molecular aspects of hpv in relation to cervical cancer
TRANSCRIPT

Molecular aspects
of HPV in relation to
cervical cancer,
epidemiology and
vaccines Roland Sahli, Institute of Microbiology, CHUV, University of Lausanne
WHO HPV Reference Laboratory for Europe
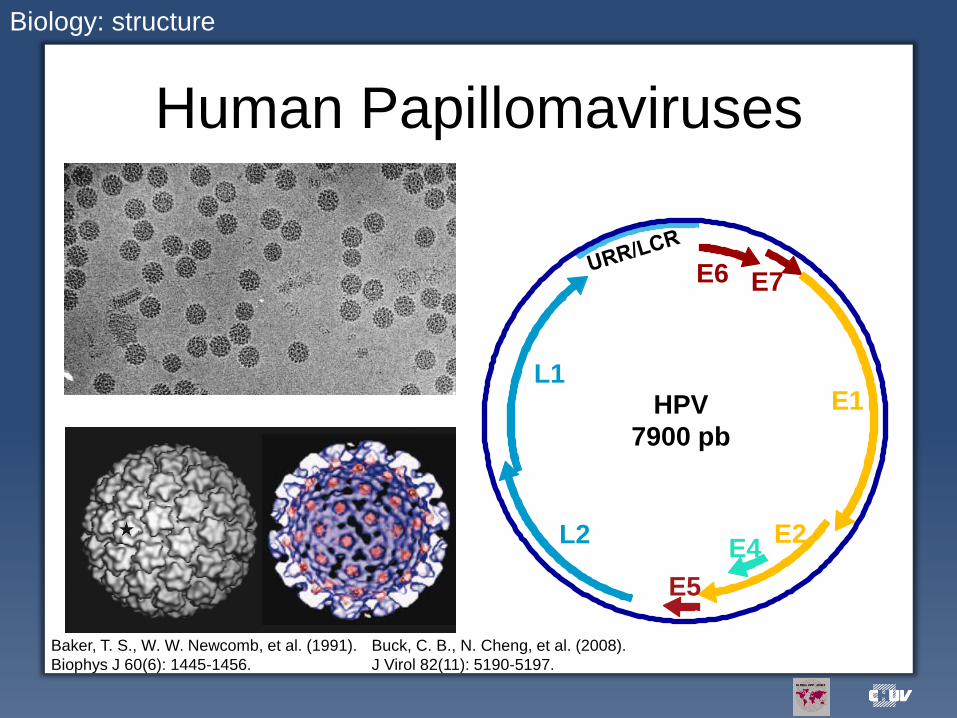
Human Papillomaviruses
Biology: structure
HPV
7900 pb
E1
E2 E4
L2
L1
E5
E6 E7
Buck, C. B., N. Cheng, et al. (2008).
J Virol 82(11): 5190-5197.
Baker, T. S., W. W. Newcomb, et al. (1991).
Biophys J 60(6): 1445-1456.

Epitheliotropic viruses
• High genetic diversity (< 90% nucleotide sequence homology: distinct genotype)
– Genotype ≡ Serotype (important for prophylactic vaccine design)
• Highly specific
– Toward the host (slow co-evolution over millions of years)
• Reptiles, birds, mammals
– Toward the infected tissue (cutaneous, mucosal)
• Cutaneous: HPV-1, -2, -4, …
• Mucosal: HPV-6, -11, -16, -18, ….
• Induce cell proliferation
– Benign tumors (warts, laryngeal papillomas, condyloma): productive cycle
of all HPV
– Cancerous tumors (cervical cancer, oro-pharyngeal cancers): non
productive virus-host cell interaction associated more frequently with
infection by High Risk (HR) HPV
• The site and mode of production hide the virus from the host defense
– Viral persistence
Biology: HPV main characteristics

More than 150 HPV genotypes
Source: IARC
Biology: HPV genetic diversity
A9: HPV-16 group
A7: HPV-18 group
70% of cervical cancer cases are due to HPV-16 and -18
Certain genotypes are oncogenic

