linfoma radiology
TRANSCRIPT

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 1/9
Radiological Manifestations of
Skeletal Lymphoma
John O’Neill, MB, BAO, BCh, MRCPI, MSc, FRCR (UK),
a,b
Karen Finlay, MD, FRCPC,a,b Eric Jurriaans, MD, FRCPC,a,b
and Lawrence Friedman, MBBCh, FRCPC, FACRa,b
Lymphoreticular neoplasms primarily arise in extraskeletallocations with skeletal involvement usually secondary tohematogenous spread or by direct invasion from surround-ing involved lymph nodes or soft tissues. Primary lym-phoma of bone is relatively rare in comparison. Lymphomaencompasses Hodgkin’s and non-Hodgkin’s disease, Bur-
kitt’s lymphoma, and mycosis fungoides. Skeletal diseasemay present with symptoms localized to the site of boneinvolvement, as an incidental finding on imaging for otherreasons, or as part of the staging of the disease. It isimportant that the radiologist is cognizant of the many presentations of skeletal lymphoma. We present a review of the radiological imaging of skeletal lymphoma withconventional radiographs, computed tomography, scinti-graphic studies, and magnetic resonance imaging.
Primary lymphoma of bone is rare and skeletal changes
are more commonly encountered either as hematogenous
dissemination to bone from a primary extraskeletal site orby direct invasion. These changes usually occur duringthe course of the disease rather than a presenting feature.
Skeletal disease may present with symptoms localized to
the site of bone involvement, as an incidental finding on
imaging for other reasons, or as part of the staging of thedisease.
The classification of lymphoma is continuously
undergoing modification with the ultimate goal of providing clinicians with a universal diagnostic basis
for therapeutic decisions. In 1994 the Revised Euro-
pean American Lymphoma classification was pro-
posed by the International Lymphomas Study Group
and has recently been incorporated into the World
Health Organization classification of tumors of hemo-poietic and lymphoid tissues.1 It is predominantly
based on cell lineage and cell differentiation utilizing
genetic, immunophenotypic, biologic, and clinical fea-tures (Table 1). Cell type and degree of differentiation
may change during the course of the disease altering
treatment and prognosis.2 In basic broad categories,lymphomas are divided into malignant lymphomas
and Hodgkin’s lymphoma, the former occurring three
times more frequently than the latter.
Skeletal involvement varies considerably depend-ing on the cell type and method of detection.3 Exam-
ples include histiocytic and lymphocytic lymphomas,
which have a 21 and 12% rate of bone involvement,
respectively.
4
Postmortem examination demonstratesskeletal changes in 50% of Hodgkin’s lymphoma
cases with significantly less detected on radiographicstudies.3 The latter, however, varies considerably with
the method of imaging. The detection and recognition of
skeletal disease is essential in both the primary diagnosis
and the staging of the disease process and thus it isimportant that the radiologist is cognizant of the many
presentations of skeletal lymphoma. We present a review
of the radiological imaging of skeletal lymphoma withconventional radiographs, computed tomography (CT),
scintigraphic studies, and magnetic resonance imaging
(MRI) and have concentrated on the following catego-ries: primary bone lymphoma, Hodgkin’s lymphoma,non-Hodgkin’s lymphoma (NHL), Burkitt’s lymphoma,
and mycosis fungoides.
Primary Lymphoma of Bone
Oberling first described this entity in 1928 and sug-gested the diagnosis of reticulum cell sarcoma but it
From the aDepartment of Radiology, St. Josephs Healthcare Hamilton,
Ontario, Canada; and bMcMaster Health Sciences, Hamilton, Ontario, Canada.
Reprint requests: John O’Neill, MB, BAO, BCh, MRCPI, MSc, FRCR(UK), Radiology Department, St. Josephs Hospital, 50 Charlton AvenueEast, Hamilton, Ontario L8N 4A6, Canada. E-mail: [email protected].
Curr Probl Diagn Radiol 2009;38:228-236.
© 2009 Published by Mosby, Inc.
