babson college benefits guidehr.babson.edu/handbook/2014_benefits_guide.pdf · the babson college...
TRANSCRIPT

Babson College
Benefits Guide
2014 Employee Benefits

TABLE OF CONTENTS
Overview of Benefits 3
Eligibility 4-5
Medical Coverage 6-10
Health Savings Account (HSA) 11
Dental Coverage 12
Vision Coverage 13
Flexible Spending Accounts (FSA) 14
HSA / FSA Comparison 15
Employee Contributions 16
Salary Continuation & Long Term Disability Coverage 17
Life and AD&D Insurance 18
Supplemental Life Insurance Rates 19
Retirement Plan 20
Tuition Benefits 21
Time-Off Benefits 22
Other Valuable Benefits 23-24
Benefit Resources 25
Compliance Notices 26-27
Appendix:
USERRA Notice
CHIP Notice
Summary of Benefits and Coverage

OVERVIEW OF BENEFITS
Page 3
Welcome!
Babson College is proud to offer you a comprehensive benefit package to meet the needs of you and your family.
The Babson College suite of benefits includes:
Medical coverage offered through Blue Cross Blue Shield of Massachusetts
A Health Savings Account administered by Wells Fargo
Dental coverage offered through Delta Dental of Massachusetts
Vision coverage offered through Vision Services Plan
Flexible Spending Accounts administered by Crosby Benefit Systems
Salary Continuation coverage self-administered by Babson College
Long Term Disability coverage administered through Cigna
Basic Life and AD&D Insurance administered through Cigna
Supplemental Life Insurance administered through Cigna
A 403(b) Defined Contribution Retirement Plan
Tuition Benefits
Time-Off Benefits
Additional programs, discounts and benefits
*Please note this guide is intended as a brief overview of benefits only. The policies, contracts or certificate for each benefit plan will govern the benefits and include more de-tails on how the benefit plan operates. See the next page for eligibility guidelines.
Full-time Employees: You are eligible to participate in the Babson full-time benefits program if you are a full-time faculty member or a member of the Babson staff regularly scheduled to work a minimum of 1,456 hours per year (or 28 hours/week).
Part-time Employees: You are eligible for part-time benefits if you are a staff member scheduled for at least 1,000 hours per year (or 20 hours/week), or if you are in a benefits eligible part-time faculty role. See the chart on the following page for a listing of benefits available for full-time and part-time employees. COVERAGE LEVELS You may choose from three coverage levels for medical, dental and vision care benefits: Employee Employee + 1 (spouse/domestic partner or child) Family ELIGIBLE DEPENDENTS Your eligible dependents for medical, dental and vision care coverage include: Your legal spouse Your eligible domestic partner A dependent child up to age 26 regardless of:
their marital, student or employment status whether they are your tax dependent whether your home is their principal place of residence
For this purpose, the term child is defined as: Your natural child A child for whom you are the legally appointed guardian with full financial
responsibility A child of a domestic partner, as long as you also cover your domestic partner Your stepchild Your child who is incapable of self-support because of a total physical or mental
disability Your legally adopted child or child placed with you for adoption A child named in a Qualified Medical Child Support Order Your child age 26 or older who is incapable of self-support because of a total
physical or mental disability that occurred while covered under the plan A child of a covered unmarried dependent . Please Contact Babson Human
Resources) An eligible domestic partner is a person of the same or opposite sex with whom you
have established a domestic partnership. To be considered domestic partners, both partners must sign an affidavit of domestic partnership and meet certain requirements. For more information, contact the Office of Human Resources, extension 5498 or 781-239-5498.
ELIGIBILITY
Page 4

ELIGIBILITY
Page 5
Comparison of Available Benefits - Full-Time vs. Part-Time
FULL-TIME BENEFITS PART-TIME BENEFITS
Medical Medical
Dental Dental
Vision Vision
Health Savings Account (PPO only) Health Savings Account (PPO only)
Flexible Spending Accounts Flexible Spending Accounts
Health Advocate Health Advocate
Retirement Plan Retirement Plan
Employee Assistance Program Employee Assistance Program
Vacation Time Vacation Time
Sick Time Sick Time
Holiday Pay Holiday Pay
Perks at Work Perks at Work
HEALTHY YOU/Be Well Programs HEALTHY YOU/Be Well Programs
Business Travel Accident Business Travel Accident
Long Term Care Long Term Care
529 Savings Plan 529 Savings Plan
WeCare+ WeCare+
Pet Insurance Pet Insurance
Life Insurance
Salary Continuation
Long Term Disability
Floating Holidays
Tuition Remission
Tuition Reimbursement
Secure Travel
Medical Rebate
Dental Rebate
The chart below lists the benefits that are included in Babson’s full-time and part-time benefit programs. Eligibility requirements for each program are detailed on the previous page of this booklet.

MEDICAL COVERAGE
Page 6
Babson College offers employees three medical plans through Blue Cross Blue Shield of MA. Employees can choose between two HMO options: the High Option- HMO Blue New England Value Plus Plan, or the Low Option-HMO Blue New England Enhanced Value Plan, or the PPO Blue Care Elect Saver Plan with a Health Savings Account. You share the cost of medical coverage through pre-tax payroll deductions.
Comparing Your Medical Options HMO Options: These plans cover services only when provided within the HMO provider network, except in emergencies. You make a copayment for certain services, and other services including preventive care, are covered in full. When you join one of the HMOs, you select a Primary Care Physician (PCP). Your PCP will coordinate your overall health care and make referrals to specialists, as necessary.
PPO and Health Savings Account: The PPO is designed to work in conjunction with a Health Savings Account (HSA). This is a consumer driven, high deductible health plan with a deductible that must be satisfied before most services are covered, with the exception of preventive care. The PPO offers the flexibility to use any provider in the extensive national PPO network. Out of network benefits are available subject to the deductible and coinsurance.
Babson contributes a portion of the PPO deductible to a Health Savings Account for you. You may also make tax-free contributions to the account to help pay for eligible out-of-pocket health care expenses. See Health Savings Account section for more information about the HSA.
Carefully review the comparison chart on the next page to see the differences among the HMO and PPO options.
Summary of Benefits and Coverage (SBC) As an employee, the health benefits available to you represent a significant component of your compensation package. They also provide important protection for you and your family in the case of illness or injury.
Your plan offers a series of health coverage options. Choosing a health coverage option is an important decision. To help you make an informed choice, your plan makes available a Summary of Benefits and Coverage (SBC), which summarizes important information about any health coverage option in a standard format, to help you compare across options.
The SBC is located in the appendix section of this Benefits Guide. A paper copy is also available, free of charge, by calling the HR Department at 781-239-5498 and Blue Cross Blue Shield at 1-888-543-8770 to request a copy of the Glossary of terms.
Waive Coverage Full-time faculty and full-time staff are eligible to receive a rebate when waiving medical coverage and/or dental coverage. If you waive medical coverage and/or dental coverage, you will not be able to enroll until the next open enrollment period, unless you have a qualified life event.

MEDICAL PLAN COMPARISON
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state
mandates may apply.
Page 7

Value Based Benefits Members with asthma, diabetes, coronary artery disease, or risk of cardiovascular disease (taking high blood pressure medications in combination with high cholesterol medications), or depression associated with any of these conditions, have coverage that helps to more affordably manage care. For certain Tier 1 and Tier 2 medications used to treat these conditions, the member will pay the same copayment for a three-month supply as the member would for a one-month supply from a retail pharmacy when filling a prescription through the BCBS convenient, low-cost mail service pharmacy. This is a savings of up to eight copayments per year for each medication. Note: For members on the high deductible PPO, the RX deductible will not apply when using the mail order for these specific medications. This benefit also applies to covered spouses and dependents who are also eligible for these savings.
To access the medication list and learn more, visit www.bluecrossma.com/valuebased.
Women’s preventive health
Annual well-woman visits
Screening for gestational diabetes
Human papillomavirus (HPV) DNA testing
Counseling for sexually transmitted infections
Counseling and screening for human immunodeficiency virus (HIV) infections
Contraceptive methods and counseling
Breastfeeding support, supplies, and counseling
Domestic violence screening
MA mandates
Coverage is provided for a child under the age of 18 for treatment of cleft lip and cleft palate. This coverage
must include benefits for the following services, as long as they are prescribed by a physician or surgeon:
Medical, dental, oral and facial surgery
Surgical management and follow-up care by oral and plastic surgeons
Orthodontic treatment and management
Preventative and restorative dentistry
Speech therapy
Audiology
Nutrition services Coverage is provided for any child 21 years of age or younger for the full cost of one hearing aid per hearing-impaired ear. The law requires coverage for up to $2,000 for each hearing aid every 36 months, upon prescription from the minor’s treating physician that the hearing aids are medically necessary. Coverage must include all related services prescribed by a licensed audiologist or hearing instrument specialist, including the initial hearing aid evaluation, fitting and adjustments, and supplies (including ear molds).
Additional BCBS Benefits
Page 8
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.

Benefits as required under the Affordable Care Act (ACA)
Fitness reimbursement—BCBS will reimburse the cost of membership fees up to 3 consecutive months for
one family or one individual for participation at a qualified fitness club Weight Loss Benefit—BCBS will reimburse the cost for up to 3 months for participation in a qualified weight
loss program each calendar year for any combination of members covered under the plan Low Protein Foods— the $5000 per member per calendar year annual limit is removed; it is now unlimited Hair Prothesis—BCBS will reimburse the cost of one wig per calendar year with no dollar limit Durable Medical Equipment—the per member per calendar year dollar limit will be removed; there will now
be a member coinsurance cost share
New BCBS Benefits effective January 1, 2014
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Page 9

Healthy You Babson is proud to join with other area colleges in the “Healthy You” initiative, dedicated to a healthier and more productive workforce. You’ll be offered wellness programs through [email protected], Blue Cross Blue Shield, on-campus partners such as Athletics and the CWEL with incentives to participate and become a healthier you! A healthier workforce will also help Babson keep medical costs under control, which benefits both you and Babson. Here’s to your health!
Health Advocate Health Advocate is a free and confidential service for you and your family members that serves as your lifeline to health care and insurance assistance. Save time and money by having Health Advocate find you qualified specialists and hospitals, untangle your medical bills, locate eldercare and support services, and help you and your loved ones with any health or insurance related question. This service is available to you and your family, whether or not you are covered by a Babson plan. To Contact Health Advocate: Call 866-695-8622, Monday - Friday, 8:00 am - 9:00 pm EST Send an email to [email protected] Website: www.healthadvocate.com
MEDICAL COVERAGE
Page 10
Prescription Drug Coverage
All three medical plans provide prescription drug coverage, which includes a mail order program. When you fill your prescription at a participating retail pharmacy, you may purchase up to a 30-day supply of covered drugs. At the pharmacy, you will need to present your ID card and make the required copayment. Mail-order Program: If you use a maintenance drug, you may use the mail order program to receive a 90-day supply at a reduced cost. To start, ask your doctor to provide a prescription for a 90-day supply of your medication, plus refills. Then order your prescription refills online.
Finding a Network Provider or Facility
You have several resources to find the right physician, specialist or facility in the BCBS MA network.
BCBS Concierge Care Center: Call 888-543-8770, Monday - Friday, 8:00 am - 6:00 pm EST
Blue Cross Blue Shield Website: Log on to www.BCBSMA.com to view a provider directory
Health & Wellness
HEALTH SAVINGS ACCOUNT (HSA)
Page 11
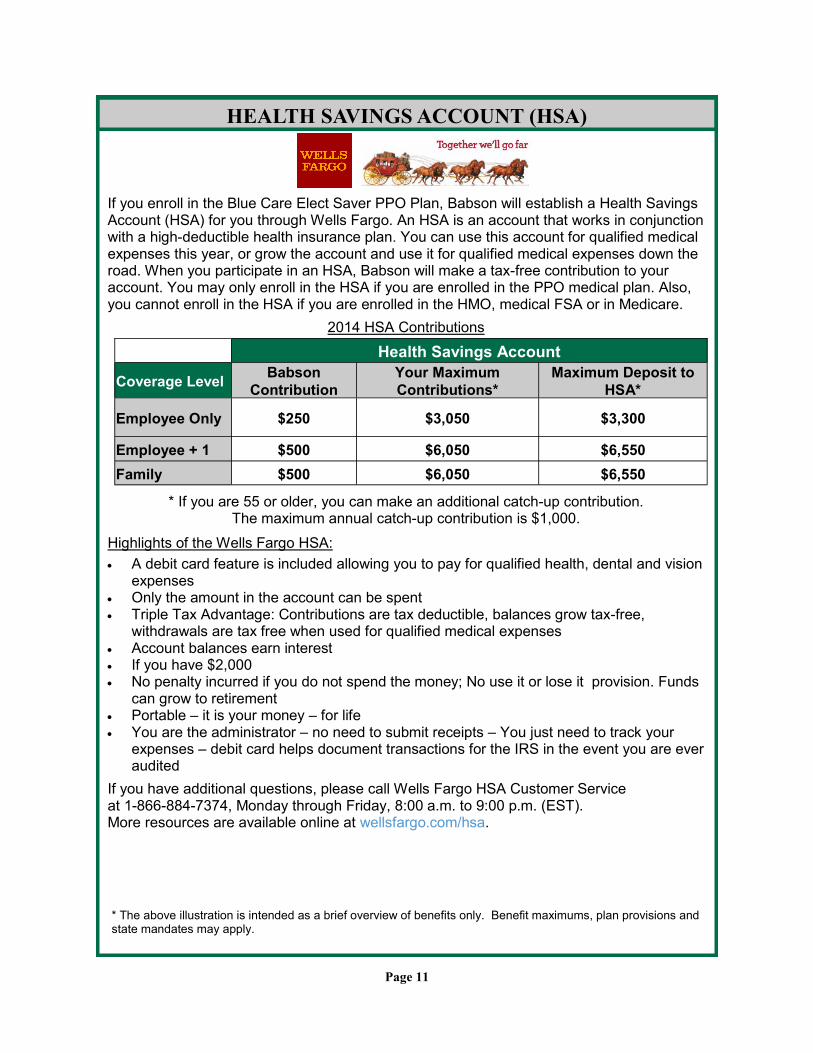
If you enroll in the Blue Care Elect Saver PPO Plan, Babson will establish a Health Savings Account (HSA) for you through Wells Fargo. An HSA is an account that works in conjunction with a high-deductible health insurance plan. You can use this account for qualified medical expenses this year, or grow the account and use it for qualified medical expenses down the road. When you participate in an HSA, Babson will make a tax-free contribution to your account. You may only enroll in the HSA if you are enrolled in the PPO medical plan. Also, you cannot enroll in the HSA if you are enrolled in the HMO, medical FSA or in Medicare.
2014 HSA Contributions
* If you are 55 or older, you can make an additional catch-up contribution. The maximum annual catch-up contribution is $1,000.
Highlights of the Wells Fargo HSA:
A debit card feature is included allowing you to pay for qualified health, dental and vision expenses
Only the amount in the account can be spent Triple Tax Advantage: Contributions are tax deductible, balances grow tax-free,
withdrawals are tax free when used for qualified medical expenses Account balances earn interest If you have $2,000 No penalty incurred if you do not spend the money; No use it or lose it provision. Funds
can grow to retirement Portable – it is your money – for life You are the administrator – no need to submit receipts – You just need to track your
expenses – debit card helps document transactions for the IRS in the event you are ever audited
If you have additional questions, please call Wells Fargo HSA Customer Service at 1-866-884-7374, Monday through Friday, 8:00 a.m. to 9:00 p.m. (EST). More resources are available online at wellsfargo.com/hsa.
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Health Savings Account
Coverage Level Babson
Contribution
Your Maximum
Contributions*
Maximum Deposit to
HSA*
Employee Only $250 $3,050 $3,300
Employee + 1 $500 $6,050 $6,550
Family $500 $6,050 $6,550

* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
DENTAL PLAN COMPARISON
Page 12
Babson offers the choice of two dental plans through Delta Dental of MA. Employees can choose between the Delta Premier Plan and the DeltaCare Plan.
A rebate is available for full-time employees who elect to waive coverage.
Manage Your Dental Health -Delta Dental provides easy access to your dental plan information. You can: Find a network dentist Verify plan eligibility and view benefit plan coverage View claims information Request an ID card -Log on to www.deltadentalma.com -Call Delta Premier at 800-872-0500 or DeltaCare at 800-327-6277 Monday - Thursday, 8:30 am - 8:00 pm EST; Friday, 8:30 am - 4:30 pm EST

VSP Provider Out of Network
Vision exams $10 copay - one every 12 months Reimbursed up to $50
Lenses every 12 months
Single vision, lined bifocal and lined trifocal lenses
$10 copay combined with exam Reimbursed up to: Single vision: $50 Lined bifocal: $75
Lined trifocal: $100
Frames every 24 months
Frame selections $120 allowance for selection of frames 20% off the amount over allowance
Reimbursed up to $70
Contact Lenses in Lieu of Eyeglasses (every 12 months)
$120 allowance for contacts and the contact lens exam (fitting and evaluation)
If you choose contact lenses you will be eligible for frames 24 months from date
the contact lenses were obtained.
Note: current soft contact lens wearers may qualify for a special program that includes a contact lens exam and initial
supply of lenses.
Reimbursed up to $105
$20 reimbursement for featured frame brands such as Bebe, Calvin Klein, Flexon, Lacoste, Michael Kors, Nike, Nine West, and others.
Network now includes Costco, Visionworks and Cohen’s.
VISION COVERAGE
Babson offers the option to purchase vision coverage through Vision Services Plan (VSP). Employees pay for the full cost of this coverage through after-tax payroll deductions.
Need Additional Information or Have a Question?
For more information about the plan and discounts or to find a VSP provider, visit the VSP
website or call VSP customer service:
Log on to www.vsp.com
Call 800-877-7195, Monday - Friday, 8:00 am - 10:00 pm EST
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Page 13

