research prioritization topic briefs · pdf fileresearch prioritization topic briefs pcori...
TRANSCRIPT

Addressing Health Disparities Topic Briefs 1
Research Prioritization Topic Briefs PCORI Scientific Program Area: Addressing Health Disparities Prepared for PCORI by researchers at the University of North Carolina at Chapel Hill April 16, 2013
Addressing Health Disparities Topic Briefs 2
TABLE OF CONTENTS
ADVISORY PANEL DISCUSSANTS 3
ADVISORY PANEL SCORING GUIDE 5
TOPIC 1: COMMUNICATING RISKS FOR MINORITIES OR LOW LITERACY PATIENTS 6
TOPIC 2: CARE COORDINATION FOR SPECIAL NEEDS PATIENTS 13
TOPIC 3: CARE COORDINATION IN PRIMARY CARE 17
TOPIC 4: INTERVENTIONS FOR IMPROVING BIRTH OUTCOMES 22
TOPIC 5: HEART ATTACKS AMONG RACIAL AND ETHNIC MINORITIES 26
TOPIC 6: TELEMEDICINE FOR RURAL CARDIOVASCULAR CARE 32
TOPIC 7: TELEMEDICINE FOR RURAL MENTAL HEALTH CARE 36
TOPIC 8: REDUCE FOOT AMPUTATIONS IN MINORITIES 40
TOPIC 9: BREAST CANCER SCREENING FOR HIGH-RISK WOMEN 45
TOPIC 10: RURAL TRAUMA CARE 49
TOPIC 11: HYPERTENSION IN MINORITIES 54
TOPIC 12: COMPLEMENTARY MEDICINE FOR JUVENILE CANCER PATIENTS 61

Addressing Health Disparities Topic Briefs 3
To start discussion of each topic on April 19-20, (and engage all panelists), *primary discussant summarizes the topic (5
minutes); secondary discussant can add any additional information (2 minutes).
Advisory Panel Discussants
Brief Num.
Short Name Topic *Primary
Secondary
1
Communicating risks for minorities or low health literacy patients
Compare the effectiveness of physician/patient communication models on improving risk communication in racial and ethnic minorities, patients with low literacy, or medically underserved populations.
*Liz Jacobs Grant Jones
2 Care coordination for special needs patients
Compare the effectiveness of care coordination and clinical decision supports in producing better health outcomes for children with disabilities and special health care needs.
*Alfiee Breland-Noble
Alan Morse
3 Care coordination in primary care
Compare the effectiveness of enhanced care coordination, including multicultural approaches on improving the health care process and outcomes in primary care settings.
*Deborah Stewart Martina Gallagher
4 Interventions for improving birth outcomes
Compare the effectiveness of multi-level interventions (e.g., community-based, health education, usual care) on reducing disparities in birth outcomes.
*Echezona Ezeanolue
Venus Gines
5 Heart attacks among racial & ethnic minorities
Compare the effectiveness of health center interventions to enhance the "Million Hearts" program and reduce major vascular events among the economically disadvantaged, including racial and ethnic minorities and rural populations.
*Kevin Fiscella Martin Gould
6 Telemedicine for rural cardiovascular care
Compare the effectiveness of telemedicine and/or expanding practice to non-physician practitioners (i.e. nurse practitioners, physician assistants) on improving cardiovascular disease outcomes in rural populations.
*Jacqueline Grant Tiffany Nelson
7 Telemedicine for rural mental health care
Compare the effectiveness of telemedicine and/or expanding practice to non-physician practitioners (i.e. nurse practitioners, physician assistants) on improving mental health disease outcomes in rural populations.
*Patrick Kitzman Alfiee Breland-
Noble
8 Reduce foot amputations in minorities
Compare the effectiveness of interventions on reducing disparities in revascularization efforts to prevent foot amputation in racial and ethnic minorities.
*Russell Rothman Mary Sander
Addressing Health Disparities Topic Briefs 4
Brief Num.
Short Name Topic *Primary Secondary
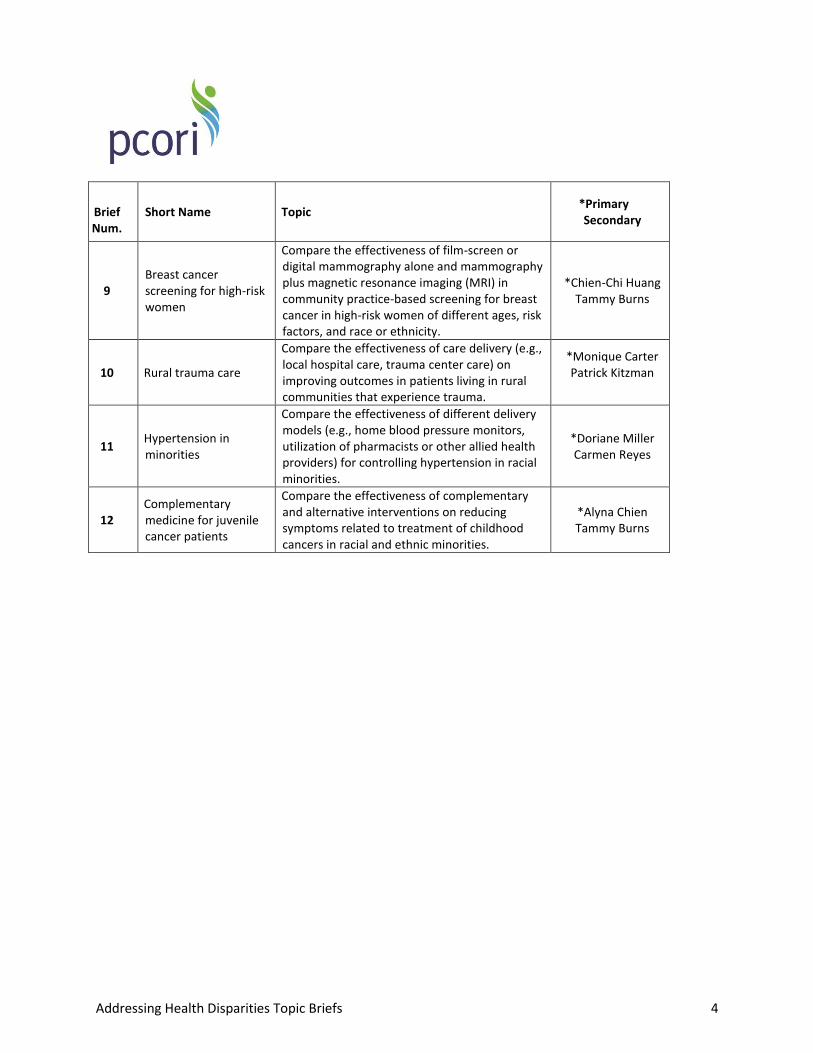
9 Breast cancer screening for high-risk women
Compare the effectiveness of film-screen or digital mammography alone and mammography plus magnetic resonance imaging (MRI) in community practice-based screening for breast cancer in high-risk women of different ages, risk factors, and race or ethnicity.
*Chien-Chi Huang Tammy Burns
10 Rural trauma care
Compare the effectiveness of care delivery (e.g., local hospital care, trauma center care) on improving outcomes in patients living in rural communities that experience trauma.
*Monique Carter Patrick Kitzman
11 Hypertension in minorities
Compare the effectiveness of different delivery models (e.g., home blood pressure monitors, utilization of pharmacists or other allied health providers) for controlling hypertension in racial minorities.
*Doriane Miller Carmen Reyes
12 Complementary medicine for juvenile cancer patients
Compare the effectiveness of complementary and alternative interventions on reducing symptoms related to treatment of childhood cancers in racial and ethnic minorities.
*Alyna Chien Tammy Burns
Addressing Health Disparities Topic Briefs 5
Please rate each topic based on the following criteria. The scale ranges from a low of one (1) to a high of five (5). Rating Scale: 1-Low 2 3 4 5-High
Patient-Centeredness. Is the proposed research focused on questions and outcomes of specific interest
to patients, their caregivers, and clinicians? Is the proposed research focused on questions and
outcomes of specific interest to patients, their caregivers, and clinicians?
Impact of the Condition on the Health of Individuals and Populations. Is the condition or disease
associated with a significant burden in the US population? Burden of disease may be measured by how
many people have the disease (prevalence); how many new cases occur every year (incidence); and
other measures such as mortality, morbidity, individual suffering, and loss of productivity. PCORI is also
interested in rare diseases.
Options for Addressing the Issue. What current guidance is available on the topic, and is there ongoing
research? How does this help determine whether further research in this area would be valuable?
Likelihood of Implementation in Practice. Would new information generated by research be likely to
have an impact in practice? Research is valuable when it leads to the use of more beneficial treatments
or interventions. Providing new evidence by itself does not ensure that the results of research will be
used in clinical practice. Several factors may influence uptake in practice, including the knowledge and
behaviors of health professionals, the acceptability to patients, and coverage or payment policies.
Durability of Information. Would new information on this topic remain current for several years, or
would it be rendered obsolete quickly by subsequent studies? Durability is generally associated with the
rate at which new clinical evidence and/or better alternatives for patient management are emerging.
Durability might be limited when there are rapid modifications to procedures and techniques. This
commonly occurs in domains such as medical device development.
Advisory Panel Scoring Guide
Addressing Health Disparities Topic Briefs 6
Compare the effectiveness of physician/patient communication models on improving risk communication in racial and ethnic minorities, patients with low literacy, or medically underserved populations.
Introduction This topic brief focuses on physician/patient communication models for improving risk communication in adult populations, with an emphasis on racial and ethnic minorities, patients with low literacy, or medically underserved populations. Risk communication involves information such as potential risks, benefits, how to avoid harm1, and how to improve self-care—all of which are critical to patients’ ability to make informed healthcare choices.2
Risk communication involves various components, including: (1) who communicates information; (2) how information is communicated (verbally, visually, with supporting materials, collaboratively); (3) how much and what kind of information is communicated; (4) where information is communicated (setting); and (5) the context of the communication (values, circumstances, preferences). Current research mainly focuses on communication related to disease, condition, or behavior, rather than highlighting how communication works within various groups of people, such as those with lower literacy, racial/ethnic minorities, and the underserved. Although limited, there are resources that describe guidelines and recommendations that can be incorporated into practice.2-4
Burden on Society Poor risk communication leads to less informed choices, less satisfaction, the potential for poor health outcomes, as well as overutilization and underutilization of health services.5,6 Individuals with low literacy, racial/ethnic minorities, the medically underserved, and non–English-speaking people are more likely to experience health disparities7, 8 and are more likely to have difficulty understanding, expressing, and acting on health information.2, 9, 10 Nearly half of the US population has low or limited health literacy skills. Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.”11 Examples of skills related to health literacy include evaluating information, analyzing risks and benefits, and interpreting test results.7 Oral language skills also factor into good communication.7 Approximately 36% of adults in the United States have limited health literacy, and only 12% of the population has a proficient health literacy level.10 Those who did not graduate from high school; speak limited English; or are Hispanic, black, poor, or older (65+) are most likely to have limited health literacy.10 Health literacy potentially explains racial/ethnic health disparities,4 and there is some evidence that limited numeracy skills may also contribute to disparities in health outcomes.5
Topic 1: Communicating Risks for Minorities or Low Literacy Patients

Addressing Health Disparities Topic Briefs 7
Limited access to care due to uninsurance is a barrier to risk communication. The medically underserved have barriers to healthcare access and are defined as uninsured, underinsured, or poor with insurance.8 Twenty-one percent of the civilian, non-institutionalized US population (18–64) was uninsured based on data from the 2011 National Health Interview Survey, while 40% of poor and 40% of near-poor adults aged 18–64 lacked coverage at the time of interview. When examining by race-ethnicity, Hispanic persons were most likely to be uninsured (more than 25%) compared to their white counterparts.12 Limited English proficiency is a barrier to appropriate risk communication. Language is an important barrier to good risk communication. According to the US Census Bureau, 20% of the US population aged 5 and older speak a language other than English inside the home, and, of those households, 24% report speaking English “not well” or “not at all.”13 Over 60% of these households speak Spanish. Evidence that Addresses Risk Communication Sparse and diverse literature exists that directly addresses risk communication among racial and ethnic minorities and the medically underserved. Adults with limited literacy skills have trouble with basic health information and understanding risks of treatments or medical care,14,15 and they are more likely to have poor health outcomes.5 Low health literacy appears to limit the quality of health decision making16,17 and patients’ ability to act on information concerning treatment risks and benefits,18
particularly among older adults.18 Although patient participation is essential in risk communication, it has been shown that individuals with lower functional literacy perceive their role in shared decision making as consenting to a treatment recommendation, whereas younger patients,19 and those with higher education and functional literacy,17,19 are more likely to view decision making as a collaborative process. There is some evidence that poor communication of risk affects patients. A study among newly diagnosed patients with lung cancer found that the decision not to pursue surgery—the only reliable treatment for cure—was associated with poor patient-physician communication. This contributed to an 11% difference between black patients, who were less likely to pursue surgery, and white patients, who were more likely.20 A study of low-income underinsured/uninsured women with heart disease risk factors found that, after one year, 66% could not recall being told their condition (e.g., high blood pressure, high cholesterol, or diabetes). Authors attributed this to a provider-patient communication gap or to difficulties in retaining health information.21 Those with the lowest levels of education were the least likely to recall their condition. Evidence addressing risk communication relevant to race and ethnicity is limited and focuses on issues such as cultural competency,22 patient and provider concordance (social concordance, racial/ethnic concordance),23,24 trust, and the role of ethnic communities in influencing risk perceptions.25 A single study comparing effectiveness of patient-centered collaborative care verses standard care among African American patients in primary care settings found similar improvements in clinical outcomes and better ratings of care for those with patient-centered collaborative care.26 One study found that African American patients’ perceptions of a physician’s race impacts patients’ accuracy in risk perceptions, where participants with a racially discordant physician had less accurate risk perceptions, independent of other factors, such as trust in the provider, engagement with the healthcare system, or

Addressing Health Disparities Topic Briefs 8
attention during the encounter.23 Finally, two studies note the role of social networks and communities as having an influential role in decision making beyond the patient-physician relationship.17,25 Options for Addressing the Issue The literature on risk communication is developing and offers limited information on communication among populations at greatest risk of poor health outcomes. Systematic reviews on risk communication focus on a small number of content areas: (1) communication design, such as how to quantitatively present risk; (2) how people process information, and whether it is preferable to present detailed versus limited information; and (3) the method of communication, such as comparing verbal versus visual presentation of risk. The literature focuses on outcomes such as informed choice, decisional clarity, decision making in accordance with values, and implications on actual behavior (such as cancer screening or smoking cessation).
The evidence to support the best interventions for improving risk communication—such as, type, format, content—is inconsistent. Much of the evidence on the best approaches to improve risk communication focuses on the format for populations who share common health conditions or procedures, and not necessarily on populations with common demographic characteristics.4, 27-31 This may provide a useful foundation for new research testing formats among populations at high risk for health disparities. One synthesis of existing empirical evidence, and consultations with experts in risk communication, could not recommend a clear communication format for presenting risk (verbal , visual, and numeric) because of: (1) lack of consistency in testing formats using the same outcomes, (2) lack of strongly designed studies comparing formats, and (3) lack of theoretical progress in explaining why one format should work better in a specific context than others.4 One promising communication tool—decision aids—has been shown to increase patient knowledge, encourage more active patient involvement in decision making, decrease levels of anxiety, and lead to informed values-based decisions. However, less is known about their effect on adherence, consultation length, patient-provider communication, and use with low literacy populations. This is an area where there is a need for further research.32-34 Motivational interviewing is a technique recommended by the Centers for Disease Control and Prevention (CDC) to promote shared decision making among Medicare beneficiaries.35 This technique echoes risk communication recommendations, where information is communicated in a personalized and collaborative manner and repeated back by the patient to make sure it is understood (“teach-back”).35,36 Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Although risk communication and shared decision making align well with patient-centered outcomes research and the principles of patient-centered medical homes, we need to learn more about how to create and disseminate strategies specifically for populations at greatest risk of poor health outcomes. Additionally, more knowledge is needed around implementing these strategies in clinical practice. One challenge to shared decision making is inadequate communication. Healthcare professional training on risk communication and shared decision making has been shown to be effective in building patient-centered skills among providers, though effects on patient satisfaction, health behavior, and health
Addressing Health Disparities Topic Briefs 9
status are mixed according to one systematic review,37 while another review says provider training on shared decision making “may be important,”33 and the adoption of shared decision making into clinical practice deserves further investigation.
New Directions for Research Research on this topic will remain current for several years. Researchers note multiple areas for further investigation, including exploring the effectiveness of different formats for presenting of probability information regarding health decisions,38 as well as exploring the best methods for communicating risk to racial/ethnic minorities, patients with low literacy, or the medically underserved, in daily clinical practice.39 Other areas include how to prioritize risks and decisions relative to others for best overall health and examination into other factors, such as personal context, social networks, or spiritual beliefs, and how they contribute to risk communication and decision making.

