thalassemia - portal.ebmt.org · ndespite progress made in sickle cell anemia(sca) management, such...
TRANSCRIPT

HematopoieticHematopoietic stem stem cellcelltransplantation transplantation
for for hemoglobinopathieshemoglobinopathies
Pr Pr JeanJean--HuguesHugues DalleDalle
EBMT meetingEBMT meeting
Paris April 2011Paris April 2011

HemoglobinopathiesHemoglobinopathies
nnThalassemiaThalassemia
nn SickleSickle CellCell DiseaseDisease

ThalassemiaThalassemia

RationnalRationnal
nn Thalassemia:Thalassemia:nn Hemoglobin disorderHemoglobin disorder
nn Most common monigenetic disorder:Most common monigenetic disorder:nn ≈≈5% of the world population with globin gene variant5% of the world population with globin gene variant
nn 80 million people with 80 million people with ββ ThalassemiaThalassemia
nn 60 000 births a year with major thalassemia60 000 births a year with major thalassemia
nn Initially from (sub) tropic areaInitially from (sub) tropic area
nn Now worldwideNow worldwide
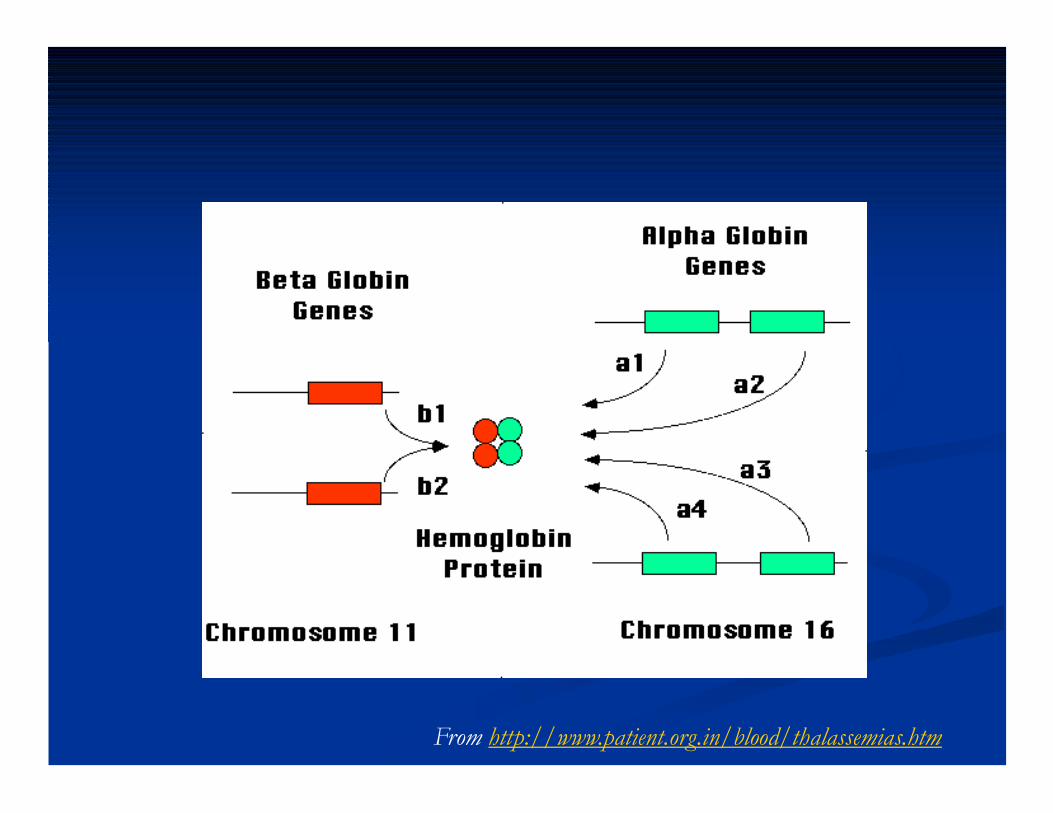
From http://www.patient.org.in/blood/thalassemias.htm