Eligible dependent care expenses must be paid to your dependent care provider directly:
FSA Claim Process: Pay your dependent care provider directly and then file a claim for reimbursement.
Eligible health care expenses can be paid for in one of two ways:
Medical Care FSA Debit Card: Use the debit card to pay for expenses at the point of service. FSA Claim Process: Pay the health care provider directly and then file a claim for
reimbursement.
Contact Crosby Benefits For More Information
Log on to www.crosbybenefits.com
Call 866-918-9711,ext. 2, Monday - Thursday, 8:00 am - 6:00 pm and Friday, 8:00 am - 5:00 pm
Fax 978-367-9626
Crosby Benefit Systems, Inc. 27 Christina Street, Newton, MA 02461
You have the opportunity to participate in a Flexible Spending Account (FSA) program administered by Crosby Benefit Systems. Employees can contribute to two types of accounts: the Medical Care FSA and the Dependent Care FSA. You need to plan carefully before you participate in an FSA, because you forfeit any unused funds at the end of the year, as legally required under the “use it or lose it” rule. You may only change your FSA elections during the year if you have a qualified life event.
FLEXIBLE SPENDING ACCOUNTS (FSA)
Page 14
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
MEDICAL CARE FLEXIBLE SPENDING ACCOUNT
2014 Annual Contribution
Maximum
$2,500 - Maximum contribution amount Note: The maximum amount you elect to contribute for the year is available to you for expenses beginning January 1. You are responsible for funding the total annual amount elected by the end
of the plan year (December 31).
Eligible Expenses
• Out-of-pocket medical costs, such as deductibles, copayments and coinsurance • Prescription drug copayments • Over-the-counter medicine (prescription required )
• Non-covered dental, vision and other eligible health care expenses
Claims Period Expenses must be incurred from January 1 through December 31
Claims Deadline Claims must be submitted by March 31 of the following year
DEPENDENT CARE FLEXIBLE SPENDING ACCOUNT
2014 Annual Contribution
Maximum
$5,000
Married, filing separate returns: $2,500
Eligible Expenses
• Pre-school or nursery school expenses • Expenses for a babysitter in your home • Day care center • Summer day camp* • Afterschool care • Adult day care center or in-home care for an adult dependent
* Overnight summer camp is not eligible.
Claims Period Expenses must be incurred from January 1 through December 31
Claims Deadline Claims must be submitted by March 31 of the following year
FLEXIBLE SPENDING ACCOUNT/HEALTH SAVINGS ACCOUNT COMPARISON
Page 15
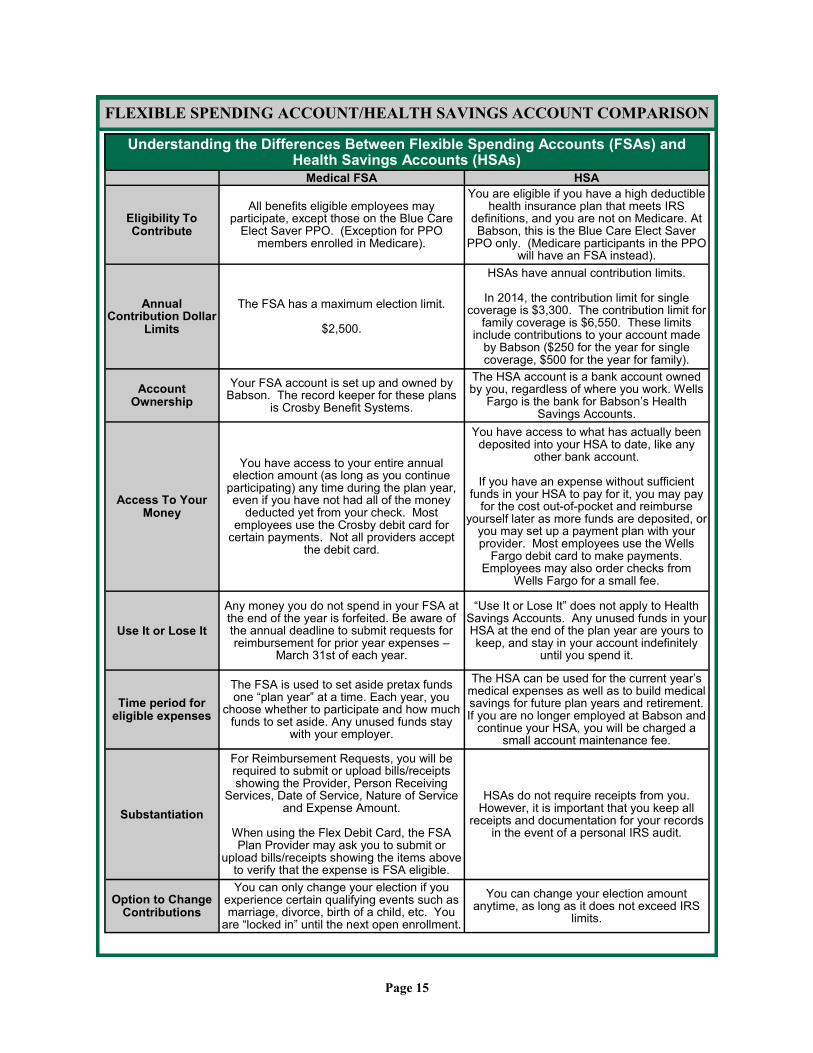
Understanding the Differences Between Flexible Spending Accounts (FSAs) and Health Savings Accounts (HSAs)
Medical FSA HSA
Eligibility To Contribute
All benefits eligible employees may participate, except those on the Blue Care
Elect Saver PPO. (Exception for PPO members enrolled in Medicare).
You are eligible if you have a high deductible health insurance plan that meets IRS
definitions, and you are not on Medicare. At Babson, this is the Blue Care Elect Saver
PPO only. (Medicare participants in the PPO will have an FSA instead).
Annual Contribution Dollar
Limits
The FSA has a maximum election limit.
$2,500.
HSAs have annual contribution limits.
In 2014, the contribution limit for single coverage is $3,300. The contribution limit for
family coverage is $6,550. These limits include contributions to your account made
by Babson ($250 for the year for single coverage, $500 for the year for family).
Account Ownership
Your FSA account is set up and owned by Babson. The record keeper for these plans
is Crosby Benefit Systems.
The HSA account is a bank account owned by you, regardless of where you work. Wells
Fargo is the bank for Babson’s Health Savings Accounts.
Access To Your Money
You have access to your entire annual election amount (as long as you continue
participating) any time during the plan year, even if you have not had all of the money
deducted yet from your check. Most employees use the Crosby debit card for
certain payments. Not all providers accept the debit card.
You have access to what has actually been deposited into your HSA to date, like any
other bank account.
If you have an expense without sufficient funds in your HSA to pay for it, you may pay
for the cost out-of-pocket and reimburse yourself later as more funds are deposited, or
you may set up a payment plan with your provider. Most employees use the Wells
Fargo debit card to make payments. Employees may also order checks from
Wells Fargo for a small fee.
Use It or Lose It
Any money you do not spend in your FSA at the end of the year is forfeited. Be aware of the annual deadline to submit requests for reimbursement for prior year expenses –
March 31st of each year.
“Use It or Lose It” does not apply to Health Savings Accounts. Any unused funds in your HSA at the end of the plan year are yours to keep, and stay in your account indefinitely
until you spend it.
Time period for eligible expenses
The FSA is used to set aside pretax funds one “plan year” at a time. Each year, you
choose whether to participate and how much funds to set aside. Any unused funds stay
with your employer.
The HSA can be used for the current year’s medical expenses as well as to build medical savings for future plan years and retirement. If you are no longer employed at Babson and
continue your HSA, you will be charged a small account maintenance fee.
Substantiation
For Reimbursement Requests, you will be required to submit or upload bills/receipts showing the Provider, Person Receiving
Services, Date of Service, Nature of Service and Expense Amount.
When using the Flex Debit Card, the FSA Plan Provider may ask you to submit or
upload bills/receipts showing the items above to verify that the expense is FSA eligible.
HSAs do not require receipts from you. However, it is important that you keep all
receipts and documentation for your records in the event of a personal IRS audit.
Option to Change Contributions
You can only change your election if you experience certain qualifying events such as marriage, divorce, birth of a child, etc. You
are “locked in” until the next open enrollment.
You can change your election amount anytime, as long as it does not exceed IRS
limits.

Full-time Employee Part-time Employee
Monthly Bi-Weekly Monthly Bi-Weekly
Babson's
Cost
Employee
Cost
Babson's
Cost
Employee's
Cost
Babson's
Cost
Employee
Cost
Babson's
Cost
Employee's
Cost
BCBS HMO Blue NE Value
Plus - High Option
Employee $398.02 $244.47 $183.70 $112.83 $215.79 $426.70 $99.60 $196.94
Employee + 1 $816.08 $521.38 $376.65 $240.64 $442.48 $894.98 $204.22 $413.07
Family $1,190.15 $760.37 $549.30 $350.94 $645.31 $1,305.21 $297.83 $602.41
BCBS HMO Blue NE
Enhanced Value - Low Option
Employee $398.01 $218.54 $183.70 $100.86 $215.79 $400.76 $99.60 $184.97
Employee + 1 $816.08 $448.15 $376.65 $206.84 $442.48 $821.75 $204.22 $379.27
Family $1,190.15 $653.59 $549.30 $301.66 $645.31 $1,198.43 $297.83 $553.12
BCBS PPO Blue Care Elect
Employee $398.02 $132.67 $183.70 $61.23 $275.96 $254.73 $127.36 $117.57
Employee + 1 $816.08 $272.02 $376.65 $125.55 $565.81 $522.29 $261.14 $241.06
Family $1,190.14 $396.72 $549.30 $183.10 $825.16 $761.70 $380.84 $351.55
Medical Rebate *
(Full-time Employee Only)
Employee $84.00 $38.77 n/a n/a
Delta Dental Premier
Employee $32.18 $10.73 $14.85 $4.95 $17.16 $25.75 $7.92 $11.88
Employee + 1 $64.96 $21.65 $29.98 $9.99 $34.64 $51.97 $15.99 $23.98
Family $121.49 $40.50 $56.07 $18.69 $64.79 $97.19 $29.90 $44.86
Delta Dental Care
Employee $25.85 $8.62 $11.93 $3.98 $13.78 $20.68 $6.36 $9.54
Employee + 1 $48.44 $16.15 $22.35 $7.45 $25.83 $38.75 $11.92 $17.88
Family $72.94 $24.31 $33.66 $11.22 $38.90 $58.35 $17.95 $26.93
Dental Rebate *
(Full-time Employee Only)
Employee $12.00 $5.54 n/a n/a
VSP Voluntary Vision
(100% employee paid)
Employee $10.57 $4.88 $10.57 $4.88
Employee + 1 $15.32 $7.07 $15.32 $7.07
Family $27.48 $12.68 $27.48 $12.68
2014 EMPLOYEE CONTRIBUTIONS
Page 16
*Rebate provided each pay when you waive this benefit. Domestic Partner benefits: The value of the premium for medical and dental coverage may be imputed as income and added to your W-2 form for tax purposes. Please consult with your tax advisor.
DISABILITY COVERAGE
Page 17
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Babson provides full-time employees with both Salary Continuation and Long Term Disability coverage at no cost. These plans are designed to replace all or a portion of your income if you become disabled due to a non-work related injury or illness.
Salary Continuation
Long Term Disability
If you are benefits eligible and actively employed for a minimum of one year and become disabled for
2 consecutive weeks or more, you may apply for Salary Continuation. Babson may continue up to
100% of your income for an approved period for up to and not to exceed 6 months of disability.
Long term disability coverage is provided by Cigna. In the event you become disabled and are unable to perform the essential functions of your job, LTD benefits will replace 60% of your salary, up to a maximum of $10,000 per month. Benefits begin after 180 days of continuous disability. Pre-existing Condition: If your disability is related to a condition for which you received treatment within the past three months, you may not be eligible for benefits until you have been covered under this plan for 12 months.
Union employees, please refer to your collective bargaining agreement for specific information about your benefits.

You may elect to purchase additional life insurance coverage in $10,000 increments, not to exceed five times your annual salary or $700,000, whichever is smaller. Benefits are reduced for employees age 65 or older. Evidence of Insurability: If you enroll in Supplemental Life Insurance within 31 days of when you first become eligible, you do not need to provide evidence of good health.
Evidence of insurability is required when: You enroll late (after the 31-day enrollment period) You want to increase your Supplemental Life Insurance coverage at any time throughout
the year You elect coverage above the guarantee issue of $250,000 under age 70
($20,000 ages 70-74) In these cases, approval for Supplemental Life Insurance is based on medical evidence of insurability.
LIFE AND AD&D INSURANCE
Page 18
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Babson provides full-time employees Life and Accidental Death & Dismemberment (AD&D) insurance through Cigna to provide financial security to your dependents if you die or are severely injured in an accident. Babson provides coverage at no cost to you and gives you the opportunity to purchase additional life coverage for yourself and your dependents.
Basic Life and AD&D
Babson provides eligible faculty and staff with Basic Life Insurance equal to one times your base salary rounded to the next $1,000, up to $400,000, at no cost to you. An equal amount of Accidental Death and Dismemberment (AD&D) Insurance is also provided. AD&D Insurance protects you in case of accidental death or injury (loss of a limb, eyesight or hearing). Benefits are reduced for employees age 65 or older.
Supplemental Life
Dependent Life
You may also purchase life insurance coverage for your spouse and eligible dependent children.
Spousal Life Insurance: As long as you elect Supplemental Life Insurance coverage for yourself, you may purchase coverage for your spouse. You may elect coverage of up to $150,000, in $5,000 increments, provided coverage does not exceed 50% of your elected coverage amount. Your spouse will be required to provide evidence of insurability if requesting more the $50,000 in coverage or enrolling after first becoming eligible. Benefits are reduced when the spouse reaches his/her age of 65. Benefits for the spouse terminate at the spouse’s age of 80.
Dependent Life Insurance: Provided you elect Supplemental Life Insurance coverage for yourself, you may purchase life insurance coverage for your eligible dependent children. You
may elect coverage of $500 per child from 14 days to six months and $10,000 per child from six months to age 25. All of your eligible children are covered at one rate and are not required to provide evidence of insurability.

SUPPLEMENTAL LIFE INSURANCE RATES
Page 19
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Supplemental Life Insurance *Must have own coverage to elect spousal coverage
Employee/Spouse Age
Employee Monthly Cost per $10,000 Unit
Spouse Monthly Cost per $5,000 Unit
Under 30 0.60 0.30
30 to 34 0.80 0.40
35 to 39 1.00 0.50
40 to 44 1.50 0.75
45 to 49 2.50 1.25
50 to 54 4.00 2.00
55 to 59 7.10 3.55
60 to 64 10.70 5.35
65 to 69 16.30 8.15
70 to 74 32.40 16.20
75 to 79 55.50 27.75
80 & Over 55.50 XXX
Note: Benefits are reduced starting at age 65. Employee coverage is in $10,000 increments. Spousal coverage is in $5,000 increments and cannot exceed 50% of the employee’s coverage amount. Benefits terminate for the spouse at the spouse’s age of 80. The monthly cost for children is $2.20 for $10,000 of coverage. One premium will insure all your eligible children, regardless of the
number of children you have.

Manage Your Retirement Plan Account You may enroll online, review your account balances and activities, make election changes, and access information, tools and resources through Fidelity Investments and/or TIAA-CREF.
Fidelity Investments www.NetBenefits.com 800-343-0860, Monday - Friday, 8:00 am - midnight EST
TIAA-CREF www.TIAA-CREF.org/Babson 800-842-2776, Monday - Friday, 8:00 am - 6:00 pm EST and Saturday, 9:00 am - 6:00 pm EST
RETIREMENT PLAN
Page 20
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
The Babson College Retirement Plan helps prepare you financially for retirement. The plan is a 403(b) defined contribution plan. As a condition of employment, you must participate in the Retirement Plan, following four full months of employment. Both you and Babson contribute to the plan. The contribution amount is based on your base earnings. You direct the investment of your Retirement Plan contributions to TIAA-CREF and/or Fidelity, and are immediately vested in your account balance (all contributions and investment earnings). Both companies offer an array of funds and a brokerage option. When you retire or leave Babson, you take your entire account balance with you.
Your Contributions If your base salary is $58,850 or less, your annual contribution to the plan is 2% of your base salary. If your base salary is more than
$58,850, you contribute 2% of your first
$58,850 ($1,137) of salary and 3% of
any amount over $58,850.
Babson’s Contributions Babson contributes an amount equal to four times your contributions to the plan: 8% of base salary up to $58,850
12% of base salary above $58,850,
up to the 403(b) earnings limit
*The amount of $58,850 is based on 2014.

Off-Campus Education Babson may provide up to $5,250 per calendar year of tax-exempt financial support for full-time regular benefits eligible staff members pursuing degree programs or specific coursework at other appropriate educational institutions, provided study is related to the staff member’s present position, professional area or career path at Babson.
TUITION BENEFITS
Page 21
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Babson supports your professional growth and the education of your family through tuition remission benefits. Full-time faculty and full-time regular benefits eligible staff, their spouses and dependent children may be eligible for tuition remission for graduate and undergraduate courses taken at Babson.
Benefits cover tuition charges (excluding books, room, board, supplies and other fees) based on the following guidelines:
Benefit Requirement Users of the tuition remission benefit must be admitted according to the general standards expected of all applicants to the College. Tuition remission is not available to non-admitted students taking courses at the College. Users of the tuition remission benefit must notify Human Resources prior to the start of each semester. Users of the tuition remission benefit are encouraged to apply for all federal, state, local and private scholarships or grants to which they may be entitled. If other funds are received, appropriate adjustments will be made.
Babson College Undergraduate and Graduate Schools
Employee
100% remission for graduate evening programs beginning the next semester falling on or after your four-month anniversary. You may take up to a maximum of 18 credits per calendar year (unless otherwise approved by your President’s Cabinet member). Note: Federal law requires that tuition remission granted in each calendar year in excess of $5,250 be reported as taxable income on the employee’s W2. Some courses may be considered tax exempt, contact HR for more
information.
Spouse or Dependent
Child
For Fast Track, undergraduate, and evening, one-year and two-year graduate programs, beginning the next semester falling on or after the employee’s anniversary of full-time employment as follows: • Second anniversary …….50% • Third anniversary …….....80% • Fourth anniversary …....100% Note: Tuition remission is not available for post-graduate MBA degree programs or for post-baccalaureate studies in the undergraduate program. Tuition remission received for undergraduate programs is tax exempt. Federal law requires that the full amount of the tuition remission granted in each calendar year for graduate programs be reported as taxable income on
the employee’s W2.
End of Full-Time Employment If you end full-time employment at Babson tuition benefits end immediately and a prorated tuition charge is made for the course(s) you and/or your spouse are taking. Dependent children taking courses will receive the tuition benefit until the end of the semester currently in session.

