dorothea orem & imogene king
TRANSCRIPT
| Amethyst Vic C. Mergal, RN

SELF CARE DEFICIT NURSING THEORY
Dorothea Orem
DOROTHEA OREM: Who is she???
Born: 1914, Baltimore, Maryland.
Father: construction, fishing
Mother: homemaker , reading
Youngest of two girlsDied: June 22, 2007
Education
Degrees: Diploma (1930's), Providence Hospital School of Nursing, Washington
DC
BSN Ed. (1939) and MSN Ed. (1945), Catholic University of America, Washington DC.
Honorary Doctorates: Doctor of Science (1976) Georgetown University, (1980)
Incarnate Word College in San Antonio, Texas
Doctor of Humane Letters (1988) Illinois Wesleyan University, Bloomington, Illinois
Doctor of Nursing Honoris Causae, (1998) University of Missouri-Columbia
Special Awards
Catholic University of America Alumni Achievement Award for Nursing Theory (1980)
Linda Richards Award, National League for Nursing (1991)
Honorary Fellow of the American Academy of Nursing (1992).
Nursing Experiences
OR nurseHospital staff nurse (pedia & adult MS units)Private duty nurseNight supervisor in the ERBiological science teacherProfessor of nursing education
Nursing Experiences
1940 – 49 = directorship: both nursing school and department at Providence Hospital, Detroit
1949 – 57(Indiana) = Division of Hospital and institutional Services (Indiana State Board of Health)
1957 –curriculum consultant: Office of Education, US DHEW
1958 – 60 = project (Guides for Developing Curricula for the Education of Practical Nurses)
CUA Member of the Nursing Models
Committee (CUA) Improvement in Nursing Group 1971 – Nursing: Concepts of Practice

Her Story
…she was asked a substantive question and didn’t have an answer because she “had no conceptualization of nursing” (McLaughlin-Renpenning & Taylor, 2002, p. xii).
she noted (Indiana University) that nurses had difficulty articulating needs to hospital
administrators in the face of demands made upon them regarding such issues as length of stay, scheduling admissions and discharges, etc.
Her Thoughts
What is nursing?”“What is the domain and
what are the boundaries of nursing as a field of practice and a field of knowledge?”
Orem (cited in Fawcett 2005) commented that the task required identification of the domain and boundaries of nursing as a science and an art (1978).

Theoretical Sources
Orem says her ideas are primarily the result of reflecting upon her experiences and she was not influenced by any one person (Hartweg, 1991).
Parsons’ structure of social actionVon Bertalnfy’s System TheoryEugenia K. Spalding = a friend and teacherOther nursing theoristsModerate realism (Kantian Philosophy)
Assumptions
1. Human beings require continuous, deliberate inputs to themselves and their environments to remain alive and function according to their capacity.
2. Human agency is exercised in the form of care for self and others in identifying and meeting needs.
3. Mature human beings experience privations in the form of limitations for action and care for self and others involving life-sustaining and function regulating inputs.
Assumptions
4. Human agency is exercised in discovering, developing, and transmitting ways and means to identify needs and make inputs to self and others.
5. Groups of human beings with structured relationships of clustered tasks and allocate responsibilities for providing care to group members who experience privations for making required deliberate input to self and others.
Orem’s General Theory of Nursing
Three Interrelated Theories:
1.Theory of Self-Care = why and how people care for themselves
2.Theory of Self-Care Deficit = why people can be helped through nursing
3.Theory of Nursing Systems = describes and explains relationships that must be made and maintained for nursing to be produced
Theory #1: Self-Care Theory
Based on the concepts of: SELF-CARE SELF-CARE AGENCY SELF-CARE REQUISITES THERAPEUTIC SELF-CARE
DEMAND
Self Care Theory Concepts
Self CareDefinition: the
performance of activities that individuals initiate and perform on their behalf to maintain life, health, and well-being.
Self Care Theory Concepts
Self-Care AgencyDefinition: the individual’s ability to perform
self-care activitiesConsists of TWO agents:
Self-care Agent - person who provides the self-care Dependent Care Agent - person other than the
individual who provides the care (such as a parent)
Affected by basic conditioning factors
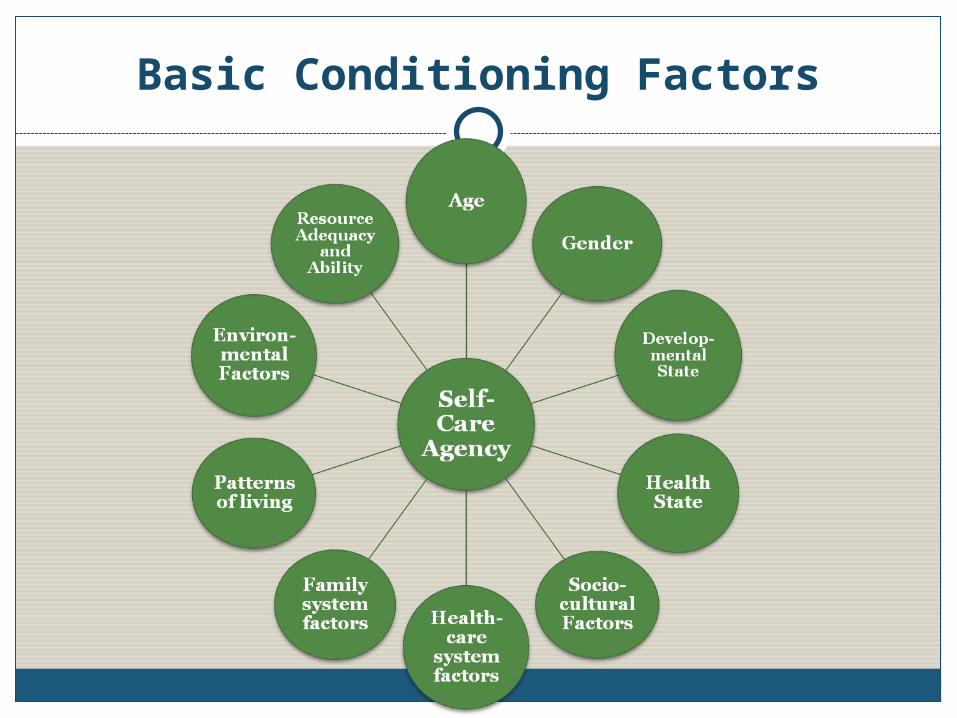
Basic Conditioning Factors
Self Care Theory Concepts
Self-Care RequisitesDefinition: reasons for which self-care is done;
these express the intended or desired resultsConsists of THREE categories:
Universal - requisites/needs that are common to all individuals (e.g. air, water, food, elimination, rest, activity, etc.)
Developmental - needs resulting from maturation or develop due to a condition or event (e.g. adjustment to new job, puberty)
Health Deviation - needs resulting from illness, injury & disease or its treatment (e.g. learning to walk with crutches after a leg fracture)
Self Care Theory Concepts
Therapeutic Self-Care DemandDefinition: the totality of “care measures”
necessary at specific times or over a duration of time for meeting an individuals self-care requisites by using appropriate methods and related sets and actions.”
Theory #2: Self-Care Deficit Nursing Theory
“The condition that validates the existence of a requirement for nursing in an adult is the health associated absence of the ability to maintain continuously the amount and
quality of therapeutic self-care in sustaining life and health, in recovering from
disease or injury, or in coping with their effects.”
Self-Care Deficit Nursing Theory
FOR CHILDREN:
“…the condition is the inability of the parent (or guardian) associated with the child’s health
state to maintain continuously for the child the amount and quality of therapeutic care.”

Self-Care Deficit Nursing Theory
Is the central focus of Orem’s grand theory of nursing
Nursing is required when adults (parent/guardian) are incapable of or limited in their ability to provide continuous effective self-care.
Describes and explains how people can be helped through nursing
Nursing meets these self-care needs through five methods of help
Five Methods of Nursing Help
1. Acting or doing for another2. Guiding and directing3. Providing physical or psychological
support4. Providing and maintaining an environment
that supports personal development5. Teaching
Theory #3: Theory of Nursing Systems
This describes: How the patient’s self care needs will be met by the
nurse , the patient, or both Nursing responsibilities Roles of the nurse and patient Rationales for the nurse-patient relationship Types of actions needed to meet the patient’s
demands
Designed by the nurseBased on the assessment of patient’s ability
to perform self-care activities
The Nursing Agency Concept
A complex property of people educated and trained as nurses that enables them to act, to know, and to help others meet their therapeutic self-care demands by exercising or developing their own self-care agency.
Three Classifications of Nursing Systems
1. Wholly Compensatory: a patient’s self-care agency is so limited that s/he depends on others for well-being.
a. Unable to engage in any form of action (e.g. coma)b. Aware and who may be able to make observations or
judgments, and decisions about self-care but cannot/should not perform actions requiring ambulation and manipulative movements (e.g. patients with C3-C4 vertebral fractures)
c. Unable to attend to themselves and make reasonable judgments about self-care but who can be ambulatory and able to perform some self-care with guidance (e.g. severely mentally retarded)
Wholly Compensatory Nursing System
Three Classifications of Nursing Systems
2. Partly Compensatory: a patient can meet some self-care requisites but needs a nurse to help meet others; either the nurse or the patient have the major role in the performance of self-care
E.g. a patient with recent abdominal surgery

