urinary cd4+ effector memory t cells reflect renal disease activity in antineutrophil cytoplasmic...
TRANSCRIPT

ARTHRITIS & RHEUMATISMVol. 60, No. 9, September 2009, pp 2830–2838DOI 10.1002/art.24747© 2009, American College of Rheumatology
Urinary CD4� Effector Memory T CellsReflect Renal Disease Activity in
Antineutrophil Cytoplasmic Antibody–Associated Vasculitis
Wayel H. Abdulahad, Cees G. M. Kallenberg, Pieter C. Limburg, and Coen A. Stegeman
Objective. Numbers of circulating CD4� effectormemory T cells are proportionally increased in patientswith proteinase 3 antineutrophil cytoplasmic antibody–associated vasculitis (AAV) whose disease is in remis-sion and are decreased during active disease, whichpresumably reflects their migration toward sites ofinflammation. Since renal infiltrating cells may appearin urine, we investigated the presence of CD4� effectormemory T cells in urinary sediment as a reflection ofrenal disease activity in AAV.
Methods. CD4� effector memory (CD45RO�CCR7�CD3�CD4�) T cells were quantitated in theurine and peripheral blood of patients with AAV withrenal involvement (n � 33), patients with AAV withoutrenal involvement (n � 18), patients with AAV whosedisease was in remission (n � 29), and patients withactive disease (n � 22), using 4-color flow cytometricanalysis. Numbers and percentages of urine CD4�effector memory T cells in 12 patients with AAV withactive renal disease were obtained over several weeks offollowup during remission induction.
Results. A notable increase in urine CD4� effec-tor memory T cell numbers was observed in patientswith active renal AAV compared with patients whosedisease was in remission and patients with active dis-ease without renal involvement. The increase in thesecells in the urine of patients with active renal AAV wasaccompanied by a reciprocal decrease in these cells inperipheral blood. Results from followup analysis
showed a clear reduction in urine CD4� effector mem-ory T cells following treatment. Moreover, a negativecorrelation was observed between percentages of circu-lating and urine CD4� effector memory T cells, consis-tent with their migration toward sites of inflammation.
Conclusion. Our findings indicate that the pres-ence of CD4� effector memory T cells in urine reflectsrenal involvement in AAV. Flow cytometric analysis ofthese cells in urine may contribute to assessing renaldisease activity in patients with AAV.
Antineutrophil cytoplasmic antibody–associatedvasculitis (AAV) constitutes a group of disorders char-acterized by necrotizing crescentic glomerulonephritiswith systemic vasculitis predominantly affecting smallvessels, and the presence of circulating antineutrophilcytoplasmic antibodies (ANCA) that are specific forproteinase 3 (PR3) or myeloperoxidase (MPO) (1–3).Considerable evidence has accumulated to support arole of T cells in the pathogenesis of AAV. The presenceof T cell infiltrates in vasculitic areas and granulomatouslesions and the observation that remission can be in-duced in patients with AAV by anti–T cell treatment areconsistent with the notion of T cell–mediated pathologyin this disease (4–8). In support of this concept, wepreviously observed increased percentages of circulatingCD4� effector memory (CD45RO�CCR7�CD3�CD4�) T cells, as well as a defect in regulatory T cellfunction, in patients with PR3 AAV (9–11).
Previous cross-sectional and followup studies ofpatients with PR3 AAV have demonstrated that levels ofcirculating CD4� effector memory T cells in patientswith active disease are significantly lower than in pa-tients in whom the disease is in remission (9). Wehypothesized that these cells migrate to sites of inflam-mation once the disease becomes active. Consistent withthis hypothesis, infiltrating T cells in and around theglomeruli of patients with ANCA-associated glomerulo-
Supported by the Groningen University Institute for DrugExploration and the DFG.
Wayel H. Abdulahad, PhD, Cees G. M. Kallenberg, MD,PhD, Pieter C. Limburg, PhD, Coen A. Stegeman, MD, PhD: Univer-sity Medical Center Groningen, Groningen, The Netherlands.
Address correspondence and reprint requests to Wayel H.Abdulahad, PhD, Department of Rheumatology and Clinical Immu-nology, University Medical Center Groningen, Hanzeplein 1, 9713 GZGroningen, The Netherlands. E-mail: [email protected].
Submitted for publication May 23, 2008; accepted in revisedform May 17, 2009.
2830

nephritis were shown to consist mainly of effector mem-ory T cells (12). These cells could appear in the urine ofpatients with AAV with active renal disease, and detec-tion of urine CD4� effector memory T cells couldprovide a way to assess active renal involvement in thisdisease.
Several reports have described the detection of Tcells in urine from patients with postinfectious glomer-ulonephritis, active IgA nephropathy (13), renal allo-graft rejection (14), and lupus nephritis (15). Numbersof urinary mononuclear cells correlated with the clinicalstage in IgA nephropathy and with acute rejection inrenal allograft recipients (13,14). In addition, numbersof urinary T cells were markedly elevated in patientswith active lupus and were correlated with renal diseaseactivity (15). Thus, detection of T cells in urine mayreflect renal disease severity.