Addressing Health Disparities Topic Briefs 10
References 1. Weinstein ND. What does it mean to understand a risk? Evaluating risk comprehension. Monogr
Natl Cancer Inst. 1999;25. 2. Fischhoff B, Brewer NT, Downs JS. Communicating Risks and Benefits: An Evidence-Based User’s
Guide: Food and Drug Administration (FDA). Rockville, Md: US Dept of Health and Human Services; 2011.
3. Doak CC, Doak LG, Root J. Teaching Patients with Low Literacy Skills. 2nd ed. Philadelphia: JB Lippincott Company; 1996.
4. Lipkus I. Numeric, verbal, and visual formats of conveying health risks: suggested best practices and future recommendations. Med Decis Making. 2007;27(5).
5. Berkman ND, Sheridan SL, Donahue KE, et al. Health literacy interventions and outcomes: an updated systematic review. Evid Rep Technol Assess. 2011;Mar(199).
6. Price-Haywood EG, Roth KG, Shelby K, Cooper LA. Cancer risk communication with low health literacy patients: a continuing medical education program. J Gen Intern Med. 2010;25(suppl 2).
7. Glassman P. Health Literacy: National Network of Libraries of Medicine. ND. 8. CDC health disparities and inequalities report—United States, 2011. MMWR. Jan 14, 2011;60(suppl). 9. National Center for Education Statistics. National Assessment of Adult Literacy, key findings.
http://nces.ed.gov/naal/kf_demographics.asp. Accessed March 5, 2013. 10. Kutner M, Greenberg E, Jin Y, Paulsen C. The health literacy of America’s adults: results from the
2003 National Assessment of Adult Literacy. 2006. http://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2006483 . Accessed March 2, 2013.
11. Nielsen-Bohlman L, Panzer A, Kindig D, Eds. Health literacy: a prescription to end confusion.2004.http://www.iom.edu/Reports/2004/Health-Literacy-A-Prescription-to-End-Confusion.aspx. Accessed March 23, 2013.
12. Cohen R, Martinez M. Health insurance coverage: early release of estimates from the National Health Interview Survey. 2011. http://www.cdc.gov/nchs/data/nhis/earlyrelease/insur201206.pdf. Accessed March 18, 2013.
13. Shin HB, Kominski RA. Language use in the United States: 2007—American Community Survey Reports. 2010. <http://www.census.gov/prod/2010pubs/acs-12.pdf>. Accessed March 22, 2013.
14. Williams MV, Davis T, Parker RM, Weiss BD. The role of health literacy in patient-physician communication. Fam Med. 2002;34(5).
15. Davis TC, Williams MV, Marin E, Parker RM, Glass J. Health literacy and cancer communication. CA Cancer J Clin. 2002;52(3).
16. Kim SP, Knight SJ, Tomori C, et al. Health literacy and shared decision making for prostate cancer patients with low socioeconomic status. Cancer Invest. 2001;19(7).
17. Smith SK, Dixon A, Trevena L, Nutbeam D, McCaffery KJ. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc Sci Med. 2009;69(12).
18. Amalraj S, Starkweather C, Nguyen C, Naeim A. Health literacy, communication, and treatment decision-making in older cancer patients. Oncology. 2009;23(4).
19. Sheridan SL, Harris RP, Woolf SH. Shared decision making about screening and chemoprevention. A suggested approach from the US Preventive Services Task Force. Am J Prev Med. 2004;26(1).
Addressing Health Disparities Topic Briefs 11
20. Cykert S, Dilworth-Anderson P, Monroe MH, et al. Factors associated with decisions to undergo surgery among patients with newly diagnosed early-stage lung cancer. JAMA. 2010;303(23):2368-2376.
21. Khavjou OA, Finkelstein EA, Farris R, Will JC. Recall of three heart disease risk factor diagnoses among low-income women. J Womens Health. 2009;18(5).
22. Anderson LM, Scrimshaw SC, Fullilove MT, Fielding JE, Normand J. Culturally competent healthcare systems—a systematic review. Am J Prev Med. 2003;24(3s).
23. Persky S, Kaphingst K, Allen VJ, Senay I. Effects of patient-provider race concordance and smoking status on lung cancer risk perception among African-Americans. Ann Behav Med. 2013;Feb 7 2013(E pub).
24. Thornton RL, Powe NR, Roter D, Cooper LA. Patient-physician social concordance, medical visit communication, and patient’s perceptions of health care quality. Patient Educ Couns. 2011;85(3).
25. Caron RM, Tshabangu-Soko T, Finefrock K. Childhood lead poisoning in a somali refugee resettlement community in New Hampshire. J Community Health. 2013;Mar 3 2013 (Epub).
26. Cooper LA, Ghods Dinoso BK, Ford DE, et al. Comparative effectiveness of standard versus patient-centered collaborative care interventions for depression among African Americans in primary care settings: the Bridge Study. Health Serv Res. 2013;48(1).
27. Epstein RM, Alper BS, Quill TE. Communicating evidence for participatory decision making. JAMA. 2004;291(19).
28. Waldron C, van der Weijden T, Ludt S, Gallacher J, Elwyn G. What are effective strategies to communicate cardiovascular risk information to patients? A systematic review. Patient Educ Couns. 2011;82(2).
29. Burkiewicz J, Vesta K, Hume A. Improving effectiveness in communicating risk to patients. Consult Pharm. 2008;23(1).
30. Hollands GJ, Hankins M, Marteau TM. Visual feedback of individuals' medical imaging results for changing health behavior. Cochrane Database of Systematic Reviews. 2010.
31. Edwards AGK, Naik G, Ahmed H, et al. Personalised risk communication for informed decision making about taking screening tests. Cochrane Database of Systematic Reviews. 2013.
32. Stacey D, Bennett CL, Barry MJ, Col NF, Eden KB. Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews. 2011.
33. Légaré F, Ratté S, Stacey D, et al. Interventions for improving the adoption of shared decision making by healthcare professionals. Cochrane Database of Systematic Reviews. 2010.
34. Lin GA, Aaronson DS, Knight SJ, Carroll PR, Dudley RA. Patient decision aids for prostate cancer treatment: a systematic review of the literature. CA Cancer J Clin. 2009;59(6).
35. Goetzel RZ, Staley P, Ogden L. A framework for patient-centered health risk assessments—providing health promotion and disease prevention services to Medicare beneficiaries. 2011. http://www.cdc.gov/policy/opth/hra Accessed March 22, 2013.
36. Epstein RM, Alper BS, Quill TE. Communicating evidence for participatory decision-making. JAMA. 2004;291(19).
37. Dwamena F, Holmes-Rovner M, Gaulden CM, et al. Interventions for providers to promote a patient-centered approach in clinical consultations. Cochrane Database of Systematic Reviews. 2012.
38. Visschers VH, Meertens RM, Passchier WW, de Vries NN. Probability information in risk communication: a review of the research literature. Risk Anal. 2009;29(2).

Addressing Health Disparities Topic Briefs 12
39. Roach P, Marrero D. A critical dialogue: communicating with type 2 diabetes patients about cardiovascular risk. Vasc Health Risk Manag. 2005;1(4).
Addressing Health Disparities Topic Briefs 13
Compare the effectiveness of care coordination and clinical decision supports in producing better health outcomes for children with disabilities and special healthcare needs
Introduction This topic brief provides an overview of the comparative effectiveness of care coordination and clinical decision supports to enhance health outcomes for children with special healthcare needs (CSHCN)*. Care coordination refers to the implementation of care plans “by a variety of service providers and programs in an organized fashion,” which involves “needs identification, assessment, prioritizing, and monitoring.”4 Clinical decision supports are computerized tools that provide healthcare providers, patients, staff, and other individuals with well-filtered clinical and patient-specific information at appropriate times in order to help improve clinical decision making.5 The population of CSHCN is broadly defined by the Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB) to include all children who have, or are at increased risk for, chronic physical, developmental, behavioral, or emotional conditions and who require health and related services beyond the needs of most children.6 The scope of this brief is focused on the overall CSHCN population, rather than any particular subgroups. Gaps exist in access to needed care and support services. The vast majority of CSHCN have consistently received some form of continuous public or private health insurance coverage within the last year, with continuous coverage for over 90% in 2010.7,8 Still, health plan coverage for about a third of families caring for CSHCN fails to provide enough financial assistance to make out-of-pocket costs reasonable, and about 14% of families with continuous coverage experience an unmet need for specific care services.9 About 20% of these families have difficulty getting referrals, which could result in a gap in continuity of care.9 Coordinated care may improve effectiveness and efficiency of care for CSHCN. One approach that can be used to improve access to needed care services while increasing the efficiency of care for CSHCN is coordinated care that is comprehensive and family-centered. Leading national advocacy groups for the health of children and their families, such as the American Academy of Pediatrics (AAP) and the MCHB, have identified effective care coordination as being essential to improve patient-centered outcomes for
* Children ages 0–17 are considered to have special healthcare needs when they meet at least one of five screening criteria
according to the 2009/2010 National Survey of Children with Special Health Care Needs (NSCSHCN): (1) they currently need or use prescription medicine, other than vitamins, for a condition which has lasted or is expected to last for a minimum of 12 months; (2) their need or use of medical care, mental health, or educational services exceeds normal care or service usage for most children of the same age; (3) their ability to participate in activities most children of the same age can do is limited or prevented by their condition(s); (4) they need or receive special therapy; or (5) they have an emotional, developmental, or behavioral problem requiring treatment or counseling.
1-3
Topic 2: Care Coordination for Special Needs Patients

Addressing Health Disparities Topic Briefs 14
CSHCN and their families. In particular, the patient-centered medical home (PCMH) model is considered to be the optimal approach to deliver coordinated care.4 Delivery of healthcare services within medical homes is guided by the needs of the individual child and family, the primary care physician’s expertise in treating CSHCN, and family/physician collaboration in coordinating care.4 Within the medical home, a practice care coordinator will ideally participate in developing a plan of care with the family and physician and also help the family access needed services.4 Despite the promise of medical home-based coordinated care, 57% of CSHCN did not receive coordinated care within a PCMH between 2009 and 2010.8 Clinical decision supports may increase patient-centeredness and appropriateness of care for CSHCN. Although not widely incorporated in the delivery of healthcare services to CSHCN, clinical decision supports have the potential not only to help clinicians provide optimal evidence-based care to CSHCN, but also to involve families in clinical decision making to a greater extent. Support tools are usually components of comprehensive electronic health record (EHR) systems, but they may also be used independently. Clinical decision supports can range from computerized reminders for providers and patients with reference information appropriate for the individual child’s needs.5 Family-oriented clinical decision supports may be especially useful for helping families of CSHCN choose the most culturally and personally acceptable services for their children. Burden on Society Prevalence: approximately 15% of children in the United States have special healthcare needs.8 Many of those children (45%) have four or more functional limitations affecting their daily lives.8 A significant portion of CSHCN experienced behavior problems (41%), and 43% experienced anxiety or depression in 2009 and 2010.8 Health service use is much higher among CSHCN. Compared with other children, CSHCN, by definition, require much more intensive healthcare services to meet their healthcare and other service needs. According to data from the 2000 Medical Expenditure Panel Survey (MEPS), CSHCN had about four times the number of hospitalizations and spent seven times as many days receiving hospital care.10 In addition, they used seven times as many annual visits to non-physician healthcare providers as other children, including other primary care providers, mental healthcare providers, and allied healthcare providers such as physical therapists. CSHCN also took five times as many prescribed medications as other children.10 In 2008, the average expenditure per CSHCN with any healthcare expenses ($4,100) exceeded that for children without special healthcare needs ($983) by nearly fourfold.11
CSHCN families face financial and employment burdens. Meeting the healthcare and other service needs of CSHCN can impose heavy financial and employment-related burdens on their families. Data from the 2000 MEPS indicate that families spent, on average, $352 annually on out-of-pocket expenses for all healthcare and special services, about twice as much as the $174 average annual out-of-pocket spending by families without CSHCN at the time.10 One recent systematic review synthesized 32 cross-sectional and longitudinal studies measuring how out-of-pocket expenses and employment status vary among families caring for CSHCN.12 Families’ burden depended on the severity and type of conditions

Addressing Health Disparities Topic Briefs 15
affecting children, with families of children with more severe conditions requiring the most out-of-pocket expenses and the greater likelihood of reducing working hours.12,13 Options for Addressing the Issue Little research exists on effectiveness of care coordination among CSHCN. One recent AHRQ systematic review included seven studies that reported improved patient-reported experiences when better care coordination existed in different PCMH interventions .14 Another review of 35 studies provided evidence that hospital-based comprehensive care emphasizing coordination is associated with positive changes in care effectiveness, family-centeredness of care, and patient safety.15 However, this review included studies that were not designed to evaluate effectiveness or that used designs that are prone to bias. Limited evidence exists about the feasibility of using family-oriented decision support interventions for CSHCN. Numerous studies have shown that provider-focused clinical decision supports can reduce medication errors for pediatric inpatients and improve vaccination rates among children with asthma, for example.16,17 However, there is only limited evidence about the feasibility of using family-oriented decision support interventions for CSHCN, and no evidence to date about the ability of such interventions to improve patient-centered outcomes.16,18 Several groups, such as the AAP, are currently working to fill this gap by promoting initiatives to integrate patient-recorded data in regular clinical practice.19 Potential for New Information to Rapidly Improve Care and Patient-Centered Outcomes The practice of coordinating the complex, multidisciplinary care appropriate for CSHCN is key in improving their patient-centered outcomes, but multiple barriers to implementation continue to persist. These may include: (1) lapses in communication among healthcare providers and organizations involved in care; (2) a lack of clearly defined roles among healthcare teams, community agencies, and families; and (3) language and cultural barriers.4 Data linking care coordination interventions to patient-centered outcomes for CSHCN is very limited, although what is available suggests that enhancing care coordination may hold promise as a strategy to improve health and related outcomes for CSHCN and their families. Healthcare reform under the Affordable Care Act has created new incentives for healthcare organizations and providers to improve quality and efficiency by implementing systems of care based on the PCMH model, which often incorporates enhanced care coordination.14 Also, clinical decision support systems have shown promise if they can be tailored to the complex needs of CSHCN and their families, and, as a result, it is expected that clinicians will begin to use decision supports more frequently. More studies on the effectiveness of those coordination efforts are needed. References 1. Bethell CD, Read D, Stein RE, Blumberg SJ, Wells N, Newacheck PW. Identifying children with special
health care needs: development and evaluation of a short screening instrument. Ambul Pediatr. Jan-Feb 2002;2(1):38-48.

Addressing Health Disparities Topic Briefs 16
2. Centers for Disease Control. 2009-2010 National Survey of Children with Special Health Care Needs Frequently Asked Questions. National Center for Health Statistics, State and Local Area Integrated Telephone Survey; 2011.
3. Centers for Disease Control. 2009-2010 National Survey of Children with Special Health Care Needs: Screener. http://www.cdc.gov/nchs/data/slaits/screener_formatted_freqs_09_10.pdf. Accessed March 21, 2013.
4. Lipkin PH. Care coordination in the medical home: integrating health and related systems of care for children with special health care needs. Pediatrics. Nov 2005;116(5):1238-1244.
5. HealthIT.gov. Clinical Decision Support (CDS). http://www.healthit.gov/policy-researchers-implementers/clinical-decision-support-cds. Accessed March 27, 2013.
6. McPherson M, Arango P, Fox H, et al. A new definition of children with special health care needs. Pediatrics. Jul 1998;102(1 Pt 1):137-140.
7. Honberg LE, Kogan MD, Allen D, Strickland BB, Newacheck PW. Progress in ensuring adequate health insurance for children with special health care needs. Pediatrics. Nov 2009;124(5):1273-1280.
8. National Survey of Children with Special Health Care Needs. NS-CSHCN 2009/10. Data query from the Child and Adolescent Health Measurement Initiative, Data Resource Center for Child and Adolescent Health website. Available at: www.childhealthdata.org. Accessed March 21, 2013.
9. Kogan MD, Newacheck PW, Honberg L, Strickland B. Association between underinsurance and access to care among children with special health care needs in the United States. Pediatrics. Nov 2005;116(5):1162-1169.
10. Newacheck PW, Kim SE. A national profile of health care utilization and expenditures for children with special health care needs. Arch Pediatr Adolesc Med. Jan 2005;159(1):10-17.
11. Davis KE. Health Care Expenses and Utilization for Children With Special Health Care Needs, 2008: Estimates for the US Civilian Noninstitutionalized Population. Rockville, MD: Agency for Healthcare Research and Quality; October 2011.
12. DeRigne L. The employment and financial effects on families raising children with special health care needs: an examination of the evidence. J Pediatr Health Care. Jul-Aug 2012;26(4):283-290.
13. Parish SL, Rose RA, Dababnah S, Yoo J, Cassiman SA. State-level income inequality and family burden of U.S. families raising children with special health care needs. Soc Sci Med. Feb 2012;74(3):399-407.
14. Williams JW, Jackson GL, Powers BJ, et al. The Patient-Centered Medical Home. Rockville, MD: Prepared by the Duke Evidence-based Practice Center under Contract No. 290-2007-10066-I; 2012. Evidence Report/Technology Assessment No. 208.
15. Cohen E, Jovcevska V, Kuo DZ, Mahant S. Hospital-based comprehensive care programs for children with special health care needs: a systematic review. Arch Pediatr Adolesc Med. Jun 2011;165(6):554-561.
16. Fiks AG. Designing computerized decision support that works for clinicians and families. Curr Probl Pediatr Adolesc Health Care. Mar 2011;41(3):60-88.
17. Shekelle PG, Morton SC, Keeler EB. Costs and benefits of health information technology. Evid Rep Technol Assess (Full Rep). Apr 2006(132):1-71.
18. Adams WG, Fuhlbrigge AL, Miller CW, et al. TLC-Asthma: an integrated information system for patient-centered monitoring, case management, and point-of-care decision support. AMIA Annu Symp Proc. 2003:1-5.
19. Schneider JH, Kim GR, Leu MG, Zuckerman AE. Policy Statement—Using personal health records to improve the quality of health care for children. Pediatrics. Jul 2009;124(1):403-409.

Addressing Health Disparities Topic Briefs 17
Compare the effectiveness of enhanced care coordination, including multicultural approaches, on improving the healthcare process and outcomes in primary care settings.
Introduction Care coordination is essential to effective delivery of health care, particularly for patients with chronic conditions and/or multiple conditions. Without efficient coordination of care, patients face increased risk of harm, disease burden, and overuse of services.1 To address the lack of coordination in health care for increasingly more complicated needs, involving multiple specialties, the National Quality Forum (NQF) defined care coordination as a “function that helps ensure that the patient’s needs and preferences for health services and information sharing across people, functions, and sites are met over time.” The NQF identified a framework with the following five key domains: (1) healthcare “home”, (2) proactive plan of care and follow-up, (3) communication, (4) information systems, and (5) transitions or handoffs.1 Given the success with which NQF posited a care coordination conceptual framework comprised of these domains, there is a strong suggestion for much more critical exploration to be completed in order to strongly recommend care coordination as an effective intervention model to improve patient-reported health outcomes. The following report is organized according to the NQF domains to identify what we know and what are important areas for development in care coordination. Burden on Society As the prevalence of chronic conditions such as diabetes increases, patients with one chronic condition may see as many as 16 physicians in one year.2 In 2000, an estimated 125 million individuals in the United States were living with at least one chronic condition, and this figure is estimated to increase to 157 million by 2020.2 Ninety-six percent of US Medicare spending is reported to cover individuals with multiple chronic conditions.3 Almost three quarters (73.1%) of US adults aged 65 and older have two or more chronic health conditions,4 and 20% of people (27 million) with a chronic illness also have activity limitations.5 With such a large and growing number of individuals having at least one chronic condition, combined with the increasing burden on the healthcare system, there is strong demand for efficiency across specialties—efficiencies building from improved communication between providers, as well as with patients. Smith and colleagues conducted a systematic review in 2012 to address the increasingly growing concern of multimorbidity.6 In their review, the authors identified organizational interventions as the most effective in addressing multimorbid health concerns. Organizational interventions target changes in health care delivery by matching the needs of patients with multimorbidity across a range of areas,
Topic 3: Care Coordination in Primary Care

Addressing Health Disparities Topic Briefs 18
such as coordination of care and medication management or incorporating other health professionals to address the needs relating to the patient’s physical and social functioning.6 Options for Addressing the Issue There is a significant body of published work that has examined several potential forms of care coordination that positively impact patient outcomes. We briefly summarize widely applied integrated care models that have been applied to various chronic conditions according to the domains of the NQF framework discussed above. Care integration may improve depression management. There are examples of care coordination models for mental health. Butler and colleagues conducted a systematic review of 26 clinical trials that tested collaborative or integrated primary care for mental illness. The authors concluded that more integration (e.g., combining primary with mental health services) was not significantly associated with improved clinical depression outcomes, but was associated with improved depression management in primary care patients.7 Chou and colleagues found that teamwork was effective for a positive impact on guideline implementation related to screening for major depressive disorder.8 In another study, the authors found no impact of a multidisciplinary team consultation on mental health (specifically, anxiety and depression), general health, and quality of life of mothers from socioeconomically deprived neighborhoods.9 Despite evidence to suggest a positive impact of care coordination, the study suggests that coordinated care for minority groups may require a unique approach that is culturally sensitive. Coordinated care may improve diabetes outcomes. Diabetes is a useful condition to consider in care coordination because management is often complex and requires coordination and consistent communication among many providers. How we incorporate information systems and technology with care coordination for diabetes and other complex conditions is important to consider when building a coordinated care team. A review by Crowley and colleagues found six studies with significant positive outcomes from coordinated care in terms of improved patient education and various diabetes mellitus outcomes (e.g., HbA1cb levels).10 Another review found a significant impact on HbA1c and LDLc in addition to the number of clinic visits and testing frequency.11 Egginton and colleagues also found evidence of positive impact on quality of life, patient satisfaction, self-care, and healthcare utilization.11 Verhoeven and colleagues reviewed teleconsultation for diabetes care. This review concluded that teleconsultations for diabetes care were feasible, cost-effective, and reliable.12 The evidence supporting coordinated care for diabetes suggests improved patient-reported outcomes in addition to improved quality of life. There is also evidence to suggest a net cost savings of coordinated care for diabetes care.12 Coordinated care may offer the additional support needed to treat patients with multimorbidity effectively. Addressing multimorbidity in patients presents complicated challenges for treatment, follow-up care, and, therefore, adherence. Coordinated care may increase likelihood for longer lasting adherence and positive health outcomes.
b A lab value that shows how well the patient is controlling his or her blood sugar over the course of a few months. c Low-density lipoprotein cholesterol, commonly referred to as “bad” cholesterol.