Partly Compensatory Nursing System
Nurse action
Performs some self-care measures for
patientCompensates for self-
care limitations of patient
Assists patient as required
Regulates self-care agency
Patient ActionPerforms some self-
care agencyAccepts care and assistance from
nurse

Three Classifications of Nursing Systems
3. Supportive-educative: a patient can meet self-care requisites but needs help in decision-making, behavior control, or knowledge acquisition; the nurse’s role is to promote the patient as a self-care agent (teacher/consultant)
E.g. a 16-year-old who is requesting birth control information
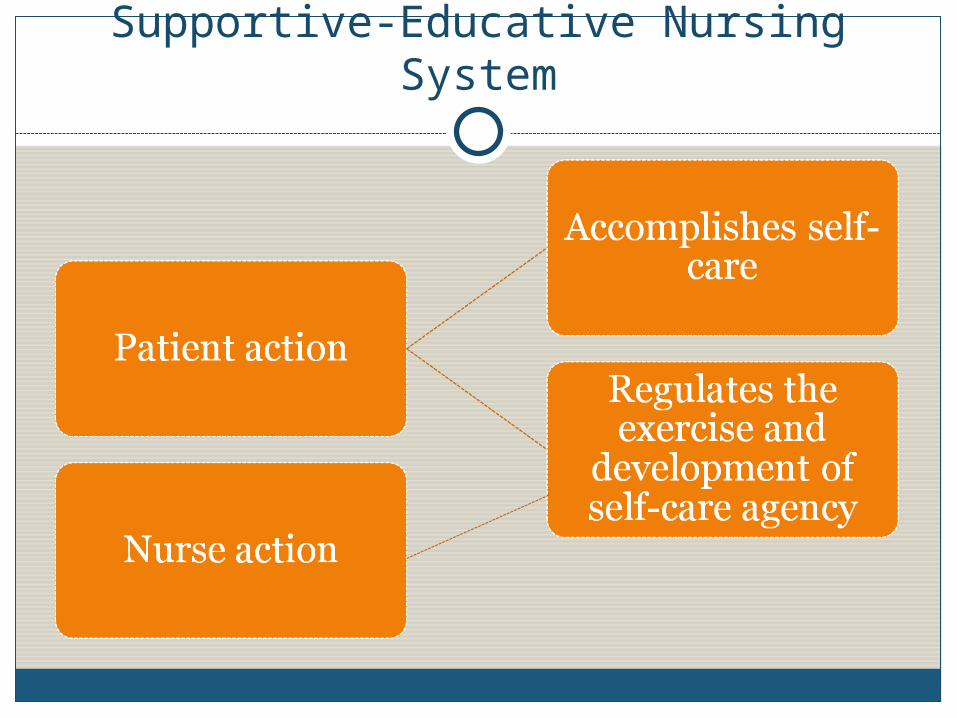
Supportive-Educative Nursing System
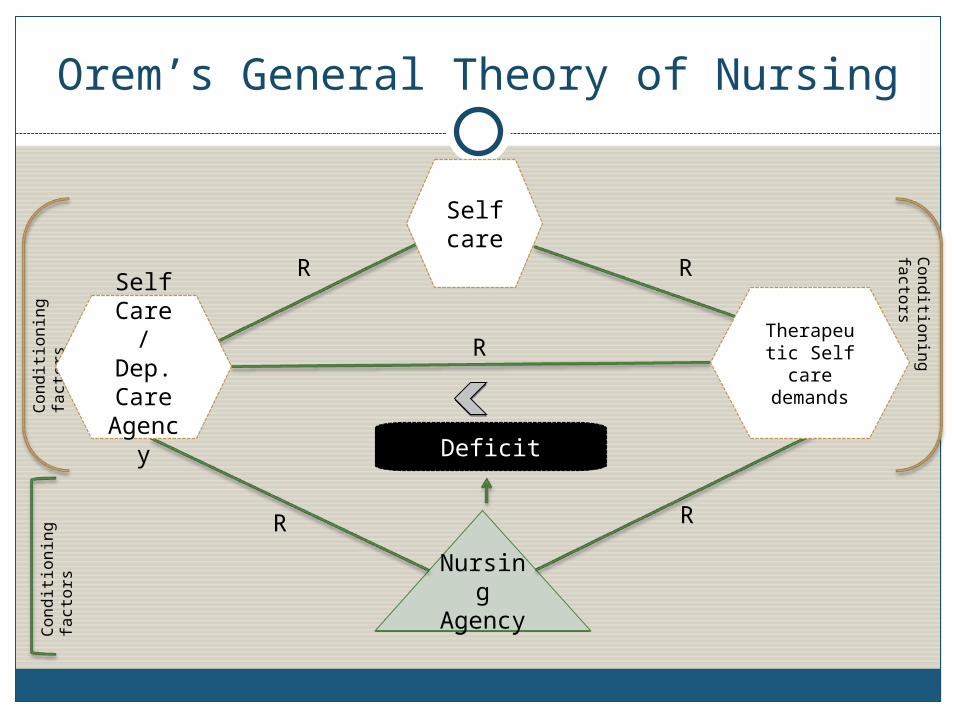
Orem’s General Theory of Nursing
Self care
Nursing
Agency
Nursing
Agency
Deficit
R R
R
R R
Con
dit
ion
ing
fa
ctors
Con
dit
ion
ing
fa
ctors
Con
ditio
nin
g
facto
rs
Therapeutic Self care
demands
Self Care / Dep. Care
Agency

Orem’s Theory & Nursing’s Metaparadigm - PERSON
“…an integrated whole composed of an internal physical, psychologic, and social nature with varying degrees of self-care ability (1971 def.)” (Chinn & Kramer, 2004)

Orem’s Theory & Nursing’s Metaparadigm - PERSON
The recipient of nursing careA being who functions biologically, symbolically,
and socially Has the potential for learning &
developmentIs subject to the forces of natureHas a capacity for self-knowledge Can engage in deliberate actions, interpret
experiences, and perform beneficial actionsCan learn to meet self-care needs (requisites)also referred to as individual, patient, multiperson
unit, self-care agent, dependent-care agent
Orem’s Theory & Nursing’s Metaparadigm - ENVIRONMENT
“…prevailing internal and external conditions in some time and place frame of reference.”
encompassed by two dimensions --- Environmental: physical, chemical and biologic
features atmosphere, pollutants, weather conditions, pets,
infectious organisms, etc. Developmental: socioeconomic features
family & community gender and age roles, cultural roles, and cultural
prescriptions of authority
Orem’s Theory & Nursing’s Metaparadigm - ENVIRONMENT
terms used are environment and environment features
Orem’s Theory & Nursing’s Metaparadigm - HEALTH
“a state of physical, mental, and social well-being, and not merely the absence of disease or infirmity”
a state of well-being, which refers to a person’s perceived condition of existence, characterized by experiences of contentment, pleasure, happiness, and movement toward self ideals and continuing personalization
Orem’s Theory & Nursing’s Metaparadigm - HEALTH
Includes promotion & maintenance of health, treatment of disease and prevention of complications
also referred to as health, health state, and well- being
Orem’s Theory & Nursing’s Metaparadigm - NURSING
“an art through which the practitioner of nursing gives specialized assistance to persons with disabilities of such a character that greater than ordinary assistance is necessary to meet daily needs for self care and to intelligently participate in the medical care they are receiving from the physician”
Components of NURSING
NURSING ART The intellectual quality of nurses which allows them to make
creative investigations, analyses, and syntheses of variables and conditioning factors in nursing situations
NURSING PRUDENCE The quality that enables the nurse to seek advice in new or
difficult situations, to make correct judgments, to decide to act in a particular manner, and/or to act
NURSING SERVICE A human service that focuses on a person’s inabilities to
maintain health care
NURSING AGENCY
Orem’s Nursing Process
Consists of 3 steps:Step 1: determine why a patient needs careStep 2: design a nursing system & plan the
delivery of careStep 3: management of nursing systems -
planning, initiating, & controlling nursing actions
OREM’S THEORY APPLIED
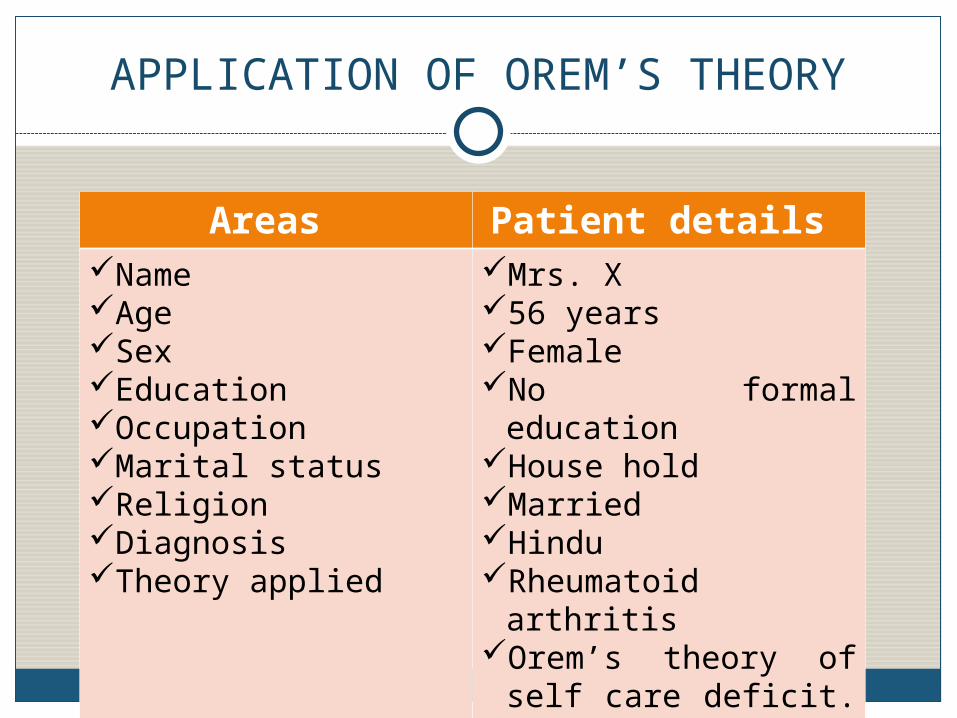
APPLICATION OF OREM’S THEORY
Areas Patient details Name Age Sex Education Occupation Marital status Religion Diagnosis Theory applied
Mrs. X 56 years Female No formal education House hold Married Hindu Rheumatoid arthritis Orem’s theory of self
care deficit.

