using and interpreting diabetes data - american association of...
TRANSCRIPT

Using and Interpreting Diabetes Data
Irl B. Hirsch, MDUniversity of Washington
Dualities
• Research: Helmsely Charitable Trust, ADA, JDRF, NIDDK
• Consulting: Abbott Diabetes Care, Roche, Intarcia, Valeritas, Adocia, Big Foot
And if you still don’t trust me…
I will be happy to share my tax forms with you

Raise Your Hand If In Your Practice…
• Every patient gets their meter downloaded
• Every patient gets their pump downloaded
• Every patient gets their CGM downloaded
• No patient gets downloaded, but you encourage your patients to download at home
• If you have at least one computer designated for downloading
• If your downloads are uploaded into your EMR

What You Need (Minimal)
• A program which allows downloading of various meters/pumps/sensors• Clinipro® (Numedics.com), Glooko/Diasend,
Carelink®, Tidepool
• Ideally, many of the native softwares are also available
• A better solution: immediate upload to “the cloud”• Livongo®, Accucheck® Aviva Connect, Dexcom
Clarity

Glucometrics• Analysis of blood glucose data
• To better understand the glycemic fingerprint of each individual patient: A1C, mean, SD, CV, TIR, LBGI
Standard Deviation
Our clinically available measurement of glycemic
variability for both SMBG and CGM
Many other statistical analysis are available but
correlation will be with CGM and outcomes, not
SMBG (current studies and new consensus using
CV)
Can determine both overall and time specific SD
SMBG: I prefer a month of data for less potential
bias/outliers
CGM: 2 weeks is fine
Calculation To Determine SD Target
SD X 2 < mean, may be difficult for some
type 1 patients. Formulas only relevant for
mean BG between 120-180
SD X 3 < MEAN
SMBG
CGM
SD X 3 < MEAN
Better metrics: CV, TIR, TBR, TAR all to
be correlated with outcomes
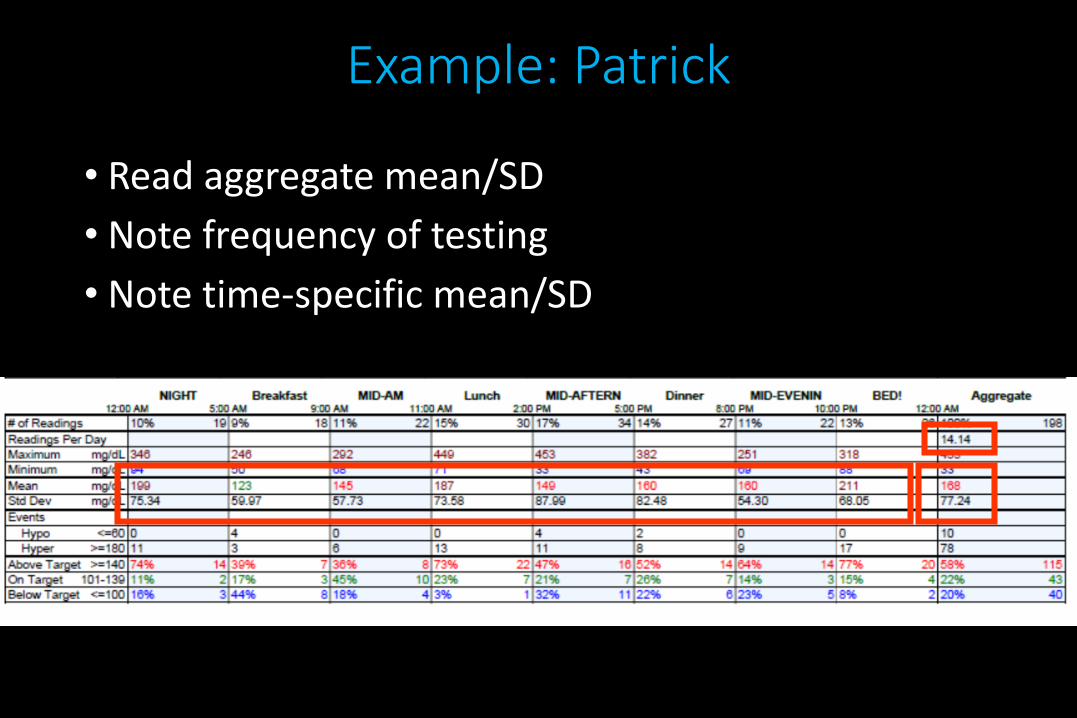
Example: Patrick
• Read aggregate mean/SD
• Note frequency of testing
• Note time-specific mean/SD
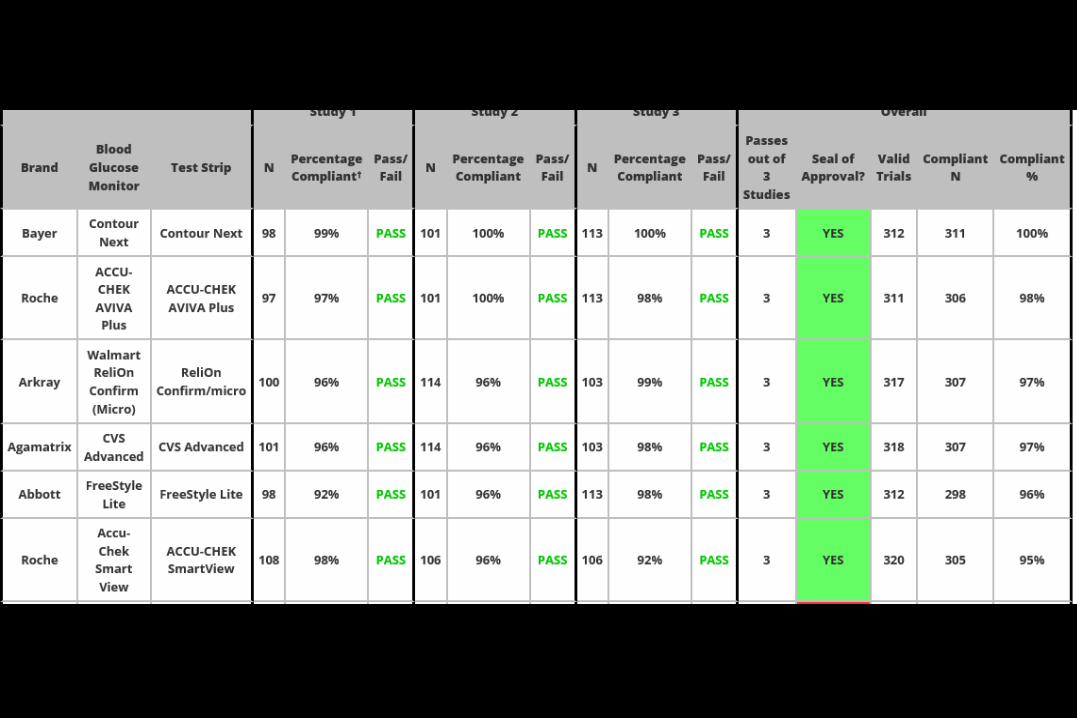
https://www.diabetestechnology.org/surveillance.shtml
Accessed August 18, 2017
N = 1035 for the latest ISO standard (ISO15197-2013)