TIME-OFF BENEFITS
Page 22
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
Babson offers a comprehensive time-off program that provides financial support when you are sick and for time away from your regular job responsibilities. The program includes vacation time, sick time and holidays.
Vacation Time You earn vacation time based on your job category and length of employment. Part-time employees accrue vacation on a prorated basis based upon your standardhours. When you leave Babson, any accrued and unused vacation time is paid out
to you. Your accrual will be prorated based on your hire date.
Sick Time During the first full 12 months of employment, full-time faculty and staff have 3 weeks of sick time. After 1 full year of employment, you may have an unspecified amount oftime. Documentation of your illness or injury may be required in order to continue to be paid. Salary Continuation, Long-Term Disability and Family and Medical Leave Act (FMLA) may apply for extended illnesses.
Holidays Babson celebrates 17 holidays each year, including national, state and floating holidays and special holidays determined annually by the President. The schedule is posted on hrinfo, accessible from the Babson portal.
Leaves of Absence Babson complies with all federal and state laws regarding leaves of absence. Family illness and parental leaves are also available.

Page 23
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
OTHER VALUABLE BENEFITS
Babson offers several additional programs, discounts and benefits that you may want to take advantage of.
Employer Paid
Employee Assistance Program
The Employee Assistance Program (EAP) is offered through Kathleen Greer Associates (KGA) and is designed to help you or your household members address personal concerns or life issues you may be facing – at home or at work. The confidential and free service provides professional counseling and referral networks. The EAP counselors provide assessments services and short-term counseling on items such as legal consultation, financial consultation, child and elder care resources, nutrition consultation, work life resources, career assessment, parenting resources and stress reduction. You have access to the EAP, 24 hours a day, 7 days a week.
Travel Benefits
Secure Travel is a free benefits for full-time employees through Cigna, administrator of our life insurance and disability plans. Se-cure Travel provides emergency medical evacuation assistance and travel services, as well as helpful pre-trip planning assis-tance, when traveling 100 miles or more away from home on college business or on vacation. The toll-free customer service center is available 24 hours a day, 365 days a year. And, in an emergency, the custom-er service center can even accept collect calls.
U.S. & Canada: 888-226-4567 Other Locations, Call Collect: 202-331-7635 www.cigna.com
Business Travel Accident Insurance, administered by AIG/Chartis, is free and provides you and your family with a degree of financial security should you die or suffer a loss resulting from an accident while traveling on business for Babson College. The benefit amount is based on your base salary and contingent on the type of loss incurred. This plan also provides business-related travel services, such as pre-travel assistance, support during your trip, medical emergency services and legal assistance. When within U.S., call 877-244-6871; When outside the U.S., call +1 715-346-0859
Access EAP Services Website: www.kgreer.com User Name: Babson Password: 9557 Phone: 800-648-9557

Perks@Work Through Perks@Work, Babson offers many different discounts related to sports and recreation, insurance, entertainment, transportation, flowers, food, personal care and more. For more information, visit hrinfo from the Babson portal.
Page 24
* The above illustration is intended as a brief overview of benefits only. Benefit maximums, plan provisions and state mandates may apply.
OTHER VALUABLE BENEFITS
Long-Term Care (LTC) Insurance Long-term Care Insurance, offered through CNA, provides financial assistance when you are no longer able to perform basic activities of daily living without help. This optional plan provides a dai-ly benefit amount for nursing home care and community based care (i.e., care outside of a nursing home, such as home healthcare, adult day care, foster care or assisted living facility). You choose the level of care, which determines your cost. You may elect LTC coverage for yourself, your spouse (including same sex or opposite sex domestic partner), parents, parents-in-law, grandparents or grandparents-in-law who are under age 90. You may enroll within 30 days of your date of hire with-out providing evidence of insurability. If you enroll outside this period, you will need to provide proof of good health. Family members are subject to approval. This plan is portable when you leave Babson.
877-777-9072 www.ltcbenefits.com
529 Savings Plan The 529 Savings Plan, offered through Fidelity Investment Advisors, allows you to make after-tax contributions to save for college expenses. The contributions are made through direct deposit and are allowed to grow on a tax-deferred basis. There is no commission fee or monthly maintenance cost when you join the plan through Babson. Distributions from the plan are tax-exempt provided they are used for qualified higher education expenses.
Fidelity/800-343-0860, www.advisor.fidelity.com
M-F, 8:00 am-midnight EST
TIAA-CREF/800-842-2776, www.TIAA-CREF.org/Babson
M-F, 8:00 am-6:00 pm EST & Saturday, 9:00 am-6:00 pm EST
Pet Health Insurance This optional benefit, offered through Blue Cross Blue Shield of MA, helps protect the non-human members of your family. Petplan Pet Insurance covers dogs and cats, and offers comprehensive coverage for most illnesses and injuries. You choose the annual deductible level you want and pay for this insurance at favorable group rates. Visit hrinfo on the Babson portal for enrollment information.
www.petplanbenefit.com
800-809-9200
Monday - Friday, 8:00 a.m. - 10:30 p.m. (EST)
Saturday,8:30 am - 8:30 pm (EST)
Sunday, 10:00 am - 6:00 pm (EST)
Voluntary
WeCare + Eldercare Support This employee paid program is designed to assist you throughout the complex process of caring and arranging care of an aging or ailing loved one whether the care is delivered in or out of state. The service includes a comprehensive in-home needs and safety assessment, a personalized plan of
care, rich resources on care providers, access to geriatric specialists and care coordination. For more information, visit hrinfo from the Babson portal.
To enroll call: 855-570-CARE (2273)
Email [email protected]

Page 25
BENEFIT RESOURCES FOR INFORMATION ABOUT… CONTACT... GO TO…
Medical Benefits Blue Cross Blue Shield
Concierge Care Center 888-543-8770,
M-F, 8:00 am-6:00 pm EST www.bcbsma.com
Health Advocate 866-695-8622, M-F, 8:00 am-9:00 pm EST
www.healthadvocate.com
Health Savings Account Wells Fargo Customer Service
Wells Fargo Health Account Manager: 866-884-7374,
M-F, 8:00 am-7:00 pm EST www.wellsfargo.com/hsa
Dental Benefits Delta Dental
Delta Premier: 800-872-0500 DeltaCare: 800-327-6277
M-Th, 8:30 am-8:00 pm EST & Friday, 8:30 am-4:30 pm EST
www.deltadentalma.com
Vision Care Benefits Vision Services Plan (VSP)
800-877-7195, M-F, 8:00 am-10:00 pm EST
www.vsp.com
Flexible Spending Accounts Crosby Benefits
866-918-9711, ext. 2, M-Th, 8:00 am-6:00 pm &
Friday, 8:00 am-5:00 pm EST www.mycrosbybenefits.com
Disability Benefits Life Insurance Benefits AD&D Insurance Benefits Cigna
617-630-4300 www.cigna.com
Retirement Benefits Fidelity TIAA-CREF
877-208-0098 M-F, 8:00 am-midnight EST
800-842-2776, M-F, 8:00 am-6:00 pm EST &
Saturday, 9:00 am-6:00 pm EST
advisor.fidelity.com www.TIAA-CREF.org/Babson
Tuition Benefits Human Resources 781-239-4128
hrinfo through the Babson portal
Employee Assistance Program KGA
800-648-9557, M-Th, 8:30 am-5:30 pm EST & Fri-
day, 8:30 am-5:00 pm EST, Hotline 24/7
www.kgreer.com User Name: Babson
Password: 9557
Secure Travel Cigna
U.S. & Canada: 888-226-4567 Other Locations, Call Collect: 202-
331-7635 www.cigna.com
Business Travel Accident Benefit AIG/Chartis Insurance
When within U.S., call 877-244-6871; When outside the U.S., call +1 715-346-0859
www.chartisinsurance.com/_1247_296622.html
Long-Term Care Benefits CNA Insurance 877-777-9072
www.ltcbenefits.com Password: babsonolin
529 Savings Plan Fidelity Advisor 529 Plan 800-522-7297 www.fidelity.com
Pet Health Insurance 800-809-9200 M-F, 8:00 am-10:30 pm (EST)
Saturday,8:30 am –8:30 pm (EST Sunday,10:00 am-6:pm (EST)
www.petplanbenefits.com
Perks@Work Babson Portal – Click “hrinfo” under Human Resources, then select Perks@Work under company info
WeCare+ Eldercare Support 855-570-CARE (2273) [email protected]
Human Resources General Benefits Information 781-239-5498
hrinfo through the Babson portal
Page 26
Special Notices Notice of HIPAA Special Enrollment Rights If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing towards your or your dependents' other coverage). However, you must request enrollment within [insert “30 days'' or any longer period that applies under the plan] after your or your dependents' other coverage ends (or after the employer stops contributing toward the other coverage). If you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within [insert “30 days'' or any longer period that applies under the plan] after the marriage, birth, adoption, or placement for adoption. If you decline enrollment for yourself or for an eligible dependent (including your spouse) while Medicaid coverage or coverage under a state children's health insurance program is in effect, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage. However, you must request enrollment within 60 days after your or your dependents' coverage ends under Medicaid or a state children's health insurance program. If you or your dependents (including your spouse) become eligible for a state premium assistance subsidy from Medi-caid or through a state children's health insurance program with respect to coverage under this plan, you may be able to enroll yourself and your dependents in this plan. However, you must request enrollment within 60 days after your or your dependents' determination of eligibility for such assistance. To request special enrollment or obtain more information, contact Human Resources at (781) 239-5498. Newborns’ and Mothers’ Health Protection Act Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, Federal law generally does not prohibit the mother's or newborn's attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under Federal law, require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
Women’s Health and Cancer Rights Act If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be pro-vided in a manner determined in consultation with the attending physician and the patient, for:
all stages of reconstruction of the breast on which the mastectomy was performed;
surgery and reconstruction of the other breast to produce a symmetrical appearance;
prostheses; and treatment of physical complications of the mastectomy, including lymphedema. These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and sur-gical benefits provided under this plan.

Patient Protection Notice Blue Cross Blue Shield generally requires the designation of a primary care provider. You have the right to designate any primary care provider who participates in our network and who is available to accept you or your family members. For information on how to select a primary care provider, and for a list of the participating primary care providers, contact Human Resources at (781) 239-5498. For children, you may designate a pediatrician as the primary care provider. You do not need prior authorization from Blue Cross Blue Shield or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology, contact Human Resources at (781) 239-5498.
Page 27

Page 28
Your Rights Under USERRA
USERRA: The Uniformed Services Employment and Reemployment Rights Act USERRA protects the job rights of individuals who voluntarily or involuntarily leave employment positions to undertake military service or certain types of service in the National Disaster Medical System. USERRA also prohibits employers from discriminating against past and present members of the uniformed services, and applicants to the uniformed services. Reemployment Rights You have the right to be reemployed in your civilian job if you leave that job to perform service in the uniformed service and:
You ensure that your employer receives advance written or verbal notice of your service;
You have five years or less of cumulative service in the uniformed services while with that particular employer;
You return to work or apply for reemployment in a timely manner after conclusion of service; and You have not been separated from service with a disqualifying discharge or under other than honorable conditions. If you are eligible to be reemployed, you must be restored to the job and benefits you would have attained if you had not been absent due to military service or, in some cases, a comparable job. Right to be Free from Discrimination and Retaliation If you:
Are a past or present member of the uniformed service
Have applied for membership in the uniformed service; or
Are obligated to serve in the uniformed service; then an employer may not deny you:
Initial employment;
Reemployment;
Retention in employment;
Promotion; or Any benefit of employment because of this status In addition, an employer may not retaliate against anyone assisting in the enforcement of USERRA rights, including testifying or making a statement in connection with a proceeding under USERRA, even if that person has no service connection. Health Insurance Protection
If you leave your job to perform military service, you have the right to elect to continue your existing employer-based health
plan coverage for you and your dependents for up to 24 months while in the military. Even if you don’t elect to continue coverage during your military service, you have the right to be reinstated in your employer’s health plan when you are reemployed, generally without any waiting periods or exclusions (e.g., pre-existing condition exclusions) except for service-connected illnesses or injuries. Enforcement
The U.S. Department of Labor, Veterans Employment and Training Service (VETS) is authorized to investigate and
resolve complaints of USERRA violations.
For other assistance in filing a complaint, or for any other information on USERRA, contact VETS at 1-866-4-USA-DOL or
visit its website at http://www.dol.gov/vets. An interactive online USERRA Advisor can be viewed at http://www.dol.gov/elaws/userra.htm.
If you file a complaint with VETS and VETS is unable to resolve it, you may request that your case be referred to the
Department of Justice or the Office of Special Counsel, as applicable, for representation. You may also bypass the VETS process and bring a civil action against an employer for violations of USERRA.

Page 29
IDAHO – Medicaid and CHIP MONTANA – Medicaid
Medicaid Website: www.accesstohealthinsurance.idaho.gov
Medicaid Phone: 1-800-926-2588 CHIP Website: www.medicaid.idaho.gov
CHIP Phone: 1-800-926-2588
Website: http://medicaidprovider.hhs.mt.gov/clientpages/ clientindex.shtml Phone: 1-800-694-3084
INDIANA – Medicaid NEBRASKA – Medicaid
Website: http://www.in.gov/fssa Phone: 1-800-889-9949
Website: www.ACCESSNebraska.ne.gov
Phone: 1-800-383-4278
IOWA – Medicaid NEVADA – Medicaid Website: www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
Medicaid Website: http://dwss.nv.gov/
Medicaid Phone: 1-800-992-0900
KANSAS – Medicaid
Website: http://www.kdheks.gov/hcf/ Phone: 1-800-792-4884
KENTUCKY – Medicaid NEW HAMPSHIRE – Medicaid Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
Website: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf Phone: 603-271-5218
LOUISIANA – Medicaid NEW JERSEY – Medicaid and CHIP
Website: http://www.lahipp.dhh.louisiana.gov Phone: 1-888-695-2447
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
MAINE – Medicaid
Website: http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-977-6740 TTY 1-800-977-6741
MASSACHUSETTS – Medicaid and CHIP NEW YORK – Medicaid Website: http://www.mass.gov/MassHealth Phone: 1-800-462-1120
Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
MINNESOTA – Medicaid NORTH CAROLINA – Medicaid Website: http://www.dhs.state.mn.us/ Click on Health Care, then Medical Assistance Phone: 1-800-657-3629
Website: http://www.ncdhhs.gov/dma Phone: 919-855-4100
MISSOURI – Medicaid NORTH DAKOTA – Medicaid Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-800-755-2604

Page 30
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP) If you or your children are eligible for Medicaid or CHIP and you are eligible for health coverage from your employer, your State may have a premium assistance program that can help pay for coverage. These States use funds from their Medicaid or CHIP programs to help people who are eligible for these programs, but also have access to health insurance through their employer. If you or your children are not eligible for Medicaid or CHIP, you will not be eligible for these premium assistance programs. If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, you can contact your State Medicaid or CHIP office to find out if premium assistance is available. If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, you can contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, you can ask the State if it has a program that might help you pay the premiums for an employer-sponsored plan. Once it is determined that you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must permit you to enroll in your employer plan if you are not already enrolled. This is called a “special enroll-ment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, you can contact the Department of Labor electronically at www.askebsa.dol.gov or by calling toll-free 1-866-444-EBSA (3272). If you live in one of the following States, you may be eligible for assistance paying your employer health plan premiums. The following list of States is current as of July 31, 2013. You should contact your State for further information on eligibility.
ALABAMA – Medicaid COLORADO – Medicaid
Website: http://www.medicaid.alabama.gov Phone: 1-855-692-5447
Medicaid Website: http://www.colorado.gov/ Medicaid Phone (In state): 1-800-866-3513 Medicaid Phone (Out of state): 1-800-221-3943
ALASKA – Medicaid
Website: http://health.hss.state.ak.us/dpa/programs/medicaid/ Phone (Outside of Anchorage): 1-888-318-8890 Phone (Anchorage): 907-269-6529
ARIZONA – CHIP FLORIDA – Medicaid
Website: http://www.azahcccs.gov/applicants Phone (Outside of Maricopa County): 1-877-764-5437 Phone (Maricopa County): 602-417-5437
Website: https://www.flmedicaidtplrecovery.com/ Phone: 1-877-357-3268
GEORGIA – Medicaid
Website: http://dch.georgia.gov/ Click on Programs, then Medicaid, then Health Insurance Premium Payment (HIPP) Phone: 1-800-869-1150

Page 31
To see if any more States have added a premium assistance program since July 31, 2013, or for more information on special enrollment rights, you can contact either: U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565 OMB Control Number 1210-0137 (expires 09/30/2013)
OKLAHOMA – Medicaid and CHIP UTAH – Medicaid and CHIP
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
Website: http://health.utah.gov/upp Phone: 1-866-435-7414
OREGON – Medicaid and CHIP VERMONT– Medicaid
Website: http://www.oregonhealthykids.gov http://www.hijossaludablesoregon.gov Phone: 1-800-699-9075
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
PENNSYLVANIA – Medicaid VIRGINIA – Medicaid and CHIP
Website: http://www.dpw.state.pa.us/hipp Phone: 1-800-692-7462
Medicaid Website: http://www.dmas.virginia.gov/rcp-HIPP.htm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.famis.org/ CHIP Phone: 1-866-873-2647
RHODE ISLAND – Medicaid WASHINGTON – Medicaid
Website: www.ohhs.ri.gov Phone: 401-462-5300
Website: http://hrsa.dshs.wa.gov/premiumpymt/Apply.shtm Phone: 1-800-562-3022 ext. 15473
SOUTH CAROLINA – Medicaid WEST VIRGINIA – Medicaid
Website: http://www.scdhhs.gov Phone: 1-888-549-0820
Website: www.dhhr.wv.gov/bms/ Phone: 1-877-598-5820, HMS Third Party Liability
SOUTH DAKOTA - Medicaid WISCONSIN – Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: http://www.badgercareplus.org/pubs/p-10095.htm Phone: 1-800-362-3002
TEXAS – Medicaid WYOMING – Medicaid
Website: https://www.gethipptexas.com/ Phone: 1-800-440-0493
Website: http://health.wyo.gov/healthcarefin/equalitycare Phone: 307-777-7531