0363-0188/2009/$36.00 0
doi:10.1067/j.cpradiol.2008.07.001
228 Curr Probl Diagn Radiol, September/October 2009

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 2/9
was not until 1939 that it was separated from Ewingsarcoma by Parker and Jackson. In the same year it
was included in the Bone Sarcoma Registry by Ewing
under the heading of reticulum cell lymphosarcoma.5
Ivins and Dahlin introduced the term primary bone
lymphoma (PBL) in 1963.6 Diagnosis requires a pri-
mary focus in a single bone, histological confirmation,
and no evidence of distant lymph node or metastasis ator within 6 months of presentation.7 Regional lymph
node disease is acceptable as is multifocal bone
involvement. PBL is responsible for less than 5% of malignant bone tumors and less than 1% of NHL.8 The
majority of PBL are from NHL, usually a diffuse
B-cell subtype, with 6% arising from Hodgkin’s lym-
phoma.Patients usually present with a long history of pain
localized to the site of involvement, or pathological
fracture (22%). In a large retrospective detailed imag-ing review of 237 patients with PBL, the following
features were recognized.7 The age ranged from 2 to
88 years with the majority evenly distributed betweenthe second and eighth decades at a mean of 42 years.
The male:female ratio was 1.8:1. Long bone involve-
ment is more common than flat bone, 71% versus
22%, and is commonly metadiaphyseal (69%) with thefemur, tibia, and humerus the commonest bones in-
volved. Lesions can be epiphyseal, metaphyseal, or
diaphyseal and may cross a joint space to involve the
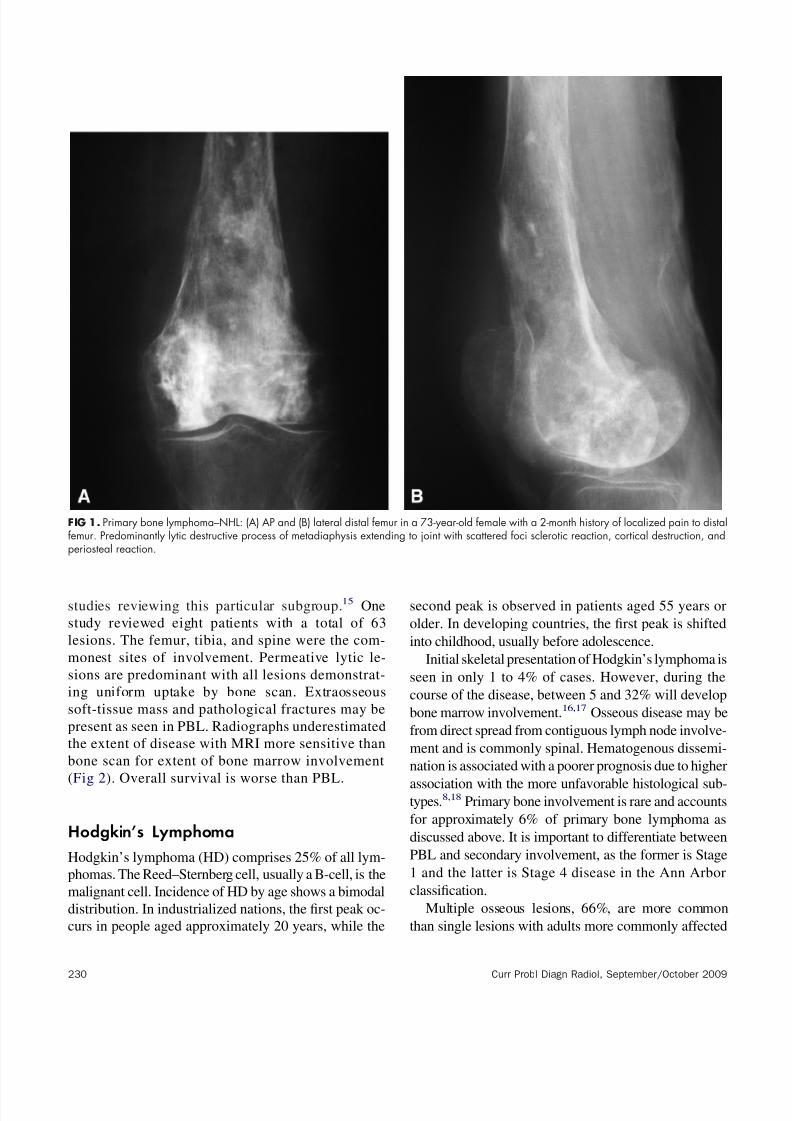
opposing bone (4%) (Fig 1). Synovitis of adjacent joint may occur and usually affects the knee. Con-
ventional radiographic features include lytic (70%),mixed (28%), and rarely, blastic (2%) patterns. Thecommonest lytic pattern is permeative or moth-eaten.
