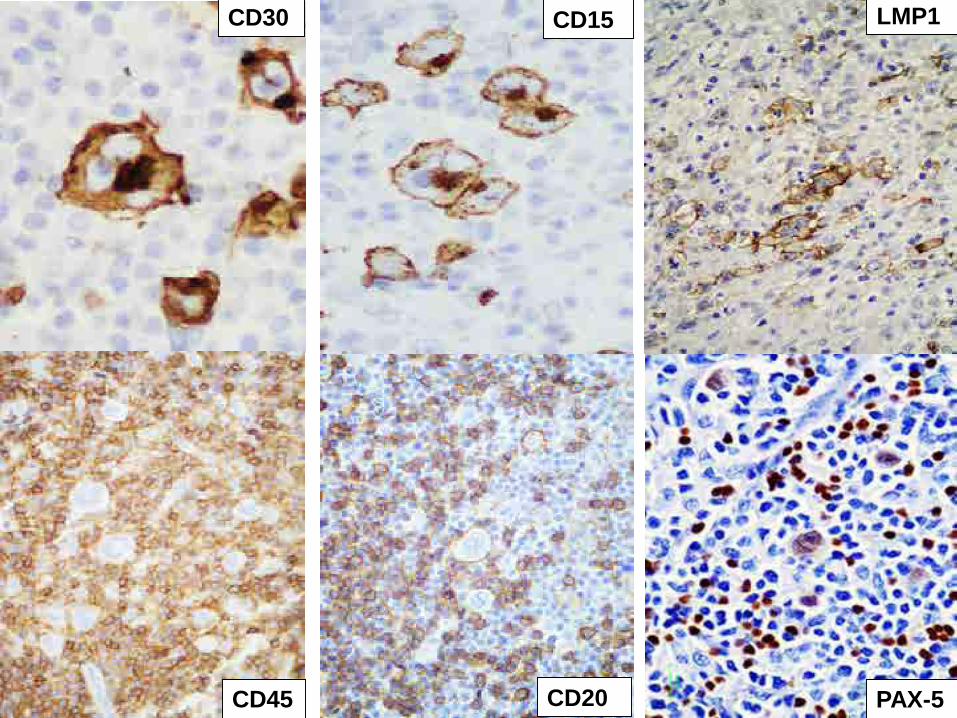
CD30 CD15
CD45 CD20 PAX-5
LMP1
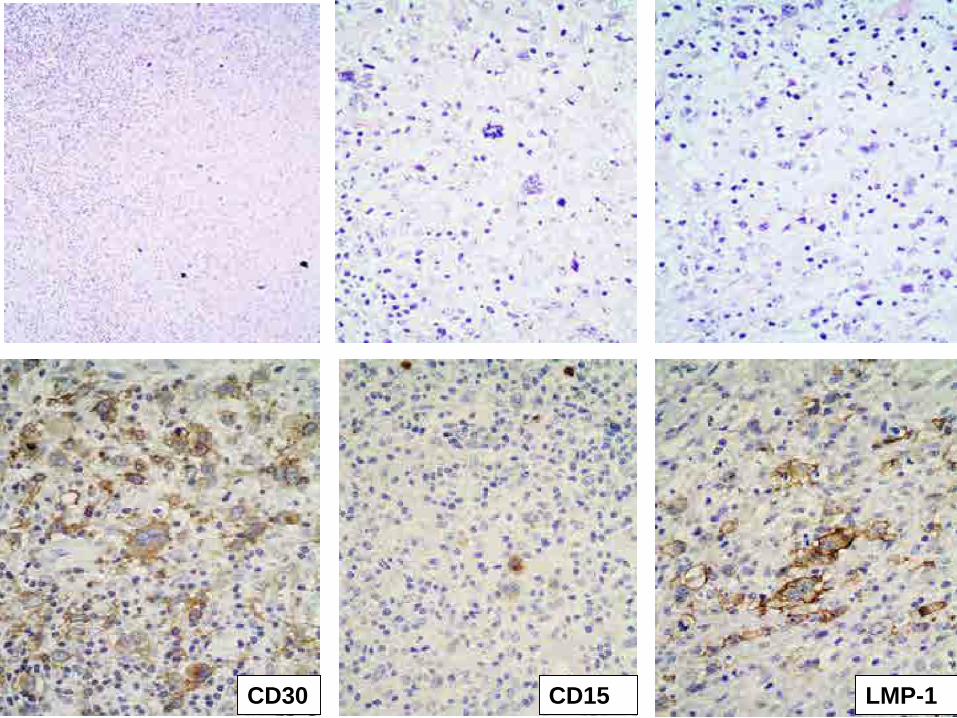
CD30 CD15 LMP-1
CLASSICAL HOSGKIN LYMPHOMACELL OF ORIGIN
MATURE B-CEL, DERIVED FROM THE GERMINAL CENTER, IN
MATURATION STAGE
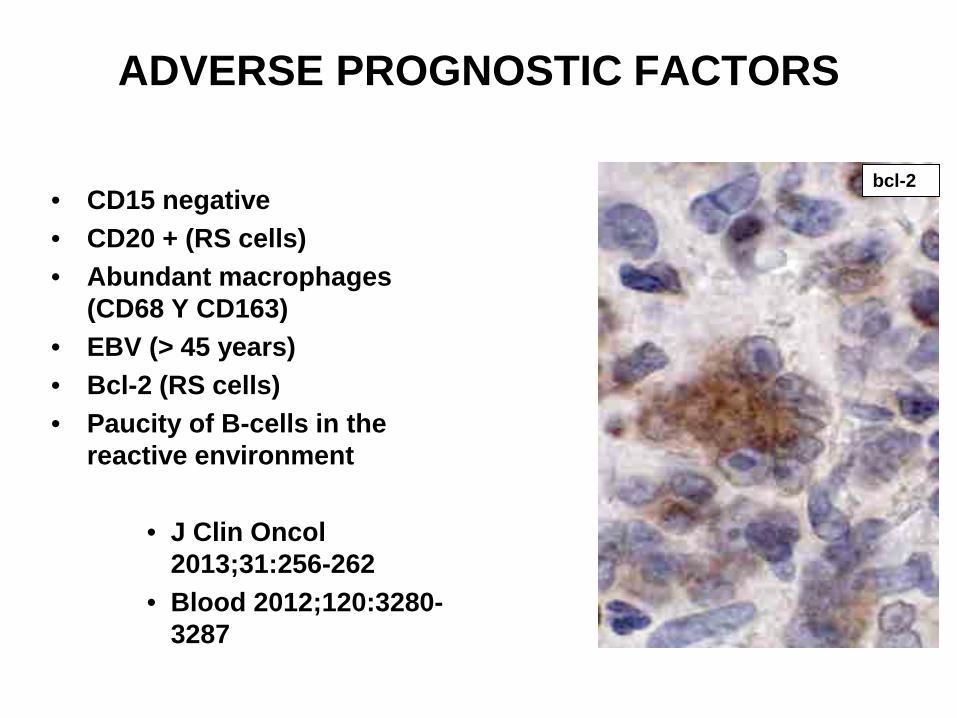
ADVERSE PROGNOSTIC FACTORS
• CD15 negative• CD20 + (RS cells)• Abundant macrophages
(CD68 Y CD163)• EBV (> 45 years)• Bcl-2 (RS cells)• Paucity of B-cells in the
reactive environment
• J Clin Oncol 2013;31:256-262
• Blood 2012;120:3280-3287
bcl-2
CLASSICAL HODGKIN LYMPHOMAFOUR SUBTYPES
• Similar features:– Inmunophenotype– Genetics
• Differences:– Clinical characteristics– Involved organs– Pattern of tissular growth– Fibrosis – RS cell type– Reactive environment– Association with EBV