The present study, therefore, was designed toinvestigate the presence of CD4� effector memory Tcells in urinary sediment as a reflection of renal diseaseactivity in patients with AAV. To this end, CD4�effector memory T cells were quantitated by 4-color flowcytometric analysis in urine and blood samples frompatients with AAV with or without renal involvement,and the absolute counts of these cells were also deter-
mined during active disease and at several time pointsafter starting treatment.
PATIENTS AND METHODS
Study population. A total of 51 patients with AAV (26men and 25 women) were enrolled in this study. Their meanage was 55 years (median 56 years, range 26–80 years). Allpatients were ANCA-positive or had been ANCA-positive atthe time of diagnosis. Of the 51 patients, 37 had PR3 ANCAand 14 had MPO ANCA. Disease activity was assessed in allpatients at the time of sampling, using the Birmingham Vas-culitis Activity Score (BVAS) (16). Remission was defined asthe complete absence of clinical signs and symptoms of activevasculitis, as indicated by a BVAS of 0. Relapse was definedbased on the presence of clinical and laboratory signs ofinflammation and new or worsening clinical manifestations ofvasculitis leading to renewed or intensified immunosuppressivetherapy. Renal involvement was defined as either an activeurinary sediment with glomerular erythrocyturia or the pres-ence of erythrocyte casts with an increase in serum creatininelevel or a reduction in creatinine clearance or a renal biopsyshowing pauci-immune necrotizing glomerulonephritis.
Based on these criteria, we recruited 4 groups ofpatients with AAV: patients with renal involvement in whomAAV was in remission (n � 17), patients without renalinvolvement in whom AAV was in remission (n � 12), patientswith active disease and renal involvement (n � 16), andpatients with active disease without renal involvement (n � 6).
Table 1. Clinical and laboratory characteristics of the patients with AAV at the time of blood and urine sampling*
Remission, no renalinvolvement
(n � 12)
Remission, renalinvolvement
(n � 17)
Active disease, norenal involvement
(n � 6)
Active disease, renalinvolvement
(n � 16)
No. of men/women 5/7 10/7 3/3 8/8Age, median (range) years 56 (42–77) 54 (34–80) 53 (27–66) 60 (26–73)No. positive/negative for ANCA† 7/5 7/10 6/0 16/0BVAS, median (range) 0 0 6 (3–9) 21 (15–32)Serum creatinine, median (range)
�moles/liter84 (62–147) 107 (66–267) 70 (56–101) 291 (49–1,406)
Urinary protein, median (range) gm/liter 0.1 0.2 (0.1–1.1) 0.1 (0.1–0.2) 0.5 (0.1–4.6)No. of patients with urinary
erythrocytes/hpf�100 0 0 0 550–100 0 0 0 620–50 0 1 0 15–20 0 0 0 42–5 2 7 1 0�1 10 9 5 0
No. of patients with �40% dysmorphicerythrocytes‡
0 0 0 13
No. of patients with erythrocyte casts 0 0 0 15No. of patients in whom renal biopsy
was performed0 0 0 7§
* AAV � ANCA-associated vasculitis; BVAS � Birmingham Vasculitis Activity Score.† Antineutrophil cytoplasmic antibody (ANCA) status at the time of analysis. All patients were ANCA positive at diagnosis.‡ The percentage of dysmorphic erythrocytes was assessed when �5 erythrocytes/high-power field (hpf) were present.§ In all 7 patients in whom a renal biopsy was performed, a pauci-immune necrotizing glomerulonephritis was found.
CD4� EFFECTOR MEMORY T CELLS AND RENAL DISEASE ACTIVITY IN AAV 2831

None of the patients had an infection at the time of sampling.Urine and blood samples were obtained, and the percentagesand absolute counts of CD4� effector memory T cells wereassessed immediately after sampling, by 4-color flow cytom-etry. Analysis of CD4� effector memory T cells in urine andblood was repeated in 12 patients with renal involvement inwhom AAV was in remission for up to several weeks after theinitial evaluation. All patients provided informed consent.Patient clinical and laboratory data are summarized in Table 1.
Antibodies. The following antibodies were used in flowcytometry: phycoerythrin (PE)–conjugated anti-CCR7, fluo-rescein isothiocyanate (FITC)–conjugated anti-CD45RO,peridin chlorophyll protein (PerCP)–conjugated anti-CD4, al-lophycocyanin (APC)–conjugated anti-CD3, MultiTEST4-color antibodies (FITC-conjugated CD3, PE-conjugatedCD8, PerCP-conjugated CD45, and APC-conjugated CD4),and isotype-matched control antibodies of irrelevant specific-ity. All were purchased from Becton Dickinson (Amsterdam,The Netherlands).
