summer webcast series for meditech users - iatric...
TRANSCRIPT

UPDATES! June 2015
Message from Senior Management
MUSE Musings, Summer Schedules, and Communication Changes
Frank Fortner President
Summer Webcast Series for MEDITECH Users
Iatric Systems Blog
Sepsis Is On The Rise
file:///C|/Users/haidee.leclair/Desktop/June2015.html (1 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
Message from Senior Management
Call 978.539.0734 or email [email protected] 24/7, 365 days a year.
MUSE Musings, Summer Schedules, and Communication Changes
Frank Fortner, President
Recently, I attended the 2015 International MUSE Conference in Nashville. Every year I enjoy the camaraderie and excitement of catching up with old friends (be they customers, partners, or shhhh… even competitors). After all, it's a small community where many people have known each other for many years — even decades! As usual, I enjoyed the many invigorating business and even social conversations. I always seem to come away with a new appreciation for the challenges our hospital clients are facing. At the same time, I find it's important to look around and listen to the overall buzz of the show in order to understand what's really going on in the big picture sense. In the immortal words of Yogi Berra, "you can observe a lot just by watching."
One of the main things I observed this year (apart from the higher attendance and bigger MEDITECH presence) was that Meaningful Use (while still a hot topic!) was not the only topic on the minds of attendees. They were also thinking about patient engagement, patient privacy, medical device integration, mobile applications, web-based EMRs, and more. Time will ultimately tell if hospitals today are less intimidated by the familiarity of Meaningful Use or (since CMS has already paid out $30B as of March 2015) simply ready to give MU3 a lower priority, possibly even ignoring it and forgoing what would be a much smaller carrot than that offered by its predecessors. Either way, the focus on non-MU items made for welcome conversations at the show and plenty of follow-up discussions now that the conference is behind us.
As we move forward into summer, I want to share a few important updates (no pun intended) related to how Iatric Systems will continue to communicate with our customers and partners, starting with our summer webcast series. Each month, we
file:///C|/Users/haidee.leclair/Desktop/June2015.html (2 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
host a number of educational webcasts around key topics such as device integration, patient privacy, connected communities, and more. If you or a co-worker are interested in learning more about these topics, then please check out our webcast schedule included in this edition of Updates!
Finally, we have been proudly publishing our Updates! newsletter for the past 14 years. While I have personally enjoyed the opportunity to share various thoughts, opinions, and news items with our readership, it feels like the right time for a change in format. As as society, we are spending much more time these days engaging with social media and blogs as a primary source for information, which tend to be much more conversational and interactive. So having said all that, this will be the final issue of Updates! In its place will be a new Iatric Systems blog, which can be accessed here. On the blog, you will have the opportunity to subscribe to specific topics such as: HIE & the Connected Community, Medical Device Integration, Interoperability, Meaningful Use, Patient Experience, Patient Privacy, and Report Writing. We want to continue making it easy for our customers and partners to communicate with us and the blog is another positive step in that direction.