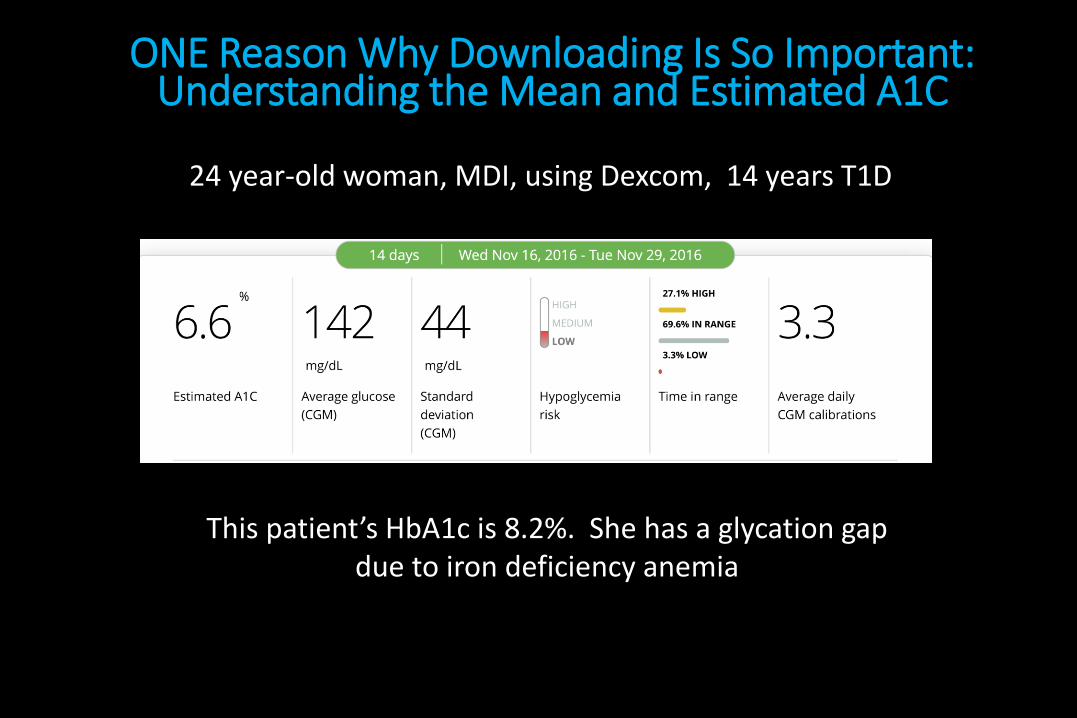
ONE Reason Why Downloading Is So Important: Understanding the Mean and Estimated A1C
This patient’s HbA1c is 8.2%. She has a glycation gap due to iron deficiency anemia
24 year-old woman, MDI, using Dexcom, 14 years T1D
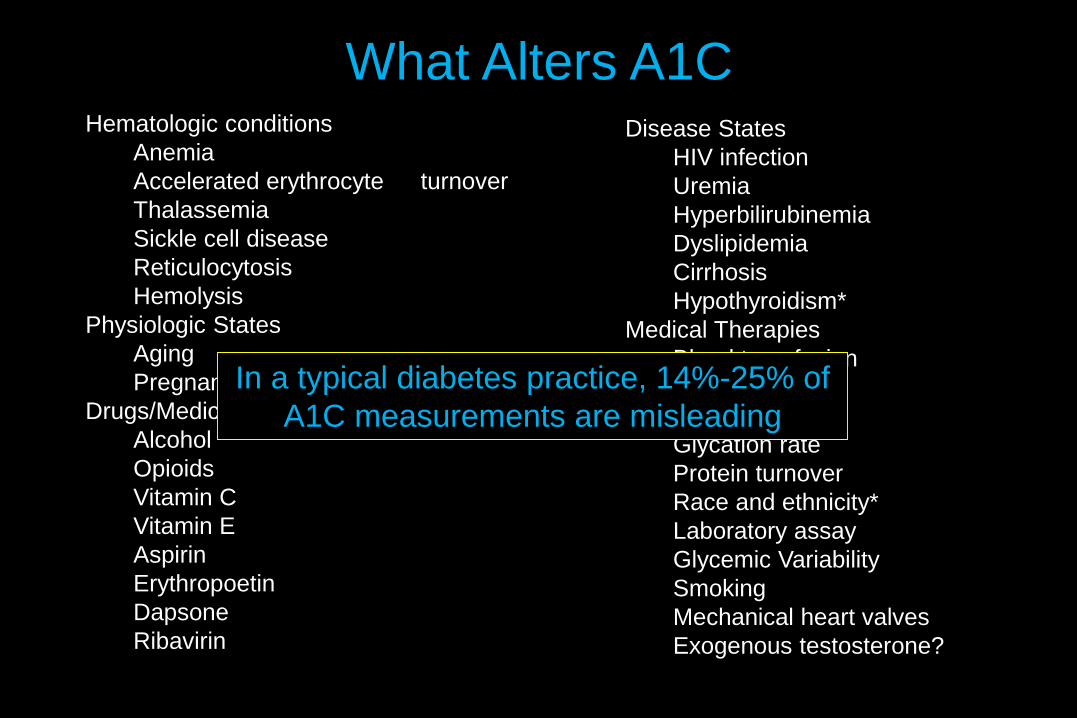
What Alters A1CHematologic conditions
Anemia
Accelerated erythrocyte turnover
Thalassemia
Sickle cell disease
Reticulocytosis
Hemolysis
Physiologic States
Aging
Pregnancy
Drugs/Medications
Alcohol
Opioids
Vitamin C
Vitamin E
Aspirin
Erythropoetin
Dapsone
Ribavirin
Disease States
HIV infection
Uremia
Hyperbilirubinemia
Dyslipidemia
Cirrhosis
Hypothyroidism*
Medical Therapies
Blood transfusion
Hemodialysis
Miscellaneous
Glycation rate
Protein turnover
Race and ethnicity*
Laboratory assay
Glycemic Variability
Smoking
Mechanical heart valves
Exogenous testosterone?
In a typical diabetes practice, 14%-25% of
A1C measurements are misleading

