thalassemia chelation update: prof raymond wong
TRANSCRIPT
RAYMOND WONG, MDHong Kong
• Consultant of the Department of Medicine & Therapeutics, Prince of Wales Hospital
• Dr. Wong received his medical degree from the Chinese University of Hong Kong and received his training in Haematology, Internal Medicine as well as Clinical Pharmacology and Therapeutics at the Prince of Wales Hospital, Hong Kong. He also obtained his Doctor of Medicine from the Chinese University of Hong Kong. He joined the Prince of Wales Hospital Poison Treatment Centre since its establishment in 2005 which is a tertiary referral centre for the management of patients with poisoning. Dr. Wong has published over 70 articles in peer-reviewed journals including Blood, Circulation, JAMA and the New England Journal of Medicine in various areas of haematology and therapeutics.

Thalassemia: Chelation Update
Dr. Raymond SM Wong
Department of Medicine & Therapeutics
The Chinese University of Hong Kong
BTG 2015
Chelation Update
•Monitoring of iron overload
•Combination of iron chelators
• Iron chelation for patients with non-transfusion-dependent thalassemia (NTDT)

Monitoring of Iron Overload
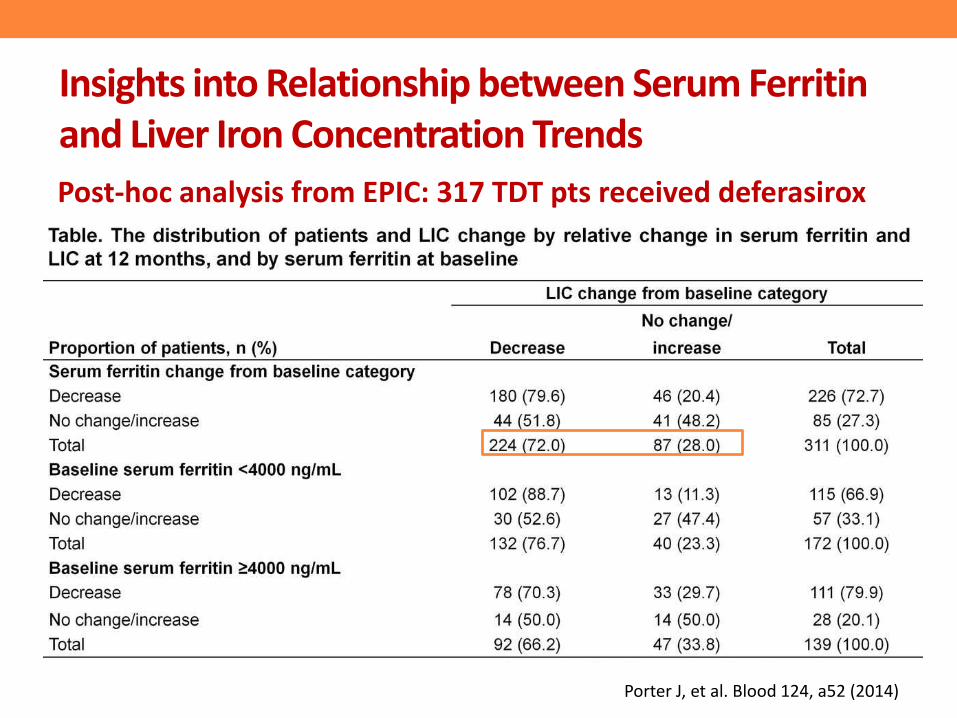
Insights into Relationship between Serum Ferritin and Liver Iron Concentration Trends
Post-hoc analysis from EPIC: 317 TDT pts received deferasirox
Porter J, et al. Blood 124, a52 (2014)
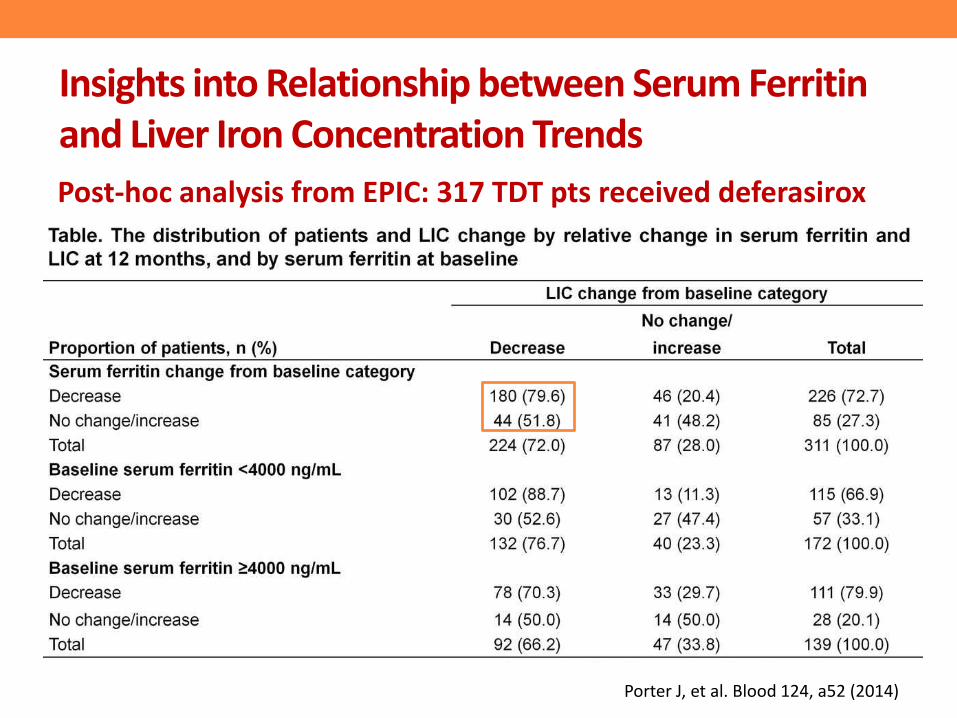
Insights into Relationship between Serum Ferritin and Liver Iron Concentration Trends
Post-hoc analysis from EPIC: 317 TDT pts received deferasirox
Porter J, et al. Blood 124, a52 (2014)
• Serum ferritin response can help predict LIC response
• In some patients treated with deferasirox, serum ferritin may not accurately reflect removal of iron from the body
