versus living transplantation - surgery journalwael mansy, division of hepato-pancreatico-biliary...
TRANSCRIPT
Remedy Publications LLC., | http://clinicsinsurgery.com/
Clinics in Surgery
2020 | Volume 5 | Article 27081
Factors Affecting HCC Recurrence Post Liver Resection versus Living Transplantation
OPEN ACCESS
*Correspondence:Wael Mansy, Division of Hepato-
Pancreatico-Biliary Surgery, Zagazig University, Egypt,
E-mail: [email protected] Date: 02 Dec 2019Accepted Date: 06 Jan 2020Published Date: 16 Jan 2020
Citation: Mohamed M, Mansy W,
Elhendawey S, Basyouny M, Boudjema K. Factors Affecting HCC
Recurrence Post Liver Resection versus Living Transplantation. Clin
Surg. 2020; 5:
2708.
Copyright © 2020 Wael Mansy. This is an open access article distributed
under the Creative Commons Attribution License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Research ArticlePublished: 16 Jan, 2020
AbstractBackground: Liver resection, liver transplantation and loco-regional ablation (Radiofrequency Ablation (RFA), Microwave Ablation (MWA) and Trans-Arterial Chemo-Embolization (TACE)) are the optimal ways of HCC management. The optimal treatment for HCC has long been debated according to patient condition.
Patients and Methods: A retrospective study from January 2012 till March 2019 on 118 patients with HCC (58 patients underwent Hepatic Resection (HR) and 58 patients underwent LDLT).
Results: There was no significant difference between the HR group and LDLT group regarding the overall survival and disease-free survival. Overall survival at 1, 3 and 5 yrs. was 94.9%, 78% and 74.5% in LDLT group while was 89.83%, 71.19% and 62.71% in HR group respectively. Disease free survival at 1, 3 and 5yrs. was 88.1%, 62.7% and 61.01% in LDLT group while was 83.05%, 57.63% and 50.85% in HR respectively.
Conclusion: In management of early stage HCC HR should be considered an alternative to LDLT. The most important factors affecting HCC recurrence were tumor behavior and preoperative AFP.
Keywords: Hepatic resection; Living donor liver transplant; Hepatocellular carcinoma; Recurrence
Morsi Mohamed1, Wael Mansy1*, Sayed Elhendawey2, Mohamed Basyouny3 and karim Boudjema4
1Hepato-Pancreatico-Biliary Surgery Department, Zagazig University, Egypt
3FRCS, Liver Transplant Unit, Maadi Armed Forces Medical Compound, Egypt4Liver Transplant and Hepatobiliary Surgery Department, Rennes University, France
IntroductionHCC considered among the commonest and lethal malignant tumors in the world [1]. Different
modalities persist for HCC management either, surgical treatment including Hepatic Resection (HR) and Liver Transplantation (LT), or intervention treatments such as RFA, MWA and TACE [2]. Surgical management is conventional treatment modality that can offer long-term survival for HCC patients [3,4].
For locally confined HCC, Surgical resection has been generally accepted as the treatment of choice [5]. The advantage of HR is to prolong overall survival and to improve quality of life via eradicating the tumor while preserving hepatic function [6]. According to these advantages (despite there are no strict criteria) patients with solitary focal lesions (<5 cm) confined to one lobe without vascular invasion and with well-preserved hepatic function are the best candidates for HR [7].
Liver transplantation is considered superior to HR because it allows treatment of the underlying liver disease, radical resection of the primary tumor, treatment of the portal hypertension, and reduces the risk of de novo lesions and progression to end-stage liver failure [8]. Cirrhotic patients with early HCC have 4-5 year overall survival rates of 70% after LT [5,6,9].
Patient and MethodsThis is a retrospective study done between January 2012 and March 2019. We had 118 patients
with HCC. LR done for 59 patients in Advanced Hepato-Pancreatico-Biliary Centre in Zagazig University and LDLT done for another 59 patients in liver transplant unit in El- Maadi Military Medical Compound, Egypt.
Routine laboratory investigations done for all patients (CBC, KFT, LFT, coagulation profile and AFP). Triphasic CT used for diagnosis. Also, CT chest and bone scan to rule-out metastases.
2General Surgery Department, Zagazig University Hospital, Egypt

Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27082
We analyzed tumor size, number and pathological findings. Also, Operative data regarding surgical procedures, operation length, volume of blood loss, intra-operative blood and plasma transfusion and postoperative complications were recorded.
The indication for HR was child A or early B, platelet count >50, good performance status and single focal lesion. While indications for LDLT was Milan criteria. Right lobe graft was the decision in all patients (Figure 1 and 2).