CASE 2
• 45 y/o Ethiopian man moved to Seattle to work as an executive for a coffee company (we don’t have Dunkin’ Donuts’ in Seattle)
• T2DM X 10 years, on insulin X8 years
• BMI 36; A1C 8.7%
• Has been on SAP for 4 years
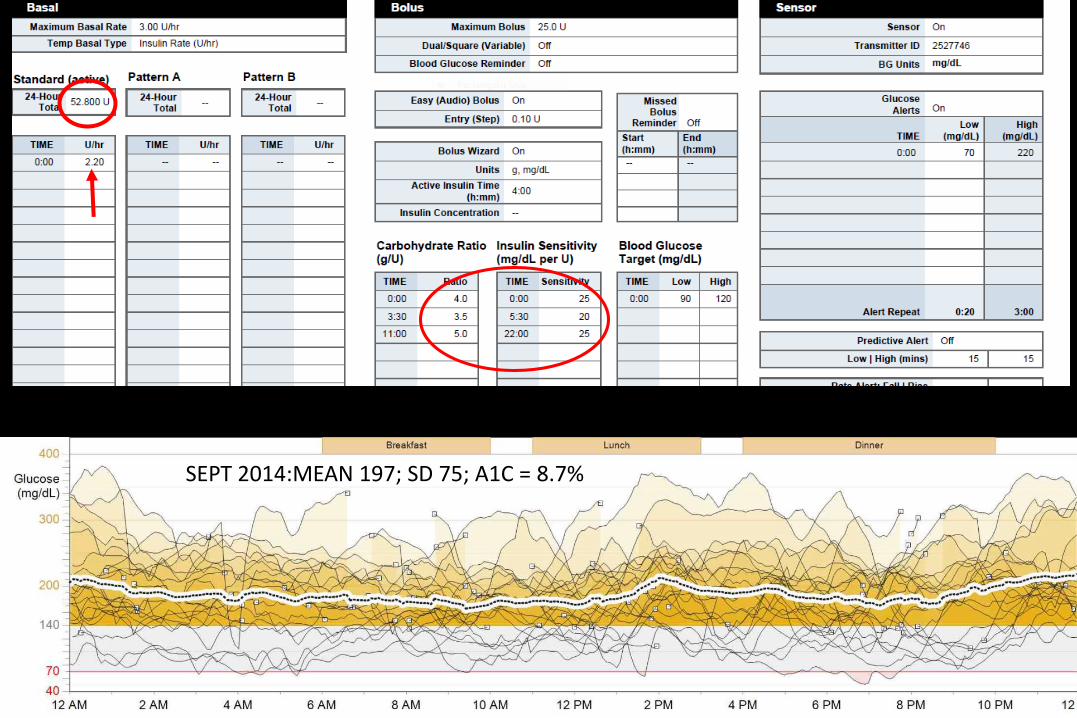
SEPT 2014:MEAN 197; SD 75; A1C = 8.7%

Good basal
60 g CHO
BC: 17U
44 g CHO
BC: 11.5 U
Stayed high: last bolus not enough
No bolus: too much basal?
Insulin given with food
Insulin given with food