CASE STUDY
For Mrs. X….She came to the hospital with complaints of pain
over all the joints, stiffness which is more in the morning and reduces by the activities.
She has these complaints since 5 years and has taken treatment from local hospital.
The symptoms were not reducing and came to --MC, Hospital for further management.
Patient was able to do the ADL by herself but the way she performed and the posture she used was making her prone to develop the complications of the disease.
She also was malnourished and was not having awareness about the deficiencies and effects.
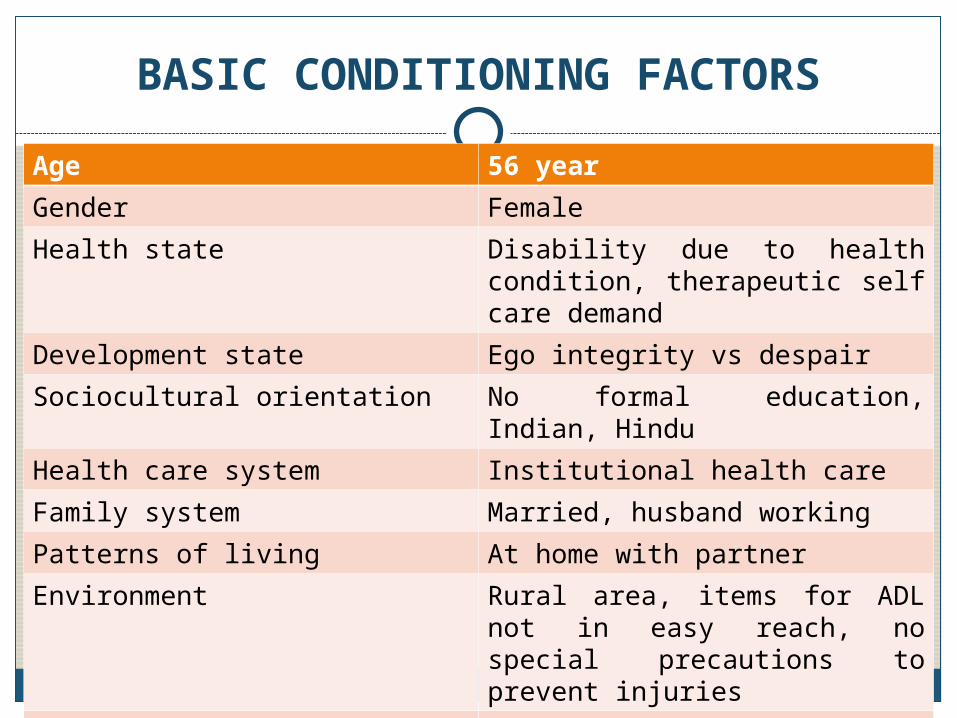
BASIC CONDITIONING FACTORS
Age 56 year
Gender Female
Health state Disability due to health condition, therapeutic self care demand
Development state Ego integrity vs despair
Sociocultural orientation No formal education, Indian, Hindu
Health care system Institutional health care
Family system Married, husband working
Patterns of living At home with partner
Environment Rural area, items for ADL not in easy reach, no special precautions to prevent injuries
Resources Husband, daughter, sister’s son
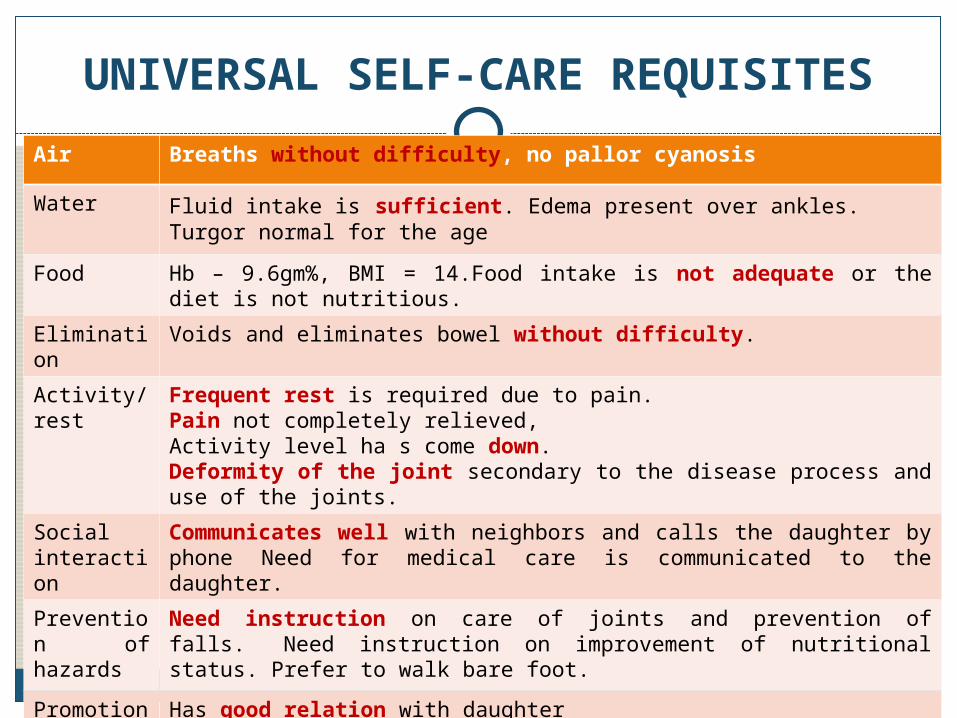
UNIVERSAL SELF-CARE REQUISITES
Air Breaths without difficulty, no pallor cyanosis
Water Fluid intake is sufficient. Edema present over ankles. Turgor normal for the age
Food Hb – 9.6gm%, BMI = 14.Food intake is not adequate or the diet is not nutritious.
Elimination
Voids and eliminates bowel without difficulty.
Activity/ rest
Frequent rest is required due to pain. Pain not completely relieved, Activity level ha s come down.Deformity of the joint secondary to the disease process and use of the joints.
Social interaction
Communicates well with neighbors and calls the daughter by phone Need for medical care is communicated to the daughter.
Prevention of hazards
Need instruction on care of joints and prevention of falls. Need instruction on improvement of nutritional status. Prefer to walk bare foot.
Promotion of normalcy
Has good relation with daughter
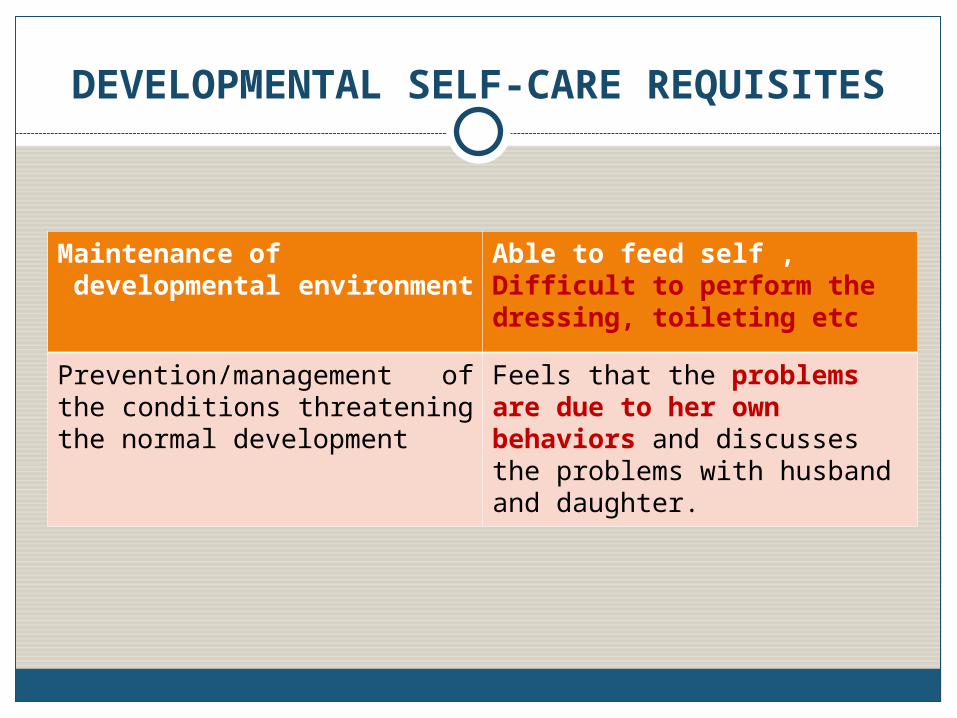
DEVELOPMENTAL SELF-CARE REQUISITES
Maintenance of developmental environment
Able to feed self , Difficult to perform the dressing, toileting etc
Prevention/management of the conditions threatening the normal development
Feels that the problems are due to her own behaviors and discusses the problems with husband and daughter.
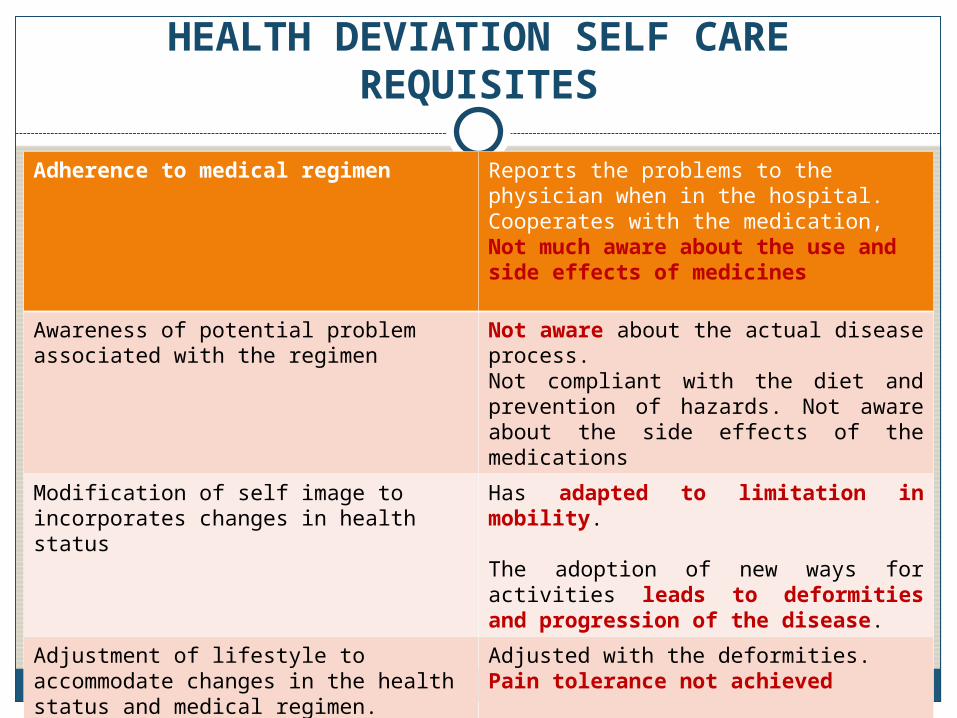
HEALTH DEVIATION SELF CARE REQUISITES
Adherence to medical regimen Reports the problems to the physician when in the hospital. Cooperates with the medication, Not much aware about the use and side effects of medicines
Awareness of potential problem associated with the regimen
Not aware about the actual disease process. Not compliant with the diet and prevention of hazards. Not aware about the side effects of the medications
Modification of self image to incorporates changes in health status
Has adapted to limitation in mobility. The adoption of new ways for activities leads to deformities and progression of the disease.
Adjustment of lifestyle to accommodate changes in the health status and medical regimen.
Adjusted with the deformities. Pain tolerance not achieved
MEDICAL PROBLEM AND PLAN
Physician’s perspective of the condition: Diagnosed with rheumatoid arthritis and is on the
following medications: T. Valus SR OD T. Pan 40 mg OD T. Tramazac 50 mg OD T. Recofix Forte BD T. Shelcal BD Syp. Heamup 2tsp TIDMedical Diagnosis: Rheumatoid arthritisMedical Treatment: Medication and physical
therapy.
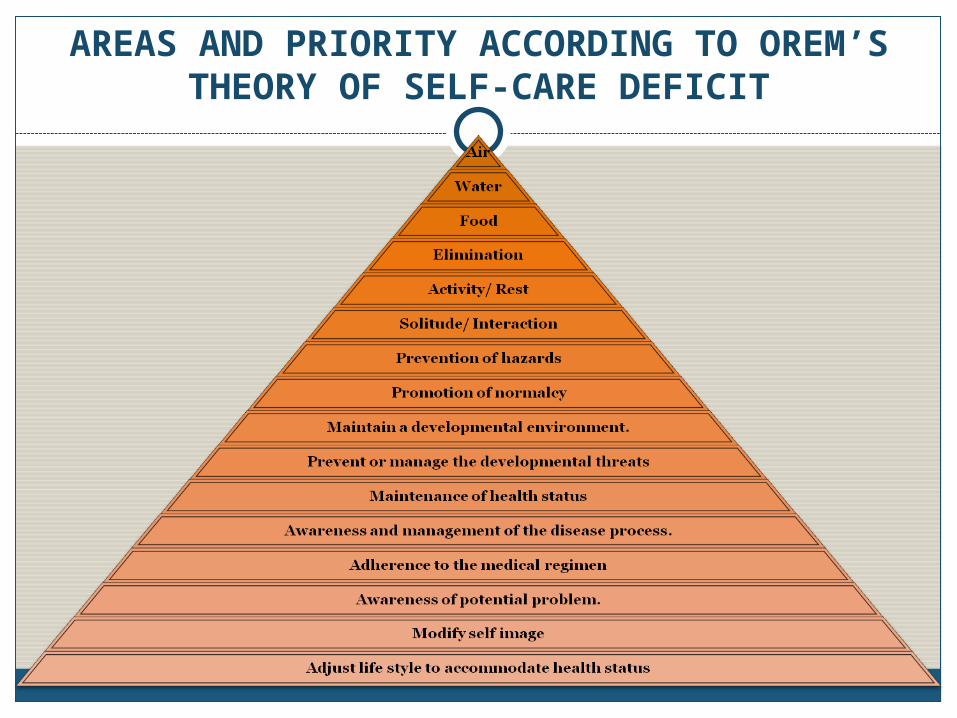
