managers’ and supervisors’ role in enhancing the safety and health climate for health care...
TRANSCRIPT

Managers’ and Supervisors’ Role in Enhancing the Safety and Health Climate
for Health Care ProvidersN. Sue Bruning
University of Manitoba
January 2012
For more information, please contact:Sue Bruning, Ph.D.I.H. Asper School of BusinessUniversity of ManitobaWinnipeg, MB R3T0C3CANADAEmail: [email protected]: +(204) 474-6566
I

Introduction Study and Community Initiatives and Research Program Two Studies – running simultaneously in healthcare and other sectors Literature on leader and supervisor influences on health and safety Looking at part of the H&S system – a major driver but not the whole system Three years from contract to data completion Thank Yous
– Bruce Cielen and Janine Swanson– Terry Goertzen and Randy Lock– Jim Sanford (MCHCU) , Sandi Mowat (MNU) and Pete Walker (MFL)– All of the RHA CEOs– The human resources and health and safety staff that supported the project– The research assistants on the project: Rebecca Jensen, Tristan Bruning, Nicole Barnabe
and Francoise Cadigan– All of the 2200 managers, supervisors and employees that completed the surveys

All Injury and Time Loss Statistics for the Healthcare Sector and Time Loss Injuries
for the Healthcare Professions
2000
2002
2004
2006
2008
0100020003000400050006000700080009000
10000
Time Loss In-juries - Healthcare ProfessionsTime Loss In-juries - Healthcare SectorAll Injuries - Healthcare Sector
Research Questions What are management and supervisors’ attitudes about and perceived threats
to the safety and health of workers in Manitoba's health care settings? What are the workers perceptions about the top management and
supervisors’ attitudes about safety and health in the organization? Are management and supervisory factors related to positive health and safety
climate perceptions? How are the safety climate perceptions related to employee outcomes,
attitudes, injuries and absences within health care settings? What actions should management and supervisors take to improve the health
and safety environment of employees in the healthcare sector? How can proposed actions be translated into H&S training for management,
supervisors and health care employees?
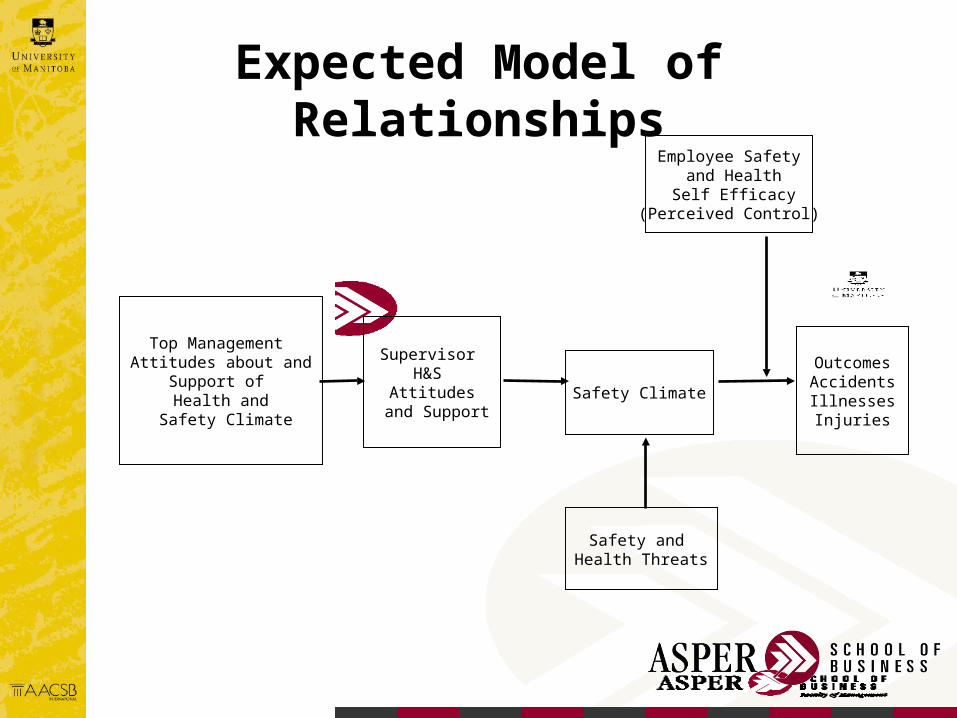
Expected Model of Relationships
Top Management Attitudes about and
Support of Health and
Safety Climate
Employee Safety and Health Self Efficacy
(Perceived Control)
Safety and Health Threats
Supervisor H&S
Attitudes and Support
Safety Climate
OutcomesAccidentsIllnessesInjuries

Project Phases
Phase 1 – Interviews with RHA Chief Executive Officers, human resource representatives and safety and health officers of the RHAs (October – November, 2009)
Phase 2 – Development and administration of the survey.– Original proposal
• 3 RHAs, all 11 RHAs participated• 1000 target – 2200 participated• 2 years – took 3 years