Addressing Health Disparities Topic Briefs 19
Smith and colleagues conducted a review to examine the effectiveness of interventions targeting multimorbidity in primary care and community settings. Ten clinical trials were reviewed, and they primarily focused on the aging population. Six of the 10 interventions applied an intervention focused on changing the organization of care delivery, usually through case management or enhanced multidisciplinary team work.6 Despite mixed results, there was a trend toward improved outcomes in terms of medication adherence.6 Williams and colleagues conducted a review of the effectiveness of strategies to improve coordination between primary care and chronic disease self-management programs for socioeconomically challenged patients. The authors identified 16 studies that used linkage strategies for a variety of functions-supporting communication, ongoing clinical care, program development, and recruitment or implementation.13 In the end, the authors concluded that there was insufficient evidence to identify the specific strategies and linkages that would most effectively link with primary healthcare providers to enhance services, transitions, and, therefore, adherence and patient outcomes. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Based on the literature reviewed, care coordination research offers some evidence to suggest both positive patient-centered outcomes and improved processes of care. Specifically, the preceding section presents various applications of care coordination that support improvements in clinical outcomes (e.g., self-care), patient satisfaction, adherence, and quality of life. But there are still several aspects of care coordination that require further empirical inquiry to more precisely measure the benefits and areas for development, particularly when coordinated care is applied to various socioeconomic and ethnic groups. The healthcare “home” model, identified as one key NQF domain, is an area for improvement that could be further explored as a viable care coordination option. The healthcare “home” is a concept that strives to provide accessible, continuous, comprehensive, and coordinated services that are delivered within a patient’s family and community context.14 It is a model that strives to provide enhanced medical services with a more efficient cost and improved patient and family experiences, as well as primary healthcare provider experiences.15 The effectiveness of “medical homes” in improving outcomes is currently one of the most active research topics, so innovations using medical homes would likely disseminate quickly. Gaps in the literature. Given gaps identified in this report, future efforts can build from the concepts defined by NQF to: (1) more specifically define and measure how care coordination should be conceptualized and implemented;16 (2) address issues with measurement of care coordination (e.g., patient perceptions of continuity, team/cross care boundary continuity);17 and (3) measure the effectiveness of care coordination for various populations.18 Future care coordination efforts could focus on identifying health service delivery strategies that are characterized by: (1) efficient use of healthcare services across specialties that have supporting evidence of the healthcare “home” model;14 (2) proactive care and follow-up by all providers involved in a coordinated care plan; (3) appropriate and shared information systems that are accessible by providers and that accurately report patient conditions; and (4) consistent communication among providers resulting in smooth transitions between services and patient handoffs.19 The service and patient-level outcomes from achievement of these domains can include: quality improvement, coordinated treatment plans, decreased burden of disease, improved medication and
Addressing Health Disparities Topic Briefs 20
treatment regimens, enhanced preventive care, and improved overall health outcomes and patient satisfaction. References 1. Preferred Practices and Performance Measures for Measuring and Reporting Care Coordination: A
Consensus Report. Washington, DC: National Quality Forum; 2010. 2. Bodenheimer T. Coordinating care—a perilous journey through the health care system. NEJM.
2008;358(10):1064-1071. 3. Chronic Conditions: Making the case for ongoing care. Baltimore, MD: Partnership for Solutions,
Johns Hopkins University and the Robert Wood Johnson Foundation; 2004. 4. Guiding principles for the care of older adults with multimorbidity: an approach for clinicians. J Am
Geriatr Soc. 2012;60(10):E1. 5. Anderson G. Chronic care: making the case for ongoing care. 2010.
http://www.rwjf.org/en/research-publications/find-rwjf-research/2010/01/chronic-care.html. Accessed April 11, 2013.
6. Smith SM, Soubhi H, Fortin M, Hudon C, O'Dowd T. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database of Systematic Reviews (online). 2012;4:CD006560.
7. Butler S, Klepacka K, Agius M, Zaman R. Depression treatment by Bedford East Community Mental Health Team: an audit to assess how many patients in a Bedfordshire Community Mental Health Team might safely be transferred to primary care. Psychiatria Danubina. Jun 2010;22(2):317-322.
8. Chou AF, Vaughn TE, McCoy KD, Doebbeling BN. Implementation of evidence-based practices: applying a goal commitment framework. Health Care Management Review. Jan-Mar 2011;36(1):4-17.
9. Chan WS, Whitford DL, Conroy R, Gibney D, Hollywood B. A multidisciplinary primary care team consultation in a socio-economically deprived community: an exploratory randomised controlled trial. BMC Health Services Research. 2011;11:15.
10. Crowley R, Wolfe I, Lock K, McKee M. Improving the transition between paediatric and adult healthcare: a systematic review. Archives of Disease in Childhood. Jun 2011;96(6):548-553.
11. Egginton JS, Ridgeway JL, Shah ND, et al. Care management for type 2 diabetes in the United States: a systematic review and meta-analysis. BMC Health Services Research. 2012;12:72.
12. Verhoeven F, Tanja-Dijkstra K, Nijland N, Eysenbach G, van Gemert-Pijnen L. Asynchronous and synchronous teleconsultation for diabetes care: a systematic literature review. Journal of Diabetes Science and Technology. May 2010;4(3):666-684.
13. Williams AM, Dennis S, Harris MF. How effective are the linkages between self-management programmes and primary care providers, especially for disadvantaged patients? Chronic Illness. Mar 2011;7(1):20-30.
14. Peikes D, Zutshi A, Genevro JL, Parchman ML, Meyers DS. Early evaluations of the medical home: building on a promising start. The American Journal of Managed Care. Feb 2012;18(2):105-116.
15. Leventhal T, Taliaferro JP, Wong K, Hughes C, Mun S. The patient-centered medical home and health information technology. Telemedicine Journal and E-Health. Mar 2012;18(2):145-149.
16. Aubin M, Giguere A, Martin M, et al. Interventions to improve continuity of care in the follow-up of patients with cancer. Cochrane Database of Systematic Reviews (online). 2012;7:CD007672.

Addressing Health Disparities Topic Briefs 21
17. Uijen AA, Schellevis FG, van den Bosch WJ, Mokkink HG, van Weel C, Schers HJ. Nijmegen Continuity Questionnaire: development and testing of a questionnaire that measures continuity of care. Journal of Clinical Epidemiology. Dec 2011;64(12):1391-1399.
18. Dudley L, Garner P. Strategies for integrating primary health services in low- and middle-income countries at the point of delivery. Cochrane Database of Systematic Reviews (online). 2011(7):CD003318.
19. Patterson ES, Wears RL. Patient handoffs: standardized and reliable measurement tools remain elusive. Joint Commission Journal on Quality and Patient Safety / Joint Commission Resources. Feb 2010;36(2):52-61.
Addressing Health Disparities Topic Briefs 22
Compare the effectiveness of multilevel interventions (e.g., community-based, health education, usual care) on reducing disparities in birth outcomes.
Introduction In 2004 (the latest year data for all countries is available), the United States ranked 29th in the world in infant mortality, tied with Poland and Slovakia.1 Although infant mortality is decreasing slowly in the United States, it is much higher than it should be in comparison with the rest of the developed world. Increasing use of prenatal care2 and decades of research have had little effect on other measures of birth outcomes. Rates of preterm birth and low birth weight have increased since the 1980s and have only started to plateau in the last five years.3 More importantly, although the proportion of black women receiving prenatal care has also increased, there has not been a coincident decrease in infant mortality and low birth weight.2(p200S) Persistent disparities exist, with preterm birth rates remaining highest for black women.4 Burden on Society The infant mortality rate for black people is twice that of white people. Three common measures of birth outcomes are the infant mortality rate (less than 1 year of age), rate of preterm birth (less than 37 weeks gestation), and the rate of low birth weight (less than 2,500 grams, or 5 pounds 8 ounces). The infant mortality rate has improved since the mid-20th century; it statistically remained the same or improved every year since 1958, with the exception of 2002.5 In 2009, black people had the highest infant mortality rate (12.4%), followed by Native American (8.5%), white (5.3%), Hispanic (5.3%), and Asian American (4.4%). The US infant mortality rate is greatly impacted by preterm births; two-thirds of all infant deaths in 2009 were infants who were born preterm. The trend has not abated; preliminary data for 2011 show that the infant mortality rate in the United States is 6.1 per 1,000 live births. The rate for white infants is 5.1, and the rate for black infants is 11.4, more than twice as high. This higher rate for the black population (relative to white) amounts to almost 4,000 more black infant deaths than white infant deaths per year.6 Preterm birth rates today are higher than in the 1980s and 1990s. From 1981 to 2006, the preterm birth rate rose by approximately 35% and, in the past five years, has fallen 8% from its peak in 2006. A decrease in preterm birth rates from 2010 to 2011 is seen across the major racial and ethnic groups (white, black, Hispanic, Native American, Asian American). Since 2006, decreases in the preterm birth rate have been greatest for white infants and black infants (8%–9% decrease) and lower for Hispanic infants (5%). The preterm birth rate of black infants (16.5%) is the highest among racial and ethnic groups, although it is the lowest reported in the last 30 years.3(p4). In economic terms, preterm birth in 2005 in the United States was estimated to have cost an average of $51,600 per infant, a $26.2 billion burden.4(p2)
Topic 4: Interventions for Improving Birth Outcomes

Addressing Health Disparities Topic Briefs 23
The rate of low birth weight is steadily declining. Similarly, the low birth weight rate increased from 6.8% in 19857 to 8.3% in 20068 and has slowly declined to 8.1% in 2011. Low birth weight rates for white infants (7.1%) and black infants (13.3%) have declined since 2006, but there has not been a consistent trend for Hispanic births.3(p4) Unplanned pregnancy rates are higher among black women and Hispanic women than white women and are associated with worse birth outcomes, such as low birth weight.9 The consistently high rates of infant mortality, preterm birth, and low birth weight in the United States compared to other developed countries and the excess mortality resulting from persistent disparities between black people and other population groups make reducing disparities in birth outcomes a high priority. This requires action to not only address the individual risk factors, but also to address the social and environmental factors that impede individual behavioral change. Simultaneously addressing factors at the individual, community, and policy levels is referred to as multilevel action. Options for Addressing the Issue To date, there are few studies on multilevel interventions to reduce adverse birth outcomes; thus, an evidence base does not yet exist. An extensive search of databases including Cochrane Review, Agency for Healthcare Research and Quality (AHRQ), NICE Guidelines, and NIH Consensus Statements, as well as PubMed, did not yield any multilevel interventions for reducing disparities in birth outcomes. Although a lot is known about individual interventions, few studies have looked at interventions at multiple levels. For example, AHRQ did rank two interventions for improved birth outcomes—group visits10 and nurse home visits11—with a strong evidence rating, but these were singular, not multilevel, interventions. At least two of three factors—individual, community, and policy—must be addressed for an intervention to be considered multilevel, and the interventions must be synergistic. A 2011 systematic review of 36 prenatal interventions in socially disadvantaged women at high risk for infant mortality and preterm birth found insufficient evidence to recommend any of the interventions. Of seven comprehensive prenatal care US programs with a possible beneficial effect on preterm birth or infant mortality, none was multilevel.12 A review of studies in the United Kingdom to identify interventions for improving birth outcomes in disadvantaged women found limited evidence of effective interventions and few studies that were designed or powered sufficiently to detect effectiveness. No multilevel studies were identified, although community-level interventions were described in some studies.13 The National Children’s Study, a multisite, multiyear birth cohort study that will follow 100,000 American children from early pregnancy (and possibly preconception) through age 21, has the potential to inform multilevel research. Started in 2009, the study will look at factors affected by individual-, community-, and policy-level actions, such as environmental exposures, diet, family dynamics, and local and cultural influences. Data on the growth, development, and health of the children in this study may lead to the development of multilevel interventions that focus on disparities in birth outcomes among racial, ethnic, and low-socioeconomic groups across the country.14

Addressing Health Disparities Topic Briefs 24
Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Because social, as well as biological, sources affect health disparities, the World Health Organization (WHO) recommends a multilevel approach. In the 1980s, the field began a transition from a focus on the prenatal (during pregnancy) to a focus on the preconceptional (before pregnancy) period for improving birth outcomes.15 This shift was prompted by discoveries that (1) there are many risk factors that must be addressed prior to pregnancy in order to improve birth outcomes (e.g., obesity, chronic disease, nutrition, tobacco and alcohol misuse); (2) women are having children later in life; and (3) preconceptional health-related issues affect health during pregnancy.16 Additionally, because one-third to one-half of pregnancies have historically been unplanned, a primary prevention approach that maximizes the health of the woman regardless of her intentions to become pregnant may be more effective.9 Recent literature promotes the concept of a multilevel approach to improving birth outcomes that starts with infancy and is designed for the racial and cultural characteristics of the population at greatest risk. The WHO Commission on Social Determinants of Health recommends a multilevel approach to promote health equity that involves: (1) improving daily living conditions; (2) tackling the inequitable distribution of power, money, and resources; and (3) measuring and understanding the problem and assessing the results of the action. This approach requires involvement of government, civil society, local communities, and business. The Commission expands the concept of preconception care to investing in the early years of life, when complete child development will increase later life chances and reduce health risks.17 Simply stated, “Infant outcomes are the foundation for adult health.”18 Proponents of this life course approach argue that historical and social inequalities have shaped current generations of black people and white people differently, and that a one-size-fits-all approach to prenatal care actually contributes to health inequity.18 Tailoring preconception interventions to women of childbearing age who are most at risk will decrease adverse birth outcomes faster than the prenatal care for the masses style we have employed for the past 30 years.19 Developing additional evidence of the comparative effectiveness of interventions to improve birth outcomes among this target population (women of childbearing age) would be beneficial. Evidence-based practices must be interdisciplinary, multilevel, and multiphased to be effective.18 In order to develop effective multilevel interventions to address disparities in birth outcomes, there is also a need for longitudinal studies, such as the National Children’s Study, to measure adverse birth outcomes with an emphasis on enrolling disadvantaged young women before pregnancy. References 1. MacDorman MF, Mathews TJ. Recent Trends in Infant Mortality in the United States. NCHS data
brief, no 9. Hyattsville, MD: National Center for Health Statistics. http://www.cdc.gov/nchs/data/databriefs/db09.pdf. Published October 2008. Accessed March 28, 2013.
2. Lu MC, Kotelchuck M, Hogan VK, Johnson K, Reyes C. Innovative strategies to reduce disparities in the quality of prenatal care in underresourced settings. Med Care Res Rev. Oct 2010;67(5 suppl):198S-230S.

Addressing Health Disparities Topic Briefs 25
3. Hamilton BE, Martin JA, Ventura SJ. Births: preliminary data for 2011. Natl Vital Stat Rep. 2012;61(5):1-20.
4. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: Institute of Medicine. http://www.iom.edu/~/media/Files/Report%20Files/2006/Preterm-Birth-Causes-Consequences-and-Prevention/Preterm%20Birth%202006%20Report%20Brief.pdf2006. Published July 2006. Accessed March 28, 2013.
5. Hoyert DL, Xu J. Deaths: preliminary data for 2011. Natl Vital Stat Rep. 2012;61(6):1-52. 6. Mathews TJ, MacDorman, MF. Infant mortality statistics from the 2009 period linked birth/infant
death data set. Natl Vital Stat Rep. 2013;61(8):1-69. 7. Infant mortality and low birth weight among black and white infants—United States, 1980-2000.
MMWR Morb Mortal Wkly Rep. Jul 12, 2002;51(27):589-592. 8. Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2006. Natl Vital Stat Rep. Jan 7,
2009;57(7):1-102. 9. Mosher WD, Jones J, Abma JC. Intended and unintended births in the United States: 1982-2010. Natl
Health Stat Report. Jul 24, 2012;(55):1-28. 10. Group Visits Focused on Prenatal Care and Parenting Improve Birth Outcomes and Provider
Efficiency. Rockville, MD: Agency for Healthcare Research and Quality; http://innovations.ahrq.gov/content.aspx?id=1909. Published April 11, 2012. Accessed March 22, 2013.
11. Nurse Home Visits Improve Birth Outcomes, Other Health and Social Indicators for Low-Income, First-Time Mothers and Their Children. Rockville, MD: Agency for Healthcare Research and Quality. http://innovations.ahrq.gov/content.aspx?id=2229. Published November 7, 2012.Accessed March 22, 2013.
12. Hollowell J, Oakley L, Kurinczuk JJ, Brocklehurst P, Gray R. The effectiveness of antenatal care programmes to reduce infant mortality and preterm birth in socially disadvantaged and vulnerable women in high-income countries: a systematic review. BMC Pregnancy Childbirth. 2011;11:13.
13. D'Souza L, Garcia J. Improving services for disadvantaged childbearing women. Child Care Health Dev. Nov 2004;30(6):599-611.
14. National Children's Study. Bethesda, MD: National Institutes of Health. http://www.nationalchildrensstudy.gov. Published March 8, 2013. Accessed March 22, 2013.
15. Moos MK. Preconceptional health promotion: progress in changing a prevention paradigm. J Perinat Neonatal Nurs. Jan-Mar 2004;18(1):2-13.
16. Hillemeier MM, Downs DS, Feinberg ME, et al. Improving women's preconceptional health: findings from a randomized trial of the Strong Healthy Women intervention in the Central Pennsylvania women's health study. Womens Health Issues. Nov-Dec 2008;18(6 suppl):S87-96.
17. Marmot M, Friel S, Bell R, Houweling TA, Taylor S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. Nov 8 2008;372(9650):1661-1669.
18. Hogan VK, Rowley D, Bennett T, Taylor KD. Life course, social determinants, and health inequities: toward a national plan for achieving health equity for African American infants—a concept paper. Matern Child Health J. Aug 2012;16(6):1143-1150.
19. Savitz DA, Murnane P. Behavioral influences on preterm birth: a review. Epidemiology. May 2010;21(3):291-299.
Addressing Health Disparities Topic Briefs 26
Compare the effectiveness of health center interventions to enhance the "Million Hearts" program and reduce major vascular events among the economically disadvantaged, including racial and ethnic minorities and rural populations.
Introduction
In 2011, the US Department of Health and Human Services launched the Million Hearts Initiative to prevent one million heart attacks and strokes by 2017. The goal is to reduce the number of people who need treatment and also to improve care for those who get treatment. To achieve this goal, the initiative aligns programs, policies, and campaigns targeting patients, providers, and communities. Community strategies may include interventions focused on tobacco use prevention or reducing sodium in foods. Clinical strategies focus specifically on promoting the “ABCS” of clinical prevention (appropriate Aspirin therapy, Blood pressure control, Cholesterol management, and Smoking cessation). The ABCS strategies have been proven to reduce death and disease burden from heart disease. Innovative approaches to clinical care include using teams to coordinate and improve the quality of patient care and using health information technology to measure and improve ABCS.1-3 For this brief, “health centers” include healthcare institutions, such as hospitals, clinics, health maintenance organizations, and community health centers, where organizational-level interventions can be developed to implement the initiative. Burden on Society
Heart disease is currently the leading cause of death in the United States.4 Heart disease is part of a group of diseases called cardiovascular disease (CVD) that involves plaque buildup in the blood vessels supplying the heart. Strokes are related to cerebrovascular disease, which affects blood vessels in the brain. In 2006, the overall annual CVD death rate (per 100,000) was 262.5. Death rates were highest for African American males (422.8) compared to white males (306.6), African American females (298.2), and white females (215.5).5 The number of CVD cases and death rates for residents of rural areas are higher compared to those in urban areas of the United States, particularly for African American women.6 Racial disparities in rural areas are amplified by factors such as limited access to quality healthcare services, socioeconomic burden, dwindling resources, underdeveloped health infrastructure, and lack of transportation.6 Over the past several decades, the risk of death from heart attack in the United States has fallen by 50%, but this condition remains a major issue, especially for low-income individuals and racial and ethnic
Topic 5: Heart Attacks Among Racial and Ethnic Minorities

