neonatal nephrology in a hurry · iugr, preterm, lbw, pre-eclampsia, gestational diabetes yearly to...
TRANSCRIPT

Neonatal nephrology in a hurry
Dr Shuman Haq
Consultant Paediatric Nephrologist
Southampton Children’s Hospital

28 weeks g
estatio
n
30 weeks g
estatio
n
34 weeks g
estatio
n
40 weeks g
estatio
n
57%
5%
23%16%
Most nephrons form by..
A. 28 weeks gestation
B. 30 weeks gestation
C. 34 weeks gestation
D. 40 weeks gestation
10 days a
fter b
irth
20 days a
fter b
irth
30 days a
fter b
irth
40 days a
fter b
irth.
12%
38%36%
14%
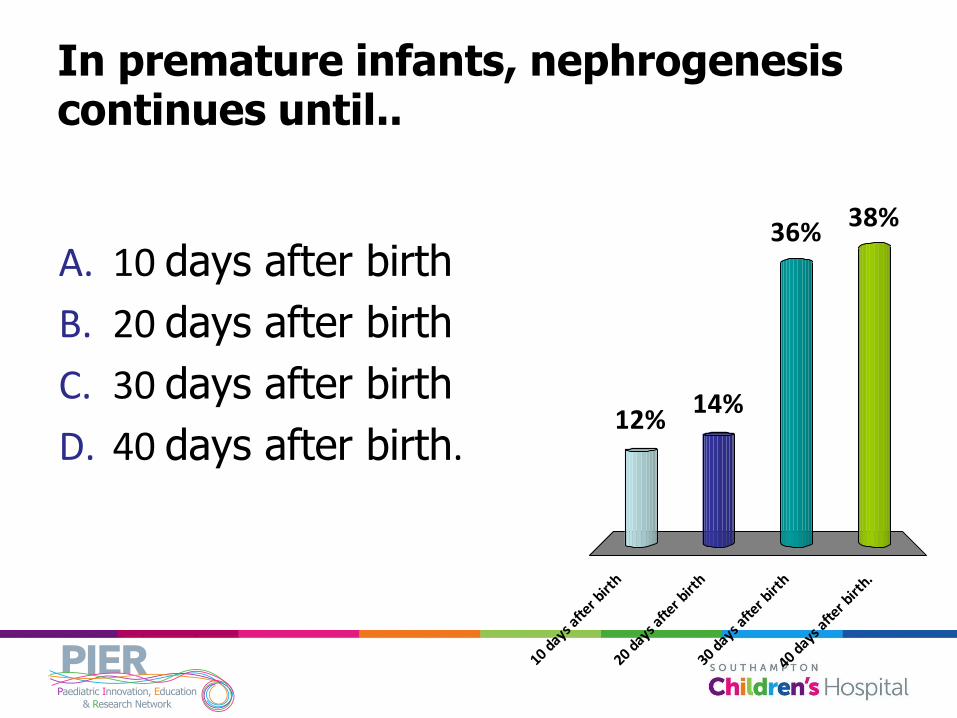
In premature infants, nephrogenesis continues until..
A. 10 days after birth
B. 20 days after birth
C. 30 days after birth
D. 40 days after birth.

10 20 30 40
10%
30%33%
28%
What is the glomerular filtration rate (GFR) at birth in a term infant?
A. 10
B. 20
C. 30
D. 40

