carcinoma pancreatico curso
TRANSCRIPT

CARCINOMA PANCREATICODR. CARLOS VILA MBCG
HCC
EPIDEMIOLOGIA Ocupa la 4ta causa de muerte gral en
E.E.U.U. Ocupa el 5to lugar como causa de muerte por
Ca en todo el país 11avo lugar en frec. de todos los Ca. Es uno de los tumores malignos del tubo
digestivos de peor pronostico 4to lugar en México de los carcinomas del
tubo digestivo
EPIDEMIOLOGIA
En el mundo mas de 185.000 nuevos casos ocurren cada año
⇑ edad avanzada, raza negra, masculino y judios
20% de todas la muertes por Ca gastrointes.
INCIDENCIA
9 x 100,000 en general frecuencia hombres 2:1 promedio de edad 6ta y 7ma década 90 % se diagnostica después de los 50 años 95% muere por la afección. Supervivencia media de 18-20 meses
FACTORES ETIOLOGICOS1.- Factores hereditarios:
a).Antecedente familiar de Ca. de páncreas.b). Pancreatitis familiar: Rara.
1.- Hereditaria.- 15 al 30%2.- Crónica calcifícate.- 7 al 25%
c).-Diabetes sacarina.- 50%2.- Tabaquismo3.- Café.4.- Dieta.5.- Exposición a algunos productos
químicos
FACTORES ETIOLOGICOS 6 síndromes genéticos incrementan el riesgo de
desarrollar Ca. De pancreas Ca. De colon no poliposico hereditario Ca. De mama familiar Síndrome de Peutz-Jeghers Síndrome de ataxia-telangiectasia Síndrome molarnelanoma múltiple atípico Pancreatitis hereditaria
Otros Diabetes mellitus, pancreatitis crónica.

ETIOPATOGENIA

ANATOMIA PATOLOGICA
⇑ 90% se originan en epitelio ductal
Adenocarcinoma 90 a 95 % Localización: 75% cabeza
25% cuerpo y cola 82% adenoCa de células
ductales.13% adenoCa de células acinares 5% carcinoma anaplasico..
BIOLOGIA MOLECULAR Demuestran Oncogen mutante Kirsten (Ki)-ras. Prevalencia de mutación codon 12(Ki)-ras
Del 89% en páncreas 13% en ampulares 20% en coledocianas

CLASIFICACIONCLASIFICACIONPRE OPERATORIAS TRANS OPERATORIASPOST OPERATORIAS POR
ETAPAS(TNM).

CLASIFICACION T.N.M.
TUMOR PRIMARIO (T)Tx El tumor no puede valorarse
T0 sin signos de tumor primario
T1 Tumor limitado al páncreasT1a Tumor menor de 2 cm.T1b Tumor de mas de 2 cm.
T2 Tumor que se extiende a duodeno, conducto biliares y tej. Peripancreático
T3 Tumor que se extiende a: Estomago, bazo, color y grandes vasos
GANGLIOS LINFATICOS REGIONALES (N)GANGLIOS LINFATICOS REGIONALES (N)
NXNX ganglios no valorablesganglios no valorables
NONO Sin metástasis a ganglios linfáticosSin metástasis a ganglios linfáticos
regionalesregionales
N1N1 Metástasis a ganglios linfáticos Metástasis a ganglios linfáticos
regionalesregionales
METASTASIS A DISTANCIA (M)METASTASIS A DISTANCIA (M)
MXMX La presencia de mets a distanciaLa presencia de mets a distancia
No puede valorarseNo puede valorarse
M0M0 Sin Mets a distanciaSin Mets a distancia
M1M1 Metástasis a distancia Metástasis a distancia

GANGLIOS LINFATICOS REGIONALESPERIPANCREATICOS
Superiores A la cabeza y cuerpo del páncreas
Inferiores A la cabeza y cuerpo del páncreas
Anteriores Pancreático duodenales anteriores, pilóricos y mesentéricos proximales
Posteriores Pancreáticos duodenales posteriores, del colédoco o pericoledocianos y ganglios mesentéricos proximales
Esplénico Hilio del bazo y cola del páncreas
ARTERIA HEPATICA
Infrapiloricos Solo para tumores de cabeza
Subpiloricos Solo para tumores de cabeza
Celiacos Solo para tumores de cabeza
MESENTERICOS SUPERIORES
Esplénicos Solo para tumores de cuerpo y cola
Retroperitoneales Solo para tumores de Cuerpo y cola
Aorticolaterales
Todos los demás se consideran distantes y deben clasificarse como M1

ESTADIFICACION
Agrupamiento por estadios
Estadio 1 T 1T2
N0N0
M0Mo
Estadio 11 T3 N0 M0
Estadio 111 Cualquier T N1 M0
Estadio 1V Cualquier T Cualquier N M1
MANIFESTACIONES CLINICAS
Al inicio de la enf. los signos y síntomas son vagos y mal definidos
Realmente manifiesto en enf. avanzada. Triada inicial. Es casi Dx.
Perdida de peso gradual y progresiva Dolor abdominal 65 al 80% Ictericia asintomática. Tardía, progresiva
75% en cabeza de páncreas. 75% ictericia,perdida de peso,dolor abdominal
profundo. 65% hepatomegalia. 25% signo de Courvoisier. 20% diabetes súbita. 13 % ictericia sola,indolora. Colangitis 10%
Manifestaciones clinicas
CUADRO CLINICOCUADRO CLINICO
CABEZACABEZA•Ictericia Perdida de pesoIctericia Perdida de peso
•Ictericia.Ictericia.
•Dolor abdominal profundoDolor abdominal profundo
•Anorexia Anorexia
•Ataque edo. Gral.Ataque edo. Gral.
•Debilidad muscular.Debilidad muscular.
CUERPOCUERPO•Perdida de pesoPerdida de peso
•AnorexiaAnorexia
•Dolor abdominal Dolor abdominal epigástrico y dorso lumbarepigástrico y dorso lumbar
•Ataque al edo Gral.Ataque al edo Gral.
•Nauseas y vomitoNauseas y vomito
•Hemorragia Hemorragia gastrointestinalgastrointestinal
SINTOMASSINTOMAS