Addressing Health Disparities Topic Briefs 27
minorities.7 In spite of these successes, less than half of the patients who could benefit from these clinical interventions receive adequate treatment.8 Extending these treatments to those not receiving them could prevent as many as 100,000 deaths a year. Strokes are a major source of adult disability, and both heart disease and stroke can negatively affect quality of life.9 The financial costs to society are extremely high, with total costs estimated at $312.6 billion in 2009, which includes healthcare expenses and lost productivity.10 Overall societal burden will likely increase as the number of affected people is expected to rise as the United States population ages. By 2030, over 40% of US adults, or 116 million people, are projected to have some form of CVD.11 Options for Addressing the Issue We do not know of any studies that address all components of the Million Hearts Initiative and long-term outcomes such as heart attacks, strokes, or CVD-related deaths. The Million Hearts Initiative is new, and its collective approach has not been evaluated. Therefore, this brief focuses on systematic reviews and randomized controlled trials (RCTs) examining components of the Million Hearts Initiative (e.g., organizational-level CVD prevention strategies to reduce risk for high blood pressure; smoking; increasing prescribed cholesterol or blood pressure treatments). We use the term “mixed evidence” when some studies have positive outcomes and some show no effect, and we use “limited evidence” when there are relatively few studies.
Mixed evidence for blood pressure reduction strategies. There is mixed evidence that organizational-level interventions improve high blood pressure control. A Cochrane review of nine RCTs found that appointment reminders by mail, phone, or computer increased follow-up appointment attendance but had inconsistent effects on controlling blood pressure.12 A large trial, the Hypertension Detection and Follow-Up Program, found that a systematic program to increase high blood pressure medication use at clinics significantly reduced blood pressure and five-year mortality from all causes by 17% compared to a group receiving usual care.13-15 The Community Preventive Services Task Force found strong evidence from 77 studies to support multidisciplinary team–based care to improve the quality of patient care for high blood pressure.16 A team-based approach involves patients, primary care providers, and other healthcare professionals, such as nurses, pharmacists, dietitians, social workers, or community health workers that cooperatively manage medications, follow up with patients, and provide education and self-management support. A subset of the reviewed articles focused on low-income populations and showed mixed results in blood pressure outcomes in three studies for low-income groups and improved blood pressure outcomes in 11 studies of low-income, public insurance (Medicaid/Medicare), or no insurance groups. Mixed evidence for interventions to quit smoking. There is mixed evidence on whether interventions in health centers to help people quit smoking are effective for low-income and minority groups. Intervention outcomes and measures were not comparable across all studies. For example, some studies investigated self-reporting of smoking status, while others examined frequency of provider-based counseling or referrals.17-21 Among women receiving maternal and child health services at health centers, there is mixed evidence that they could maintain their ability to avoid smoking following pregnancy.22,23 Of three studies, one found no difference in smoking quit rates, but there was a significant increase in smoking cessation medication use after one year; one found decreased smoking

Addressing Health Disparities Topic Briefs 28
at two and six months post intervention, and one found decreased smoking in African American and white study participants, but not in Hispanic participants.24-26 Mixed evidence for interventions to increase medication use. Aspirin, statins, and other medications can reduce heart attacks and strokes in those at high risk,27,28 but there is mixed evidence on the effectiveness of health center interventions to increase medication use. An observational study by Kaiser Permanente found that its CVD prevention program increased first prescriptions for at least one of three recommended CVD medications (aspirin, statins, or ACE inhibitors) among 1,125 community clinic patients in Southern California and 1,120 patients in Northern California.29 A longitudinal study found increased adherence to guidelines published by the American Heart Association for aspirin and beta blocker use among hospitalized coronary artery disease patients.30 A retrospective review of 499 medical records found that Denver Health’s team-based program increased use of a four-drug regimen (aspirin, statins, beta blockers, and ACE inhibitors) among hospitalized patients from 18% in 1998–1999 to 72% in 2002.31 Another trial found that automated telephone reminders to purchase prescriptions significantly increased statin use (42.3% vs. 26% for controls).32 Tailored interventions, such as interactive voice recognition calls and mailed guides, increased statin use, while computerized decision aids and mailed reminders increased aspirin use.33,34 Adding a flag to a registry database for high-risk patients intensified blood pressure and cholesterol medication use at three months, but these differences disappeared after six months.35 Limited and mixed evidence for community health center settings. There is limited and somewhat mixed evidence showing that federally funded community health centers (CHC) are effective environments for CVD prevention interventions. A trial with African American patients diagnosed with heart disease, type 2 diabetes, high cholesterol, or high blood pressure compared a risk reduction program led by a nurse practitioner or community health worker with a usual care group.36 After a year, the intervention group significantly improved total cholesterol levels, low-density lipoprotein (LDL) cholesterol, and systolic and diastolic blood pressure. A second trial with African American patients from primary care practices showed no significant blood pressure changes, but the intervention group showed higher rates of medication compliance.37 A third study was an evaluation of a federal collaborative program in 44 CHCs intended to reduce health disparities, which showed little effect on changing racial/ethnic disparities in quality of care measures for high blood pressure.38 There was limited information on interventions in CHCs in rural settings. A trial of a telehealth educational program compared to usual care in three rural health centers primarily targeting African Americans with diabetes (sample size of 165 individuals), found that the 85 participants in the program had lower LDL cholesterol levels after 12 months.39 Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly
Bundled interventions can improve cardiovascular outcomes at multiple levels. Although these interventions are not novel, the focus on these specific items as a “bundle” of interventions is new. These bundled interventions require systems for identifying provider teams and eligible patients, including health information systems such as disease registries, resources for provider training, and new policies and procedures in health centers.16 They may also require changes to established provider communication patterns and feedback mechanisms within health centers. Assessing the organizational
Addressing Health Disparities Topic Briefs 29
context of the practice or clinic will be important to determine factors that facilitate or discourage successful adoption of the interventions, including cost implications. To better understand the impact of health center interventions on racial/ethnic, economic, and rural CVD disparities, more comparative effectiveness studies that include multiple health systems with bundled interventions targeted specifically to address these disparities and use short- and long-term clinical outcomes are needed.38 Dissemination and implementation studies could help assess where to allocate resources to have the greatest effect on reducing CVD disparities. Many clinics will likely be implementing components of the Million Hearts Initiative, and assessing the comprehensiveness of the interventions is an important evaluation design issue. Due to the limited number of large-scale CVD prevention studies involving multiple health center systems with attention to enrolling low-income, minority, and rural participants, information gained from this type of design would remain relevant for several years. References
1. Sacco RL, Frieden TR, Blakeman DE, Jauch EC, Mohl S. What the Million Hearts Initiative means for stroke: a presidential advisory from the American Heart Association/American Stroke Association. Stroke.Mar 2012;43(3):924-928.
2. Tomaselli GF, Harty MB, Horton K, Schoeberl M. The American Heart Association and the Million Hearts Initiative: a presidential advisory from the American Heart Association. Circulation. Oct 18 2011;124(16):1795-1799.
3. Benjamin RM. The Million Hearts Initiative: progress in preventing heart attacks and strokes. Public Health Reports. Nov-Dec 2012;127(6):558-560.
4. Heart Disease Fact Sheet. Atlanta, GA: Centers for Disease Control and Prevention. 2013. http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_disease.htm. Accessed March 5, 2013.
5. Compressed mortality file: underlying cause of death, 1979 to 2005. Atlanta, GA: Centers for Disease Control and Prevention. 2013. http://wonder.cdc.gov/mortSQL.html. Accessed March 13, 2013.
6. Taylor HA, Hughes GD, Garrison RJ. Cardiovascular disease among women residing in rural America: epidemiology, explanations, and challenges. Am J Public Health. Apr 2002;92(4):548-551.
7. Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. Jun 7 2007;356(23):2388-2398.
8. Frieden TR, Berwick DM. The "Million Hearts" initiative—preventing heart attacks and strokes. N Engl J Med. Sep 29 2011;365(13):e27.
9. Horner RD. The high cost of stroke to society, the family, and the patient. Pharmacotherapy. May-Jun 1998;18(3 pt 2):87S-93S; discussion 85S-86S.
10. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. Jan 1 2013;127(1):e6-e245.
11. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. Mar 1 2011;123(8):933-944.
Addressing Health Disparities Topic Briefs 30
12. Glynn LG, Murphy AW, Smith SM, Schroeder K, Fahey T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Db Syst Rev. 2010(3).
13. National Heart Lung and Blood Institute. Hypertension Detection and Follow-up Program Cooperative Group. Five-Year Findings of the Hypertension Detection and Follow-up Program. Bethesda, MD: Dept. of Health, Education, and Welfare, National Institutes of Health; 1979.
14. Therapeutic control of blood pressure in the Hypertension Detection and Follow-up Program. Hypertension Detection and Follow-up Program Cooperative Group. Preventive Medicine. Jan 1979;8(1):2-13.
15. Glynn LG, Murphy AW, Smith SM, Schroeder K, Fahey T. Self-monitoring and other non-pharmacological interventions to improve the management of hypertension in primary care: a systematic review. Br J Gen Pract. Dec 2010;60(581):e476-488.
16. Guide to Community Preventive Services: Cardiovascular Disease Prevention and Control. Atlanta, GA: Community Preventive Services Task Force; 2012. www.thecommunityguide.org/cvd/index.html. Accessed March 15, 2013.
17. DePue JD, Goldstein MG, Schilling A, et al. Dissemination of the AHCPR clinical practice guideline in community health centres. Tob Control. Dec 2002;11(4):329-335.
18. Fisher E, Musick J, Scott C, et al. Improving clinic- and neighborhood-based smoking cessation services within federally qualified health centers serving low-income, minority neighborhoods. Nicotine Tob Res. Apr 2005;7:S45-S56.
19. Shelley D, Cantrell J. The effect of linking community health centers to a state-level smoker's quitline on rates of cessation assistance. BMC Health Serv Res. Jan 25 2010;10.
20. Maizlish NA, Ruland J, Rosinski ME, Hendry K. A systems-based intervention to promote smoking as a vital sign in patients served by community health centers. Am J Med Qual. May-Jun 2006;21(3):169-177.
21. Caplan L, Stout C, Blumenthal DS. Training physicians to do office-based smoking cessation increases adherence to PHS guidelines. J Community Health. Apr 2011;36(2):238-243.
22. Pbert L, Ockene JK, Zapka J, et al. A community health center smoking-cessation intervention for pregnant and postpartum women. Am J Prev Med. Jun 2004;26(5):377-385.
23. Manfredi C, Crittenden KS, Cho YI, Gao S. Long-term effects (up to 18 months) of a smoking cessation program among women smokers in public health clinics. Prev Med. Jan 2004;38(1):10-19.
24. Joseph AM, Arikian NJ, An LC, et al. Results of a randomized controlled trial of intervention to implement smoking guidelines in Veterans Affairs medical centers: increased use of medications without cessation benefit. Med Care. Nov 2004;42(11):1100-1110.
25. Katz DA, Muehlenbruch DR, Brown RL, Fiore MC, Baker TB, Guid ASC. Effectiveness of implementing the Agency for Healthcare Research and Quality smoking cessation clinical practice guideline: a randomized, controlled trial. J Natl Cancer Inst. Apr 21, 2004;96(8):594-603.
26. Gordon JS, Andrews JA, Albert DA, Crews KM, Payne TJ, Severson HH. Tobacco cessation via public dental clinics: results of a randomized trial. Am J Public Health. Jul 2010;100(7):1307-1312.
27. Antithrombotic Trialists Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. Jan 12, 2002;324(7329):71-86.

Addressing Health Disparities Topic Briefs 31
28. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. Oct 8, 2005;366(9493):1267-1278.
29. Wong W, Jaffe M, Wong M, Dudl RJ. Community implementation and translation of Kaiser Permanente's cardiovascular disease risk-reduction strategy. The Permanente Journal. Winter 2011;15(1):36-41.
30. Xian Y, Pan WQ, Peterson ED, et al. Are quality improvements associated with the Get With the Guidelines–Coronary Artery Disease (GWTG-CAD) program sustained over time?: a longitudinal comparison of GWTG-CAD hospitals versus non–GWTG-CAD hospitals. Am Heart J. Feb 2010;159(2).
31. Krantz MJ, Baker WA, Estacio RO, et al. Comprehensive coronary artery disease care in a safety-net hospital: results of Get With The Guidelines quality improvement initiative. J Manage Care Pharm. May 2007;13(4):319-325.
32. Derose SF, Green K, Marrett E, et al. Automated outreach to increase primary adherence to cholesterol-lowering medications. JAMA Internal Medicine. Jan 14, 2013;173(1):38-43.
33. Stacy JN, Schwartz SM, Ershoff D, Shreve MS. Incorporating tailored interactive patient solutions using interactive voice response technology to improve statin adherence: results of a randomized clinical trial in a managed care setting. Population Health Management. Oct 2009;12(5):241-254.
34. Sheridan SL, Draeger LB, Pignone MP, et al. A randomized trial of an intervention to improve use and adherence to effective coronary heart disease prevention strategies. BMC Health Serv Res. Dec 5, 2011;11.
35. Selby JV, Schmittdiel JA, Fireman B, et al. Improving treatment intensification to reduce cardiovascular disease risk: a cluster randomized trial. BMC Health Serv Res. 2012;12:183.
36. Allen JK, Dennison-Himmelfarb CR, Szanton SL, et al. Community Outreach and Cardiovascular Health (COACH) Trial: a randomized, controlled trial of nurse practitioner/community health worker cardiovascular disease risk reduction in urban community health centers. Circulation. Nov 1, 2011;4(6):595-602.
37. Ogedegbe GO, Boutin-Foster C, Wells MT, et al. A randomized controlled trial of positive-affect intervention and medication adherence in hypertensive African Americans. Arch Intern Med. Feb 27, 2012;172(4):322-326.
38. Hicks LS, O'Malley AJ, Lieu TA, et al. Impact of health disparities collaboratives on racial/ethnic and insurance disparities in US community health centers. Arch Intern Med. Feb 8, 2010;170(3):279-286.
39. Davis RM, Hitch AD, Salaam MM, Herman WH, Zimmer-Galler IE, Mayer-Davis EJ. TeleHealth improves diabetes self-management in an underserved community: diabetes TeleCare. Diabetes Care. Aug 2010;33(8):1712-1717.

Addressing Health Disparities Topic Briefs 32
Compare the effectiveness of telemedicine and/or expanding practice to non-physician practitioners (i.e., nurse practitioners, physician assistants) on improving cardiovascular disease outcomes in rural populations.
Introduction The cardiovascular disease (CVD) mortality risk is higher in rural4 populations than in urban populations, even after adjusting for age. A probable reason for this disparity is reduced access to timely care. In contextual analysis, Starfield and colleagues1 found that counties with a lower primary care supply had higher mortality from CVD. Additionally, because cardiologists tend to cluster disproportionally in larger counties,2 rural residents are less likely to use a cardiologist to manage their cardiovascular disease. Two potential strategies attempt to address this disparity and the challenge of having fewer physicians in rural areas: (1) expanding practice to non-physician professionals (e.g., nurse practitioners, physician assistants, and pharmacists; hereafter “expansion of the team”) and/or (2) using telemedicine approaches to connect rural residents and providers with care teams in larger healthcare systems. Using telemedicine allows the practitioner to provide more routine monitoring of patients from a remote location. Not only would this facilitate more routine care, but it would alleviate some of the burden patients may face having to travel long distances for every appointment. Both telemedicine and expansion of the team show promise as methods to reduce the CVD disparity in rural areas. Burden on Society Cardiovascular disease is highly prevalent and more common in rural areas. CVD is a broad set of conditions including heart failure, hypertension, and stroke. It is the most common cause of death among Americans, the cause of nearly one-third of all deaths in 2010. The age-adjusted death rate from CVD (per 100,000) was higher in nonmetropolitan counties (249.4) compared to metropolitan counties (230.2). Similar disparities were seen in rural counties. In fact, the death rate in rural counties was 16% higher than in large “fringe” metropolitan (e.g., suburban) counties.3,4 Certain CVD risk factors, such as obesity and smoking, are more prevalent among rural residents than urban.3(p1) Stroke incidence is nearly 50% higher in rural areas than in urban areas.5 One study found hypertension and diabetes (a risk factor for CVD) were more poorly controlled among rural African Americans than urban.6
Options for Addressing the Issue The use of telemedicine to manage cardiovascular conditions appears to be effective for both acute and non-acute conditions. The use of telemedicine (which includes teleconsulting, telemonitoring, and other methods using technology to transmit medical information) to support the management of acute cardiovascular events, especially stroke, appears to be effective. Because telemedicine in this context is specifically designed to improve access to specialist care, which is lacking in the community,
4 In this brief, “metro” refers to metropolitan counties. Micropolitan areas have an urbanized population of 10,000 to 49,999.
“Rural” and “noncore” refer to the remaining counties (http://www.whitehouse.gov/omb/inforeg_statpolicy#ms).
Topic 6: Telemedicine for Rural Cardiovascular Care

Addressing Health Disparities Topic Briefs 33
telemedicine may have greater potential in rural populations. Moulin et al.7 reviewed evidence demonstrating that limited timely access to technology can lead to suboptimal care for strokes in rural areas (e.g., limited use of Tissue Plasminogen Activator [tPA]).5 A systematic review of telestroke management by Johansson and Wild8 found that, in most studies, hospitals with telestroke care had an increased use of tPA. Another way to improve stroke care is by providing specialist consultations to rural providers. One review found that some rural hospitals not providing tPA actually have the capacity to do so, but do not because local physicians are reluctant to provide tPA without local neurologic expertise; this expertise could be provided via telemedicine.9 The effective use of telemedicine in stroke care may also suggest strategies for non-acute CVD conditions. Telemedicine for non-acute events has also generally been found to be effective for numerous conditions, including cardiovascular conditions and risk factor management. For example, a Cochrane review concluded that structured telephone support and telemonitoring6 programs for those with heart failure were effective in reducing mortality and hospitalizations.10 A review of home-based telehealth concluded that telehealth showed improved health outcomes.11 In another review, Kraai et al.12 concluded that patients are generally satisfied with telemedicine. Literature on redesigning the care team is more limited, but generally positive. Redesigning the healthcare team by extending to non-physician providers also appears to be an effective way to deliver CVD care in both rural and urban areas. A systematic review by Walsh13 concluded that the most effective intervention for improving hypertension management was a change in the provider team (assignment of some physician responsibility to a non-physician professional). Majumdar14 found that diabetes care teams providing outreach to people with diabetes improved control of hypertension but not control of diabetes.7 Bray et al.15 reported improved diabetes care by the addition of an advanced practice nurse and some prompts in the electronic health record (including a registry and visit reminder). Bove et al.16 found nurse management reduced the CVD risk among underserved asymptomatic rural and urban patients with moderate to high risk. Nkansah17 found that nontraditional use of pharmacists in outpatient settings led to improved outcomes, although few of the studies focused on rural populations specifically, and many were non-CVD. The use of pharmacists in rural settings represents a gap in the literature; the use of pharmacist counseling, pharmacists-assisted training, and so forth are relatively under-researched strategies. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Both of these strategies are active topics in the research community, especially given the high prevalence of CVD and the rural-urban disparity. Advances in telemedicine technology and system-wide efforts to redesign the organization of the healthcare team suggest further advances in this field for the foreseeable future and widespread interest in these topics. The combined (tele) strategy of (1) providing access to specialist; (2) overcoming barriers such as transportation, healthcare access, and utilization;
5 A substance used to dissolves clots that cause strokes.
6 Telemonitoring involves remotely monitoring patients who are not at the same location as the healthcare provider. A patient
may have devices at home, and the results of these devices will be transmitted via telephone to the healthcare provider. 7 A lab value that shows how well the patient is controlling his or her blood sugar over the course of a few months.
Addressing Health Disparities Topic Briefs 34
and (3) improving patient-based care via training of multiple types of providers should be explored further to demonstrate its effectiveness. Notably, recent research has used both telemedicine and expanded teams to deliver multifaceted interventions, and these multifaceted interventions could improve CVD outcomes for rural populations. Would new information from research on this topic remain current for several years, or would it be rendered obsolete quickly by subsequent studies? The technology of health communication is rapidly changing, as is our ability to integrate these communication types with electronic health records (a prior limitation). Similarly, payment systems to incentivize these types of care are changing. Given capital and time costs of installing and learning to use these technologies, research will be quite useful. Studies should be designed to be short in duration so as to disseminate results to the users while relevant, in case future advances in technology or changes in the healthcare system make the research obsolete. References 1. Starfield B, Shi L, Grover A, Macinko J. The effects of specialist supply on populations' health:
assessing the evidence. Health Aff (Millwood). 2005. 2. Aneja S, Ross JS, Wang Y, et al. US cardiologist workforce from 1995 to 2007: modest growth, lasting
geographic maldistribution especially in rural areas. Health Aff (Millwood). 2011;30(12):2301-2309. doi: 10.1377/hlthaff.2011.0255; 10.1377/hlthaff.2011.0255.
3. Rural Health Research & Policy Analysis Center. Rural health snapshot. http://www.shepscenter.unc.edu/rural/snapshot.html2010. Updated August 2010. Accessed March 23, 2013.
4. Centers for Disease Control and Prevention. CDC Wonder.Detailed mortality analysis. http://wonder.cdc.gov/2013.
5. Yiannakoulias N, Svenson LW, Hill MD, et al. Incident cerebrovascular disease in rural and urban Alberta. Cerebrovasc Dis. 2004;17(1):72-78. doi: 10.1159/000073903.
6. Mainous AG 3rd, King DE, Garr DR, Pearson WS. Race, rural residence, and control of diabetes and hypertension. Ann Fam Med. 2004;2(6):563-568. doi: 10.1370/afm.119.
7. Moulin T, Joubert J, Joubert, JB, de Bustos, EM. Telemedicine in stroke: potentials, limitations and ongoing issues. In: Graschew G, ed. Advances in Telemedicine: Applications in Various Medical Disciplines and Geographical Regions. Vol 2. Rijeka, Croatia: InTech; 2011:1.
8. Johansson T, Wild C. Telemedicine in acute stroke management: systematic review. Int J Technol Assess Health Care. 2010;26(2):149-155. doi: 10.1017/S0266462310000139.
9. Leira EC, Hess DC, Torner JC, Adams HP Jr. Rural-urban differences in acute stroke management practices: a modifiable disparity. Arch Neurol. 2008;65(7):887-891. doi: 10.1001/archneur.65.7.887.
10. Inglis SC, Clark RA, McAlister FA, et al. Structured telephone support or telemonitoring programmes for patients with chronic heart failure. Cochrane Database Syst Rev. 2010;(8)(8):CD007228. doi: 10.1002/14651858.CD007228.pub2.
11. Dellifraine JL, Dansky KH. Home-based telehealth: a review and meta-analysis. J Telemed Telecare. 2008;14(2):62-66. doi: 10.1258/jtt.2007.070709; 10.1258/jtt.2007.070709.
12. Kraai IH, Luttik ML, de Jong RM, Jaarsma T, Hillege HL. Heart failure patients monitored with telemedicine: patient satisfaction, a review of the literature. J Card Fail. 2011;17(8):684-690. doi: 10.1016/j.cardfail.2011.03.009; 10.1016/j.cardfail.2011.03.009.
Addressing Health Disparities Topic Briefs 35
13. Walsh JM, McDonald KM, Shojania KG, et al. Quality improvement strategies for hypertension management: a systematic review. Med Care. 2006;44(7):646-657. doi: 10.1097/01.mlr.0000220260.30768.32.
14. Majumdar SR, Guirguis LM, Toth EL, Lewanczuk RZ, Lee TK, Johnson JA. Controlled trial of a multifaceted intervention for improving quality of care for rural patients with type 2 diabetes. Diabetes Care. 2003;26(11):3061-3066.
15. Bray P, Roupe M, Young S, Harrell J, Cummings DM, Whetstone LM. Feasibility and effectiveness of system redesign for diabetes care management in rural areas: the eastern North Carolina experience. Diabetes Educ. 2005;31(5):712-718. doi: 10.1177/ 0145721705280830.
16. Bove AA, Santamore WP, Homko C, et al. Reducing cardiovascular disease risk in medically underserved urban and rural communities. Am Heart J. 2011;161(2):351-359. doi: 10.1016/j.ahj.2010.11.008.
17. Nkansah N, Mostovetsky O, Yu C, et al. Effect of outpatient pharmacists' non-dispensing roles on patient outcomes and prescribing patterns. Cochrane Database Syst Rev. 2010;(7):CD000336. doi(7):CD000336; doi: 10.1002/14651858.CD000336.pub2.