CLASSICAL HODGKIN LYMPHOMACLINICAL FEATURES
• Bimodal age distribution– 15-35 years– Adults > 55 years
• Associated with EBV: increased incidence in cHL– Particularly MC and LD– Geographical variation
• Peripheral lymphadenopathy– > 60% in I or II stages
• B symptoms– 40%
FRECUENCY OF THE SUBTYPES
• Nodular Sclerosis 62%• Mixed Cellularity: 27%• Nodular Lymphocyte Predominance: 5%• Lymphocyte Rich: 5%• Lymphocyte Depletion: 1%
» German Hodgkin Study Group» L Clin Oncol 23:5739, 2005
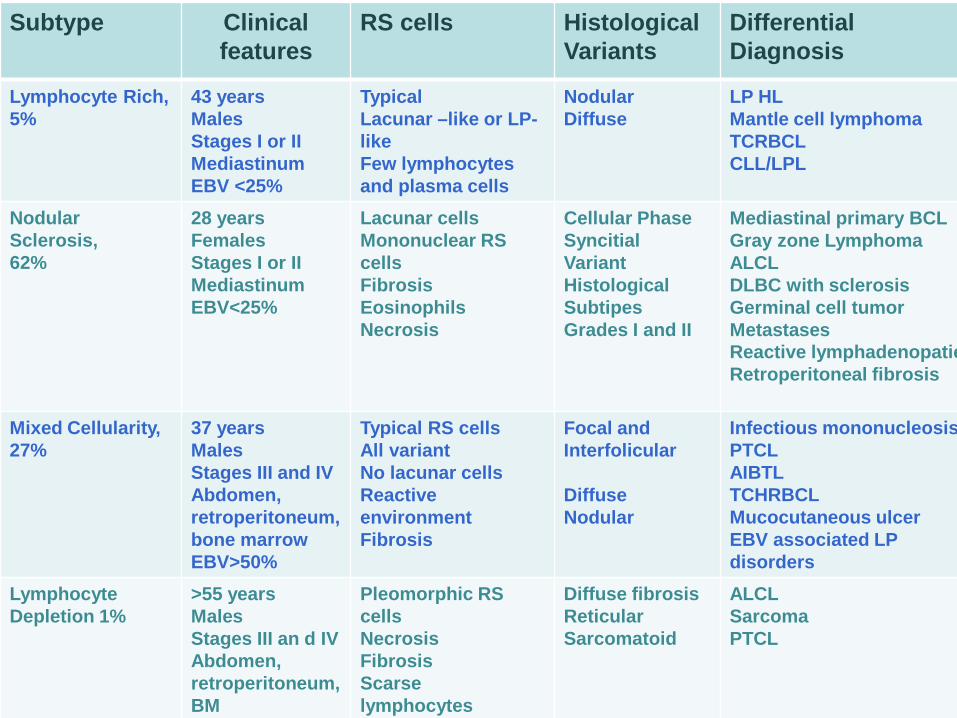
Subtype Clinicalfeatures
RS cells HistologicalVariants
DifferentialDiagnosis
Lymphocyte Rich, 5%
43 yearsMalesStages I or IIMediastinumEBV <25%
TypicalLacunar –like or LP-likeFew lymphocytesand plasma cells
NodularDiffuse
LP HLMantle cell lymphomaTCRBCLCLL/LPL