CUADRO CLINICOCUADRO CLINICOSIGNOSSIGNOS
CABEZACABEZA
•IctericiaIctericia
•HepatomegaliaHepatomegalia
•Masa abdominal Masa abdominal palpablepalpable
•AscitisAscitis
•Sind. Corvuosier terrierSind. Corvuosier terrier
CUERPOCUERPO
•HepatomegaliaHepatomegalia
•Masa abdominal Masa abdominal palpablepalpable
•AscitisAscitis
•IctericiaIctericia

Diagnostico Diagnostico
CLINICO:”alto índice de sospecha”.Ultrasonido.:investigacion inicial, S-E 80-90%.TAC dinamica.
– ”la mejor modalidad”, lesiones > 1 cm,ganglios <2 cm ,falsos positivos 10%,valora irresecabilidad en 95%.y la predice en 70% aunque la tercera parte resulta resecable.S-E 85-95%
SOSPECHA DIAGNOSTICA
Ictericia obstructiva. Perdida de peso de mas 10% Dolor abdominal alto, lumbar rec. Inexplicable Dispepsia reciente Diabetes mellitus de aparición. brusca sin fac. p.
Obesidad Historia. familiar
Aparición brusca de esteatorrea Ataque de pancreatitis ideopatica
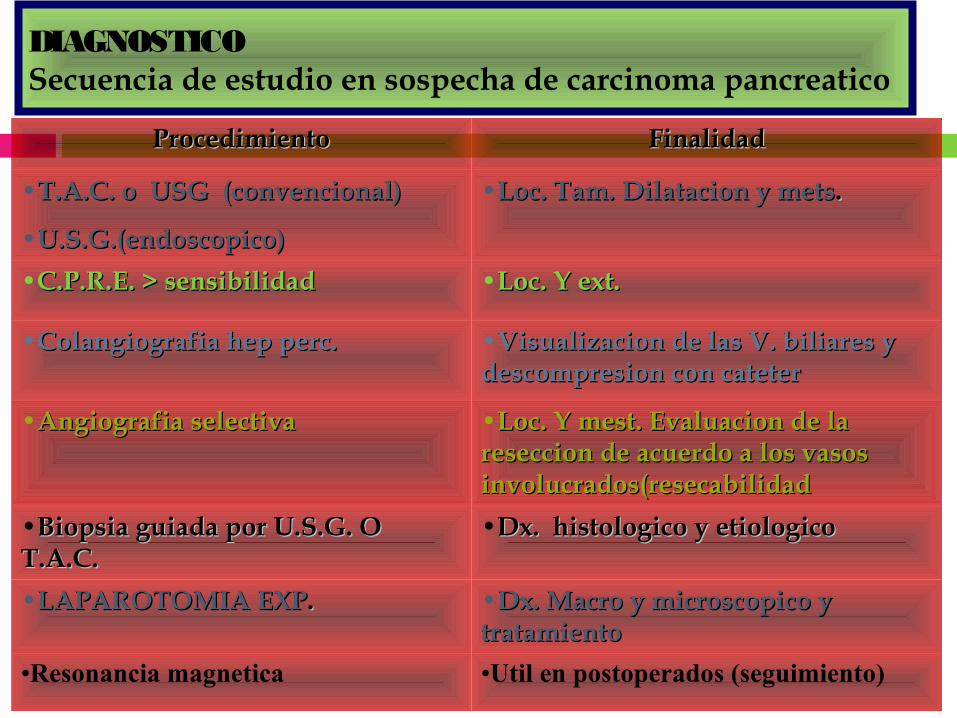
DIAGNOSTICOSecuencia de estudio en sospecha de carcinoma pancreatico
ProcedimientoProcedimiento FinalidadFinalidad
•T.A.C. o USG (convencional)T.A.C. o USG (convencional)
•U.S.G.(endoscopico)U.S.G.(endoscopico)
•Loc. Tam. Dilatacion y metsLoc. Tam. Dilatacion y mets..
•C.P.R.E. > sensibilidadC.P.R.E. > sensibilidad •Loc. Y ext.Loc. Y ext.
•Colangiografia hep perc.Colangiografia hep perc. •Visualizacion de las V. biliares y Visualizacion de las V. biliares y descompresion con cateterdescompresion con cateter
•Angiografia selectivaAngiografia selectiva •Loc. Y mest. Evaluacion de la Loc. Y mest. Evaluacion de la reseccion de acuerdo a los vasos reseccion de acuerdo a los vasos involucrados(resecabilidadinvolucrados(resecabilidad
•Biopsia guiada por U.S.G. O Biopsia guiada por U.S.G. O T.A.C.T.A.C.
•Dx. histologico y etiologicoDx. histologico y etiologico
•LAPAROTOMIA EXPLAPAROTOMIA EXP.. •Dx. Macro y microscopico y Dx. Macro y microscopico y tratamientotratamiento
•Resonancia magnetica •Util en postoperados (seguimiento)
T.A.C.
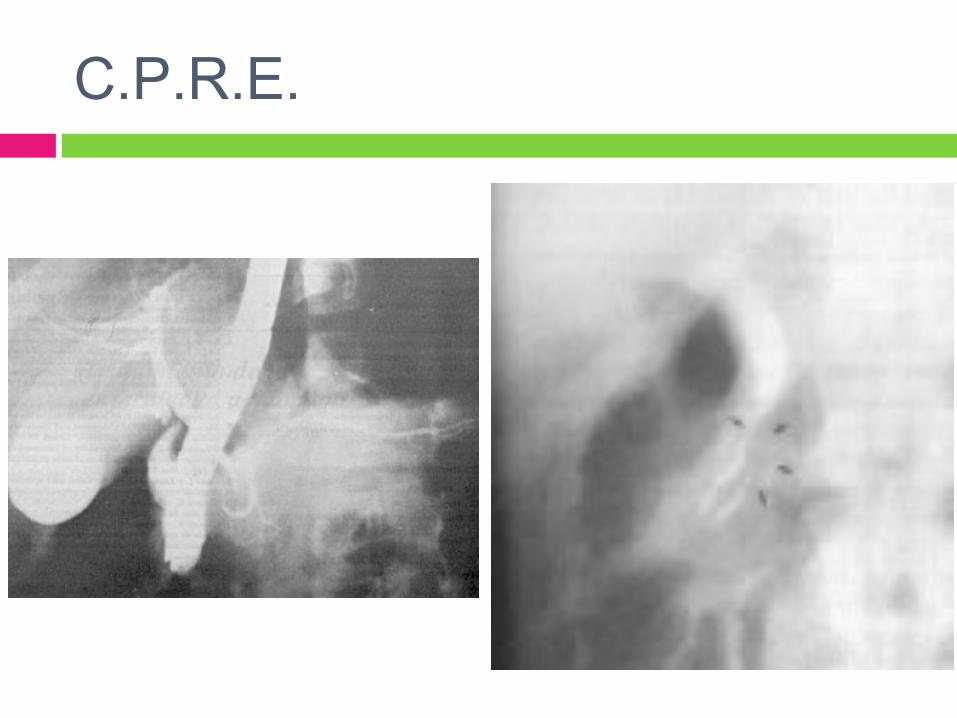
C.P.R.E.
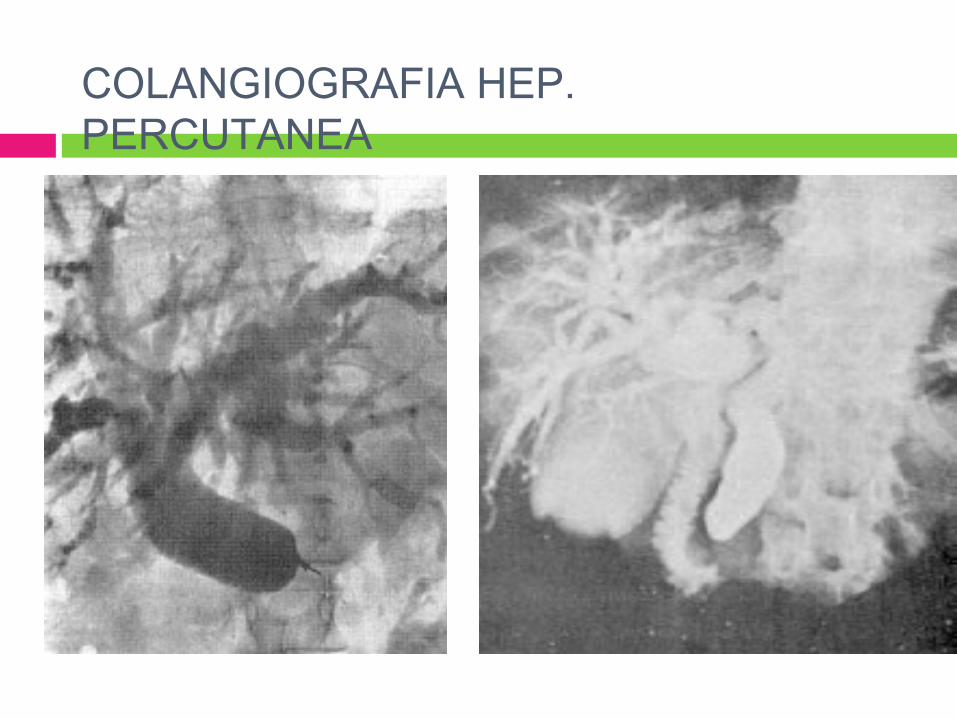
COLANGIOGRAFIA HEP. PERCUTANEA