From http://www.patient.org.in/blood/thalassemias.htm
Alpha-thalassemia

From http://sickle.bwh.harvard.edu/thal_inheritance.html

Beta-thalassemia
From http://www.patient.org.in/blood/thalassemias.htm
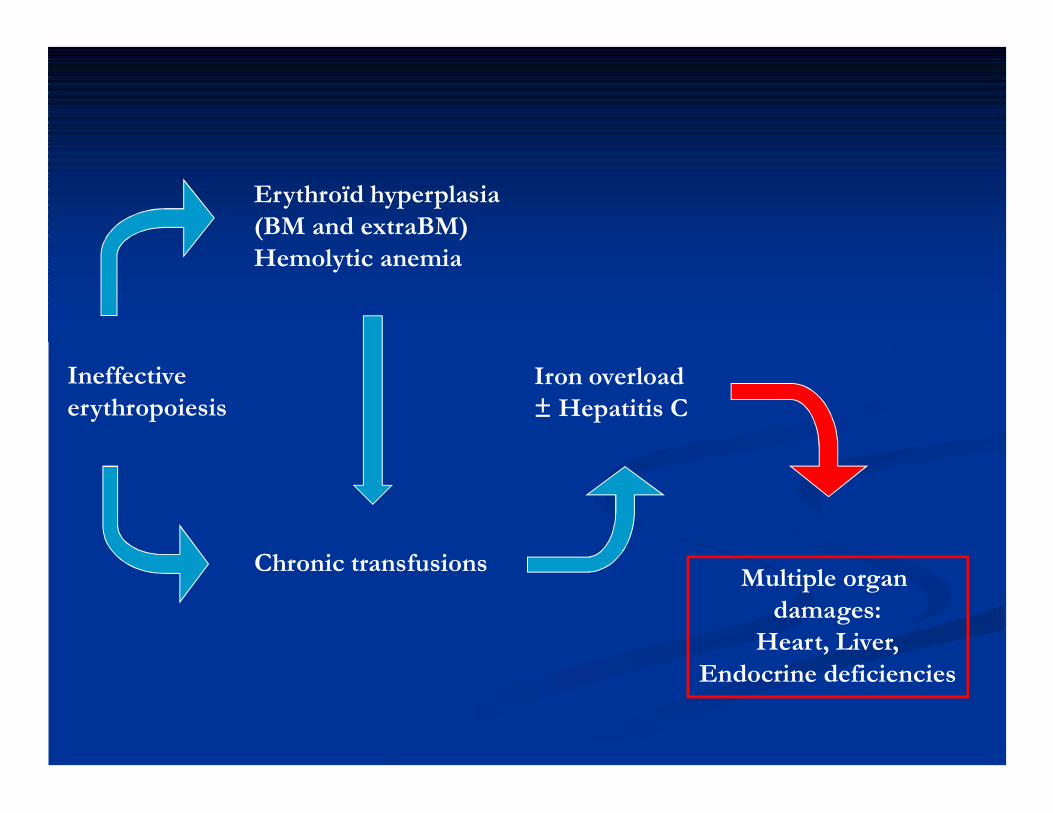
Ineffective erythropoiesis
Erythroïd hyperplasia(BM and extraBM)Hemolytic anemia
Chronic transfusions
Iron overload± Hepatitis C
Multiple organ damages:
Heart, Liver,Endocrine deficiencies

nn To To avoidavoid earlyearly deathdeath::nn ChronicChronic transfusiontransfusion
nn Permanent and efficient Permanent and efficient ironiron chelationchelation therapytherapynnDeferoxamineDeferoxamine
nnDeferiproneDeferiprone
nnDeferasiroxDeferasirox
nn But < 50% of patients But < 50% of patients stillstill remainremain alivealive afterafter 35 35 yearyear of of ageage
HSCT HSCT isis the the onlyonly curative curative treatmenttreatment
for major for major ββ--thalassemiathalassemia
1981 : 1981 : First HSCT for thalassemiaFirst HSCT for thalassemia
nn Seattle groupSeattle groupnn 14 14 monthmonth oldold girlgirlnn HLA HLA identicalidentical sistersistern Successful outcome
nn Pesaro groupPesaro groupnn 16 16 yearyear--oldold heavelyheavely transfusedtransfused thalassemiathalassemia patientpatientnn HLA HLA identicalidentical brotherbrothern Rejection

Angelucci, E. et al. Haematologica 2008;93:1780-1784
Figure 2. Numbers of HSCT performed for thalassemia through the years in centers of the EBMT
First report and First report and resultsresultsLucarelliLucarelli et coll., NEJM 1990et coll., NEJM 1990
nn 222 patients < 17 years of age222 patients < 17 years of agenn OS: 82%OS: 82%nn EFS: 75%EFS: 75%
nn Multivariate analysis for 116 ptsMultivariate analysis for 116 ptsnn Highly homogeneous patient group and therapyHighly homogeneous patient group and therapynn Bu14 + Cy200Bu14 + Cy200nn GvHD prophylaxis:GvHD prophylaxis:
nn CSA + MP CSA + MP nn ±± ATGATG

Pesaro scorePesaro score
Class 1Class 1 Class 2Class 2 Class 3Class 3
ChelationChelation RegularRegular Regular/Regular/
IrregularIrregular
IrregularIrregular
HepatomegalyHepatomegaly
> 2 cm> 2 cm
NoNo No/YesNo/Yes YesYes
Liver FibrosisLiver Fibrosis
(biopsy)(biopsy)
NoNo No/YesNo/Yes YesYes
RiskFactors
RiskClasses
OSOS 94%94% 80%80% 61%61%
EFSEFS 94%94% 77%77% 53%53%
RecurrenceRecurrence 0%0% 9%9% 16%16%

HSCT from related donors for HSCT from related donors for Class 1 & Class 2 patients under 17y.o.Class 1 & Class 2 patients under 17y.o.
About 515 classes 1-2 patients under 17 years of ageIn order to decrease the rate of rejection: + Thiotepa for patients less than 4 yearsand short course MTX
Lucarelli & Gaziev, Blood Reviews 2008

nn Bu14 + Cy200: Bu14 + Cy200: highhigh TRMTRMnn Bu14 + Bu14 + CyCy 120 to 160:120 to 160:
nn BetterBetter overalloverall survivalsurvival (53 to79%)(53 to79%)nn HigherHigher rejection rate (7 to 30%)rejection rate (7 to 30%)
nn Protocol 26 Protocol 26 fromfrom 19971997nn AzathioprineAzathioprine 3mg/kg/d 3mg/kg/d fromfrom DD--4545nn HydroxyureaHydroxyurea 30mg/k/d 30mg/k/d fromfrom DD--4545nn HypertransfusionHypertransfusion regimenregimen ((HbHb>14g/dl) + >14g/dl) + continuouscontinuous
chelationchelationnn GrowthGrowth factorsfactors twicetwice weeklyweeklynn FludarabineFludarabine 20mg/m²/d 20mg/m²/d fromfrom DD--17 to D17 to D--1313nn Bu14 + Bu14 + CyCy 160160
HSCT from related donors for HSCT from related donors for Class 3 patients under 17y.o.Class 3 patients under 17y.o.