AREAS AND PRIORITY ACCORDING TO OREM’S THEORY OF SELF-CARE DEFICIT
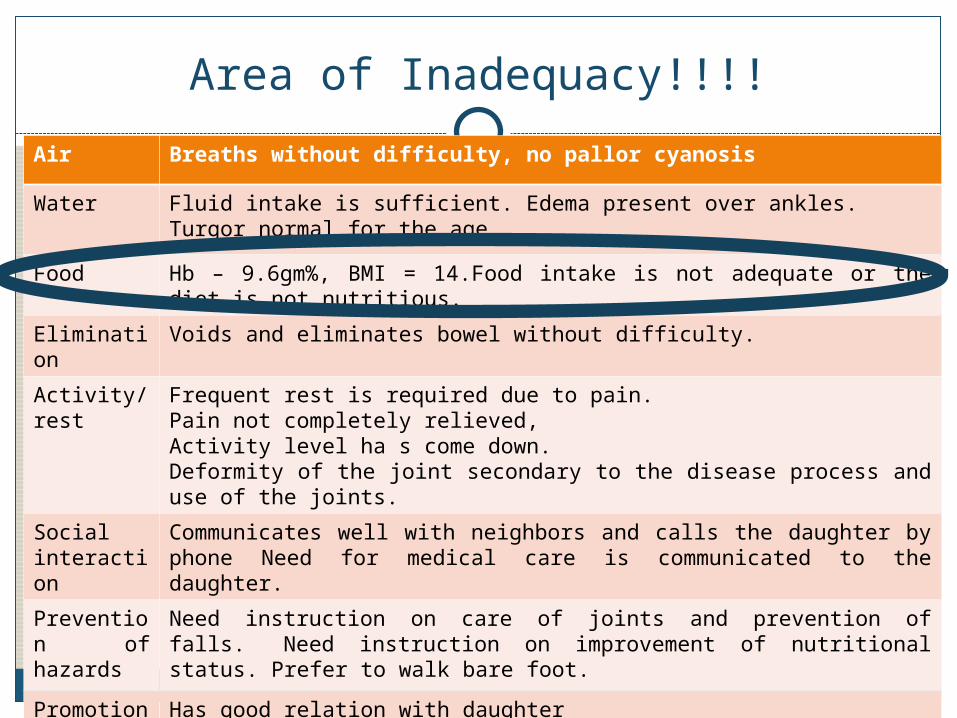
Area of Inadequacy!!!!
Air Breaths without difficulty, no pallor cyanosis
Water Fluid intake is sufficient. Edema present over ankles. Turgor normal for the age
Food Hb – 9.6gm%, BMI = 14.Food intake is not adequate or the diet is not nutritious.
Elimination
Voids and eliminates bowel without difficulty.
Activity/ rest
Frequent rest is required due to pain. Pain not completely relieved, Activity level ha s come down.Deformity of the joint secondary to the disease process and use of the joints.
Social interaction
Communicates well with neighbors and calls the daughter by phone Need for medical care is communicated to the daughter.
Prevention of hazards
Need instruction on care of joints and prevention of falls. Need instruction on improvement of nutritional status. Prefer to walk bare foot.
Promotion of normalcy
Has good relation with daughter
NURSING CARE PLAN
Therapeutic self care demand: Deficient area: food
Adequacy of self care agency: Inadequate
NURSING DIAGNOSIS
Inability to maintain the ideal nutrition related to inadequate intake and knowledge deficit
OUTCOMES AND PLAN
Outcome: improved nutrition Maintenance of a balanced diet with
adequate iron supplementation. Nursing Goals and objectives Goal: to achieve optimal levels of nutrition. Objectives: Mrs. X will:
state the importance of maintaining a balanced diet. List the food items rich in iron , that are available in the
locality.
Design of the nursing system: supportive educativeMethod of helping: guidance Support Teaching Providing developmental environment
IMPLEMENTATION
Mutually planned and identified the objectives and the patient were made to understand about the required changes in the behavior to have the requisites met.
EVALUATION
Mrs. X understood the importance of maintaining an optimum nutrition.
She verbalized that she will select the iron rich diet for her food.
She listed the foods that are rich in iron and that are locally available.
The self care deficit in terms of food is decreased with the initiation of the nutritional intake.
The supportive educative system was useful for Mrs. X .
Usefulness of Theory: RESEARCH
Development of research instruments Exercise of Self Care Agency (Yamashita, Japan) Appraisal of Self Care Agency Self-As-Carer Inventory
Studies that test elements of the theory in various populations Children and adolescents Diabetes mellitus Hemodialysis patients
Usefulness of Theory: EDUCATION
Laying out of the structure of nursing knowledge and explicating the domains of nursing knowledge
Strong and effective framework for curricular design 45 schools in the US use the SCDNT
as the basis for their curriculum
Usefulness of Theory: PRACTICE
Health promotion and care of the sickTeaching self-care to individuals
Renal failure, hemo/peritoneal dialysis, renal transplant Post-stroke conditions Malignancies Elderly
Definition and description of various roles for nurses Clinical nurse-specialist role Case-management role Advanced practice role Primary-care role
Theory Analysis: Simplicity
Presented in a straightforward mannerRelationship among entities can be presented
in a simple diagram
Theory Analysis: Clarity
Precisely definedConsistent with the
language used in action theory and philosophy
Congruent
Theory Analysis: Generality
All of those who need nursing care
All of situations in which individuals (including children) cannot meet all their self-care needs
Appears that the theory is illness oriented rather with no indication of its use in wellness settings