I hope you will take advantage of the summer webcasts and the new blog in order to not only hear from us, but more importantly, to let us hear from you!
Summer Webcast Series for MEDITECH Users
Education and Demonstrations
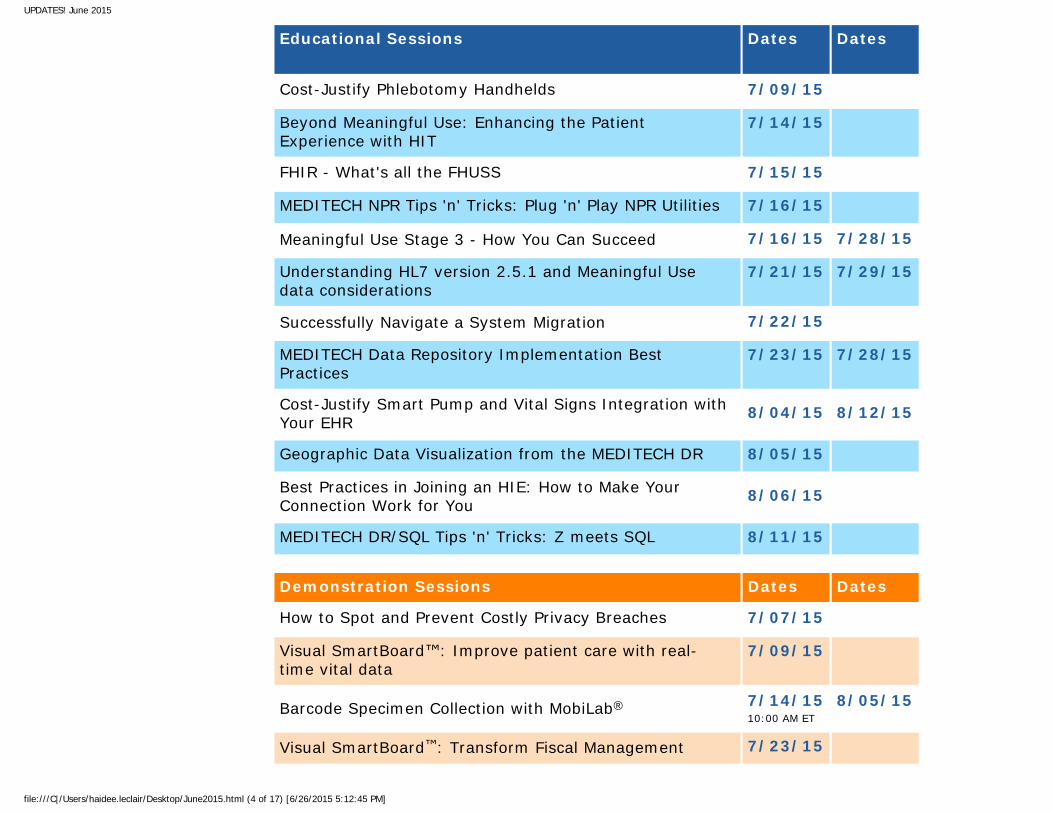
International MUSE 2015 has ended, but the learning goes on. Whether you attended or not, you can expand your knowledge all summer long, simply by registering for the sessions related to your most pressing challenges. Each presents valuable insight on advancing your hospital's capabilities with integrated solutions for MEDITECH.
To register for our FREE webcasts, click on the link under the date column for each of your selections. All webcasts times are at 2:00 p.m. ET unless otherwise noted. We look forward to your participation.
file:///C|/Users/haidee.leclair/Desktop/June2015.html (3 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
Educational Sessions Dates Dates
Cost-Justify Phlebotomy Handhelds 7/09/15
Beyond Meaningful Use: Enhancing the Patient Experience with HIT
7/14/15
FHIR - What's all the FHUSS 7/15/15
MEDITECH NPR Tips 'n' Tricks: Plug 'n' Play NPR Utilities 7/16/15
Meaningful Use Stage 3 - How You Can Succeed 7/16/15 7/28/15
Understanding HL7 version 2.5.1 and Meaningful Use data considerations
7/21/15 7/29/15
Successfully Navigate a System Migration 7/22/15
MEDITECH Data Repository Implementation Best Practices
7/23/15 7/28/15
Cost-Justify Smart Pump and Vital Signs Integration with Your EHR 8/04/15 8/12/15
Geographic Data Visualization from the MEDITECH DR 8/05/15
Best Practices in Joining an HIE: How to Make Your Connection Work for You 8/06/15
MEDITECH DR/SQL Tips 'n' Tricks: Z meets SQL 8/11/15
Demonstration Sessions Dates Dates
How to Spot and Prevent Costly Privacy Breaches 7/07/15
Visual SmartBoard™: Improve patient care with real-time vital data
7/09/15
Barcode Specimen Collection with MobiLab® 7/14/15 10:00 AM ET
8/05/15
Visual SmartBoard™: Transform Fiscal Management 7/23/15
file:///C|/Users/haidee.leclair/Desktop/June2015.html (4 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
Visual SmartBoard™: Transform Your Lab Order Management
8/06/15
Get MEDITECH Data Repository Help with DR Resource Center™
8/18/15 8/26/15
Connect Smart Pumps and Monitors to Your EHR with Accelero Connect®
8/19/15 8/25/15
If you have any questions, please contact Amanda Howell at [email protected] or 978-674-8121.
Iatric Systems Blog
Iatric Systems is now making it even easier for you, a current UPDATES! newsletter subscriber, to get both practical information and interact with your peers on how to solve your biggest healthcare challenges. Topic-specific blog posts replace general newsletters. Instead of our more general info newsletter, you can select the blog post topics of interest and join the conversations about the topics that are important to you:
● HIE & the Connected Community● Interoperability/Integration● Meaningful Use● Medical Device Integration● Patient Experience● Patient Privacy● Report Writing
Check out our new solution-based Website, too. Our newly designed Website is now organized by solution and healthcare topic of interest. This way you can quickly find valuable educational content, stories from your peers, and more.
file:///C|/Users/haidee.leclair/Desktop/June2015.html (5 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
It's never been easier to talk to your peers or to find answers on how to meet your healthcare challenges.