B
lue C
are E
lect S
aver
B
abso
n Co
llege
Su
mm
ary o
f Ben
efits
and
Cove
rage
: Wha
t this
Plan
Cov
ers &
Wha
t it C
osts
Cove
rage
Per
iod:
01/01
/2014
-12/3
1/201
4Co
vera
ge fo
r: Ind
ividu
al an
d Fam
ily | P
lan Ty
pe: P
PO
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at w
ww.b
luec
ross
ma.c
om/sb
cglo
ssar
y or c
all 1-
888-
543-
8770
to re
ques
t a co
py.
1 of 9
Blue
Cro
ss B
lue S
hield
of Ma
ssac
huse
tts is
an In
depe
nden
t Lice
nsee
of th
e Blue
Cro
ss an
d Blue
Shie
ld As
socia
tion
This
is on
ly a s
umm
ary.
If you
wan
t mor
e deta
il abo
ut yo
ur co
vera
ge an
d cos
ts, yo
u can
get th
e com
plete
terms
in th
e poli
cy or
plan
docu
ment
at
ww
w.b
luec
ross
ma.
com
or by
callin
g 1-8
88-5
43-8
770.
Impo
rtan
t Que
stio
nsA
nsw
ers
Why
this
Mat
ters
:
Wha
t is th
e ove
rall
dedu
ctib
le?
$1,50
0 ind
ividu
al co
ntrac
t / $3
,000
family
contr
act. D
oes n
ot ap
ply to
pr
even
tive c
are,
in-ne
twor
k pre
natal
ca
re
You m
ust p
ay al
l the c
osts
up to
the d
educ
tible
amou
nt be
fore t
his pl
an be
gins t
o pay
for c
over
ed
servi
ces y
ou us
e. Ch
eck y
our p
olicy
or pl
an do
cume
nt to
see w
hen t
he d
educ
tible
starts
over
(u
suall
y, bu
t not
alway
s, Ja
nuar
y 1st)
. See
the c
hart
startin
g on p
age 2
for h
ow m
uch y
ou pa
y for
co
vere
d ser
vices
after
you m
eet th
e ded
uctib
le.Ar
e the
re o
ther
de
duct
ibles
for s
pecifi
c se
rvice
s?No
.Yo
u don
’t hav
e to m
eet d
educ
tibles
for s
pecifi
c ser
vices
, but
see t
he ch
art s
tartin
g on p
age 2
for
other
costs
for s
ervic
es th
is pla
n cov
ers.
Is th
ere a
n ou
t-of-p
ocke
t lim
it on
my e
xpen
ses?
Yes.
$5,00
0 ind
ividu
al co
ntrac
t / $1
0,000
fami
ly co
ntrac
tTh
e out
-of-p
ocke
t lim
it is t
he m
ost y
ou co
uld pa
y dur
ing a
cove
rage
perio
d (us
ually
one y
ear)
for
your
shar
e of th
e cos
t of c
over
ed se
rvice
s. Th
is lim
it help
s you
plan
for h
ealth
care
expe
nses
.W
hat is
not
inclu
ded
in th
e ou
t-of-p
ocke
t lim
it?Pr
emium
s, ba
lance
-bille
d cha
rges
, and
he
alth c
are t
his pl
an do
esn’t
cove
r.Ev
en th
ough
you p
ay th
ese e
xpen
ses,
they d
on’t c
ount
towar
d the
out
-of-p
ocke
t lim
it.
Does
this
plan
use
a ne
twor
k of p
rovid
ers?
Yes.
See w
ww.b
luec
ross
ma.c
om/
finda
doct
or o
r call
1-80
0-82
1-13
88 fo
r a l
ist of
prefe
rred p
rovid
ers.
If you
use a
n in-
netw
ork d
octor
or ot
her h
ealth
care
pro
vider
, this
plan w
ill pa
y som
e or a
ll of
the co
sts of
cove
red s
ervic
es. B
e awa
re, y
our in
-netw
ork d
octor
or ho
spita
l may
use a
n out-
of-ne
twor
k pro
vider
for s
ome s
ervic
es. P
lans u
se th
e ter
m in-
netw
ork,
pref
erre
d, or
partic
ipatin
g for
pr
ovid
ers i
n the
ir net
work
. See
the c
hart
startin
g on p
age 2
for h
ow th
is pla
n pay
s diffe
rent
kinds
of
prov
ider
s.Do
I nee
d a r
efer
ral to
see
a spe
cialis
t?No
.Yo
u can
see t
he sp
ecial
ist yo
u cho
ose w
ithou
t per
miss
ion fr
om th
is pla
n.
Are t
here
serv
ices t
his
plan
doe
sn’t c
over
?Ye
s.So
me of
the s
ervic
es th
is pla
n doe
sn’t c
over
are l
isted
on pa
ge 6.
See
your
polic
y or p
lan do
cume
nt for
addit
ional
infor
matio
n abo
ut ex
clude
d se
rvice
s.

2 of 9
•Co
paym
ents
are fi
xed d
ollar
amou
nts (f
or ex
ample
, $15
) you
pay f
or co
vere
d hea
lth ca
re, u
suall
y whe
n you
rece
ive th
e ser
vice.
•Co
insu
ranc
e is y
our s
hare
of th
e cos
ts of
a cov
ered
servi
ce, c
alcula
ted as
a pe
rcent
of the
allo
wed
amou
nt (o
r pro
vider
’s ch
arge
if it i
s les
s tha
n the
allo
wed
amou
nt) fo
r the
servi
ce. F
or ex
ample
, if th
e plan
’s all
owed
amou
nt fo
r an o
vern
ight s
tay is
$1,00
0 (an
d it is
less
than
the p
rovid
er’s
char
ge),
your
coin
sura
nce
paym
ent o
f 20%
wou
ld be
$200
. This
may
chan
ge if
you h
aven
’t met
your
ded
uctib
le.•
The a
moun
t the p
lan pa
ys fo
r cov
ered
servi
ces i
s bas
ed on
the a
llowe
d am
ount
. If an
out-o
f-netw
ork p
rovid
er ch
arge
s mor
e tha
n the
allo
wed
amou
nt, y
ou
may h
ave t
o pay
the d
iffere
nce.
For e
xamp
le, if
an ou
t-of-n
etwor
k hos
pital
char
ges $
1,500
for a
n ove
rnigh
t stay
and t
he al
lowe
d am
ount
is $1
,000,
you m
ay
have
to pa
y the
$500
diffe
renc
e. (T
his is
calle
d bala
nce b
illing
.)•
This
plan m
ay en
cour
age y
ou to
use i
n-ne
twor
k pro
vider
s by c
harg
ing yo
u low
er d
educ
tibles
, cop
aym
ents
and c
oins
uran
ce a
moun
ts. (
If you
are e
ligibl
e to
elect
a Hea
lth R
eimbu
rseme
nt Ac
coun
t (HR
A), F
lexibl
e Spe
nding
Acc
ount
(FSA
) or y
ou ha
ve el
ected
a He
alth S
aving
s Acc
ount
(HSA
), yo
u may
have
ac
cess
to ad
dition
al fun
ds to
help
cove
r cer
tain o
ut-o
f-poc
ket e
xpen
ses s
uch a
s cop
aym
ents
, coi
nsur
ance
, ded
uctib
les an
d cos
ts re
lated
to se
rvice
s not
other
wise
cove
red.)
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
visit
a he
alth
care
pr
ovid
er’s
offic
e or c
linic
Prim
ary c
are v
isit to
trea
t an i
njury
or ill
ness
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
Spec
ialist
visit
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
Othe
r pra
ctitio
ner o
ffice v
isit
No ch
arge
/ ch
iropr
actor
visit
20%
coins
uran
ce /
chiro
prac
tor vi
sitDe
ducti
ble ap
plies
first
Prev
entiv
e car
e/scre
ening
/immu
nizati
onNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st for
out-o
f-ne
twor
k; lim
ited t
o age
base
d sch
edule
an
d / or
freq
uenc
y
If you
hav
e a te
st
Diag
nosti
c tes
t (x-r
ay, b
lood w
ork)
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
Imag
ing (C
T/PE
T sca
ns, M
RIs)
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first

3 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
nee
d dr
ugs t
o tre
at
your
illne
ss o
r con
ditio
n
More
infor
matio
n abo
ut pr
escr
iptio
n dr
ug
cove
rage
is av
ailab
le at
www.
blue
cros
sma.c
om.
Gene
ric dr
ugs
$10 /
retai
l or $
20
($10
for v
alue d
rugs
) / m
ail se
rvice
supp
ly$2
0 / re
tail
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; de
ducti
ble ap
plies
first;
cost
shar
e waiv
ed fo
r birth
contr
ol, sm
oking
ce
ssati
on an
d cer
tain o
rally
admi
nister
ed
antic
ance
r dru
gs; p
re-a
uthor
izatio
n re
quire
d for
certa
in dr
ugs
Prefe
rred b
rand
drug
s$2
5 / re
tail o
r $50
($
25 fo
r valu
e dru
gs)
servi
ce su
pply
$50 /
retai
l
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; de
ducti
ble ap
plies
first;
cost
shar
e waiv
ed fo
r smo
king c
essa
tion a
nd
certa
in or
ally a
dmini
stere
d anti
canc
er
drug
s; pr
e-au
thoriz
ation
requ
ired f
or
certa
in dr
ugs
Non-
prefe
rred b
rand
drug
s$4
5 / re
tail o
r $90
/ ma
il ser
vice s
upply
$90 /
retai
l
Up to
30-d
ay re
tail (9
0-da
y mail
se
rvice
) sup
ply; d
educ
tible
appli
es fir
st;
cost
shar
e waiv
ed fo
r cer
tain o
rally
ad
minis
tered
antic
ance
r dru
gs;
pre-
autho
rizati
on re
quire
d fo
certa
in dr
ugs
Spec
ialty
drug
sAp
plica
ble co
st sh
are
(gen
eric,
prefe
rred,
non-
prefe
rred
Not c
over
edW
hen o
btaine
d fro
m a d
esign
ated
spec
ialty
phar
macy
; pre
-auth
oriza
tion
requ
ired f
or ce
rtain
drug
sIf y
ou h
ave o
utpa
tient
su
rger
yFa
cility
fee (
e.g., a
mbula
tory s
urge
ry ce
nter)
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
Phys
ician
/surg
eon f
ees
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
If you
nee
d im
med
iate
med
ical a
ttent
ion
Emer
genc
y roo
m se
rvice
s$1
50 / v
isit
$150
/ visi
tDe
ducti
ble ap
plies
first;
copa
ymen
t wa
ived i
f adm
itted o
r for
obse
rvatio
n stay
Emer
genc
y med
ical tr
ansp
ortat
ionNo
char
geNo
char
geDe
ducti
ble ap
plies
first
Urge
nt ca
reNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st

4 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
hav
e a h
ospi
tal s
tay
Facil
ity fe
e (e.g
., hos
pital
room
)No
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; pr
e-au
thoriz
ation
re
quire
d
Phys
ician
/surg
eon f
eeNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; pr
e-au
thoriz
ation
re
quire
d
If you
hav
e men
tal h
ealth
, be
havio
ral h
ealth
, or
subs
tanc
e abu
se n
eeds
Menta
l/Beh
avior
al he
alth o
utpati
ent s
ervic
esNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st
Menta
l/Beh
avior
al he
alth i
npati
ent s
ervic
esNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; pr
e-au
thoriz
ation
re
quire
dSu
bstan
ce us
e diso
rder
outpa
tient
servi
ces
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
Subs
tance
use d
isord
er in
patie
nt se
rvice
sNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; pr
e-au
thoriz
ation
re
quire
d
If you
are p
regn
ant
Pren
atal a
nd po
stnata
l car
e
No ch
arge
for
pren
atal c
are;
no ch
arge
after
de
ducti
ble fo
r po
stnata
l car
e
20%
coins
uran
ceDe
ducti
ble ap
plies
first
for in
-netw
ork
postn
atal c
are a
nd ou
t-of-n
etwor
k for
pr
enata
l and
postn
atal c
are
Deliv
ery a
nd al
l inpa
tient
servi
ces
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first

5 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
nee
d he
lp
reco
verin
g or
hav
e oth
er
spec
ial h
ealth
nee
ds
Home
healt
h car
eNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; pr
e-au
thoriz
ation
re
quire
d
Reha
bilita
tion s
ervic
esNo
char
ge20
% co
insur
ance
Dedu
ctible
appli
es fir
st; lim
ited t
o 100
vis
its pe
r cale
ndar
year
(othe
r tha
n for
au
tism,
home
healt
h car
e, an
d spe
ech
thera
py)
Habil
itatio
n ser
vices
No ch
arge
20%
coins
uran
ce
Dedu
ctible
appli
es fir
st; re
habil
itatio
n the
rapy
cove
rage
limits
apply
; cos
t sha
re
and c
over
age l
imits
waiv
ed fo
r ear
ly int
erve
ntion
servi
ces f
or el
igible
child
ren
Skille
d nur
sing c
are
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first;
limite
d to 1
00
days
per c
alend
ar ye
ar; p
re-a
uthor
izatio
n re
quire
d
Dura
ble m
edica
l equ
ipmen
t20
% co
insur
ance
20%
coins
uran
ceDe
ducti
ble ap
plies
first;
in-n
etwor
k cos
t sh
are w
aived
for o
ne br
east
pump
per
birth
Hosp
ice se
rvice
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
If you
r chi
ld n
eeds
den
tal
or ey
e car
e
Eye e
xam
No ch
arge
20%
coins
uran
ceDe
ducti
ble ap
plies
first
for ou
t-of-
netw
ork;
limite
d to o
ne ex
am ev
ery 2
4 mo
nths
Glas
ses
Not c
over
edNo
t cov
ered
——
— no
ne —
——
Denta
l che
ck-u
p
No ch
arge
for
memb
ers w
ith a
cleft p
alate
/ clef
t lip
cond
ition
20%
coins
uran
ce
for m
embe
rs wi
th a
cleft p
alate
/ clef
t lip
cond
ition
Limite
d to m
embe
rs un
der a
ge 18
; de
ducti
ble ap
plies
first
out-o
f-netw
ork

6 of 9
Excl
uded
Ser
vice
s &
Oth
er C
over
ed S
ervi
ces:
•Ac
upun
cture
•Ch
ildre
n’s gl
asse
s
•Co
smeti
c sur
gery
•De
ntal c
are (
adult
)
•Lo
ng-te
rm ca
re
•Pr
ivate-
duty
nursi
ng
Serv
ices Y
our P
lan D
oes N
OT C
over
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er ex
clude
d se
rvice
s.)
•Ba
riatric
surg
ery
•Ch
iropr
actic
care
•He
aring
aids
($2,0
00 pe
r ear
ever
y 36 m
onths
for
memb
ers a
ge 21
or yo
unge
r)
•Inf
ertili
ty tre
atmen
t
•No
n-em
erge
ncy c
are w
hen t
rave
ling o
utside
the U
.S.
•Ro
utine
eye c
are -
adult
(limi
ted to
one e
xam
ever
y 24
mon
ths)
•Ro
utine
foot
care
(only
for p
atien
ts wi
th sy
stemi
c cir
culat
ory d
iseas
e)
•W
eight
loss p
rogr
ams (
three
mon
ths in
quali
fied
prog
ram(
s) pe
r con
tract
per c
alend
ar ye
ar)
Othe
r Cov
ered
Ser
vices
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er co
vere
d se
rvice
s and
your
cost
s for
thes
e ser
vices
.)

7 of 9
Your
Rig
hts
to C
ontin
ue C
over
age:
If you
lose
cove
rage
unde
r the
plan
, then
, dep
endin
g upo
n the
circu
mstan
ces,
Fede
ral a
nd S
tate l
aws m
ay pr
ovide
prote
ction
s tha
t allo
w yo
u to k
eep h
ealth
cove
rage
. Any
su
ch rig
hts m
ay be
limite
d in d
urati
on an
d will
requ
ire yo
u to p
ay a
prem
ium
, whic
h may
be si
gnific
antly
high
er th
an th
e pre
mium
you p
ay w
hile c
over
ed un
der t
he pl
an.
Othe
r limi
tation
s on y
our r
ights
to co
ntinu
e cov
erag
e may
also
apply
. Fo
r mor
e info
rmati
on on
your
rights
to co
ntinu
e cov
erag
e, co
ntact
your
plan
spon
sor. N
ote: A
plan
spon
sor is
usua
lly th
e mem
ber’s
emplo
yer o
r org
aniza
tion t
hat p
rovid
es
grou
p hea
lth co
vera
ge to
the m
embe
r. You
may
also
conta
ct yo
ur st
ate in
sura
nce d
epar
tmen
t, the
U.S
. Dep
artm
ent o
f Lab
or, E
mploy
ee B
enefi
ts Se
curity
Adm
inistr
ation
at
1-86
6-44
4-32
72 or
www
.dol.g
ov/eb
sa, o
r the
U.S
. Dep
artm
ent o
f Hea
lth an
d Hum
an S
ervic
es at
1-87
7-26
7-23
23 x6
1565
or w
ww.cc
iio.cm
s.gov
.
Your
Grie
vanc
e an
d A
ppea
ls R
ight
s:If y
ou ha
ve a
comp
laint
or ar
e diss
atisfi
ed w
ith a
denia
l of c
over
age f
or cl
aims u
nder
your
plan
, you
may
be ab
le to
appe
al or
file a
griev
ance
. For
ques
tions
abou
t you
r rig
hts, th
is no
tice,
or as
sistan
ce, y
ou ca
n con
tact th
e Mem
ber S
ervic
e num
ber li
sted o
n you
r ID
card
or co
ntact
your
plan
spon
sor. N
ote: A
plan
spon
sor is
usua
lly th
e me
mber
’s em
ploye
r or o
rgan
izatio
n tha
t pro
vides
grou
p hea
lth co
vera
ge to
the m
embe
r. .
Doe
s th
is C
over
age
Prov
ide
Min
imum
Ess
entia
l Cov
erag
e?Th
e Affo
rdab
le Ca
re A
ct re
quire
s mos
t peo
ple to
have
healt
h car
e cov
erag
e tha
t qua
lifies
as “m
inimu
m es
senti
al co
vera
ge.”
This
plan
or p
olicy
doe
s pro
vide m
inim
um
esse
ntial
cove
rage
.
Doe
s th
is C
over
age
Mee
t the
Min
imum
Val
ue S
tand
ard?
The A
fford
able
Care
Act
estab
lishe
s a m
inimu
m va
lue st
anda
rd of
bene
fits of
a he
alth p
lan. T
he m
inimu
m va
lue st
anda
rd is
60%
(actu
arial
value
). Th
is he
alth
cove
rage
do
es m
eet t
he m
inim
um va
lue s
tand
ard
for t
he b
enefi
ts it
prov
ides
.
Lang
uage
Ass
ista
nce
D
iscl
aim
er:
This
docu
ment
conta
ins on
ly a p
artia
l des
cripti
on of
the b
enefi
ts, lim
itatio
ns, e
xclus
ions a
nd ot
her p
rovis
ions o
f this
healt
h car
e plan
. It is
not a
polic
y. It i
s a ge
nera
l ove
rview
on
ly. It
does
not p
rovid
e all t
he de
tails
of thi
s cov
erag
e, inc
luding
bene
fits, e
xclus
ions a
nd po
licy l
imita
tions
. In th
e eve
nt the
re ar
e disc
repa
ncies
betw
een t
his do
cume
nt an
d the
polic
y, the
term
s and
cond
itions
of th
e poli
cy w
ill go
vern
.
To se
e exa
mples
of ho
w thi
s plan
migh
t cov
er co
sts fo
r a sa
mple
medic
al sit
uatio
n, se
e the
next
page
.