Sequestra may occasionally be seen. Initial radio-
graphs may be normal (5%), but abnormalities can be
demonstrated on bone scan or MRI before conven-tional radiographic changes. On average, conventional
radiographs become abnormal in this subgroup within
10 months. Periosteal reaction ranges from an inter-
rupted single or multiple layers to a single continuous
layer and is present in almost 50% of patients. Very
rarely disease may be confined to the periosteum.Radionuclide bone scans are abnormal in the vast
majority of patients, 98%, demonstrating mild to
marked increased uptake. CT is excellent in delineat-
ing cortical destruction, whereas MRI is more sensi-tive than CT for assessing degree of soft tissue
involvement, 48%, which indicates a more aggressive
lesion with a poorer long-term outcome.MRI signal characteristics were inhomogeneous
and variable with the majority of lesions isointense or
hypointense to muscle on T1 and hypo/iso/hyperin-
tense to subcutaneous fat on T2. Low signal intensityon both T1 and T2 is speculated to be related to a high
content of fibrous tissue.9 A recent MRI study of 29
patients with PBL marrow signal intensity were non-
specific intermediate on T1 and high signal on T2.10
Enhancement patterns were heterogeneous in 59%.Soft-tissue extension was present in 76% and demon-
strated a more homogenous appearance on T1, 90%
iso-intense to muscle, T2, 91% high signal intensity(SI), and diffuse enhancement in 82%. Interestingly
cortical bone was abnormal in the majority, 93%, with
permeative cortical destruction with linear foci 52%.
Intramedullary extension is best assessed on MRI andin this series a clear line of demarcation with normal
marrow was present in 55%.10 Rarely PBL may be
confined to the periosteum or cortex with diffusecortical thickening without medullary involvement.10
The differential diagnosis is dependent on the age at
presentation. In children, Ewing’s sarcoma, osteomy-elitis, metastatic neuroblastoma, and Langerhans’ cell
histiocytosis should be considered, whereas in the
second decade lytic osteosarcoma should be included.
Adult differential includes metastatic disease and my-eloma. Overall survival is 91% at 5 years and 87% at
10 years with combined modality of chemotherapy
and radiotherapy.11,12
Primary Multifocal Bone LymphomaPrimary multifocal bone lymphoma is a subtype of
primary bone lymphoma and comprises between 11
and 33% of PBL.13,14 Diagnosis requires the involve-
ment of multiple bone sites without distant lymphnode or visceral involvement for 6 months post pre-
sentation. Patient presentation and imaging character-
istics are similar to those in PBL, allowing for multiplebone involvement, although there are no large
TABLE 1. Basic WHO classification of lymphomas
B-cell neoplasms
● Precursor B-cell neoplasm
● Mature B-cell neoplasms (incl. Burkitt lymphoma)
● B-cell proliferations of uncertain malignant potential
T-cell and NK-cell neoplasms
● Precursor T-cell neoplasms
● Mature T-cell and NK-cell neoplasms (incl. Mycosis
fungoides)● T-cell proliferations of uncertain malignant potential
Hodgkin lymphoma
Curr Probl Diagn Radiol, September/October 2009 229
8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 3/9

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 4/9
than children. Presentation is usually with local pain and
tenderness. The dorsolumbar spine, pelvis, ribs, femora,
and sternum are the commonest sites in order of frequen-
cy.19 Osteolytic lesions are commonest but lesions may
be mixed or sclerotic. The latter occur between 15 and
45%. An ivory vertebra represents diffuse sclerosis,
homogenous or heterogenous, of a vertebral body. Ver-tebra plana, a flattened vertebral body, is a less common
finding but both may occur and are not limited to
lymphoma. Localized sclerosis of a vertebra, sternum, orpelvis secondary to adjacent to lymph node disease iscommon. Anterior erosion may occur from involvement
of paravertebral lymphadenopathy. Diffuse skeletal os-
teosclerosis may occur in response to extensive marrowdisease or diffuse bone marrow fibrosis. Ill-defined os-
tiolytic lesions, which may have a sclerotic rim, are often
associated with a periosteal reaction, lamellated or with a
“sunburst” pattern.19 Rarely, hypertrophic osteoarthrop-
athy occurs, usually in patients with mediastinal involve-
ment.