• Among patients with no serum ferritin response, up to half may be responding with respect to iron balance
• MRI should be prioritized for patients with serum ferritin increase/no change
Insights into Relationship between Serum Ferritin and Liver Iron Concentration Trends
Porter J, et al. Blood 124, a52 (2014)

Iron Chelators in Clinical Use
Sheth S. Curr Opin Hematol 2014

Combination of Iron Chelators
Sheth S. Curr Opin Hematol 2014
• 1 year prospective study (n=20) comparing deferoxamine (DFO) monotherapy or when combined with deferiprone (DFP) for patients with LVEF <56%
• DFO 50–60 mg/kg 12–24 hour/day sc/iv 7 times per week +/- DFP 75 mg/kg/day
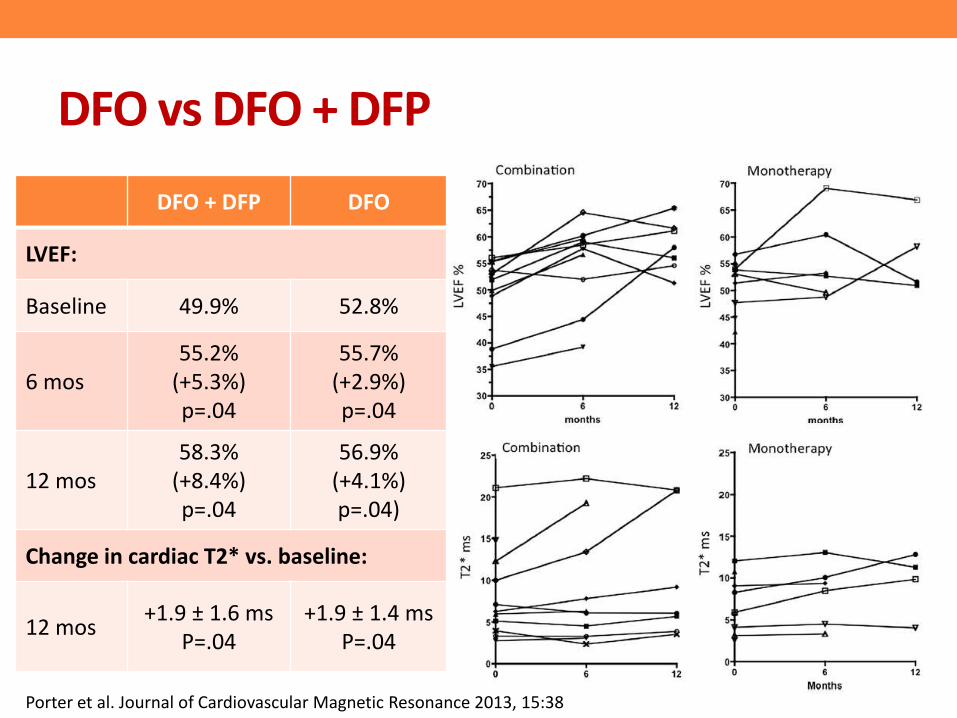
DFO vs DFO + DFP
DFO + DFP DFO
LVEF:
Baseline 49.9% 52.8%
6 mos55.2%
(+5.3%)p=.04
55.7%(+2.9%) p=.04
12 mos58.3%
(+8.4%)p=.04
56.9%(+4.1%) p=.04)
Change in cardiac T2* vs. baseline:
12 mos+1.9 ± 1.6 ms
P=.04+1.9 ± 1.4 ms
P=.04
Porter et al. Journal of Cardiovascular Magnetic Resonance 2013, 15:38