With All of This Technology, His Major Problem is Easy (or Should Be) to Fix
• Insulin needs to be given before one eats!
•Why is this so difficult for so many patients?
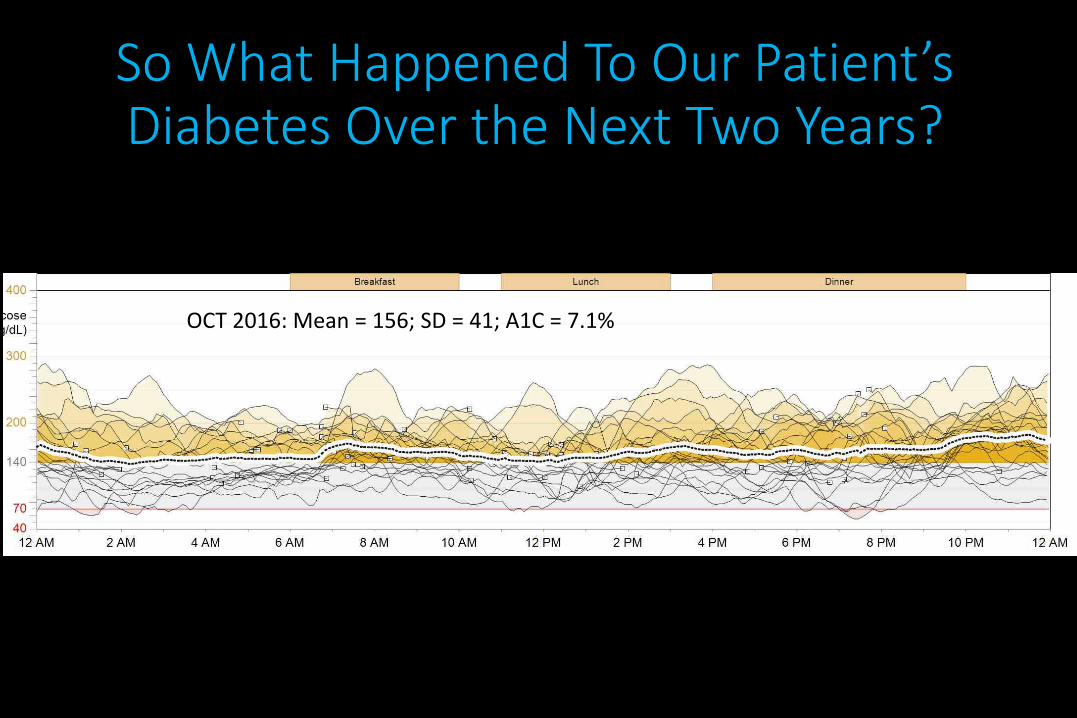
OCT 2016: Mean = 156; SD = 41; A1C = 7.1%
So What Happened To Our Patient’s Diabetes Over the Next Two Years?
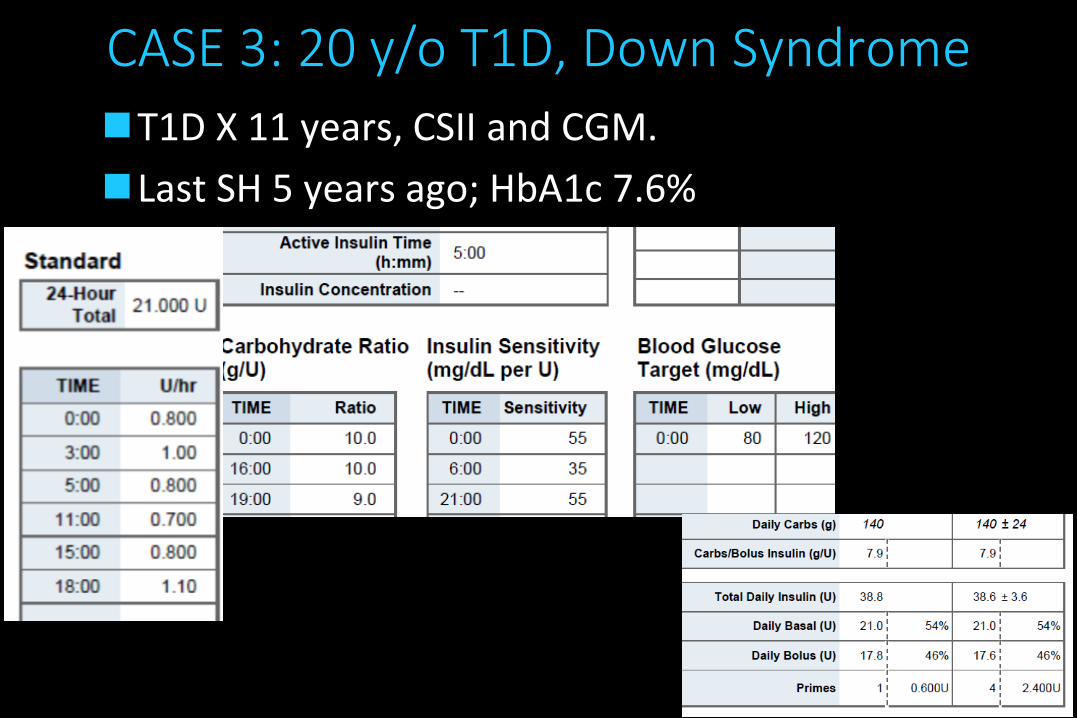
CASE 3: 20 y/o T1D, Down Syndrome
T1D X 11 years, CSII and CGM.
Last SH 5 years ago; HbA1c 7.6%