Sample preparation and flow cytometric analysis. Im-mediately after voiding, 100 ml of urine was diluted 1:1 withcold phosphate buffered saline (PBS) and centrifuged at 1,800revolutions per minute for 15 minutes. The supernatant wasremoved, and the sediment was resuspended in 10 ml of PBS.Fifty microliters of the cell suspension was used for quantita-tive measurement with a TrueCount tube, as described below,whereas mononuclear cells were isolated from the remainingcell suspension by density-gradient centrifugation on Lym-phoprep (Axis-Shield, Oslo, Norway). Next, mononuclear cells
were resuspended in wash buffer (1% bovine serum albumin inPBS) and mixed with appropriate concentrations of FITC-conjugated anti-CD45RO, PE-conjugated anti-CCR7, PerCP-conjugated anti-CD4, and APC-conjugated anti-CD3 for 15minutes at room temperature in the dark. Isotype-matchednonspecific antibodies were used as negative controls. Inparallel, blood samples were labeled with the monoclonalantibodies described above. Afterward, cells were successivelytreated with 2 ml of diluted fluorescence-activated cell sorting(FACS) lysing solution (Becton Dickinson) for 10 minutes, andsamples were washed twice in wash buffer and immediatelyanalyzed by flow cytometry. Four-color staining was analyzedusing FACSCalibur (Becton Dickinson), and data were col-lected for 105 events for each sample and plotted usingWin-List software (Verity Software House, Topsham, ME).Positively and negatively stained populations were calculatedby quadrant dot plot analysis, as determined by the isotypecontrols. Representative examples are shown in Figure 1.
Quantification of CD4� effector memory T cells.CD4� T cells were quantified in urine using TrueCount tubes(Becton Dickinson). Briefly, 20 �l of MultiTEST 4-colorantibodies (FITC-conjugated CD3, PE-conjugated CD8,PerCP-conjugated CD45, and APC-conjugated CD4) and 50�l of sample (urine or blood) were added to bead-containingTrueCount tubes. Tubes were incubated for 15 minutes atroom temperature, and 450 �l of 1� FACS lysing solution wasadded. The intensity of the fluorescence was measured using aFACSCalibur flow cytometer, and analysis was performedusing CellQuest software (Becton Dickinson). The bead pop-
Figure 1. Four-color flow cytometric analysis of CD4� effector memory T cells in urine and peripheral blood from a patient with antineutrophilcytoplasmic antibody–associated vasculitis. Samples were stained with allophycocyanin (APC)–conjugated anti-CD3, peridin chlorophyll protein(PerCP)–conjugated anti-CD4, phycoerythrin (PE)–conjugated anti-CCR7, and fluorescein isothiocyanate (FITC)–conjugated anti-CD45RO. A,CD4� effector memory T cells in urine. The encircled area shows T cells. B, CD4� effector memory T cells in peripheral blood. The encircled areashows the lymphocyte region in peripheral blood. Positively and negatively stained populations for CCR7 and CD45RO within CD4� T cells werecalculated by quadrant dot plot analysis, determined with the appropriate isotype controls. Boxed areas show CD4� T cells.
2832 ABDULAHAD ET AL

ulation and the CD45 lymphocyte versus side scatter popula-tion were manually gated, and the absolute number ofCD3�CD4� T cells was determined by comparing cellularevents with bead events.
Absolute counts of CD4� effector memory T cells in1 ml of urine were calculated as the number of CD4� effectormemory T cells/ml sample � (volume of urine cell suspensionafter the first wash [10 ml]/total volume of collected urine[100 ml]) � % CD4� effector memory T cells in urine. In
order to correct for variation in urine dilution, the quantitativeresults of urine CD4� effector memory T cells were alsoexpressed as ratios to urine creatinine concentration.
Microscopic examination of urinary sediment. Tenmilliliters of freshly voided urine was centrifuged for 10minutes at 1,500g. After centrifugation, 9.5 ml of the superna-tant was aspirated, and the urinary sediment was resuspendedin the remaining 0.5 ml. One drop of the resuspended sedimentwas transferred to a microscope glass slide, covered with an
Figure 2. CD4� effector memory T cells (TEM) in urine and peripheral blood of patients with antineutrophil cytoplasmic antibody–associatedvasculitis (AAV) without renal involvement whose disease was in remission (non rR-AAV; n � 12), patients with AAV with renal involvement whosedisease was in remission (rR-AAV; n � 17), patients with active AAV without renal involvement (non rA-AAV; n � 6), and patients with activeAAV with renal involvement (rA-AAV; n � 16). A, Absolute count of urine CD4� effector memory T cells. B, Ratio of number of CD4� effectormemory T cells in urine to urine creatinine concentration. C, Percentage of CD4� effector memory T cells in urine. D, Percentage of CD4� effectormemory T cells in peripheral blood. Flow cytometry was performed as described in Patients and Methods. Bars show the mean. P values weredetermined by nonparametric Mann-Whitney U test.