About 73 class 3 patients under 17 y.oLucarelli & Gaziev, Blood Reviews 2008
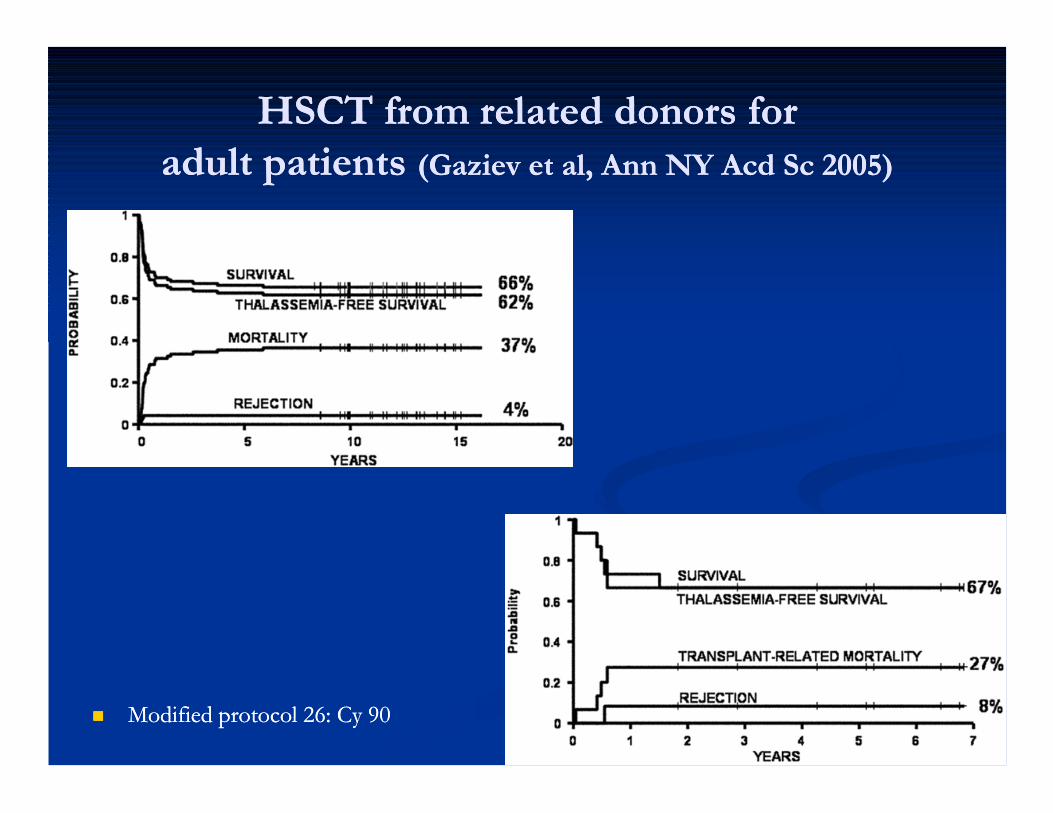
HSCT from related donors for HSCT from related donors for adult patients adult patients (Gaziev et al, Ann NY Acd Sc 2005)(Gaziev et al, Ann NY Acd Sc 2005)
nn Modified protocol 26: Cy 90Modified protocol 26: Cy 90

HSCT from 9 or 10/10HSCT from 9 or 10/10matched unrelated donormatched unrelated donor
nn Bu14 + Cy 200Bu14 + Cy 200
nn Bu 14 + Cy 120/200 + ThiotepaBu 14 + Cy 120/200 + Thiotepa
nn Bu14 + TT10 + Flu 160Bu14 + TT10 + Flu 160
nn GvHD prophylaxis: CSA + MTX +/GvHD prophylaxis: CSA + MTX +/-- ALGALG
nn Autologous rescue of BMAutologous rescue of BM
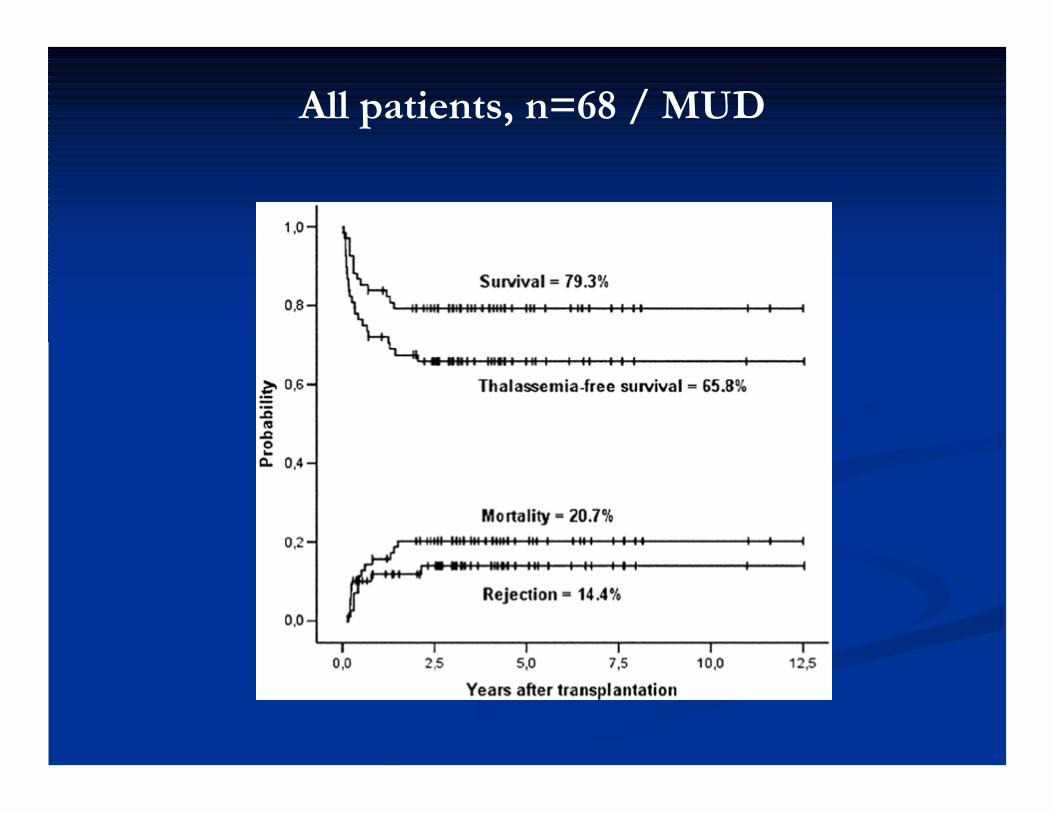
All patients, n=68 / MUD