Theory Analysis: Empirical Precision
Generates hypothesesGives additional
knowledgeExtremely contagious
Theory of Goal Attainment
IMOGENE KING, RN, MSN, EdD, FAAN
HER LIFEBorn in January 30,
1923 (West Point, Iowa)
Youngest of three children
Died on December 24, 2007, two days after suffering stroke

EDUCATIONAL BACKGROUND1945 – Nursing diploma from St. John’s Hospital of
Nursing, St. Louis, Missouri1948 – BS Nursing & Education with minors in
philosophy & chemistry from St. Louis University, St. Louis, Missouri
1957 – MS Nursing from St. John’s University1961 – Ed.D. from Teachers College, Columbia
University1980 – Honorary Ph. D from Southern Illinois UniversityPostdoctoral study in research design, statistics and
computer
WORK EXPERIENCESAdministrator (Ohio State University)Educator (St. John’s Hospital School of
Nursing; Loyola University; University of South Florida)
Practitioner (Adult Medical-Surgical Nursing)
Assistant chief of the Research Grants Branch, Division of Nursing, Department of Health, Education and Welfare
Professor emeritus at University of South Florida

ACHIEVEMENTSFounder of King
International Nursing Group (KING) (1998)
Jessie M. Scott award (ANA convention)Award presented to a
registered nurse whose accomplishments in a field of practice, education, or research with significance for the improvement of nursing and health care
MAJOR FACTORS OF THE TIME THAT INFLUENCED KING’S THEORY
EnvironmentKnowledge ExplosionSocial ChangesEducational ChangesScope of the Nursing PracticeCurrent GoalsDimensions
…nursing was striving for status as a science and a legitimate profession.
HER STORY1963.. challenged by her
philosophy professors with a question, “Have you or any other nurses defined the ‘nursing act’?”
1972.. reading course work led King to the Literature Systems analysis and General Systems Theory and hence to another set of questions

HER THOUGHTSWhat is the goal of
nursing?What are the functions
of nurses?How can nurses
continue to expand their knowledge to provide quality care?
THEORETICAL SOURCES1971, 1981.. students, academic colleagues,
nurse researchers, and clinicians thinking1981.. General System Theory (Von Bertalanffy)
conceptual framework1988 .. Kaufman, Orlando and Peplau thinking1988.. Kaufman’s 1958 doctoral dissertation
explore concepts of perception, time and stress…research conducted at Yale University School
of Nursing to test Orlando’s (1961) theory of the deliberative nursing process thinking
THEORETICAL SOURCESKing and Peplau (as cited in
Takahashi, 1992) pointed out the connections between their works with regard to patient outcome.
1988.. a review of her 1971 book by Rosemary Ellis encouraged her to continue her work by deriving a theory from the General Systems Framework. The result…the Theory of Goal Attainment.

ASSUMPTIONSHuman Beings Open systems in constant interaction
with environment Individuals are social beings. Individuals are sentient beings. Individuals are rational beings. Individuals are reacting beings. Individuals are perceiving beings. Individuals are controlling beings. Individuals are purposeful beings. Individuals are action-oriented beings. Individuals are time-oriented beings.
King’s Theory and Nursing’s Metaparadigm - PERSON
…social beings who are rational and sentient
…communicate their thoughts, actions, customs, and beliefs through language
…exhibit common characteristics like ability to perceive, to think, to feel, to choose between alternative courses of action, to set goals, to select means to achieve goals, and to make decisions

HUMAN NEEDSAccording to King, human being has three
fundamental needs:
(a) The need for the health information that is unable at the time when it is needed and can be used
(b) The need for care that seek to prevent illness, and
(c) The need for care when human beings are unable to help themselves.
ASSUMPTIONSNursingThe care of human beingsPerceiving, thinking, relating, judging, and acting
of same behaviors of patientsNursing situation: the immediate environment in
which two individuals establish a relationship to cope with situational events
Goal of Nursing: help individuals and groups attain, maintain, restore health or help individuals die with dignity.
King’s Theory and Nursing’s Metaparadigm - NURSING
…a process of action, reaction, and interaction whereby nurse and client share information about their perceptions in the nursing situation
… nurse and patient share goals, problems, and concerns and explore means to achieve a goal.

NURSINGGoal of nurse: “To help
individuals to maintain their health so they can function in their roles.”
Domain of nurse: “includes promoting, maintaining, and restoring health, and caring for the sick, injured and dying.
Function of professional nurse: “To interpret information in nursing process to plan, implement and evaluate nursing care.
ASSUMPTIONSNurse-Client InteractionsPerceptions of nurse & client influence interaction
process. Goals, needs & values of nurse & client influence
interaction.Individuals have a right to knowledge about
themselves. Individuals have a right to participate in decisions
that influence their life, their health, and community services.

ASSUMPTIONSNurse-Client InteractionsHealth professionals have
responsibility to share information to helps individuals make decisions about their health care.
Individuals have a right to accept or to reject health care.
Goals of health professionals and goals of recipients of health care may be incongruent.
King’s Theory and Nursing’s Metaparadigm - HEALTH
…dynamic life experience of a human being…implies continuous adjustment to
stressors in the external and internal environment through optimum use of one’s resources to achieve maximum potential for daily living
King’s Theory and Nursing’s Metaparadigm - ENVIRONMENT
…the background for human actions
Internal environment: transforms energy to enable person to adjust to continuous external environmental changes
External environment: involves formal and informal organizations. Nurse is a part of the patient’s environment.

