demystifying the neurology examination. aims introduce the principles underpinning a structured...
TRANSCRIPT

Demystifying the neurology examination

Aims
• Introduce the principles underpinning a structured neurological examination
• Revise some neuroanatomy• Show some pathologies
• Not creating instant experts• Not the only neurology talk you’ll ever need to
attend• Not a substitute for practice

Format• Cranial nerves
– Names and function– Some anatomy
• Motor system• Reflexes• Sensory system• Some practicalities of examination
– Cranial nerves and more anatomy– Limbs
• Images– Normality and pathology

• Cranial nerves
• Arms• Torso• Legs
• Higher mental function
• Observation • Tone • Power • Co-ordination • Reflexes• Sensation
– Light touch – Proprioception – Vibration sense– Pin prick – Temperature
I - XII

• Cranial nerves
• Arms• Torso• Legs
• Higher mental function
• Observation Ex/Pyr• Tone C/Sp• Power C/Sp• Co-ordination Cblr• Reflexes• Sensation
– Light touch – Proprioception D/Col – Vibration sense– Pin prick
S/Thal– Temperature
Gait


Cranial nerves
1
2
3
4
6
Smell
Vision
Eye movements

Cranial nerves
5
7
8
9
10
12
11
Face – motor and sensory
Face – motor (+ taste)
Hearing and balance
Palatal movement and gag reflex
Tongue movement
Head/shoulder movements

Cranial nerves – 1
Olfactory
• Sense of smell– Rarely formally tested– Ask directly– Bedside foodstuffs

Cranial nerves – 2
Optic
• Visual acuity– Snellen chart, newspaper
• Visual fields
• Direct light reflex
• (Consensual light reflex)

Retina
Optic nerve
Optic chiasm
Lateral geniculate bodies
Pretectal nucleus
Edinger-Westfahl nucleus
Ciliary ganglion
Pupil
III

L RVisual fields
Optic radiation
Retina
Optic nerve
Optic chiasm
Bitemporal hemianopia
RIGHT homonymous hemianopia

Cranial nerves – 3, 4 and 6
Occulomotor, Trochlear and Abducens
• Eye movements, pupil dilatation– SO4, LR6
• Double vision? Nystagmus? INO?
• Ptosis

Cranial nerves – 5
Trigeminal
• Motor– Masseter, temporalis
• Sensory– Va, Vb, Vc– Corneal reflex (unpleasant)

Cranial nerves – 7
Facial• Motor
– Frontalis (UMN v LMN)– Other facial muscles– Stapedius
• Sensory– Taste from anterior 2/3 of tongue via chordi
tympani

Cranial nerves – 8
Vestibulocochlear
• Hearing– Crude bedside testing
• Balance
• Rinne– Normal is positive
• Weber– Towards a conductive defect

Cranial nerves – 9 and 10
Glossopharyngeal and vagus
• Palatal movement with “aaaah”
• Gag reflex – bilateral
• IX: taste from posterior 1/3 of tongue

Cranial nerves – 12
Hypoglossal
• Tongue movement (NB: fasciculation)– Deviates towards the lesion

Cranial nerves – 11
Accessory
• Shoulder and head movements– Sternocleidomastoid and trapezius muscles

Cranial nerves – ‘epilogue’
Fundoscopy!
• Optic disc - only part of the brain that you can see
• Retina, vessels
• Cataracts

The Motor System
1. Corticospinal system = pyramidal- Cortex anterior horn cells- skilled, strong, organized movement
2. Extra-pyramidal = basal ganglia- facilitates fast fluid movements
3. Cerebellum- coordination
4. Lower motor neurones

1. Corticospinal tracts
• Main nerve fibres meet in internal capsule• Cross in medulla• Lesions UMN signs
= contralateral hemiparesis, spasticityNB: upper limb drift(UL: flexors; LL extensors predominate)
• Causes:– Most common = CVA– SOL– MS

Leg
Arm
Head and neck
Internal capsule
Cerebral cortex

2. Extra-pyramidal system
• Reduction in speed with muscle rigidity
• Involuntary movements
• Most common disorder = Parkinson’s

Corpus striatum
Caudate nucleus
Globus pallidus
Putamen
Cerebral cortex
Substantia nigraThalamus
Subthalamic nuclei
Cerebellum Reticular formation
Cranial nerve nuclei
Spinal cord

3. Cerebellum
• Coordination (rather than speed)
• Lateral lobes coordinate ipsilateral limb
• Vermis – axial posture and balance
Signs: intention tremor, ataxia, nystagmus, dysarthria (bilateral)