Class 1-2 patients / MUD

Class 3 patients / MUD
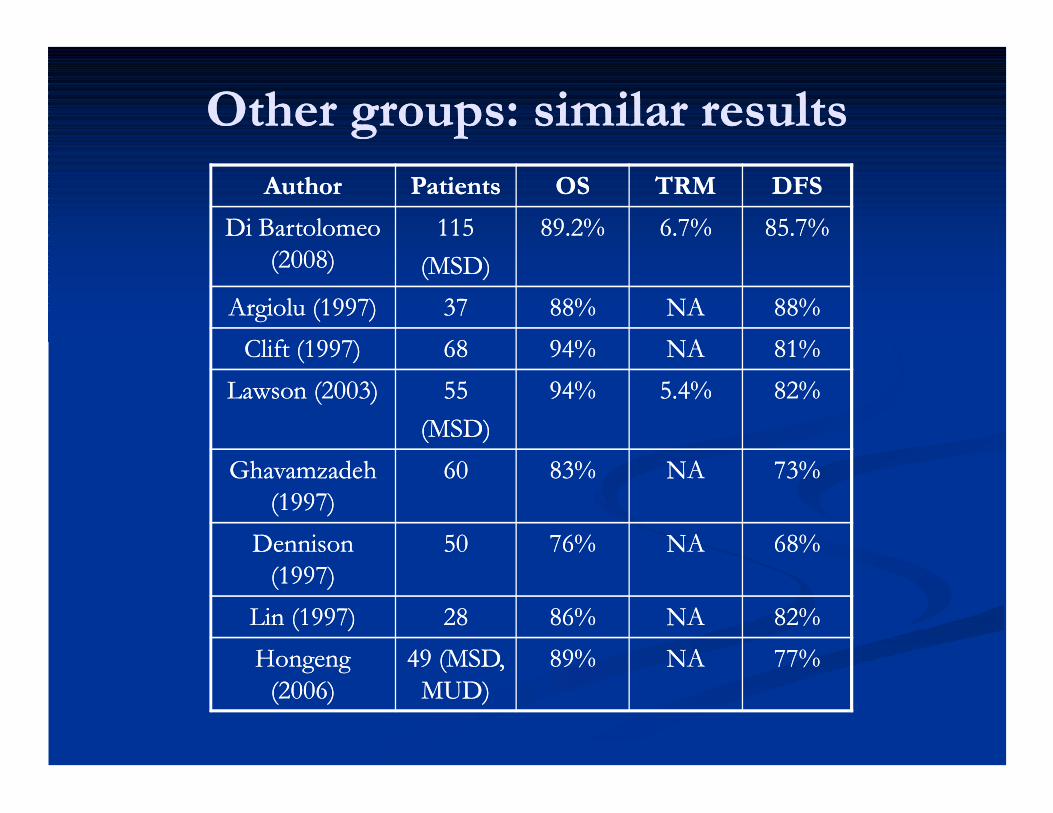
OtherOther groups: groups: similarsimilar resultsresultsAuthorAuthor PatientsPatients OSOS TRMTRM DFSDFS
Di Bartolomeo Di Bartolomeo (2008)(2008)
115115
(MSD)(MSD)
89.2%89.2% 6.7%6.7% 85.7%85.7%
Argiolu (1997)Argiolu (1997) 3737 88%88% NANA 88%88%
Clift (1997)Clift (1997) 6868 94%94% NANA 81%81%
Lawson (2003)Lawson (2003) 5555
(MSD)(MSD)
94%94% 5.4%5.4% 82%82%
Ghavamzadeh Ghavamzadeh (1997)(1997)
6060 83%83% NANA 73%73%
Dennison Dennison (1997)(1997)
5050 76%76% NANA 68%68%
Lin (1997)Lin (1997) 2828 86%86% NANA 82%82%
Hongeng Hongeng (2006)(2006)
49 (MSD, 49 (MSD, MUD)MUD)
89%89% NANA 77%77%

Mixed Mixed chimerismchimerismnn RelativelyRelatively commoncommon situationsituation
nn RepresentsRepresents a a riskrisk factor for rejection:factor for rejection:nn Persistant Persistant recipientrecipient cellscells::
nn > 25% : ≈ 100% > 25% : ≈ 100% secondarysecondary graftgraft failurefailure
nn 1010--25%: 41% 25%: 41% secondarysecondary graftgraft failurefailure
nn < 10%: 13% < 10%: 13% secondarysecondary graftgraft failurefailure
Andreanni et al, Bone Marrow Transplant 2000

« New » « New » conditioningconditioning regimenregimen
nn RICRICnn PoorPoor resultsresults
nn TreosulfanTreosulfan basedbased cond’regimencond’regimen
Bernardo et al, BJH 2008
N=20(17MUD/3MSD)Thiotepa 7mg/m² x 1Treosulfan 14g/m² x 3Fludarabine 40mg/m² x 4
nn RICRICnn PoorPoor resultsresults