HPV genotypes according to their prevalence in cancer vs. normal cases
Biology: HPV genotype and oncogenic risk
Combes, J. D., P. Guan, et al. (2015). Int J Cancer. 136(3): 740-742
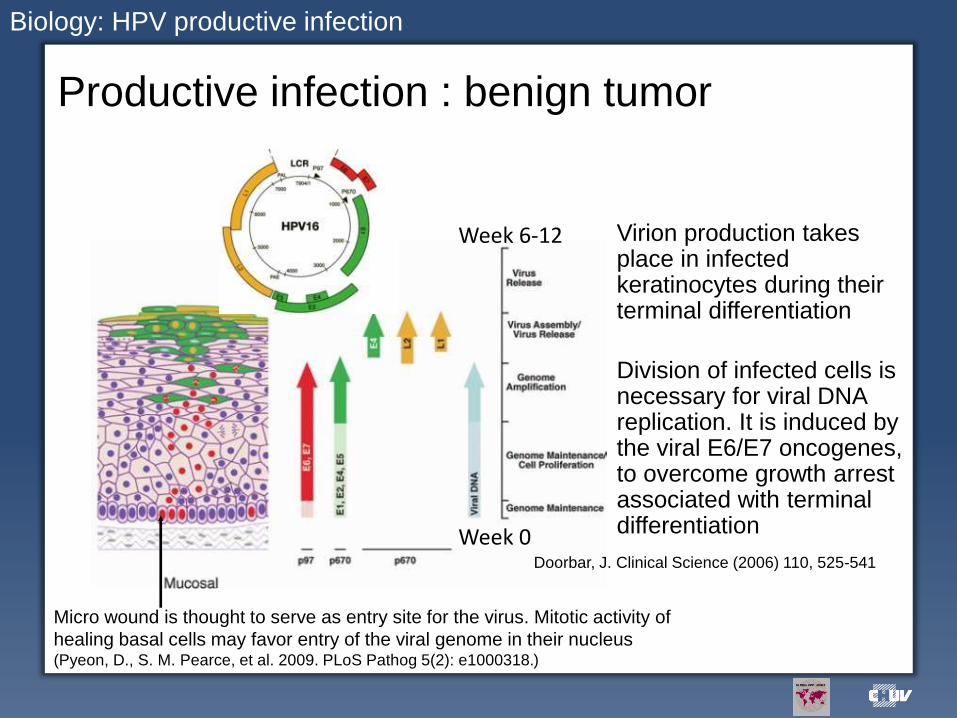
Productive infection : benign tumor
Micro wound is thought to serve as entry site for the virus. Mitotic activity of
healing basal cells may favor entry of the viral genome in their nucleus (Pyeon, D., S. M. Pearce, et al. 2009. PLoS Pathog 5(2): e1000318.)
Week 6-12
Week 0
Biology: HPV productive infection
Virion production takes place in infected keratinocytes during their terminal differentiation
Division of infected cells is necessary for viral DNA replication. It is induced by the viral E6/E7 oncogenes, to overcome growth arrest associated with terminal differentiation
Doorbar, J. Clinical Science (2006) 110, 525-541

The viral DNA is integrated into the chromosomes
of malignant tumor cells: dead end for the virus
Maintenance and continuous expression of E6/E7 is mandatory for tumor cell growth:
natural selection of cells with integrated viral DNA
Carcinogenesis: non productive interaction between HPV and its host cell
Principles of virology, 2nd edition

Cancer cell survival depends on the continuous
expression of the viral oncogenes E6/E7
J. Doorbar, Clinical Science (2006) 110, 525-541
H e L a c e lls (H P V 1 8 E 6 /E 7 )
0 .5 1 .0 1 .5 2 .0 2 .5 3 .0
-2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
M O I (lo g 1 0 ) : A d E 2 e x p re s s in g H P V 1 6 E 2 (in h ib ito r o f E 6 /E 7 ) o r A d e G F P c o n tro l
Ce
ll s
urv
iva
l
R. Sahli, unpublished
Carcinogenesis: histologic progression and viral oncogene expression

Mechanism of cellular
transformation
Carcinogenesis: regulatory pathways in response to viral oncogene expression
Doorbar, J., N. Egawa, et al. (2015). Rev Med Virol 25 Suppl 1: 2-23.
•HR HPV differ from LR HPV by their ability to efficiently promote cell immortalization and telomerase activation, as well as by promoting the degradation of pRb and p53. •Many interactions between the E6 and E7 proteins with their respective cellular partners can differentiate LR HPV and HR HPV with regard to cell transformation.