ANGIOGRAFIA SELECTIVA

BIOPSIA /T.A.C.
DIAGNOSTICO
MARCADORES TUMORALES Ant. Carc. Emb. Senc. ⇓ , ⇑ lesiones
benignas y malignas. Ca. 19-9 mas util que el A.C.E. Pero no es
especif. ⇑ en ca de colon y V. Biliar. DU-PAN –2(antigeno onco-fetal pancreat.) galactosiltransferasa No han sido utiles Útiles solamente para seguimiento
DIAGNOSTICO TEMPRANO
Los parámetros que se toman en cuenta:1.-Tumor diámetro menos de 2 cm.2.- no exista evidencia histológica de invasión
a la cápsula3.- Ausencia durante la Laparotomía de mets.
a distancia.4.- Después de una disección y reseccion del
tumor ausencia de nódulos linfáticos afectados

TRATAMIENTO
QUIRURGICO:Paliativo.-Potencialmente curativo.-
1.- Derivación biliodigestiva.2.- Pancreatectomia distal.3.- Pancreatoduodenectomia.4.- WHIPPLE.

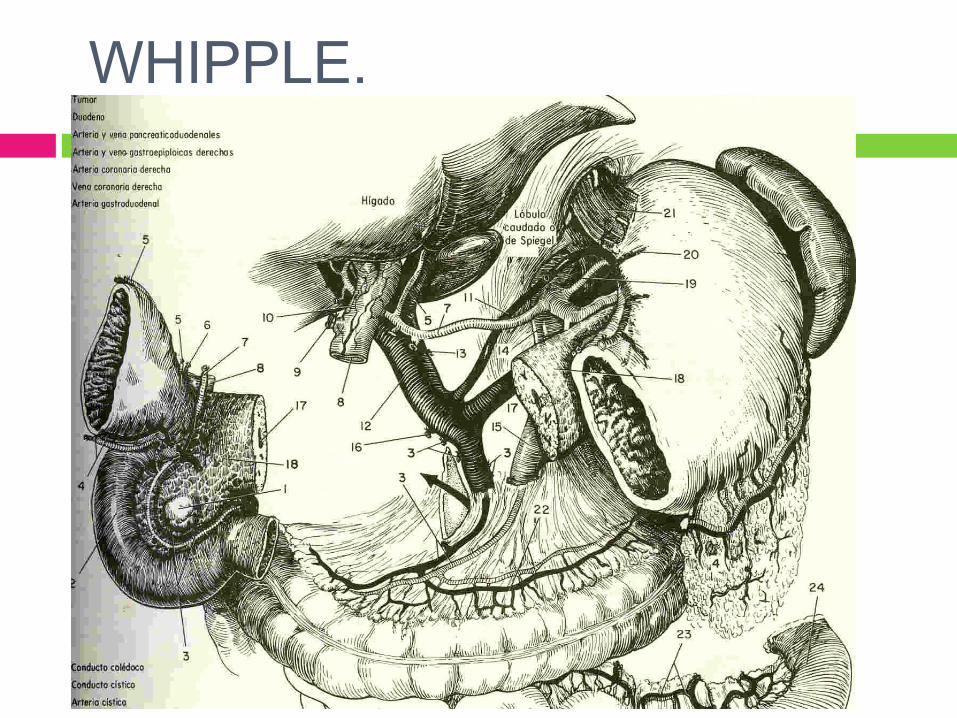
WHIPPLE.