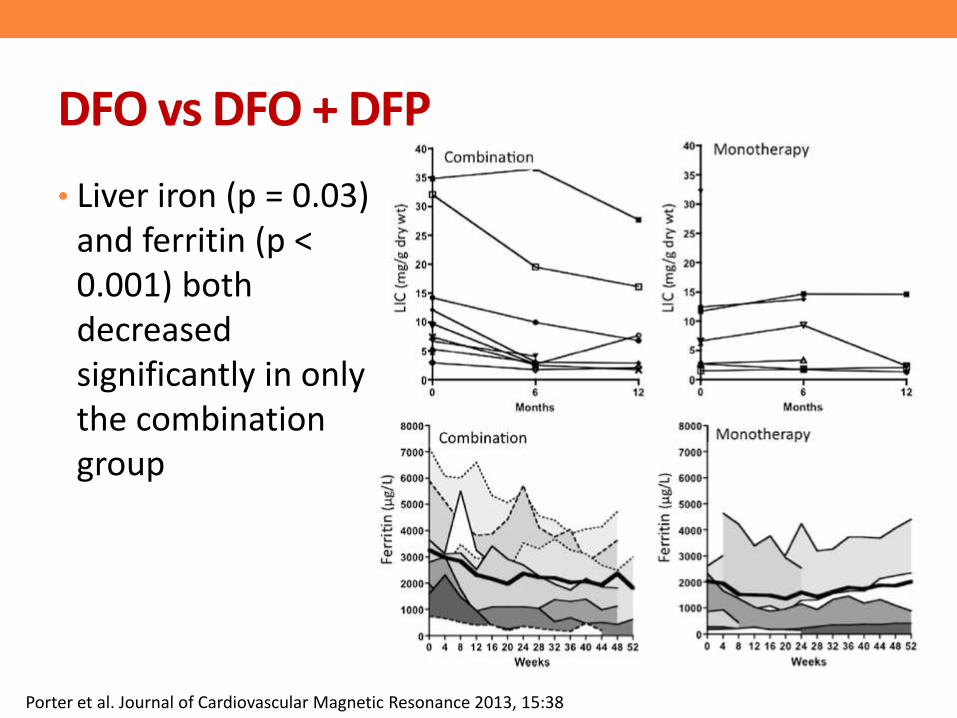
DFO vs DFO + DFP
• Liver iron (p = 0.03) and ferritin (p < 0.001) both decreased significantly in only the combination group
Porter et al. Journal of Cardiovascular Magnetic Resonance 2013, 15:38
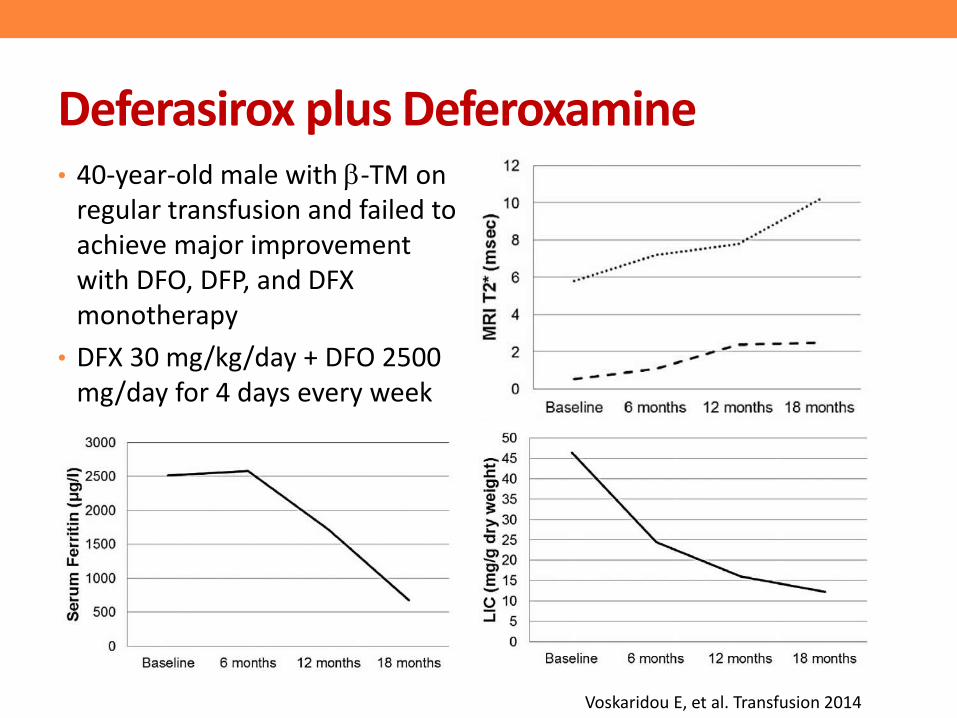
Deferasirox plus Deferoxamine• 40-year-old male with b-TM on
regular transfusion and failed to achieve major improvement with DFO, DFP, and DFX monotherapy
• DFX 30 mg/kg/day + DFO 2500 mg/day for 4 days every week
Voskaridou E, et al. Transfusion 2014
• To evaluate the safety and efficacy of combined therapy with deferasirox (DFX, 20-30 mg/kg daily) and deferoxamine (DFO, 35-50 mg/kg on 3-7 days/week) in 22 patients with persistent iron overload or organ damage
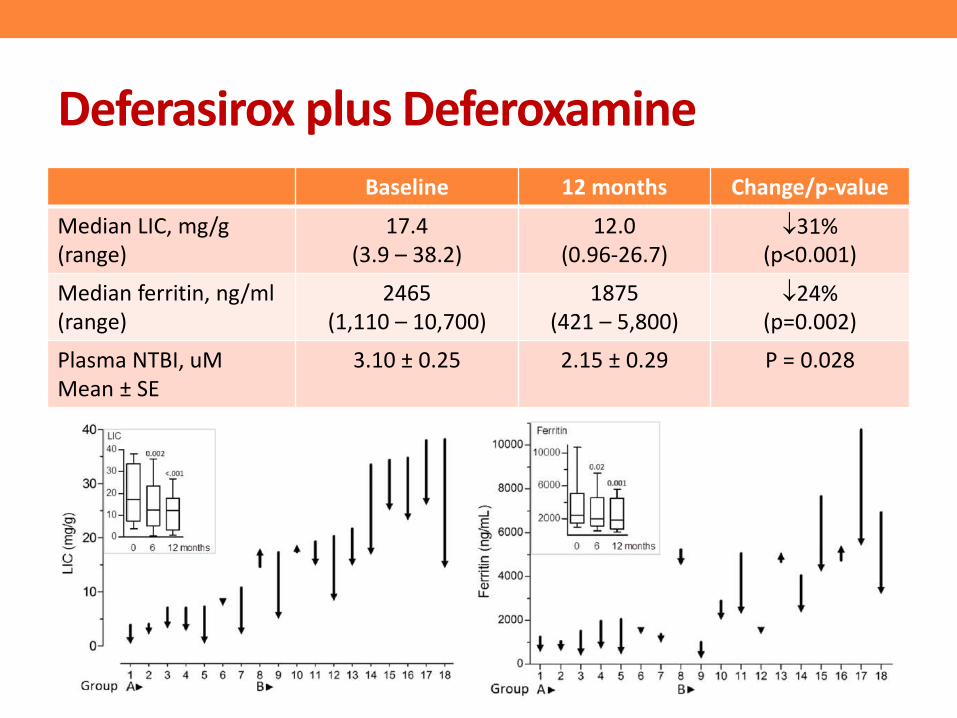
Deferasirox plus Deferoxamine
Baseline 12 months Change/p-value
Median LIC, mg/g(range)
17.4 (3.9 – 38.2)