Hepatic resection distributed as follows:
1. Non-anatomical resection in 17 patients.
2. Anatomical resection in 42 patients.
a. Left lateral resection in 14 patients
b. Right posterior resection in 6 patients
c. Segmentectomy in 22 patients (caudate resection in 5).
For LDLT preoperative loco-regional management was as follows:
1. TACE in 25 patients.
2. MWA in 2 patients.
3. Combined MWA & TACE in 3 patients.
Immunosuppressant regimen was methylprednisolone, plus Calcineurin Inhibitors (CNI), such as tacrolimus plus mycophenolate mofetil. When patients develop complications from tacrolimus; we shift to mammalian Target of Rapamycin (m-TOR) inhibitors (everolimus or sirolimus).
All patients were followed-up at 1year, 3 and 5 years respectively. We depended on AFP level and Triphasic CT to assess tumor recurrence during follow-up.
The aim of this study is to detect HCC recurrence after HR and LDLT. Find the factors affecting HCC recurrence. Also, to compare between LDLT and HR regarding Overall Survival (OS) and Disease-Free Survival (DFS). Overall Survival (OS) was calculated from date of diagnosis till date of death or date of last follow up. Disease Free Survival (DFS) was calculated from date of transplantation till date of recurrence or death or last follow-up for those who not recurred.
Statistical AnalysisData was analyzed using IBM SPSS advanced statistics version 22
(SPSS Inc., Chicago, IL). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Survival analysis was done using Kaplan-Meier method and comparison between two survival curves was done using log-rank test. Cox-regression method was used for calculation of the Hazard Ratio (HR) with its 95% Confidence Interval (CI) was used for risk estimation. All tests were two-tailed. A p-value <0.05 was considered significant.
ResultsFifty three males and 6 females included in LDLT group with
mean age 52. While 45 males and 14 females included in HR group with mean age 59. Hepatitis C virus infection was the sole cause of cirrhosis in the vast majority of patients in both groups (54 (91.6%) patients in LDLT group and 53 (89.83%) patients in HR group). Most of our patients were having Child score A in both groups (38 patients (64.4%) patients in LDLT group while 48 (81.36%) patients in HR).
Regarding the size and number of focal lesions in our study. In LDLT group, one lesion was in 30 (50.8%), two lesions were in 18 (30.5%), 10 patients (16.9%) had 3 lesions and only one patient (1.7%) had 4 lesions. The size of the single HCC lesion or the biggest lesion in multiple tumors was ranging from 1.5 cm to 5 cm with a mean of 3.5 cm. While in HR group, all patients had solitary lesion and most of these lesions (47 patients (79.66%)) had size <5 cm.
AFP level in LDLT group varied as in 49 patients (83.1%) the level was less than 400 ng/ml, while only in 10 patients (16.9%) the level was more than 400 ng/ml, reaching in 3 patients only more than 1000 ng/ml. In HR group, 52 patients (88.14%) were less than 400 ng/ml and 7 patients (11.86%) were more than 400 ng/ml.
Mean operative time was 10 ± 2.1 h in LDLT group, but in HR group was 4 ± 1.7 h. Packed RBCs transfusion was 6 ± 4.3 units in LDLT group while was 2 ± 2.8 units in HR group. FFP transfusion was 12.8 ± 7.5 units in LDLT group, while was 4 ± 2.5 units in HR group.
In LDLT group, median graft size was 785 g. While median of GRWR was 0.85. CIT (Cold Ischemia Time) was 41 ± 6 min and WIT (Worm Ischemia Time) median was 45 ± 23 min.
Pathological finding in LDLT group, among 24 patients having single focal lesion; capsular invasion was detected in 5 explanted liver patients only. Microvascular invasion was detected in the explanted liver in 16 patients (27.1%) while 43 patients (72.9%) were free.
Figure 1: Hepatic resection for HCC. A) HCC segment II, III. B) Left lateral hepatectomy. C) Resection bed. D) 5 years after resection.
Figure 2: Follow up post liver transplantation for HCC. A) Right lobe HCC. B) 1year post LDLT. C) 3 years post LDLT. D) 5 years post LDLT.
Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27083
Lymph node metastasis was negative in all patients. Post-operative pathological finding in HR, all patients had grade II tumour. Most of the patients 40 (67.8%) had well differentiated tumour, while 15 (25.4%) patients had capsular infiltration.