CD4� EFFECTOR MEMORY T CELLS AND RENAL DISEASE ACTIVITY IN AAV 2833

18 � 18–mm cover, and immediately examined at 100� and400� magnification by a trained nephrologist (CAS). Thenumber of erythrocytes per field at 400� magnification wasrecorded, and when �5 erythrocytes per field were present, thepercentage of dysmorphic erythrocytes was assessed by differ-entiating �100 erythrocytes. In addition, the presence orabsence of erythrocyte casts was recorded. Urinary sedimentreflected active glomerular disease if �5 erythrocytes permicroscopic field at 400� magnification were present and�40% of the erythrocytes were dysmorphic in combinationwith the presence of acanthocytes and/or erythrocyte casts. Allurinary sediments were examined within 2 hours of voiding.
Statistical analysis. Results are presented as themean � SD. The nonparametric Mann-Whitney U test wasused for comparison of values between groups. Correlationwas assessed using Spearman’s rank correlation coefficient. Pvalues less than 0.05 (2-tailed) were considered significant.
RESULTS
Increase in urine CD4� effector memory T cellsand decrease in circulating CD4� effector memory Tcells in patients with AAV with active renal disease.First, we determined the absolute numbers of CD4�effector memory T cells in the urine of patients withAAV with or without renal involvement, during remis-sion and active disease. The number of urine CD4�
effector memory T cells was significantly increased inpatients with active renal AAV when compared witheither patients with AAV in whom disease was inremission (with or without renal involvement) or pa-tients with active disease without renal involvement(Figure 2A). In order to take into account varyingdegrees of urine dilution, data were also expressed as theratio of CD4� effector memory T cell numbers (cells/ml) to urine creatinine concentration (�moles/ml). Thedifferences between patient groups in CD4� effectormemory T cell numbers after correction for creatinineconcentration (Figure 2B) were similar to those beforecorrection (Figure 2A).
To address the question of whether the decreasein circulating CD4� effector memory T cells in patientswith active AAV is accompanied by a reciprocal increasein CD4� effector memory T cells at the site of inflam-mation, we examined percentages of CD4� effectormemory T cells in peripheral blood and urine in patientswith AAV. Patients with active AAV with renal involve-ment exhibited a significant increase in percentages ofCD4� effector memory T cells in urine as comparedwith both patients with AAV whose disease was inremission (with or without renal involvement) and pa-
Figure 3. Urine CD4� effector memory T cells and serum creatinine in 12 patients with AAV who were followed up for several weeks aftertreatment. The left y-axes show the number of CD4� effector memory T cells in urine (cells/ml) divided by renal creatinine (�moles/ml) (solidcircles), and the right y-axes show the concentration of serum creatinine (�moles/liter) (open circles). The x-axes show intervals in weeks. Plus andminus signs represent active and inactive urinary sediment, respectively, defined by microscopic examination as described in Patients and Methods.See Figure 2 for definitions.
2834 ABDULAHAD ET AL
tients with active AAV without renal involvement (Fig-ure 2C). In contrast, we observed lower percentages ofCD4� effector memory T cells in peripheral blood frompatients with AAV with active renal disease when com-pared with those whose disease was in remission (Figure2D). Thus, decreased numbers of circulating CD4�effector memory T cells in patients with AAV withactive renal involvement are accompanied by their re-ciprocal increase in urine.
Quantification of urine CD4� effector memory Tcells as a useful tool for assessing disease activity inpatients with AAV with renal involvement. Since num-bers of urine CD4� effector memory T cells wereincreased in patients with active renal AAV comparedwith patients with AAV whose disease was in remission,we investigated whether changes in the number of urineCD4� effector memory T cells occurred during induc-tion of remission. To this end, we analyzed absolutenumbers of urine CD4� effector memory T cells in 12patients at the time of active renal disease and at severaltime points during remission induction therapy. Resultswere corrected for urine creatinine concentration. Asshown in Figure 3, ratios of urine CD4� effectormemory T cells to urine creatinine concentration inpatients with AAV clearly decreased during treatmentand were lower during remission induction as comparedwith their ratios during the active phase of the disease.
In 9 patients with AAV, the number of urineCD4� effector memory cells decreased, coinciding witha drop in the level of serum creatinine (patients 1–5, 8,9, 11, and 12 in Figure 3). In 1 patient (patient 6 inFigure 3), an initial drop in the number of urinaryCD4� effector memory T cells coincided with a drop inserum creatinine level, while a subsequent increase inthe number of urinary CD4� effector memory T cellswas associated with stabilization without further de-crease in serum creatinine level. In 2 patients (patients 7and 10 in Figure 3), the association between changes inurinary CD4� effector memory T cell numbers andchanges in serum creatinine level were less clear. Fur-ther analysis showed that the presence of high numbersof CD4� effector memory T cells in urine was associ-ated with active glomerular disease, as assessed bymicroscopic urinary sediment analysis. These resultsstrongly suggest a link between numbers of urine CD4�effector memory T cells and renal disease activity inpatients with AAV.