Subscribe to your topics of interest now.
Sepsis Is On The Rise
A recent report from the Centers of Medicare and Medicaid Services named sepsis as the second-most billed diagnosis that hospitals submitted to Medicare - only behind major joint replacements. Sepsis was responsible for a total of about $7.2 billion of Medicare’s payments to hospitals in 2013 — an increase of 9.5% from the prior year.
Dr. Eric Adkins, Assistant Professor of Emergency Medicine at the Ohio State University, believes the sepsis increase is due to higher numbers of at-risk patients, like the elderly, but some of the increase was a result of better diagnoses and coding for the disease. Compared to other diseases, more lives can be saved when sepsis is diagnosed early and treated effectively. It is critical that our arsenal to battle sepsis includes the best technology available.
Our customer and development partner Elk Regional, recently worked with Iatric Systems to develop a new Visual SmartBoard™ for sepsis. This smart board improves patient outcomes by finding the disease in its early stages. Visual SmartBoard (VSB) presents a customized view of multiple patients’ key clinical data on a single screen, including key sepsis indicators. Caregivers can quickly see the specific sepsis related information they need to monitor. VSB provides overall patient scores on three key criteria: Systemic Inflammatory Response, Organ Dysfunction, and Infection. In addition, VSB will provide a total score based on the multiple criteria and rate the patients with the highest severity for immediate treatment.
Please join us for a VSB demonstration on July 9th to see how we are working to identify and catch sepsis early in the process.
file:///C|/Users/haidee.leclair/Desktop/June2015.html (6 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
Compliance Corner Kay Jackson, Education and Advisory Manager
"Right to Be Forgotten…" Does it Apply to Healthcare?
As the U.S. moves to more interoperability and sharing of clinical data, and with all the data breaches happening every day, I’m often left wondering if, and how, patients will care about and trust this new mode of data sharing.
CMS is pushing the sharing of clinical data under Meaningful Use to multiple providers, but are patients and providers really ready for what could be an overload of data?
I’ve heard the concern from many hospitals that providers who receive a CCD under Stage 2 Core 12 often do not want to consume the CCD for fear of overloading their EHR with excess data. For the provider, it becomes a very real concern of trying to reconcile the receipt and consumption of clinical data going forward.
For example, let’s assume I visit my PCP for a knee injury. Pushed to him via CCD are my results from a lab test at the dermatologist two weeks prior. In this example, will that information really provide better healthcare? Does my PCP even have time to look at the CCD? How can he determine quickly and easily what information is of value to my current condition?
The example above leads me to ask: will we become a nation of clinical data overload? I recently read that the European Union privacy panel has called for search engines such as Google to take down links to embarrassing or outdated content throughout the world in what they are calling “right to be forgotten.” Will this law eventually apply to patient information? Will patients push for the right to have outdated clinical information purged from other providers’ EHRs after a few years – or shared with only certain providers?
It is critical for patients to clearly understand their rights about clinical data – including the concepts of being forgotten or never even shared. When a patient signs consent for data sharing, we must ask ourselves if it’s truly clear what data sharing means in this new normal of Meaningful Use. Healthcare owes patients more information and clear guidelines about what is being shared, especially as we move forward with Stage 3 in 2018. We must keep in mind who truly owns the clinical data
file:///C|/Users/haidee.leclair/Desktop/June2015.html (7 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
we’re talking about.
Report Writing Tips
DR+SQL Tip: Testing Code for ICD-10
by Thomas Harlan, Iatric Reporting Services Team
October 1 is coming fast, which means that this year (2015) US healthcare finally gets to join the rest of the world in using the ICD-10 codeset for diagnoses.
MEDITECH is already in reasonable shape for the ICD-10 conversion because their overseas customers have been using ICD-10 for many years. The data structures in the DR, therefore, reflect the proper storage sizes and code-sets.
Where trouble looms its ugly head for a facility, however, is:
● Files going out to a vendor need to be tested and verified for being able to properly send ICD-10 codes.
● Vendors may request dual-coded (ICD-9 and ICD-10) files (or pairs of files for the same account(s).
● Reports or extracts may have hard-coded lists of ICD-9 codes embedded in their logic.
● Select lists on a report may either have hard-coded lists of ICD-9 codes or may pass ICD-9 related parameters that are too small, now that ICD-10 has bigger possible code sizes.