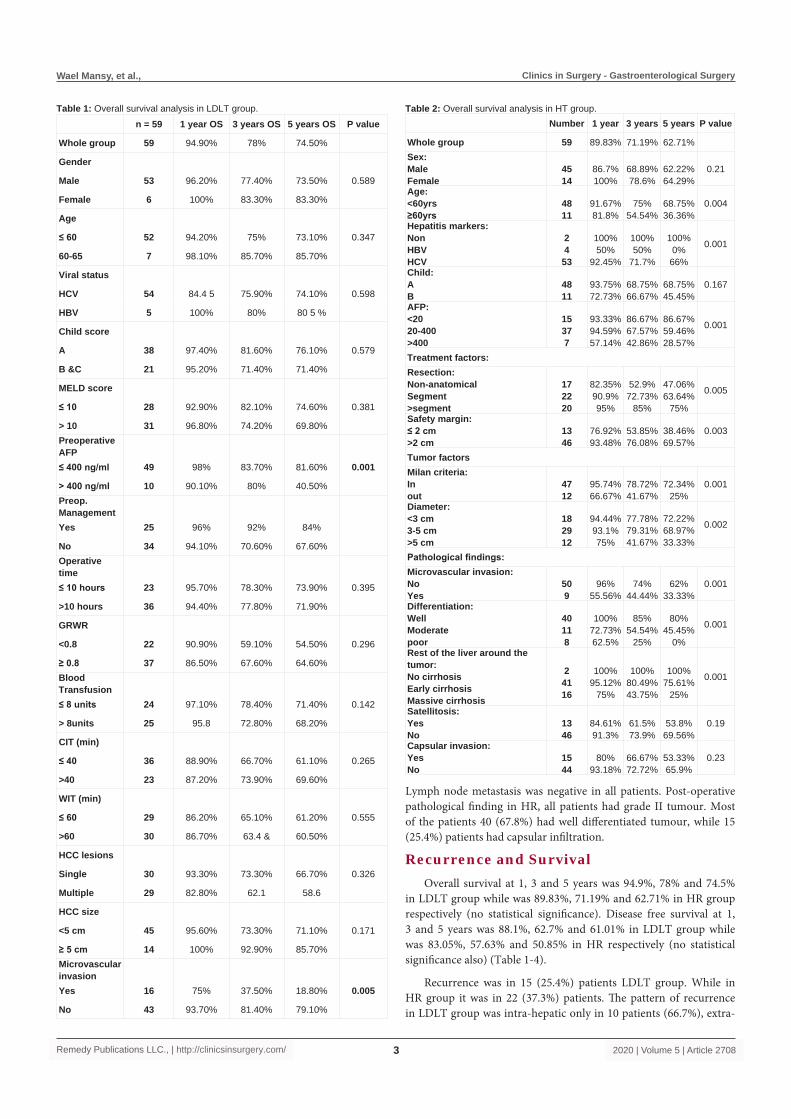
Recurrence and SurvivalOverall survival at 1, 3 and 5 years was 94.9%, 78% and 74.5%
in LDLT group while was 89.83%, 71.19% and 62.71% in HR group respectively (no statistical significance). Disease free survival at 1, 3 and 5 years was 88.1%, 62.7% and 61.01% in LDLT group while was 83.05%, 57.63% and 50.85% in HR respectively (no statistical significance also) (Table 1-4).