8 of 9
Abo
ut th
ese
Cov
erag
e Ex
ampl
es:
Thes
e exa
mples
show
how
this p
lan m
ight
cove
r med
ical c
are i
n give
n situ
ation
s. Us
e the
se ex
ample
s to s
ee, in
gene
ral, h
ow m
uch
finan
cial p
rotec
tion a
samp
le pa
tient
migh
t ge
t if th
ey ar
e cov
ered
unde
r diffe
rent
plans
.
This
is
not a
cos
t es
timat
or.
Don’t
use t
hese
exam
ples t
o esti
mate
your
actua
l cos
ts un
der t
his pl
an.
The a
ctual
care
you r
eceiv
e will
be
differ
ent fr
om th
ese e
xamp
les, a
nd
the co
st of
that c
are a
lso w
ill be
dif
feren
t.
See t
he ne
xt pa
ge fo
r impo
rtant
infor
matio
n abo
ut the
se ex
ample
s.
Hav
ing
a ba
by(n
orm
al d
eliv
ery)
n A
mou
nt o
wed
to p
rovid
ers:
$7,5
40n
Plan
pay
s $4
,370
n P
atien
t Pay
s $3
,170
Sam
ple c
are c
osts
:Ho
spita
l cha
rges
(moth
er)
$2,70
0Ro
utine
obste
tric ca
re$2
,100
Hosp
ital c
harg
es (b
aby)
$900
Anes
thesia
$900
Labo
rator
y tes
ts$5
00Pr
escri
ption
s$2
00Ra
diolog
y$2
00Va
ccine
s, oth
er pr
even
tive
$40
Tota
l$7
,540
Patie
nt P
ays:
Dedu
ctible
s$3
,000
Copa
ys$2
0Co
insur
ance
$0Lim
its or
exclu
sions
$150
Tota
l$3
,170
Man
agin
g ty
pe 2
dia
bete
s(ro
utin
e m
aint
enan
ce o
f a w
ell-c
ontro
lled
cond
ition
)
n A
mou
nt o
wed
to p
rovid
ers:
$5,4
00n
Plan
pay
s $1
,440
n P
atien
t Pay
s $3
,960
Sam
ple c
are c
osts
:Pr
escri
ption
s$2
,900
Medic
al Eq
uipme
nt an
d Sup
plies
$1,30
0Of
fice V
isits
and P
roce
dure
s$7
00Ed
ucati
on$3
00La
bora
tory t
ests
$100
Vacc
ines,
other
prev
entiv
e$1
00To
tal
$5,40
0
Patie
nt P
ays:
Dedu
ctible
s$3
,000
Copa
ys$8
80Co
insur
ance
$0Lim
its or
exclu
sions
$80
Tota
l$3
,960

9 of 9
Que
stio
ns a
nd a
nsw
ers
abou
t the
Cov
erag
e Ex
ampl
es:
Wha
t are
som
e of t
he as
sum
ptio
ns
behi
nd th
e Cov
erag
e Exa
mpl
es?
•Co
sts do
n’t in
clude
pre
miu
ms.
•Sa
mple
care
costs
are b
ased
on na
tiona
l ave
rage
s su
pplie
d to t
he U
.S. D
epar
tmen
t of H
ealth
and
Huma
n Ser
vices
, and
aren
’t spe
cific t
o a pa
rticula
r ge
ogra
phic
area
or he
alth p
lan.
•Th
e pati
ent’s
cond
ition w
as no
t an e
xclud
ed or
pr
eexis
ting c
ondit
ion.
•Al
l ser
vices
and t
reatm
ents
starte
d and
ende
d in
the sa
me co
vera
ge pe
riod.
•Th
ere a
re no
othe
r med
ical e
xpen
ses f
or an
y me
mber
cove
red u
nder
this
plan.
•Ou
t-of-p
ocke
t exp
ense
s are
base
d only
on tr
eatin
g the
cond
ition i
n the
exam
ple.
•Th
e pati
ent r
eceiv
ed al
l car
e fro
m in-
netw
ork
prov
ider
s. If t
he pa
tient
had r
eceiv
ed ca
re fr
om
out-o
f-netw
ork p
rovid
ers,
costs
wou
ld ha
ve be
en
highe
r.•
The p
atien
t is en
rolle
d in a
fami
ly pla
n.
Wha
t doe
s a C
over
age E
xam
ple
show
?Fo
r eac
h tre
atmen
t situ
ation
, the C
over
age E
xamp
le he
lps yo
u see
how
dedu
ctib
les, c
opay
men
ts, a
nd
coin
sura
nce c
an ad
d up.
It also
helps
you s
ee w
hat
expe
nses
migh
t be l
eft up
to yo
u to p
ay be
caus
e the
servi
ce or
trea
tmen
t isn’t
cove
red o
r pay
ment
is lim
ited.
Does
the C
over
age E
xam
ple p
redi
ct m
y ow
n ca
re n
eeds
?
û N
o. Tr
eatm
ents
show
n are
just
exam
ples.
The
care
you w
ould
rece
ive fo
r this
cond
ition c
ould
be
differ
ent b
ased
on yo
ur do
ctor’s
advic
e, yo
ur ag
e, ho
w se
rious
your
cond
ition i
s, an
d man
y othe
r fac
tors.
Does
the C
over
age E
xam
ple p
redi
ct m
y fu
ture
expe
nses
?
û N
o. Co
vera
ge E
xamp
les ar
e not
cost
estim
ators.
You c
an’t u
se th
e exa
mples
to
estim
ate co
sts fo
r an a
ctual
cond
ition.
They
ar
e for
comp
arati
ve pu
rpos
es on
ly. Yo
ur ow
n co
sts w
ill be
diffe
rent
depe
nding
on th
e car
e you
re
ceive
, the p
rices
your
pro
vider
s cha
rge,
and
the re
imbu
rseme
nt yo
ur he
alth p
lan al
lows.
Can
I use
Cov
erag
e Exa
mpl
es to
co
mpa
re p
lans?
üYe
s. W
hen y
ou lo
ok at
the S
umma
ry of
Bene
fits
and C
over
age f
or ot
her p
lans,
you’l
l find
the
same
Cov
erag
e Exa
mples
. Whe
n you
comp
are
plans
, che
ck th
e “Pa
tient
Pays
” box
in ea
ch
exam
ple. T
he sm
aller
that
numb
er, th
e mor
e co
vera
ge th
e plan
prov
ides .
Are t
here
oth
er co
sts I
shou
ld co
nsid
er
when
com
parin
g pl
ans?
üYe
s. An
impo
rtant
cost
is the
pre
miu
m yo
u pa
y. Ge
nera
lly, th
e low
er yo
ur p
rem
ium
, the
more
you’l
l pay
in ou
t-of-p
ocke
t cos
ts, su
ch as
co
paym
ents
, ded
uctib
les, a
nd co
insu
ranc
e. Yo
u also
shou
ld co
nside
r con
tributi
ons t
o ac
coun
ts su
ch as
healt
h sav
ings a
ccou
nts
(HSA
s), fle
xible
spen
ding a
rrang
emen
ts (F
SAs)
or he
alth r
eimbu
rseme
nt ac
coun
ts (H
RAs)
that
help
you p
ay ou
t-of-p
ocke
t exp
ense
s.
® Re
gister
ed M
arks
of th
e Blue
Cro
ss an
d Blue
Shie
ld As
socia
tion.©
2013
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
, Inc.,
and
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
HMO
Blue
, Inc.
11
3023
4BS
(9/13
) 4C
JI
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at w
ww.b
luec
ross
ma.c
om/sb
cglo
ssar
y or c
all 1-
888-
543-
8770
to re
ques
t a co
py.


This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect as of January 1, 2014, as part of the Massachusetts Health Care Reform Law.
MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2013 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 129108 55-0647 (7/13) 150M


HMO
Blu
e New
Eng
land
Valu
e Plu
s B
abso
n Co
llege
Hig
h Op
tion
Sum
mar
y of B
enefi
ts an
d Co
vera
ge: W
hat th
is Pl
an C
over
s & W
hat it
Cos
ts
C
over
age P
erio
d: 0
1/01/2
014 -
12/31
/2014
Cove
rage
for:
Indivi
dual
and F
amily
| Plan
Type
: HMO
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at ww
w.bl
uecr
ossm
a.com
/sbcg
loss
ary o
r call
1-88
8-54
3-87
70 to
requ
est a
copy
.1 o
f 9Bl
ue C
ross
Blue
Shie
ld of
Mass
achu
setts
is an
Inde
pend
ent L
icens
ee of
the B
lue C
ross
and B
lue S
hield
Asso
ciatio
n
This
is on
ly a s
umm
ary.
If you
wan
t mor
e deta
il abo
ut yo
ur co
vera
ge an
d cos
ts, yo
u can
get th
e com
plete
terms
in th
e poli
cy or
plan
docu
ment
at ww
w.bl
uecr
ossm
a.com
or by
callin
g 1-8
88-5
43-8
770 .
Impo
rtan
t Que
stio
nsA
nsw
ers
Why
this
Mat
ters
:W
hat is
the o
vera
ll de
duct
ible?
$0Se
e the
char
t star
ting o
n pag
e 2 fo
r you
r cos
ts for
servi
ces t
his pl
an co
vers.
Are t
here
oth
er
dedu
ctib
les fo
r spe
cific
serv
ices?
No.
You d
on’t h
ave t
o mee
t ded
uctib
les fo
r spe
cific s
ervic
es, b
ut se
e the
char
t star
ting o
n pag
e 2 fo
r oth
er co
sts fo
r ser
vices
this
plan c
over
s.
Is th
ere a
n ou
t-of-p
ocke
t lim
it on
my e
xpen
ses?
Yes.
$1,00
0 mem
ber /
$2,00
0 fam
ilyTh
e out
-of-p
ocke
t lim
it is t
he m
ost y
ou co
uld pa
y dur
ing a
cove
rage
perio
d (us
ually
one y
ear)
for
your
shar
e of th
e cos
t of c
over
ed se
rvice
s. Th
is lim
it help
s you
plan
for h
ealth
care
expe
nses
.
Wha
t is n
ot in
clude
d in
the
out-o
f-poc
ket li
mit?
Prem
iums,
pres
cripti
on dr
ugs,
balan
ce-
billed
char
ges,
and h
ealth
care
this
plan
does
n’t co
ver.
Even
thou
gh yo
u pay
thes
e exp
ense
s, the
y don
’t cou
nt tow
ard t
he o
ut-o
f-poc
ket li
mit.
Does
this
plan
use
a ne
twor
k of p
rovid
ers?
Yes.
See w
ww.b
luec
ross
ma.c
om/
finda
doct
or o
r call
1-80
0-82
1-13
88 fo
r a l
ist of
netw
ork p
rovid
ers.
If you
use a
n in-
netw
ork d
octor
or ot
her h
ealth
care
pro
vider
, this
plan w
ill pa
y som
e or a
ll of
the co
sts of
cove
red s
ervic
es. B
e awa
re, y
our in
-netw
ork d
octor
or ho
spita
l may
use a
n out-
of-ne
twor
k pro
vider
for s
ome s
ervic
es. P
lans u
se th
e ter
m in-
netw
ork,
pref
erre
d, or
partic
ipatin
g for
pr
ovid
ers i
n the
ir net
work
. See
the c
hart
startin
g on p
age 2
for h
ow th
is pla
n pay
s diffe
rent
kinds
of
prov
ider
s.Do
I nee
d a r
efer
ral to
see
a spe
cialis
t?Ye
s.Th
is pla
n will
pay s
ome o
r all o
f the c
osts
to se
e a sp
ecial
ist fo
r cov
ered
servi
ces b
ut on
ly if y
ou
have
the p
lan’s
perm
ission
befor
e you
see t
he sp
ecial
ist.
Are t
here
serv
ices t
his
plan
doe
sn’t c
over
?Ye
s.So
me of
the s
ervic
es th
is pla
n doe
sn’t c
over
are l
isted
on pa
ge 6.
See
your
polic
y or p
lan do
cume
nt for
addit
ional
infor
matio
n abo
ut ex
clude
d se
rvice
s.
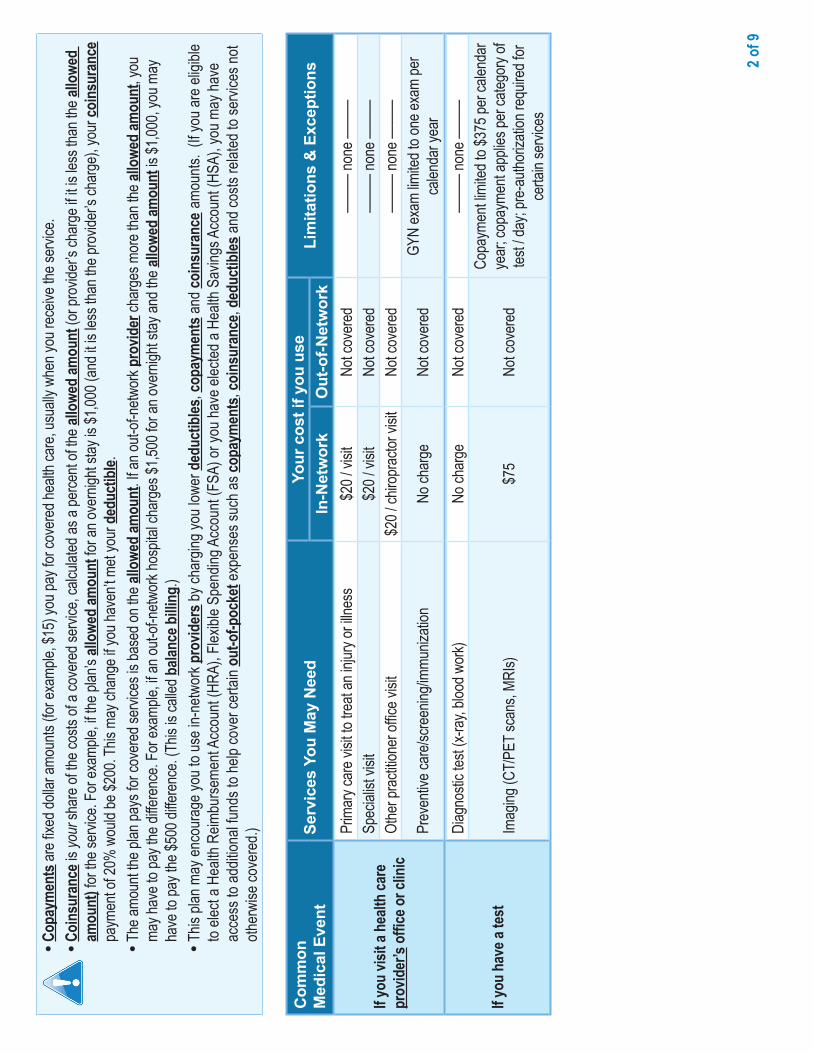
2 of 9
•Co
paym
ents
are fi
xed d
ollar
amou
nts (f
or ex
ample
, $15
) you
pay f
or co
vere
d hea
lth ca
re, u
suall
y whe
n you
rece
ive th
e ser
vice.
•Co
insu
ranc
e is y
our s
hare
of th
e cos
ts of
a cov
ered
servi
ce, c
alcula
ted as
a pe
rcent
of the
allo
wed
amou
nt (o
r pro
vider
’s ch
arge
if it i
s les
s tha
n the
allo
wed
amou
nt) fo
r the
servi
ce. F
or ex
ample
, if th
e plan
’s all
owed
amou
nt fo
r an o
vern
ight s
tay is
$1,00
0 (an
d it is
less
than
the p
rovid
er’s
char
ge),
your
coin
sura
nce
paym
ent o
f 20%
wou
ld be
$200
. This
may
chan
ge if
you h
aven
’t met
your
ded
uctib
le.•
The a
moun
t the p
lan pa
ys fo
r cov
ered
servi
ces i
s bas
ed on
the a
llowe
d am
ount
. If an
out-o
f-netw
ork p
rovid
er ch
arge
s mor
e tha
n the
allo
wed
amou
nt, y
ou
may h
ave t
o pay
the d
iffere
nce.
For e
xamp
le, if
an ou
t-of-n
etwor
k hos
pital
char
ges $
1,500
for a
n ove
rnigh
t stay
and t
he al
lowe
d am
ount
is $1
,000,
you m
ay
have
to pa
y the
$500
diffe
renc
e. (T
his is
calle
d bala
nce b
illing
.)•
This
plan m
ay en
cour
age y
ou to
use i
n-ne
twor
k pro
vider
s by c
harg
ing yo
u low
er d
educ
tibles
, cop
aym
ents
and c
oins
uran
ce a
moun
ts. (
If you
are e
ligibl
e to
elect
a Hea
lth R
eimbu
rseme
nt Ac
coun
t (HR
A), F
lexibl
e Spe
nding
Acc
ount
(FSA
) or y
ou ha
ve el
ected
a He
alth S
aving
s Acc
ount
(HSA
), yo
u may
have
ac
cess
to ad
dition
al fun
ds to
help
cove
r cer
tain o
ut-o
f-poc
ket e
xpen
ses s
uch a
s cop
aym
ents
, coi
nsur
ance
, ded
uctib
les an
d cos
ts re
lated
to se
rvice
s not
other
wise
cove
red.)
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
visit
a he
alth
care
pr
ovid
er’s
offic
e or c
linic
Prim
ary c
are v
isit to
trea
t an i
njury
or ill
ness
$20 /
visit
Not c
over
ed—
——
none
——
—Sp
ecial
ist vi
sit$2
0 / vi
sitNo
t cov
ered
——
— no
ne —
——
Othe
r pra
ctitio
ner o
ffice v
isit
$20 /
chiro
prac
tor vi
sitNo
t cov
ered
——
— no
ne —
——
Prev
entiv
e car
e/scre
ening
/immu
nizati
onNo
char
geNo
t cov
ered
GYN
exam
limite
d to o
ne ex
am pe
r ca
lenda
r yea
r
If you
hav
e a te
st
Diag
nosti
c tes
t (x-r
ay, b
lood w
ork)
No ch
arge
Not c
over
ed—
——
none
——
—
Imag
ing (C
T/PE
T sca
ns, M
RIs)
$75
Not c
over
ed
Copa
ymen
t limi
ted to
$375
per c
alend
ar
year
; cop
ayme
nt ap
plies
per c
atego
ry of
tes
t / da
y; pr
e-au
thoriz
ation
requ
ired f
or
certa
in se
rvice
s