The HPV life cycle is virtually hidden
from the immune system
• Cycle within the
epithelium
• Virions are released
from dead cells during
desquamation
• Neither cytolysis nor
necrosis
– Weak to no inflammation
• Favors viral persistence
– Risk of genetic alterations
Stanley, M. A. (2012). Clin Microbiol Rev 25(2): 215-222. Stanley, M. (2008). Gynecol Oncol 109(2 Suppl): S15-21.
Biology: the immune response against HPV is in a defavourable context

Cervical cancer is a rare outcome of a persistent infection
(>15 ans) by a high risk genotype
Adapted from Syrjänen and Syrjänen: Papillomavirus infections in human pathology. Wiley & Sons, Chichester; 2000.p. 143-165
CIN = cervical intraepithelial neoplasia; HPV = Human PapillomaVirus; HSIL = high grade squamous intraepithelial neoplasia
LSIL = low grade squamous intraepithelial neoplasia.
>99 % high
risk HPV
1-2 y-----------------------------------10 y and + (cancer 15-20 y)
Initial
HPV
infection
CIN 1, LSIL CIN 2/3, HSIL Cancer
~20% high
risk HPV
< 0.5-1% of the
initial infections Persistent Infections
90% HPV infections
are cleared within 2 y
Cervical cancer screening: natural history of HPV infection
Virological aspects of cervical
cancer prevention Prior to infection
Neutralisation of infection through prophylactic vaccination
Bivalent (Cervarix: 16, 18) or quadrivalent (Gardasil: 6,11,16, 18)
vaccines are available (potential: 70% of cases)
Nonavalent vaccine (Gardasil 9: 6,11,16,18, 31, 33, 45, 52, 58) will soon
be available (potential: 80-90% of cases)
Post infection
Identification of "at risk" patients
High risk HPV detection as an adjunct to cytology
High risk HPV detection can be used for primary screening under
specific conditions
Treatment of tumors via therapeutic vaccines
Prevention of cervical cancer: role of virology

PRIOR TO INFECTION
PROPHYLACTIC VACCINES

Exposed loops at the surface of L1
pentamers display genotype- and
conformation-specific neutralizing epitopes
Bishop, B., J. Dasgupta, et al. (2007). J Biol Chem 282(43): 31803-31811.
HPV16
HPV11
HPV18
HPV35
Immunodominant neutralizing Ab generated by L1 VLPs are:
type-specific not cross-neutralizing
Highly homologous L1 VLPs share cross-neutralisation epitopes which are less immunogenic than the type-specific ones Stanley et al. 2006. Vaccine 24S3 106-113
Prophylactic vaccine: neutralisation epitopes

Only limited cross-protection is observed
from L1 VLPs
Chen, X. S., R. L. Garcea, et al. (2000). Mol Cell 5(3): 557-567.
Highly variable positions are seen on the surface of the VLPs in extended loops
Neutralization epitopes are positioned in genotype-specific areas, and HPV variant selection may be driven by escape from neutralization by the host Limited cross-protection is favourable for HPVs in terms of evolution/selection
Prophylactic vaccine: cross neutralisation

Improved vaccine formulation Gardasil-9: HPV vaccine formulation (6, 11, 16, 18, 31, 33, 45, 52, 58)
http://clinicaltrials.gov/show/NCT00543543 Joura, E. A., A. R. Giuliano, et al. (2015). N Engl J Med 372(8): 711-723.
Prophylactic vaccine: Gardasil-9

POST INFECTION
The effect of vaccination on cervical cancer burden will not be seen
for decades

The majority of HPV infections are clinically irrelevant, and
their rate vary with the age of the patients
Cervical cancer screening using HPV tests: context
Schiffman MH. Epidemiology of cervical human papillomaviruses. In: zur Hausen H,
ed. Human pathogenic papillomaviruses. Heidelberg: Springer-Verlag, 1994
•HPV can be detected in a cytologically normal context (transient infections) •HPV positive results without clinical relevance is particularly high in patients aged less than 30 •HPV testing is highly sensitive but poorly specific •Positive predictive value can be improved by taking persistence in consideration