12.0 (0.96-26.7)
31% (p<0.001)
Median ferritin, ng/ml (range)
2465 (1,110 – 10,700)
1875 (421 – 5,800)
24% (p=0.002)
Plasma NTBI, uMMean ± SE
3.10 ± 0.25 2.15 ± 0.29 P = 0.028

Deferasirox plus Deferoxamine
• Administration of DFX during infusion of DFO further lowered NTBI (-0.28 ±0.08 μM, p=0.004) and labile plasma iron (LPI, -0.03 ± 0.01 μM, p=0.006)
• The simultaneous administration of DFO and DFX rapidly reduced systemic and myocardial iron, and provided an excellent control of the toxic labile plasma iron species without an increase in toxicity
Lal A, et al. Blood Cells Mol Dis 2013

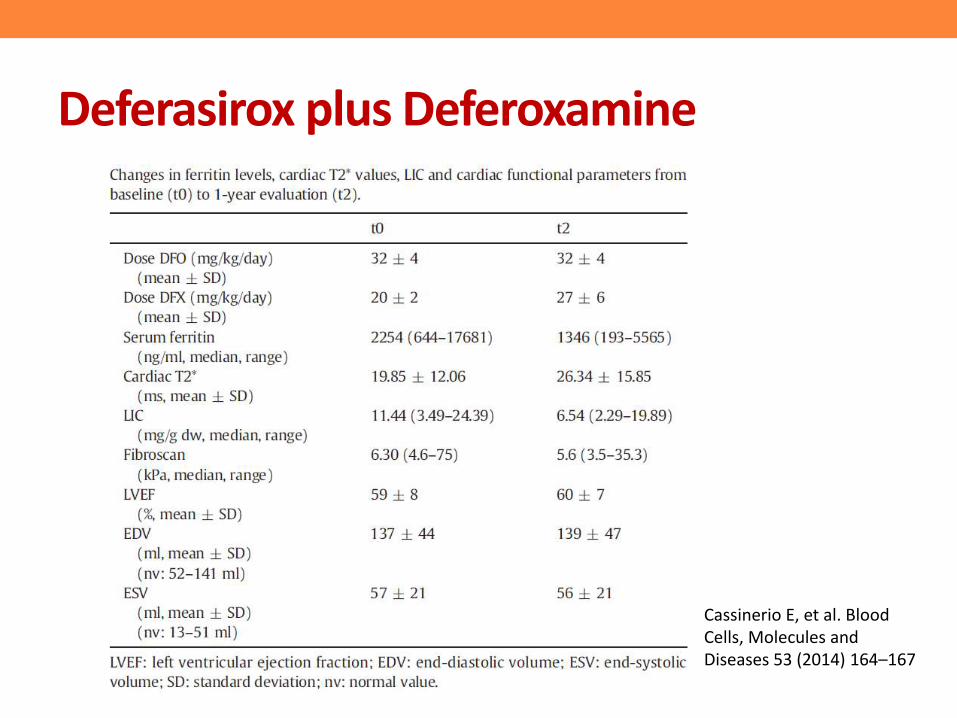
• 10 TDT patients received DFX/DFO for lack of efficacy with monotherapy or adverse events
• Starting doses: DFO 32 ± 4 mg/kg/day for 3–4 days a week and DFX 20 ± 2 mg/kg/day
Cassinerio E, et al. Blood Cells, Molecules and Diseases 53 (2014) 164–167
Deferasirox plus Deferoxamine