There are more than250 tables in the DR that contain diagnosis codes, or references thereto, but the two primary ones of interest in are…:
livedb.dbo.AbsDrgDiagnoses livedb.dbo.AbsDrgDiagnoses2 – Main dual-coded diagnoses
Plus possibly:
file:///C|/Users/haidee.leclair/Desktop/June2015.html (8 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
livedb.dbo.AbsDrgDataDualCodes – Dual-coded admitting diagnosis codes livedb.dbo.AbsDrgProcedures2 – Dual-coded Procedures
A further complication is added when you need to generate files from your Test ring data, and you likely have a combined LIVE+TEST DR (rather than each database on a separate server as we’d recommend).
Initial Spadework
● Talk to your ICD-10 conversion team (HIM, plus the billing analysts) and get a list of account numbers currently in TEST with ICD-10 coding.
● Also find out if they are dual-coding accounts in LIVE, currently, and get a list of those accounts.
● Find out who on the ICD-10 implementation team can provide you with ICD-10 code equivalencies for ICD-9 codes that are hard-coded in your reports or extracts.
● Identify which reports display or use diagnosis codes.● Using that list of reports, contact either the HIM ICD-10 team or key user
areas (like Performance Improvement or Clinical Decision Support) to see which reports they need to validate against dual-coded accounts.
● Identify which vendor extracts you have in play, and whether they contain diagnosis code information.
● From that list of vendors, collect the latest contact information for their technical representative.
● Reach out to each vendor:�❍ Let them know you are starting to test extracts for ICD-10, including
theirs.�❍ Query them to see if they want an ICD-10 test file and/or a dual-
coding test file.�❍ Get the file naming convention and layout specifications for ICD-10
test files.�❍ Get the file naming convention and layout specifications for dual-
coding test files.● Get to work generating test files and validating reports!
First Pass at Converting ICD-9 to ICD-10
If your HIM/ICD-10 team is overloaded, you might be able to help them by taking a crack at pre-translating the ICD-9 codes to ICD-10 using a utility like:
http://www.icd10data.com/Convertfile:///C|/Users/haidee.leclair/Desktop/June2015.html (9 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
But do not put any codes into production without review and approval of your HIM/ICD-10 team!
Warning about Duplicated Codes
You must be aware that there are some codes in ICD-9 which have near-duplicates in ICD-10 with vastly different meanings. The codes are differentiated by having embedded periods in ICD-10, so it is absolutely necessary to not remove any letters or punctuation from the codes.
http://www.icd10data.com/ICD10CM/Duplicate_Codes
Finding Dual Coded Accounts
Note! If HIM does not have a list of accounts they’ve been dual coding on… you can generate it yourself:
SELECT ABD.AccountNumber FROM livedb.dbo.AbsDrgDiagnoses2 DX2 JOIN livedb.dbo.AbstractData ABD ON ( ABD.AbstractID = DX2.AbstractID AND ABD.SourceID = DX2.SourceID ) GROUP BY ABD.AccountNumber ;
Remember to check TEST as well!
Stored Procedures Using Diagnosis Codes
If you’ve based all of your reports and extracts off of stored procedures (and you did follow that best practice, didn’t you?), you can do a search like this to find stored procedures that use the diagnosis code table:
SELECT OBJECT_NAME(SSM.object_id) AS ObjectName ,SOB.type_desc AS ObjectType FROM sys.sql_modules SSM LEFT JOIN sys.objects SOB ON ( SOB.object_id = SSM.object_id ) WHERE SSM.[definition] LIKE '%AbsDrgDiagnoses%' ;
Testing Reports
Now you’ve got a list of stored procedures and reports to review:
Single-Codingfile:///C|/Users/haidee.leclair/Desktop/June2015.html (10 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
● Review the stored procedure(s) you are using in a given report looking for CAST or CONVERT or LEFT function calls that might wrap around AbsDrgDiagnosis.Diagnosis and reduce it to less than thirty (30) characters.
● Review the stored procedure(s) for hard-coded lists of diagnosis codes. Contact your HIM team to get lists of equivalent ICD-10 codes.
● Remediate the stored procedure(s) as necessary; remembering to add the new ICD-10 codes to any lists. Your users will still be running reports against pre-Oct 1 date ranges, and you don’t want the reports to break unexpectedly.
● In this scenario it is safe to update the stored procedures in LIVE before the October 1 cutover, as you want to ensure the reports are still working with ICD-9 coding.
● With the stored procedure(s) updated, review the reports looking for:�❍ Field formatting that would truncate a diagnosis code field to less
than six (6) characters.�❍ Field formatting that would truncate a diagnosis description to less
than 250 characters.�❍ Check for grouping formulas utilizing lists of ICD-9 codes in the report.�❍ Check for report-level filters utilizing ICD-9 codes in some way. (By
the way, report-level filtering should always be reviewed. Sometimes it is the way to go, but mostly not).