Addressing Health Disparities Topic Briefs 36
Compare the effectiveness of telemedicine and/or expanding practice to non-physician practitioners (i.e., nurse practitioners, physician assistants) on improving mental health disease outcomes in rural populations.
Introduction This brief focuses on two potential strategies to improve management and treatment of mental health outcomes in rural populations. Both address potential barriers to access for mental health care in rural communities: telepsychiatry allows remote management and treatment by practitioners in other communities, and expansion of mental health services to non-physicians clinicians can leverage existing practitioner supply. Burden on Society Approximately 25% of the US adult population is reported to have a mental illness, and 50% of US adults will develop one mental illness over the course of a lifetime.1 Further, recent estimates about 20% of the US population (62 million people) live in rural areas.2 Among those individuals in rural areas, 16% to 20% are reported to struggle with mental illness, substance abuse, and medical-psychiatric comorbid conditions.2 Incidence rates of mental health disorders for urban and rural individuals are not significantly different, but due to differing environmental factors, experiences of mentally ill rural individuals and their families are distinctly different from their urban counterparts.3 Specifically, research has found that rural communities have higher suicide rates as a result of mental illness than their urban counterparts.3 Mental health service provision is different in rural areas due to three primary factors: availability, accessibility, and acceptability.3 Only 9% to 11% of practicing psychiatrists in the United States are reported to work in rural areas of the country.4 Given the high incidence of national mental illness, coupled with the limited availability, accessibility, and acceptability of mental health services in rural areas, along with a worldwide shortage of psychiatrists to respond to this significant international need for service, telemedicine is an apparent option to consider. Staller5 published a report in 2006 addressing the significant need for mental healthcare services for youth in rural areas. This report noted that despite the Surgeon General’s 2001 action plan agenda that identified a critical need for mental health care for American youths, there remained a perpetual shortage of child psychiatrists, particularly in rural areas of the country. Staller described the various successes of an innovative program in New York State, which is unique because it provides specialty certification to nurse practitioners who complete advanced training and experience. In addition to meeting a critical workforce need, the program example provided by Staller’s report illustrates how successfully and easily barriers to communication, cost, and care coordination among multiple providers can be overcome.
Options for Addressing the Issue
Topic 7: Telemedicine for Rural mental Health Care

Addressing Health Disparities Topic Briefs 37
Telemedicine is an effective option for providing primary care providers (PCPs) with the clinical support needed to provide needed mental health services to rural or isolated patients. The following studies indicate that telepsychiatry8 can be implemented in an effective manner with little negative impact on treatment adherence or patient perceptions of physician competence. Freuh and colleagues7 conducted a secondary analysis of data collected from a randomized controlled trial in which telepsychiatry and “same room” psychiatry were compared. The findings of their analysis found no significant difference between the two modes of psychiatric care; that is, telepsychiatry did not compromise the perceptions of physician competence, nor did it negatively impact treatment adherence. In another study, Hilty and colleagues8 pilot tested the effectiveness of providing an electronic consultation service to PCPs via telephone and e-mail. The most common consultation included advice in the areas of psychiatry, gastroenterology, and medical genetics. The authors found that PCPs had favorable experiences with the electronic consultation services and that service delivery to rural populations and clinical outcomes were enhanced by this electronic service. Indeed, the practitioner community seems to embracing mental health as the service most conducive to telemedicine services; a MedPAC analysis found that nearly two-thirds (62%) of Medicare telehealth claims in 2009 were for mental health services. MedPAC concluded that an AHRQ review showed telemedicine “was most effective for specialties that rely on verbal discourse and not necessarily physical contact, including mental health and neurology”.9,10 Telemedicine can be a source for facilitating a collaborative model of care with non-physician mental health providers. When considering telemedicine, it is important to identify the various service providers and specialties that will provide the services on both sides of the service spectrum (e.g., frontline workers, peer advisors, other non-physician providers). In some instances, integrating non-physician providers may be a viable and strong option, but this remains an understudied area in research. Tschirch and colleagues11 evaluated an innovative project that developed and provided a telemedicine network for victims of domestic violence. The intervention relied on nurses who were involved in the design, implementation, and evaluation of the project. The authors concluded that the network responded to a significant need for women who previously did not have access to appropriate mental health services despite their significant need. The authors also concluded that nurses offered valuable clinical and organizational value in the promising delivery of their mental health network and mental health services overall. Effectiveness of non-physician clinicians to manage mental health is relatively unknown. Innovative models have been developed that use non-physician practitioners to treat and manage mental health. For example, psychiatric nurse practitioners12 and paramedics9 expand the set of potential providers who can refer or manage mental disorders. Grossman et al.13 explore the potential role of psychiatric nurses in school-based clinics. There are limited studies evaluating the effectiveness of these kinds of models, however. One trial comparing practice-based and telemedicine-based collaborative care models in rural Federally Qualified Health Centers (FQHCs) found that telemedicine-based models were more effective, suggesting that the combination of telemedicine and collaborative care models may be most effective.14 Some models implemented in other countries may also suggest innovative models; one Australian trial found practice nurses were effective in reducing depression symptoms.15
8 For a broader overview of telemedicine, its potential for improving outcomes among rural populations, and barriers to wider
implementation and use, see reference 6.

Addressing Health Disparities Topic Briefs 38
Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly. Future directions. One area in which telemedicine has been scarcely examined has been the context of the “train-the-trainer” model that refers to training paraprofessionals to provide them with skills for mental health service provision. At a time when the healthcare system is feeling overburdened with a shortage of providers to address the increasing needs of individuals, there is growing evidence of the promising impact of models that follow a lay health advisor/peer-support framework, such as the train-the-trainer model. Telemedicine has been shown to enhance other specialties through a collaborative physician-to-physician model and also by training other clinicians with much needed mental health expertise in an effective and efficient manner with little negative impact. Knowing this, using telemedicine as a mechanism for training peers and other paraprofessionals (in a train-the-trainer model) to address mental health needs, particularly for underserved populations, is an important area to further examine.16 With further research to identify, implement, and measure specific telemedicine strategies, there is great promise for telemedicine to enhance existing clinical services and also additional service options, via other professionals and paraprofessionals, to respond to the increasing demand to address mental health needs. Though the empirical body of literature focused on telemedicine and non-physician providers is limited, the published works support the integration of non-physician providers to address significant mental health needs in rural areas. Turning to non-physician providers provides a solution to a long-standing shortage of psychiatrists in rural areas, using inexpensive and available modes of telemedicine delivery (i.e., telephones) to provide an effective service delivery solution based on a collaborative model that can also improve physician and patient satisfaction,17 in addition to increasing the availability of providers to respond to the great need for mental health care. References 1. CDC. U.S. Adult Mental Illness Surveillance Report.
http://www.cdc.gov/Features/MentalHealthSurveillance/. Published September 5, 2011. Accessed April 11, 2013.
2. National Center for Health Statistics. Population by region and urbanization level: United States, 1998—Data Tables on Urban and Rural Health, in Health, United States, 2001 With Urban and Rural Health Chartbook DHHS Publication No (PHS) 01-1232. Washington, DC: U.S. Government Printing Office; 2001.
3. Wagenfeld, MO. Mental Health and Rural America: 1980–1993. Rockville, MD: Office of Rural Health Policy, Health Resources and Services Administration: Office of Rural Mental Health Research, National Institute of Mental Health, National Institutes of Health: U.S. Dept. of Health and Human Services, Public Health Service; 1994. NIH Publication No. 94-3500.
4. Workforce Series: Rural Behavioral Health. Washington DC: Government Affairs Office; 2008. 5. Staller JA. Psychiatric nurse practitioners in rural pediatric telepsychiatry. Psychiatr Serv. Jan
2006;57(1):138. 6. UnitedHealth Group. New models of technology—the promise of rural telemedicine. In:
Modernizing Rural Health Care: Coverage, Quality, and Innovation. Minnetonka, MN: UnitedHealth Center for Health Reform & Modernization; 2011.

Addressing Health Disparities Topic Briefs 39
7. Frueh BC, Monnier J, Grubaugh AL, Elhai JD, Yim E, Knapp R. Therapist adherence and competence with manualized cognitive-behavioral therapy for PTSD delivered via videoconferencing technology.Behav Modif. 2007;31(6):856-866.
8. Hilty DM, Ingraham RL, Yang SP, Anders TF. Multispecialty telephone and e-mail consultation for patients with developmental disabilities in rural California. Telemedicine Journal and E-Health. Winter 2004;10(4):413-421.
9. Service Delivery Innovation Profile: Trained paramedics provide ongoing support to frequent 911 callers, reducing use of ambulance and emergency department services. Rockville, MD: AHRQ Health Care Innovations Exchange. http://www.innovations.ahrq.gov/content.aspx?id=3343. Published January 18, 2012. Updated February 13, 2013. Accessed April 11, 2013.
10. Hersh WR, Hickam DH, Severance SM, Dana TL, Krages KP, Helfand M. Telemedicine for the medicare population: update. Evid Rep Technol Assess (Full Rep). Feb 2006(131):1-41.
11. Tschirch P, Walker G, Calvacca LT. Nursing in tele-mental health. J Psychosoc Nurs Ment Health Serv. May 2006;44(5):20-27.
12. Delaney KR. The psychiatric nurse practitioner 1993–2003: a decade that unsettled a specialty. Arch Psychiatr Nurs. 2005;19(3):107-115.
13. Grossman J, Laken M, Stevens J, Hughes-Joyner F, Sholar M, Gormley CK. Use of psychiatric nurse practitioner students to provide services in rural school-based health clinics. J Child Adolesc Psychiatr Nurs. Nov 2007;20(4):234-242.
14. Fortney JC, Pyne JM, Mouden SB, et al. Practice-based versus telemedicine-based collaborative care for depression in rural federally qualified health centers: a pragmatic randomized comparative effectiveness trial. Am J Psychiatry. Apr 1 2013;170(4):414-425.
15. Morgan MA, Coates MJ, Dunbar JA, Reddy P, Schlicht K, Fuller J. The TrueBlue model of collaborative care using practice nurses as case managers for depression alongside diabetes or heart disease: a randomised trial. BMJ Open. 2013;3(1).
16. Byrne MK, Willis A, Deane FP, Hawkins B, Quinn R. Training inpatient mental health staff how to enhance patient engagement with medications: Medication Alliance training and dissemination outcomes in a large US mental health hospital. J Eval Clin Pract. Feb 2010;16(1):114-120.
17. Agius M, Murphy CL, Zaman R. Does shared care help in the treatment of depression? Psychiatria Danubina. Nov 2010;22 suppl 1:S18-22.

Addressing Health Disparities Topic Briefs 40
Introduction Individuals with diabetes experience an increased risk of amputation. Co-morbid conditions like peripheral neuropathy (i.e., reduced sensation) and/or peripheral vascular disease (i.e., arterial disease that reduces blood flow) in addition to practicing inadequate foot care increases the likelihood that people with diabetes may overlook minor foot injuries. Over time, such injuries may become infected, thereby necessitating medical interventions such as revascularization or amputation. Revascularization procedures are intended to restore blood flow to an injured limb, while amputation, most frequently of the toe or foot, is used either as a first treatment or when revascularization measures are deemed ineffective.1-3 Interventions focusing solely on disparity reduction among individuals diagnosed with peripheral arterial disease (PAD), resulting from atherosclerotic disease, are beyond the scope of this topic brief. A disproportionate number of racial/ethnic minorities in the US have diabetes.4 Numerous studies have reported that among patients with diabetes, there are disparities between racial groups and between genders with respect to rates of lower extremity amputations (LEAs). Diabetes-related LEAs are performed disproportionately more often among blacks and Hispanics. With respect to gender differences, men, especially non-Hispanic black and Hispanic men, are more likely to receive LEAs than women. Among women, black women are more likely to receive LEAs than white women.5-12 Information about the effectiveness of interventions aimed at reducing these disparities may help racial/ethnic minorities gain greater access to better preventive health management for diabetes,13 multidisciplinary foot care specialists, and foot care self-management education to prevent amputations. Burden on society Diabetes is prevalent, underdiagnosed, and disproportionately affects racial and ethnic minorities. According to the 2011 National Diabetes Fact Sheet, 8.3% (25.8 million people) of the US population has diabetes, although it is highly underdiagnosed: only 27% (7.0 million people) of those with diabetes have received a clinical diagnosis (See Table 1). In 2010, 26.9% of people aged 65 and older had diabetes. Diabetes is also prevalent in younger age groups. Among those 20 years and older, 10.8% of females and 11.8% of males have diabetes. With respect to race-ethnicity, 7.1% of non-Hispanic whites, 12.6% of non-Hispanic blacks, 8.4% of Asian Americans, and 11.8% of Hispanics aged 20 years or older had diagnosed diabetes.14
Topic 8: Reduce foot amputations in minorities
Compare the effectiveness of interventions on reducing disparities in revascularization efforts to prevent foot amputation in racial and ethnic minorities.

Addressing Health Disparities Topic Briefs 41
Lower extremity amputations are much more common among those with diabetes, and racial/ethnic disparities in amputation rates exist. Complications from diabetes are numerous,9 with amputation being one of the most common, costly, and severe.14,15 The Centers for Disease Control and Prevention (CDC) report that over 60% of LEAs are performed on people with diabetes.14 From 1996 to 2009, the age-adjusted hospital discharge rate for nontraumatic LEA declined from 9.0 to 3.2 per 1,000 diabetic population.16 With respect to sex, from 1998 to 2009, compared to females, males had a consistently greater age-adjusted hospital discharge rate for nontraumatic LEA. By 2009, the rate for males was almost twice the rate for females (4.1 vs. 2.2 per 1,000 diabetic population).17 Despite declining nontraumatic LEA rates among blacks beginning in 1988 and whites beginning in 1999, the rate among blacks remained nearly twice that of whites in 2009 (4.5 vs. 2.3 per 1,000 diabetic population, respectively).18 Compared to people without diabetes, people with diabetes are 7 years younger at age of first amputation, more likely to be men, and have more comorbidities.19 Diabetes is a common cause of death, and those with LEAs are more likely to die prematurely. Mortality: In 2007, the CDC reported that diabetes was the seventh leading cause of death in the US, and the risk of death was almost twice as great for people with diabetes compared to people without.14 Moreover, mortality rates are higher among blacks and Hispanics with diabetes compared to whites.20 Table 1. Demographic Characteristics of the 2010 US Diabetic Population14
Demographic Characteristics Individuals with Diabetes (%)
Clinical Diagnosis:
Diagnosed 27%
Not Diagnosed 73%
Age1:
65 and older 26.9%
Sex1:
Female 10.8%
Male 11.8%
Race-Ethnicity1:
Asian American 8.4%
Black, non-Hispanic 12.6%
Hispanic 11.8%
White, non-Hispanic 7.1% 1 Among individuals with a clinical diagnosis. Among people who have undergone amputation, 29% of individuals with diabetes die within 30 days of the operation and 67% die within 1 year.21,22
9 Heart disease and stroke, hypertension, blindness and eye problems, kidney disease, nervous system disease, dental disease, complications of pregnancy,
diabetic ketoacidosis, hyperosmolar coma, greater susceptibility to other illnesses, depression, reduced ability to walk distances, climb stairs, or do
housework.