Cassinerio E, et al. Blood Cells, Molecules and Diseases 53 (2014) 164–167

Deferasirox plus Deferoxamine
• At 1 year an increased dose of DFX was administered (27±6 mg/kg/day vs 20±2 mg/kg/day at baseline, p= 0.01) with a stable dose of DFO (32 ± 4 mg/kg/day)
Cassinerio E, et al. Blood Cells, Molecules and Diseases 53 (2014) 164–167
Cardiac T2*
LIC
Deferasirox (DFX)/deferiprone (DFP) vs. deferoxamine (DFO)/deferiprone
• A prospective randomized trial on 96 young β-TM patients with severe iron overload
• Patients were randomized to receive either DFP + DFO (arm 1) or DFP + DFX (arm 2)
• Efficacy endpoints difference between two groups in the change of:
• serum ferritin(SF)
• liver iron concentration (LIC)
• cardiac MRI
• quality of life (QoL)Elalfy MS, et al. EJH 2015

Elalfy MS, et al. EJH 2015
DFP + DFX
DFP + DFO
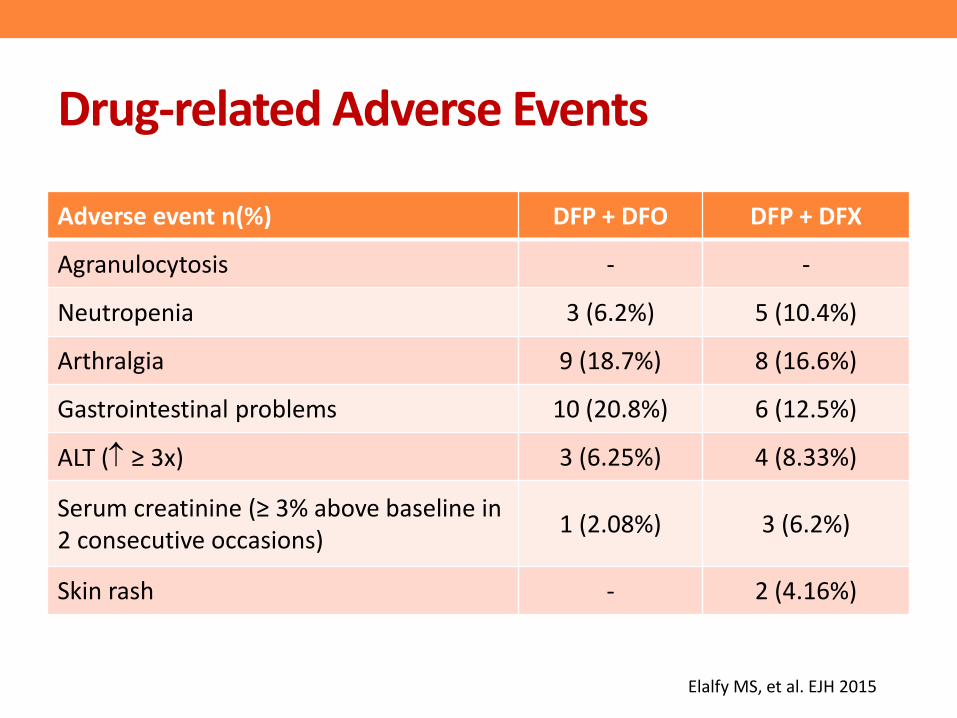
Drug-related Adverse Events
Adverse event n(%) DFP + DFO DFP + DFX