Umbilical Cord Blood Transplantation for Children with Thalassemia and Sickle Cell Disease
Annalisa Ruggeri, Mary Eapen, Andromachi Scaravadou, Mitchell S. Cairo, Monica Bhatia, Joanne Kurtzberg, John Wingard, Anders Fasth, Luca Lo Nigro, Mouhab Ayas, Duncan Purtill, Karim
Boudjedir, Wagnara Chaves, Mark Walters, John Wagner, Eliane Gluckman, Vanderson Rocha and for the Eurocord Registry, the Center for International Blood and Marrow Transplant Research and the
New York Blood Center
Biology of Blood and Marrow TransplantationDOI: 10.1016/j.bbmt.2011.01.012
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions

Figure 2
Source: Biology of Blood and Marrow Transplantation (DOI:10.1016/j.bbmt.2011.01.012 )
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions

Figure 1
Source: Biology of Blood and Marrow Transplantation (DOI:10.1016/j.bbmt.2011.01.012 )
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions
With the authorization of Dr Françoise Bernaudin With the authorization of Dr Françoise Bernaudin
Stem Cell Transplantation for Sickle Cell Disease

Regular red cells Sickle cells


Epidemiologyn In North America:
n About 8% of African-American people carry sickle cellgene
n In Sub-Saharian African 10% to 30% of peaople have Sickle cell trait or disease
because of protective effect against malaria in endemicregions that leads to positive selection for the genemutation.
n In Francen 1/3360 live births (≈380/y)n 1/950 live births in Paris and sub-urban area (250 à
270/y)n Approximately 1 in 10 patients who have sickle-related
disease have sickle beta-thalassaemia, which is a variant morecommon among people of Mediterranean origin.

(Steinberg NEJM, 1999)
Mutation on codon 6 of β globin
Transversion A →TGlu → ValHb A→S:Under low O2 level : Polymerisation ofdéoxy-HbS


Clinical expression
n S/S > S-βThal > S/C
n Very wide phenotype, including into a same family

ChallengeChallenge
nn SickleSickle CellCell DiseaseDiseasenn LowLow earlyearly mortalitymortality but but highhigh morbiditymorbidity riskrisknn WideWide phenotypephenotype
nn Stem Stem cellcell transplantation transplantation nn ToxicityToxicity risksrisks (GVHD, (GVHD, gonadicgonadic failurefailure) but ) but offersoffers hopehope of of
cure and cure and betterbetter qualityquality of lifeof life
Benefits
Risks

>20>20--year experience with year experience with SCT for SCD patientsSCT for SCD patients
nn French French experienceexperience beganbegan in 1988 in 1988 followingfollowing twotworeportsreportsnn one SCD one SCD leukemicleukemic patient patient successfullysuccessfully engraftedengrafted in USin US
nn 5 SCD patients 5 SCD patients successfullysuccessfully engraftedengrafted in in BelgiumBelgium

Related Related MyeloablativeMyeloablativeStem Cell Transplantation Stem Cell Transplantation
to Cure Sickle Cell to Cure Sickle Cell AnemiaAnemia: : Update of French ResultsUpdate of French Results
Françoise Bernaudin, Marie Robin, Christèle Ferry, Françoise Bernaudin, Marie Robin, Christèle Ferry, Karima Yacouben, JeanKarima Yacouben, Jean--Hugues Dalle, Régis Peffault de Latour, Hugues Dalle, Régis Peffault de Latour,
Yves Bertrand, Corinne Pondarre, Mathieu Kuentz, Yves Bertrand, Corinne Pondarre, Mathieu Kuentz, JeanJean--Pierre Vannier, Alain Fischer, Isabelle Thuret, Pierre Vannier, Alain Fischer, Isabelle Thuret,
Patrick Lutz, Pierre Bordigoni, Pierre Rohrlich, Patrick Lutz, Pierre Bordigoni, Pierre Rohrlich, JeanJean--Louis Stephan, Nathalie Dhedin, Jean Paul Vernant, Louis Stephan, Nathalie Dhedin, Jean Paul Vernant,
JeanJean--Yves Cahn, Francois Demeocq, Bernard Rio, Yves Cahn, Francois Demeocq, Bernard Rio, Dominique Bories, Eliane Gluckman and Gérard Socié Dominique Bories, Eliane Gluckman and Gérard Socié
for the SFGMfor the SFGM--TCTC
ASH Orlando December 2010

nn Despite progress Despite progress made in sickle cell made in sickle cell anemiaanemia (SCA) (SCA) management, such as management, such as nn the prevention of the prevention of detection detection with with transcranialtranscranial
DopplerpneumococcalDopplerpneumococcal infectionsinfectionsnn introduction of introduction of hydroxyureahydroxyurea therapy therapy nn and early cerebral and early cerebral vasculopathyvasculopathySevere SCA Severe SCA remains a disease with high risk of remains a disease with high risk of
morbidity and early deathmorbidity and early death
n Allogeneic hematopoietic stem cell transplantation (HSCT) is the only curative treatment for SCA nn nevertheless, its use has been limited by the risks of nevertheless, its use has been limited by the risks of
transplanttransplant--related mortality (TRM), graftrelated mortality (TRM), graft--versusversus--host host disease and infertilitydisease and infertility

n Our first experience, reported in Blood 2007, included 87 consecutive severe SCA- patients transplanted in France between 1988 and Dec-2004
nn Global Global results were similar to worldwide experienceresults were similar to worldwide experience