Hypoglycemic seizure at 1:30am. Why?
High basals in the evening do help to “cushion” dinner but usually result in hypoglycemia if not snacking. Timing of nocturnal basal change is important!
CASE 4-Other Downloading Options
• 44 y/o woman, T1D X 22 years, using Omnipod and Dexcom
• Frustrated with downloading choices
• Decided to try Tidepool (Tidepool.org)
• Last HbA1c 6.8%
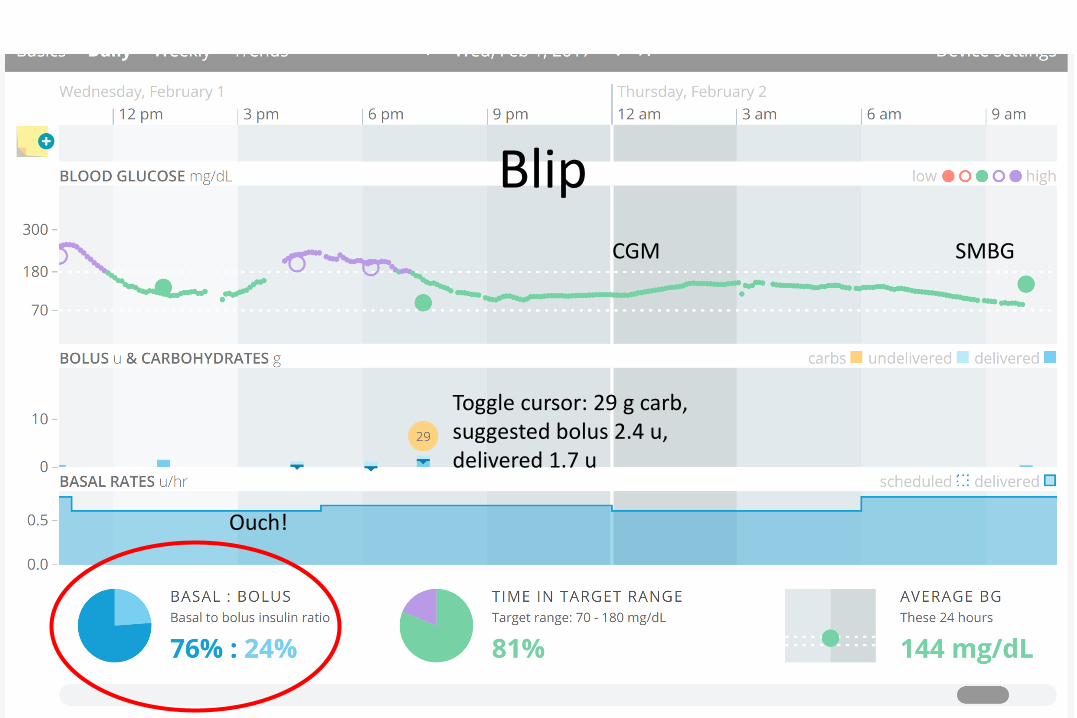
CGM SMBG
Toggle cursor: 29 g carb, suggested bolus 2.4 u, delivered 1.7 u
Ouch!
Blip
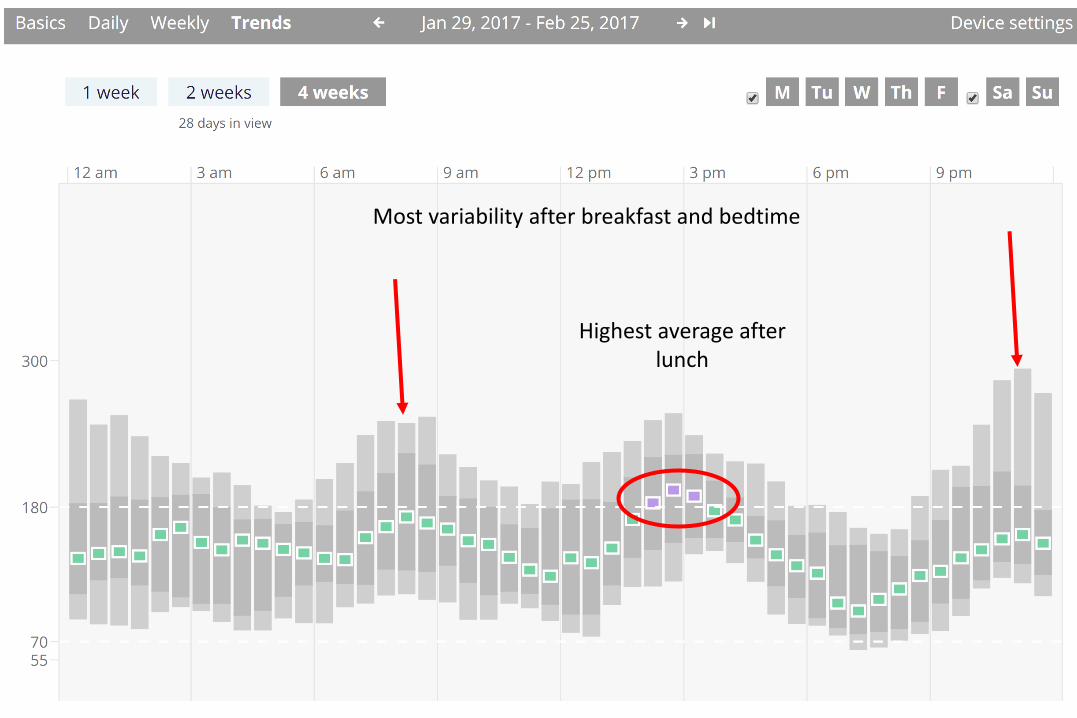
Case 8a: Twin Sister! Dexcom, No Pump
Highest average after lunch
Most variability after breakfast and bedtime

Move the cursor
BAD DAY

GOOD DAY
CASE 5
• 60 y/o woman, 41 years T1D using Animas Vibe
• Past history significant for PDR s/p PRP, DAN with gastroparesis
• After many years of no diagnosis, found in 2010 to have stiff-person’s syndrome
• HbA1c prior to SPS Dx usually in the 7-8% range, after Dxmost in 9-11% range.
• 75-80% of total daily insulin is basal insulin
• What’s going on?