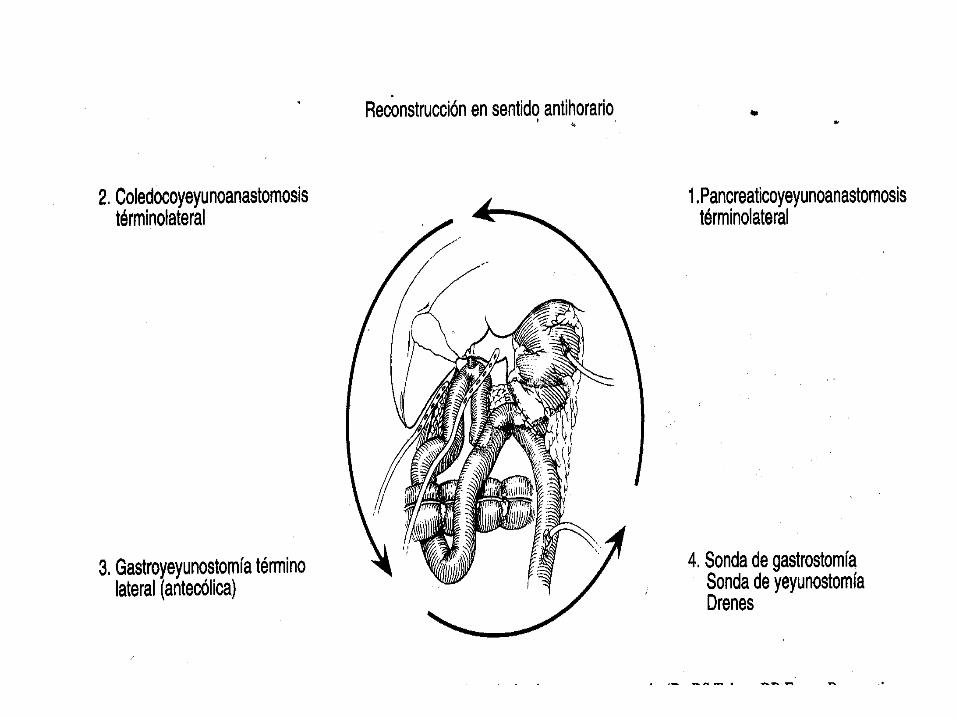
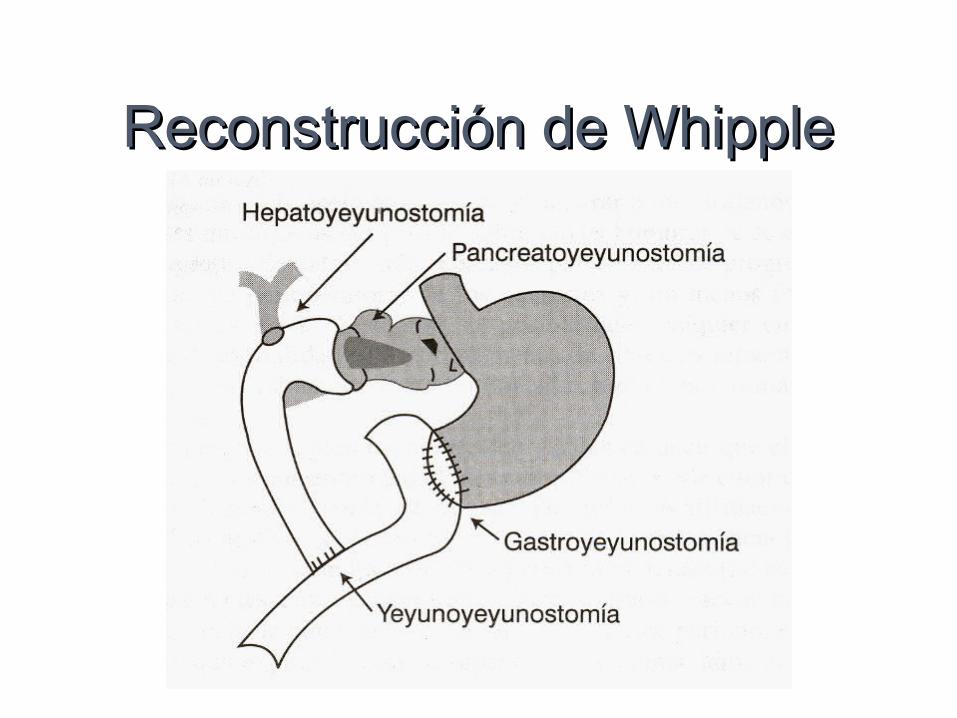
Reconstrucción de WhippleReconstrucción de Whipple
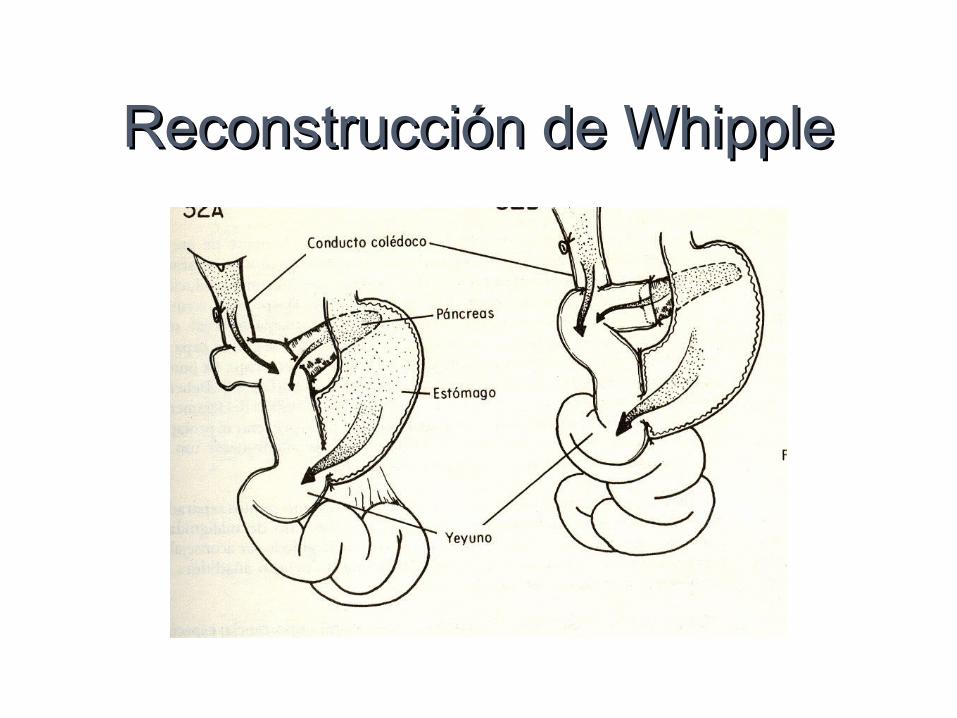
Reconstrucción de WhippleReconstrucción de Whipple

