sodium and the renin-angiotensin system in essential hypertension and mineralocorticoid excess
TRANSCRIPT

308
SODIUM AND THE RENIN-ANGIOTENSIN
SYSTEM IN ESSENTIAL HYPERTENSION
AND MINERALOCORTICOID EXCESS
M. LEBEL
J. J. BROWND. KREMER
J. I. S. ROBERTSC
M. A. SCHALEKAMPD. L. DAVIESA. F. LEVER
)N M. TREE
D. G. BEEVERSR. FRASER
J. J. MORTONA. WILSON
Medical Research Council Blood Pressure Unit, andDepartment of Medicine, Western Infirmary,
Glasgow G11 6NT
Summary Exchangeable sodium (NaE) was in-creased in untreated primary hyper-
aldosteronism but normal in treated primary hyper-aldosteronism and in untreated essential hypertension,low-renin hypertension, and hypertension with excess11-deoxycorticosterone (DOC). The relation betweenNaE and plasma-renin was normal in essential hyper-tension and primary hyperaldosteronism but subnormalin low-renin hypertension and DOC excess. Depres-sion of renin in low-renin hypertension cannot there-fore be attributed to abnormal sodium retention.
Introduction -
BECAUSE an abnormal relation between sodiumstatus and the renin-angiotensin system probably con-tributes to the rise of blood-pressure in renal andmalignant-phase hypertension,I we have tried to relateexchangeable sodium (NaE) to plasma levels of reninand angiotensin 11 in four other forms of hypertension:essential and low-renin hypertension and two types ofmineralocorticoid excess. Low-renin hypertensionwas of particular interest because the depression ofrenin has been attributed to abnormal sodium reten-tion (see Discussion). Data on plasma volume andextracellular-fluid volume in low-renin hypertensionand essential hypertension are given elsewhere.2
Patients and Methods
MethodsNaE was measured and expressed as previously.
Methods used to determine the plasma concentrations ofrenin,5 angiotensin 11,6 aldosterone,7 and 11-deoxycorti-costerone (DOC) 8 have been described. Blood-sampleswere taken between 8 and 9 A.M. with the patient inbed having fasted and lain recumbent overnight. Reninand angiotensin 11 were assayed in samples taken on themorning of NaE measurement.
Patients were either untreated or had had treatmentwithdrawn (hypotensive agents for 1 week, diuretics,spironolactone and potassium supplements for 4 weeks,and oral contraceptives for 3 months). 82 of 99 measure-ments of NaE were made with the patient on a fixed
dietary intake of sodium (135 meq. per day) and potassium(60 meq. per day). The remaining seventeen patients werestudied on a normal ward diet. The study was repeatedduring control of blood-pressure by spironolactone (fifteenpatients) or after adrenal surgery (eleven patients).
Patients
Seventy-three hypertensive patients (forty-eight female),aged 16 to 64, were studied. All had a diastolic pressuregreater than 95 mm. Hg in the outpatient department whenuntreated. Patients with essential hypertension and low-renin hypertension showed no clinical, radiological, or
biochemical features of aortic coarctation, Cushing’s syn-
drome, renal hypertension, or phseochromocytoma. Intra-venous urography was normal and blood-urea below 45 mg.per 100 ml. in each case.
Primary hyperaldosteronism was diagnosed in twenty-one patients as previously" All underwent adrenalsurgery; nineteen had an adrenocortical adenoma and twohad bilateral adrenocortical hyperplasia.
Seven patients had increased plasma levels of DOC.Details in five of these have been published.11
Essential hypertension was diagnosed in thirty-threepatients by exclusion (see above). Plasma levels of renin,aldosterone, and potassium were persistently normal ineach case.
Low-renin hypertension was arbitrarily distinguishedfrom essential hypertension (see Discussion) in twelve
patients. While untreated, each had a mean plasma-reninbelow 6 units per litre (normal 4-20) and at least onesubnormal plasma-renin. Hypokalsemia not due to treat-ment was present in four cases (mean potassium valuesof 2-4, 3’2, 3’4, and 3’6 meq. per litre). Plasma levelsof Doc and aldosterone were normal in all patients.