NodularSclerosis,62%
28 yearsFemalesStages I or IIMediastinumEBV<25%
Lacunar cellsMononuclear RS cellsFibrosisEosinophilsNecrosis
Cellular PhaseSyncitialVariantHistologicalSubtipesGrades I and II
Mediastinal primary BCLGray zone LymphomaALCLDLBC with sclerosisGerminal cell tumorMetastasesReactive lymphadenopatieRetroperitoneal fibrosis
Mixed Cellularity, 27%
37 yearsMalesStages III and IVAbdomen, retroperitoneum, bone marrowEBV>50%
Typical RS cellsAll variantNo lacunar cellsReactive environmentFibrosis
Focal and Interfolicular
DiffuseNodular
Infectious mononucleosisPTCLAIBTLTCHRBCLMucocutaneous ulcerEBV associated LP disorders
LymphocyteDepletion 1%
>55 yearsMalesStages III an d IVAbdomen, retroperitoneum, BM
Pleomorphic RS cellsNecrosisFibrosisScarselymphocytes
Diffuse fibrosisReticularSarcomatoid
ALCLSarcomaPTCL
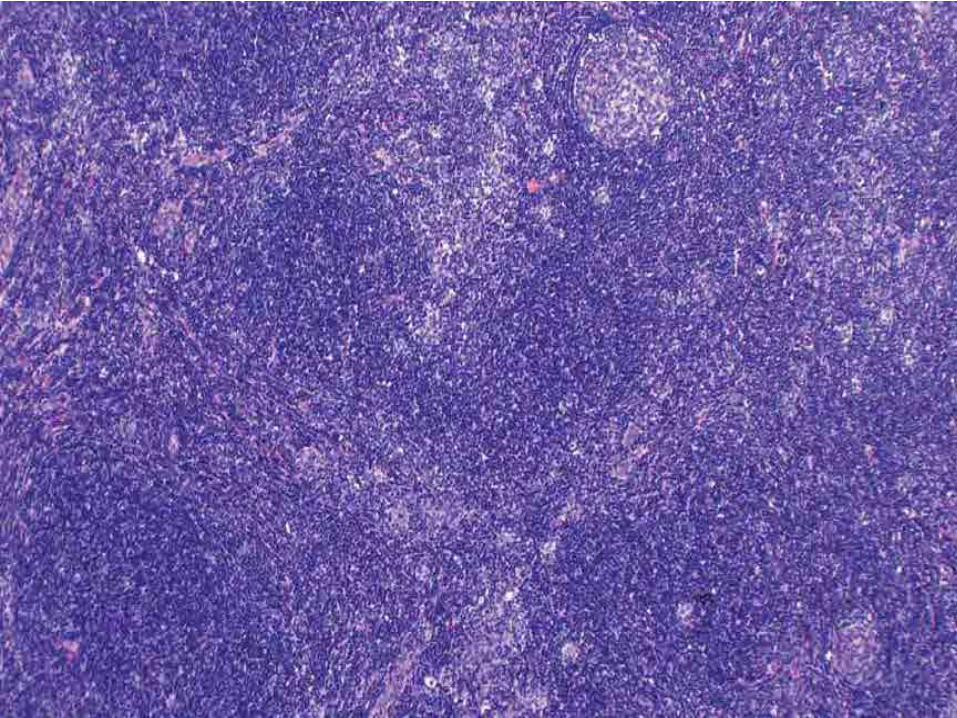
LYMPHOCYTE RICH
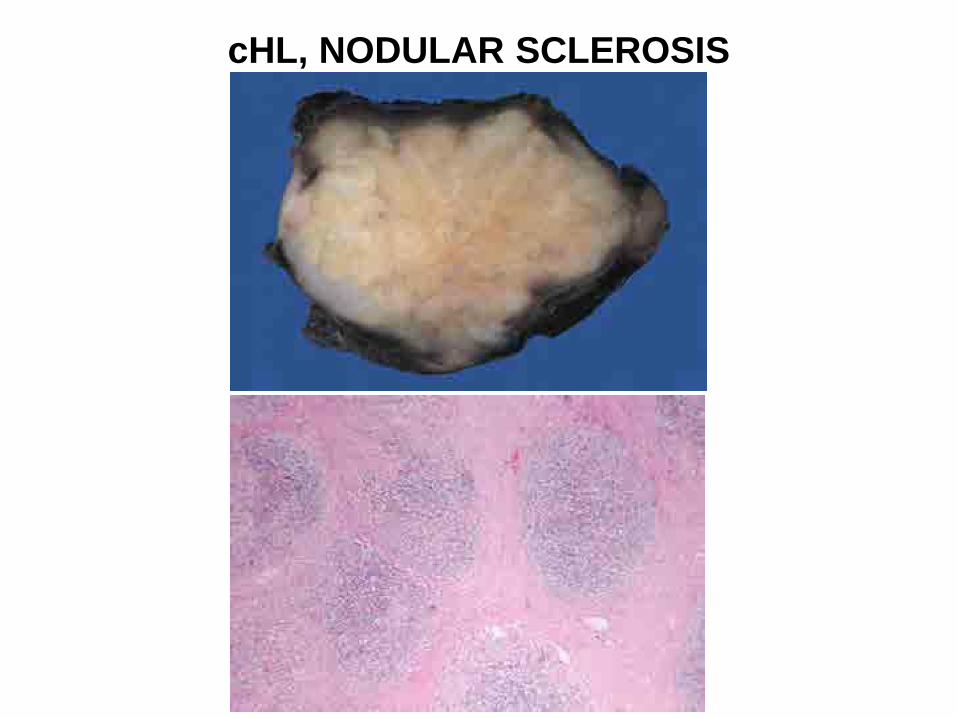
cHL, NODULAR SCLEROSIS

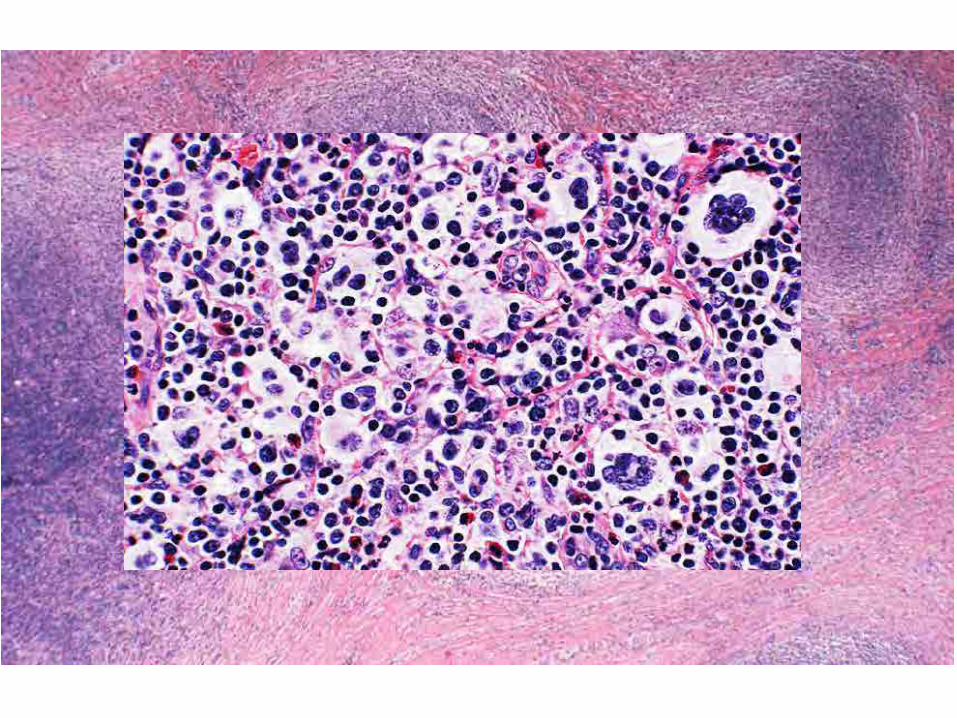

MONONUCLEAR AND LACUNAR CELLS
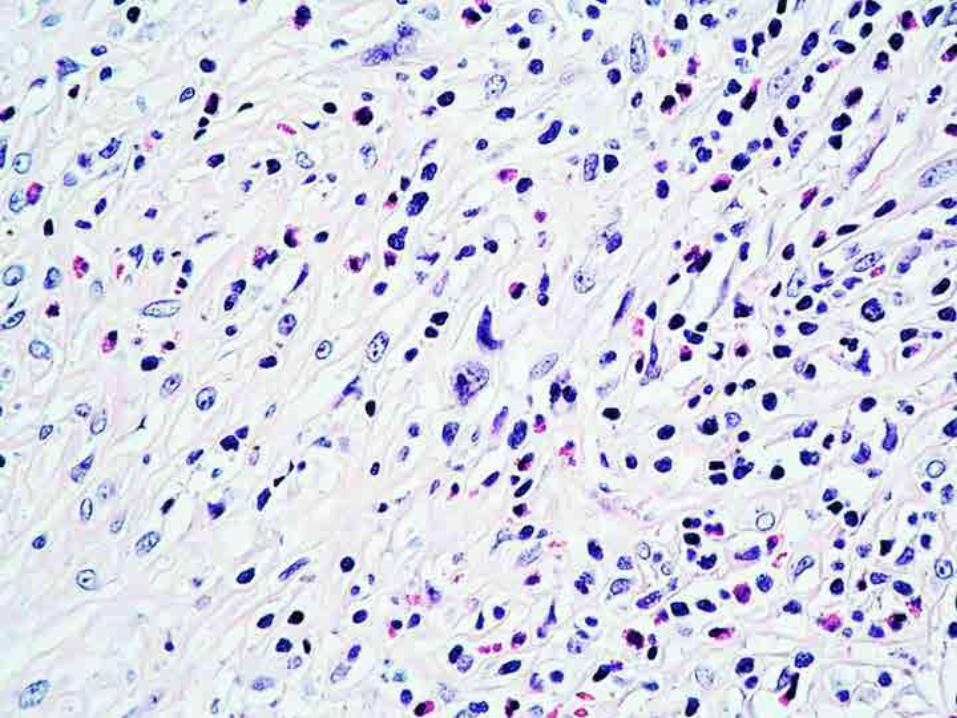
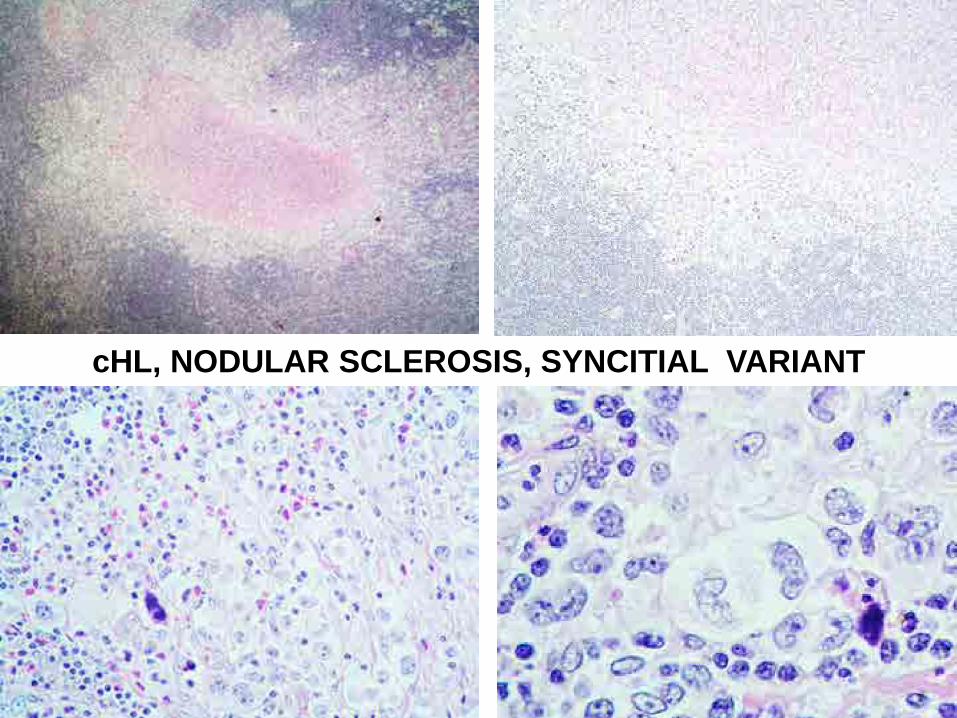
cHL, NODULAR SCLEROSIS, SYNCITIAL VARIANT
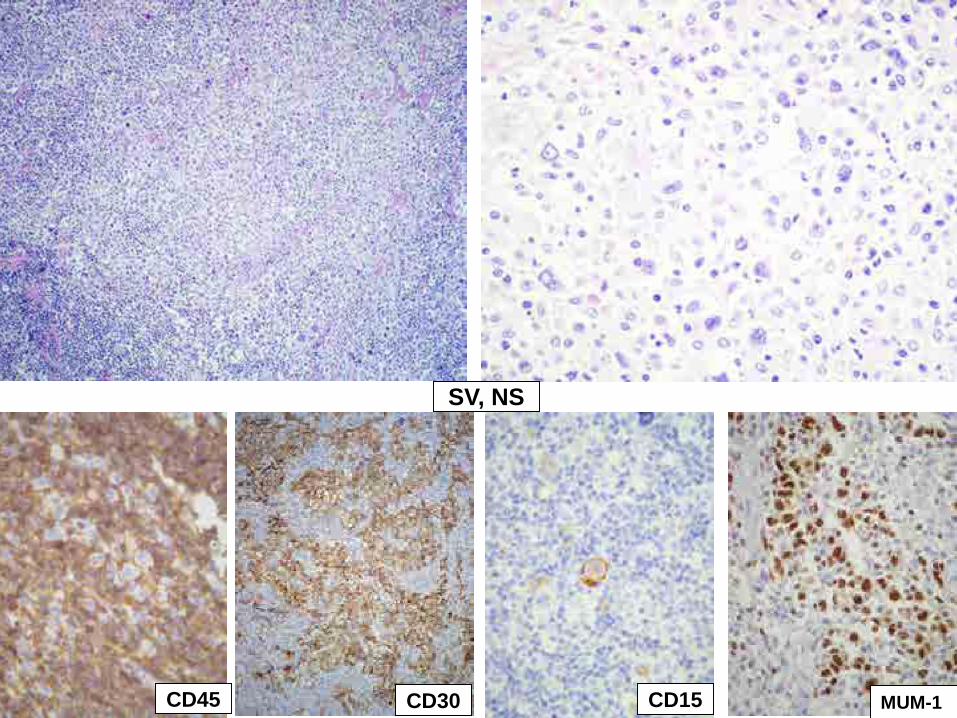
CD45 CD30 CD15
SV, NS
MUM-1
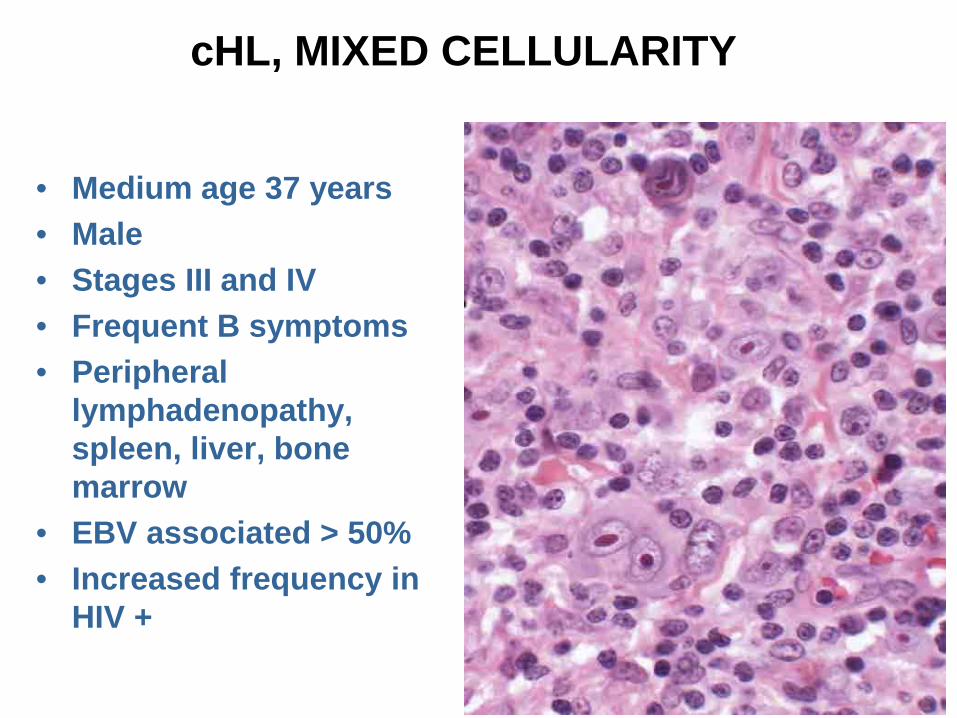
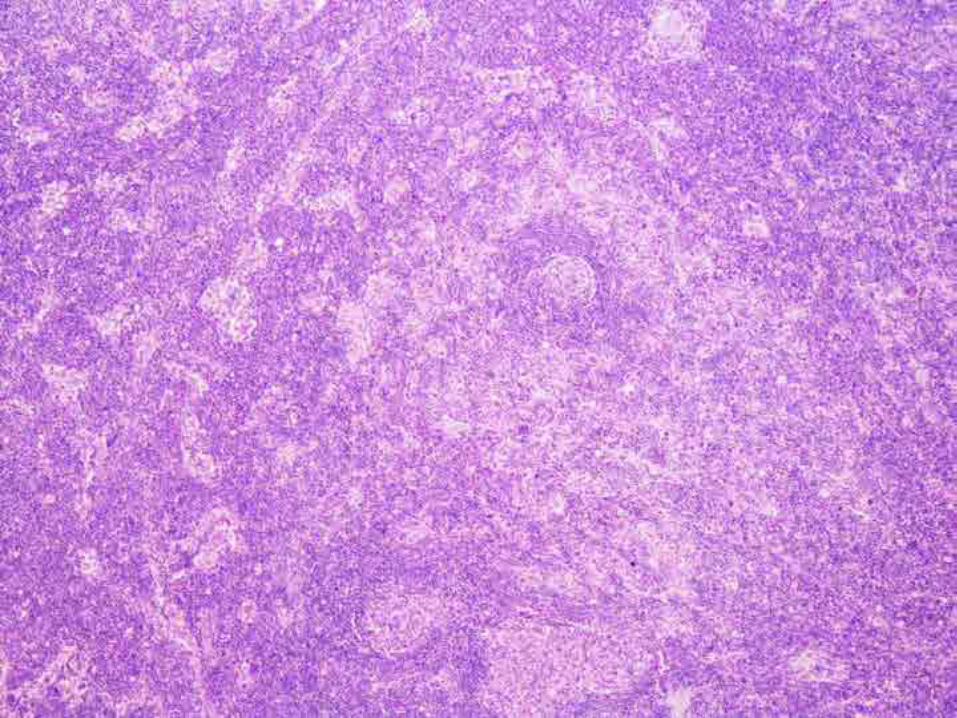
cHL, MIXED CELLULARITY
• Medium age 37 years• Male• Stages III and IV• Frequent B symptoms• Peripheral
lymphadenopathy, spleen, liver, bone marrow
• EBV associated > 50%• Increased frequency in
HIV +
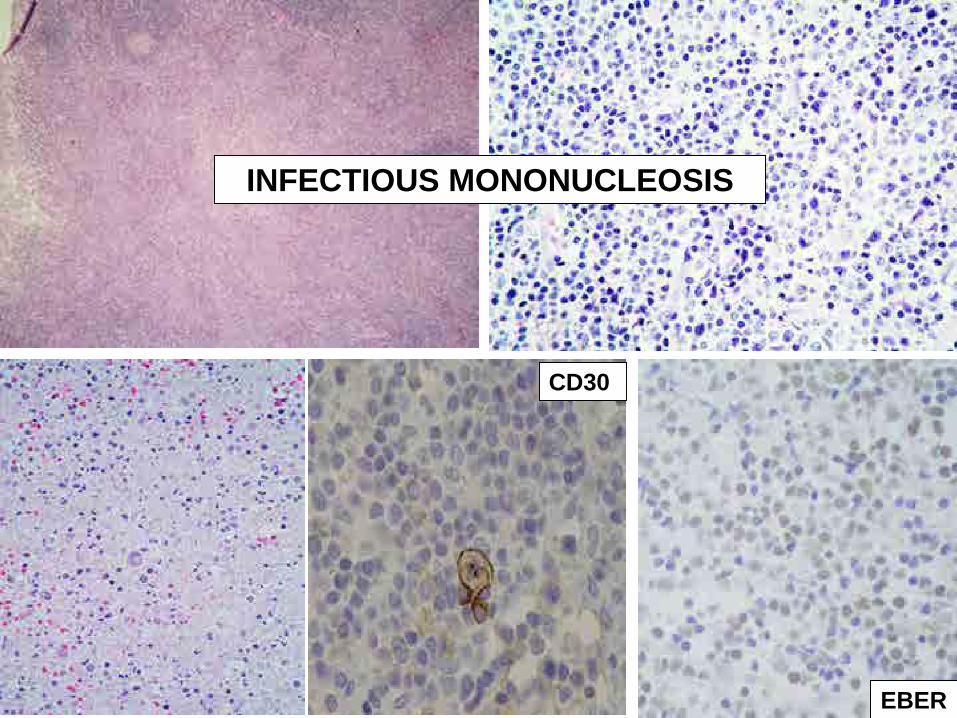
CD30
EBER
INFECTIOUS MONONUCLEOSIS