�❍ Watch out for code that would strip off any letters or periods in the ICD-10 code. That is no longer an advisable behavior, as we have noted above.
● Remediate as necessary.● Hand off to your end-users to test.● Rinse and repeat!
Dual-Coding
● This is painful. You need to join to two different tables (AbsDrgDiagnoses and AbsDrgDiagnoses2) and then group the results appropriately.
● Make a new version of your affected stored procedure.● In the code, when you JOIN to the regular table (AbsDrgDiagnoses)
replace that simple JOIN with a derived-table JOIN which looks like this:
LEFT JOIN ( SELECT 'ICD9' AS CodeSet ,ODX.SourceID AS SourceID
file:///C|/Users/haidee.leclair/Desktop/June2015.html (11 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
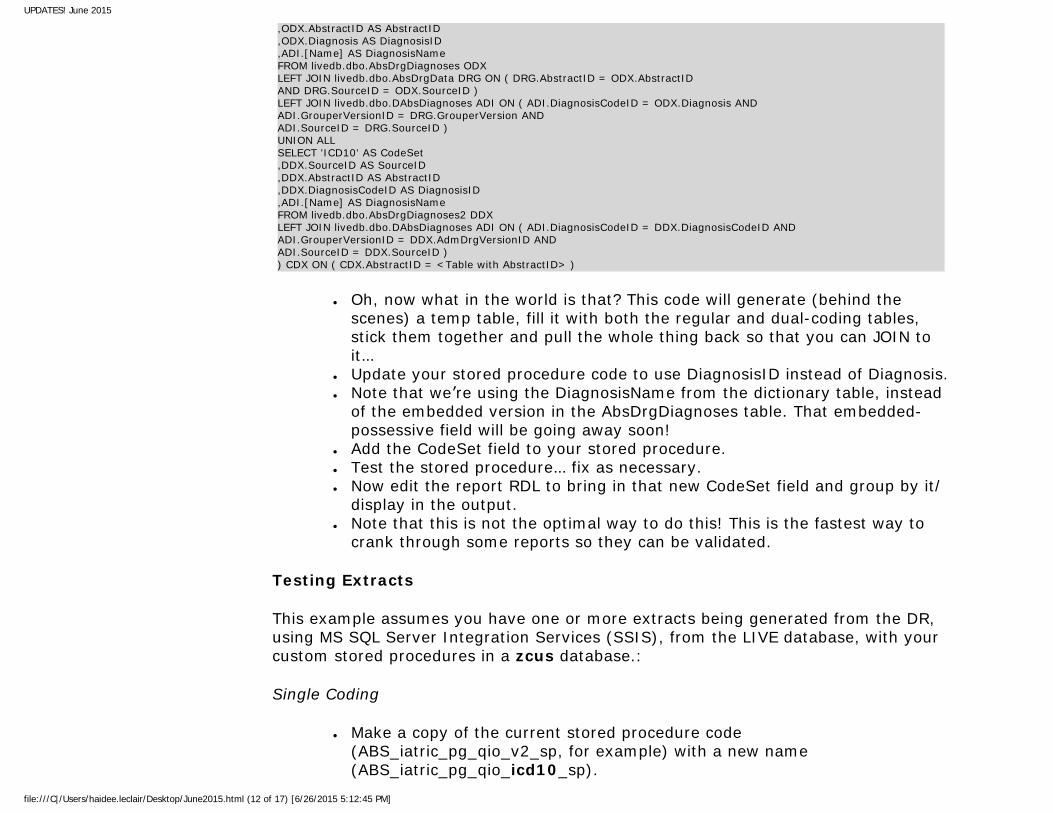
,ODX.AbstractID AS AbstractID ,ODX.Diagnosis AS DiagnosisID ,ADI.[Name] AS DiagnosisName FROM livedb.dbo.AbsDrgDiagnoses ODX LEFT JOIN livedb.dbo.AbsDrgData DRG ON ( DRG.AbstractID = ODX.AbstractID AND DRG.SourceID = ODX.SourceID ) LEFT JOIN livedb.dbo.DAbsDiagnoses ADI ON ( ADI.DiagnosisCodeID = ODX.Diagnosis AND ADI.GrouperVersionID = DRG.GrouperVersion AND ADI.SourceID = DRG.SourceID ) UNION ALL SELECT 'ICD10' AS CodeSet ,DDX.SourceID AS SourceID ,DDX.AbstractID AS AbstractID ,DDX.DiagnosisCodeID AS DiagnosisID ,ADI.[Name] AS DiagnosisName FROM livedb.dbo.AbsDrgDiagnoses2 DDX LEFT JOIN livedb.dbo.DAbsDiagnoses ADI ON ( ADI.DiagnosisCodeID = DDX.DiagnosisCodeID AND ADI.GrouperVersionID = DDX.AdmDrgVersionID AND ADI.SourceID = DDX.SourceID ) ) CDX ON ( CDX.AbstractID = <Table with AbstractID> )
● Oh, now what in the world is that? This code will generate (behind the scenes) a temp table, fill it with both the regular and dual-coding tables, stick them together and pull the whole thing back so that you can JOIN to it…
● Update your stored procedure code to use DiagnosisID instead of Diagnosis.● Note that we’re using the DiagnosisName from the dictionary table, instead
of the embedded version in the AbsDrgDiagnoses table. That embedded-possessive field will be going away soon!