Addressing Health Disparities Topic Briefs 42
Burden: Efforts to explain racial/ethnic disparities in the use of amputation vary. Some research finds that, relative to whites, blacks tend to be diagnosed with diabetes or seek treatment for diabetic complications too late for limb-saving measures. In such cases, blacks may initially seek treatment with worse circulation, greater nerve damage, and more severe damage, making them less viable candidates for revascularization efforts.6,12,13 Systemic reasons such as racial/ethnic minorities lacking access to and receiving lower quality medical and preventive, multidisciplinary foot care than whites, 1,15,23,24 may explain why they have more advanced disease when they initially seek care. Research also indicates that provider bias or stereotyping negatively impacts the quality of physician-patient communication for racial/ethnic minority patients.25 Other reasons for racial/ethnic differences in amputation may include socioeconomic status, level of education, low health literacy, or cultural beliefs.15,24,26-29 Options for addressing the issue Patient education and increasing access to multidisciplinary foot care facilities were the most commonly utilized interventions in a recent literature search on efforts to reduce disparities in revascularization efforts among racial/ethnic minorities. Evidence from existing literature: We identified four studies in the last decade focused on interventions to reduce diabetes-related amputation rates and health disparities by educating racial/ethnic minorities about foot care self-management practices or increasing access to foot care services in low-income communities.3,30-32 These studies were not designed specifically to increase use of revascularization procedures. One case study30 used a multi-faceted community-level approach to amputation reduction and foot care examination by implementing individual targeting provider, policy, and health-systems interventions. The study showed statistically significant amputation reductions among blacks, whites, and the overall study population. However, despite reductions, LEA remained high for blacks. A single cohort study31 to determine the change in prevalence of diabetes-related foot problems and the rate of LEAs after implementing a 1 year multidisciplinary diabetes LEA prevention program among low income blacks found a statistically significant reduction in LEAs, foot operations, and other outcomes. Another study3 described the impact of a church-based educational intervention on proper foot care techniques and risk factors to prevent amputation. A small sample composed of 25 black participants completed pre- and post-education surveys, and their changes in scores were reported. While study results are inconclusive, given the small sample size and lack of formal statistical analyses, researchers were optimistic about the educational intervention’s utility. Improving access to quality medical care and increasing access to and knowledge about preventive management for diabetes and its complications appear to be promising research aims for reducing the disparity in revascularization efforts to prevent foot amputation among racial/ethnic minorities. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly The relatively few interventions included in this topic brief indicate that efforts to improve patient-centered foot-care education and increase access to multidisciplinary foot care practices are currently being underutilized by physicians, researchers, and community educators. These interventions have the potential to improve diabetic self-management practices and to reduce the prevalence of amputations in this population. Furthermore, these interventions appear to have had some success with improving the quality of care received by and reducing the need for amputation in people with diabetes. Available evidence on the efficacy of future interventions targeting this population is likely to be adapted and applied quickly if disseminated broadly to providers, community outreach coordinators,

Addressing Health Disparities Topic Briefs 43
and educators. Additional research is needed to examine the benefits and harms of these interventions and to examine the comparative effectiveness of these interventions to improve diabetes-related outcomes and reduce disparities. References 1. Apelqvist J, Bakker K, van Houtum WH, Nabuurs-Franssen MH, Schaper NC. International consensus
and practical guidelines on the management and the prevention of the diabetic foot. International Working Group on the Diabetic Foot. Diabetes Metab Res Rev. Sep-Oct 2000;16 Suppl 1:S84-92.
2. Caputo GM, Cavanagh PR, Ulbrecht JS, Gibbons GW, Karchmer AW. Assessment and management of foot disease in patients with diabetes. N Engl J Med. Sep 29 1994;331(13):854-860.
3. Scollan-Koliopoulos M. Theory-guided intervention for preventing diabetes-related amputations in African Americans. J Vasc Nurs. Dec 2004;22(4):126-133.
4. Mier N, Ory M, Zhan D, Villarreal E, Alen M, Bolin J. Ethnic and health correlates of diabetes-related amputations at the Texas-Mexico border. Rev Panam Salud Publica. Sep 2010;28(3):214-220.
5. Feinglass J, Rucker-Whitaker C, Lindquist L, McCarthy WJ, Pearce WH. Racial differences in primary and repeat lower extremity amputation: results from a multihospital study. J Vasc Surg. May 2005;41(5):823-829.
6. Rucker-Whitaker C, Feinglass J, Pearce WH. Explaining racial variation in lower extremity amputation: a 5-year retrospective claims data and medical record review at an urban teaching hospital. Arch Surg. Dec 2003;138(12):1347-1351.
7. Feinglass J, Abadin S, Thompson J, Pearce WH. A census-based analysis of racial disparities in lower extremity amputation rates in Northern Illinois, 1987-2004. J Vasc Surg. May 2008;47(5):1001-1007; discussion 1007.
8. Guadagnoli E, Ayanian JZ, Gibbons G, McNeil BJ, LoGerfo FW. The influence of race on the use of surgical procedures for treatment of peripheral vascular disease of the lower extremities. Arch Surg. Apr 1995;130(4):381-386.
9. Lavery LA, Ashry HR, van Houtum W, Pugh JA, Harkless LB, Basu S. Variation in the incidence and proportion of diabetes-related amputations in minorities. Diabetes Care. Jan 1996;19(1):48-52.
10. Schulman KA, Berlin JA, Harless W, et al. The effect of race and sex on physicians' recommendations for cardiac catheterization. New Engl J Med. Feb 25 1999;340(8):618-626.
11. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in the quality of care for diabetes. Womens Health Issues. Mar-Apr 2006;16(2):56-65.
12. Resnick HE, Valsania P, Phillips CL. Diabetes mellitus and nontraumatic lower extremity amputation in black and white Americans: the National Health and Nutrition Examination Survey Epidemiologic Follow-up Study, 1971-1992. Arch Intern Med. Nov 8 1999;159(20):2470-2475.
13. Regenbogen SE, Gawande AA, Lipsitz SR, Greenberg CC, Jha AK. Do differences in hospital and surgeon quality explain racial disparities in lower-extremity vascular amputations? Ann Surg. Sep 2009;250(3):424-431.
14. National Center for Chronic Disease Prevention and Health Promotion, Translation DoD. 2011 National Diabetes Fact Sheet. 2011; http://www.cdc.gov/diabetes/pubs/estimates11.htm#12. Accessed March 14, 2013.
15. Diamant AL, Babey SH, Hastert TA, Brown ER. Diabetes: the growing epidemic. Policy Brief UCLA Cent Health Policy Res. Aug 2007(PB2007-9):1-12.
Addressing Health Disparities Topic Briefs 44
16. Prevention CfDCa. Crude and Age-Adjusted Hospital Discharge Rates for Nontraumatic Lower Extremity Amputation per 1,000 Diabetic Population, United States, 1988–2009: National Center for Chronic Disease Prevention and Health Promotion Division of Diabetes Translation; 2012.
17. Prevention CfDCa. Age-Adjusted Hospital Discharge Rates for Nontraumatic Lower Extremity Amputation per 1,000 Diabetic Population, by Sex, United States, 1988–2009. 2012.
18. Prevention CfDCa. Age-Adjusted Hospital Discharge Rates for Nontraumatic Lower Extremity Amputation per 1,000 Diabetic Population, by Race, United States, 1988–2009.2012.
19. Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. Mar 2005;86(3):480-486.
20. Mokdad AH, Ford ES, Bowman BA, et al. Diabetes trends in the U.S.: 1990-1998. Diabetes Care. Sep 2000;23(9):1278-1283.
21. Faglia E, Clerici G, Caminiti M, et al. Mortality after major amputation in diabetic patients with critical limb ischemia who did and did not undergo previous peripheral revascularization Data of a cohort study of 564 consecutive diabetic patients. J Diabetes Complications. Jul-Aug 2010;24(4):265-269.
22. Kristensen MT, Holm G, Kirketerp-Moller K, Krasheninnikoff M, Gebuhr P. Very low survival rates after non-traumatic lower limb amputation in a consecutive series: what to do? Interact Cardiovasc Thorac Surg. May 2012;14(5):543-547.
23. Hasnain-Wynia R, Baker DW, Nerenz D, et al. Disparities in health care are driven by where minority patients seek care: examination of the hospital quality alliance measures. Arch Intern Med. Jun 25 2007;167(12):1233-1239.
24. Thackeray R, Merrill RM, Neiger BL. Disparities in diabetes management practice between racial and ethnic groups in the United States. Diabetes Educ. Jul-Aug 2004;30(4):665-675.
25. van Ryn M. Research on the provider contribution to race/ethnicity disparities in medical care. Med Care. Jan 2002;40(1 Suppl):I140-151.
26. Wachtel MS. Family poverty accounts for differences in lower-extremity amputation rates of minorities 50 years old or more with diabetes. J Natl Med Assoc. Mar 2005;97(3):334-338.
27. Oladele CR, Barnett E. Racial/Ethnic and social class differences in preventive care practices among persons with diabetes. BMC Public Health. 2006;6:259.
28. van Ryn M, Burke J. The effect of patient race and socio-economic status on physicians' perceptions of patients. Soc Sci Med. Mar 2000;50(6):813-828.
29. Feinglass J, Shively VP, Martin GJ, et al. How 'preventable' are lower extremity amputations? A qualitative study of patient perceptions of precipitating factors. Disabil Rehabil. 2012;34(25):2158-2165.
30. Jenkins C, Myers P, Heidari K, Kelechi TJ, Buckner-Brown J. Efforts to decrease diabetes-related amputations in African Americans by the Racial and Ethnic Approaches to Community Health Charleston and Georgetown Diabetes Coalition. Fam Community Health. Jan-Mar 2011;34 Suppl 1:S63-78.
31. Patout CA, Jr., Birke JA, Horswell R, Williams D, Cerise FP. Effectiveness of a comprehensive diabetes lower-extremity amputation prevention program in a predominantly low-income African-American population. Diabetes Care. Sep 2000;23(9):1339-1342.
32. El Sakka K, Fassiadis N, Gambhir RP, et al. An integrated care pathway to save the critically ischaemic diabetic foot. Int J Clin Pract. Jun 2006;60(6):667-669.

Addressing Health Disparities Topic Briefs 45
Introduction Mammography is recommended as the best screening method for breast cancer in women ages 50 to 74.1 Randomized controlled trials that have shown the benefit of screening mammography have all used film mammography rather than digital mammography. For various reasons, film mammography is gradually being replaced with higher resolution digital mammography. Although studies show that digital mammography is more sensitive than film mammography at detecting breast lesions in younger women with very dense breast tissue,2 there is no evidence that this increased detection leads to a reduction in mortality from breast cancer.3 In fact, there is concern that digital mammography may detect fewer breast cancers among older women, who have a higher risk of breast cancer because of their age. There are pros and cons of using digital mammography or magnetic resonance imaging (MRI) to screen women at high risk for breast cancer. Women at high risk include those with BRCA1 (breast cancer 1, early onset) or BRCA2 (breast cancer 2, early onset) mutations, or first-degree relatives of women with BRCA mutations.4 Some studies have found that for younger women at high risk of breast cancer (greater than a 20% lifetime risk of developing breast cancer), a combination of digital mammography and MRI can detect more breast cancers than either test alone.5 However, because MRI is so sensitive, it also detects far more lesions that are not cancer (false positives) than film mammography or digital mammography. A false positive would call for additional testing, but would not result in a cancer diagnosis.4 Using more intensive methods of screening (such as every year versus every two years, or using MRI screening or digital rather than film mammography) results in more false positives and over-diagnosis of breast cancer. Over-diagnosis can result in being treated unnecessarily with the treatment causing harms of its own.6 Understanding the benefits and harms of film or digital mammography and MRI screening is important for women at high risk to make informed decisions regarding personal screening.3 Burden on Society Breast cancer is the most common cancer in women and the second leading cause of cancer death among women in the United States. In 2009, 211,731 women were diagnosed with breast cancer, and
Topic 9: Breast Cancer Screening for High-Risk Women
Compare the effectiveness of film-screen or digital mammography alone and mammography plus magnetic resonance imaging (MRI) in community practice-based screening for breast cancer in high-risk women of different ages, risk factors, and race or ethnicity.

Addressing Health Disparities Topic Briefs 46
40,676 died from the disease.7 Hereditary cancers, such as those from BRCA mutations, make up only 10% to 15% of all breast cancers, but women with hereditary cancers are at higher risk of cancer death.8 Little data on disparities in women with hereditary breast cancers. Breast cancer incidence is higher for white women than for other ethnic groups and is thought to be due to higher screening rates and greater use of hormone replacement therapy. However, breast cancer mortality is highest for black women compared to any other racial/ethnic group. Other racial and ethnic groups have lower breast cancer incidence and mortality than white women and black women. For all stages of breast cancer, the five-year relative survival rate is lower for black women than other ethnic groups. These disparities may be due to differences in access to quality health care, existing comorbidities,9 and/or racial differences in tumor biology.10 In a group of Medicare beneficiaries studied from 1992 to 2002, there was little improvement in overall use of care or reducing racial disparities of cancer therapies among black patients.11 Improved screening in recent years has led to a small reduction in breast cancer mortality overall, but advances in treatment have been at least as important in reducing mortality.12 In 2010, the prevalence of screening mammograms for white women and black women was almost equal (51.5% and 50.6%), but somewhat greater than for Hispanic women and Asian American women (46.5% and 47.7%). Options for Addressing the Issue Guidelines and recommendations for women at high risk of breast cancer (greater than 20% lifetime risk) have been developed based on observational studies, case series, and expert opinion.4 A 2008 systematic review of 11 prospective, nonrandomized studies included women with BRCA1 or BRCA2 mutations or a family history consistent with hereditary breast cancer who were screened with both annual MRI and mammography. The results strongly support the addition of MRI to mammography screening for detecting cancer among women at high risk.5 However, questions about screening interval and ages of enhanced screening require additional research. MRI screening detects more breast cancers than either digital or film mammography at the expense of increased numbers of false positives. A review of seven prospective observational screening studies, including women at high risk of breast cancer, that used MRI in addition to mammography showed that screening MRI sensitivity is higher than mammography alone and detected almost all cancers in combination with mammography. MRI effectively detected cancers that were small and frequently node-negative. Across all seven studies, the sensitivity of MRI screening was 81% and, in combination with mammography, was increased to 92%. However, the number of false positive tests was also increased with MRI screening.4 No data could be found on survival as an endpoint, making it unclear whether there is a benefit to MRI screening.13 For the smaller number of women with high risk of breast cancer (greater than 20% lifetime risk), some have suggested staggered or concurrent mammography and MRI screening. In a retrospective study of 73 patients with BRCA mutations who were screened alternately with mammography and MRI every six months, 12 of 13 cancers were detected by MRI, but not by mammography six months earlier.14 For these high-risk women, there are disadvantages to using MRI for screening. Compared to mammography, MRI is more expensive, involves an intravenous injection, requires more time, and has
Addressing Health Disparities Topic Briefs 47
more people who cannot tolerate it.4 Screening with MRI has more false positives than mammography alone, leading to follow-up testing, patient anxiety, and the possibility of unnecessary biopsies and procedures.3 New research could determine if cancers detected with MRI would have been detected later with mammography alone. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Determining if women at high risk for breast cancer are being identified early and appropriately screened would inform next steps. Public information and awareness about the characteristics of women who could be at high risk for breast cancer could further identify these women and increase rates of early screening. Cost can be a major factor in a patient’s decision not only about screening but also treatment. Costs of screening and treatment are a major barrier for low-income women at high risk who do not have health insurance. Another concern for high-risk women is a lack of availability of MRI screening and MRI-guided biopsy in many communities. The ability to perform MRI-guided biopsy is essential to MRI screening because many small cancers will only be detected with MRI.15 Longer term randomized trials or large cohort studies would help to determine benefits and harms of different screening methods so that high-risk women can make good decisions about when and how to get screened. References 1. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann
Intern Med. Nov 17 2009;151(10):716-726, W-236. 2. Pisano ED, Hendrick RE, Yaffe MJ, et al. Diagnostic accuracy of digital versus film mammography:
exploratory analysis of selected population subgroups in DMIST. Radiology. Feb 2008;246(2):376-383.
3. Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L. Screening for breast cancer: an update for the U.S. Preventive Services Task Force. Ann Intern Med. Nov 17 2009;151(10):727-737, W237-742.
4. Sickles EA. The use of breast imaging to screen women at high risk for cancer. Radiol Clin North Am. Sep 2010;48(5):859-878.
5. Warner E, Messersmith H, Causer P, Eisen A, Shumak R, Plewes D. Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med. May 6 2008;148(9):671-679.
6. Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Inst. May 5 2010;102(9):605-613. 7. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2009 Incidence and
Mortality Web-based Report. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute. http://apps.nccd.cdc.gov/uscs/.. Accessed March 6, 2013.
8. Griffin JL, Pearlman MD. Breast cancer screening in women at average risk and high risk. Obstet Gynecol. Dec 2010;116(6):1410-1421.
9. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. Jan 2013;63(1):11-30. 10. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina
Breast Cancer Study. JAMA. Jun 7 2006;295(21):2492-2502.

Addressing Health Disparities Topic Briefs 48
11. Gross CP, Smith BD, Wolf E, Andersen M. Racial disparities in cancer therapy: did the gap narrow between 1992 and 2002? Cancer. Feb 15 2008;112(4):900-908.
12. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. Oct 27 2005;353(17):1784-1792.
13. Morrow M, Waters J, Morris E. MRI for breast cancer screening, diagnosis, and treatment. Lancet. Nov 19 2011;378(9805):1804-1811.
14. Le-Petross HT, Whitman GJ, Atchley DP, et al. Effectiveness of alternating mammography and magnetic resonance imaging for screening women with deleterious BRCA mutations at high risk of breast cancer. Cancer. Sep 1 2011;117(17):3900-3907.
15. Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. Mar-Apr 2007;57(2):75-89.

Addressing Health Disparities Topic Briefs 49
Introduction Rural populations and health care providers are less prepared to treat trauma. Roughly 62.5 million people (about 20% of the US population) live in rural areas.1 On average, rural populations have more older adults and children, higher unemployment and underemployment rates, and lower population density with higher percentages of poor, uninsured, and underinsured residents. Disparities in access to trauma care have been found in these vulnerable populations.2 Health services in rural areas can differ from urban areas on many dimensions including, longer travel distances (on average); fewer physicians per capita, including specialists required for comprehensive trauma care; health care facilities with limited scopes of service. While these factors do not uniformly mean that there is lower access to care compared to urban areas, they can make it more challenging to deliver trauma care in rural areas.3-5 Access to advanced trauma care is lower in rural areas. Advanced trauma care is particularly lacking in rural areas. The American College of Surgeons Committee on Trauma (ACS-COT) has designated trauma centers into levels I-IV, with Level I or II trauma centers having the most comprehensive resources required to provide high-level trauma care, and Level I centers able to provide the highest level of care in addition to trauma education research and outreach.6,7 Trauma care at a Level I center has been shown to reduce risk of mortality in the severely injured by 25%.8 The most advanced trauma centers are not distributed evenly across the nation; approximately 45 million Americans do not live within one hour of the highest level of trauma care.1 There is a marked rural-urban disparity in access; at least 31% of rural residents are more than an hour from a Level I-III trauma center compared to only 12% of urban residents.2 Burden on society Risk factors for trauma are higher in rural areas. The characteristics of rural trauma suggest a higher injury severity due to injury mechanism and associated social and behavioral dynamics. For example, rural motor vehicular crashes are associated with increased driver speed and inappropriate use of protective devices such as helmets and seatbelts.9,10 In rural areas, there is also a higher prevalence of alcohol use while driving;11 a higher prevalence of loaded unlocked firearms at home;12 an increase in life-threatening/serious farm related-injuries due to exposure to agricultural machinery;13 and when injuries occur, there is the associated issue of prolonged discovery and extrication (period from discovery to treatment) times.11,14 As compared to trauma patients sustaining the same types of injuries
Topic 10: Rural trauma care
Compare the effectiveness of care delivery (e.g., local hospital care, trauma center care) on improving outcomes in patients living in rural communities who experience trauma.

