thrombosis and thrombo-embolisms megan connolly block 2 6/2011
TRANSCRIPT

Thrombosis and Thrombo-embolismsMegan ConnollyBlock 26/2011
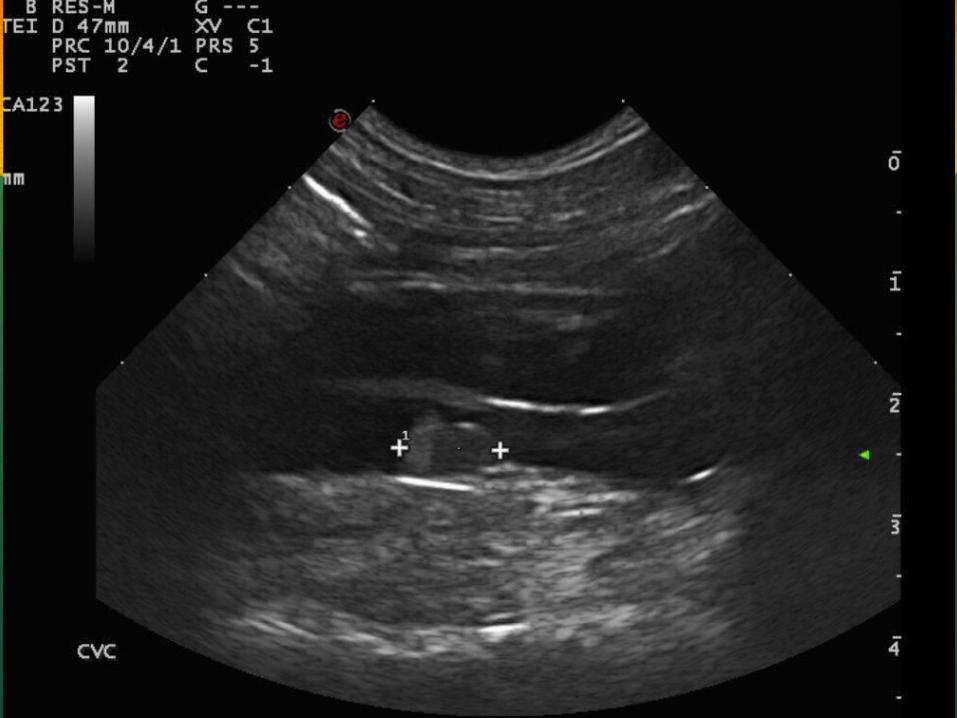
How is a thrombus identified ultrasonographically? B-mode U/S exam Doppler- helps evaluate the degree of vascular
compromise
Acute phase thrombi typically appear anechoic. Some faint echogenicity within the vessel may be seen as color flows around the filling defect when using Doppler.
After several days the thrombus organizes into a visible structure with intermediate echogenicity.
Older thrombi may contract resulting in visualization of flow seen around it.

How to evaluate a thrombus
1. Use Doppler to identify an acute thrombus
2. Evaluate the extent and location of visible thrombi
3. Check for peripheral flow with color Doppler
4. Look for evidence of neoplasia
5. Assess for the sequelae of thrombosisischemia, ascites, etc.

• Thrombosis- formation of a clot/thrombus at a site of blood stasis or vascular injury.
• Thrombo-embolus- obstruction of a vessel downstream of the site of a clot formation.

Common sites of thrombo-embolus formation:
Aortic trifurcationaortic-iliac bifurcation Caudal vena cava Renal arteries Pulmonary arteries Mesenteric arteries


Pulmonary Thromboembolism
Complication of many systemic diseases that predisposes the patient to a hypercoaguable state
Heartworm disease Pulmonary artery thrombosis pulmonary thrombo-embolism
Glomerulonephropathies Loss of antithrombin III through glomerular basement membrane
hypercoagulation
IMHA
Hyperadrenocorticism Secondary to erythrocytosis, hypertension and hypercoaguable state
DIC Intravascular deposition of fibrinthrombosis
Neoplasia Caudal vena cava- most common tumor that invades this vessel is an
adrenal tumor (pheochromocytomas); tumor thrombus travels down phrenicoabdominal vein to reach the vena cava.
Sepsis

Clinical signs of PTE: Acute respiratory compromise and a
ventilation-perfusion mismatch that can be mild or subclinical depending on the degree of embolization.
Difficulty breathing (tachypnea and hyperpnea), coughing (can be productive), wheezing, anorexia, vomiting, lethargy, weightloss.
Cardiac Thrombi and Aortic Thrombo-
embolism Can occur with both HCM, DCM and Restrictive CM.
Stasis of blood activation of clotting factors thrombus formation in left atrium, ventricle or both.
Thrombus can dislodge and form an emboli that may obstruct aortic branches (most commonly at the aortic trifurcation). “saddle thrombus”
Clinical signs: Pain, cold extremities, cyanotic extremities, lack of palpable femoral pulse, signs of CHF. If obstruction is partial may observe neurological
deficits in the hindlimbs or unilateral paresis.






Clinical Signs of other Thromboembolisms
(difficult to identify via ultrasound)
Cerebral TE Change in consciousness, seizures, weakness. If the brain
stem area is affected, then cranial nerve dysfunction, cerebellar signs, coma, or weakness may result.
Mesenteric artery TE often found with GDV, will cause gastrointestinal signs
and abdominal pain.
Renal TE or thrombosis leading to renal infarction : decrease in renal function, pyrexia, back pain, proteinuria
and hematuria or anuria if bilateral and potentially renal failure.