Results
NaE was increased in untreated primary hyperaldos-teronism (t=4-559, P<0.001) but normal in all other
groups (fig. 1). No difference emerged when malesand females were analysed separately. In contrast tothe situation in renal and malignant hypertension,1plasma-renin was either normal or reduced whenrelated to concurrent NaE (fig. 2); in primary hyper-aldosteronism NaE was increased and plasma-renindepressed to a level comparable with that in normoten-sive subjects having similar expansion of NaE (fig. 2);treatment with spironolactone or surgery’ reducedNaE and raised plasma-renin, but the relation betweenthe two remained close to the normotensive mean
1° HYPERALDOSTERONISM
Fig. 1—NaE in controls and patients with four types of hyper-tension.
Details of the controls and the method of expressing NaE aregiven in Davies et al.4 Expressed in the same way, mean NaEfor normal subjects was 99-9% of our mean control value in thestudy of Crane et al.15 and 95-5% of our mean in the study ofHollander et al.40 Amongst cases of primary hyperaldosteron-ism, 0 represents those with, and . those without, adreno-cortical adenoma.
309
Fig. 2-Relation between NaE and plasma-renin.
A and / = Primary hyperaldosteronism before (&Dgr;) and after(/, ) treatment by spironolactone or surgery. =Essential hypertension.[]=Low-renin hypertension.0 =DOC excess.
Bars represent 1 S.E.M. and parallel lines show mean 2 S.D.of data for normotensive subjects. 4
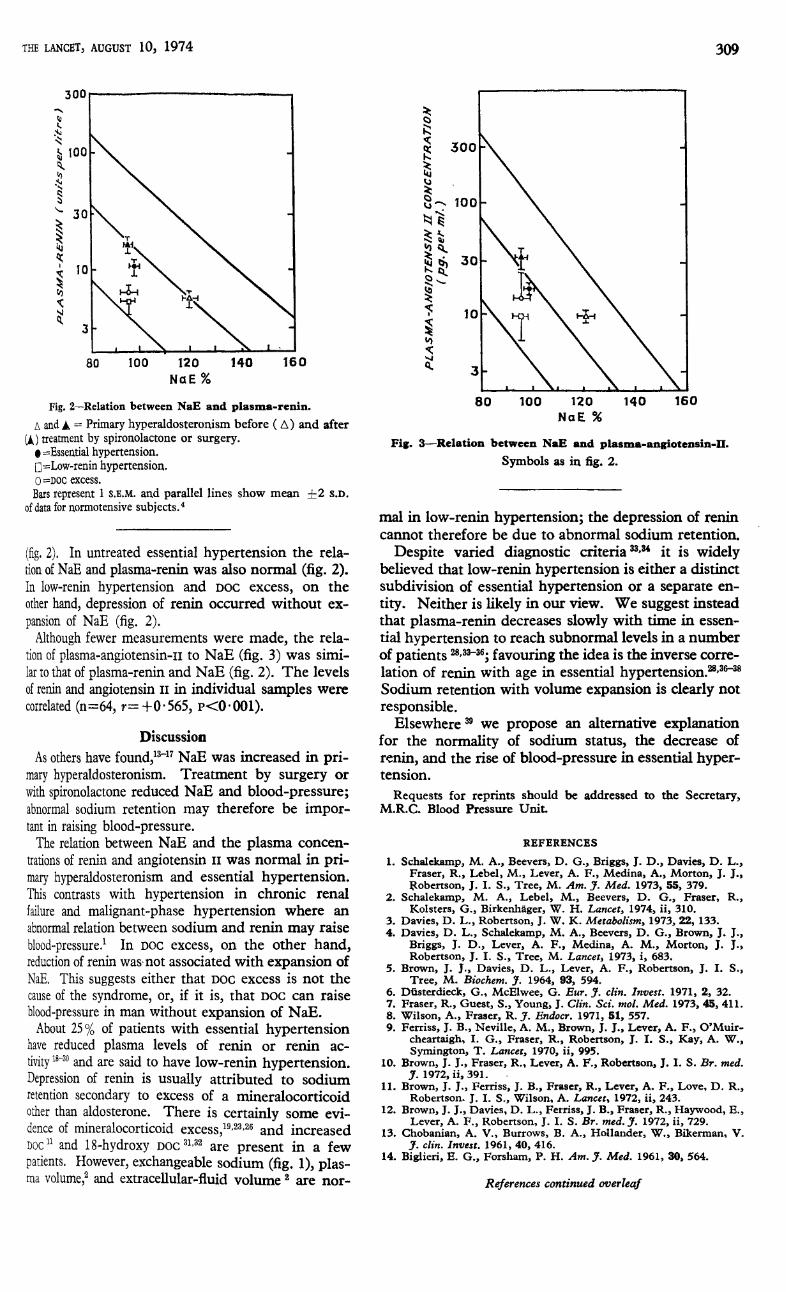
(fig. 2). In untreated essential hypertension the rela-tion of NaE and plasma-renin was also normal (fig. 2).In low-renin hypertension and Doc excess, on the
. other hand, depression of renin occurred without ex-pansion of NaE (fig. 2).Although fewer measurements were made, the rela-
tion of plasma-angiotensin-n to NaE (fig. 3) was simi-lar to that of plasma-renin and NaE (fig. 2). The levelsof renin and angiotensin 11 in individual samples werecorrelated (n=64, r= - 0 565, P<0.001).