The Whipple Procedure
Pancreaticoduodenectomy - Whipple pancreatic head
duodenumgallbladder
bile duct+/- gastric antrum

Step 1 - SMV The lesser sac is entered, and the hepatic
flexure of the colon is taken down The inferior border of the pancreas is
identified at the level of the proximal body of the gland
The visceral peritoneum and root of mesentery are incised from this point, in a lateral direction, heading toward the junction of the second and third portions of the duodenum in an effort to expose the anterior wall of the superior mesenteric vein (SMV)
The SMV is exposed at the inferior border of the neck of the pancreas, adjacent to the uncinate process
The middle colic vein and gastroepiploic vein often arise from a common trunk, which occasionally also involves the right colic vein.
Any or all of these veins may require ligation and division to safely expose the SMV.

Step 2 - Kocherize A Kocher maneuver has been
performed by first identifying the inferior vena cava (IVC) at the level of the proximal portion of the transverse segment of the duodenum (D3)
One can then mobilize the duodenum and pancreatic head off of the IVC in a cephalad direction
Remove all soft tissue anterior to the IVC
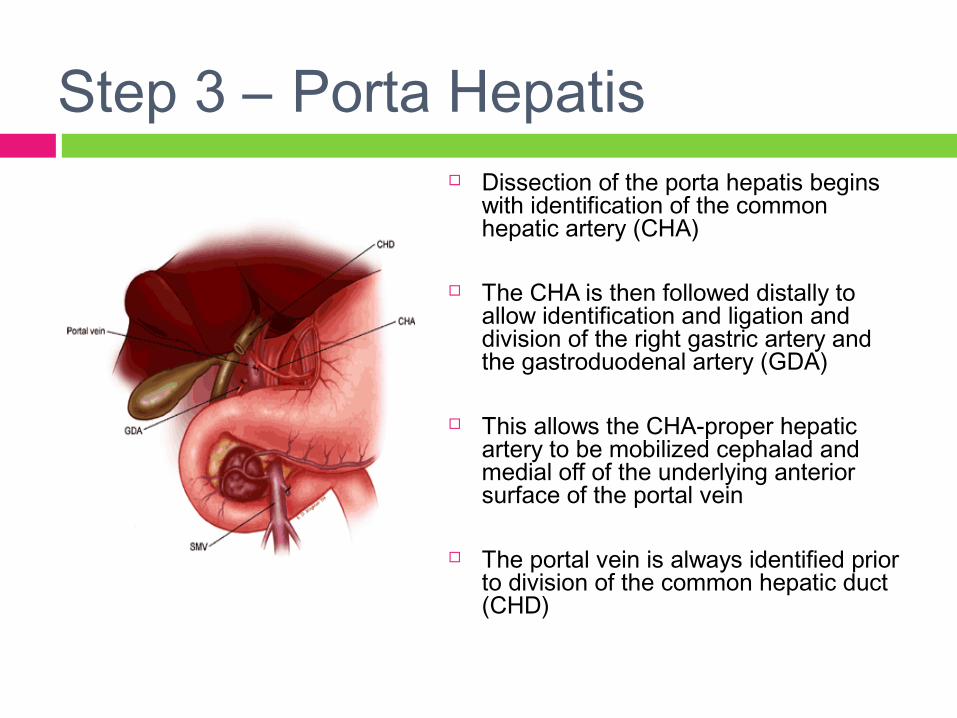
Step 3 – Porta Hepatis Dissection of the porta hepatis begins
with identification of the common hepatic artery (CHA)
The CHA is then followed distally to allow identification and ligation and division of the right gastric artery and the gastroduodenal artery (GDA)
This allows the CHA-proper hepatic artery to be mobilized cephalad and medial off of the underlying anterior surface of the portal vein
The portal vein is always identified prior to division of the common hepatic duct (CHD)