Addressing Health Disparities Topic Briefs 50
treated in an urban or larger metropolitan hospital, rural hospitals have fewer resources (e.g., trauma surgeons, emergency physicians, sophisticated diagnostic radiology, and blood bank reserves).15 Rural populations are more likely to die and have major disease burden from trauma. Trauma is the most common cause of death in people age 1-44, the third most common cause overall, and is one of the top 5 most costly conditions.16,17 While only 20% of our population reside in rural regions, more than 60% of the trauma deaths in America occur in these remote geographic segments of the country.13
Rural patients are more likely to experience preventable deaths due to trauma for several reasons. Esposito et al found that the time for discovery of the injury and transport from the location of the trauma to the hospital is twice as long, on average, in rural locations as in urban areas. Because the first 60 minutes post-injury (the “golden hour”) substantially predicts health outcomes, delays in receiving treatment can lead to worse outcomes. Initial contact with a physician in the emergency room averaged six times longer in rural locations than in urban settings. As a result, the crude death rate in rural settings was three times that of the urban areas.18 One study found that a significant portion of deaths occurred not on the way to the hospital, but in a rural hospital's emergency room.19 In other words, these victims managed to survive the distance to the hospital, but upon arrival, the hospital was unable to save them. The overall “possibly preventable” (as determined by the authors) death rate was double the urban rates in rural incidents. When stratified by phase of care, rate of possibly preventable death was three times greater for the emergency department phase in rural areas than in urban ones.18
The burden of trauma continues after hospitalization. In 2000, injury accounted for $326 billion dollars in lost productivity alone in the United States.20 In addition, for the 1.7 million traumatic brain injuries that occur each year, a third result in death, and about 125,000 result in permanent damage and disability.21 Those who survive to discharge frequently need additional health care services such as home health, physical; occupational; and speech therapy, skilled nursing, and acute rehabilitation. Clinically appropriate courses of treatment for traumatic brain injury and many other traumatic injuries have demonstrated that these services are particularly important and should be assessed as part of clinical comparative effectiveness of treatment.22 However, research has determined rural patients are less likely to receive such comprehensive outpatient therapy services.23 Options for addressing the issue Rural trauma is a high-impact target for improving trauma outcomes. There are many components to this problem from a prehospital, perihospital, and post-acute care treatment that lend themselves to patient centered outcomes research. These include:
injury prevention education,
pre-hospital resuscitation and triage management,
improved resource allocation at Critical Access Hospitals,
more accessible trauma resuscitation and treatment education,
consultation via telemedicine (for example: bridging workforce gaps by improving relationships with higher-level trauma centers via telemedicine),
development of improved regional trauma systems and studying the improvement of care,
addressing out-of-hospital patient death and disability, and
evaluating rural disparities in
Addressing Health Disparities Topic Briefs 51
access to comprehensive trauma center care, and
access to some rehabilitation sources shown to improve patients’ functional status
In an attempt to decrease the impact of the limited resources available at rural hospitals, many states have organized their regional trauma systems to ease transfers of injured patients from non-trauma center hospitals to higher levels of care. Statewide regional trauma systems have demonstrated improvement in injury-related mortality as compared to states will less developed trauma systems.24 Currently, 9 states and districts lack a statewide trauma system, and of the remaining 42 states, only 24 have state-funded trauma systems.25 Telemedicine may be a helpful resource. Telemedicine is a strategy that has improved many aspects of medical care, including trauma in rural areas. It was initially found to be beneficial in the military as an aid in resuscitation.26 In a study conducted in rural Mississippi, telemedicine resulted in improved evaluation and management of trauma patients and more efficient and timely transfer of severely injured patients with decreased costs.27 Further, this technology may be expanded upon as tele-presence in trauma surgery—a remote trauma or specialist surgeon could be connected to the rural operating room with video of the injury to provide real time guidance in surgical decision making. Approaches like this could help address the relatively lower supply of surgical specialists in rural communities, which is a workforce issue with no immediate or quick solutions. Potential for new information to improve care and patient-centered outcomes rapidly There are many opportunities for study and rapid implementation of these improvements. Efforts to improve the maldistribution of surgeons and other trauma caregivers and limited access to resources could address the rural-urban divide in trauma outcomes. Study and implementation of the transfer arrangements from centers with fewer resources and the effect on survival are critical to determine if our current paradigm is effective in rural areas and ways to improve. The frequently preventable causes of rural trauma deaths suggest there is value in targeting research, policy, and providers to improve education, the delivery of preliminary trauma care, and in-hospital trauma care in rural environments, and ultimately, patient-centered outcomes.
Trauma outcome data are rich and underused. The ACS-COT has been integrally involved in standardizing and creating efficient trauma systems. The Guideline for Field Triage provides pre-hospital care providers with algorithms to recognize injured patients who are most likely to benefit from specialized trauma center resources.8 The Rural Trauma Team Development Course is designed to teach rural receiving facilities the fundamental elements of injury resuscitation, utilization of the available resources, and regional system relationships.28 The ACS-COT also serves as a verification committee to optimize trauma care in the United States and audits trauma center verification level as outlined in the Resources for Optimal Care of the Injured Patient.29 Trauma diagnosis, outcome, and hospital characteristic data are collected across trauma centers within the National Trauma Databank, which can be accessed for comparative effectiveness research.
Addressing Health Disparities Topic Briefs 52
References
1. Health Resources and Services Administration. Defining the Rural Population. http://www.hrsa.gov/ruralhealth/definition_of_rural.html. Accessed 3/12/2103, 2013.
2. Hsia R, Shen YC. Possible geographical barriers to trauma center access for vulnerable patients in the United States: An analysis of urban and rural communities. Arch Surg. 2011;146(1):46-52.
3. Fuguitt G, Brown D, Beale C. Rural and small town America. New York, NY: Rusell Sage Foundation; 1989.
4. Ricketts TC III, ed. Rural health in the United States. New York, NY: Oxford University Press; 1999. 5. Hart J. The rural landscape. Baltimore, MD: Johns Hopkins University Press; 1998. 6. American College of Surgeons Committee on Trauma. Resources for optimal care of the injured
patient. Chicago, IL: American College of Surgeons; 1999. 7. MacKenzie EJ, Hoyt DB, Sacra JC, et al. National inventory of hospital trauma centers. JAMA.
2003;289(12):1515-1522. 8. Sasser SM, Hunt RC, Faul M, et al. Guidelines For field triage of injured patients: recommendations of
the national expert panel on field triage, 2011. MMWR Recomm Rep. 2012;61(RR-1):1-20. 9. Muelleman RL, Mueller K. Fatal motor vehicle crashes: variations of crash characteristics within rural
regions of different population densities. J Trauma. 1996;41(2):315-320. 10. Zwerling C, Merchant JA, Nordstrom DL, et al. Risk factors for injury in rural Iowa: round one of the
Keokuk county rural health study. Am J Prev Med. 2001;20(3):230-233. 11. Gonzalez RP, Cummings G, Mulekar M, Rodning CB. Increased mortality in rural vehicular trauma:
Identifying contributing factors through data linkage. J Trauma. 2006;61(2):404-409. 12. Nordstrom DL, Zwerling C, Stromquist AM, Burmeister LF, Merchant JA. Rural population survey of
behavioral and demographic risk factors for loaded firearms. Inj Prev. 2001;7(2):112-116. 13. McSwain N, Rotondo M, Meade P, Duchesne J. A model for rural trauma care. Br J Surg.
2012;99(3):309-314. 14. Peek-Asa C, Zwerling C, Stallones L. Acute traumatic injuries in rural populations. Am J Public Health.
2004;94(10):1689-1693. 15. How rural is it? Bulletin of the American College of Surgeons. 2008(47-48). 16. Centers for Disease Control and Prevention (CDC). CDC faststats. http://www.cdc.gov/. Accessed
3/12/2013, 2013. 17. Agency for Healthcare Research and Quality. Heart conditions, cancer, trauma-related disorders,
mental disorders, and asthma were the five most costly conditions in 1996 and 2006. http://www.ahrq.gov/legacy/news/nn/nn080509.htm. Accessed 3/13/2013, 2013.
18. Esposito T, Maier R, Rivera F, Griffith J, Lazear S, Hogan S. The impact of variation in trauma care times: urban versus rural. Prehosp Disaster Med. 1995;10(3):161-6.
19. Gomez D, Berube M, Xiong W, et al. Identifying targets for potential interventions to reduce rural trauma deaths: a population-based analysis. J Trauma. 2010;69(3):633-639.
20. Mann NC, Mullins RJ, MacKenzie EJ, Jurkovich GJ, Mock CN. Systematic review of published evidence regarding trauma system effectiveness. J Trauma. 1999;47(3 Suppl):S25-33.
21. Corso P, Finkelstein E, Miller T, Fiebelkorn I, Zaloshnja E. Incidence and lifetime costs of injuries in the United States. Inj Prev. 2006;12(4):212-218.
22. Faul M, Xu L, Wald M, Coronado V. Tramutic brain injury in the United States: Emergency department visits, hospitalizations, and deaths. http://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf. Accessed 3/11/2013, 2013.

Addressing Health Disparities Topic Briefs 53
23. Shames J, Treger I, Ring H, Giaquinto S. Return to work following traumatic brain injury: Trends and challenges. Disabil Rehabil. 2007;29(17):1387-1395.
24. Health Resources and Services Administration. Model trauma system planning and evaluation. 2006. 25. Chan L, Wang H, Terdiman J, et al. Disparities in outpatient and home health service utilization
following stroke: Results of a 9-year cohort study in northern California. Physicial Medicine and Rehabiliation. 2009;1:997-1003.
26. Menu JP, Comtet G, Di Giusto V, Colomb F, de Saint-Julien J. Military telemedicine: A network of networks. Bull Acad Natl Med. 2006;190(2):339-47; discussion 347-8.
27. Duchesne JC, Kyle A, Simmons J, et al. Impact of telemedicine upon rural trauma care. J Trauma. 2008;64(1):92-7; discussion 97-8.
28. American College of Surgeons. Rural trauma team development course. http://www.facs.org/trauma/rttdc/. Accessed 3/11/2013, 2013.
29. American College of Surgeons. FAQ for resources for optimal care of the injured patient: 2006. http://www.facs.org/trauma/optimalcare.pdf. Accessed 3/11/2013, 2013.

Addressing Health Disparities Topic Briefs 54
Introduction Hypertension—systolic and a diastolic blood pressure level of >140/90 mmHg—is a major risk factor for cardiovascular diseases and stroke.1 Historically, many people with hypertension have been unaware of their condition, but ongoing education and prevention efforts have led to an increase in the number of individuals with controlled or treated high blood pressure.2 Despite these successes, 31% of US adults continue to suffer from hypertension, with minorities being more likely to have the condition. Of these, 25% have uncontrolled blood pressure.3,4 Data from the National Health and Nutrition Examination Survey (NHANES) for 1999–2002 showed that the hypertension prevalence rate was highest among African Americans—almost 50% higher than white people. Minorities face a number of barriers to controlling hypertension, and understanding these barriers is a first step to appropriately selecting and targeting effective treatment plans.5 Some of the barriers to controlling hypertension for minorities include perceived judgment and/or mistreatment, stress, inability to adhere to medications, limited healthcare access and utilization, low health literacy, distrust in clinical community, power struggles, and language/cultural barriers.6 African Americans develop hypertension at an early age, reach advanced levels of hypertension, are prone to experience further complications, and are less likely to attain control of their hypertension.3 Burden on Society Hypertension is highly prevalent among the adult population.7-9 The Framingham Heart Study found that the lifetime risk for developing high blood pressure among non-hypertensive adults in the United States is 90%. Hypertension is a risk factor for other cardiovascular conditions, such as heart disease or stroke; therefore, this lifetime risk underscores the population risk of hypertension.10,11 As a result, 116 million people will have one or more forms of heart disease or stroke, and almost 25 million people are expected to die from heart disease or stroke by 2030.12 Prevalence and mortality associated with hypertension is higher among minorities, particularly African Americans. Hypertension is a leading cause of preventable death in the United States and among African Americans. African Americans have the highest risk for hypertension-related deaths (see Table 1).3 Further, among all racial/ethnic groups, African American women have the highest prevalence (45%)13 and lowest control of high blood pressure (59%).9,14,15 According to Dodani et al, “African Americans have 1.3-times greater rate of nonfatal stroke, a 1.8-times greater rate of fatal stroke, a 1.5-times
Topic 11: Hypertension in Minorities
Compare the effectiveness of different delivery models (e.g., home blood pressure monitors, utilization of pharmacists or other allied health providers) for controlling hypertension in racial minorities.

Addressing Health Disparities Topic Briefs 55
greater rate of death due to heart disease and a 4.2-times greater rate of end-stage kidney disease” compared to white people.16-18 Approximately 25% of all Hispanic adults are hypertensive in the United States. Hispanic people are also less likely to be screened and receive treatment for hypertension.19 American Indians are 1.3 times more likely to have high blood pressure compared to white people.20 There are limited hypertension data for other minority groups.21
Minorities with hypertension are less likely to have their blood pressure under control. According to the Framingham Heart Study, less than half of all men (38%) and women (23%) aged 80 years and older suffering from hypertension had their blood pressure under control per established guidelines.22 These trends were similar for men (38%) and women (38%) aged 60 years or younger.23 NHANES data examining the 2001–2010 time period also showed African Americans were more likely to have uncontrolled hypertension than white people and Hispanic people.15 Poor adherence to medication has been identified as a major contributor to uncontrolled hypertension among African American patients. While the treatment rates for African Americans were 12.9% higher than white patients, the control rate among those treated was 18.1% lower than those of white patients.24 It has also been shown that African Americans who have uncontrolled high blood pressure do not take any antihypertensive medications and are usually young men who do not have frequent contact with a physician.25 Due to its high prevalence, hypertension is a costly condition. Healthcare costs due to hypertension alone are speculated to reach $258.3 billion by 2030. Further, it is estimated that over $3.1 billion in prescription drug costs and other consequences of high blood pressure could be avoided through understanding the most cost-effective options.26,27 A study that examined costs for several conditions found that hypertensive patients incurred the highest costs for treatment and drug expenditures.28 Hypertension is also one of the top 10 most costly health conditions for US employers.29 The Milken Institute found that among the most common chronic diseases, low and lost productivity was highest for hypertension, with close to $3 billion in costs.30 As the number of people with hypertension continues to increase, research to better explain trends in hypertension risk and evidence-based practices to improve patient-centered outcomes will be imperative for addressing the hypertension epidemic.31

Addressing Health Disparities Topic Briefs 56
Table 1. Prevalence, Use of Antihypertensive Medication, Uncontrolled, and Mortality Rates by Race
White Black Hispanic
American Indian/Alaska
Native
Asian American
Prevalence rate 28.8%a 42.0%a 25.5%a 27%a 20%b
Use of antihypertensive medication
78.5%d 75.3%c 68.1%c Not available Not available
Uncontrolled* 41.2%a 58.8%a 68.2%a Not available Not available
Mortality rate 15.6 per 1000
21.3 per 1000d
Not available
Not available Not available
* Includes treated and untreated Sources: a: Keenan N, Rosendorf K. Prevalence of hypertension and controlled hypertension—United States,
2005–2008. MMWR. Surveillance summaries: Morbidity and mortality weekly report. Surveillance summaries/CDC. 2011;60:94.
b: Casper M, Denny C, Coolidge J, et al. Atlas of heart disease and stroke among American Indians and Alaska Natives. 2005.
c: Gu Q, Burt V, Dillon C. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: The National Health and Nutrition Examination Survey, 2001–2010. Journal of Vascular Surgery. 2013;57(3):893-893.
d: Ford ES. Trends in mortality from all causes and cardiovascular disease among hypertensive and non-hypertensive adults in the United States clinical perspective. Circulation. 2011;123(16):1737-1744
Options for Addressing the Issue Drug therapy. Pharmacological treatment is needed for most patients to control their blood pressure.22 However, a segment of the population is resistant to hypertensive medications and may require a combination of three or more drugs to achieve blood pressure control.14 The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) found that only one-third of participants’ blood pressures was controlled with one drug as compared to two-thirds of the participants whose blood pressure needed multiple antihypertensive agents to be controlled.32 Three other large randomized controlled trials that have shown uccess in controlling high blood pressure include antihypertensive agents to achieve the control.33-35 Non-pharmacological interventions. National guidelines recommend that management of hypertension should begin with lifestyle modifications and be complemented with drug therapy. Some of those methods include home blood pressure monitoring, health coaching,36 diet modifications,37 patient-provider communication, pharmacist interventions, and telemedicine.38-42 Systematic reviews suggest that the use of home monitors may improve control of hypertension.43 An Agency for Healthcare Research and Quality (AHRQ) study comparing the effectiveness of self-blood pressure monitoring

Addressing Health Disparities Topic Briefs 57
across 48 studies found that standardized self-monitoring should be implemented in order to determine—with additional research—how effective this method is.9,44 Physician communication and rapport-building are important factors that enhance patient trust, particularly among African American patients, and have been shown to improve blood pressure control when implemented into patient care.45,46 A systematic review and meta-analysis conducted by Machado et al, found that systolic blood pressure is sensitive to pharmacists’ interventions, including methods using pharmacist blood pressure evaluations, pharmacist counseling on controlling and treatment, pharmacist blood pressure management, and pharmacist input in primary care and support in patient decision making. Researchers also recommended the need for high-quality studies to determine effectiveness of pharmacist interventions to control blood pressure. Other interventions to improve patient education and increase support from health professionals may lead to compliance with prescriptions and doctor’s instructions, which could improve blood pressure control.38 Other methods that foster behavior change, such as the Dietary Approaches to Stop Hypertension (DASH) plan, have shown that inclusion of heart healthy foods that are low in cholesterol and sodium have been very beneficial in promoting weight loss, reduction of blood pressure in hypertensive individuals, and reduction in low-density lipoproteins (LDLs).47 Approaches that focus on empowering patients to be involved and “in control” of their condition, such as using home blood pressure monitoring and the health coaching method, have been shown to be effective in controlling hypertension, yet the extent of the advantage is unknown.9 Quality improvement strategies as an avenue to control hypertension. Another systematic review assessed the effectiveness of quality improvement as an approach to hypertension management. Quality improvement strategies, such as provider education, provider reminders, patient education, self-management, audit and feedback, team change, or financial incentives, have shown to lower systolic blood pressure by as much as 10mmHg.48 The review suggested that team change, a method that involves developing and utilizing a multidisciplinary team to assist in disease management, was associated with the greatest reduction in hypertension outcomes. Outcome measures selected for the review across all studies were limited, hence our limited understanding of effective quality improvement strategies. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly The understanding of high blood pressure and how to manage it in clinical settings has advanced greatly.22 There is general consensus on the medications that are most effective in lowering blood pressure. However, there is little information on the best alternate option if the pressure remains elevated despite drug treatment.46 Current evidence for interventions that included patient education, home blood pressure monitoring, decision support from pharmacists, and computerized decision-support systems for physicians shows that implementing one or a few of these processes into daily care may yield results that are different across the spectrum of delivery models. Several studies49-52 have evaluated strategies that bundle and implement multiple delivery methods to control hypertension in minority populations.49,53 One concluded that the most probable strategy to control hypertension would include a combination of several techniques. While the bundling of delivery methods has been proven effective, large-scale, stakeholder-driven studies evaluating its effectiveness across multiple communities is nonexistent.

Addressing Health Disparities Topic Briefs 58
References 1. Heron MP, Hoyert DL, Xu J, Scott C, Tejada-Vera B. Deaths: preliminary data for 2006. Natl Vital Stat
Rep. 2008;56(16):1-52. 2. Jones DW, Hall JE. The National High Blood Pressure Education Program thirty years and counting.
Hypertension. 2002;39(5):941-942. 3. Odedosu T, Schoenthaler A, Vieira Dl, Agyemang C, Ogedegbe G. Overcoming barriers to
hypertension control in African Americans. Cleve Clin J Med. 2012;79(1):46-56. 4. Go AS, Mozaffarian D, Roger VL, et al. Executive summary: heart disease and stroke statistics—2013
update: a report from the American Heart Association. Circulation. 2013;127(1):143-152. 5. Gibbs C, Beevers D, Lip G. The management of hypertensive disease in black patients. QJM.
1999;92(4):187-192. 6. Mount DL, Davis C, Kennedy B, et al. Factors influencing enrollment of African Americans in the Look
AHEAD trial. Clin Trials. 2012;9(1):80-89. 7. Danaei G, Rimm EB, Oza S, Kulkarni SC, Murray CJ, Ezzati M. The promise of prevention: the effects
of four preventable risk factors on national life expectancy and life expectancy disparities by race and county in the United States. PLOS Med. 2010;7(3):e1000248.
8. Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics—2010 update. Circulation. 2010;121(7):e46-e215.
9. Uhlig K, Balk EM, Patel K, et al. Self-Measured Blood Pressure Monitoring: Comparative Effectiveness. Rockville, MD: Agency for Healthcare Research and Quality; 2012. Comparative Effectiveness Reviews, No. 45.
10. Lackland DT. Hypertension: Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure guidelines. Curr Opin Neurol. 2013;26(1):8-12.
11. Vasan RS, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men. JAMA. 2002;287(8):1003-1010.
12. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123(8):933-944.
13. Heart Disease and Stroke Statistics—2006 Update. Dallas, TX: American Heart Association; 2006. 14. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a
scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403-1419.
15. Gu Q, Burt V, Dillon C. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: The National Health and Nutrition Examination Survey, 2001–2010. J Vasc Surg. 2013;57(3):893-893.
16. Dodani S, Sullivan D, Pankey S, Champagne C. HEALS: a faith-based hypertension control and prevention program for African American churches: training of church leaders as program interventionists. Int J Hypertens. 2011(2011); Article ID 820101. doi:10.4061/2011/820101.
17. Ford CD, Kim MJ, Dancy BL. Perceptions of hypertension and contributing personal and environmental factors among rural Southern African American women. Ethn Dis. 2009;19(4):407.
18. Hicks LS, Fairchild DG, Horng MS, Orav EJ, Bates DW, Ayanian JZ. Determinants of JNC VI guideline adherence, intensity of drug therapy, and blood pressure control by race and ethnicity. Hypertension. 2004;44(4):429-434.