Characteristics and use of HPV tests
HPV tests
•HPV molecular tests •High analytical sensitivity
•High negative predictive value
•Low positive predictive value
•(Semi-) Quantitative HPV tests may be
easier to adapt for primary screening
(threshold of detection) •Against clinical endpoint (≥CIN2)
•Against HCII
•Patients > 30 years old Meijer, C.J. et al. (2009). Int J Cancer 124: 516-520
•HPV genotyping assays
•Treatment follow up, triage of ASC-US
•Epidemiology •Sensitivity: LOD 50 (HPV16/18)-500 ge
•Specificity: > 97%
Snijders et al., J Pathol 2003; 201: 1–6.
A. The viral load is associated with the grade of the disease
B. Persistence is associated with a
higher relative risk of HSIL Schlecht et al., JAMA 2001; 286: 3106
C. As un adjunct to pathology
D. Vaccine evaluation requires
genotyping

HPV testing for primary screening
• DNA assays
– Hybrid capture (HCII): gold std, targets the whole genome
– Cobas taqman HPV (ROCHE), RealTime High-risk HPV (ABBOTT)
• HPV16/HPV18 + (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, [66], [68])
• Validated against HCII: performances non inferior to HCII
• Distinguish HPV16 and 18 from the other HR genotypes
• Cannot evaluate persistence of other HR HPV
– Seegene Anyplex II HR assay
• HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, [66], [68]
• Can evaluate persistence
• Under clinical validation (Prof. Meijer's laboratory)
• RNA assays
– Aptima (Hologic)
• HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, [66], [68]
Biased selection of HPV assays

Hybrid capture assay (HC2)
HPV screening: signal amplification
Commercial assay (Qiagen/Digene), standardized, approved for
clinical use
Group-specific (13 HR HPV)
Sensitivity and specificity depend on the threshold of detection
(pg/ml): sensitivity (1 pg/ml) > 97%
Cross reactions with several LR types: clinical specificity may be
suboptimal
Cannot assess persistence of a specific genotype
Reference test against which new assays can be validated
Hybridization in solution