Step 4 - Antrum The antrum of the stomach is resected with
the main specimen by dividing the stomach at the level of the third or fourth transverse vein on the lesser curvature
Pylorus preservation may be considered in patients with small periampullary neoplasms
Appropriate caution must be exercised during the portal dissection to avoid unnecessary injury to the nerves of Latarjet The fundamental technical difference in the
pylorus-preserving procedure and is essential to avoid postoperative gastroparesis
Should not be performed in patients with bulky pancreatic head tumors duodenal tumors involving the first or second
portions of the duodenum lesions associated with grossly positive pyloric
or peripyloric lymph nodes
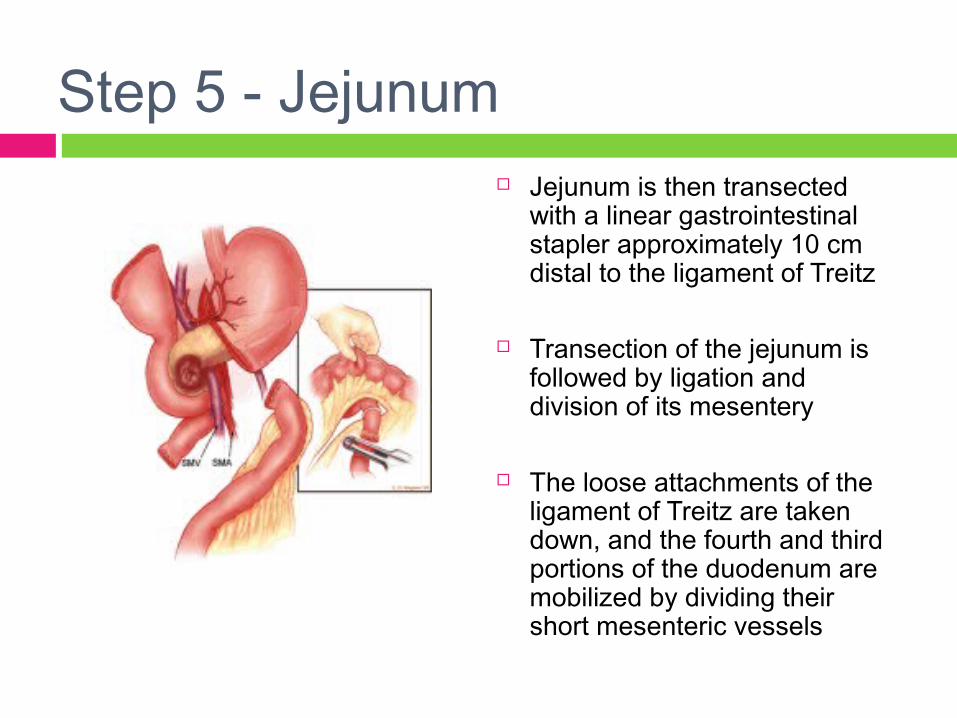
Step 5 - Jejunum Jejunum is then transected
with a linear gastrointestinal stapler approximately 10 cm distal to the ligament of Treitz
Transection of the jejunum is followed by ligation and division of its mesentery
The loose attachments of the ligament of Treitz are taken down, and the fourth and third portions of the duodenum are mobilized by dividing their short mesenteric vessels

Step 6 - Pancreas The pancreatic head and
uncinate process are separated from the superior mesenteric-portal vein confluence
The pancreas has been transected at the level of the portal vein and the pancreatic head is reflected laterally allowing identification of small
venous tributaries from the portal vein and superior mesenteric vein (SMV)
These tributaries are ligated and divided
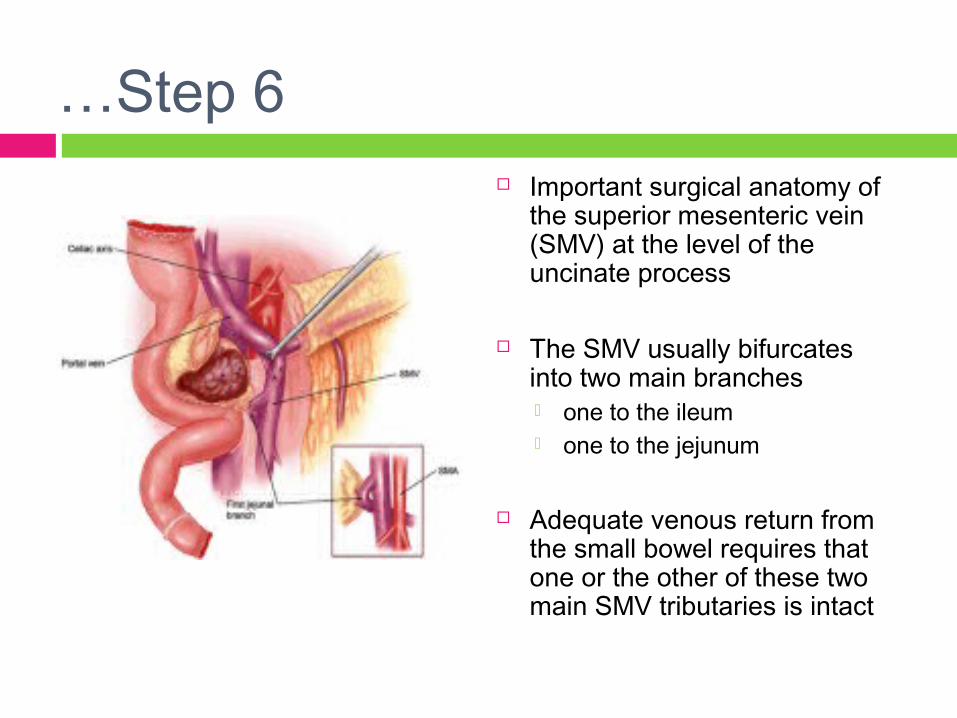
…Step 6 Important surgical anatomy of
the superior mesenteric vein (SMV) at the level of the uncinate process
The SMV usually bifurcates into two main branches one to the ileum one to the jejunum
Adequate venous return from the small bowel requires that one or the other of these two main SMV tributaries is intact

…Step 6 Medial retraction of the superior
mesenteric-portal vein confluence facilitates dissection of the soft tissues adjacent to the lateral wall of the proximal superior mesenteric artery (SMA)
This site represents the SMA margin
The inferior pancreaticoduodenal artery is identified at its origin from the SMA, ligated, and divided