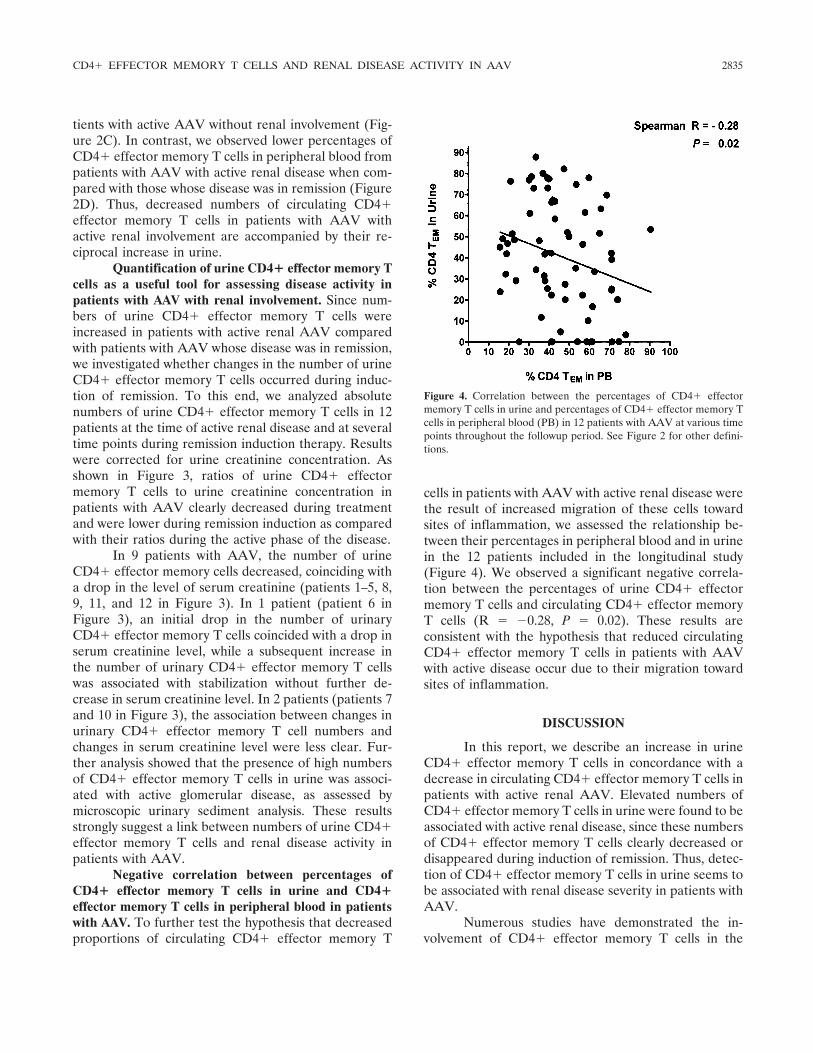
Negative correlation between percentages ofCD4� effector memory T cells in urine and CD4�effector memory T cells in peripheral blood in patientswith AAV. To further test the hypothesis that decreasedproportions of circulating CD4� effector memory T
cells in patients with AAV with active renal disease werethe result of increased migration of these cells towardsites of inflammation, we assessed the relationship be-tween their percentages in peripheral blood and in urinein the 12 patients included in the longitudinal study(Figure 4). We observed a significant negative correla-tion between the percentages of urine CD4� effectormemory T cells and circulating CD4� effector memoryT cells (R � �0.28, P � 0.02). These results areconsistent with the hypothesis that reduced circulatingCD4� effector memory T cells in patients with AAVwith active disease occur due to their migration towardsites of inflammation.
DISCUSSION
In this report, we describe an increase in urineCD4� effector memory T cells in concordance with adecrease in circulating CD4� effector memory T cells inpatients with active renal AAV. Elevated numbers ofCD4� effector memory T cells in urine were found to beassociated with active renal disease, since these numbersof CD4� effector memory T cells clearly decreased ordisappeared during induction of remission. Thus, detec-tion of CD4� effector memory T cells in urine seems tobe associated with renal disease severity in patients withAAV.
Numerous studies have demonstrated the in-volvement of CD4� effector memory T cells in the
Figure 4. Correlation between the percentages of CD4� effectormemory T cells in urine and percentages of CD4� effector memory Tcells in peripheral blood (PB) in 12 patients with AAV at various timepoints throughout the followup period. See Figure 2 for other defini-tions.