DYNAMIC INTERACTING SYSTEMS
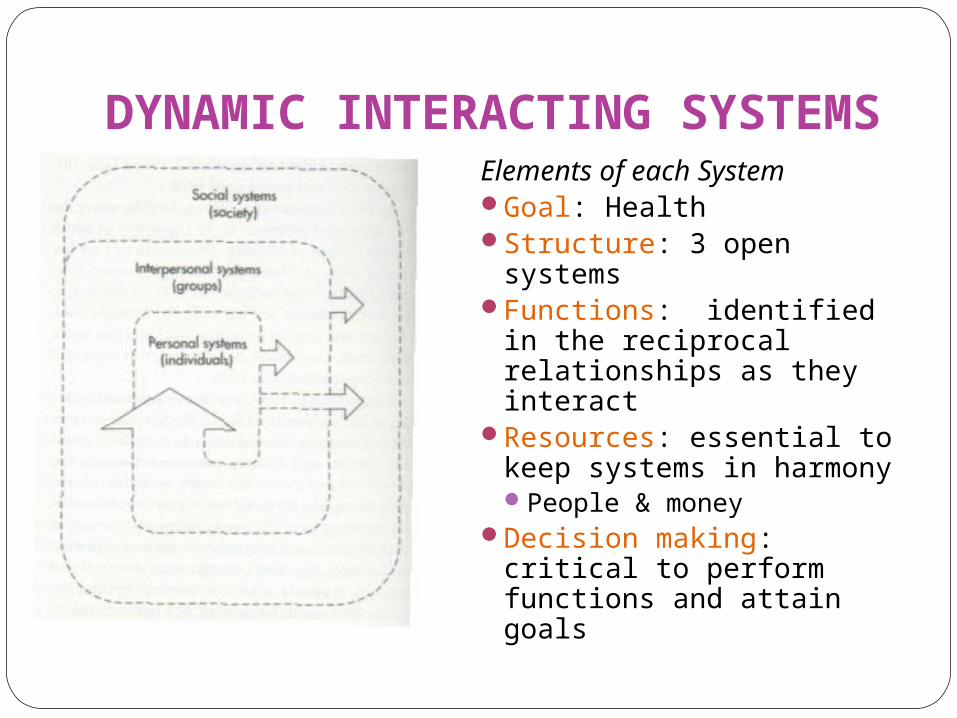
Three systems in the conceptual framework:Personal System (the
individual) Interpersonal Systems
(individuals interacting with one another)
Social System (groups of people in a community/society sharing common goals, interests, and values)
Study systems as a whole rather than as isolated parts of a system
DYNAMIC INTERACTING SYSTEMS
Elements of each SystemGoal: HealthStructure: 3 open systemsFunctions: identified in the
reciprocal relationships as they interact
Resources: essential to keep systems in harmonyPeople & money
Decision making: critical to perform functions and attain goals
Personal System ConceptsPerceptionSelf
awareness of being a person separate from others
Growth and DevelopmentBody Image
personal & subjective; acquired or learned; dynamic and changing
includes how person sees self & other’s reactions to one’s appearance)
SpaceTimeLearning (1986, not defined)
Interpersonal System Concepts
InteractionCommunicationTransactionsRoleStress
Social System ConceptsOrganization
formal or informal structure that orders positions and activitiesmade up of persons with roles and positions to meet goals
Authority regularity, direction and responsibility for actions
Powerenergy necessary to avoid chaos in a society
Statusrelationship of one’s place in a group to others
Decision Makingchanging and orderly process wherein choices are made in
relation to goals
THEORY OF GOAL ATTAINMENT…elements are seen in the
interpersonal systems in which two people, who are usually strangers, come together in a health care organization to help and be helped to maintain a state of health that permits functioning of roles.
…reflects King’s belief that the practice of nursing is differentiated from other healthcare professions by what nurses do with and for individuals
nurse and client communicate information, set goal mutually and then act to attain those goals
MAJOR CONCEPTS OF THE THEORYInteraction
process of perception and communication between person and environment and between person and person
represented by verbal or non-verbal behaviors that seek to reach goals

Feedback
Feedback
KING’S DIAGRAM OF INTERACTION
MAJOR CONCEPTS OF THE THEORYPerception
reality as seen by an individualorganizing, interpreting, and transforming
information from sensory to memory
MAJOR CONCEPTS OF THE THEORYCommunication
exchange of information between people (face-to-face, electronic media, written)
may be intrapersonal / interpersonal
MAJOR CONCEPTS OF THE THEORYTransaction
process of interactions in which human beings communicate with the environment to achieve goals that are valued
goal-directed human behaviors
mutual goal setting
MAJOR CONCEPTS OF THE THEORYRole
set of expected behaviorsPositionRights and
responsibilitiesRelationship between
individuals
MAJOR CONCEPTS OF THE THEORYStress
ever changing condition where an individual interacts with the environment to maintain balance for growth, development, and performance
it is the exchange of information between human and environment for regulation and control of stressors
MAJOR CONCEPTS OF THE THEORYGrowth and Development
ever occurring changes in behavior and at the cellular and molecular level of an individual
Moves a person from potential to achievement
MAJOR CONCEPTS OF THE THEORYTime
an interval between two events that is experienced differently by each person
MAJOR CONCEPTS OF THE THEORYSpace
exists in every direction and is the same in all directions
includes that physical area named territory
defined by the behaviors of a person
THEORETICAL ASSERTIONSIf perceptual accuracy (PA) is present in nurse-
client (I) interactions, transactions (T) will occur.
PA (I) =T
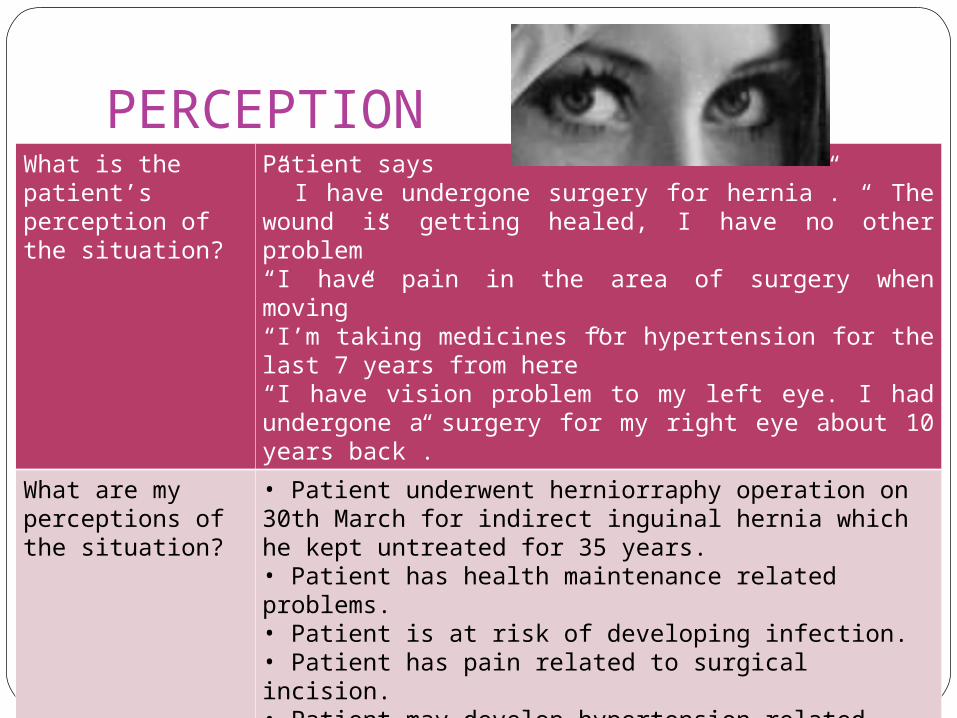
PERCEPTIONWhat is the patient’s perception of the situation?
Patient says” I have undergone surgery for hernia”. “ The wound is getting healed, I have no other problem”“I have pain in the area of surgery when moving”“I’m taking medicines for hypertension for the last 7 years from here”“I have vision problem to my left eye. I had undergone a surgery for my right eye about 10 years back”.
What are my perceptions of the situation?
• Patient underwent herniorraphy operation on 30th March for indirect inguinal hernia which he kept untreated for 35 years.• Patient has health maintenance related problems. • Patient is at risk of developing infection.• Patient has pain related to surgical incision. • Patient may develop hypertension related complications in future.
THEORETICAL ASSERTIONSIf nurse and client make transactions (T), goals
will be attained (GA).
THEORETICAL ASSERTIONSIf goals are attained (GA), satisfactions (S) will
occur.
THEORETICAL ASSERTIONSIf goals are attained (GA), effective nursing care
(NCe) will occur.
THEORETICAL ASSERTIONSIf transactions (T) are made in nurse-client
interactions (I), growth and development (GD) will be enhanced.

THEORETICAL ASSERTIONSIf role expectations and role performance as
perceived by nurse and client are congruent (RCN), transactions (T) will occur.
THEORETICAL ASSERTIONSIf role conflict (RC) is experienced by nurse and
client or both, stress (ST) in nurse-client interactions (I) will occur.

THEORETICAL ASSERTIONSIf nurses with special knowledge and skills
communicate (CM) appropriate information to clients, mutual goal setting (T) and goal attainment (GA) will occur. [Mutual goal setting is a step in transaction and thus has been programmed as transaction.]
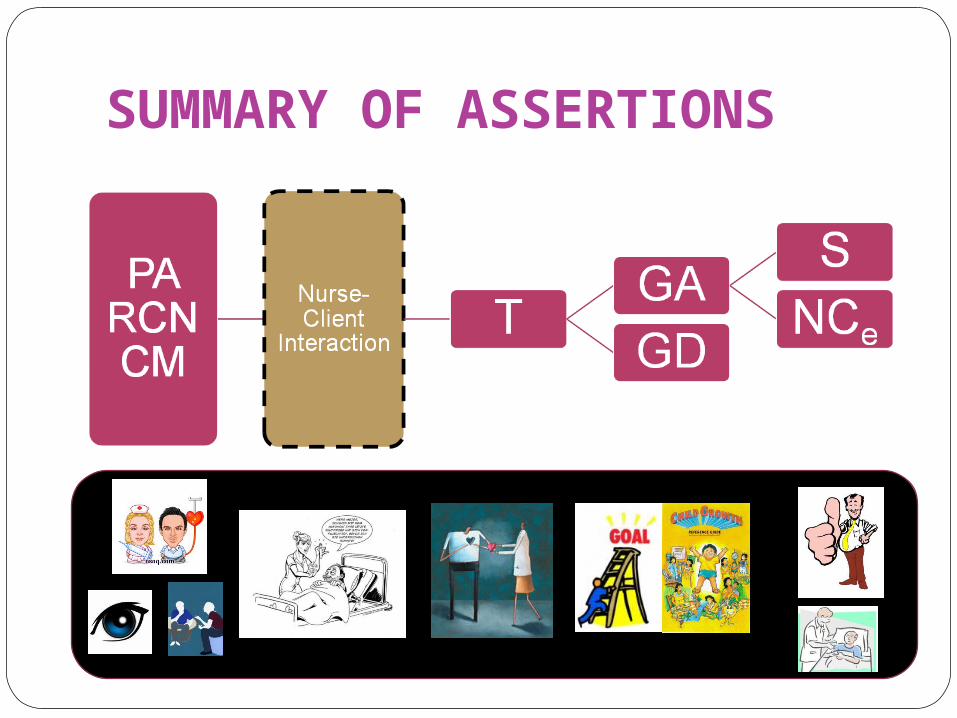
SUMMARY OF ASSERTIONS