Vascular Resection Segmental venous resection is
required and the decision is made to divide the splenic vein
Ligate the splenic vein only when the tumor involves the splenic vein confluence
By dividing the splenic vein, the superior mesenteric artery (SMA), which is identified medial to the superior mesenteric vein (SMV), can be exposed to its origin from the aorta and the pancreatic head
Reconstruction is performed (during inflow occlusion) by an end-to-end anastomosis of the portal vein and the SMV with interrupted 6-0 Prolene sutures
Vascular Resection
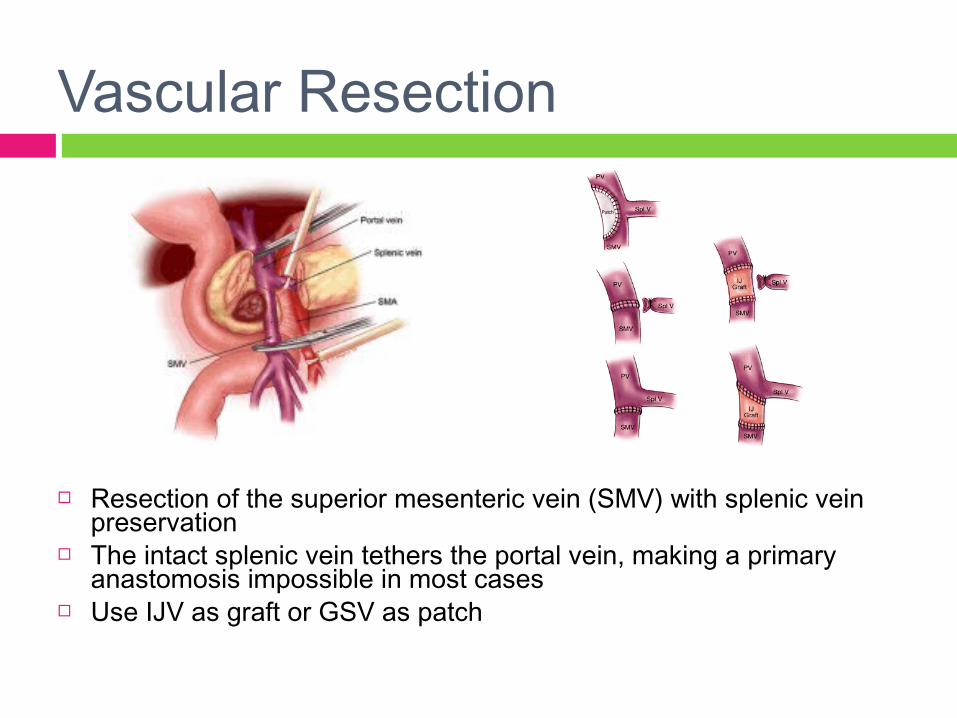
Resection of the superior mesenteric vein (SMV) with splenic vein preservation
The intact splenic vein tethers the portal vein, making a primary anastomosis impossible in most cases
Use IJV as graft or GSV as patch
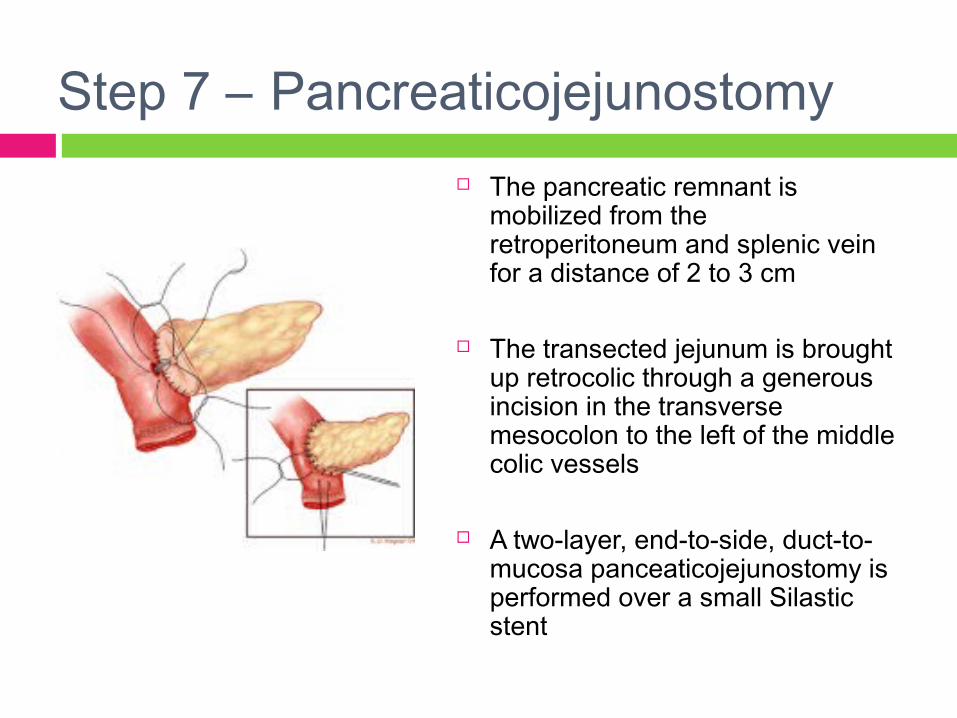
Step 7 – Pancreaticojejunostomy The pancreatic remnant is
mobilized from the retroperitoneum and splenic vein for a distance of 2 to 3 cm
The transected jejunum is brought up retrocolic through a generous incision in the transverse mesocolon to the left of the middle colic vessels
A two-layer, end-to-side, duct-to-mucosa panceaticojejunostomy is performed over a small Silastic stent
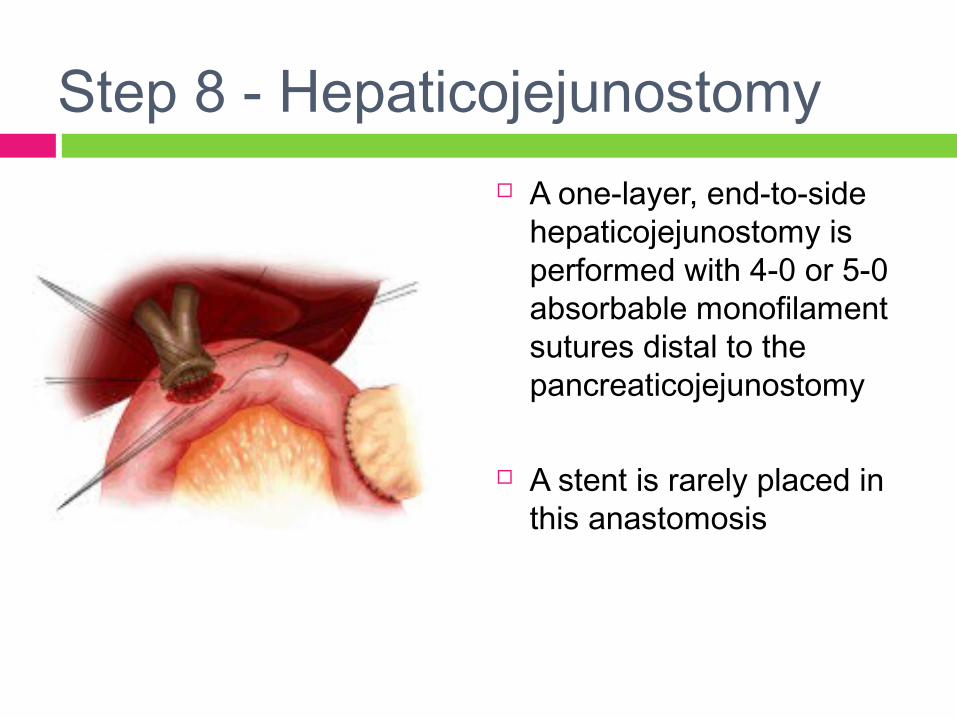
Step 8 - Hepaticojejunostomy A one-layer, end-to-side
hepaticojejunostomy is performed with 4-0 or 5-0 absorbable monofilament sutures distal to the pancreaticojejunostomy
A stent is rarely placed in this anastomosis
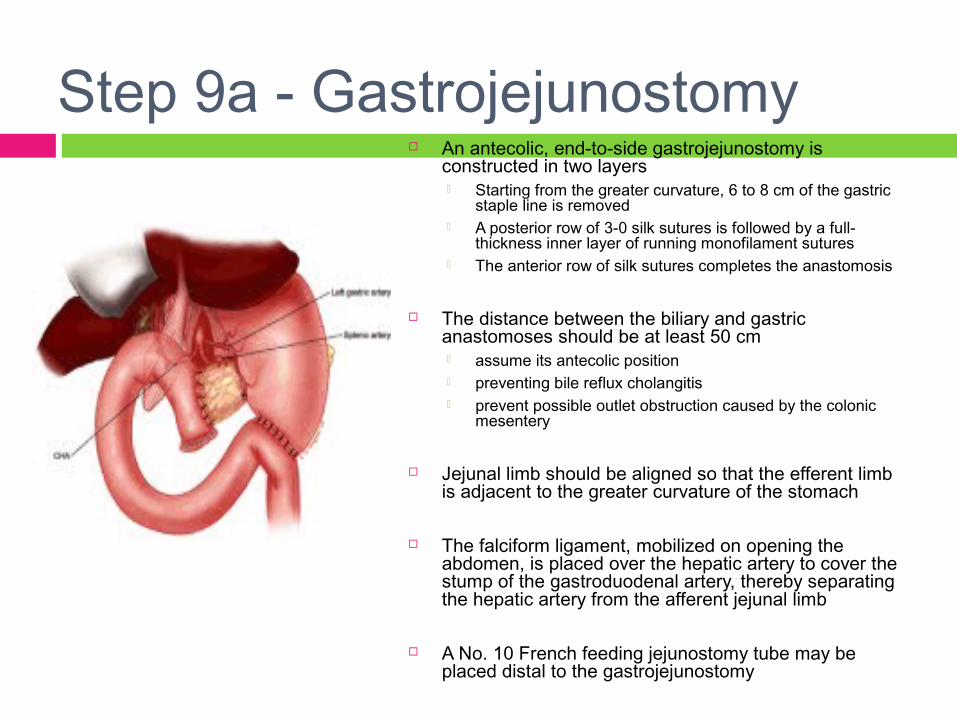
Step 9a - Gastrojejunostomy An antecolic, end-to-side gastrojejunostomy is