h
Case 5: AGP from 60 y/o Woman with SPSFeb 2016, HbA1c 10.1%
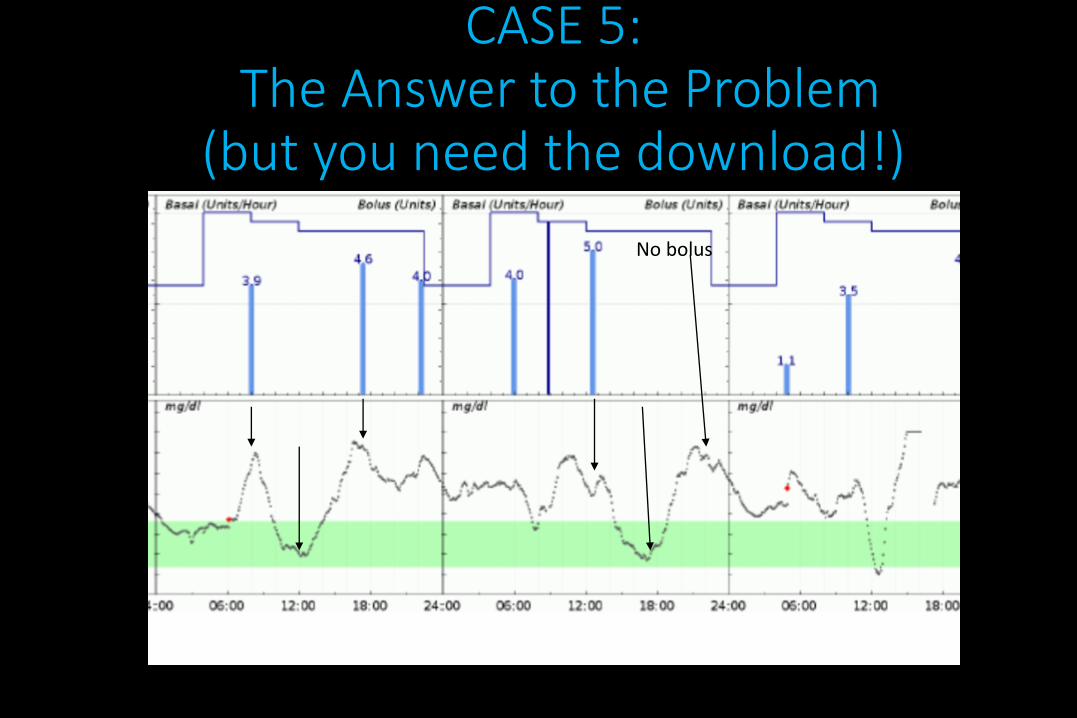
CASE 5:The Answer to the Problem
(but you need the download!)
No bolus