Recurrence was in 15 (25.4%) patients LDLT group. While in HR group it was in 22 (37.3%) patients. The pattern of recurrence in LDLT group was intra-hepatic only in 10 patients (66.7%), extra-
n = 59 1 year OS 3 years OS 5 years OS P value
Whole group 59 94.90% 78% 74.50%
Gender
Male 53 96.20% 77.40% 73.50% 0.589
Female 6 100% 83.30% 83.30%
Age
≤ 60 52 94.20% 75% 73.10% 0.347
60-65 7 98.10% 85.70% 85.70%
Viral status
HCV 54 84.4 5 75.90% 74.10% 0.598
HBV 5 100% 80% 80 5 %
Child score
A 38 97.40% 81.60% 76.10% 0.579
B &C 21 95.20% 71.40% 71.40%
MELD score
≤ 10 28 92.90% 82.10% 74.60% 0.381
> 10 31 96.80% 74.20% 69.80%Preoperative AFP≤ 400 ng/ml 49 98% 83.70% 81.60% 0.001
> 400 ng/ml 10 90.10% 80% 40.50%Preop. ManagementYes 25 96% 92% 84%
No 34 94.10% 70.60% 67.60%Operative time≤ 10 hours 23 95.70% 78.30% 73.90% 0.395
>10 hours 36 94.40% 77.80% 71.90%
GRWR
<0.8 22 90.90% 59.10% 54.50% 0.296
≥ 0.8 37 86.50% 67.60% 64.60%Blood Transfusion≤ 8 units 24 97.10% 78.40% 71.40% 0.142
> 8units 25 95.8 72.80% 68.20%
CIT (min)
≤ 40 36 88.90% 66.70% 61.10% 0.265
>40 23 87.20% 73.90% 69.60%
WIT (min)
≤ 60 29 86.20% 65.10% 61.20% 0.555
>60 30 86.70% 63.4 & 60.50%
HCC lesions
Single 30 93.30% 73.30% 66.70% 0.326
Multiple 29 82.80% 62.1 58.6
HCC size
<5 cm 45 95.60% 73.30% 71.10% 0.171
≥ 5 cm 14 100% 92.90% 85.70%Microvascular invasionYes 16 75% 37.50% 18.80% 0.005
No 43 93.70% 81.40% 79.10%
Table 1: Overall survival analysis in LDLT group.Number 1 year 3 years 5 years P value
Whole group 59 89.83% 71.19% 62.71%Sex:MaleFemale
4514
86.7%100%
68.89%78.6%
62.22%64.29%
0.21
Age:<60yrs≥60yrs
4811
91.67%81.8%
75%54.54%
68.75%36.36%
0.004
Hepatitis markers:NonHBVHCV
24
53
100%50%
92.45%
100%50%
71.7%
100%0%
66%
0.001
Child:AB
4811
93.75%72.73%
68.75%66.67%
68.75%45.45%
0.167
AFP:<2020-400>400
15377
93.33%94.59%57.14%
86.67%67.57%42.86%
86.67%59.46%28.57%
0.001
Treatment factors:Resection:Non-anatomicalSegment>segment
172220
82.35%90.9%95%
52.9%72.73%
85%
47.06%63.64%
75%
0.005
Safety margin:≤ 2 cm>2 cm
1346
76.92%93.48%
53.85%76.08%
38.46%69.57%
0.003
Tumor factorsMilan criteria:Inout
4712
95.74%66.67%
78.72%41.67%
72.34%25%
0.001
Diameter:<3 cm3-5 cm>5 cm
182912
94.44%93.1%75%
77.78%79.31%41.67%
72.22%68.97%33.33%
0.002
Pathological findings:Microvascular invasion:NoYes
509
96%55.56%
74%44.44%
62%33.33%
0.001
Differentiation:WellModeratepoor
40118
100%72.73%62.5%
85%54.54%
25%
80%45.45%
0%
0.001
Rest of the liver around the tumor:No cirrhosisEarly cirrhosisMassive cirrhosis
24116
100%95.12%
75%
100%80.49%43.75%
100%75.61%
25%
0.001
Satellitosis:YesNo
1346
84.61%91.3%
61.5%73.9%
53.8%69.56%
0.19
Capsular invasion:YesNo
1544
80%93.18%
66.67%72.72%
53.33%65.9%
0.23
Table 2: Overall survival analysis in HT group.

Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27084
hepatic only in 2 patients (13.3%) (One patient developed bone mets and the other one developed lung mets) and mixed intra and extra-hepatic in 3 patients (20%). Two patients had recurrence twice and 1 patient had recurrence three times. The pattern of recurrence in HR group was Intra-hepatic in all patients.
In LDLT group management was as follows:1. Resection once in 3 patients.
2. Resection 3 times in 1 patient.
3. TACE and resection in 1 patient.
4. RFA in 1 patient.
5. Radiotherapy to bone metastasis in 1 patient.
6. Sorafenib in 1 patient.
7. Supportive treatments in 7 patients.
8. One patient needed re-transplant.
In HR group management was as follows:1. RFA in 3 patients.
2. TACE in 7 patients.
3. Sorafenib in 2 patients.
4. Supportive treatments in 10 patients.
Regarding mortality, 17 patients died in LDLT group:1. HCC recurrence in 9 (52.9%) patients.
2. Due to other causes in 8 (47.1%) patients:
a. Biliary complications in 3 patients.
b. Rejection in 1 patient.
c. Primary non-function graft in 1 patient.
d. Fungal infection in 1 patient.
e. Stroke in 1 patient.
f. Myocardial infarction in 1 patient.
While 21 patients died in HR group:1. HCC recurrence in 14 (66.67%) patients.
2. Due to other causes in 7 (33.33%) patients:
a. Liver cell failure in 4 patients.
b. Stroke in 1 patient.
c. Myocardial infarction in 1 patient.
d. MVO in 1 patient.