PCR
Measurement of the amplicons after the last cycle (classical PCR): qualitative Measurement of the amplicons at each synthesis step with fluorescent probes (Real time PCR): quantitative
RealTime High Risk HPV test (Abbott )
16/18, HR
Cobas 4800 HPV test (Roche)
16/18, HR
HPV screening: target amplification
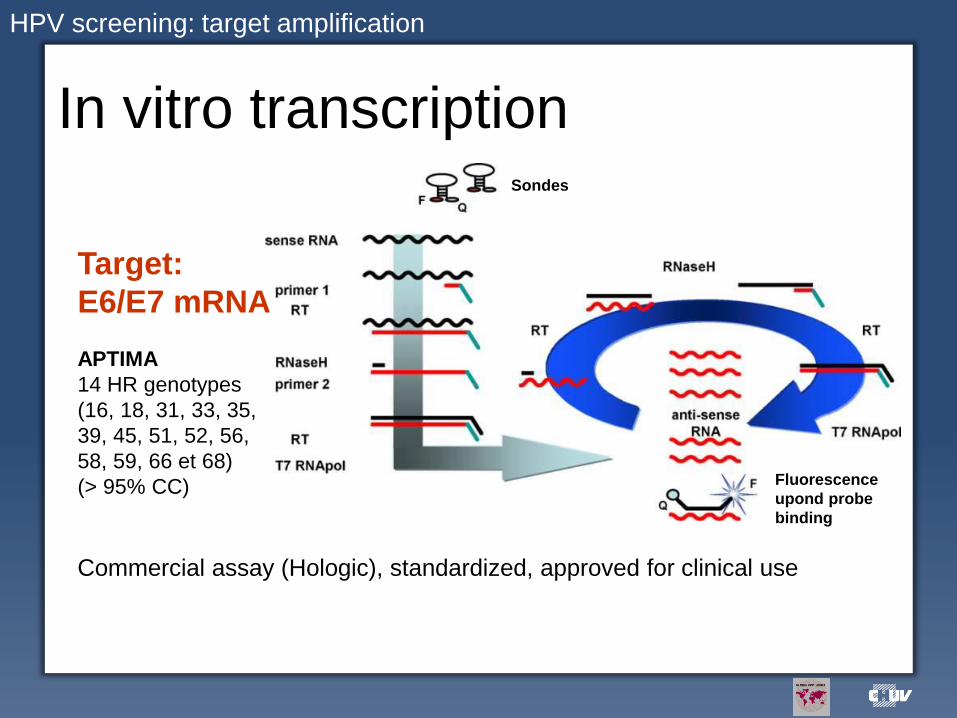
In vitro transcription
Target:
E6/E7 mRNA
APTIMA
14 HR genotypes
(16, 18, 31, 33, 35,
39, 45, 51, 52, 56,
58, 59, 66 et 68)
(> 95% CC)
Commercial assay (Hologic), standardized, approved for clinical use
Sondes
Fluorescence
upond probe
binding
HPV screening: target amplification
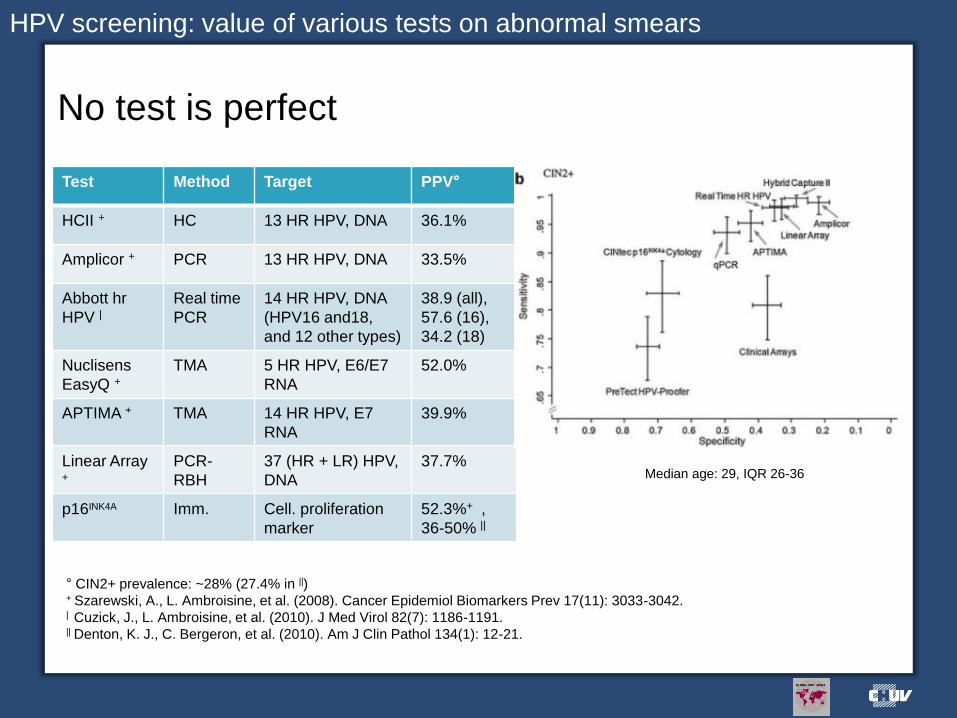
No test is perfect
° CIN2+ prevalence: ~28% (27.4% in ||) + Szarewski, A., L. Ambroisine, et al. (2008). Cancer Epidemiol Biomarkers Prev 17(11): 3033-3042. | Cuzick, J., L. Ambroisine, et al. (2010). J Med Virol 82(7): 1186-1191. || Denton, K. J., C. Bergeron, et al. (2010). Am J Clin Pathol 134(1): 12-21.
Test Method Target PPV°
HCII + HC 13 HR HPV, DNA 36.1%
Amplicor + PCR 13 HR HPV, DNA 33.5%
Abbott hr
HPV | Real time
PCR
14 HR HPV, DNA
(HPV16 and18,
and 12 other types)
38.9 (all),
57.6 (16),
34.2 (18)
Nuclisens
EasyQ +
TMA 5 HR HPV, E6/E7
RNA
52.0%
APTIMA + TMA 14 HR HPV, E7
RNA
39.9%
Linear Array +
PCR-
RBH
37 (HR + LR) HPV,
DNA
37.7%
p16INK4A Imm. Cell. proliferation
marker
52.3%+ ,
36-50% ||
Median age: 29, IQR 26-36
HPV screening: value of various tests on abnormal smears