Case 6 : 59 y/o Man, CSII Without CGM
• T1D x 21 years, CSII X 10 years, last seen by an endocrinologist more than 15 years ago
• Referred by concerned family member due to first-ever severe hypoglycemia
• No interest in CGM
• HbA1c ranges 8 to 9.2%, most recent 8.5%
• First visit: 2-3 tests per day, mean/SD 202/85
• Where to start?
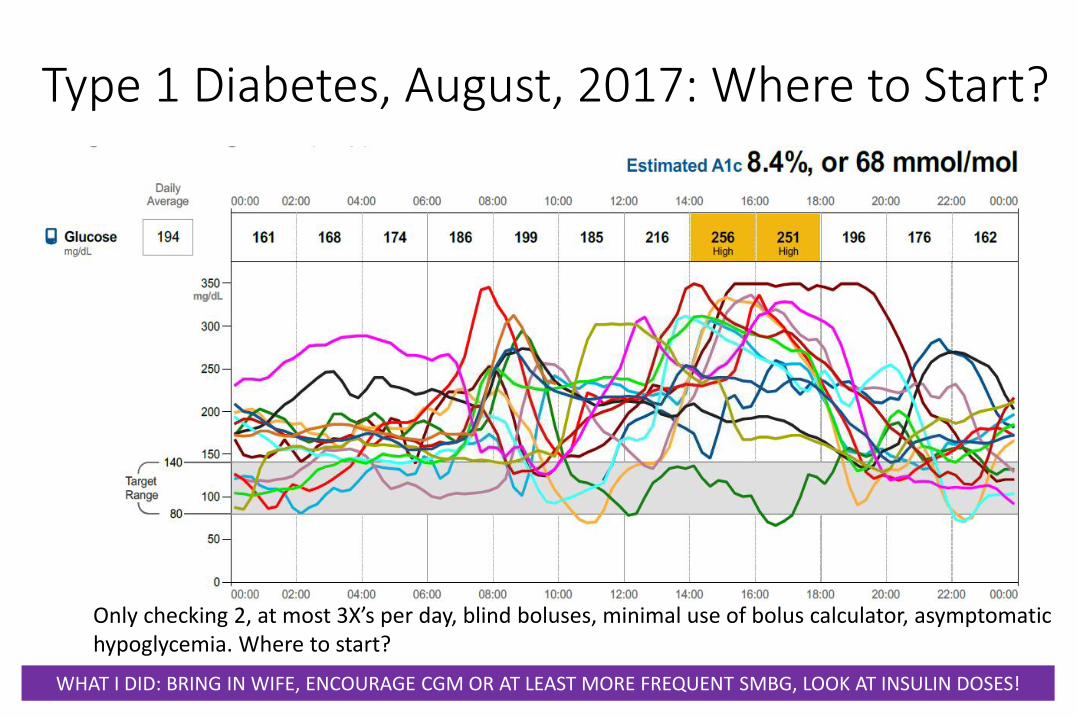
Type 1 Diabetes, August, 2017: Where to Start?
Only checking 2, at most 3X’s per day, blind boluses, minimal use of bolus calculator, asymptomatic hypoglycemia. Where to start?
WHAT I DID: BRING IN WIFE, ENCOURAGE CGM OR AT LEAST MORE FREQUENT SMBG, LOOK AT INSULIN DOSES!
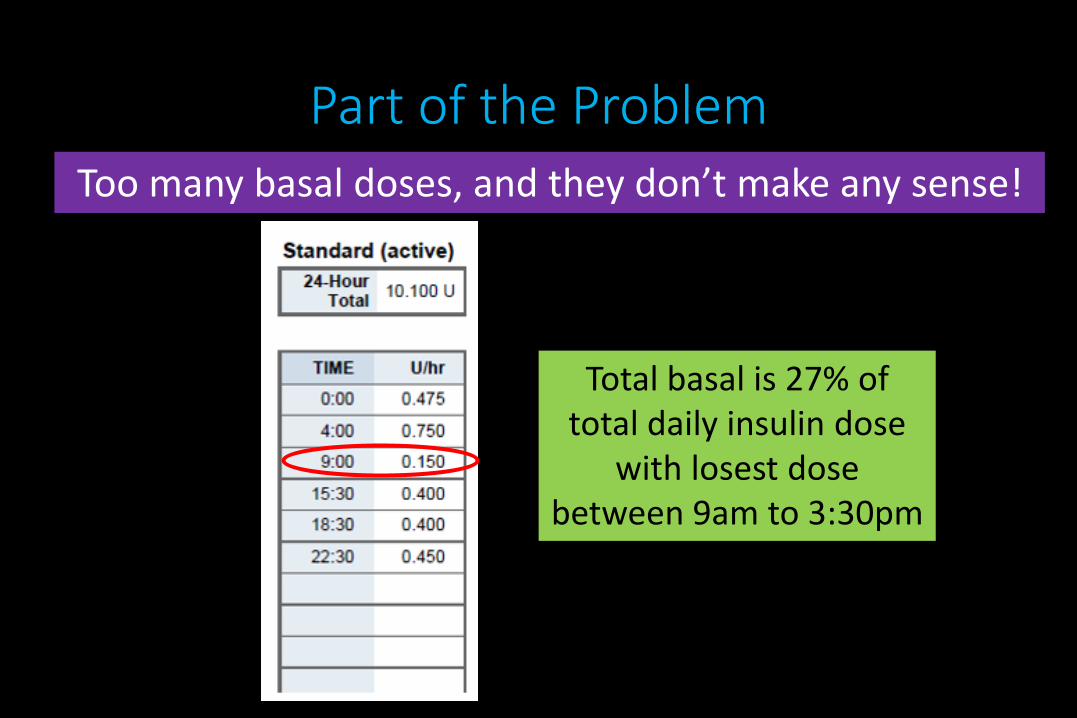
Part of the ProblemToo many basal doses, and they don’t make any sense!
Total basal is 27% of total daily insulin dose
with losest dose between 9am to 3:30pm
Important Point
• In the US, about 30% of our type 1 patients use CSII (60% in the T1D Exchange) and most agree the majority of adult type 1 patients receive their care by non-endocrinologists (one recent estimate was that 2/3 of T1D is only seen by primary care)
• The majority of patients use MDI-will closed loop systems increase CSII use for those who are cared for by both endocrinologists and non-specialists?
• DIAMOND and GOLD studies (JAMA, 2017): outcomes improved with CGM and MDI
What About the 70% of T1D Who Use MDI?
• Companion Medical “InPen” system
• Approved by FDA 8/16, to be launched 2017 (?)
• Will track prandial insulin doses (cartridge pens) and send to paired app via Bluetooth
• App also includes a bolus calculator (with real-time IOB)
• Many other companies working on these blue-tooth enabled insulin pens

What does it look like?

Sensors: Continual Evolution For the Near Future
Guardian Sensor 3
Dexcom Gen 6
Freestyle Libre
Sensionics Implantable Sensor
Glysense Implantable Sensor
Raise you hand if you use the FreeStyle Libre Pro routinely in your practice?

What’s Going On?
• 85 y/o man, no cognitive concerns, changed 5 years ago to multiple injections from 70/30 premix
• Mean/SD on glucose testing at home 185/60 testing 2.5 times daily on meter first started to use 18 months ago
• HbA1c now 11.8%
• What to do?

No glycation gap! Not enough blood on “new” CMS meter, readings consistently low when compared to FGM

Fingerstick BG 95 162 188

Sometimes the FLP Gives Us “TMI”
• 32 y/o woman with 14 years T1D, divorced for 1 year. Works as a commercial realtor. No children
• On MDI, stopped CGM as it “inhibits my social life”
• Agreed to wear FLP for 14 days
• Conclusion?