Transplantation procedurenn HbSHbS < 30% < 30% nn MyeloMyelo--ablative ablative ConditioningConditioning RegimenRegimennn BUBU--CY (1988CY (1988--1992) 1992) nn4/12 4/12 unstableunstable chimerismchimerism, rejection, rejection
nn BUBU--CYCY--rabbitrabbit ATG (ATG (ThymoglobulinThymoglobulin 20 mg/kg)20 mg/kg)nnBusulfanBusulfan DayDay--10 to 10 to ––7 7 nn Oral 485 mg/m2 (>= 16 mg/kg)Oral 485 mg/m2 (>= 16 mg/kg)nn IntravenousIntravenous > 2001> 2001
nnCY 200 mg/kg ( 50 mg/kg/d x 4: CY 200 mg/kg ( 50 mg/kg/d x 4: dayday ––5 to 5 to ––2)2)nnRabbitRabbit ATG 20 mg/kg (5 mg/kg x 4 ATG 20 mg/kg (5 mg/kg x 4 dayday ––6 to 6 to ––3)3)

Transplantation Transplantation procedureprocedure (2)(2)
n GVHD prophylaxis (6-9 months)n CSA-MTX for BMT and CSA alone for CBT
n Seizure preventionn Clonazepam during conditioning and CSA therapyn Hemoglobin maintained 9-11g/dln Platelet count > 50,000/mm3n Arterial hypertension strictly controlledn Magnesium deficiency promptly correctedn After 2002, CSA replaced by MMF in case of GVHD
requiring steroids

BU
CY
ATG
Day -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0
Conditioning RegimenSCT
CSA 6CSA 6--9 9 monthsmonthsShort MTX Short MTX

ConsecutiveConsecutive GenoGeno--identicalidentical myeloablativemyeloablativeSCT for SCD (n=161)SCT for SCD (n=161)
nn SFGMSFGM--TC data in TC data in PromisePromise
nn FollowFollow--Up Up stoppedstopped on on 21 March 201021 March 2010
nn ConditioningConditioning RegimenRegimen: : BUBU--CYCY
n without ATG n= 17
n with ATG n=144

Analysis of the data in the patients prepared withATG (n=144) from 1992 to 2010
nn CentersCenters n=16n=16nn Patients Patients (SS, Sb0)(SS, Sb0)nn SexSex: 84 M, 60 F: 84 M, 60 Fnn CMV+ (n=109/144=76%)CMV+ (n=109/144=76%)nn MMedianedian age at transplantage at transplantnn 9.0 years (range:3.29.0 years (range:3.2--27.5)27.5)nn12 patients 12 patients olderolder thanthan 16 16 yearsyears
nn CellCell SourceSource nnnn BoneBone MarrowMarrow 121121nn PBCPBC 11nn CordCord BloodBlood 2121nn CB + BMCB + BM 11

Indications (n=144)Indications (n=144)nn CerebralCerebral vasculopathyvasculopathy 8989n Overt Strokes 39n TIA 3n Stenoses +/- silent strokes 20n Abnormal TCD 9n Silent stokes ± anemia, cogn.deficit 18
nn ErythroidErythroid polyalloimmunisationpolyalloimmunisation 44nn ≥ 3 VOC/≥ 3 VOC/yryr ±± ACS ACS 41 41 nn OsteonecrosisOsteonecrosis 77nn 1 ALL, 1 AML 1 ALL, 1 AML 22nn TRJV > 2.5 m/secTRJV > 2.5 m/sec 11
EngraftmentEngraftment
n Successful: 142/144
n 2 non-engraftment (cord bloods)
n 1 early prolongated pancytopenia
n PN > 500/mm3 : mean 22.3 ± 8.2 daysnBM: 21.3 ± 6.7 vs CB: 32.1 ± 9.8 p < 0.001
n Platelets > 50,000/mm3: mean 29.7 ± 15.5 nBM: 28.3 ± 16.6 vs CB: 48.5 ± 20.3 p < 0.001
n Mean FU: 3.9 years ± 3.9

Acute GVHD Acute GVHD
nn
nn Non Non evaluableevaluable 1 1
nn Absent grade 0Absent grade 0 100100
nn Grade IGrade I 1111
nn Grade IIGrade II 2525
nn Grade IIIGrade III 33
nn Grade IVGrade IV 44
GVH ≥ II 32 (23%)
ChronicChronic GVHGVHn Non evaluable 1
n Absent 128
n Present 14 (9.7%)
nMild 9
nExtensive 4 … … .deaths
nResolved 1
n No AGVH ≥ II and no chronic GVHD
after CBT

Events (n=9)
n Non-engraftment (n=2)
n Rejections (n=1) at 3.2 years post-transplant
n Deaths (n=6)n Sepsis during aplasia (n=1)
n Hemorrhagic stroke (n=1) at day32 in a patient with severe Moya
n Extensive GVHD (n=4)
n death at 2, 4 12, 30 months post-transplantn obliterans bronchiolitis (n=2)
n Aspergillosis, CMV, adenovirus… ..