● Add the CodeSet field to your stored procedure.● Test the stored procedure… fix as necessary.● Now edit the report RDL to bring in that new CodeSet field and group by it/
display in the output.● Note that this is not the optimal way to do this! This is the fastest way to
crank through some reports so they can be validated.
Testing Extracts
This example assumes you have one or more extracts being generated from the DR, using MS SQL Server Integration Services (SSIS), from the LIVE database, with your custom stored procedures in a zcus database.:
Single Coding
● Make a copy of the current stored procedure code (ABS_iatric_pg_qio_v2_sp, for example) with a new name (ABS_iatric_pg_qio_icd10_sp).
file:///C|/Users/haidee.leclair/Desktop/June2015.html (12 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
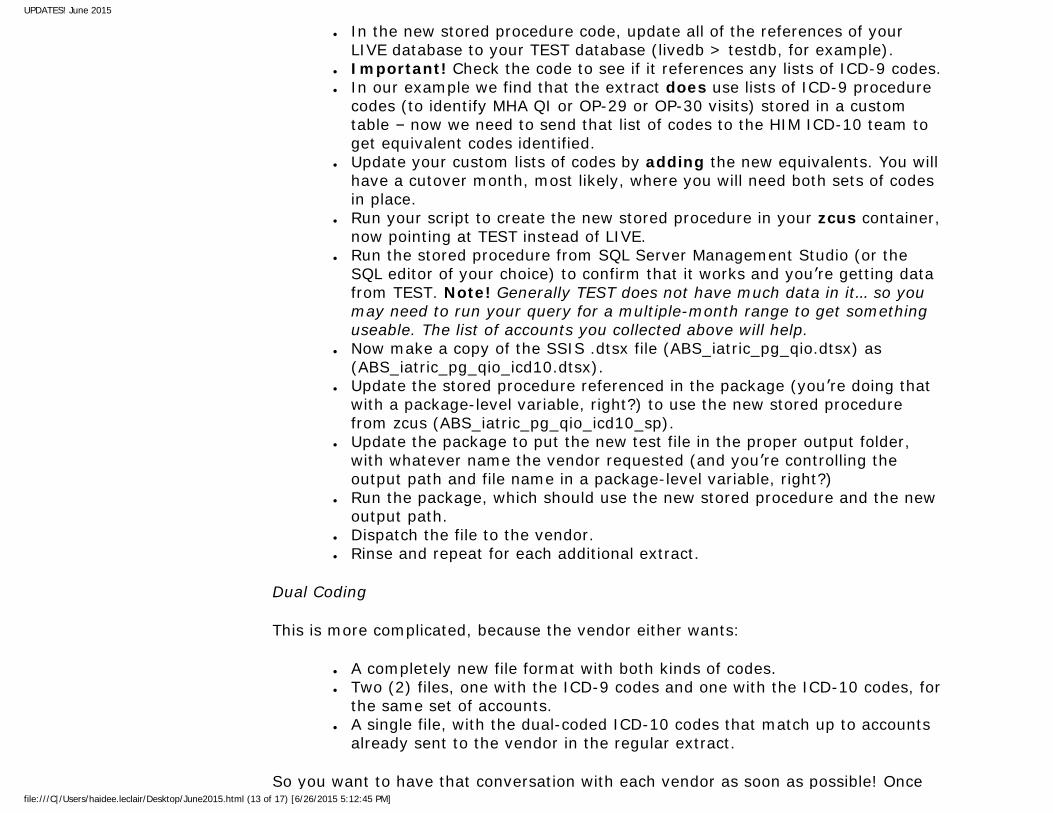
● In the new stored procedure code, update all of the references of your LIVE database to your TEST database (livedb > testdb, for example).