CD4� EFFECTOR MEMORY T CELLS AND RENAL DISEASE ACTIVITY IN AAV 2835

pathogenesis of autoimmune diseases. It has been shownthat autoreactive T cells in type 1 diabetes mellitus,multiple sclerosis, and rheumatoid arthritis are predom-inantly CD4� effector memory T cells (17–20). Thesecells lack the chemokine receptor CCR7, which preventstheir entry into lymphoid organs, but they express otherchemokine receptors, such as CCR5 and CCR3, alongwith selectins and adhesion molecules, which play apivotal role in the trafficking of these cells into areas ofinflammation. Indeed, enrichment of these effector cellswas demonstrated in the synovial fluid of patients withrheumatoid arthritis or juvenile idiopathic arthritis, inskin lesions of patients with psoriasis, and in infiltratesoccurring in multiple sclerosis brain tissue, as well as inglomeruli and periglomerular interstitial lesions in pa-tients with glomerulonephritis (12,21,22).
Our previous study of the distribution of circulat-ing CD4� T cell subpopulations in patients with AAVdemonstrated a significant decrease in CD4� effectormemory T cells during active disease compared with thatduring complete remission, which is consistent withincreased migration of these cells to sites of inflamma-tion once disease activity occurs (9). The results of thepresent study extend these findings and strongly suggestan increase in the numbers of CD4� effector memory Tcells in target organs, such as the kidneys, during activedisease and provide a plausible explanation for theobserved decrease in circulating CD4� effector memoryT cells in active AAV.
The presence of CD4� effector memory T cellsin the urine of patients with AAV may reflect cell-mediated immunity in the pathogenesis of renal lesionsin this disease. It has recently become evident thatCD4� effector memory T cells act as key effectors oftissue injury. Shiao and colleagues (23) have demon-strated that adoptive transfer of human CD4� effectormemory T cells into a SCID chimera model bearinghuman skin graft results in infiltration of the graft anddestruction of endothelial cells in the graft. Likewise, arecent study demonstrated the contribution of CD4�effector memory T cells to tissue injury in a model ofMPO ANCA–associated glomerulonephritis (24). In amouse model of experimental autoimmune anti-MPOglomerulonephritis, depletion of CD4� effector mem-ory T cells significantly reduced the development ofcrescentic glomerulonephritis and attenuated effectorcell influx in glomeruli as compared with control-treatedmice. This confirms the role of CD4� effector memoryT cells in renal injury in ANCA-associated vasculitis.
Consistent with these findings, in the currentstudy higher numbers of urine CD4� effector memory T
cells were observed during active renal disease, whereasthese cells clearly decreased or disappeared duringremission. Importantly, levels of circulating CD4� ef-fector memory T cells correlated negatively with theirpercentages in urine. These results support the idea thatCD4� effector memory T cells migrate to and areinvolved in renal lesions in AAV and could provide anew approach for assessing disease severity in patientswith AAV with renal involvement. The advantages ofthis approach over a renal biopsy are that it can berepeated as often as necessary and that it offers theopportunity for monitoring response to therapy. It isimportant to note that the design of our study did notinclude immunohistochemical analysis of renal biopsyspecimens. In addition, the number of patients in eachstudy group was relatively small. Owing to these limita-tions, further studies are needed to confirm our findings.
Induction of tissue injury by CD4� effectormemory T cells may require cell–cell contact with thetargeted tissue. It has previously been shown thatHLA–DR antigens are strongly expressed on renalvascular endothelial cells (25). In addition, a recentstudy by Shiao et al (23) demonstrated that the targetendothelial cells deliver costimulatory signals to CD4�effector memory T cells via the interaction of lympho-cyte function–associated antigen 3 (on endothelial cells)with CD2 (on CD4� effector memory T cells). Althoughthe in vivo function of HLA–DR expression on endo-thelial cells has not been fully elucidated, antigen pre-sentation by cultured human endothelial cells augmentstransendothelial migration of CD4� memory T cells(26). This suggests that endothelial cells are capable ofmediating CD4� effector memory T cell activation andmigration in a class II major histocompatibility complex–dependent manner.
However, CD4� effector memory T cells sharephenotypic as well as functional features with naturalkiller (NK) cells, which secrete the cytolytic moleculesperforin and granzymes, and express NK receptors(NKRs) that act as a costimulation molecule in theabsence of CD28 to induce cytotoxic activity (27–29). Ithas been shown that triggering of stimulatory KIR2DS2(an NKR) on cytotoxic CD4� T cells from patients withunstable angina induces cytotoxic activity and effectivelykills endothelial cells in vitro in a perforin-dependentway (30). In addition, the cytotoxic molecules (perforinand granzymes) effectively induce morphologic alter-ation as well as apoptosis of cultured endothelial cells,and contribute to intimal thickening of vessels in cardiactransplants in mice (31,32).
In addition to KIR2DS2, costimulation via
2836 ABDULAHAD ET AL

NKG2D enhances tissue destruction and inflammatoryresponse. It has been shown that CD4� NKG2D� Tcell clones from patients with Crohn’s disease can killtargets that express MICA via NKG2D–MICA interac-tion (33). Based on these findings, it is possible thatrenal injury in patients with AAV occurs due to thecytotoxicity of CD4� effector memory T cells, butcostimulatory triggering of these cells through NKRs,which is essential to achieve their cytotoxic function,must be present. Indeed, up-regulation of MICA hasbeen demonstrated in peritubular endothelium and glo-merular epithelial cells in the kidneys of patients withAAV during active disease, whereas no expression ofMICA was observed in normal kidneys (34). It is,therefore, possible that MICA induces the cytotoxicityof CD4� effector memory T cells in renal tissue inpatients with AAV and may contribute to renal injuryand disease progression. In this regard, further studiesare needed to delineate the cytotoxicity of CD4� effec-tor memory T cells in AAV.