In LDLT group, Survival analysis regarding overall survival and recurrence free survival we found that AFP level, micro-vascular invasion in the explanted liver were independent risk factors. Also, Preoperative management was very close to be significant. While the other proposed factors failed to show any significance.
In HR group, Survival analysis regarding overall survival and recurrence free survival showed we found that patient factors (age, viral status and AFP level), tumor factors (Milan criteria, size of the tumor, micro-vascular invasion, tumor differentiation and degree of cirrhosis) and treatment factors (type of resection and safety margin)
n=59 1 year DFS 3 years DFS
5 years DFS P-value
Whole group 59 88.10% 62.70% 61.01%
Gender
Male 53 88.70% 60.40% 58.50% 0.316
Female 6 83.30% 83.30% 83.30%
Age
≤ 60 52 86.50% 61.50% 59.60% 0.496
>60 7 100% 85.70% 71.40%
Viral status
HCV 54 87% 61.10% 59.30% 0.375
HBV 5 100% 80% 80%
Child score
A 38 86.80% 63.20% 60.50% 0.618
B &C 21 90.50% 61.90% 61.90%
MELD score
≤ 10 28 92.90% 64.30% 64.30% 0.113
> 10 31 83.90% 61.30% 58.10%Preoperative AFP< 400 ng/ml 49 91.80% 73.50% 73.50% <0.001
≥ 400 ng/ml 10 70% 20% 0.00%
< 200 ng/ml 39 92.30% 76.90% 76.90% <0.001
≥ 200 ng/ml 20 80% 35% 30%Pre-op. ManagementYes 25 88% 76% 76% 0.053
No 34 88.20% 52.90% 50%Operative time≤ 10 hours 23 91.30% 65.20% 60.90% 0.979
>10 hours 36 86.10% 61.10% 61.10%
GRWR
≤ 0.8 22 90.90% 54.50% 54.50% 0.296
> 0.8 37 86.50% 67.60% 64.90%Blood Transfusion≤ 8 units 24 94.30% 74.30% 74.30% 0.115
> 8units 25 81.20% 65.80% 61.70%
CIT (min)
≤ 40 36 88.90% 55.60% 55.60% 0.285
> 40 23 87% 73.90% 69.60%
WIT (min)
≤ 60 29 86.20% 62.10% 62.10% 0.595
> 60 30 90% 63.30% 60%
HCC lesions
Single 24 91.70% 70.80% 66.70% 0.524
Multiple 35 85.70% 57.10% 57.10%
HCC size
< 5 cm 45 87.20% 61.70% 59.60% 0.137
≥ 5 cm 14 91.70% 66.70% 66.70%Microvascular invasionYes 16 75% 18.80% 12.50% <0.001
No 43 93% 79.10% 79.10%
Table 3: Recurrence free survival analysis in LDLT group.

Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27085
were independent risk factors. While the other proposed factors failed to show any significance.
DiscussionHepatocellular carcinoma represents the 5th most frequent
malignant tumor in the world and the 3rd cause of death due to cancer [10]. Cirrhotic Patients are at substantial risk for HCC; the yearly incidence in such patients is 3%. The prognosis is poor, because the number of newly discovered cases roughly equals the number of deaths [4].