3 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
nee
d dr
ugs t
o tre
at
your
illne
ss o
r con
ditio
n
More
info
rmat
ion
abou
t pr
escr
iptio
n dr
ug
cove
rage
is av
ailab
le at
ww
w.bl
uecr
ossm
a.com
.
Gene
ric dr
ugs
$10 /
retai
l or $
20
($10
for v
alue d
rugs
) / m
ail se
rvice
supp
lyNo
t cov
ered
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for b
irth
contr
ol, sm
oking
cess
ation
and c
ertai
n or
ally a
dmini
stere
d anti
canc
er dr
ugs;
pre-
autho
rizati
on re
quire
d for
certa
in dr
ugs
Prefe
rred b
rand
drug
s$2
5 / re
tail o
r $50
($
25 fo
r valu
e dru
gs)
servi
ce su
pply
Not c
over
ed
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for s
mokin
g ce
ssati
on an
d cer
tain o
rally
admi
nister
ed
antic
ance
r dru
gs; p
re-a
uthor
izatio
n re
quire
d for
certa
in dr
ugs
Non-
prefe
rred b
rand
drug
s$4
5 / re
tail o
r $90
/ ma
il ser
vice s
upply
Not c
over
ed
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for c
ertai
n or
ally a
dmini
stere
d anti
canc
er dr
ugs;
pre-
autho
rizati
on re
quire
d for
certa
in dr
ugs
Spec
ialty
drug
sAp
plica
ble co
st sh
are
(gen
eric,
prefe
rred,
non-
prefe
rred)
Not c
over
edW
hen o
btaine
d fro
m a d
esign
ated
spec
ialty
phar
macy
; pre
-auth
oriza
tion
requ
ired f
or ce
rtain
drug
s
If you
hav
e out
patie
nt
surg
ery
Facil
ity fe
e (e.g
., amb
ulator
y sur
gery
cente
r)$1
50 / a
dmisi
son
Not c
over
edPr
e-au
thoriz
ation
requ
ired f
or ce
rtain
servi
ces
Phys
ician
/surg
eon f
ees
No ch
arge
Not c
over
edPr
e-au
thoriz
ation
requ
ired f
or ce
rtain
servi
ces
If you
nee
d im
med
iate
med
ical a
ttent
ion
Emer
genc
y roo
m se
rvice
s$1
50 / v
isit
$150
/ visi
tCo
apym
ent w
aived
if ad
mitte
d or f
or
obse
rvatio
n stay
Emer
genc
y med
ical tr
ansp
ortat
ionNo
char
geNo
char
ge—
——
none
——
—
Urge
nt ca
re$2
0 / vi
sit$2
0 / vi
sitOu
t-of-n
etwor
k cov
erag
e lim
ited t
o out
of se
rvice
area

4 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
hav
e a h
ospi
tal s
tay
Facil
ity fe
e (e.g
., hos
pital
room
)$2
50 / a
dmiss
ionNo
t cov
ered
Pre-
autho
rizati
on re
quire
d
Phys
ician
/surg
eon f
eeNo
char
geNo
t cov
ered
Pre-
autho
rizati
on re
quire
d
If you
hav
e men
tal h
ealth
, be
havio
ral h
ealth
, or
subs
tanc
e abu
se n
eeds
Menta
l/Beh
avior
al he
alth o
utpati
ent s
ervic
es$2
0 / vi
sitNo
t cov
ered
Pre-
autho
rizati
on re
quire
d for
certa
in se
rvice
sMe
ntal/B
ehav
ioral
healt
h inp
atien
t ser
vices
$250
/ adm
ission
Not c
over
edPr
e-au
thoriz
ation
requ
ired
Subs
tance
use d
isord
er ou
tpatie
nt se
rvice
s$2
0 / vi
sitNo
t cov
ered
Pre-
autho
rizati
on re
quire
d for
certa
in se
rvice
sSu
bstan
ce us
e diso
rder
inpa
tient
servi
ces
$250
/ adm
ission
Not c
over
edPr
e-au
thoriz
ation
requ
ired
If you
are p
regn
ant
Pren
atal a
nd po
stnata
l car
eNo
char
geNo
t cov
ered
——
— no
ne —
——
Deliv
ery a
nd al
l inpa
tient
servi
ces
$250
/ adm
ission
Not c
over
ed—
——
none
——
—
If you
nee
d he
lp
reco
verin
g or
hav
e oth
er
spec
ial h
ealth
nee
ds
Home
healt
h car
eNo
char
geNo
t cov
ered
Pre-
autho
rizati
on re
quire
d
Reha
bilita
tion s
ervic
es$2
0 / vi
sitNo
t cov
ered
Limite
d to 6
0 visi
ts pe
r cale
ndar
year
(o
ther t
han f
or au
tism,
home
healt
h car
e, an
d spe
ech t
hera
py)
Habil
itatio
n ser
vices
$20 /
visit
Not c
over
ed
Reha
bilita
tion t
hera
py co
vera
ge lim
its
apply
; cos
t sha
re an
d cov
erag
e lim
its
waive
d for
early
inter
venti
on se
rvice
s for
eli
gible
child
ren
Skille
d nur
sing c
are
No ch
arge
Not c
over
edLim
ited t
o 100
days
per c
alend
ar ye
ar;
pre-
autho
rizati
on re
quire
d
Dura
ble m
edica
l equ
ipmen
t20
% co
insur
ance
Not c
over
edCo
st sh
are w
aived
for o
ne br
east
pump
pe
r birth
Hosp
ice se
rvice
No ch
arge
Not c
over
edPr
e-au
thoriz
ation
requ
ired f
or ce
rtain
servi
ces

5 of 9
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
r chi
ld n
eeds
den
tal
or ey
e car
e
Eye e
xam
No ch
arge
Not c
over
edLim
ited t
o one
exam
ever
y 24 m
onths
Glas
ses
Not c
over
edNo
t cov
ered
——
— no
ne —
——
Denta
l che
ck-u
pNo
char
geNo
t cov
ered
Limite
d to c
hildr
en un
der a
ge 12
(eve
ry 6 m
onths
) and
unde
r age
18 w
ith a
cleft
palat
e / cl
eft lip
cond
ition

6 of 9
Excl
uded
Ser
vice
s &
Oth
er C
over
ed S
ervi
ces:
•Ac
upun
cture
•Ch
ildre
n’s gl
asse
s
•Co
smeti
c sur
gery
•De
ntal c
are (
adult
)
•Lo
ng-te
rm ca
re
•No
n-em
erge
ncy c
are w
hen t
rave
ling o
utside
the U
.S.
•Pr
ivate-
duty
nursi
ng
Serv
ices Y
our P
lan D
oes N
OT C
over
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er ex
clude
d se
rvice
s.)
•Ba
riatric
surg
ery
•Ch
iropr
actic
care
•He
aring
aids
($2,0
00 pe
r ear
ever
y 36 m
onths
for
memb
ers a
ge 21
or yo
unge
r)
•Inf
ertili
ty tre
atmen
t
•Ro
utine
eye c
are -
adult
(limi
ted to
one e
xam
ever
y 24
mon
ths)
•Ro
utine
foot
care
(only
for p
atien
ts wi
th sy
stemi
c cir
culat
ory d
iseas
e)
•W
eight
loss p
rogr
ams (
three
mon
ths in
quali
fied
prog
ram(
s) pe
r con
tract
per c
alend
ar ye
ar)
Othe
r Cov
ered
Ser
vices
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er co
vere
d se
rvice
s and
your
cost
s for
thes
e ser
vices
.)

7 of 9
Your
Rig
hts
to C
ontin
ue C
over
age:
If you
lose
cove
rage
unde
r the
plan
, then
, dep
endin
g upo
n the
circu
mstan
ces,
Fede
ral a
nd S
tate l
aws m
ay pr
ovide
prote
ction
s tha
t allo
w yo
u to k
eep h
ealth
cove
rage
. Any
su
ch rig
hts m
ay be
limite
d in d
urati
on an
d will
requ
ire yo
u to p
ay a
prem
ium
, whic
h may
be si
gnific
antly
high
er th
an th
e pre
mium
you p
ay w
hile c
over
ed un
der t
he pl
an.
Othe
r limi
tation
s on y
our r
ights
to co
ntinu
e cov
erag
e may
also
apply
. Fo
r mor
e info
rmati
on on
your
rights
to co
ntinu
e cov
erag
e, co
ntact
your
plan
spon
sor. N
ote: A
plan
spon
sor is
usua
lly th
e mem
ber’s
emplo
yer o
r org
aniza
tion t
hat p
rovid
es
grou
p hea
lth co
vera
ge to
the m
embe
r. You
may
also
conta
ct yo
ur st
ate in
sura
nce d
epar
tmen
t, the
U.S
. Dep
artm
ent o
f Lab
or, E
mploy
ee B
enefi
ts Se
curity
Adm
inistr
ation
at
1-86
6-44
4-32
72 or
www
.dol.g
ov/eb
sa, o
r the
U.S
. Dep
artm
ent o
f Hea
lth an
d Hum
an S
ervic
es at
1-87
7-26
7-23
23 x6
1565
or w
ww.cc
iio.cm
s.gov
.Yo
ur G
rieva
nce
and
App
eals
Rig
hts:
If you
have
a co
mplai
nt or
are d
issati
sfied
with
a de
nial o
f cov
erag
e for
claim
s und
er yo
ur pl
an, y
ou m
ay be
able
to ap
peal
or fil
e a gr
ievan
ce. F
or qu
estio
ns ab
out y
our
rights
, this
notic
e, or
assis
tance
, you
can c
ontac
t the M
embe
r Ser
vice n
umbe
r liste
d on y
our I
D ca
rd or
conta
ct yo
ur pl
an sp
onso
r. Note
: A pl
an sp
onso
r is us
ually
the
memb
er’s
emplo
yer o
r org
aniza
tion t
hat p
rovid
es gr
oup h
ealth
cove
rage
to th
e mem
ber. .
Doe
s th
is C
over
age
Prov
ide
Min
imum
Ess
entia
l Cov
erag
e?Th
e Affo
rdab
le Ca
re A
ct re
quire
s mos
t peo
ple to
have
healt
h car
e cov
erag
e tha
t qua
lifies
as “m
inimu
m es
senti
al co
vera
ge.”
This
plan
or p
olicy
doe
s pro
vide m
inim
um
esse
ntial
cove
rage
.
Doe
s th
is C
over
age
Mee
t the
Min
imum
Val
ue S
tand
ard?
The A
fford
able
Care
Act
estab
lishe
s a m
inimu
m va
lue st
anda
rd of
bene
fits of
a he
alth p
lan. T
he m
inimu
m va
lue st
anda
rd is
60%
(actu
arial
value
). Th
is he
alth
cove
rage
do
es m
eet t
he m
inim
um va
lue s
tand
ard
for t
he b
enefi
ts it
prov
ides
.
Lang
uage
Ass
ista
nce
D
iscl
aim
er:
This
docu
ment
conta
ins on
ly a p
artia
l des
cripti
on of
the b
enefi
ts, lim
itatio
ns, e
xclus
ions a
nd ot
her p
rovis
ions o
f this
healt
h car
e plan
. It is
not a
polic
y. It i
s a ge
nera
l ove
rview
on
ly. It
does
not p
rovid
e all t
he de
tails
of thi
s cov
erag
e, inc
luding
bene
fits, e
xclus
ions a
nd po
licy l
imita
tions
. In th
e eve
nt the
re ar
e disc
repa
ncies
betw
een t
his do
cume
nt an
d the
polic
y, the
term
s and
cond
itions
of th
e poli
cy w
ill go
vern
.
To se
e exa
mples
of ho
w thi
s plan
migh
t cov
er co
sts fo
r a sa
mple
medic
al sit
uatio
n, se
e the
next
page
.

8 of 9
Abo
ut th
ese
C
over
age
Exam
ples
:
Thes
e exa
mples
show
how
this p
lan m
ight
cove
r med
ical c
are i
n give
n situ
ation
s. Us
e the
se ex
ample
s to s
ee, in
gene
ral, h
ow m
uch
finan
cial p
rotec
tion a
samp
le pa
tient
migh
t ge
t if th
ey ar
e cov
ered
unde
r diffe
rent
plans
.
This
is
not a
cos
t es
timat
or.
Don’t
use t
hese
exam
ples t
o esti
mate
your
actua
l cos
ts un
der t
his pl
an.
The a
ctual
care
you r
eceiv
e will
be
differ
ent fr
om th
ese e
xamp
les, a
nd
the co
st of
that c
are a
lso w
ill be
dif
feren
t.
See t
he ne
xt pa
ge fo
r impo
rtant
infor
matio
n abo
ut the
se ex
ample
s.
Hav
ing
a ba
by(n
orm
al d
eliv
ery)
n A
mou
nt o
wed
to p
rovid
ers:
$7,5
40n
Plan
pay
s $7
,120
n P
atien
t Pay
s $4
20
Sam
ple c
are c
osts
:Ho
spita
l cha
rges
(moth
er)
$2,70
0Ro
utine
obste
tric ca
re$2
,100
Hosp
ital c
harg
es (b
aby)
$900
Anes
thesia
$900
Labo
rator
y tes
ts$5
00Pr
escri
ption
s$2
00Ra
diolog
y$2
00Va
ccine
s, oth
er pr
even
tive
$40
Tota
l$7
,540
Patie
nt P
ays:
Dedu
ctible
s$0
Copa
ys$2
70Co
insur
ance
$0Lim
its or
exclu
sions
$150
Tota
l$4
20
Man
agin
g ty
pe 2
dia
bete
s(ro
utin
e m
aint
enan
ce o
f a w
ell-c
ontro
lled
cond
ition
)
n A
mou
nt o
wed
to p
rovid
ers:
$5,4
00n
Plan
pay
s $5
,140
n P
atien
t Pay
s $2
60
Sam
ple c
are c
osts
:Pr
escri
ption
s$2
,900
Medic
al Eq
uipme
nt an
d Sup
plies
$1,30
0Of
fice V
isits
and P
roce
dure
s$7
00Ed
ucati
on$3
00La
bora
tory t
ests
$100
Vacc
ines,
other
prev
entiv
e$1
00To
tal
$5,40
0
Patie
nt P
ays:
Dedu
ctible
s$0
Copa
ys$1
80Co
insur
ance
$0Lim
its or
exclu
sions
$80
Tota
l$2
60

9 of 9
Que
stio
ns a
nd a
nsw
ers
abou
t the
Cov
erag
e Ex
ampl
es:
Wha
t are
som
e of t
he as
sum
ptio
ns
behi
nd th
e Cov
erag
e Exa
mpl
es?
•Co
sts do
n’t in
clude
pre
miu
ms.
•Sa
mple
care
costs
are b
ased
on na
tiona
l ave
rage
s su
pplie
d to t
he U
.S. D
epar
tmen
t of H
ealth
and
Huma
n Ser
vices
, and
aren
’t spe
cific t
o a pa
rticula
r ge
ogra
phic
area
or he
alth p
lan.
•Th
e pati
ent’s
cond
ition w
as no
t an e
xclud
ed or
pr
eexis
ting c
ondit
ion.
•Al
l ser
vices
and t
reatm
ents
starte
d and
ende
d in
the sa
me co
vera
ge pe
riod.
•Th
ere a
re no
othe
r med
ical e
xpen
ses f
or an
y me
mber
cove
red u
nder
this
plan.
•Ou
t-of-p
ocke
t exp
ense
s are
base
d only
on tr
eatin
g the
cond
ition i
n the
exam
ple.
•Th
e pati
ent r
eceiv
ed al
l car
e fro
m in-
netw
ork
prov
ider
s. If t
he pa
tient
had r
eceiv
ed ca
re fr
om
out-o
f-netw
ork p
rovid
ers,
costs
wou
ld ha
ve be
en
highe
r.
Wha
t doe
s a C
over
age E
xam
ple
show
?Fo
r eac
h tre
atmen
t situ
ation
, the C
over
age E
xamp
le he
lps yo
u see
how
dedu
ctib
les, c
opay
men
ts, a
nd
coin
sura
nce c
an ad
d up.
It also
helps
you s
ee w
hat
expe
nses
migh
t be l
eft up
to yo
u to p
ay be
caus
e the
servi
ce or
trea
tmen
t isn’t
cove
red o
r pay
ment
is lim
ited.
Does
the C
over
age E
xam
ple p
redi
ct m
y ow
n ca
re n
eeds
?
û N
o. Tr
eatm
ents
show
n are
just
exam
ples.
The
care
you w
ould
rece
ive fo
r this
cond
ition c
ould
be
differ
ent b
ased
on yo
ur do
ctor’s
advic
e, yo
ur ag
e, ho
w se
rious
your
cond
ition i
s, an
d man
y othe
r fac
tors.
Does
the C
over
age E
xam
ple p
redi
ct m
y fu
ture
expe
nses
?
û N
o. Co
vera
ge E
xamp
les ar
e not
cost
estim
ators.
You c
an’t u
se th
e exa
mples
to
estim
ate co
sts fo
r an a
ctual
cond
ition.
They
ar
e for
comp
arati
ve pu
rpos
es on
ly. Yo
ur ow
n co
sts w
ill be
diffe
rent
depe
nding
on th
e car
e you
re
ceive
, the p
rices
your
pro
vider
s cha
rge,
and
the re
imbu
rseme
nt yo
ur he
alth p
lan al
lows.
Can
I use
Cov
erag
e Exa
mpl
es to
co
mpa
re p
lans?
üYe
s. W
hen y
ou lo
ok at
the S
umma
ry of
Bene
fits
and C
over
age f
or ot
her p
lans,
you’l
l find
the
same
Cov
erag
e Exa
mples
. Whe
n you
comp
are
plans
, che
ck th
e “Pa
tient
Pays
” box
in ea
ch
exam
ple. T
he sm
aller
that
numb
er, th
e mor
e co
vera
ge th
e plan
prov
ides .
Are t
here
oth
er co
sts I
shou
ld co
nsid
er
when
com
parin
g pl
ans?
üYe
s. An
impo
rtant
cost
is the
pre
miu
m yo
u pa
y. Ge
nera
lly, th
e low
er yo
ur p
rem
ium
, the
more
you’l
l pay
in ou
t-of-p
ocke
t cos
ts, su
ch as
co
paym
ents
, ded
uctib
les, a
nd co
insu
ranc
e. Yo
u also
shou
ld co
nside
r con
tributi
ons t
o ac
coun
ts su
ch as
healt
h sav
ings a
ccou
nts
(HSA
s), fle
xible
spen
ding a
rrang
emen
ts (F
SAs)
or he
alth r
eimbu
rseme
nt ac
coun
ts (H
RAs)
that
help
you p
ay ou
t-of-p
ocke
t exp
ense
s.
® Re
gister
ed M
arks
of th
e Blue
Cro
ss an
d Blue
Shie
ld As
socia
tion.©
2013
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
, Inc.,
and
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
HMO
Blue
, Inc.
11
3023
2B (9
/13) P
DF JI
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at ww
w.bl
uecr
ossm
a.com
/sbcg
loss
ary o
r call
1-88
8-54
3-87
70 to
requ
est a
copy
.