Bone marrow disease is often focal in nature and
thus may not be identified on bilateral iliac crestmarrow sampling. MRI is beneficial in these cases as
it is sensitive in demonstrating marrow infiltration and
in addition may help in guiding biopsy.17,18 In a studyassessing the value of MRI versus bone marrow
biopsy involving 26 patients, MRI identified seven
cases of spinal disease, only three of which werepositive on crest biopsy. MRI-positive patients had a
higher relapse rate in the 24-month follow-up period
than the MRI-negative patients.17
Lymphocytic-predominant and nodular sclerosis are
less aggressive histological subtypes than mixed cellu-
larity and depleted lymphocytes and carries a better
prognosis. The latter has a greater incidence of boneinvolvement and aggressive osteolytic lesions. The dif-
FIG 2. Multifocal primary bone lymphoma–HD. 40-year-old male with 3-month history of multifocal back pain. (A) Lateral lower thoracic spinedemonstrating wedge compression fracture with increased AP diameter of a 10th thoracic vertebra. Corresponding sagittal T2 (B) thoracic spinewith diffuse increase signal intensity and collapse of T10, T4, and L1 with secondary spinal stenosis at T4. Signal intensity was of uniform low signalon T1 (not shown).
Curr Probl Diagn Radiol, September/October 2009 231
8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 5/9
ferential diagnosis for new bone lesions occurring in
treated HD includes recurrent disease, development of
NHL, and osteomyelitis due to immunosuppression. The
overall 5-year survival for all stages of Hodgkin’s disease
is 91% with higher stage disease survival as low as 70%.
Non-Hodgkin’s Lymphoma
NHL is the most prevalent hematopoietic neoplasm and
includes many clinicopathologic subtypes, the majority
of which are of B-cell origin. Each subtype has its own
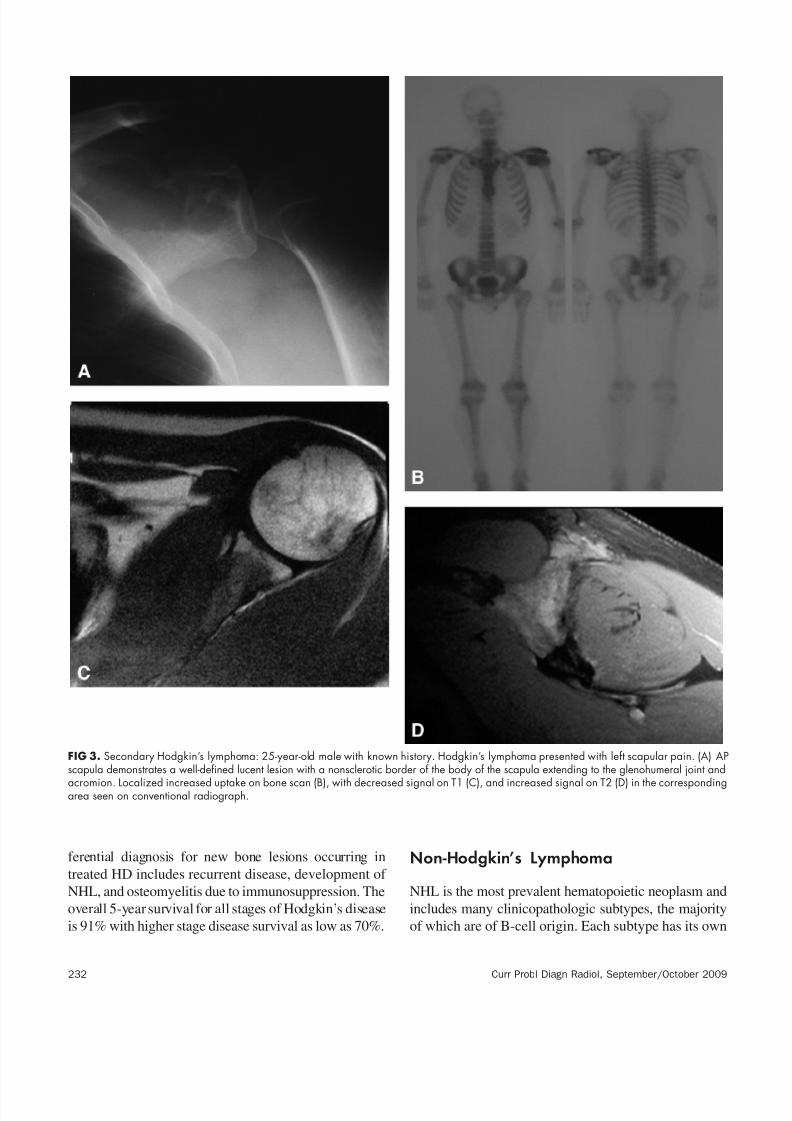
FIG 3. Secondary Hodgkin’s lymphoma: 25-year-old male with known history. Hodgkin’s lymphoma presented with left scapular pain. (A) APscapula demonstrates a well-defined lucent lesion with a nonsclerotic border of the body of the scapula extending to the glenohumeral joint and
acromion. Localized increased uptake on bone scan (B), with decreased signal on T1 (C), and increased signal on T2 (D) in the correspondingarea seen on conventional radiograph.