In the first-line treatment of early HCC, the selection of three main curative therapies (loco-regional, LR and LT) had been intensively investigated [11,12]. Many factors affect selection as,
N. 1 year 3 years 5 years P value
Whole group 59 83.05% 57.63% 50.85%
Patient factors:Sex:MaleFemale
4514
82.22%85.7%
55.56%57.14%
51.11%50%
0.26
Age:<60 yrs≥ 60 yrs
4811
87.5%63.63%
60%45.45%
56.25%27.27%
0.002
Hepatitis markers:NonHBVHCV
2453
100%50%
84.9%
100%50%
56.56%
100%0%
52.8%
0.001
Child:AB
4811
85.41%72.72%
58.33%54.54%
50%45.45%
0.257
AFP:<2020-400>400
15377
86.67%86.49%57.14%
73.33%54.06%32.86%
66.67%48.65%28.57%
0.003
Treatment factors:Resection:Non-anatomicalSegment>segment
172220
70.59%81.82%
95%
41.18%63.64%
65%
35.29%54.54%
60%
0.002
Safety margin:≤ 2 cm>2 cm
1346
61.54%89.13%
38.46%65.22%
30.77%56.52%
0.001
Tumor factorsMilan criteria:Inout
4712
89.36%58.33%
63.83%33.33%
57.45%25%
0.001
Diameter:<3 cm3-5 cm>5 cm
182912
94.44%86.22%58.33%
66.67%58.6%41.67%
61.11%51.72%33.33%
0.001
Pathological finding:Microvascular invasion:NoYes
509
90%44.44%
62%33.33%
56%22.22%
0.001
Differentiation:WellModeratepoor
40118
95%63.64%
50%
72.5%36.36%
25%
67.5%27.27%
0%
0.001
Rest of the liver around the tumor:No cirrhosisEarly cirrhosisMassive cirrhosis
24116
100%87.8%68.75%
100%63.41%37.5%
100%75.61%
25%
0.002
Satellitosis:YesNo
1346
76.92%84.78%
53.85%58.69%
46.15%52.17%
0.25
Capsular invasion:YesNo
1544
80%84.09%
53.33%59.1%
46.67%52.27%
0.19
Table 4: Recurrence free survival analysis in HR group. tumor characteristics (number, location, size and vascular invasion) and patient status (liver function, performance status, portal hypertension and child score). Additionally, other external factors also had impact on treatment selection. One of the most important factors was the contradiction between increasing demand of LT and the deficiency of organ donors [13]. Taking into consideration both urgency and cost-effectiveness, LT now used to be recommended as a second-line treatment for very early HCC [14].
Our study was to compare factors affecting recurrence between HR and LDLT for HCC using data from two centers in Egypt. The overall survival after 5 years was 74.5% and 62.71% after LDLT and HR respectively and recurrence free survival after 5 years was 61.01% and 50.85% after LDLT and HR respectively. The recurrence rate was 25.4% after LDLT, while was 37.3% after HR. It was clearly demonstrated that there was no statistically difference between the two groups. This was due to two reasons; first, most of our patients that underwent HR were child A, with AFP <400 ng/ml, good general performance with early cirrhosis and had early stage HCC. Second in LDLT group, we depend completely on living donation and also, we might have different HCC pathology than elsewhere as we have different form of HCV infection (genotype). This result may encourage the transplant community in Egypt to develop new criteria based on the findings drawn from our patients.
The results of our study were similar to the study of Kaido et al. [15]. Who reported that there was no significant difference among the two groups (OS 5 years was 53% in HR and 63% in LT) but he noticed that the 5 years recurrence rate was significant less in LT (21%) than HR (74%). Dhir et al. [16] recently carried a meta-analysis of 10 published reports to compare survival outcomes after HR and LT in patients with early HCC, namely, within the Milan criteria, and well-compensated cirrhosis. The meta-analysis of all 10 published studies discovered a survival advantage for LT (P=0.027). Most recently, Proneth et al. [17] found that no survival advantage of LT could be found compared with HR in a meta-analysis by use of 7 studies with a total of 1572 patients.
LT found to be a better option for HCC patients with severe fibrosis or cirrhosis (fibrosis score 5-6), but LT was not superior to LR for patients with none to moderate fibrosis (fibrosis score 0-4) [18]. And this was similar to the study of Yang et al. [13].
Patient selection using Milan criteria yields 4-5 years overall survival rates of 70%, with recurrence rates of 15% [19]. In our study, the 5 years. Survival post LDLT was 75.7%. While post LR was 72.34%. A US group notified a 5-year survival rate of 70% after HR for patients with transplantable HCC [20]. In Chinese cirrhotic patients with HCC that met the Milan criteria, a 5-year survival rate of 66% was found [5]. The results of our study were similar to these two series, because of, most of our patients had solitary lesion with good hepatic reserve. This had significance that Milan criteria affect HCC recurrence post resection.
While the Milan Criteria (MC) considered the benchmark for the selection of candidates for LT, recurrence of HCC still occurs in 10% to 20% of patients within the first 5 yrs after LT. It has become strongly evident that additional factors beyond the number and size of HCC are important determinants of outcome. Identification of biologic and tumor markers that may dependably predict tumor recurrence or micro-vascular invasion has been a new era for research interest [21].

Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27086
AFP has been for a long period used to predict the early recurrence of HCC, even in the absence of micro-vascular invasion [22,23]. However, AFP levels are raised in nearly 60% of patients with HCC, reflecting the biological behavior of malignant tumors [24]. The present data indicate that patients with low AFP levels before surgery have a lower recurrence rate. Also, there was a significant correlation between AFP levels of ≥ 400 ng/ml and HCC recurrence and survival after liver transplantation (p<0.001).