’
Discussion
As others have found,"" NaE was increased in pri-. mary hyperaldosteronism. Treatment by surgery or
with spironolactone reduced NaE and blood-pressure;, abnormal sodium retention may therefore be impor-
, tant in raising blood-pressure.. The relation between NaE and the plasma concen-
trations of renin and angiotensin 11 was normal in pri-- mary hyperaldosteronism and essential hypertension.
This contrasts with hypertension in chronic renal° failure and malignant-phase hypertension where an
abnormal relation between sodium and renin may raise
blood-pressure 1 In Doc excess, on the other hand,reduction of renin was not associated with expansion ofNaE. This suggests either that DOC excess is not thecause of the syndrome, or, if it is, that DOC can raiseblood-pressure in man without expansion of NaE.About 25% of patients with essential hypertension
have reduced plasma levels of renin or renin ac-
tivity 18-30 and are said to have low-renin hypertension.’’ Depression of renin is usually attributed to sodium
, retention secondary to excess of a mineralocorticoid
,; other than aldosterone. There is certainly some evi-: dence of mineralocorticoid excess,19, 23, 26 and increased
DOC 11 and 18-hydroxy DOC31, 32 are present in a fewpatients. However, exchangeable sodium (fig. 1), plas-ma volume,’ and extracellular-fluid volume are nor-
Fig. 3-Relation between NaE and plasma-angiotensin-H.
Symbols as in fig. 2.
mal in low-renin hypertension; the depression of renincannot therefore be due to abnormal sodium retention.Despite varied diagnostic criteria 33, 34 it is widely
believed that low-renin hypertension is either a distinctsubdivision of essential hypertension or a separate en-tity. Neither is likely in our view. We suggest insteadthat plasma-renin decreases slowly with time in essen-tial hypertension to reach subnormal levels in a numberof patients 28, 33-36; favouring the idea is the inverse corre-lation of renin with age in essential hypertension.28, 36-38Sodium retention with volume expansion is clearly notresponsible.Elsewhere39 we propose an alternative explanation
for the normality of sodium status, the decrease ofrenin, and the rise of blood-pressure in essential hyper-tension.
Requests for reprints should be addressed to the Secretary,M.R.C. Blood Pressure Unit.
REFERENCES
1. Schalekamp, M. A., Beevers, D. G., Briggs, J. D., Davies, D. L.,Fraser, R., Lebel, M., Lever, A. F., Medina, A., Morton, J. J.,Robertson, J. I. S., Tree, M. Am. J. Med. 1973, 55, 379.
2. Schalekamp, M. A., Lebel, M., Beevers, D. G., Fraser, R.,Kolsters, G., Birkenhäger, W. H. Lancet, 1974, ii, 310.
3. Davies, D. L., Robertson, J. W. K. Metabolism, 1973, 22, 133.4. Davies, D. L., Schalekamp, M. A., Beevers, D. G., Brown, J. J.,
Briggs, J. D., Lever, A. F., Medina, A. M., Morton, J. J.,Robertson, J. I. S., Tree, M. Lancet, 1973, i, 683.