4. Lower motor neurones
• Motor pathway from anterior horn cell (or cranial nerve nucleus) via peripheral nerve to end plate
• Weakness, hypotonia, wasting, loss of reflexes• Causes:
– Bell’s, MND, polio– Spinal root compression– Peripheral nerve trauma, entrapment, mononeuritis
multiplex

UMN v LMN
Cortex
UMN
LMN
Muscle
Spasticity Flaccidity

Reflexes – the spinal reflex arc
• Activation of stretch receptors = first order sensory neurones
• Synapse directly with motor efferent fibres at local spinal level
• Activate LMNs contraction
REINFORCEMENT

Myotomes


Reflexes – spinal levels
• Supinator C 5-6
• Biceps C 5-6
• Triceps C 7-8
• Knee L 3-4
• Ankle S 1-2
Plantar reflex

Reflexes – spinal levels
• Supinator C 5-6
• Biceps C 5-6
• Triceps C 7-8
• Knee L 3-4
• Ankle S 1-2
Plantar reflex

Reflexes – spinal levels
• Supinator C 5-6
• Biceps C 5-6
• Triceps C 7-8
• Knee L 3-4
• Ankle S 1-2
Plantar reflex

Reflexes – spinal levels
• Supinator C 5-6
• Biceps C 5-6
• Triceps C 7-8
• Knee L 3-4
• Ankle S 1-2
Plantar reflex

Reflexes – spinal levels
• Supinator C 5-6
• Biceps C 5-6
• Triceps C 7-8
• Knee L 3-4
• Ankle S 1-2
Plantar reflex

Plantar reflex – Babinski’s sign
• Normal = downgoing (flexor)
• Extensor in UMN lesions
• Most receptive – posterior 1/3 of the lateral aspect of the sole
• Dorsiflexion and fanning of other toes

Abdominal reflex
• Contraction of oblique muscles in response to sensory stimulus
• Ipsilateral loss in UMN lesions

Sensory pathways
• Posterior columns
• Spinothalamic tracts

Posterior columns
• Travel ipsilaterally to brainstem, then cross to form medial lemniscus and pass to the thalamus
• Carry:– light touch (and 2-point discrimination)– vibration sense– proprioception (joint position sense)

Spinothalamic tracts
• Axons synapse in the dorsal horn and cross within two levels
• Then pass to the thalamus and reticular formation
• Carry:– pain– temperature

Sensory symptoms
• Paraesthesia
• Numbness
• Pain
• Quality and distribution suggest site of lesion
Spinal root and cord lesions
• Root pain– Worse with stretch
• Posterior column lesions– Lhermitte’s phenomenon
• Spinothalamic lesions– Dissociated sensory loss
• Cord compression– External (tumour, abcess) or internal (syrinx)

The Practicalities

Clinical examination
• Introduction– Shake hands (myotonia)
• General observation– Tremor, chorea– Obvious wasting– Asymmetry
• ‘Clues’– Diabetic accessories– ‘White stick’

Cranial nerves
• Face the patient• Observe for:
– ptosis (NB: myasthenia), asymmetry, scars
• Go through in logical order– (1) 2 ‘3 4 6’ 5(+r) 7 8 ‘9 10 12’ 11
• Equipment required:– Snellen chart, pen-torch, red hatpin, cotton
wool, needle, orange stick, tuning fork, opthalmoscope

Clinical abnormalities
• Horner’s syndrome– Unilateral pupillary constriction, partial ptosis,
enopthalmos
• Causes:– Brain stem – pontine glioma, LMS– Cervical cord – syringomyelia, tumour– T1 root lesions – bronchial apical tumour, cervical rib– Sympathetic chain in the neck – neoplastic infiltration,
post-surgery, carotid artery occlusion– Others - congenital

Occular and pupillary abnormalities
• Argyll Robertson pupil– neurosyphilis
• Holmes-Adie pupil (myotonic pupil)• Internuclear opthalmoplegia
– MS (lesion in MLF)
• Diplopia• Strabismus (squint)
– Paralytic, non-paralytic

Pons
Medulla
Spinal cord
6th nucleus
7th nucleus
VG
Pontine nucleus of 5
Spinal nucleus of 5
Va
Vb
Vc
SUPERIOR ORBITAL FISSURE
FORAMEN ROTUNDUM
FORAMEN
OVALE