This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect as of January 1, 2014, as part of the Massachusetts Health Care Reform Law.
MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2013 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 129108 55-0647 (7/13) 150M


HMO
Blu
e New
Eng
land
Enha
nced
Valu
e B
abso
n Co
llege
Low
Opt
ion
Sum
mar
y of B
enefi
ts an
d Co
vera
ge: W
hat th
is Pl
an C
over
s & W
hat it
Cos
ts
Cove
rage
Per
iod:
01/01
/2014
- 12/3
1/201
4Co
vera
ge fo
r: Ind
ividu
al an
d Fam
ily | P
lan Ty
pe: H
MO
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at w
ww.b
luec
ross
ma.c
om/sb
cglo
ssar
y or c
all 1-
888-
543-
8770
to re
ques
t a co
py.
1 of 8
Blue
Cro
ss B
lue S
hield
of Ma
ssac
huse
tts is
an In
depe
nden
t Lice
nsee
of th
e Blue
Cro
ss an
d Blue
Shie
ld As
socia
tion
This
is on
ly a s
umm
ary.
If you
wan
t mor
e deta
il abo
ut yo
ur co
vera
ge an
d cos
ts, yo
u can
get th
e com
plete
terms
in th
e poli
cy or
plan
docu
ment
at
www.
blue
cros
sma.c
om or
by ca
lling 1
-888
-543
-877
0.
Impo
rtan
t Que
stio
nsA
nsw
ers
Why
this
Mat
ters
:W
hat is
the o
vera
ll de
duct
ible?
$0Se
e the
char
t star
ting o
n pag
e 2 fo
r you
r cos
ts for
servi
ces t
his pl
an co
vers.
Are t
here
oth
er
dedu
ctib
les fo
r spe
cific
serv
ices?
No.
You d
on’t h
ave t
o mee
t ded
uctib
les fo
r spe
cific s
ervic
es, b
ut se
e the
char
t star
ting o
n pag
e 2 fo
r oth
er co
sts fo
r ser
vices
this
plan c
over
s.
Is th
ere a
n ou
t-of-p
ocke
t lim
it on
my e
xpen
ses?
Yes.
$2,00
0 mem
ber /
$4,00
0 fam
ily.Th
e out
-of-p
ocke
t lim
it is t
he m
ost y
ou co
uld pa
y dur
ing a
cove
rage
perio
d (us
ually
one y
ear)
for
your
shar
e of th
e cos
t of c
over
ed se
rvice
s. Th
is lim
it help
s you
plan
for h
ealth
care
expe
nses
.
Wha
t is n
ot in
clude
d in
the
out-o
f-poc
ket li
mit?
Prem
iums,
pres
cripti
on dr
ugs,
balan
ce-
billed
char
ges,
and h
ealth
care
this
plan
does
n’t co
ver.
Even
thou
gh yo
u pay
thes
e exp
ense
s, the
y don
’t cou
nt tow
ard t
he o
ut-o
f-poc
ket li
mit.
Does
this
plan
use
a ne
twor
k of p
rovid
ers?
Yes.
See w
ww.b
luec
ross
ma.c
om/
finda
doct
or o
r call
1-80
0-82
1-13
88 fo
r a l
ist of
netw
ork p
rovid
ers.
If you
use a
n in-
netw
ork d
octor
or ot
her h
ealth
care
pro
vider
, this
plan w
ill pa
y som
e or a
ll of
the co
sts of
cove
red s
ervic
es. B
e awa
re, y
our in
-netw
ork d
octor
or ho
spita
l may
use a
n out-
of-ne
twor
k pro
vider
for s
ome s
ervic
es. P
lans u
se th
e ter
m in-
netw
ork,
pref
erre
d, or
partic
ipatin
g for
pr
ovid
ers i
n the
ir net
work
. See
the c
hart
startin
g on p
age 2
for h
ow th
is pla
n pay
s diffe
rent
kinds
of
prov
ider
s.Do
I nee
d a r
efer
ral to
see
a spe
cialis
t?Ye
s.Th
is pla
n will
pay s
ome o
r all o
f the c
osts
to se
e a sp
ecial
ist fo
r cov
ered
servi
ces b
ut on
ly if y
ou
have
the p
lan’s
perm
ission
befor
e you
see t
he sp
ecial
ist.
Are t
here
serv
ices t
his
plan
doe
sn’t c
over
?Ye
s.So
me of
the s
ervic
es th
is pla
n doe
sn’t c
over
are l
isted
on pa
ge 5.
See
your
polic
y or p
lan do
cume
nt for
addit
ional
infor
matio
n abo
ut ex
clude
d se
rvice
s.
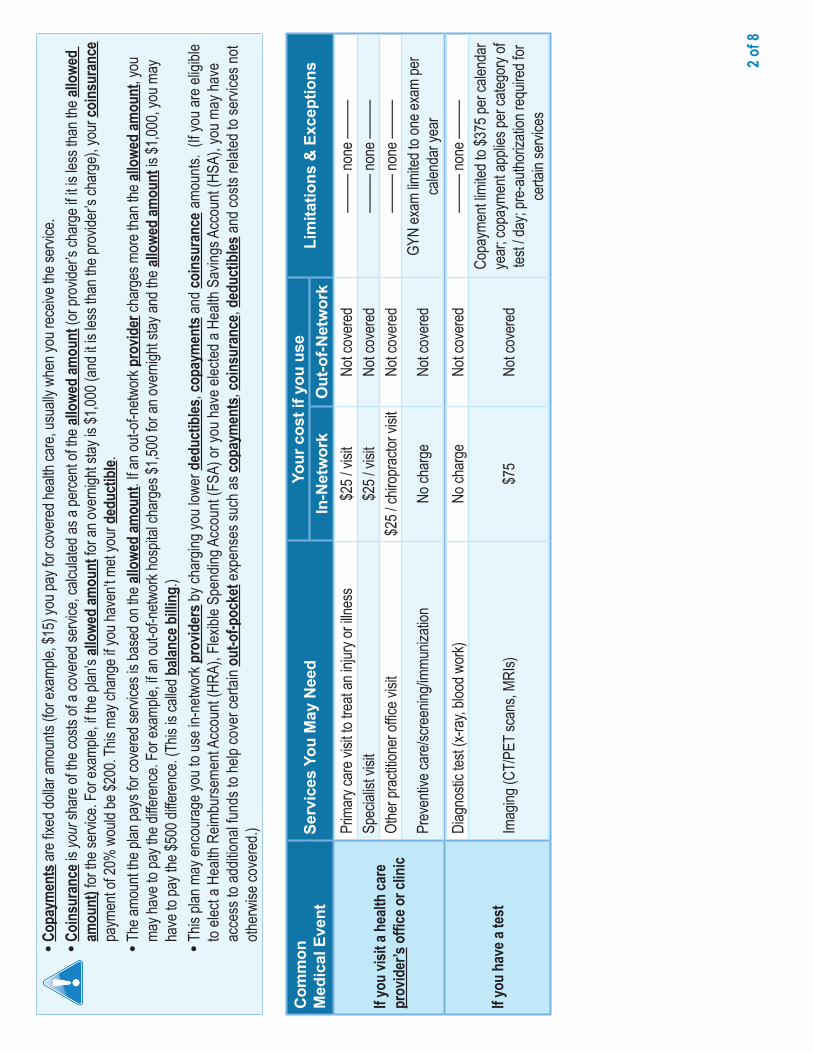
2 of 8
•Co
paym
ents
are fi
xed d
ollar
amou
nts (f
or ex
ample
, $15
) you
pay f
or co
vere
d hea
lth ca
re, u
suall
y whe
n you
rece
ive th
e ser
vice.
•Co
insu
ranc
e is y
our s
hare
of th
e cos
ts of
a cov
ered
servi
ce, c
alcula
ted as
a pe
rcent
of the
allo
wed
amou
nt (o
r pro
vider
’s ch
arge
if it i
s les
s tha
n the
allo
wed
amou
nt) fo
r the
servi
ce. F
or ex
ample
, if th
e plan
’s all
owed
amou
nt fo
r an o
vern
ight s
tay is
$1,00
0 (an
d it is
less
than
the p
rovid
er’s
char
ge),
your
coin
sura
nce
paym
ent o
f 20%
wou
ld be
$200
. This
may
chan
ge if
you h
aven
’t met
your
ded
uctib
le.•
The a
moun
t the p
lan pa
ys fo
r cov
ered
servi
ces i
s bas
ed on
the a
llowe
d am
ount
. If an
out-o
f-netw
ork p
rovid
er ch
arge
s mor
e tha
n the
allo
wed
amou
nt, y
ou
may h
ave t
o pay
the d
iffere
nce.
For e
xamp
le, if
an ou
t-of-n
etwor
k hos
pital
char
ges $
1,500
for a
n ove
rnigh
t stay
and t
he al
lowe
d am
ount
is $1
,000,
you m
ay
have
to pa
y the
$500
diffe
renc
e. (T
his is
calle
d bala
nce b
illing
.)•
This
plan m
ay en
cour
age y
ou to
use i
n-ne
twor
k pro
vider
s by c
harg
ing yo
u low
er d
educ
tibles
, cop
aym
ents
and c
oins
uran
ce a
moun
ts. (
If you
are e
ligibl
e to
elect
a Hea
lth R
eimbu
rseme
nt Ac
coun
t (HR
A), F
lexibl
e Spe
nding
Acc
ount
(FSA
) or y
ou ha
ve el
ected
a He
alth S
aving
s Acc
ount
(HSA
), yo
u may
have
ac
cess
to ad
dition
al fun
ds to
help
cove
r cer
tain o
ut-o
f-poc
ket e
xpen
ses s
uch a
s cop
aym
ents
, coi
nsur
ance
, ded
uctib
les an
d cos
ts re
lated
to se
rvice
s not
other
wise
cove
red.)
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
visit
a he
alth
care
pr
ovid
er’s
offic
e or c
linic
Prim
ary c
are v
isit to
trea
t an i
njury
or ill
ness
$25 /
visit
Not c
over
ed—
——
none
——
—Sp
ecial
ist vi
sit$2
5 / vi
sitNo
t cov
ered
——
— no
ne —
——
Othe
r pra
ctitio
ner o
ffice v
isit
$25 /
chiro
prac
tor vi
sitNo
t cov
ered
——
— no
ne —
——
Prev
entiv
e car
e/scre
ening
/immu
nizati
onNo
char
geNo
t cov
ered
GYN
exam
limite
d to o
ne ex
am pe
r ca
lenda
r yea
r
If you
hav
e a te
st
Diag
nosti
c tes
t (x-r
ay, b
lood w
ork)
No ch
arge
Not c
over
ed—
——
none
——
—
Imag
ing (C
T/PE
T sca
ns, M
RIs)
$75
Not c
over
ed
Copa
ymen
t limi
ted to
$375
per c
alend
ar
year
; cop
ayme
nt ap
plies
per c
atego
ry of
tes
t / da
y; pr
e-au
thoriz
ation
requ
ired f
or
certa
in se
rvice
s

3 of 8
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
nee
d dr
ugs t
o tre
at
your
illne
ss o
r con
ditio
n
More
info
rmat
ion
abou
t pr
escr
iptio
n dr
ug
cove
rage
is av
ailab
le at
ww
w.bl
uecr
ossm
a.com
.
Gene
ric dr
ugs
$15 /
retai
l or $
30
($15
for v
alue d
rugs
) / m
ail se
rvice
supp
lyNo
t cov
ered
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for b
irth
contr
ol, sm
oking
cess
ation
and c
ertai
n or
ally a
dmini
stere
d anti
canc
er dr
ugs;
pre-
autho
rizati
on re
quire
d for
ce
rtain
drug
s
Prefe
rred b
rand
drug
s$3
0 / re
tail o
r $60
($
30 fo
r valu
e dru
gs)
servi
ce su
pply
Not c
over
ed
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for s
mokin
g ce
ssati
on sm
oking
cess
ation
and c
ertai
n or
ally a
dmini
stere
d anti
canc
er dr
ugs;
pre-
autho
rizati
on re
quire
d for
ce
rtain
drug
s
Non-
prefe
rred b
rand
drug
s$5
0 / re
tail o
r $10
0 /
mail s
ervic
e sup
plyNo
t cov
ered
Up to
30-d
ay re
tail (9
0-da
y mail
servi
ce)
supp
ly; co
st sh
are w
aived
for c
ertai
n or
ally a
dmini
stere
d anti
canc
er dr
ugs;
pr
e-au
thoriz
ation
requ
ired f
or
certa
in dr
ugs
Spec
ialty
drug
sAp
plica
ble co
st sh
are
(gen
eric,
prefe
rred,
non-
prefe
rred)
Not c
over
edW
hen o
btaine
d fro
m a d
esign
ated
spec
ialty
phar
macy
; pre
-auth
oriza
tion
requ
ired f
or ce
rtain
drug
s
If you
hav
e out
patie
nt
surg
ery
Facil
ity fe
e (e.g
., amb
ulator
y sur
gery
cente
r)$2
50 / a
dmisi
son
Not c
over
edPr
e-au
thoriz
ation
requ
ired
Phys
ician
/surg
eon f
ees
No ch
arge
Not c
over
edPr
e-au
thoriz
ation
requ
ired f
or ce
rtain
servi
ces
If you
nee
d im
med
iate
med
ical a
ttent
ion
Emer
genc
y roo
m se
rvice
s$1
50 / v
isit
$150
/ visi
tCo
paym
ent w
aived
if ad
mitte
d or f
or
obse
rvatio
n stay
Emer
genc
y med
ical tr
ansp
ortat
ionNo
char
geNo
char
ge—
——
none
——
—
Urge
nt ca
re$2
5 / vi
sit$2
5 / vi
sitOu
t-of-n
etwor
k cov
erag
e lim
ited t
o out
of se
rvice
area
If you
hav
e a h
ospi
tal s
tay
Facil
ity fe
e (e.g
., hos
pital
room
)$5
00 / a
dmiss
ionNo
t cov
ered
Pre-
autho
rizati
on re
quire
d
Phys
ician
/surg
eon f
eeNo
char
geNo
t cov
ered
Pre-
autho
rizati
on re
quire
d