constructed in two layers Starting from the greater curvature, 6 to 8 cm of the gastric
staple line is removed A posterior row of 3-0 silk sutures is followed by a full-
thickness inner layer of running monofilament sutures The anterior row of silk sutures completes the anastomosis
The distance between the biliary and gastric anastomoses should be at least 50 cm assume its antecolic position preventing bile reflux cholangitis prevent possible outlet obstruction caused by the colonic
mesentery
Jejunal limb should be aligned so that the efferent limb is adjacent to the greater curvature of the stomach
The falciform ligament, mobilized on opening the abdomen, is placed over the hepatic artery to cover the stump of the gastroduodenal artery, thereby separating the hepatic artery from the afferent jejunal limb
A No. 10 French feeding jejunostomy tube may be placed distal to the gastrojejunostomy

Paliacion quirurgica del Ca de Paliacion quirurgica del Ca de pancreas.pancreas.Objetivo:Objetivo:
Ictericia obstructivaObstruccion duodenal dolor

ICTERICIA OBSTRUCTIVAICTERICIA OBSTRUCTIVA
70 % de los Ca al momento del DX. Sin tratamiento evolucionan: disfuncion hepatica-
insuficiencia hepatica-muerte.
TECNICAS: Internas; coledocodudodenostomia
Colecistoyeyunostomia
Hepatoyeyunostomia
TECNICA :Externa
Sonda en T.
Obstruccion duodenalObstruccion duodenal
30-50 % nausea y vomito en el DxA cualquier nivel duodenal según el sitio
del tumor.TECNICA: GastroyeyunoanastomosisCON OBSTRUCCION DUODENAL LA
UNICA OPCION ES CIRUGIA.
DOLORDOLOR
ES EL SINTOMA MAS MOLESTO E INCAPACITANTE.
TECNICA:ESPLACNICECTOMIA QUIMICA
TRANSOPERATORIA
GRACIAS