● Important! Check the code to see if it references any lists of ICD-9 codes.● In our example we find that the extract does use lists of ICD-9 procedure
codes (to identify MHA QI or OP-29 or OP-30 visits) stored in a custom table – now we need to send that list of codes to the HIM ICD-10 team to get equivalent codes identified.
● Update your custom lists of codes by adding the new equivalents. You will have a cutover month, most likely, where you will need both sets of codes in place.
● Run your script to create the new stored procedure in your zcus container, now pointing at TEST instead of LIVE.
● Run the stored procedure from SQL Server Management Studio (or the SQL editor of your choice) to confirm that it works and you’re getting data from TEST. Note! Generally TEST does not have much data in it… so you may need to run your query for a multiple-month range to get something useable. The list of accounts you collected above will help.
● Now make a copy of the SSIS .dtsx file (ABS_iatric_pg_qio.dtsx) as (ABS_iatric_pg_qio_icd10.dtsx).
● Update the stored procedure referenced in the package (you’re doing that with a package-level variable, right?) to use the new stored procedure from zcus (ABS_iatric_pg_qio_icd10_sp).
● Update the package to put the new test file in the proper output folder, with whatever name the vendor requested (and you’re controlling the output path and file name in a package-level variable, right?)
● Run the package, which should use the new stored procedure and the new output path.
● Dispatch the file to the vendor.● Rinse and repeat for each additional extract.
Dual Coding
This is more complicated, because the vendor either wants:
● A completely new file format with both kinds of codes.● Two (2) files, one with the ICD-9 codes and one with the ICD-10 codes, for
the same set of accounts.● A single file, with the dual-coded ICD-10 codes that match up to accounts
already sent to the vendor in the regular extract.
So you want to have that conversation with each vendor as soon as possible! Once file:///C|/Users/haidee.leclair/Desktop/June2015.html (13 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
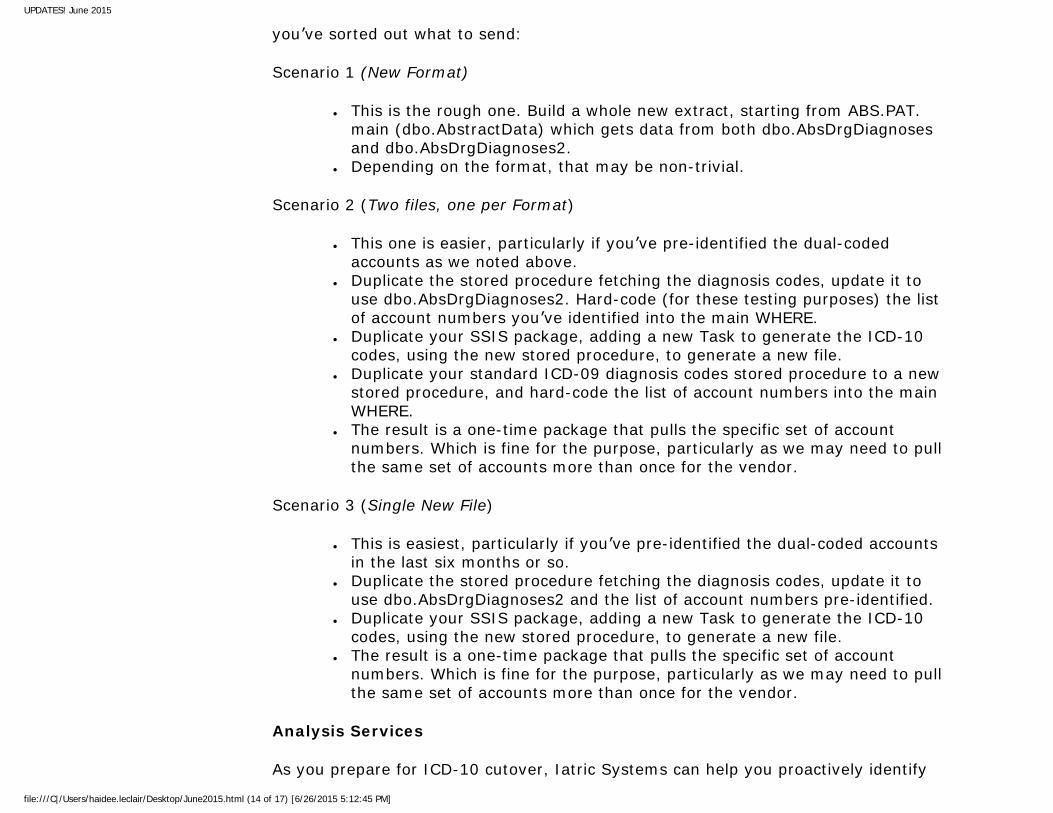
you’ve sorted out what to send:
Scenario 1 (New Format)
● This is the rough one. Build a whole new extract, starting from ABS.PAT.main (dbo.AbstractData) which gets data from both dbo.AbsDrgDiagnoses and dbo.AbsDrgDiagnoses2.