In summary, the current study demonstrates aprominent increase in urine CD4� effector memory Tcells in association with active renal disease in AAV.Taken together, this finding and our previous observa-tions suggest that CD4� effector memory T cells mi-grate toward sites of inflammation and act as effectorcells in renal injury in patients with AAV. Thus, detec-tion of elevated urine CD4� effector memory T cellscould be clinically useful for evaluating and monitoringrenal disease activity in patients with AAV.
ACKNOWLEDGMENTS
We thank Marcel J. van der Leij for technical assis-tance, and we are grateful to the patients for their cooperationand participation in this study.
AUTHOR CONTRIBUTIONS
Dr. Abdulahad had full access to all of the data in the studyand takes responsibility for the integrity of the data and the accuracyof the data analysis.Study design. Abdulahad.Acquisition of data. Abdulahad, Kallenberg, Limburg, Stegeman.Analysis and interpretation of data. Abdulahad, Kallenberg, Limburg,Stegeman.Manuscript preparation. Abdulahad, Kallenberg, Limburg, Stegeman.Statistical analysis. Abdulahad.
REFERENCES
1. Jennette JC, Falk RJ. Small-vessel vasculitis. N Engl J Med1997;337:1512–23.
2. Savage CO, Harper L, Adu D. Primary systemic vasculitis. Lancet1997;349:553–8.
3. Kallenberg CG. Churg-Strauss syndrome: just one disease entity?[editorial]. Arthritis Rheum 2005;52:2589–93.
4. Gephardt GN, Ahmad M, Tubbs RR. Pulmonary vasculitis (We-gener’s granulomatosis): immunohistochemical study of T and Bcell markers. Am J Med 1983;74:700–4.
5. Ten Berge IJ, Wilmink JM, Meyer CJ, Surachno J, ten Veen KH,Balk TG, et al. Clinical and immunological follow-up of patientswith severe renal disease in Wegener’s granulomatosis. Am JNephrol 1985;5:21–9.
6. Bolton WK, Innes DJ Jr, Sturgill BC, Kaiser DL. T-cells andmacrophages in rapidly progressive glomerulonephritis: clinico-pathologic correlations. Kidney Int 1987;32:869–76.
7. Lockwood CM, Thiru S, Stewart S, Hale G, Isaacs J, Wraight P, etal. Treatment of refractory Wegener’s granulomatosis with hu-manized monoclonal antibodies. QJM 1996;89:903–12.
8. Hagen EC, de Keizer RJ, Andrassy K, van Boven WP, Bruijn JA,van Es LA, et al. Compassionate treatment of Wegener’s granu-lomatosis with rabbit anti-thymocyte globulin. Clin Nephrol 1995;43:351–9.
9. Abdulahad WH, van der Geld YM, Stegeman CA, Kallenberg CG.Persistent expansion of CD4� effector memory T cells in Wege-ner’s granulomatosis. Kidney Int 2006;70:938–47.
10. Abdulahad WH, Stegeman CA, van der Geld YM, Doornbos-vander Meer B, Limburg PC, Kallenberg CG. Functional defect ofcirculating regulatory CD4� T cells in patients with Wegener’sgranulomatosis in remission. Arthritis Rheum 2007;56:2080–91.
11. Abdulahad WH, Stegeman CA, Limburg PC, Kallenberg CG.CD4-positive effector memory T cells participate in disease ex-pression in ANCA-associated vasculitis. Ann N Y Acad Sci2007;1107:22–31.
12. Sakatsume M, Xie Y, Ueno M, Obayashi H, Goto S, Narita I, et al.Human glomerulonephritis accompanied by active cellular infil-trates shows effector T cells in urine. J Am Soc Nephrol 2001;12:2636–44.
13. Deenitchina SS, Ando T, Akazawa K, Hirakata H, Fujishima M.Prediction of the clinical and histological severity of IgA nephrop-athy by flow cytometry of urinary mononuclear cells. Clin ExpNephrol 1999;3:272–8.
14. Grunewald RW, Fiedler GM, Stock B, Grunewald JM, MullerGA. Immunocytological determination of lymphocytes and mono-cytes/macrophages in urinary sediments of renal allograft recipi-ents. Nephrol Dial Transplant 2000;15:888–92.
15. Chan RW, Lai FM, Li EK, Tam LS, Chung KY, Chow KM, et al.Urinary mononuclear cell and disease activity of systemic lupuserythematosus. Lupus 2006;15:262–7.
16. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P,et al. Birmingham Vasculitis Activity Score (BVAS) in systemicnecrotizing vasculitis. QJM 1994;87:671–8.
17. Viglietta V, Kent SC, Orban T, Hafler DA. GAD65-reactive Tcells are activated in patients with autoimmune type 1a diabetes[published erratum appears in J Clin Invest 2002;109:1511]. J ClinInvest 2002;109:895–903.
18. Wulff H, Calabresi PA, Allie R, Yun S, Pennington M, Beeton C,et al. The voltage-gated Kv1.3 K� channel in effector memory Tcells as new target for MS [published erratum appears in J ClinInvest 2003;112:298]. J Clin Invest 2003;111:1703–13.
19. Burns J, Bartholomew B, Lobo S. Isolation of myelin basicprotein-specific T cells predominantly from the memory T-cellcompartment in multiple sclerosis. Ann Neurol 1999;45:33–9.
20. Beeton C, Wulff H, Standifer NE, Azam P, Mullen KM, Penning-ton MW, et al. Kv1.3 channels are a therapeutic target for Tcell-mediated autoimmune diseases. Proc Natl Acad Sci U S A2006;103:17414–9.
21. Friedrich M, Krammig S, Henze M, Docke WD, Sterry W,Asadullah K. Flow cytometric characterization of lesional T cellsin psoriasis: intracellular cytokine and surface antigen expression
CD4� EFFECTOR MEMORY T CELLS AND RENAL DISEASE ACTIVITY IN AAV 2837

indicates an activated, memory/effector type 1 immunophenotype.Arch Dermatol Res 2000;292:519–21.
22. Gattorno M, Prigione I, Morandi F, Gregorio A, Chiesa S, FerlitoF, et al. Phenotypic and functional characterisation of CCR7� andCCR7� CD4� memory T cells homing to the joints in juvenileidiopathic arthritis. Arthritis Res Ther 2005;7:R256–67.
23. Shiao SL, Kirkiles-Smith NC, Shepherd BR, McNiff JM, Carr EJ,Pober JS. Human effector memory CD4� T cells directly recog-nize allogeneic endothelial cells in vitro and in vivo. J Immunol2007;179:4397–404.
24. Ruth AJ, Kitching AR, Kwan RY, Odobasic D, Ooi JD, Timos-hanko JR, et al. Anti-neutrophil cytoplasmic antibodies and effec-tor CD4� cells play nonredundant roles in anti-myeloperoxidasecrescentic glomerulonephritis. J Am Soc Nephrol 2006;17:1940–9.
25. Hayry P, von Willebrand E, Andersson LC. Expression of HLA-ABC and -DR locus antigens on human kidney, endothelial,tubular and glomerular cells. Scand J Immunol 1980;11:303–10.
26. Marelli-Berg FM, Frasca L, Weng L, Lombardi G, Lechler RI.Antigen recognition influences transendothelial migration ofCD4� T cells. J Immunol 1999;162:696–703.
27. Appay V, Zaunders JJ, Papagno L, Sutton J, Jaramillo A, WatersA, et al. Characterization of CD4� CTLs ex vivo. J Immunol2002;168:5954–8.
28. Van Bergen J, Thompson A, van der Slik A, Ottenhoff TH,Gussekloo J, Koning F. Phenotypic and functional characteriza-
tion of CD4 T cells expressing killer Ig-like receptors. J Immunol2004;173:6719–26.
29. Snyder MR, Weyand CM, Goronzy JJ. The double life of NKreceptors: stimulation or co-stimulation? Trends Immunol 2004;25:25–32.
30. Nakajima T, Schulte S, Warrington KJ, Kopecky SL, Frye RL,Goronzy JJ, et al. T-cell-mediated lysis of endothelial cells in acutecoronary syndromes. Circulation 2002;105:570–5.
31. Choy JC, Cruz RP, Kerjner A, Geisbrecht J, Sawchuk T, FraserSA, et al. Granzyme B induces endothelial cell apoptosis andcontributes to the development of transplant vascular disease.Am J Transplant 2005;5:494–9.
32. Choy JC, Kerjner A, Wong BW, McManus BM, Granville DJ.Perforin mediates endothelial cell death and resultant transplantvascular disease in cardiac allografts. Am J Pathol 2004;165:127–33.
33. Allez M, Tieng V, Nakazawa A, Treton X, Pacault V, Dulphy N,et al. CD4�NKG2D� T cells in Crohn’s disease mediate inflam-matory and cytotoxic responses through MICA interactions. Gas-troenterology 2007;132:2346–58.
34. Holmen C, Elsheikh E, Stenvinkel P, Qureshi AR, Pettersson E,Jalkanen S, et al. Circulating inflammatory endothelial cellscontribute to endothelial progenitor cell dysfunction in patientswith vasculitis and kidney involvement. J Am Soc Nephrol 2005;16:3110–20.
2838 ABDULAHAD ET AL