4 of 8
Com
mon
Med
ical
Eve
ntSe
rvic
es Y
ou M
ay N
eed
Your
cos
t if y
ou u
seLi
mita
tions
& E
xcep
tions
In-N
etw
ork
Out
-of-N
etw
ork
If you
hav
e men
tal h
ealth
, be
havio
ral h
ealth
, or
subs
tanc
e abu
se n
eeds
Menta
l/Beh
avior
al he
alth o
utpati
ent s
ervic
es$2
5 / vi
sitNo
t cov
ered
Pre-
autho
rizati
on re
quire
d for
certa
in se
rvice
sMe
ntal/B
ehav
ioral
healt
h inp
atien
t ser
vices
$500
/ adm
ission
Not c
over
edPr
e-au
thoriz
ation
requ
ired.
Subs
tance
use d
isord
er ou
tpatie
nt se
rvice
s$2
5 / vi
sitNo
t cov
ered
Pre-
autho
rizati
on re
quire
d for
certa
in se
rvice
sSu
bstan
ce us
e diso
rder
inpa
tient
servi
ces
$500
/ adm
ission
Not c
over
edPr
e-au
thoriz
ation
requ
ired
If you
are p
regn
ant
Pren
atal a
nd po
stnata
l car
eNo
char
geNo
t cov
ered
——
— no
ne —
——
Deliv
ery a
nd al
l inpa
tient
servi
ces
$500
/ adm
ission
Not c
over
ed—
——
none
——
—
If you
nee
d he
lp
reco
verin
g or
hav
e oth
er
spec
ial h
ealth
nee
ds
Home
healt
h car
eNo
char
geNo
t cov
ered
Pre-
autho
rizati
on re
quire
d
Reha
bilita
tion s
ervic
es$2
5 / vi
sitNo
t cov
ered
Limite
d to 6
0 visi
ts pe
r cale
ndar
year
(o
ther t
han f
or au
tism,
home
healt
h car
e, an
d spe
ech t
hera
py)
Habil
itatio
n ser
vices
$25 /
visit
Not c
over
ed
Reha
bilita
tion t
hera
py co
vera
ge lim
its
apply
; cos
t sha
re an
d cov
erag
e lim
its
waive
d for
early
inter
venti
on se
rvice
s for
eli
gible
child
ren
Skille
d nur
sing c
are
No ch
arge
Not c
over
edLim
ited t
o 100
days
per c
alend
ar ye
ar;
pre-
autho
rizati
on re
quire
d
Dura
ble m
edica
l equ
ipmen
t20
% co
insur
ance
Not c
over
edCo
st sh
are w
aived
for o
ne br
east
pump
pe
r birth
Hosp
ice se
rvice
No ch
arge
Not c
over
edPr
e-au
thoriz
ation
requ
ired f
or ce
rtain
servi
ces
If you
r chi
ld n
eeds
den
tal
or ey
e car
e
Eye e
xam
No ch
arge
Not c
over
edLim
ited t
o one
exam
ever
y 24 m
onths
Glas
ses
Not c
over
edNo
t cov
ered
——
— no
ne —
——
Denta
l che
ck-u
pNo
char
geNo
t cov
ered
Limite
d to c
hildr
en un
der a
ge 12
(eve
ry 6 m
onths
) and
unde
r age
18 w
ith a
cleft
palat
e / cl
eft lip
cond
ition
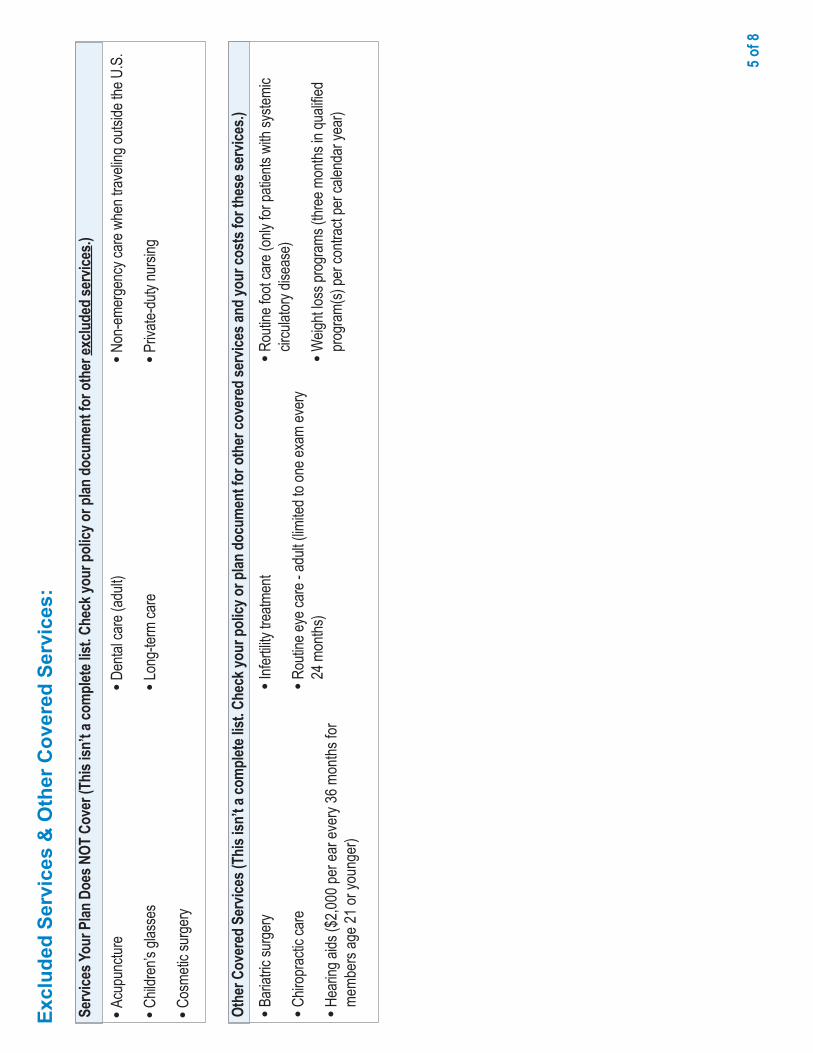
5 of 8
Excl
uded
Ser
vice
s &
Oth
er C
over
ed S
ervi
ces:
•Ac
upun
cture
•Ch
ildre
n’s gl
asse
s
•Co
smeti
c sur
gery
•De
ntal c
are (
adult
)
•Lo
ng-te
rm ca
re
•No
n-em
erge
ncy c
are w
hen t
rave
ling o
utside
the U
.S.
•Pr
ivate-
duty
nursi
ng
Serv
ices Y
our P
lan D
oes N
OT C
over
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er ex
clude
d se
rvice
s.)
•Ba
riatric
surg
ery
•Ch
iropr
actic
care
•He
aring
aids
($2,0
00 pe
r ear
ever
y 36 m
onths
for
memb
ers a
ge 21
or yo
unge
r)
•Inf
ertili
ty tre
atmen
t
•Ro
utine
eye c
are -
adult
(limi
ted to
one e
xam
ever
y 24
mon
ths)
•Ro
utine
foot
care
(only
for p
atien
ts wi
th sy
stemi
c cir
culat
ory d
iseas
e)
•W
eight
loss p
rogr
ams (
three
mon
ths in
quali
fied
prog
ram(
s) pe
r con
tract
per c
alend
ar ye
ar)
Othe
r Cov
ered
Ser
vices
(Thi
s isn
’t a co
mpl
ete l
ist. C
heck
your
pol
icy o
r plan
doc
umen
t for
oth
er co
vere
d se
rvice
s and
your
cost
s for
thes
e ser
vices
.)

6 of 8
Your
Rig
hts
to C
ontin
ue C
over
age:
If you
lose
cove
rage
unde
r the
plan
, then
, dep
endin
g upo
n the
circu
mstan
ces,
Fede
ral a
nd S
tate l
aws m
ay pr
ovide
prote
ction
s tha
t allo
w yo
u to k
eep h
ealth
cove
rage
. Any
su
ch rig
hts m
ay be
limite
d in d
urati
on an
d will
requ
ire yo
u to p
ay a
prem
ium
, whic
h may
be si
gnific
antly
high
er th
an th
e pre
mium
you p
ay w
hile c
over
ed un
der t
he pl
an.
Othe
r limi
tation
s on y
our r
ights
to co
ntinu
e cov
erag
e may
also
apply
. Fo
r mor
e info
rmati
on on
your
rights
to co
ntinu
e cov
erag
e, co
ntact
your
plan
spon
sor. N
ote: A
plan
spon
sor is
usua
lly th
e mem
ber’s
emplo
yer o
r org
aniza
tion t
hat p
rovid
es
grou
p hea
lth co
vera
ge to
the m
embe
r. You
may
also
conta
ct yo
ur st
ate in
sura
nce d
epar
tmen
t, the
U.S
. Dep
artm
ent o
f Lab
or, E
mploy
ee B
enefi
ts Se
curity
Adm
inistr
ation
at
1-86
6-44
4-32
72 or
www
.dol.g
ov/eb
sa, o
r the
U.S
. Dep
artm
ent o
f Hea
lth an
d Hum
an S
ervic
es at
1-87
7-26
7-23
23 x6
1565
or w
ww.cc
iio.cm
s.gov
.Yo
ur G
rieva
nce
and
App
eals
Rig
hts:
If you
have
a co
mplai
nt or
are d
issati
sfied
with
a de
nial o
f cov
erag
e for
claim
s und
er yo
ur pl
an, y
ou m
ay be
able
to ap
peal
or fil
e a gr
ievan
ce. F
or qu
estio
ns ab
out y
our
rights
, this
notic
e, or
assis
tance
, you
can c
ontac
t the M
embe
r Ser
vice n
umbe
r liste
d on y
our I
D ca
rd or
conta
ct yo
ur pl
an sp
onso
r. Note
: A pl
an sp
onso
r is us
ually
the
memb
er’s
emplo
yer o
r org
aniza
tion t
hat p
rovid
es gr
oup h
ealth
cove
rage
to th
e mem
ber. .
Doe
s th
is C
over
age
Prov
ide
Min
imum
Ess
entia
l Cov
erag
e?Th
e Affo
rdab
le Ca
re A
ct re
quire
s mos
t peo
ple to
have
healt
h car
e cov
erag
e tha
t qua
lifies
as “m
inimu
m es
senti
al co
vera
ge.”
This
plan
or p
olicy
doe
s pro
vide m
inim
um
esse
ntial
cove
rage
.
Doe
s th
is C
over
age
Mee
t the
Min
imum
Val
ue S
tand
ard?
The A
fford
able
Care
Act
estab
lishe
s a m
inimu
m va
lue st
anda
rd of
bene
fits of
a he
alth p
lan. T
he m
inimu
m va
lue st
anda
rd is
60%
(actu
arial
value
). Th
is he
alth
cove
rage
do
es m
eet t
he m
inim
um va
lue s
tand
ard
for t
he b
enefi
ts it
prov
ides
.
Lang
uage
Ass
ista
nce
D
iscl
aim
er:
This
docu
ment
conta
ins on
ly a p
artia
l des
cripti
on of
the b
enefi
ts, lim
itatio
ns, e
xclus
ions a
nd ot
her p
rovis
ions o
f this
healt
h car
e plan
. It is
not a
polic
y. It i
s a ge
nera
l ove
rview
on
ly. It
does
not p
rovid
e all t
he de
tails
of thi
s cov
erag
e, inc
luding
bene
fits, e
xclus
ions a
nd po
licy l
imita
tions
. In th
e eve
nt the
re ar
e disc
repa
ncies
betw
een t
his do
cume
nt an
d the
polic
y, the
term
s and
cond
itions
of th
e poli
cy w
ill go
vern
.
To se
e exa
mples
of ho
w thi
s plan
migh
t cov
er co
sts fo
r a sa
mple
medic
al sit
uatio
n, se
e the
next
page
.

7 of 8
Abo
ut th
ese
C
over
age
Exam
ples
:
Thes
e exa
mples
show
how
this p
lan m
ight
cove
r med
ical c
are i
n give
n situ
ation
s. Us
e the
se ex
ample
s to s
ee, in
gene
ral, h
ow m
uch
finan
cial p
rotec
tion a
samp
le pa
tient
migh
t ge
t if th
ey ar
e cov
ered
unde
r diffe
rent
plans
.
This
is
not a
cos
t es
timat
or.
Don’t
use t
hese
exam
ples t
o esti
mate
your
actua
l cos
ts un
der t
his pl
an.
The a
ctual
care
you r
eceiv
e will
be
differ
ent fr
om th
ese e
xamp
les, a
nd
the co
st of
that c
are a
lso w
ill be
dif
feren
t.
See t
he ne
xt pa
ge fo
r impo
rtant
infor
matio
n abo
ut the
se ex
ample
s.
Hav
ing
a ba
by(n
orm
al d
eliv
ery)
n A
mou
nt o
wed
to p
rovid
ers:
$7,5
40n
Plan
pay
s $6
,870
n P
atien
t Pay
s $6
70
Sam
ple c
are c
osts
:Ho
spita
l cha
rges
(moth
er)
$2,70
0Ro
utine
obste
tric ca
re$2
,100
Hosp
ital c
harg
es (b
aby)
$900
Anes
thesia
$900
Labo
rator
y tes
ts$5
00Pr
escri
ption
s$2
00Ra
diolog
y$2
00Va
ccine
s, oth
er pr
even
tive
$40
Tota
l$7
,540
Patie
nt P
ays:
Dedu
ctible
s$0
Copa
ys$5
20Co
insur
ance
$0Lim
its or
exclu
sions
$150
Tota
l$6
70
Man
agin
g ty
pe 2
dia
bete
s(ro
utin
e m
aint
enan
ce o
f a w
ell-c
ontro
lled
cond
ition
)
n A
mou
nt o
wed
to p
rovid
ers:
$5,4
00n
Plan
pay
s $3
,330
n P
atien
t Pay
s $2
,070
Sam
ple c
are c
osts
:Pr
escri
ption
s$2
,900
Medic
al Eq
uipme
nt an
d Sup
plies
$1,30
0Of
fice V
isits
and P
roce
dure
s$7
00Ed
ucati
on$3
00La
bora
tory t
ests
$100
Vacc
ines,
other
prev
entiv
e$1
00To
tal
$5,40
0
Patie
nt P
ays:
Dedu
ctible
s$0
Copa
ys$1
,990
Coins
uran
ce$0
Limits
or ex
clusio
ns$8
0To
tal
$2,07
0

8 of 8
Que
stio
ns a
nd a
nsw
ers
abou
t the
Cov
erag
e Ex
ampl
es:
Wha
t are
som
e of t
he as
sum
ptio
ns
behi
nd th
e Cov
erag
e Exa
mpl
es?
•Co
sts do
n’t in
clude
pre
miu
ms.
•Sa
mple
care
costs
are b
ased
on na
tiona
l ave
rage
s su
pplie
d to t
he U
.S. D
epar
tmen
t of H
ealth
and
Huma
n Ser
vices
, and
aren
’t spe
cific t
o a pa
rticula
r ge
ogra
phic
area
or he
alth p
lan.
•Th
e pati
ent’s
cond
ition w
as no
t an e
xclud
ed or
pr
eexis
ting c
ondit
ion.
•Al
l ser
vices
and t
reatm
ents
starte
d and
ende
d in
the sa
me co
vera
ge pe
riod.
•Th
ere a
re no
othe
r med
ical e
xpen
ses f
or an
y me
mber
cove
red u
nder
this
plan.
•Ou
t-of-p
ocke
t exp
ense
s are
base
d only
on tr
eatin
g the
cond
ition i
n the
exam
ple.
•Th
e pati
ent r
eceiv
ed al
l car
e fro
m in-
netw
ork
prov
ider
s. If t
he pa
tient
had r
eceiv
ed ca
re fr
om
out-o
f-netw
ork p
rovid
ers,
costs
wou
ld ha
ve be
en
highe
r.
Wha
t doe
s a C
over
age E
xam
ple
show
?Fo
r eac
h tre
atmen
t situ
ation
, the C
over
age E
xamp
le he
lps yo
u see
how
dedu
ctib
les, c
opay
men
ts, a
nd
coin
sura
nce c
an ad
d up.
It also
helps
you s
ee w
hat
expe
nses
migh
t be l
eft up
to yo
u to p
ay be
caus
e the
servi
ce or
trea
tmen
t isn’t
cove
red o
r pay
ment
is lim
ited.
Does
the C
over
age E
xam
ple p
redi
ct m
y ow
n ca
re n
eeds
?
û N
o. Tr
eatm
ents
show
n are
just
exam
ples.
The
care
you w
ould
rece
ive fo
r this
cond
ition c
ould
be
differ
ent b
ased
on yo
ur do
ctor’s
advic
e, yo
ur ag
e, ho
w se
rious
your
cond
ition i
s, an
d man
y othe
r fac
tors.
Does
the C
over
age E
xam
ple p
redi
ct m
y fu
ture
expe
nses
?
û N
o. Co
vera
ge E
xamp
les ar
e not
cost
estim
ators.
You c
an’t u
se th
e exa
mples
to
estim
ate co
sts fo
r an a
ctual
cond
ition.
They
ar
e for
comp
arati
ve pu
rpos
es on
ly. Yo
ur ow
n co
sts w
ill be
diffe
rent
depe
nding
on th
e car
e you
re
ceive
, the p
rices
your
pro
vider
s cha
rge,
and
the re
imbu
rseme
nt yo
ur he
alth p
lan al
lows.
Can
I use
Cov
erag
e Exa
mpl
es to
co
mpa
re p
lans?
üYe
s. W
hen y
ou lo
ok at
the S
umma
ry of
Bene
fits
and C
over
age f
or ot
her p
lans,
you’l
l find
the
same
Cov
erag
e Exa
mples
. Whe
n you
comp
are
plans
, che
ck th
e “Pa
tient
Pays
” box
in ea
ch
exam
ple. T
he sm
aller
that
numb
er, th
e mor
e co
vera
ge th
e plan
prov
ides .
Are t
here
oth
er co
sts I
shou
ld co
nsid
er
when
com
parin
g pl
ans?
üYe
s. An
impo
rtant
cost
is the
pre
miu
m yo
u pa
y. Ge
nera
lly, th
e low
er yo
ur p
rem
ium
, the
more
you’l
l pay
in ou
t-of-p
ocke
t cos
ts, su
ch as
co
paym
ents
, ded
uctib
les, a
nd co
insu
ranc
e. Yo
u also
shou
ld co
nside
r con
tributi
ons t
o ac
coun
ts su
ch as
healt
h sav
ings a
ccou
nts
(HSA
s), fle
xible
spen
ding a
rrang
emen
ts (F
SAs)
or he
alth r
eimbu
rseme
nt ac
coun
ts (H
RAs)
that
help
you p
ay ou
t-of-p
ocke
t exp
ense
s.
® Re
gister
ed M
arks
of th
e Blue
Cro
ss an
d Blue
Shie
ld As
socia
tion.©
2013
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
, Inc.,
and
Blue
Cro
ss an
d Blue
Shie
ld of
Mass
achu
setts
HMO
Blue
, Inc.
13
0233
BS (9
/13) 4
C JI
Ques
tions
: Call
1-88
8-54
3-87
70 or
visit
us at
www
.blu
ecro
ssm
a.com
.If y
ou ar
en’t c
lear a
bout
any o
f the u
nder
lined
term
s use
d in t
his fo
rm, s
ee th
e Glos
sary.
You c
an vi
ew th
e Glos
sary
at ww
w.bl
uecr
ossm
a.com
/sbcg
loss
ary o
r call
1-88
8-54
3-87
70 to
requ
est a
copy
.

This health plan meets Minimum Creditable Coverage Standards for Massachusetts residents that went into effect as of January 1, 2014, as part of the Massachusetts Health Care Reform Law.
MCC Compliance
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association. ® Registered Marks of the Blue Cross and Blue Shield Association. © 2013 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc. 129108 55-0647 (7/13) 150M



This Booklet provided to you by:
Thorbahn is a full service Employee Benefits consulting firm. We partner with our clients to provide the most cost efficient,
comprehensive employee benefits programs, products, and services.
141 Longwater Drive, Suite 101
Norwell, MA 02061
(617) 847-3900