Genotyping assays
• Can be used as an adjunct to validated assays
• Persistence evaluation
• Treatment follow up
• Research tool
• INNO-LiPA, Linear Array, PGMY-CHUV and other in-
house assays
• Seegene Anyplex HPV28
HPV assays

L1 target
1 50 100 150 200 250 300 350 400 450
Similarity
SPF: Inno Lipa
GP5+/6+ : Multimetrix
PGMY: Linear Array (LA), PGMY-CHUV
HPV
P97
E1
E2 E4 L2
L1
E5
E6 E7
PGMY11 PGMY09
The sequence of the MY amplicon predicts the genotype determined by whole genome analysis
PGMY-CHUV: preferably with DNA from cervical smears and unfixed biopsy samples Se: LOD95 10 gen-eq (>98% vs LA) Sp: 100% (vs sequencing) SPF and GP5+/6+: valid for FFPE samples Se similar to PGMY-CHUV Sp SPF < PGMY-CHUV (proficency panels)
HPV screening: genotyping

PGMY-CHUV
HPV
P97
E1
E2 E4 L2
L1
E5
E6 E7
PGMY11
PGMY09
+
HLA PCR/gel
hyb
ridizatio
n
Genotypes
Acc
ess
D
atab
ase
Parallel array of type-specific probes
Detection
Used as an adjunct to cytology; Genotype-specific: persistence
LOD: 5-50 IU (HPV16/18), 50-500 ge (others); Probe specificity = 100%;
Low cost method transferred through WHO to ref. lab. worldwide Estrade, C., P. A. Menoud, et al. (2011). J Clin Microbiol 49(10): 3474-3481.
Estrade, C. and R. Sahli (2014). J Clin Microbiol 52(11): 4033-4035.
HPV genotyping: in house test
5 PGMY11 13 PGMY09 1RSMY09 2 HLA primers AmpliTaq Gold 1.5 or 3 mM MgCl2

Seegene Anyplex HPV28 assay
HPV genotyping: Real time PCR
28 genotypes can be identified in only 2 reactions!
Used as an adjunct to cytology; Genotype-specific: persistence
LOD: 5-50 IU (HR HPV); Probe specificity = 100%

HPV genotyping: assay validation
Comparison of the Seegene H28 assay
to the PGMY-CHUV assay
Estrade, C. and R. Sahli (2014). J Clin Microbiol 52(2): 607-612.

Analysis of discordant samples
Multiple infections status is associated with discordance for HPV42 Lower viral load is associated with discordance except for HPV51 and HPV68
Comparison of Seegene HPV28 assay to PGMY-CHUV
Estrade, C. and R. Sahli (2014). J Clin Microbiol 52(2): 607-612.

Comparison of Seegene HPV28 assay to PGMY-CHUV
HPV51 discordants
DNA sequencing performed by Seegene on our HPV51 discordants revealed mismatches with the Seegene HPV28 assay primers and probe A new version was thus implemented (RUO-HPV51 kit) and compared to HPV28 kit using PGMY-CHUV as a reference
Significant improvement of HPV51 detection by RUO-HPV51 compared with HPV28 kit (p<0.004 by 2 tailed McNemar's test)

HPV68 discordants
Comparison of Seegene HPV28 assay to PGMY-CHUV
The PGMY primers are known to miss a subtype of HPV68 (HPV68a) Inefficient priming thus occurs. However HPV68a at high viral load can be detected by the PGMY-primers DNA sequencing of a rare HPV68a amplicon identified the PGMY09_L primer as the closest HPV68a compatible primer RSPGMY09_L was thus designed and added to the PGMY primer cocktail

HPV genotyping: validation of PGMY-CHUV version 2
Correction of the HPV68a defect in
PGMY-CHUV version 2
Estrade, C. and R. Sahli (2014). J Clin Microbiol 52(11): 4033-4035.