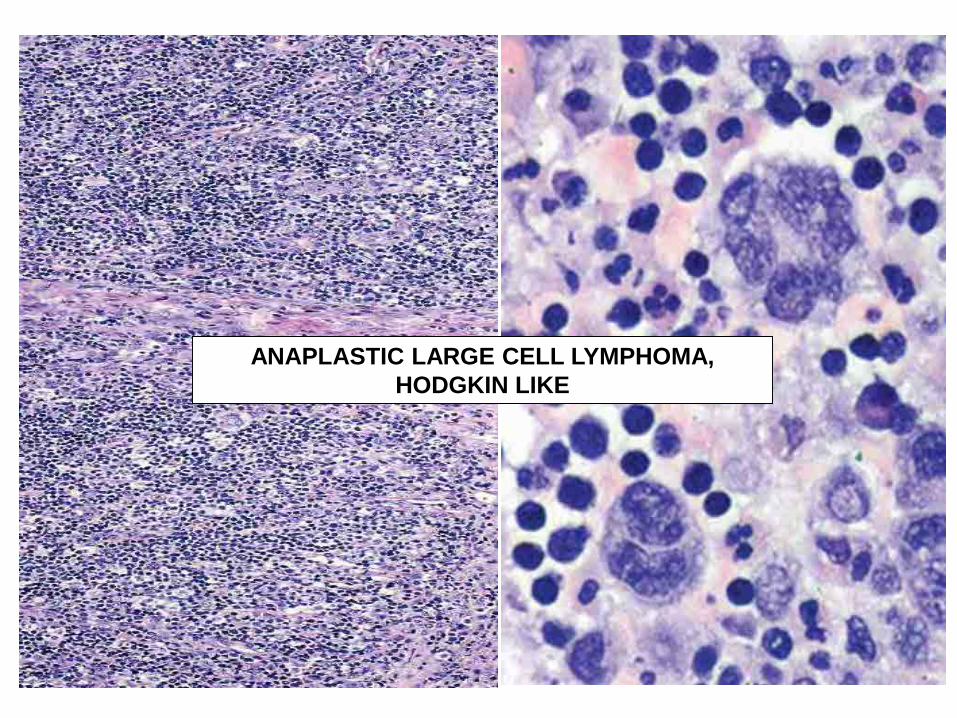
ANAPLASTIC LARGE CELL LYMPHOMA, HODGKIN LIKE
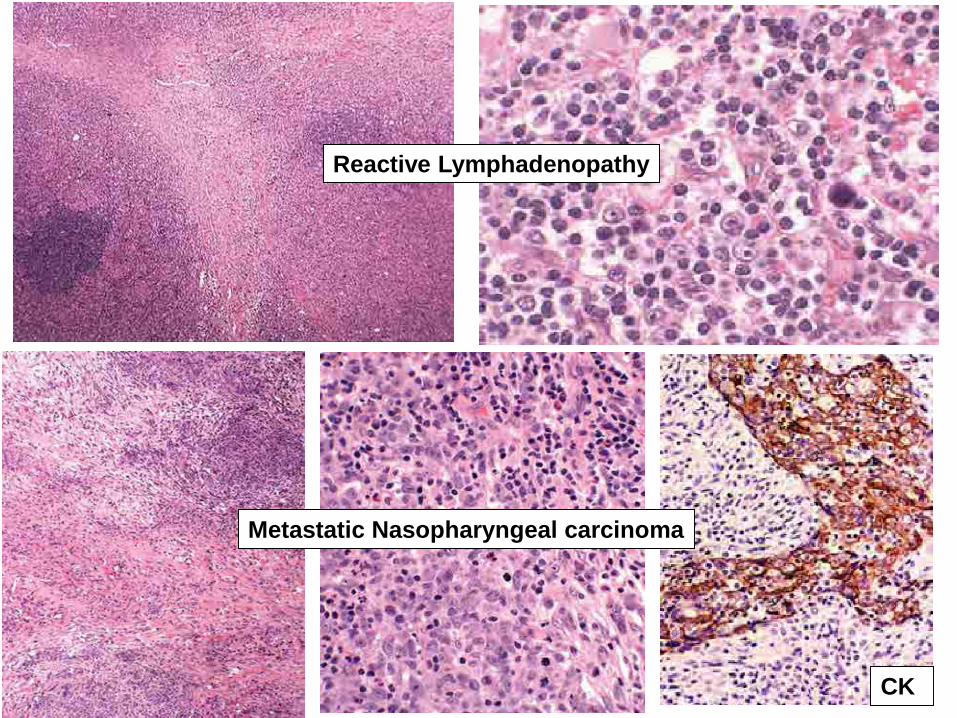
CK
Reactive Lymphadenopathy
Metastatic Nasopharyngeal carcinoma
cHL, LYMPHOCYTE DEPLETION
• Less frequent, < 1%• 30 to 40 years old or > 55 years• Male predominance (60 - 75%)• Clinical stage III or IV, most aggressive• B symptoms: 80%• EBV: 95% with HIV + and developing countries• Differential diagnosis: ALCL
• Involved organs– Abdomen and retroperitoneum– Bone marrow
Diffuse growth pattern
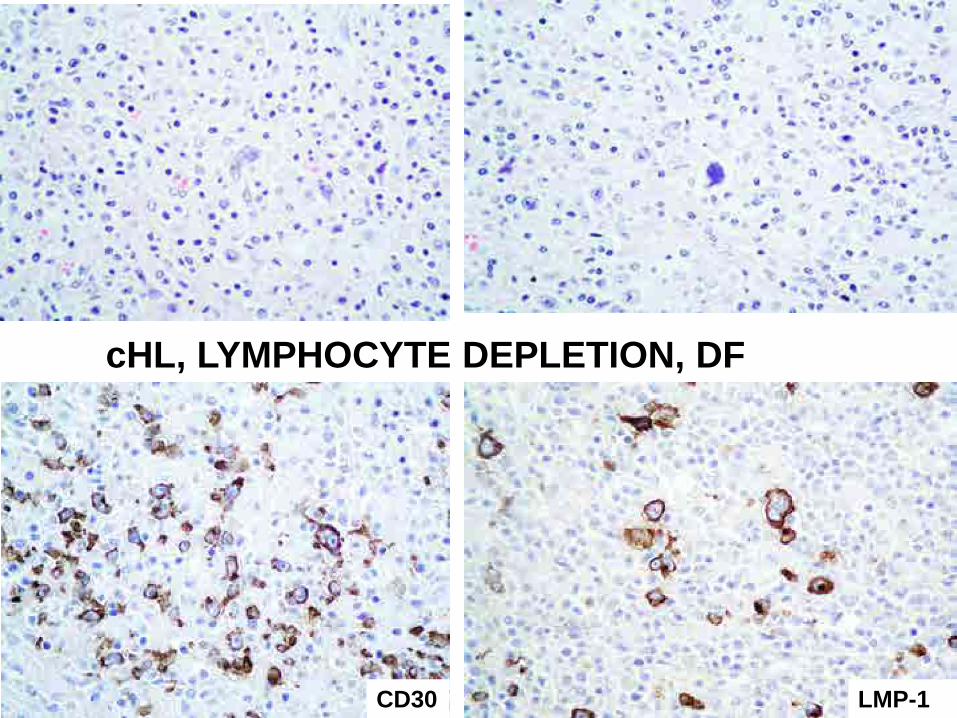
cHL, LYMPHOCYTE DEPLETION, DF
CD30 LMP-1
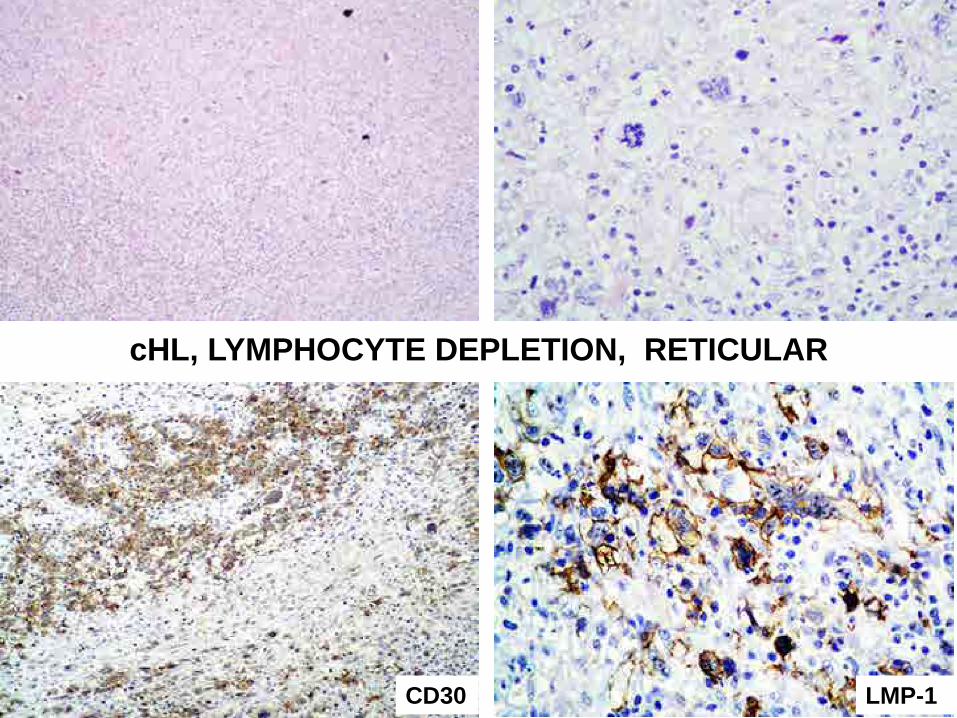
CD30 LMP-1
cHL, LYMPHOCYTE DEPLETION, RETICULAR
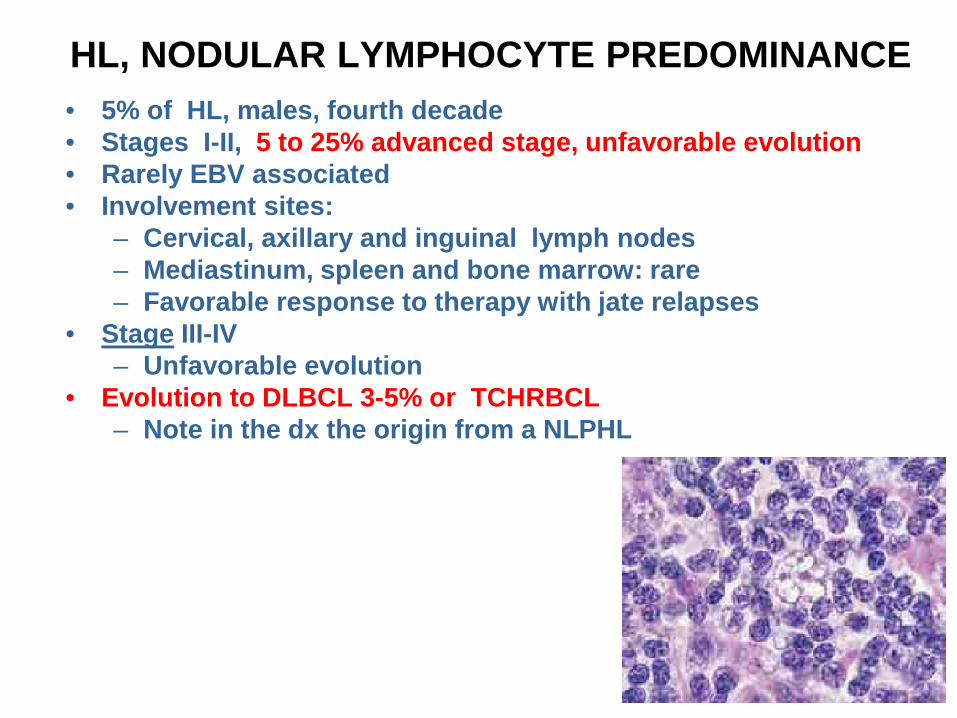
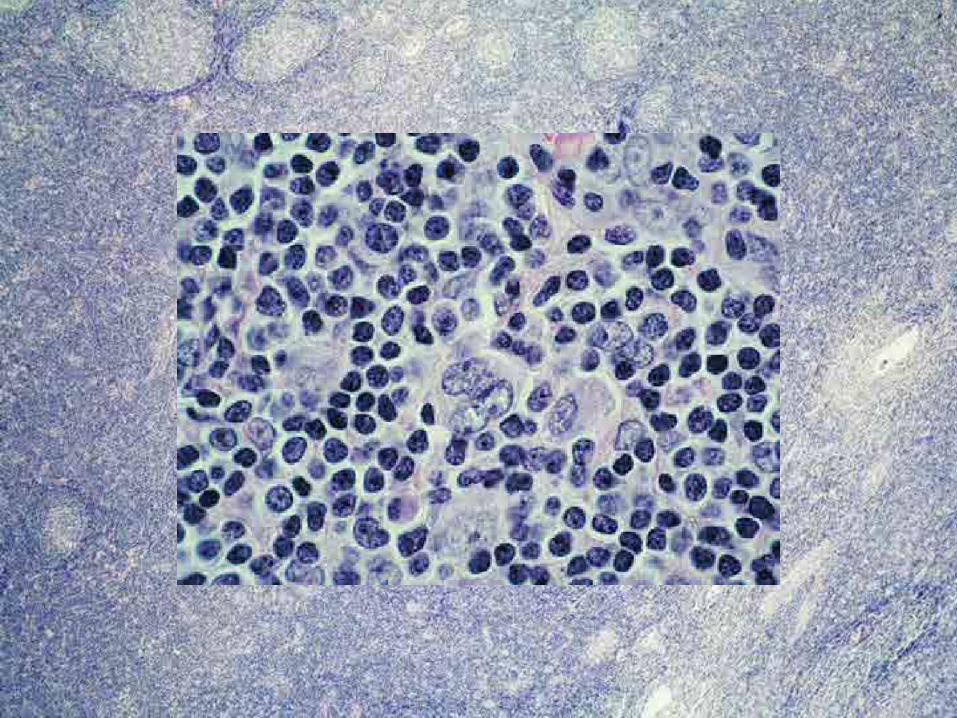