SUMMARY OF ASSERTIONS
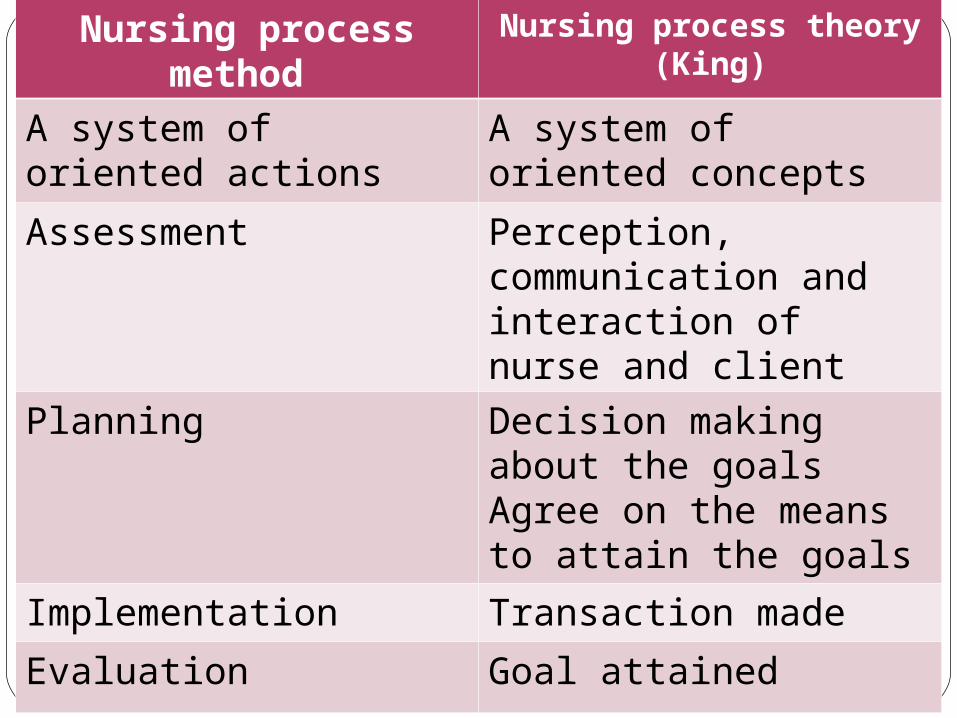
Nursing process method Nursing process theory (King)
A system of oriented actions
A system of oriented concepts
Assessment Perception, communication and interaction of nurse and client
Planning Decision making about the goals Agree on the means to attain the goals
Implementation Transaction made
Evaluation Goal attained
KING’S THEORY APPLIED
Mr. Sy is 74yrs old, married, got admitted in L3 ward of ...Hospital on 03/27/08 with a diagnosis of indirect inguinal hernia, underwent herniorraphy with prolene mesh done on 03/30/08.