Future of cervical cancer screening
• Combine high specificity of cytology with high sensitivity of HPV testing
– Screening interval
– Improvement of cytology in the vaccine era • Cytology will be more difficult to interpret because the
disease prevalence will diminish (low PPV)
• Take advantage of identifying persistent vs. transient infections
• How to target the 50% cancer cases from women who do not consult?
Way to improve cervical cancer screening?

Acknowledgements
• Christine Estrade
• Joakim Dillner
• Elizabeth Unger

Low cross protection confered by the first
generation vaccines against non-vaccine
HPV types in HPV-naive women
Van de Velde, N., M. C. Boily, et al. (2012). J Natl Cancer Inst. 104(22): 1712-1723.
In addition, the time-dependent lower cross-protection observed in studies Patricia (4 years), HPV-007 (6 years) and HPV-023 (9 years) suggests waning of cross-protection.
Prophylactic vaccine: cross protection

La VPN des test HPV est très élevée –
Probabilité très faible de lésions à 5 ans
Apport des tests HPV: augmentation de l’intervalle de temps entre visites
P[CIN3+ à 5 ans] si les deux types de tests sont positifs: 33%!
P[CIN3+ à 5 ans] si le test HPV est positif: 8%!
P[CIN3+ à 5 ans] si le test cytologique est positif: 3%
P[CIN3+ à 5 ans] si les deux types de tests sont négatifs: < 0.2%
P[CIN3+ à 5 ans] si le test HPV est négatif: < 0.3%
P[CIN3+ à 5 ans] si le test cytologique est négatif: 0.8%
Test HPV: capture d’hybride (HCII) ou PCR (GP5+/6+)
Dillner, J., M. Rebolj, et al. (2008). "Long term predictive values of
cytology and human papillomavirus testing in cervical cancer
screening: joint European cohort study. BMJ 337: a1754.

Cytologie et génotypage pourraient être combinés
sans augmentation exagérée du nombre de tests
Naucler, P., W. Ryd, et al. (2009). Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in
primary cervical cancer screening. J Natl Cancer Inst 101(2): 88-99.
Triage organisé (Suède) pour femmes de 34-38 ans; Test HPV validé pour tri
primaire et capable de génotypage; Persistance à > 1 an; Thin Prep facilite la
gestion des échantillons
Apport des tests HPV: amélioration de l’efficience par le génotypage

Cytology vs. HPV
Primary screening
Mayrand, M. H. et al. (2007). N Engl J Med 357(16): 1579-1588. Patientes de plus de 30 ans
•Superior sensitivity of HPV test
•Superior specificity of PAP
•Neither method is perfect (see low PPV)

HPV triage improves protection
against cervical cancer
Ronco, G., J. Dillner, et al. (2014). Lancet 383(9916): 524-532.
This reflects the vey high sensitivity of HPV testing
“HPV-based screening provides 60-70% greater protection against invasive cervical carcinomas
compared with cytology. Data of large-scale randomised trials support initiation of HPV-based
screening from age 30 years and extension of screening intervals to at least 5 years.”
HPV triage vs. cytology