232 Curr Probl Diagn Radiol, September/October 2009
8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 6/9
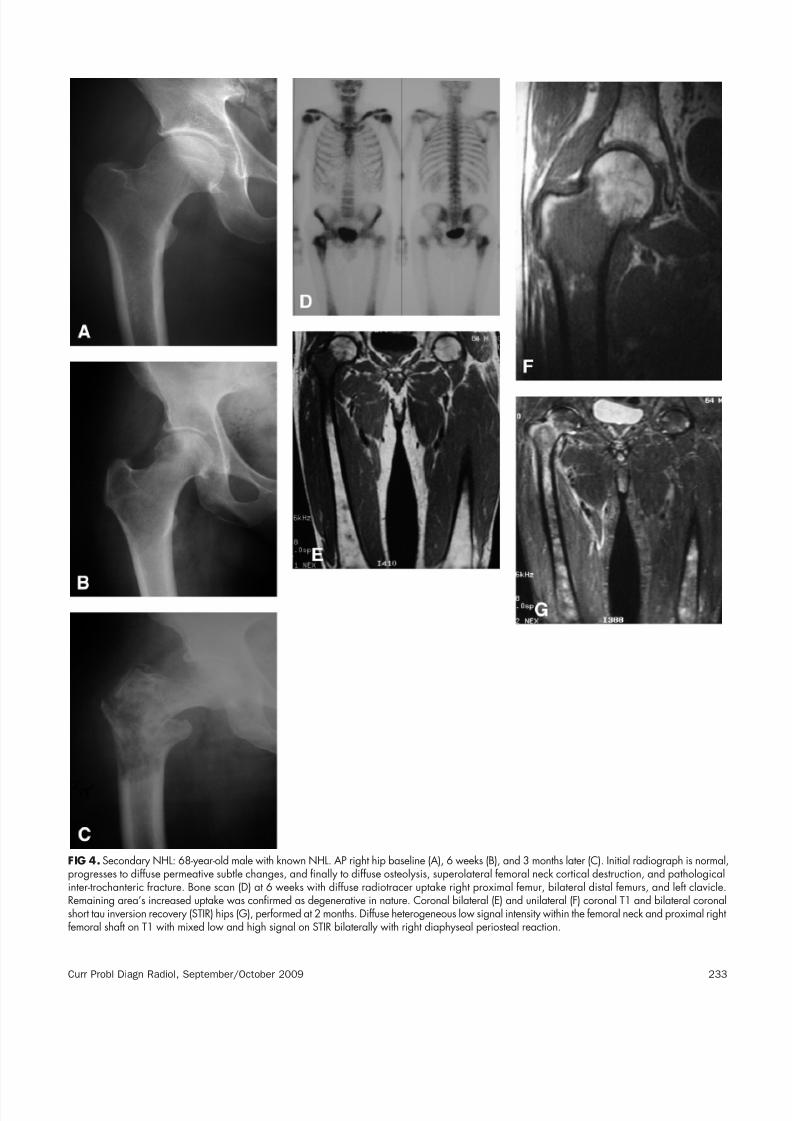
FIG 4. Secondary NHL: 68-year-old male with known NHL. AP right hip baseline (A), 6 weeks (B), and 3 months later (C). Initial radiograph is normal,progresses to diffuse permeative subtle changes, and finally to diffuse osteolysis, superolateral femoral neck cortical destruction, and pathologicalinter-trochanteric fracture. Bone scan (D) at 6 weeks with diffuse radiotracer uptake right proximal femur, bilateral distal femurs, and left clavicle.Remaining area’s increased uptake was confirmed as degenerative in nature. Coronal bilateral (E) and unilateral (F) coronal T1 and bilateral coronalshort tau inversion recovery (STIR) hips (G), performed at 2 months. Diffuse heterogeneous low signal intensity within the femoral neck and proximal rightfemoral shaft on T1 with mixed low and high signal on STIR bilaterally with right diaphyseal periosteal reaction.