5. Brown, J. J., Davies, D. L., Lever, A. F., Robertson, J. I. S.,Tree, M. Biochem. J. 1964, 93, 594.
6. Düsterdieck, G., McElwee, G. Eur. J. clin. Invest. 1971, 2, 32.7. Fraser, R., Guest, S., Young, J. Clin. Sci. mol. Med. 1973, 45, 411.8. Wilson, A., Fraser, R. J. Endocr. 1971, 51, 557.9. Ferriss, J. B., Neville, A. M., Brown, J. J., Lever, A. F., O’Muir-
cheartaigh, I. G., Fraser, R., Robertson, J. I. S., Kay, A. W.,Symington, T. Lancet, 1970, ii, 995.
10. Brown, J. J., Fraser, R., Lever, A. F., Robertson, J. I. S. Br. med.J. 1972, ii, 391.
11. Brown, J. J., Ferriss, J. B., Fraser, R., Lever, A. F., Love, D. R.,Robertson. J. I. S., Wilson, A. Lancet, 1972, ii, 243.
12. Brown, J. J., Davies, D. L., Ferriss, J. B., Fraser, R., Haywood, E.,Lever, A. F., Robertson, J. I. S. Br. med. J. 1972, ii, 729.
13. Chobanian, A. V., Burrows, B. A., Hollander, W., Bikerman, V.J. clin. Invest. 1961, 40, 416.
14. Biglieri, E. G., Forsham, P. H. Am. J. Med. 1961, 30, 564.

310
15. Crane, M. G., Harris, J. J., Holloway, J. E. J. Lab. clin. Med. 1963,61, 51.
16. Brown, J. J., Davies, D. L., Lever, A. F., Peart, W. S., Robertson,J. I. S. J. Endocr. 1965, 33, 279.
17. Novak, L. P., Strong, C. G., Hunt, J. C. in Hypertension ’72(edited by J. Genest and E. Koiw); p. 444. Berlin, 1972.
18. Helmer, O. M., Judson, W. E. Circulation, 1968, 38, 965.19. Woods, J. W., Liddle, G. W., Stant, E. G., Michelakis, A. M.,
Brill, A. B. Archs intern. Med. 1969, 123, 366.20. Channick, B. J., Adlin, V., Marks, A. D. ibid. 1969, 123, 131.21. Jose, A., Crout, R., Kaplan, N. M. Ann. intern. Med. 1970, 72, 9.22. Gunnells, J. C., McGuffin, W. L., Robinson, R. R. ibid. 1970, 72,
901.23. Spark, R. F., Melby, J. C. ibid. 1971, 75, 831.24. Crane, M. G., Harris, J. J., Johns, V. J. Am. J. Med. 1972, 52, 457.25. Dustan, H. P., Bravo, E. L., Tarazi, R. C. Am. J. Cardiol. 1973,
31, 606. 26. Carey, R. M., Douglas, J. G., Schweikert, J. R., Liddle, G. W.
Archs intern. Med. 1972, 130, 849.27. Brunner, H. R., Sealey, J. E., Laragh, J. H. Circulation Res. 1973,
32, suppl. 1, 99.28. Schalekamp, M. A. D. H., Schalekamp-Kuyken, M. P. A.,
Birkenhäger, W. H. Clin. Sci. 1970, 38, 101.29. Jerums, G., Doyle, A. E. ibid. 1969, 37, 79.30. Coghlan, J. P., Doyle, A. E., Jerums, G., Scoggins, B. A. ibid. 1972,
42, 15.31. Melby, J. C., Dale, S. L., Grekin, R. J., Gaunt, R., Wilson, T. E.
Rec. Progr. Hormone Res. 1972, 28, 287.32. Genest, J., Nowaczynski, W., Kuchel, O., Sasaki, C. in Hypertension
’72 (edited by J. Genest and E. Koiw); p. 293. Berlin, 1972.33. Kaplan, N. M. Clinical Hypertension. New York, 1973.34. Dunn, M. J., Tannen, R. L. Kidney Int. 1974, 5, 317.35. Ledingham, J. M. Practitioner, 1971, 207, 5.36. Tuck, M., Williams, C. H., Cain, J. P., Sullivan, J. M., Dluhy, R. G
Am. J. Cardiol. 1973, 32, 637.37. Schalekamp, M. A. D. H., Kolsters, G., Birkenhäger, W. H.