Long-term prediction of impact of bivalent,
quadrivalent and nonavalent HPV vaccines
Van de Velde, N., M. C. Boily, et al. (2012). "Population-Level Impact of the Bivalent, Quadrivalent, and Nonavalent Human Papillomavirus Vaccines: A Model-Based Analysis." J Natl Cancer Inst. Published online 27.10.2012
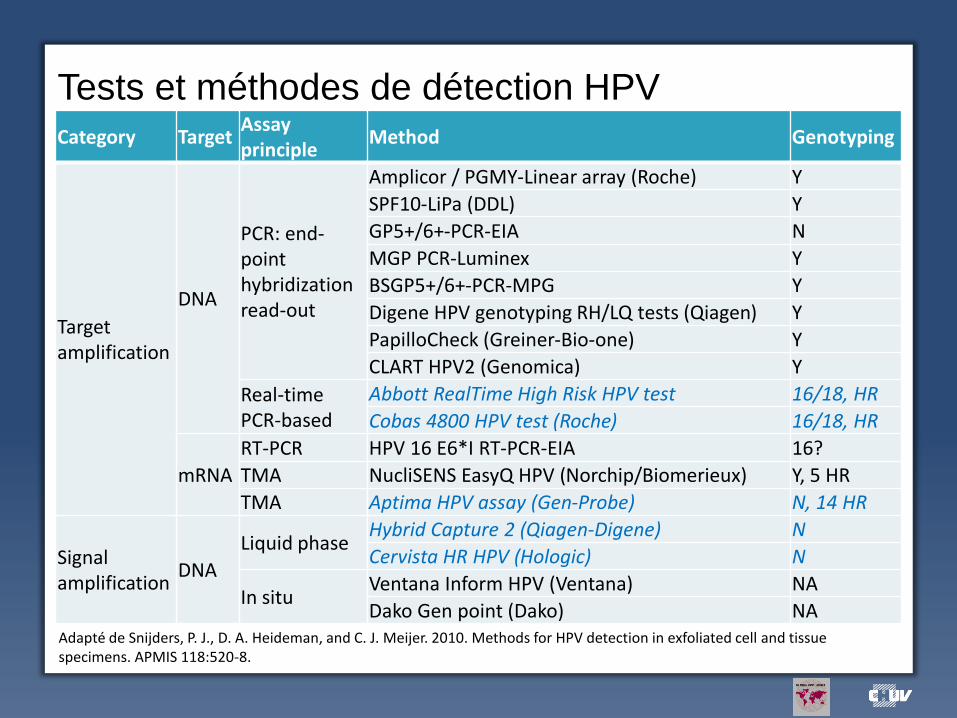
Tests et méthodes de détection HPV
Category Target Assay principle
Method Genotyping
Target amplification
DNA
PCR: end-point hybridization read-out
Amplicor / PGMY-Linear array (Roche) Y
SPF10-LiPa (DDL) Y
GP5+/6+-PCR-EIA N
MGP PCR-Luminex Y
BSGP5+/6+-PCR-MPG Y
Digene HPV genotyping RH/LQ tests (Qiagen) Y
PapilloCheck (Greiner-Bio-one) Y
CLART HPV2 (Genomica) Y
Real-time PCR-based
Abbott RealTime High Risk HPV test 16/18, HR
Cobas 4800 HPV test (Roche) 16/18, HR
mRNA
RT-PCR HPV 16 E6*I RT-PCR-EIA 16?
TMA NucliSENS EasyQ HPV (Norchip/Biomerieux) Y, 5 HR
TMA Aptima HPV assay (Gen-Probe) N, 14 HR
Signal amplification
DNA
Liquid phase Hybrid Capture 2 (Qiagen-Digene) N
Cervista HR HPV (Hologic) N
In situ Ventana Inform HPV (Ventana) NA
Dako Gen point (Dako) NA Adapté de Snijders, P. J., D. A. Heideman, and C. J. Meijer. 2010. Methods for HPV detection in exfoliated cell and tissue specimens. APMIS 118:520-8.

Caractéristiques cliniques de tests
HPV bien étudiés (CIN2+)
Test Sensibilité Spécificité VPP
HCII 99.6% 28.4% 36.1%
Amplicor 98.9% 21.5% 33.5%
PreTect 73.6% 73.1% 52.0%
APTIMA 95.2% 42.2% 39.9%
Linear Array 98.2% 32.8% 37.7%
Population: patientes avec cytologie anormale, prévalence de CIN2+ par
conséquent supérieure à celle d’une population en tri primaire
Szarewski, A., L. Ambroisine, et al. (2008). "Comparison of predictors for high-grade cervical
intraepithelial neoplasia in women with abnormal smears." Cancer Epidemiol Biomarkers Prev 17(11):
3033-3042.

Meta-analyse des données comparatives de
test mRNA vs. DNA (CIN2+)
Burger, E. A., H. Kornor, et al. (2011). "HPV mRNA tests for the detection of cervical intraepithelial neoplasia: a systematic review." Gynecol Oncol 120(3): 430-438.
The review suggests that mRNA tests have diagnostic relevance, but additional studies and economic evaluations must be conducted in order to make a solid conclusion regarding the clinical applicability of HPV mRNA testing. APTIMA vs. EasyQ vs. HCII/PCR