OtherOther ComplicationsComplications
nn VenoVeno--occlusive occlusive diseasedisease n=1n=1
nn SubduralSubdural hematomahematoma n=1n=1
nn EBV EBV proliferationsproliferations , , treatmenttreatment withwith antianti--CD20 n=3CD20 n=3nn EarlyEarly pancytopeniapancytopenia
nn SecondarySecondary PancytopeniaPancytopenia 12 12 monthsmonths postpost--transplant transplant withwith 100% total 100% total donordonor chimerismchimerismn Successfull outcome following donor CD34 addback
nn NephroticNephrotic syndrome n=1syndrome n=1
nn PerPericaicarditisrditis n=1n=1
nn HemorrhagicHemorrhagic CystitisCystitis n=10n=10n 2 highly severe
0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Su
rviv
al p
rob
ab
ility
(%
)
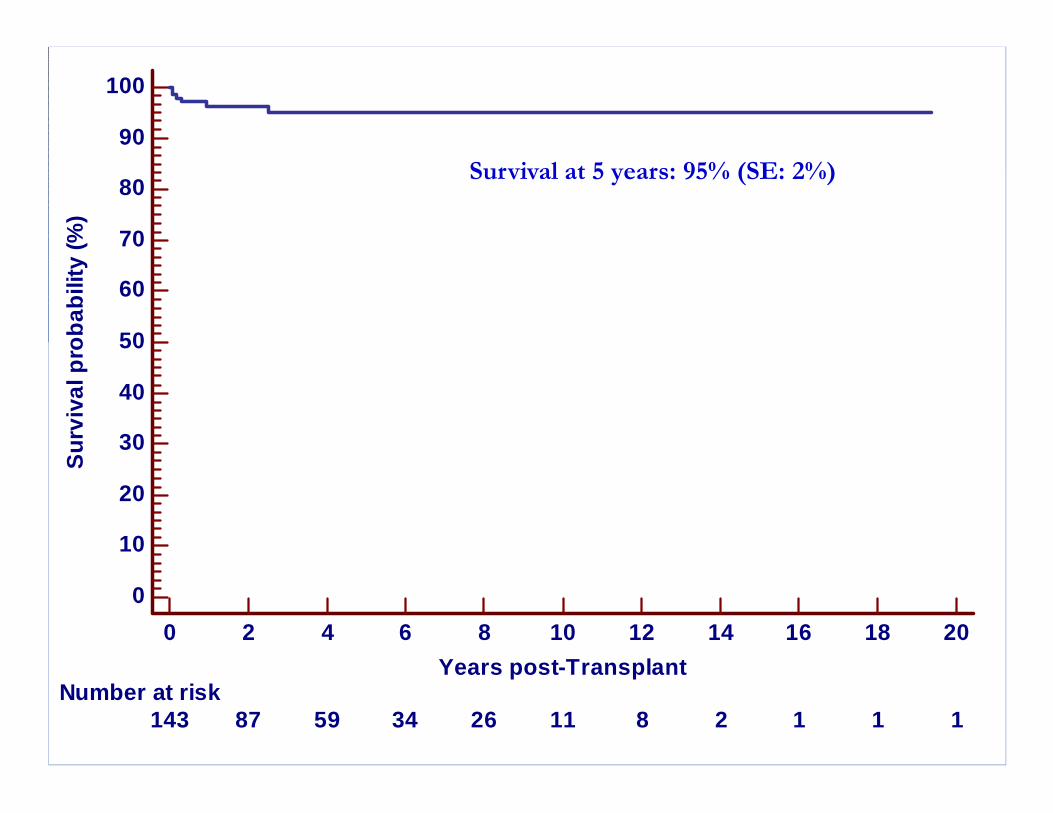
Number at risk143 87 59 34 26 11 8 2 1 1 1
Survival at 5 years: 95% (SE: 2%)

0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Re
jec
tio
n p
rob
ab
ility
(%
)
Number at risk142 85 57 32 25 11 8 2 1 1 1
Rejection at 5 years : 2.8% (SE: 1.7%)

Event-free (Disease-free) Survival at 5 years 92.2% (SE: 2.6%)
0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Ev
en
t-fr
ee
Su
rviv
al p
rob
ab
ility
(%
)
Number at risk142 85 57 32 25 11 8 2 1 1 1
Event-free (Disease-free) Survival at 5 years 92.2% (SE: 2.6%)

EFS at 5 y: 73.9% (SE 9.2%)
Log Rank: p=0.0001
EFS at 5y: 95.8% (SE 2.5%)
0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Ev
en
t-F
ree
Su
rviv
al p
rob
ab
ility
(%
)
Number at riskGroup: 0
23 17 17 15 15 11 8 2 1 1 1Group: 1
119 68 40 17 10 0 0 0 0 0 0
Year of Transplant0= < 20001= > 2000
EFS at 5 y: 73.9% (SE 9.2%)
Log Rank: p=0.0001
EFS at 5y: 95.8% (SE 2.5%)

EFS at 5 years: 90.2% (SE 6.6%) vs 92.4% (SE 2.9%)
Log Rank: p=0.53 NS
0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Even
t-F
ree S
urv
ival p
rob
ab
ility
(%
)
Number at riskGroup: cord blood
19 14 11 5 4 0 0 0 0 0 0Group: other
123 71 46 27 21 11 8 2 1 1 1
Cell SourceCord BloodBM or PBC
EFS at 5 years: 90.2% (SE 6.6%) vs 92.4% (SE 2.9%)

0 1 2 3 4 5 6 7 8 9 10
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Ev
en
t-F
ree
Su
rviv
al p
rob
ab
ility
(%
)
Age at Transplant< 16 years (n=132)> 16 years (=12)

0 2 4 6 8 10 12 14 16 18 20
100
90
80
70
60
50
40
30
20
10
0
Years post-Transplant
Ev
en
t-F
ree
Su
rviv
al p
rob
ab
ility
(%
)
Number at riskGroup: 0
130 83 55 30 23 11 8 2 1 1 1Group: 1
12 2 2 2 2 0 0 0 0 0 0
Age at Transplant0= < 16 years1= > 16 years
n These results with 121 patients transplanted with BU-CY-ATG since year 2000 confirm that it is possible to offer more than 95% chances of cure to SCA-children
nn HLAHLA--genogeno--identical HSCT after identical HSCT after myeloablativemyeloablative conditioning conditioning with ATG should be considered as standard of care for SCA with ATG should be considered as standard of care for SCA children, children, nn not only for those at high risk of stroke not only for those at high risk of stroke nn but also for children experiencing crises or other but also for children experiencing crises or other
complications requiring intensive therapy such as complications requiring intensive therapy such as transfusion program or transfusion program or hydroxyureahydroxyurea..
nn and also for young adults and also for young adults nn Sibling cordSibling cord--blood cryopreservation should be systematically blood cryopreservation should be systematically
offered offered n pre-implantation genetic diagnosis coupled with HLA
selection should be early discussed with the parents?