Major Project Changes Web-based survey (1 RHA requested paper and pencil
survey) Extended the survey to broader range of employees in
health care units– Summarize data for total group of respondents and direct
care providers Absence information not available from all RHAs –
utilized self-report absenteeism and injury rates Result – larger and more diversified sample than
originally planned

Interview Data – Phase 1
MSIs greatest threat and age related issues Violence and aggression is a growing threat Mixed in level of inclusion of H&S at Executive
levels Mixed in level of development of H&S plans All were interested in the study and in
participation

Questionnaires – Phase 2Senior/Middle Management Questionnaire. The health and safety attitude questions were adapted from the Strategic Leadership Questionnaire provided by the Worker's Compensation Board of Manitoba. Sixty-six of the questions were deemed relevant to the publicly funded health care sector and were adapted to fit the health care environment. Unit supervisor Questionnaire - views of senior/middle managements support of the health and safety process and programs within the facility.
Employee Questionnaire. The employee questionnaire consisted of 13 demographic questions and 157 questionnaire items. The questionnaire scales included:
• attitudes about top management support for health and safety of employees• direct supervisor support for health and safety• safety climate (3 scales)• stress • organizational commitment (2 scales)• perceived control • workload • responsibility for others• job satisfaction • workplace injuries, days absent due to injuries and health • psychosomatic complaints• intent to leave

Senior/Middle Management Questionnaire Institute of Work and Health – University of Toronto Original survey 70 items
– Eliminated 4 items, adapted the items to the health care sector Sample Questions:
– Senior/middle managers must be involved with employee health & safety (H&S) issues on a daily basis.
– Healthcare workers are more responsible for accidents than their supervisors.– Senior/middle managers should spend the same amount of time in formal and informal H&S
activities.– Senior/middle managers should only deal with major H&S hazards at the hospital/clinic.– Minor H&S hazards should be the responsibility of direct supervisors.
The question examine a number of issues and perspectives on senior/middle management involvement and support in health and safety
Would be a great discussion document amongst senior/middle management to explore support for H&S and how the support should be manifest and communicated to employees
Unit Supervisor Questionnaire
Unit Supervisors – small group 16 questions Sample questions:
– Requires each manager to help improve H&S in his/her work unit.– Invests a lot of time and money in H&S training for workers.– Uses any available information to improve existing H&S rules.– Listens carefully to workers' ideas about improving H&S.– Considers H&S when setting work assignment schedules.

Employee Questionnaire – Management Attitudes
Same 16 items about top management – provides a direct comparison with unit supervisor attitudes
16 items about direct supervisor support of health and safety Sample items:
– Frequently checks to see if we are all obeying the H&S rules.– Discusses how to improve H&S with us.– Uses explanations (not just compliance) to get us to act in a safe and healthful manner.– Emphasizes H&S procedures when we are working under pressure.– Frequently tells us about hazards in our work environment.– Pays attention to H&S rules even when work falls behind schedule.
Other scales – discussed later

Summary of RHA Data Collection Process
RHA Date of Administration of Survey
Assiniboine January-February, 2011
Brandon October-Nov, 2010
Burntwood January-February, 2011
Central May-June, 2011
Churchill November, 2010
Interlake November, 2010
NOR-MAN May, 2011
N Eastman November, 2010
Parkland April, 2011
S. Eastman March-April, 2011 (mail survey)
Winnipeg February-April, 2011

Sample Characteristics
88% female 79% married/partnered .82 Average number of work related injuries 5.3 average days of absence due to work injuries

RHAs and Response Numbers
RHA Response %Assiniboine 271 12.5%Burntwood 123 5.7%Central 98 4.5%Churchill 13 .6%Interlake 175 8.1%North Eastman 56 2.6%Parkland 103 4.8%South Eastman 319 14.7%Brandon 343 15.8%Winnipeg 559 25.8%Total 2165 100%

# Job Categories Response Other Subcategories %
1 Aide: physio/rehabilitation 15 .7%2 Health Care Aide 186 8.6%3 LPN 87 4%4 Nurse 431 19.9%5 Nurse Specialist/practitioner 40 1.8%6 Recreation/pastoral care 32 1.5%
7 Therapist: occupational/physio/respiratory/speech 148 6.8%
8 Mental health/social worker 137 6.3%9 Unit supervisor 56 2.6%
10 Senior/Middle manager 200 9.2%11 Other (please specify)*: 837 (46%)
12 Admin Position - Patient Contact 164 7.6%13 Admin Position - Management 116 5.3%14 - Admin Position - Staff Support 243 11.2%15 - Skilled - Non-medical 77 3.5%16 - Skilled - Medical 98 4.5%17 - Home care 42 1.9%18 - Pharmacist 37 1.7%11 - Unclear 60 2.8%Total 2169 837 100%
* The study was expanded to a broader set of employees. The following job categories were the additional participants surveyed.