HL, NODULAR LYMPHOCYTE PREDOMINANCE• 5% of HL, males, fourth decade• Stages I-II, 5 to 25% advanced stage, unfavorable evolution • Rarely EBV associated• Involvement sites:
– Cervical, axillary and inguinal lymph nodes– Mediastinum, spleen and bone marrow: rare– Favorable response to therapy with jate relapses
• Stage III-IV– Unfavorable evolution
• Evolution to DLBCL 3-5% or TCHRBCL– Note in the dx the origin from a NLPHL
NODULAR LP HL
• Frequency: 5%• Inmunophenotype (B-cell CD20+, PAX-5+, bcl-6+)• Histological variants (6 types)• Differential diagnosis:
– Progressive transformation of the germinal centers– T-cell rich B cell lymphoma– Follicular lymphoma– cHL, lymphocyte rich– Peripheral T cell lymphoma, NOS– Chronic lymphocytic leukemia /small lymphocytic
lymphoma
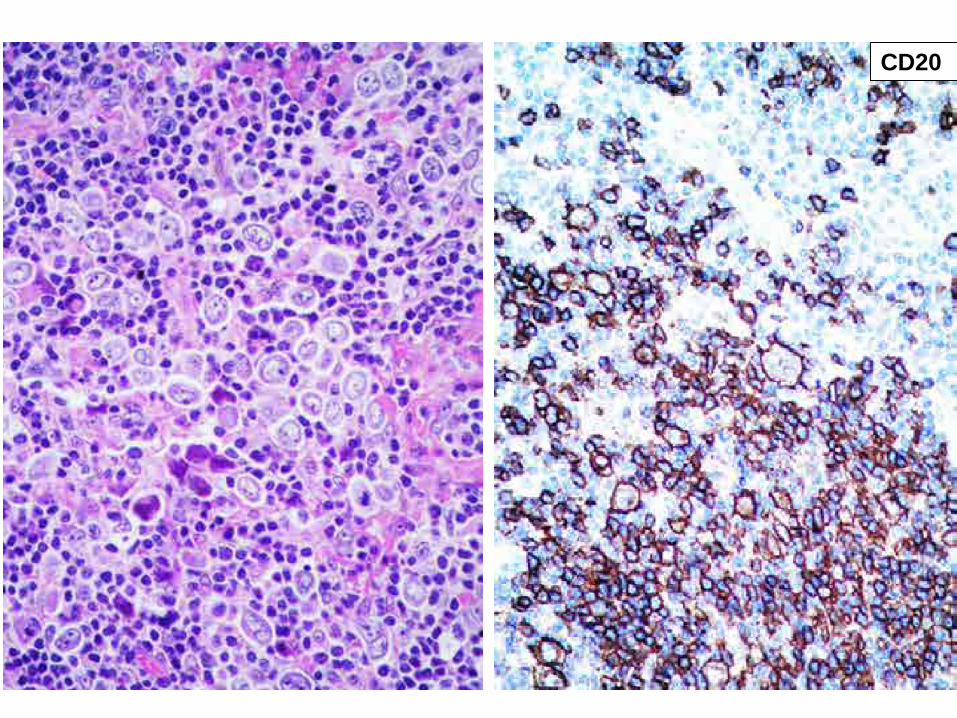
CD20
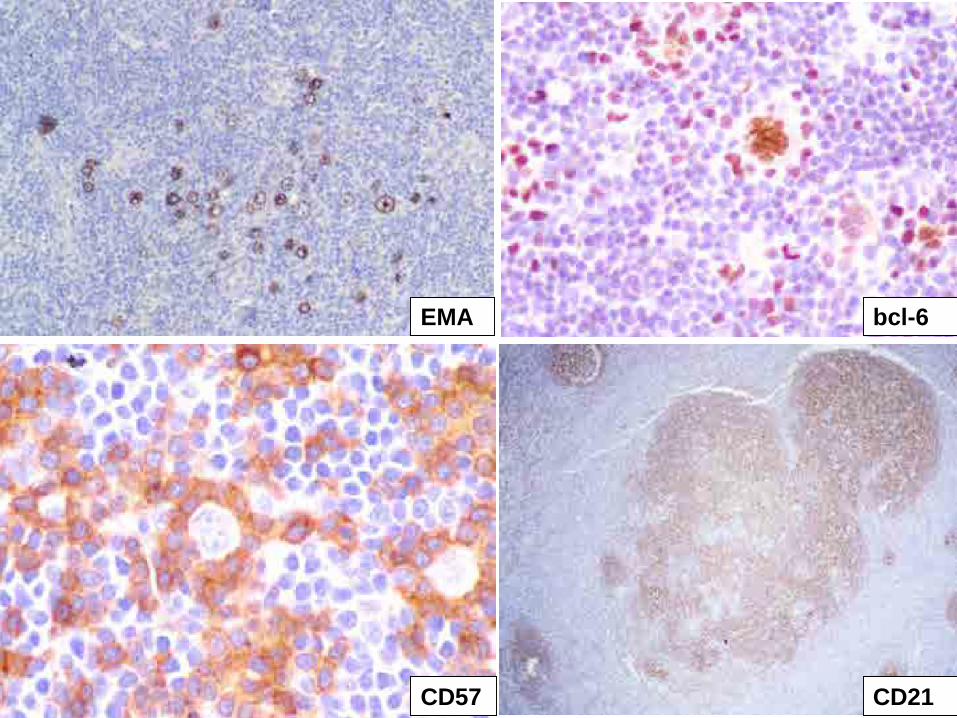
EMA bcl-6
CD57 CD21

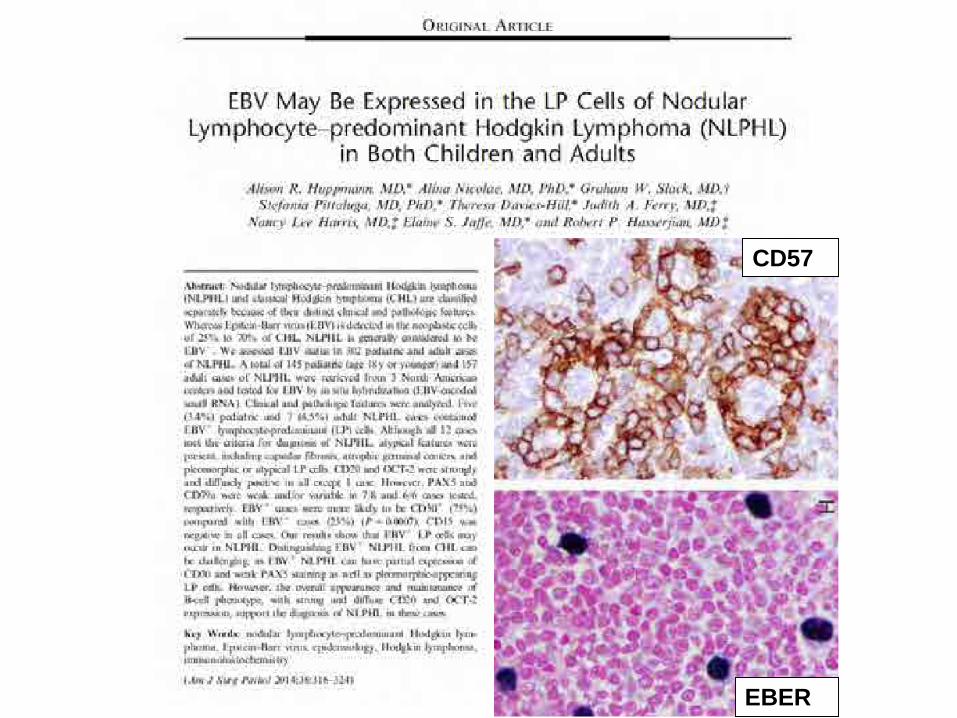
CD57
EBER
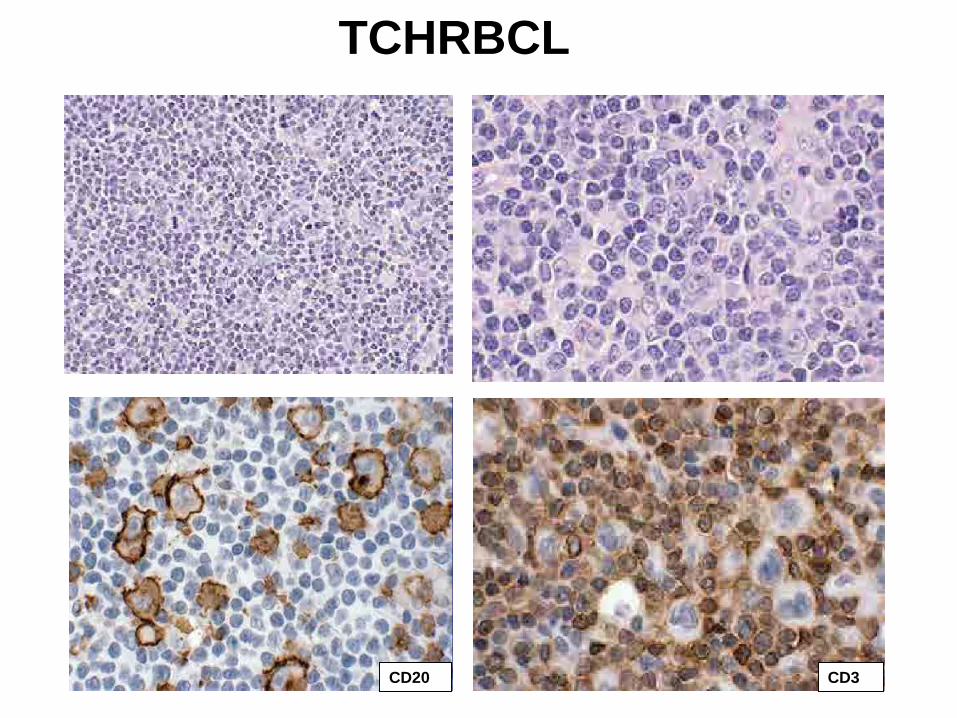
TCHRBCL
CD20 CD3
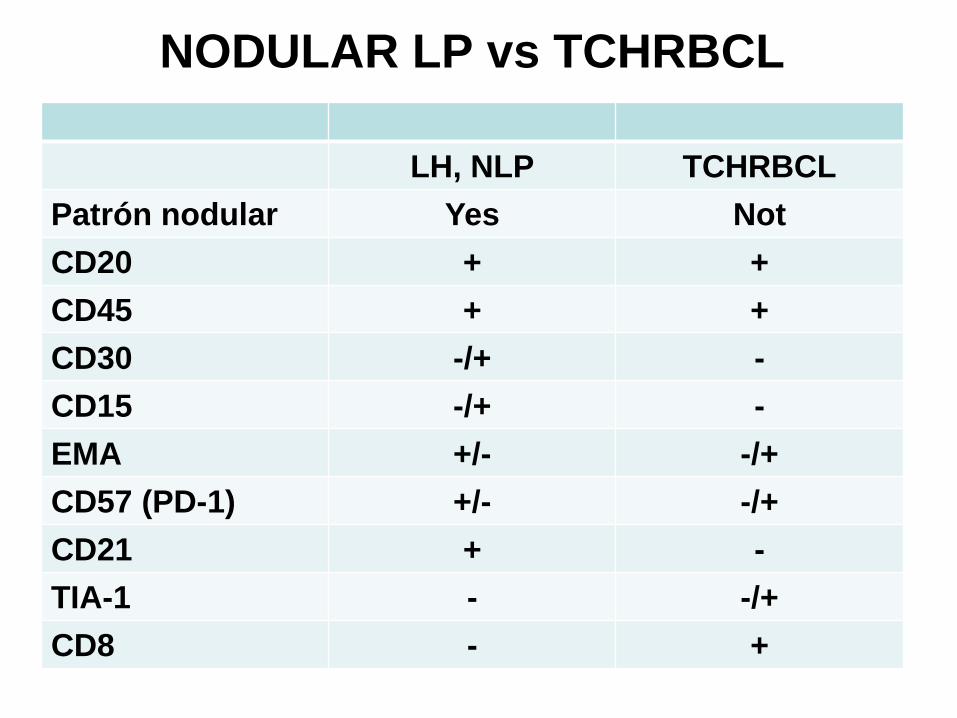
NODULAR LP vs TCHRBCL
LH, NLP TCHRBCLPatrón nodular Yes NotCD20 + +CD45 + +CD30 -/+ -CD15 -/+ -EMA +/- -/+CD57 (PD-1) +/- -/+CD21 + -TIA-1 - -/+CD8 - +
CLASSICAL HODGKIN LYMPHOMASECONDARY SITES (BONE MARROW AND LIVER)
• Mononuclear cells expressing CD15 and CD30
• Appropriate reactive cellular environment• Classical RS cells are not required if the
diagnosis was made in another site• Bone marrow: stage IV• Vascular disemination
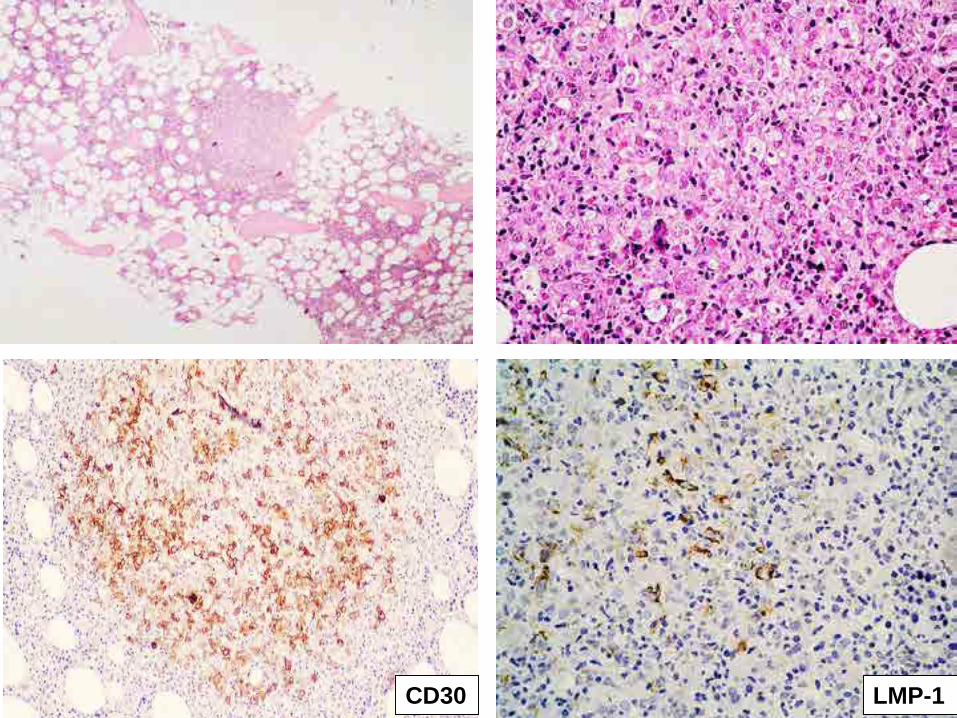
CD30 LMP-1
cHL, EXTRANODAL
• Very rare (except in HIV +)• 0.25% of cHL• Initial differential diagnosis: DLBCL• Mostly by contiguous extension or retrogradous
lymphatic disemination • Site
– GI tract– Lung, most common– Skin 0.5% (T-cell CD30 + cutaneous lymphoproliferative
disorders)– Waldeyer’s ring– Bone
HODGKIN LYMPHOMA PATHOLOGY OF THE RELAPSING DISEASE
• Modern therapy success• > 30% relapsing
– 1 to 13% late relapse (3 to 4 years)• More frequent:
– Advanced stages– Systemic symptoms– Bulky mediastinal disease
• Most frequent subtype: nodular sclerosis• Previously involved sites
HODGKIN LYMPHOMACAUSES OF DEATH
• Chemotherapy complications• Secondary neoplasms, hearth disease and
infections• < 40% persistent disease
• Secondary neoplasms:– Solid tumors– Acute myeloid leukemia– Non Hodgkin lymphoma
THANK YOU VERY MUCH FOR YOUR
ATTENTION