Osteonecrosis (n=13)
n Modification of MRI
n bright T1 signal corresponding to normal fatty replacement
n Rapid reconstructive repairn In a patient with
pre-SCT destruction of the humeral head
Pre-SCT 14 m. post-SCT
Pre-SCT Post-SCT

Outcome of macro-vasculopathy
nn VascularVascular occlusions occlusions persistedpersisted
nn Variable Variable outcomeoutcome of of stenosesstenosesnn 5 5 resolvedresolved
nn 16 16 remainedremained unchangedunchanged
nn 2 2 progressedprogressedPre-SCT 18m post-SCT

GrowthGrowth and and developmentdevelopment
nn GrowthGrowth postpost--transplant transplant waswas normalnormal
nn MeanMean WeightWeight SDS SDS significantlysignificantly improvedimproved --0.1 to +0.1 to +0.05 0.05 SDSD
nn GirlsGirls
nn PostPost--pubertalpubertal atat SCT (n=7)SCT (n=7)
nn AmenorrheaAmenorrhea, , lowlow estradiolestradiol, , elevatedelevated FSH et LH FSH et LH
nnNecessitatingNecessitating hormone replacement hormone replacement therapytherapy
nn PrepubertalPrepubertal atat SCT (n=33)SCT (n=33)
nn AmongAmong 17 17 assessableassessable youngyoung femalefemale
nn 5 5 hadhad spontaneousspontaneous pubertypuberty ((signif.youngersignif.younger atat SCT:5.9 vs SCT:5.9 vs 10.1)10.1)
nn 12 12 requiredrequired hormone hormone therapytherapy for for pubertypuberty inductioninduction
nn Boys : normal Boys : normal pubertypuberty withwith normal FSH, LH and normal FSH, LH and testotesto but but anyanysemensemen analysisanalysis performedperformed

Development of Psycho-Intellectual Performances of Transplanted
Sickle Cell Disease Patients: a ProspectiveStudy From Pre-Transplant Period
to 5 Years After HSCT
J.Bockenmeyer, K.Yakouben, D.Adjaoud, B.Lescoeur, M. Ouachée-Chardin, M. Benkerrou, JH. Dalle and A.Baruchel.
Robert Debré Hospital - Paris 7 Paris Diderot University - France
ASH Meeting 2009
Patients and Methods
n Longitudinal and prospective study
n Time-points:n Before HSCT
n + 3 years
n + 5 years
n Wechsler ScalesnWPPSI for children < 6 y.o.
nWISC III and IV (Aug 2003) for children > 6 y.o.
nWISC IV adds picture concepts, matrix reasoning and word reasoning
Wechsler Scalesn Composite index from 4 index and 15 sub-tests
n Verbal Comprehension Index (VCI)
n Perceptual Reasoning Index (PRI)
nWorking Memory Index (WMI)
n Processing Speed Index (PSI)
n Global IQ is calculated from these 4 indexn IQ = 100 is the reference for considered age group

Patients and Methods
n 15 SCD children
n Allogeneic HSCT from sibling donor
n From 12/1992 to 06/2006
n HSCT Indication : n CVA (n=13)n Cerebral vasculopathy (n=2)

Results of pre-HSCT evaluations
n All index were < 100
n Mean global IQ was 85

IQ
VCI
PRI
WMI
PSI

Minimal intensity regimenIannone R. (Biol.Bl.Bm.Transplant. 2003)
•No toxicity , no serious GVHD survival 100% but no stable mixed chimerism were obtained:
- increased cell dose (CD34, CD3) with the use of CSP?
- prolong post transplant immunosuppression?
- pre transplant HU and/or azathioprine?
- add ATG? Increase conditioning intensity from reduced to mild?

Umbilical Cord Blood Transplantation for Children with Thalassemia and Sickle Cell Disease
Annalisa Ruggeri, Mary Eapen, Andromachi Scaravadou, Mitchell S. Cairo, Monica Bhatia, Joanne Kurtzberg, John Wingard, Anders Fasth, Luca Lo Nigro, Mouhab Ayas, Duncan Purtill, Karim
Boudjedir, Wagnara Chaves, Mark Walters, John Wagner, Eliane Gluckman, Vanderson Rocha and for the Eurocord Registry, the Center for International Blood and Marrow Transplant Research and the
New York Blood Center
Biology of Blood and Marrow TransplantationDOI: 10.1016/j.bbmt.2011.01.012
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions

Figure 2
Source: Biology of Blood and Marrow Transplantation (DOI:10.1016/j.bbmt.2011.01.012 )
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions

Figure 1
Source: Biology of Blood and Marrow Transplantation (DOI:10.1016/j.bbmt.2011.01.012 )
Copyright © American Society for Blood and Marrow Transplantation Terms and Conditions

Concerns for boththalassemia and SCD
nn PostPost--HSCT:HSCT:nn HypofertilityHypofertility
nn SomeSome (but few) (but few) pregnanciespregnancies have been have been reportedreported
nnOvaryOvary cryopreservationcryopreservation
nn SecondarySecondary tumortumor
nn PrePre--HSCT:HSCT:nn In vitro In vitro fecondationfecondation withwith double double diagnosisdiagnosis: absence : absence
of of diseasedisease and HLA compatibility and HLA compatibility withwith previousprevious sicksickchildchild??

Future
nn Gene Gene therapytherapy