In the present study, we showed that AFP level at listing was an independent predictor of recurrence after transplantation for HCC and also predicted post-transplantation survival. On this basis, now we combine AFP level at listing with the usual criteria of tumor size and number. This practice significantly improves prediction of HCC recurrence compared with the Milan criteria alone. Pre-transplantation levels higher than 400 ng/mL have been associated with reduced post-transplantation survival.
Recent studies have shown the importance of microscopic vascular invasion as an independent prognostic factor for HCC patients undergoing resection or transplantation, but this histopathologic parameter cannot be used for preoperative selection because it is only assessable by histopathology on the explanted liver [25]. We found micro-vascular invasion reported after examining the explanted liver was associated with HCC recurrence, and also one of the independent predictors of post-transplant survival. Vascular invasion detected in 16 patients and 14 of them experienced recurrence and disease-free survival was negatively affected (p-value <0.0001). Also, overall survival was poor in the presence of vascular invasion (p-value =0.005). We also, found it in the resected liver in HR group in 9 patients, 6 of them experienced recurrence and disease-free survival was negatively affected (p-value <0.0001).
The type of resection and extension showed significant correlation with the risk of recurrence provided that the surgery is radical. The same consideration arises from other surgical experiences; the low rate of marginal recurrence supports this conclusion [26]. In our study, anatomical resection was better than non-anatomical resection. Also, resection with safety margin >2 cm was better (5 years survival was about 70%).
It has been demonstrated that HCC progression under loco-regional bridging therapy was one of the independent risk factors for post LT HCC recurrence. Prognostic significance of post-interventional tumor necrosis in the setting of LT for advanced also has been reported [27]. In the present study pre-transplant loco-regional interventions was done in 25 patients most of them received TACE for different indications. Cox regression analysis showed that pre-transplant interventions have hazard ratio of 2.443 (95% CI was 0.965 to 6.209) and a p-value of 0.061. Also, on survival analysis this variable has more positive effect on recurrence free survival that overall survival with a p-value of 0.053 and 0.107 respectively. The figures are not statistically significant but were very close and this could be due to low power of the sample size.
ConclusionHR should be considered a valid alternative to LDLT especially
in early stage HCC and transplantation is recommended only as a second line therapy in case of tumor recurrence or liver failure after resection. Also, we found that the most important factors affecting HCC recurrence were preoperative AFP and tumor behavior.
References1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of
Worldwide Burden of Cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893-917.
2. Forner A, Llovet JM, Bruix J. Hepatocellular Carcinoma. Lancet. 2012;379(9822):1245-55.
3. Liu JH, Chen PW, Asch SM, Busuttil RW, Ko CY. Surgery for Hepatocellular Carcinoma: Does it Improve Survival? Ann Surg Oncol. 2004;11(3):298-303.
4. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N Engl J Med. 1996;334(11):693-9.
5. Poon RT, Fan ST, Lo CM, Liu CL, Wong J. Long-Term Survival and Pattern of Recurrence after Resection of Small Hepatocellular Carcinoma in Patients with Preserved Liver Function: Implications for a Strategy of Salvage Transplantation. Ann Surg. 2002;235(3):373-82.
6. Botha JF, Grant WJ, Shaw BW. Surgical options for the treatment of hepatocellular carcinoma. In: Schiff ER, Sorrell MF, Maddrey WC, editors. Schiff’s Diseases of the Liver. 10th ed. Philadelphia: Lippincott Williams & Wilkins. 2007;2:1266-71.
7. Song TJ, Ip EW, Fong Y. Hepatocellular Carcinoma: Current Surgical Management. Gastroenterology. 2004;127(5 Suppl 1):S248–S260.
8. Bartlett A, Heaton N. Hepatocellular Carcinoma: Defining the Place of Surgery in an era of Organ Shortage. World J Gastroenterol. 2008;14(28):4445-53.
9. Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Dennison A. Liver Resection versus Transplantation for Hepatocellular Carcinoma in Cirrhotic Patients. Ann Surg. 1993;218:145-51.
10. Zimmerman MA, Ghobrial RM, Tong MJ, Hiatt JR, Cameron AM, Hong J, et al. Recurrence of Hepatocellular Carcinoma Following Liver Transplantation: A Review of Preoperative and Postoperative Prognostic Indicators. Arch Surg. 2008;143(2):182-8.
11. Vitale A, Peck-Radosavljevic M, Giannini EG, Vibert E, Sieghart W, Van Poucke S, et al. Personalized Treatment of Patients with Very Early Hepatocellular Carcinoma. J Hepatol. 2017;66(2):412-23.