Curr Probl Diagn Radiol, September/October 2009 233

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 7/9
distinct epidemiology, etiology, morphology, immuno-
phenotype, genetics, clinical features, and response to
therapy.20 In general, those of a large cell type withdiffuse rather than nodular type growth have a more
aggressive pattern of growth. It is more common in
males, 1.4:1, and affects all ages with a median age of 55
years. Patients predisposed to developing NHL includethose with congenital immunosuppression, those with
FIG 5. Primary bone lymphoma: 60-year-old male with left ankle tenderness post trauma. (A) AP ankle demonstrating a subtle permeativedestruction distal tibial diametaphysis initially thought normal. Repeat radiograph (B) at 10 weeks shows rapid progression with diffuse osteolysisextending into diaphysis with exuberant periosteal reaction. Coronal T1 (C) and sagittal STIR (D) MRI sequences correlate with above findings withdiffuse low signal intensity on T1 and high signal on STIR with cortical destruction on medial and lateral borders. Extensive soft-tissue infiltration,low on T1, and high signal on STIR, not appreciated on radiographs. This example stresses the initial subtle changes that may progress rapidly.
234 Curr Probl Diagn Radiol, September/October 2009

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 8/9

8/18/2019 LinFoma radiology
http://slidepdf.com/reader/full/linfoma-radiology 9/9
ous T-cell lymphoma (CTCL). MF is the most com-
mon type of CTCL. Sezary syndrome is a variant of MF occurring in 5% of cases. The skin is the primary
site of involvement. Stage IVB disease is character-
ized by visceral, including skeletal, involvement. The
disease occurs more frequently in men, 2:1, and mayoccur in all age groups, but patients are commonly in
the sixth decade with a mean age at presentation of 50
years.Three separate types of bone lesion occur and
predominantly affect the appendicular skeleton: osteo-
lytic, osteoblastic, and diffuse osteoporosis.25-27 Cor-tical bone destruction with associated soft-tissue mass
and periostitis may occur. Sezary syndrome is the
leukemic phase of MF with generalized erythroder-
ma.28 It is associated with a symmetrical seronegative
polyarthritis secondary to malignant synovial infiltra-
tion.29 Marrow involvement occurs in up to 20% of
patients with CTCL and is often present at the time of diagnosis and may be nodular localized or infiltrative.
When the latter is present, it is associated with diffuse
dissemination and a shortened survival time.29 StageIVB disease has a mean survival of 18 months.
REFERENCES1. Jaffe ES, Harris NL, Stein H, et al. World Health Organization
Classification of Tumors: Pathology and Genetics of Tumors
of Haematopoietic and Lymphoid Tissues. Lyon, France:
IARC Press, 2001.
2. Miller TP, Jones SE. Hodgkin’s disease and non-Hodgkin’s
lymphoma. In: Stein JH, editor. Internal Medicine, 3rd edition.Boston, MA: Little, Brown, 1990, p 1136.
3. Resnick D. Diagnosis of Bone and Joint Disorders, 4th
edition. Philadelphia, PA: WB Saunders, 2002. p. 2303-45.
4. Coles WC, Schulz MD. Bone involvement in malignant
lymphoma. Radiology 1948;50:458.
5. Ewing J. A review of the classification of bone tumors. Surg
Gynecol Obstet 1939;68:971-76.
6. Mulligan ME. Lymphoma, bone. Available at: www.emedicine.
com. Accessed August 30, 2001.