20 30 40 50
2%
39%
44%
15%
What is the GFR 4 weeks after term delivery?
A. 20
B. 30
C. 40
D. 50
Intra
uterin
e gro
wth
reta
...
Poor mate
rnal d
iet d
urin...
Antenata
l glu
coco
rtico
ids
Two o
f the above
All of t
he above
7%2%
73%
16%
2%
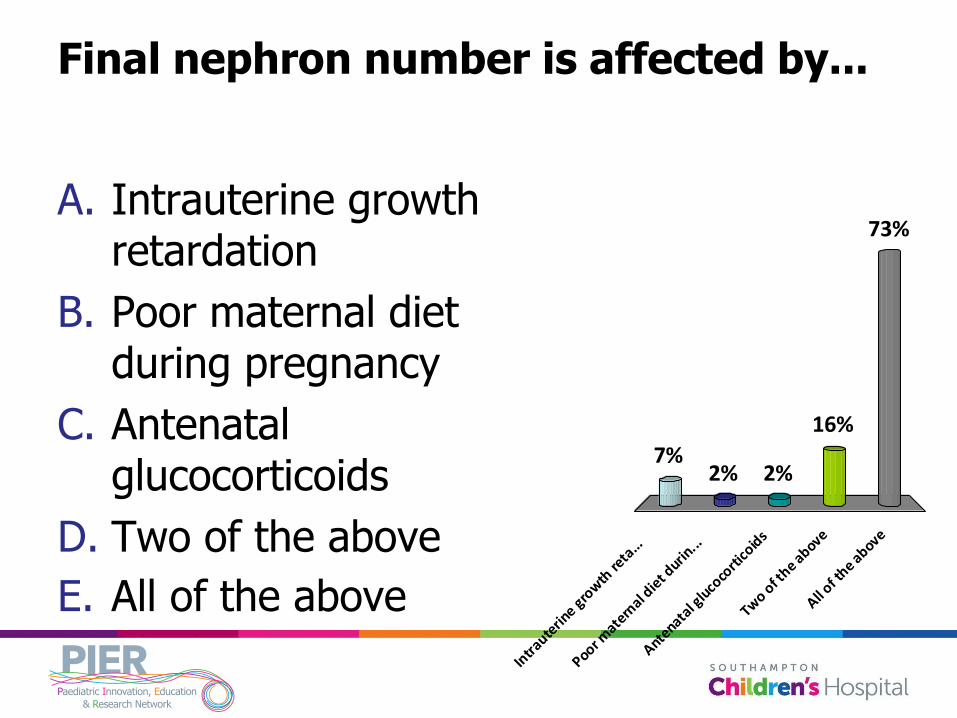
Final nephron number is affected by...
A. Intrauterine growth retardation
B. Poor maternal diet during pregnancy
C. Antenatal glucocorticoids
D. Two of the above
E. All of the above

Neonates and their kidneys
Children are not just small adults
Neonates are not just small children

Neonates and their kidneys
What happens in utero?
What happens after birth?
Why are their kidneys so vulnerable?
Foetal and infant origins of adult disease

Embryology
Nephrogenesis – starts at 5 weeks, complete by 34 weeks
Glomerular development - 9 weeks
Nephron number 750,000 per kidney (250,000 to 1,900,000)
If low Hypertension
Heart disease
Renal impairment

Renal function in utero
Placenta
Equilibration of plasma creatinine from 20 weeks gestation
Fetal urine 10 weeks
2-5 ml/hr at 22 weeks
25-40 ml/hr at term
Majority of amniotic fluid
Immediate postnatal period 1-3 ml/hr

Oligohydramnios
Renal causes
Renal agenesis
Urinary tract obstruction
Potter facies
Polyhydramnios
Renal causes
Diabetes insipidus
Bartter’s syndrome

Renal function in newborn
‘Deficient’ glomerular and tubular function
Adequate function to deal with normal physiological burden
Limited adaptive response to stress

Renal function in the newborn
Renal blood flow
Glomerular filtration rate
Fluid homeostasis
Acid-base balance

Renal blood flow
15-20% of cardiac output v 25% in adult
Mostly directed to juxtamedullary nephrons most mature sodium and water conservation
High renal vascular resistance
Blood flow distribution changes in days Favours outer cortical nephrons

Glomerular filtration rate
Birth Low systemic BP
High vascular resistance
Limited filtration surface
Low GFR
Rise in GFR over first 4 weeks

Neonatal fluid homeostasis
Birth TBW 75%, ECF 40%
Within days TBW , ECF , ICF
9 months TBW 62%, ECF 27%, ICF 35%
Neonatal fluid homeostasis
Term infants lose 5-10% body weight
ECF
Leaky capillaries

Urine concentrating ability
Low capacity
Dangers of water depletion
Maturation: 1-2 months