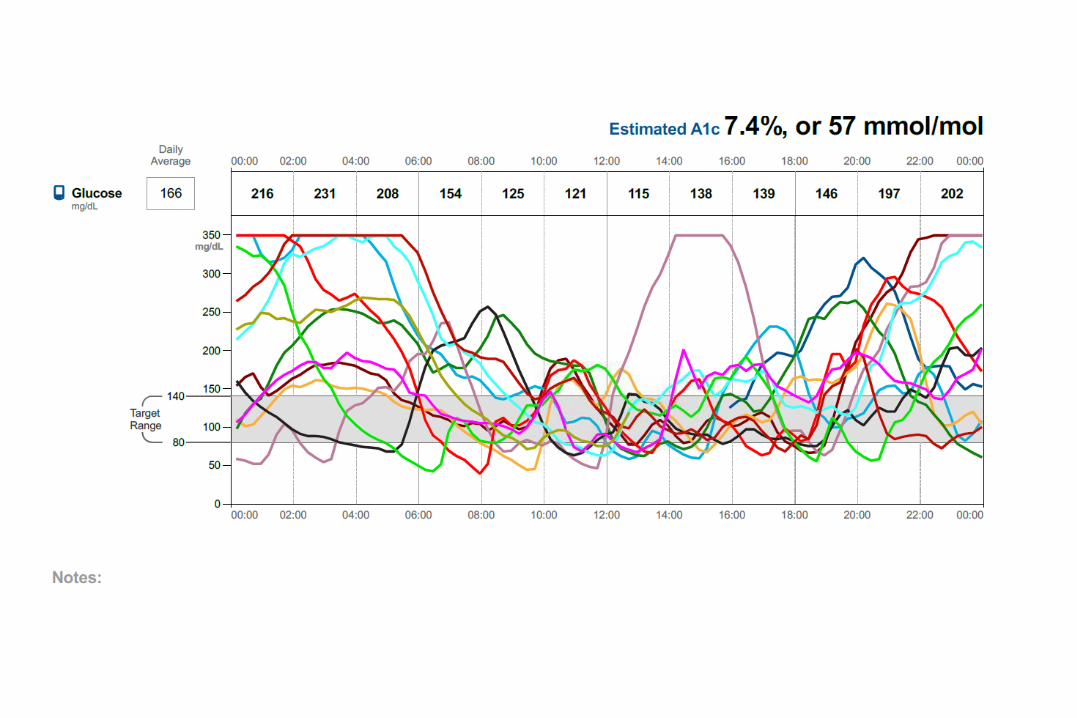
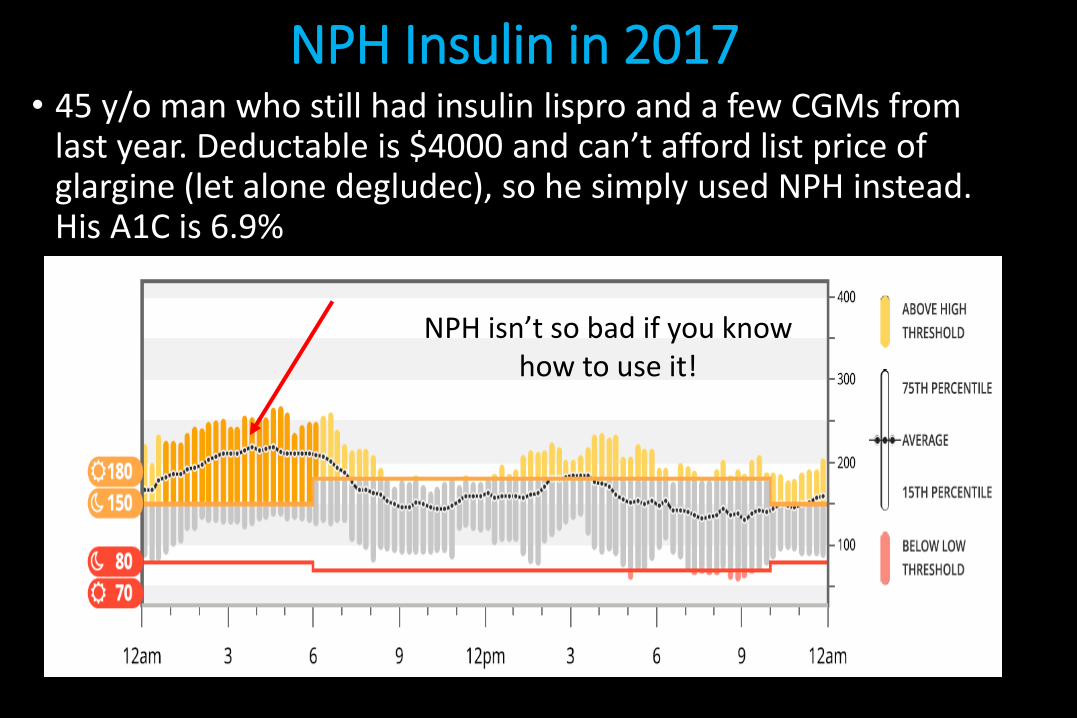
NPH Insulin in 2017• 45 y/o man who still had insulin lispro and a few CGMs from
last year. Deductable is $4000 and can’t afford list price of glargine (let alone degludec), so he simply used NPH instead. His A1C is 6.9%
NPH isn’t so bad if you know how to use it!

NPH and Regular, August 201755 y/o man, T1D for more than 40 years. Can’t
afford analogue insulin

Raise Your Hand if You Have Patients on Our First Hybrid Closed Loop?
•Patient still needs to bolus for meals and notify the system for exercise.
•Won’t be for everyone-many love it, others don’t want the extra burden on their diabetes, yet others don’t find it aggressive enough.

Key Pearls for 670G for Hybrid Closed Loop
• Patients HAVE to use bolus calculator for “auto mode” to engage
• In “auto mode”, glycemia is maintained by changing basal doses
• Manual mode basal rates have no bearing in auto mode
• Meal doses: generally need higher doses (ICR), IOB 2-3 hours work best; algorithm determines auto basal, ISF, targets!
• Programmed manual mode ISF dose not apply in auto mode
• Calibration of CGM: 3-4 times daily
Conclusion
• Technology for MDI is finally improving, but still a lot of problems with SMBG accuracy and understanding of HbA1c
• Downloading should be part of the “vital signs” for every patient using a meter, pump, or sensor
• The downloading software is improving, is connected to the cloud, and should assist us in helping our patients
• How the endocrinologist can efficiently utilize all of this technology in our current system requires further research