Age Distribution of Sample
<25 26-30 31-35 36-40 41-45 46-50 51-55 56-60 61-65 >650
2
4
6
8
10
12
14
16
18
20

Highest Level of Education
Som
e hi
gh S
choo
l
HS
dipl
oma
Som
e co
llege
/Ass
oc col
Prof
trng
/cer
tifica
tion
Bache
lor's
deg
ree
Mas
ter's
deg
ree
Ph.D
. deg
ree
Oth
er0
10
20
30
40

Tenure Distribution of Sample
<1
year
4-6
yrs
11-1
4 yr
s
18-2
0 yr
s
24-2
6 yr
s
>30
yrs
0
5
10
15
20
25
Job tenureFacility tenureHealthcare Expe-rience

Self-Reported Workplace Injuries
zero 1 2 3 4 5 or more
0
10
20
30
40
50
60
70

Senior/Middle Manager attitudes Emphasized the importance of a focus on employee health and
safety; Expressed the need for Senior/Middle managers to be engaged
in H&S activities; Shared attitudes about effective improvement of the health and
safety environment; Identified opinions about the prospects of eliminating health and
safety issues within healthcare environments; Highlighted positive benefits from improved safety and health.

The most positive attitudes were– Top management's requirement for managers to improve the H&S of their units– Use of available information to improve H&S rules– Quick responses to H&S issues/problems– Emphasis on continuous improvement– Attempts to gather ideas from employees about how to improve H&S and other areas.
The average responses to the questions about top management support for health and safety were above 3.5 (out of 5) for 12 of the 16 items.
Total scale average Top Management Support of Health and Safety. The average score on the scale was 3.65.
Views from Unit Supervisors about Top Management Support of Health and Safety

Views from Employees about Top Management Support of Health and Safety
Employee attitudes were generally less positive than direct supervisors were about Top Management Support of Health and Safety
Employees most positive responses were that – Top management requires managers to improve health and safety within their work units– Use available information to improve existing H&S rules– Reacts quickly to solve the problem when told about H&S hazards – Provides the necessary H&S equipment for healthcare workers – The averages of the responses are just over the midpoint of the scale and hover at the mid-
point for the direct care workers. The lowest rating was on whether top management regularly hold H&S
awareness events (e.g. presentations, ceremonies). These data from employees would question whether top management's intended messages about their health and safety priorities have been effectively communicated to employees.
Overall, the non-supervisor employees view top management support of health and safety slightly above the midpoint on the scale

Views from Employees about Direct Supervisor Support of Health and Safety
Employee attitudes are less positive (statistically significant) about Direct Supervisor support of health and safety than of top management
Employees most positive responses were that – Direct supervisors' insist that H&S rules are followed when dealing with patients– Overall, the total scale resulted in an average at the midpoint for both groups – These data suggest that as a group, the direct supervisors are perceived to provide modest
support to employee health and safety issues.

Management and Supervisor Attitudes
Management and Supervisor Attitudes about Health and Safety are related to employee:– Commitment to remain in the organization– Affective Commitment – Job satisfaction– Intention to leave– Psychosomatic complaints– Self reported health– Self reported absences – Workplace injuries

Health and Safety Climate
Health and safety climate (job, coworker and program), in particular views about job safety and the safety program are related to:– Affective Commitment (job and program)– Job satisfaction (job and program)– Intention to Stay (program)– Psychosomatic complaints (job)– Self reported health (job)– Self reported absences (program)– Workplace injuries (job)
Summary of Key Attitudes from the Strategic Leadership Questionnaire
Improved communication and support from top management for the positive development of health and safety policies and practices for employees. Suggestive in the responses and as evident in the research literature, the health and safety of patients and employees within the healthcare sector are interdependent. Positive practices in one domain tend to reinforce positive practices in the other.
Top managers and supervisors who are engaged in the development of a positive health and safety program and climate are related to more positive employee health and safety outcomes. Engagement involves the setting of policies, the inclusion of health and safety information in top management meetings, the visibility and support of health and safety initiatives, inclusion of health and safety performance of units in managerial performance appraisals are examples of strategies that can improve health and safety performance.
Managers recognize that while health and safety incurs costs, there are also significant returns in declines in accident, injury and illness rates, as well as, in positive impacts on the work environment. What can and should be done to better document these relationships?
Dispersed responsibility with positive health and safety attitudes and behaviours generally lead to the most positive returns (according to the research literature).
Accidents and injuries are not primarily chance events. Managers who view the health and safety environment as one where actions and behaviours can reduce hazards and risks will tend to focus on controllable threats to health and safety.

Recommended Actions Summarize the results of the study findings for different groups of health care
providers and employees working in health care settings. These groups should include senior and middle managers, health care professionals and support personnel.
Dissemination of the managerial implications of the results through various practitioner journals, including various RHA publications.
Presentation of the results to various audiences to encourage dialogue and discussion, such as SAFE Healthcare conference in Manitoba.
Development of more health and safety climate training modules/tools/materials for online, continuing education use for medical professionals.
Provide information for web portals for different provincial healthcare websites related to safety climate information in health care.
Increase the academic knowledge of health and safety climate in health care by dissemination of the results in academic journals and at professional conferences.