● Depending on the format, that may be non-trivial.
Scenario 2 (Two files, one per Format)
● This one is easier, particularly if you’ve pre-identified the dual-coded accounts as we noted above.
● Duplicate the stored procedure fetching the diagnosis codes, update it to use dbo.AbsDrgDiagnoses2. Hard-code (for these testing purposes) the list of account numbers you’ve identified into the main WHERE.
● Duplicate your SSIS package, adding a new Task to generate the ICD-10 codes, using the new stored procedure, to generate a new file.
● Duplicate your standard ICD-09 diagnosis codes stored procedure to a new stored procedure, and hard-code the list of account numbers into the main WHERE.
● The result is a one-time package that pulls the specific set of account numbers. Which is fine for the purpose, particularly as we may need to pull the same set of accounts more than once for the vendor.
Scenario 3 (Single New File)
● This is easiest, particularly if you’ve pre-identified the dual-coded accounts in the last six months or so.
● Duplicate the stored procedure fetching the diagnosis codes, update it to use dbo.AbsDrgDiagnoses2 and the list of account numbers pre-identified.
● Duplicate your SSIS package, adding a new Task to generate the ICD-10 codes, using the new stored procedure, to generate a new file.
● The result is a one-time package that pulls the specific set of account numbers. Which is fine for the purpose, particularly as we may need to pull the same set of accounts more than once for the vendor.
Analysis Services
As you prepare for ICD-10 cutover, Iatric Systems can help you proactively identify
file:///C|/Users/haidee.leclair/Desktop/June2015.html (14 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
NPR, RD and DR-based reports and extracts that will be impacted. We also offer remediation services to update reports and extracts. For more information, please contact your Iatric Systems Sales representative.
(end)
Visit our report library at http://new.iatric.com/report-library-search.
You can find additional Report Writing Tips on our website, as well as information about our on-site Report Writer Training and Report Writing Services.
Learn about our classes or subscribe for email notifications for new Report Writing classes.
For more information, please contact Karen Roemer at 978.805.3142 or email [email protected].
Follow us on:
Achievements:
2014 Healthcare Informatics
Top 100
2014 Best Places to Work in Healthcare IT
Inc. 5000
Sign-up/Contact Us
Subscribe to our new blog at http://new.iatric.com/blog-home, or update your subscriptions at http://pages.iatric.com/blog-subscription-page.
You can unsubscribe from this newsletter using the SafeUnsubscribe link at the bottom of this email or by sending us a request at [email protected].
If you received this newsletter via email, you may give us feedback by simply replying to the email. However, if you would like to reach someone directly, please feel free to contact one of the individuals listed below. Joel Berman, CEO, [email protected], 978.805.4101 John Danahey, Executive Vice President of Customer Services, [email protected], 978.805.4153
Upcoming Eventsfile:///C|/Users/haidee.leclair/Desktop/June2015.html (15 of 17) [6/26/2015 5:12:45 PM]
UPDATES! June 2015
THT Healthcare Governance Conference Austin, Texas July 30, 2015 - August 1, 2015
NCHICA 2015 Annual Conference Pinehurst, North Carolina September 13-16, 2015
InSight 2015 Nashville, Tennessee September 15-18, 2015
CIOhealth - Boston Boston, Massachusetts September 24, 2015
MPACT Summit 2015 Boston, Massachusetts September 25, 2015
AEHIX15 Fall Forum Orlando, Florida October 7-9, 2015
Healthland Connect 2015 Minneapolis, Minnesota October 26-29, 2015
Hospital and Healthcare IT Reverse Expo Fall 2015 Los Angeles, California October 5-7, 2015
CHIME LEAD Forum Atlanta, Georgia December 1, 2015
Privacy & Security Forum 2015 Boston, Massachusetts
file:///C|/Users/haidee.leclair/Desktop/June2015.html (16 of 17) [6/26/2015 5:12:45 PM]

UPDATES! June 2015
December 1-3, 2015
27 Great Pond Drive, Boxford, MA 01921, USA - 978.805.4100
Copyright 1996-2015 Iatric Systems, Inc. -All Rights Reserved-
file:///C|/Users/haidee.leclair/Desktop/June2015.html (17 of 17) [6/26/2015 5:12:45 PM]