12. Akamatsu N, Cillo U, Cucchetti A, Donadon M, Pinna AD, Torzilli G, et al. Surgery and Hepatocellular Carcinoma. Liver Cancer. 2016;6:44-50.
13. Yang A, Ju W, Yuan X, Han M, Wang X, Guo Z, et al. Comparison between Liver Resection and Liver Transplantation on outcomes in Patients with Solitary Hepatocellular Carcinoma Meeting UNOS Criteria: A Population-Based Study of the SEER Database. Oncotarget. 2017;8(57):97428-38.
14. Lim KC, Wang VW, Siddiqui FJ, Shi L, Chan ES, Oh HC, et al. Cost-Effectiveness Analysis of Liver Resection Versus Transplantation for Early Hepatocellular Carcinoma within the Milan Criteria. Hepatology. 2015;61:227-37.
15. Kaido T, Morita S, Tanaka S, Ogawa K, Mori A, Hatano E, et al. Long-Term Outcomes of Hepatic Resection versus Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Propensity Score-Matching Study. Hindawi Publishing Corporation. Disease Markers. 2015, Article ID 425926, 7 pages.
16. Dhir M, Lyden E, Smith L, Are C. Comparison of Outcomes of Transplantation and Resection in Patients with Early Hepatocellular Carcinoma: A Meta-Analysis. HPB. 2012;14(9):635-45.
17. Proneth A, Zeman F, Schlitt H, Schnitzbauer A. Is Resection or Transplantation the Ideal Treatment in Patients with Hepatocellular Carcinoma in Cirrhosis if Both Are Possible? A Systematic Review and Meta-Analysis. Ann Surg Oncol. 2014;21(9):3096-107.
18. Foltys D, Zimmermann T, Kaths M, Strempel M, Heise M, Hoppe-

Wael Mansy, et al., Clinics in Surgery - Gastroenterological Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2020 | Volume 5 | Article 27087
Lotichius M, et al. Hepatocellular carcinoma in Child's A cirrhosis: a retrospective analysis of matched pairs following liver transplantation vs. liver resection according to the intention-to-treat principle. Clin Transplant. 2014;28(1):37-46.
19. Jonas S, Bechstein WO, Steinmüller T, Herrmann M, Radke C, Berg T, et al. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology. 2001;33(5):1080-6.
20. Cha CH, Ruo L, Fong Y, Jarnagin WR, Shia J, Blumgart LH, et al. Resection of hepatocellular carcinoma in patients otherwise eligible for transplantation. Ann Surg. 2003;238(3):315-21.
21. Macdonald B, Sewell JL, Harper AM, Roberts JP, Yao FY. Liver transplantation for hepatocellular carcinoma: analysis of factors predicting outcome in 1074 patients in OPTN Region 5. Clin Transplant. 2015;29: 506-12.
22. Shimada K, Sano T, Sakamoto Y, Kosuge T. A Long-Term Follow-up and Management Study of Hepatocellular Carcinoma Patients Surviving for 10 Years or Longer after Curative Hepatectomy. Cancer. 2005;104(9):1939-47.
23. Shirabe K, Shimada M, Kajiyama K, Gion T, Ikeda Y, Hasegawa H, et al. Clinico-Pathological Features of Patients with Hepatocellular Carcinoma Surviving >10 years after Hepatic Resection. Cancer. 1998;83(11):2312-16.
24. Grąt M, Kornasiewicz O, Lewandowski Z, Hołówko W, Grąt K, Kobryń K, et al. Combination of Morphologic Criteria and α-Fetoprotein in Selection of Patients with Hepatocellular Carcinoma for Liver Transplantation Minimizes the Problem of Posttransplant Tumor Recurrence. World J Surg. 2014;38:2698-707.
25. Cillo U, Vitale A, Bassanello M, Boccagni P, Brolese A, Zanus G, et al. Liver Transplantation for the Treatment of Moderately or Well Differentiated Hepatocellular Carcinoma. Ann Surg. 2004;239(2):150-9.
26. Eguchi S, Kanematsu T, Arii S, Omata M, Kudo M, Sakamoto M, et al. Recurrence-free survival more than 10 years after liver resection for hepatocellular carcinoma. Br J Surg. 2011;98(4):552-7.
27. De Carlis L, Di Sandro S, Giacomoni A, Slim A, Lauterio A, Mangoni I, et al. Beyond the Milan Criteria: what Risks for Patients with Hepatocellular Carcinoma Progression before Liver Transplantation? J Clin Gastroenterol. 2012;46(1):78-86.