Facial nerve palsies
• Part of facial nucleus supplying frontalis receives supranuclear fibres from each hemisphere
• UMN– Upper part of face spared
• LMN– Whole face affected
• Ramsay Hunt syndrome• Hyperacusis

Stylomastoid foramen
Pons
Medulla
Spinal cord
6th nucleus
7th nucleus
Facial muscles
Nerve to stapedius
GG

Pons
Medulla
Spinal cord
VG
Va
Vb
Vc
SUPERIOR ORBITAL FISSURE
FORAMEN ROTUNDUM
FORAMEN OVALE
6
5
7
5
Facial muscles
N to S
Tongue
Relationship between V and VII
CHORDA TYMPANI
GG


9
10
11
‘Aldermanic’ nerve

Upper limbs
• Visual inspection– Wasting, fasciculation, tremor, chorea, burns
• Test tone– ‘cogwheel’, ‘clasp knife’, lead pipe’
• Power – main myotomes / muscle groups– Grade 1–5 out of 5
• Coordination (need power)– “finger-nose”, dysdiadochokinesis
• Reflexes– Supinator, biceps, triceps
• Sensation– L/T, joint position, vibration, pin-prick, temperature

Lower limbs• Visual inspection
– Wasting, fasciculation, tremor, burns, trophic changes• Test tone, clonus• Power – main myotomes / muscle groups
– Grade 0–5 out of 5• Coordination (need power)
– “heel-shin”, “tapping foot”• Reflexes
– Abdominal, knee, ankle, plantar• Sensation
– Include testing for sensory level over abdomen/chest– (Perianal sensation, anal tone)– Romberg’s test: proprioception NOT cerebellum
• Gait

“Other neurology to test”
• Higher mental function– Speech, memory, recognition, numeracy,
emotion
• Sympathetics and parasympathetics
• Disorders of micturition
• Urinary and faecal continence
• Disorders of sexual function
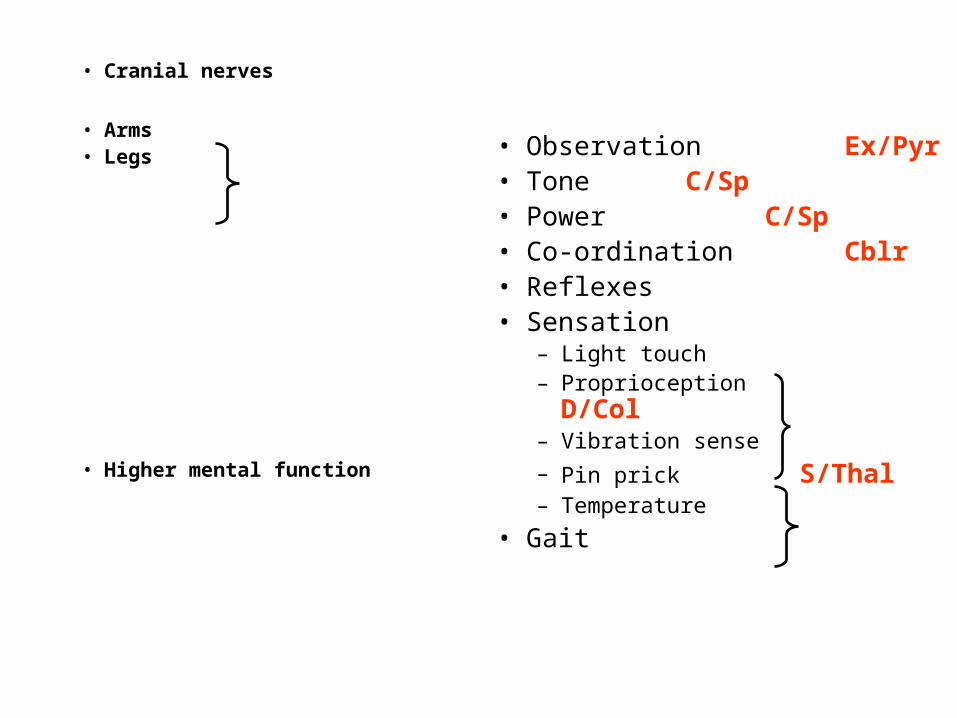
• Cranial nerves
• Arms• Legs
• Higher mental function
• Observation Ex/Pyr• Tone C/Sp• Power C/Sp• Co-ordination Cblr• Reflexes• Sensation
– Light touch – Proprioception D/Col – Vibration sense
– Pin prick S/Thal– Temperature
• Gait