Lever, A. F. in Hypertension (edited by A. Distler and H. PWolff) (in the press).
38. Klaus, D., Klumpp, F., Zehner, J. Therapie Woche, 1973, 45, 424339. Brown, J. J., Lever, A. F., Robertson, J. I. S., Schalekamp, M. A
Lancet, 1974, ii, 320.40. Hollander, W., Chobanian, A. V., Burrows, B. A., Bikerman, V.
J. clin. Invest. 1961, 40, 408.
BODY-FLUID VOLUME IN LOW-RENIN
HYPERTENSION
M. A. SCHALEKAMPD. G. BEEVERSG. KOLSTERS
M. LEBELR. FRASER
W. H. BIRKENHÄGER
Department of Internal Medicine, Zuiderziekenhuis,Rotterdam, Netherlands, and Medical Research Council
Blood Pressure Unit, Western Infirmary, Glasgow
Summary Plasma and extracellular-fluid volumeswere normal in thirty-eight patients
with normal-renin hypertension and in seventeen
patients with low-renin hypertension, there being nodifference between the two groups. This stronglysuggests that reduction of renin in low-renin hyper-tension is not brought about by sodium retention withvolume expansion.
Introduction
PLASMA-RENIN levels are subnormal or unresponsiveto stimuli in about 25% of patients with essentialhypertension, the group being classified as low-reninhypertension. Because sodium retention with expan-sion of body-fluid volume can raise blood-pressureand suppress renin 5-8 it is widely suspected thatvolume expansion is important in low-renin hyperten-sion.3,9-14We present here data on plasma and extracellular-
fluid (E.C.F.) volumes in controls and in hypertensivepatients with normal and low plasma-renin concentra-tions. Measurements of exchangeable sodium (NaE)in similar groups of patients are reported elsewhere 15
Patients, Controls, and MethodsMethods
Plasma levels of renin16 and aldosterone 17 were measuredas described previously. Aldosterone secretion was deter-mined by isotope dilution with thin-layer 18 and ’ Celite ’ 19chromatography of the urinary extract. Blood-sampleswere taken as in the NaE study.l5 Measurements of
plasma and E.C.F. volume were made between 9 A.M. andnoon using techniques described elsewhere.20,21
Patients and Controls
Diagnostic criteria for essential hypertension were as
in other studies.15, 16, 20 All hypotensive drugs were stopped3 weeks before the study; no patient had received oral
contraceptives or reserpine. The control group comprisednormal individuals (six) and patients with healing fractures(four) or uncomplicated peptic ulcer (thirty). Controlsand hypertensive patients were admitted to hospital andstudied after 5-7 days on a fixed sodium intake of 50 meq.per day. Low-renin hypertension was arbitrarily diagnosedby a subnormal plasma-renin on at least three occasionsand a rise of plasma-renin after head-up tilting to 45
°
for 1 hour which was less than 1 ng. per ml. per hour(2-8 in ten normal subjects). Plasma-renin was normalin all other hypertensive patients, normal-renin hyper-tension being diagnosed.
Results
Despite the striking difference of plasma-renin,plasma-aldosterone concentration, aldosterone secre-
tion, plasma volume, and E.c.F volume were very simi-lar in controls and in the two groups of hypertensivepatients (see figure and table). Reference of plasmaand E.C.F. volume to body weight, height, and surfacearea revealed no differences, nor was there a differ-ence when males and females were considered separ-ately (see figure). Referral of the Glasgow data onNaE 15 to the same indices of body build showed nosignificant difference between low and normal reninhypertension; mean NaE for the former being respec-tively 8, 5, and 4% lower when related to weight,height, and surface area.
Controls N.R.H. L.R.H. Controls N.R.H. L.R.H.Plasma and E.C.F. volume in controls and in patients with
normal-renin or low-renin hypertension.Mean values are indicated by the horizontal bars. Measurements in
females (o) and in males (•).