ASSESSMENTWhat other information do I need to assist this patient to achieve health?
HistoryIdentification detailsPresent History of IllnessPast health historyFamily HistorySocioeconomic StatusLife StylePhysical examinationReview of SystemsLaboratory InvestigationsOther investigations
What does this information mean to this situation?
Patient neglected a health problem for 35 yearsPatient has acute pain at the site of surgical woundPatient has family history of inguinal hernia and risk for recurrencePatient has a risk for recurrence due to constipation.Patient has risk for infection due to inadequate knowledge and age.Patient is at risk of developing complications of hypertensionPatient requires education regarding health maintenance
PERCEPTIONWhat is the patient’s perception of the situation?
Patient says” I have undergone surgery for hernia”. “ The wound is getting healed, I have no other problem”“I have pain in the area of surgery when moving”“I’m taking medicines for hypertension for the last 7 years from here”“I have vision problem to my left eye. I had undergone a surgery for my right eye about 10 years back”.
What are my perceptions of the situation?
• Patient underwent herniorraphy operation on 30th March for indirect inguinal hernia which he kept untreated for 35 years.• Patient has health maintenance related problems. • Patient is at risk of developing infection.• Patient has pain related to surgical incision. • Patient may develop hypertension related complications in future.
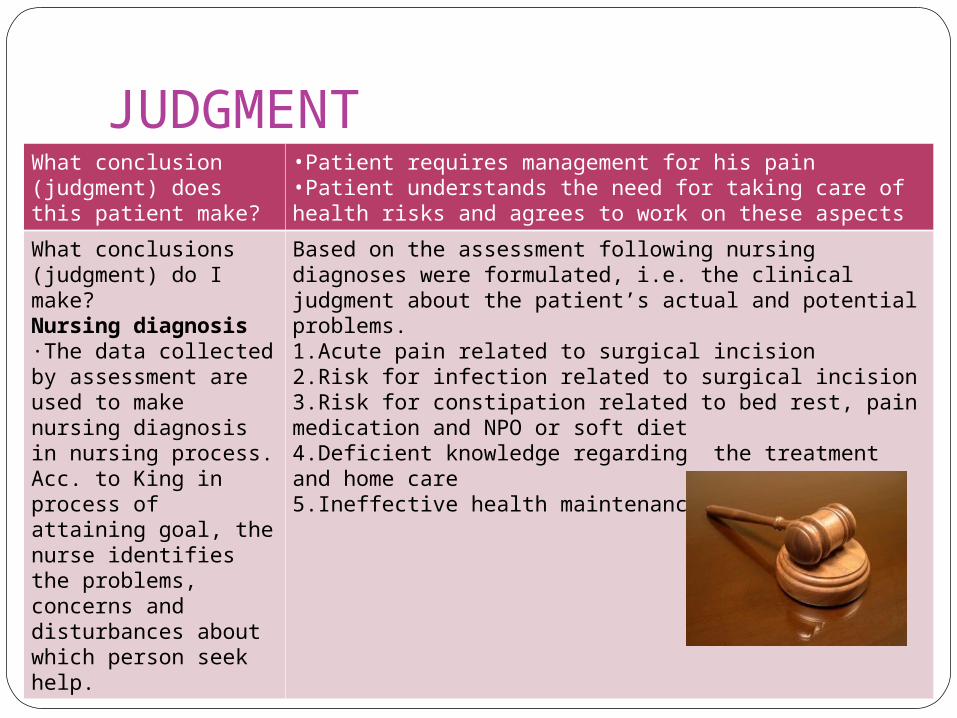
JUDGMENTWhat conclusion (judgment) does this patient make?
•Patient requires management for his pain•Patient understands the need for taking care of health risks and agrees to work on these aspects
What conclusions (judgment) do I make?Nursing diagnosis·The data collected by assessment are used to make nursing diagnosis in nursing process. Acc. to King in process of attaining goal, the nurse identifies the problems, concerns and disturbances about which person seek help.
Based on the assessment following nursing diagnoses were formulated, i.e. the clinical judgment about the patient’s actual and potential problems.1.Acute pain related to surgical incision 2.Risk for infection related to surgical incision 3.Risk for constipation related to bed rest, pain medication and NPO or soft diet 4.Deficient knowledge regarding the treatment and home care 5.Ineffective health maintenance
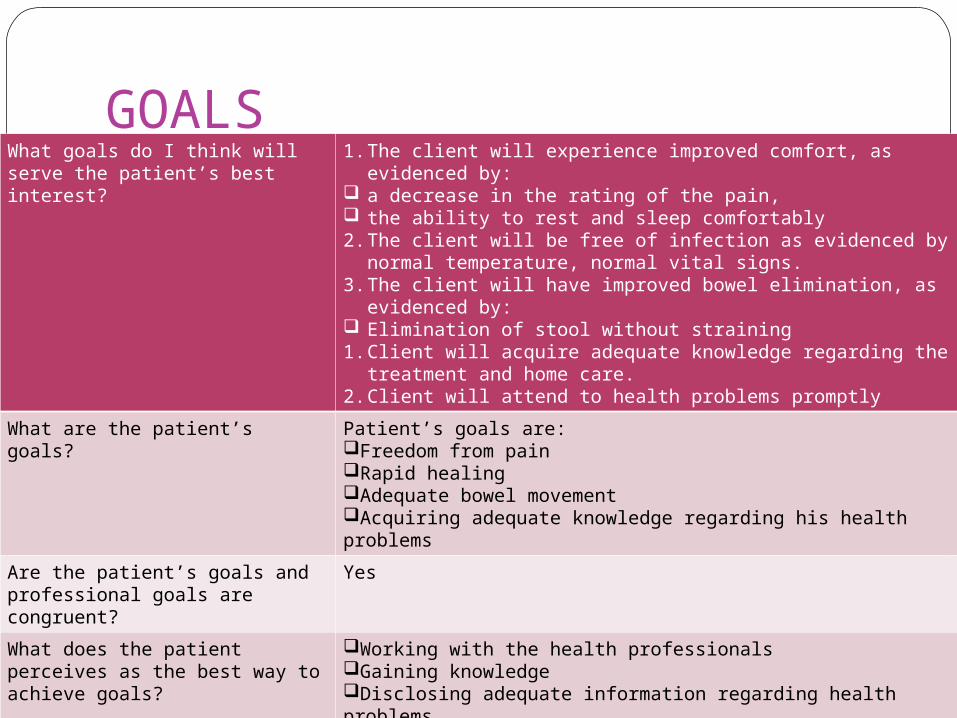
GOALSWhat goals do I think will serve the patient’s best interest?
1. The client will experience improved comfort, as evidenced by: a decrease in the rating of the pain, the ability to rest and sleep comfortably2. The client will be free of infection as evidenced by normal
temperature, normal vital signs.3. The client will have improved bowel elimination, as evidenced
by: Elimination of stool without straining 1. Client will acquire adequate knowledge regarding the
treatment and home care. 2. Client will attend to health problems promptly
What are the patient’s goals? Patient’s goals are:Freedom from painRapid healingAdequate bowel movementAcquiring adequate knowledge regarding his health problems
Are the patient’s goals and professional goals are congruent?
Yes
What does the patient perceives as the best way to achieve goals?
Working with the health professionals Gaining knowledge Disclosing adequate information regarding health problems
Is the patient willing to work towards the goals?
Yes
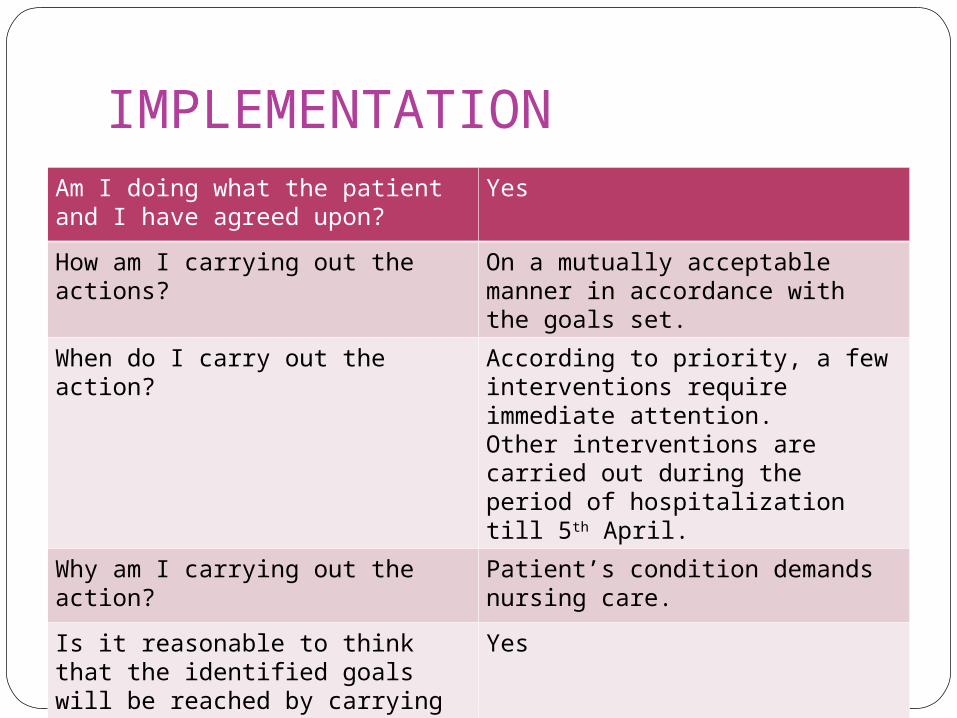
IMPLEMENTATIONAm I doing what the patient and I have agreed upon?
Yes
How am I carrying out the actions?
On a mutually acceptable manner in accordance with the goals set.
When do I carry out the action? According to priority, a few interventions require immediate attention.Other interventions are carried out during the period of hospitalization till 5th April.
Why am I carrying out the action? Patient’s condition demands nursing care.
Is it reasonable to think that the identified goals will be reached by carrying out the action?
Yes
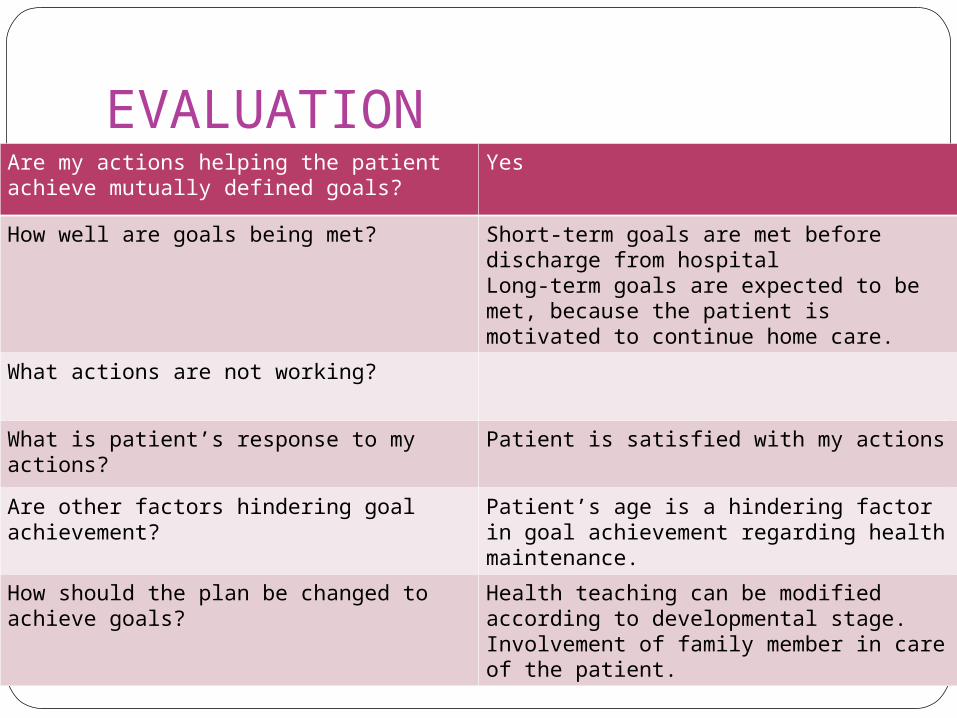
EVALUATIONAre my actions helping the patient achieve mutually defined goals?
Yes
How well are goals being met? Short-term goals are met before discharge from hospitalLong-term goals are expected to be met, because the patient is motivated to continue home care.
What actions are not working?
What is patient’s response to my actions? Patient is satisfied with my actions
Are other factors hindering goal achievement?
Patient’s age is a hindering factor in goal achievement regarding health maintenance.
How should the plan be changed to achieve goals?
Health teaching can be modified according to developmental stage.Involvement of family member in care of the patient.

Usefulness of Theory: RESEARCHBasis for development of
middle-range nursing theoriesModel for Multicultural
Nursing Practice (Rooda, 1992)
Theory of Personal System Empathy (Alligood & May, 2000)
Theory of Family Health (Doornbos, 2000)
Usefulness of Theory: EDUCATIONFramework for the baccalaureate program (Ohio
State University School of Nursing)Educational reform resulting in nursing education
(Sweden)
Usefulness of Theory: PRACTICEA model for bedside nursing practice in the
hospital setting (Coker & Schreiber, 1990)Managed care program in hospital settings
(Hampton, 1994)Goal-Oriented Nursing Record system for
documentationStructure of Quality Assurance Program

Theory AnalysisSIMPLICITY
Easily understoodCLARITY
Clear and conceptually defined from research literature at the time the theory was developed
GENERALITYOthers have critiqued it to
have limited application to nursing esp. in patients who are unable to competently interact with the nurse
King’s Response to Critique:
70% of communication is
non-verbalIt is impossible for a theory
to address every person, event and situation
Even Einstein’s Theory of Relativity could not be tested until space travel made testing possible
Theory AnalysisEmpirical Precision
From a study of 17 patients, goals were attained in 12 cases (70%).
King believes that if nursing students are taught the theory of goal attainment and it is used in nursing practice, goal attainment can be measured and the effectiveness of nursing care can be demonstrated.Promoting health behaviors of
adolescents (Hanna)Interaction analysis between nurses and
patients (Kameoka)

REFERENCES:
George, J.B. (Ed.) (2008). Nursing theories: the base for professional nursing practice. Upper Saddle River, N.J. : Prentice Hall.
Marriner-Tomey, A. & Alligood, M. (2006). Nursing theorists and their work. St. Louis, Mo. : Mosby.
McEwen, M. & Willis, E. (2002). Theoretical basis for nursing. Philadelphia: Lippincott Williams & Wilkins.
Nursing theories. (2008). Retrieved July 29, 2009 from http://www.currentnursing.com/nursing_theory.
Parker, M.E. (Ed.) (1990). Nursing theories in practice. New York: Northeastern Press.