Addressing Health Disparities Topic Briefs 59
19. Viruell-Fuentes EA, Ponce NA, Alegría M. Neighborhood context and hypertension outcomes among Latinos in Chicago. J Immigr Minor Health. 2012:1-9.
20. Barnes PM, Adams PF, Powell-Griner E. Health characteristics of the American Indian or Alaska Native adult population: United States, 2004–2008. Hyattsville, MD: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; Mar 9, 2010. National Health Statistics Report, No. 20.
21. del Pilar Rocha-Goldberg M, Corsino L, Batch B, et al. Hypertension Improvement Project (HIP) Latino: results of a pilot study of lifestyle intervention for lowering blood pressure in Latino adults. Ethn Health. 2010;15(3):269-282.
22. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206-1252.
23. Vasan R, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men: the Framingham Heart Study. Med Princ Pract. 2010;19:22-27.
24. Hunte H, Mentz G, House JS, et al. Variations in hypertension-related outcomes among blacks, whites and Hispanics in two large urban areas and in the United States. Ethn Dis. 2011;22(4):391-397.
25. Rose LE, Kim MT, Dennison CR, Hill MN. The contexts of adherence for African Americans with high blood pressure. J Adv Nurs. 2001;32(3):587-594.
26. Garber AM, Sox HC. The role of costs in comparative effectiveness research. Health Aff. 2010;29(10):1805-1811.
27. Mushlin AI, Ghomrawi H. Health care reform and the need for comparative-effectiveness research. N Engl J Med. 2010;362(3).
28. Goetzel RZ, Long SR, Ozminkowski RJ, Hawkins K, Wang S, Lynch W. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions affecting US employers. J. Occup. Env. Med. 2004;46(4):398-412.
29. Campbell KP, Lanza A, Dixon R, Chattopadhyay S, Molinari N, Finch R. A Purchaser’s Guide to Clinical Preventive Services: Moving Science into Coverage. Washington, DC: National Business Group on Health; 2006.
30. DeVol R, Bedroussian A, Charuworn A, Chatterjee A, Kim I, Kim S. An Unhealthy America: The Economic Burden of Chronic Disease. Santa Monica, CA: Milken Institute; 2007.
31. Quinones AR, Liang J, Ye W. Racial and ethnic differences in hypertension risk: new diagnoses after age 50. Ethn Dis. 2012;22:175.
32. Cutler JA, MacMahon S, Furberg CD. Controlled clinical trials of drug treatment for hypertension. A review. Hypertension. 1989;13(5 suppl):I36.
33. Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet. 1997;350(9080):757-764.
34. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000;342(3):145.
35. Staessen Ja, Jiguang W. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. Commentary. Lancet. 2001;358(9287):1033-1041.
36. Margolius D, Bodenheimer T, Bennett H, et al. Health coaching to improve hypertension treatment in a low-income, minority population. Ann Fam Med. 2012;10(3):199-205.
Addressing Health Disparities Topic Briefs 60
37. Whitt-Glover MC, Hunter JC, Foy CG, et al. Peer reviewed: Translating the Dietary Approaches to Stop Hypertension (DASH) diet for use in underresourced, urban African American communities, 2010. Prev Chronic Dis. 2013;10.
38. Kerry SM, Markus HS, Khong TK, et al. Home blood pressure monitoring with nurse-led telephone support among patients with hypertension and a history of stroke: a community-based randomized controlled trial. Can Med Assoc J. 2013;185(1):23-31.
39. Blumenthal JA, Babyak MA, Sherwood A, et al. Effects of the dietary approaches to stop hypertension diet alone and in combination with exercise and caloric restriction on insulin sensitivity and lipids. Hypertension. 2010;55(5):1199-1205.
40. Pavlik VN, Greisinger AJ, Pool J, Haidet P, Hyman DJ. Does reducing physician uncertainty improve hypertension control? Rationale and methods. Circ Cardiovasc Qual Outcomes. 2009;2(3):257-263.
41. Paré G, Moqadem K, Pineau G, St-Hilaire C. Clinical effects of home telemonitoring in the context of diabetes, asthma, heart failure and hypertension: a systematic review. J Med Internet Res. 2010;12(2):e21. doi: 10.2196/jmir.1357
42. Clark CE, Smith LF, Taylor RS, Campbell JL. Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis. BMJ. 2010;341.
43. Alvarado M. Patient-Centered Medical Home Technology Effects on Hypertension and Diabetes Control [dissertation]. Houston, TX: The University of Texas, School of Biomedical Informatics; 2012.
44. Fernandez S, Tobin JN, Cassells A, Diaz-Gloster M, Kalida C, Ogedegbe G. The Counseling African Americans to Control Hypertension (CAATCH) trial: baseline demographic, clinical, psychosocial, and behavioral characteristics. Implement Sci. 2011;6(1):100.
45. Martin KD, Roter DL, Beach MC, Carson KA, Cooper LA. Physician communication behaviors and trust among black and white patients with hypertension. Medical Care. 2013;51(2):151-157.
46. Morgan J. Treatment of hypertension in blacks. JNMA. 1988;80(8):844. 47. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and
the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001;344(1):3-10. 48. Walsh JM, McDonald KM, Shojania KG, et al. Quality improvement strategies for hypertension
management: a systematic review. Med Care. 2006;44(7):646-657. 49. McKee MD, Fletcher J, Sigal I, Giftos J, Schechter C, Walker EA. A collaborative approach to control
hypertension in diabetes outcomes of a pilot intervention. JPCCH. 2011;2(3):148-152. 50. Kim MT, Han HR, Hedlin H, et al. Teletransmitted monitoring of blood pressure and bilingual nurse
counseling–sustained improvements in blood pressure control during 12 months in hypertensive Korean Americans. J Clin Hypertens. 2011;13(8):605-612.
51. Margolis KL, Kerby TJ, Asche SE, et al. Design and rationale for Home Blood Pressure Telemonitoring and Case Management to Control Hypertension (HyperLink): a cluster randomized trial. Contemp Clin Trials. 2012 Jul;33(4):794-803. doi: 10.1016/ j.cct.2012.03.014.
52. Fahey T, Schroeder K, Ebrahim S, Glynn L. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst Rev. 2006;4.
53. Weng C, Coppini D, Sönksen P. Geographic and social factors are related to increased morbidity and mortality rates in diabetic patients. Diabetic Med. 2001;17(8):612-617.

Addressing Health Disparities Topic Briefs 61
Compare the effectiveness of complementary and alternative interventions on reducing symptoms related to treatment of childhood cancers in racial and ethnic minorities.
Introduction This topic brief focuses on the comparative effectiveness of complementary and alternative medicine (CAM)10 to reduce symptoms related to conventional cancer treatment among children in racial and ethnic minority groups, ages 0 to 18 years, with any type of cancer. Conventional medical treatments for childhood cancers include chemotherapy and radiation. Common short-term treatment–related symptoms include, but are not limited to, nausea, diarrhea, hair loss, fatigue, skin and weight changes, kidney problems, and anxiety.2,3 Information about the comparative effectiveness of CAM may help children with cancer and their caregivers make informed choices about options to reduce symptoms related to cancer treatment. It may also lead to improved outcomes that are important to children, their parents, and caregivers. In addition, increased knowledge about positive and negative interactions between CAM and conventional cancer therapies, as well as conventional treatments for symptoms, may foster communication between doctors and families about using CAM to reduce treatment-related symptoms. Burden on Society Childhood cancer incidence has increased but is lower among minority children. Although cancer in children is uncommon, data indicate an upward trend in the number of new cases (incidence) of childhood cancer. The incidence of childhood cancer increased from 11.5 cases per 100,000 children in 1975 to 14.8 per 100,000 in 2004.4 This trend continued with an annual increase of 0.6% in the number of new cases each year between 2005 and 2009.5 The American Cancer Society (ACS) projects that 11,630 new cases of childhood cancer among children ages 0 to 14 years will be diagnosed in 2013.5 The most recent data we identified for childhood cancer incidence among racial and ethnic groups was SEER data collected from 1990 to 1995. These data show that black children had lower cancer incidence rates than white children during that time period. Hispanic and Asian/Pacific Islander children’s cancer
10
The National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of diverse medical and healthcare systems, practices, and products that are not generally considered part of conventional medicine. Conventional medicine (also called Western or allopathic medicine) is medicine as practiced by holders of M.D. (medical doctor) and D.O. (doctor of osteopathic medicine) degrees and by allied health professionals, such as physical therapists, psychologists, and registered nurses. The boundaries between CAM and conventional medicine are not absolute, and specific CAM practices may, over time, become widely accepted.
1 Subgroups of CAM therapies are (1) biologically based therapies (e.g., herbals,
supplements, special diets); (2) mind-body therapies (e.g., mindfulness, hypnosis, guided imagery); (3) manipulative and body-based therapies (e.g., massage); (4) energy therapies (e.g., acupuncture and Reiki); and (5) alternative medicine systems (e.g., traditional Chinese medicine, Ayurveda, homeopathy).
Topic 12: Complementary Medicine for Juvenile Cancer Patients

Addressing Health Disparities Topic Briefs 62
incidence rates were between those for white children and black children. Incidence among American Indian children was the lowest.6 In January of 2009, the estimated number of children aged 0 to 19 years living with cancer was 363,000.7 CAM is used by children with cancer. Herbal remedies, diets and nutrition, and faith-healing were the most commonly studied CAM in a recent systematic review on the prevalence of CAM use. Fewer studies in the review reported on the use of homeopathy, megavitamins, mind-body therapies, and massage. Seven studies included in the review evaluated the association between race/ethnicity and CAM use; however, the review authors did not synthesize the results from these studies.8 Estimates of CAM use among children with cancer vary widely, but most studies found that greater than 30% of children used CAM.8,9 A commonly reported reason for CAM use is to relieve adverse effects (such as nausea or pain) from cancer treatment.8 Minority children may be less likely to use CAM. Data from the National Health Interview Survey, which was not limited to children with cancer, show that one in nine children use CAM. These data also show that CAM use is approximately two times more common among white children (12.8%) than black children (5.9%), and that non-Hispanic children (12.8%) are about 1.5 times as likely to use CAM as Hispanic children (7.9%).10 These data are not limited to children with cancer, and it is not clear if the same patterns of use apply to that group of children. Options for Addressing the Issue There is little evidence on the comparative effectiveness of CAM interventions among children with cancer. Likewise, there is little information about racial and ethnic differences around CAM use in pediatric cancer populations. Two recent systematic reviews identified by our searches took a comprehensive approach to investigating CAM use in childhood cancer. These reviews were not limited to a specific therapy or specific type of cancer and also did not clearly differentiate between use of CAM to treat cancer or to reduce symptoms related to cancer treatment. These reviews primarily reported descriptive results detailing how often and what type of CAM is used.8,11 Very few of the studies included in these reviews compared types of CAM with each other or with conventional symptom treatments, providing little evidence of the relative benefits or harms of CAM. We also identified one recent review that focused on specific symptoms and any type of CAM. This review considered CAM for the management of procedure-related pain, anxiety, and distress. Based on 32 studies, the authors concluded that hypnosis, distraction, and imagery are the three most common CAM therapies used to address pain, anxiety, and distress, and they may be effective when used alone or in conjunction with pharmacological therapies.12 However, the review did not address questions related to race and ethnicity. We identified three systematic reviews that synthesized data on acupressure/acupuncture type therapies for reducing either post-operative or chemotherapy-induced nausea and vomiting. Two of these reviews13,14 focused on studies of acupressure to reduce post-operative nausea and vomiting, and each reported data from studies of pediatric populations, but the studies used in the analyses did not include or were not limited to children with cancer. The third review, which was focused on acupressure for reducing chemotherapy-induced nausea and vomiting, included at least one study of pediatric populations, but did not analyze data among children separately from adults.15 These reviews did not include results related to race and ethnicity.

Addressing Health Disparities Topic Briefs 63
Guidelines from the Society for Integrative Oncology set forth general recommendations for discussing the use and availability of CAM therapies with cancer patients, as well as recommendations about the use of specific CAM therapies. The guidelines present evidence for each recommendation; however, very little information about childhood cancers and pediatric cancer patients is included in the guidelines.16 We did not find any clinical practice guidelines specific to CAM use for children. Based on available evidence, we cannot draw conclusions about the effectiveness of CAM on reducing symptoms related to treatment of childhood cancers. Nor can we draw conclusions about the presence of disparities between racial and ethnic groups in (1) the incidence of symptoms related to childhood cancer treatment or (2) the use of or effectiveness of CAM therapies for relieving symptoms related to cancer treatment among groups. Directly applicable research on the use of CAM in pediatric cancer populations is lacking. In 2006, one study noted that approximately 900 reports of clinical trials using a CAM intervention for children were found. However, most studies of CAM among cancer patients do not include children.17 Data from adult studies are not always applicable to pediatric populations; children may have different experiences than adults with side effects and drug interactions.18 Research that is directly applicable; describes or addresses differences, if any, among racial and ethnic minorities; and can be used to guide the use of CAM in pediatric cancer patients is lacking. Future work would likely require collecting new information over time. The National Cancer Institute (NCI) states that improvements in overall childhood cancer survival mean that researchers, patients, parents, and healthcare providers are focusing more on reducing the burden of cancer and its treatment.19 In 1998, NCI established the Office of Cancer Complementary and Alternative Medicine,20 and several studies listed on its website are focused on pediatric populations,21 suggesting momentum in this area. It is not clear if any of the ongoing studies will address questions of racial and ethnic disparities or explore issues of access related to socioeconomic status. Ongoing and future research that resolves questions about potential disparities and the comparative effectiveness of CAM may lead to more informed choices about options for reducing symptoms related to cancer treatment. High-quality evidence about positive and negative interactions between CAM and conventional cancer therapies may foster communication between doctors and families about the use of CAM. Potential for New Information to Improve Care and Patient-Centered Outcomes Rapidly Evidence regarding disparities, efficacy, and patient preferences is a necessary foundation for future research. Because pediatric cancer patients are already using CAM, healthcare providers, patients, and parents need access to reliable information about the comparative benefits and harms of CAM therapies. Available evidence is likely to be adapted and applied quickly if it is broadly disseminated, given the small number of providers treating these children. However, there are some barriers to the implementation of integrating CAM with conventional cancer treatment. Parents and healthcare providers may need training in order to deliver and apply some therapies. Also, clinical practice guidelines and standardization for some CAM therapies are lacking. Access to CAM may be limited to those who can afford to pay for them and who live where CAM resources and services are available.
Addressing Health Disparities Topic Briefs 64
Research to lessen disparities in the use or benefit of CAM in this population should be considered only after there is documentation that shows disparities exist. This research should also be preceded by evidence that CAM interventions perform better than or as well as conventional medical treatments or evidence showing that patients prefer them even if they do not work quite as well. Comparative effectiveness of and interactions between CAM therapies and conventional treatments may need to be updated as advancements are made in conventional cancer and supportive treatments. References 1. National Center for Complementary and Alternative Medicine. What is complementary and
alternative medicine? Defining CAM. http://nccam.nih.gov/health/whatiscam#definingcam. Published October 2008. Updated May 2012. Accessed February 28, 2013.
2. American Cancer Society. Children diagnosed with cancer: late effects of cancer treatment. http://www.cancer.org/treatment/childrenandcancer/whenyourchildhascancer/children-diagnosed-with-cancer-late-effects-of-cancer-treatment. Reviewed and revised January 31, 2012. Accessed February 28, 2013.
3. KidsHealth. Side effects of chemo and radiation. The Nemours Foundation. http://kidshealth.org/parent/medical/cancer/side_effects.html. Accessed February 28, 2013.
4. National Cancer Institute. FactSheet: Childhood Cancers. Bethesda, MD: National Institutes of Health. http://www.cancer.gov/cancertopics/factsheet/Sites-Types/childhood. Reviewed January 10, 2008. Accessed February 28, 2013.
5. American Cancer Society. Cancer Facts & Figures 2013. Atlanta, GA: American Cancer Society; 2013. 6. Ries LAG SM, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR, eds. Cancer Incidence and Survival
among Children and Adolescents: United States SEER Program 1975-1995. Bethesda, MD: National Cancer Institute, SEER Program; 1999.
7. American Cancer Society. Cancer prevalence: how many people have cancer? http://www.cancer.org/cancer/cancerbasics/cancer-prevalence. Reviewed and revised October 23, 2012. Accessed February 28, 2013.
8. Bishop FL, Prescott P, Chan YK, Saville J, von Elm E, Lewith GT. Prevalence of complementary medicine use in pediatric cancer: a systematic review. Pediatrics. Apr 2010;125(4):768-776.
9. Kelly KM. Complementary and alternative medicines for use in supportive care in pediatric cancer. Support Care Cancer. Apr 2007;15(4):457-460.
10. Barnes PM, Bloom B, Nahin R. Complementary and alternative medicine use among adults and children: United States, 2007. National Health Statistics Reports. December 10, 2008;12.
11. Rheingans JI. A systematic review of nonpharmacologic adjunctive therapies for symptom management in children with cancer. J Pediatr Oncol Nurs. Mar-Apr 2007;24(2):81-94.
12. Landier W, Tse AM. Use of complementary and alternative medical interventions for the management of procedure-related pain, anxiety, and distress in pediatric oncology: an integrative review. J Pediatr Nurs. Dec 2010;25(6):566-579.
13. Lee A, Done ML. Stimulation of the wrist acupuncture point P6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2004(3):CD003281.
14. Dune LS, Shiao SY. Meta-analysis of acustimulation effects on postoperative nausea and vomiting in children. Explore (NY). Jul-Aug 2006;2(4):314-320.
15. Ezzo JM, Richardson MA, Vickers A, et al. Acupuncture-point stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst Rev. 2006(2):CD002285.
Addressing Health Disparities Topic Briefs 65
16. Deng GE, Frenkel M, Cohen L, et al. Evidence-based clinical practice guidelines for integrative oncology: complementary therapies and botanicals. J Soc Integr Oncol. Summer 2009;7(3):85-120.
17. Post-White J. Complementary and alternative medicine in pediatric oncology. J Pediatr Oncol Nurs. Sep-Oct 2006;23(5):244-253.
18. National Center for Complementary and Alternative Medicine. Complementary and Alternative Medicine Use and Children. Bethesda, MD: National Institutes of Health. http://nccam.nih.gov/health/children. Published May 2007. Updated April 2010. Accessed February 28, 2013.
19. National Cancer Institute. Pediatric Supportive Care: Overview. Bethesda, MD: National Institutes of Health. http://www.cancer.gov/cancertopics/pdq/supportivecare/pediatric/healthprofessional. Updated January 9, 2013. Accessed February 28, 2013.
20. O'Mara A. Complementary and alternative medicine research and cooperative groups: can it happen? J Pediatr Oncol Nurs. Sep-Oct 2006;23(5):258-260.
21. National Cancer Institute. Clinical trials search results. Bethesda, MD: National Institutes of Health. http://www.cancer.gov/clinicaltrials/search/results?protocolsearchid=6791991. Accessed March 7, 2013.