Premature infant
(28-30 weeks)
Term infant
3 days 3 days 2 weeks
Urine output
(ml/kg/hr)
0.6 – 3.1 1.0 – 3.1 1.0 - 5
Maximal urine osmolality
(mOsm/Kg H2O)
400-500 500-600 540-700
GFR
(ml/min/1.73 m2)
10 20 40

Acid-base balance
Extracellular and intracelluar buffers
From birth
Respiratory adaptation
From birth
Respiratory function
Neurology
Renal adaptation
Limited

Acid-base balance
Renal threshold for bicarbonate
Premature infants: 14 mmol/l
Term infant: 18-20 mmol/l
12 months adulthood: 24-26 mmol/l

Acid-base balance
Aggravated by
Asphyxia
Sepsis
Volume depletion
Drugs

Presentation of renal disease
Antenatal evaluation
Postnatal evaluation
Antenatal evaluation
Congenital abnormalities of the kidneys and urinary tract (CAKUT)
Liquor volume
Postnatal evaluation Eye abnormalities
Ear abnormalities
Branchial fistulae and cysts
Potter facies
Heart failure
Deficiency of abdominal musculature and cryptorchidism
Deformities of lumbar and sacral spine
Other skeletal anomalies
Imperforate anus
Bladder extrophy
Genital abnormalities
Oedema

Postnatal evaluation: urine output
Newborn oliguria <0.5ml/kg/hr
Polyuria >4ml/kg/hr
Urinary stream

Bedside postnatal evaluation
Proteinuria
Physiological
Vascular disorders
Congenital nephrotic syndrome
Infections
Nephrotoxins
Acute tubular necrosis
Bedside postnatal evaluation
Haematuria
Bleeding diathesis
Vascular disorders
Cystic diseases
Tumours
Trauma
Nephritis

Postnatal evaluation: lab tests
Creatinine
Gestational age
Body length
Body weight
Increases transiently in VLBW infants
Cystatin C

Congenital renal disease
CAKUT
Congenital nephrotic syndrome
Bartters’ syndrome
Nephrogenic diabetes insipidus

Acute kidney injury
Antenatal vascular damage
Maternal drugs
Twins
Primary renal and urological diseases
CAKUT
Congenital nephrotic syndrome
Acquired postnatal diseases
All the dangers of the neonatal unit!

Pre-renal acute kidney injury
Gastrointestinal losses
Haemorrhage
Sudden compartmental fluid shifts
Favourable prognosis

Intrinsic acute kidney injury
Acute vascular events
Renal venous thrombosis, renal artery stenosis
Acute interstitial nephritis
Congenital nephrotic syndrome
Poorest prognosis
Post-renal acute kidney injury
Urinary tract obstruction
Prognosis variable

Lab results in AKI
Dip the urine!
Proteinuria
Haematuria

Lab results in AKI
Pre-renal AKI Intrinsic AKI
Urine osmo > 400mosm/kg H2O Urine osmo < 400mosm/kg H2O
Urine Na < 40 mmol/l Urine Na > 40mmol/l
Urine/Plasma Osmolality >1.3 Urine/Plasma Osmolality <1.0
FeNa <2% FeNA >3.0%

The future for these children?
Low birth weight and pre-term birth linked with reduced nephron number
Proteinuria
Hypertension
Renal impairment
But who’s watching?

Neonates and their kidneys
Unique vulnerabilities
Effects on nephron mass
Who do we follow up?
How do we follow up?

An example of how seriously some take this...

Birth weight and nephron number working group
IUGR, Preterm, LBW, pre-eclampsia, gestational diabetes
Yearly to 2 yearly BP and urinalysis from 3 yr old
<32/40, VLBW, AKI
Screen from before 1 yr old
AKI, hypertension, proteinuria, cardiovascular disease, CAKUT, obesity, diabetes
Renal profile and urinary protein every 2 years
Baseline renal ultrasound scan
From 18 yrs old
BP, BMI, Urinalysis – every 2 yrs until 40 yrs old, yearly thereafter

Birth weight and nephron number working group
Education about lifestyle and avoidance of nephrotoxins
Avoid rapid catch-up growth to prevent obesity associated exacerbation of renal risk
Caution in potential living kidney donors