7. Mulligan ME, McRae GA, Murphey MD. Imaging features of
primary lymphoma of bone. AJR 1999;173:1691-7.
8. Parker BR, Marglin S, Castellino RA. Skeletal manifestations
of leukemia, Hodgkin’s disease and non-Hodgkin’s lym-
phoma. Semin Roentgenol 1980;15:302.
9. Hermann G, Klein MJ, Adbelwahab IF, et al. MRI appearance
of primary non-Hodgkin’s lymphoma of bone. Skeletal Radiol
1997;26:629-32.
10. Heyning F, Kroon H, Hogendoorn P, et al. MR imaging charac-
teristics in primary lymphoma of bone with emphasis on non-
aggressive appearance. Skeletal Radiol 2007;36:937-44.
11. Fidias P, Spiro I, Sobczak ML. Long-term results of combined
modality therapy in primary bone lymphomas. Int J Radiat
Oncol Biol Phys 1999;45:1213-8.
12. Beal K, Allen L, Yahalom J. Primary bone lymphoma treat-
ment results and prognostic factors with long-term follow-up
of 82 patients. Cancer 2006;106:2652-6.13. Huvos AG. Skeletal manifestations of malignant lymphomas
and leukemias. In: Huvos AG, editor. Bone Tumors: Diagno-
sis, Treatment and Prognosis. Philadelphia, PA: WB Saun-
ders, 1979. p. 625-37.
14. Ostrowski ML, Unni KK, Banks PM, et al. Malignant lym-
phoma of bone. Cancer 1986;58:2646-55.
15. Melamed JW, Martinez S, Hoffman CJ. Imaging of primary
multifocal osseous lymphoma. Skeletal Radiol 1997,26:35-41.
16. Linden A, Zankovich R, Theissen P, et al. Malignant
lymphoma: Bone marrow imaging versus biopsy. Radiology
1989;173:335-9.
17. Varan A, Cila A, Buyukpamukcu M. Prognostic importance of
magnetic resonance imaging in bone marrow involvement of Hodgkin disease. Med Pediatr Oncol 1999;32:267-71.
18. Edeiken-Monroe B, Edeiken J, Kim EE. Radiologic concepts
of lymphoma of bone. Radiol Clin North Am 1990;28:841-64.
19. Guermazi A, Brice P, de Kerviler EE, et al. Extranodal
Hodgkin disease: Spectrum of disease. Radiographics 2001;
21:161-79.
20. Estrada D, Rajdev L, Sparano JA. Lymphoma, Non-Hodgkin’s.
Available at: www.emedicine.com. Accessed July 2002.
21. Moazzam N, Malik AA, Potti A. B-cell lymphoma mimicking
multiple myeloma. J Nucl Med 2002;43:1295-303.
22. Ahmed M, Khan AH, Mansoor A, et al. Burkitt’s lymphoma—
A study of 50 consecutive cases. J Pak Med Assoc 1993;43:
151-3.
23. Sariban E, Donahue A, Magrath IT. Jaw involvement inAmerican Burkitt’s lymphoma. Cancer 1984;53:1777-82.
24. Anavi Y, Kaplinsky C, Calderon S, et al. Head, neck and
maxillofacial childhood Burkitt’s lymphoma: A retrospective
analysis of 31 patients. J Oral Maxillofac Surg 1990;48:708-13.
25. Brigham BA, Bunn PA Jr, Horton JE, et al. Skeletal manifes-
tations in cutaneous T-cell lymphomas. Arch Dermatol 1982;
118:461-7.
26. Greer KE, Legum LL, Hess CE. Multiple osteolytic lesions in
a patient with mycosis fungoides. Arch Dermatol 1977;113:
1242-4.
27. O’Reilly GV, Clark TM, Crum CP. Skeletal involvement in
mycosis fungoides. AJR 1977;129:741-3.
28. Savin H, Zimmermann B 3rd, Aaron RK, et al. Seronegativesymmetric polyarthritis in Sezary syndrome. J Rheumatol
1991;18:464-7.
29. Salhany KE, Greer JP, Cousar JB, et al. Marrow involvement
in cutaneous T-cell lymphoma. A clinicopathologic study of
60 cases. Am J Clin Pathol 1989;92:747-54.
236 Curr Probl Diagn Radiol, September/October 2009