Agranulocytosis - -
Neutropenia 3 (6.2%) 5 (10.4%)
Arthralgia 9 (18.7%) 8 (16.6%)
Gastrointestinal problems 10 (20.8%) 6 (12.5%)
ALT ( ≥ 3x) 3 (6.25%) 4 (8.33%)
Serum creatinine (≥ 3% above baseline in 2 consecutive occasions)
1 (2.08%) 3 (6.2%)
Skin rash - 2 (4.16%)
Elalfy MS, et al. EJH 2015
• Both iron chelation combination regimens were equally effective in reducing iron overload and improving quality of life
• DFP/DFX combination proved superior in improving cardiac T2*, treatment compliance and patients satisfaction with no greater adverse events
Deferasirox (DFX)/deferiprone (DFP) vs. deferoxamine (DFO)/deferiprone
Elalfy MS, et al. EJH 2015
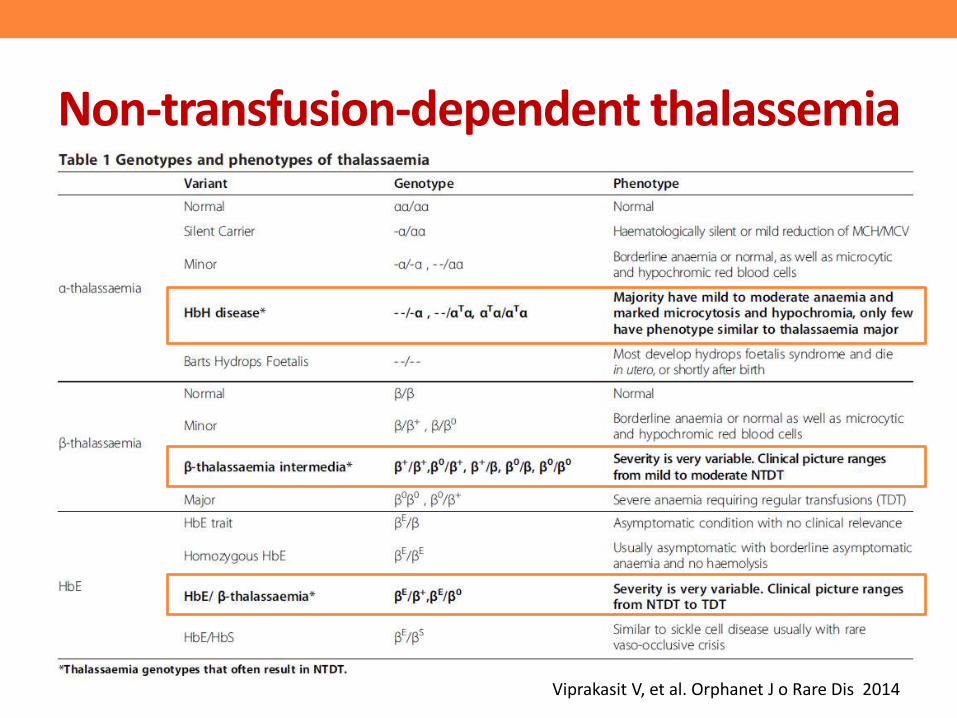
Non-transfusion-dependent thalassemia
Viprakasit V, et al. Orphanet J o Rare Dis 2014
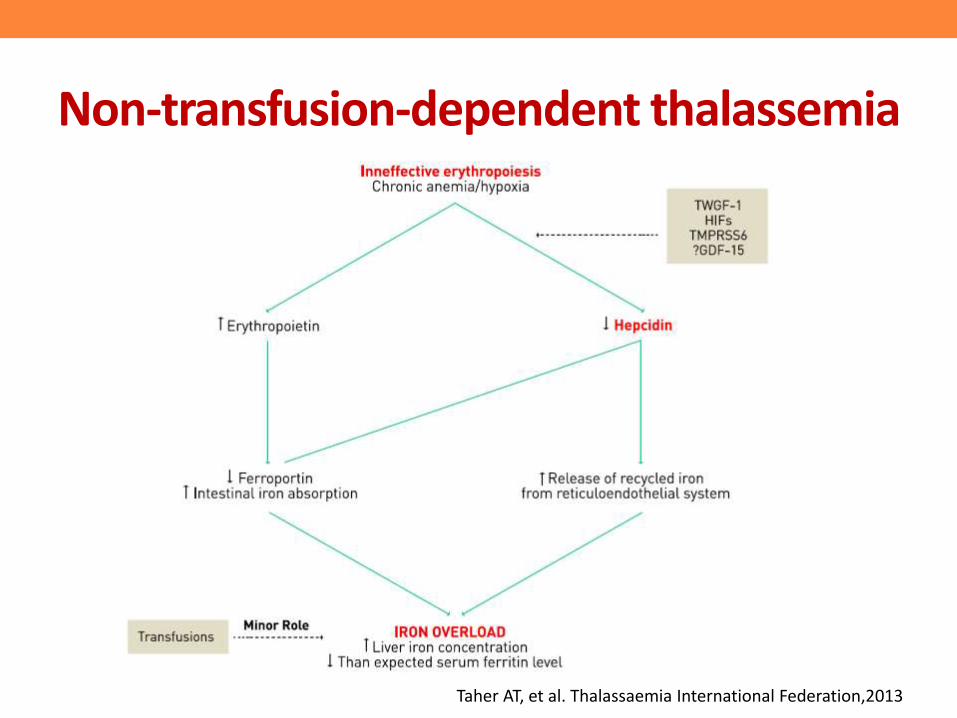
Non-transfusion-dependent thalassemia
Taher AT, et al. Thalassaemia International Federation,2013
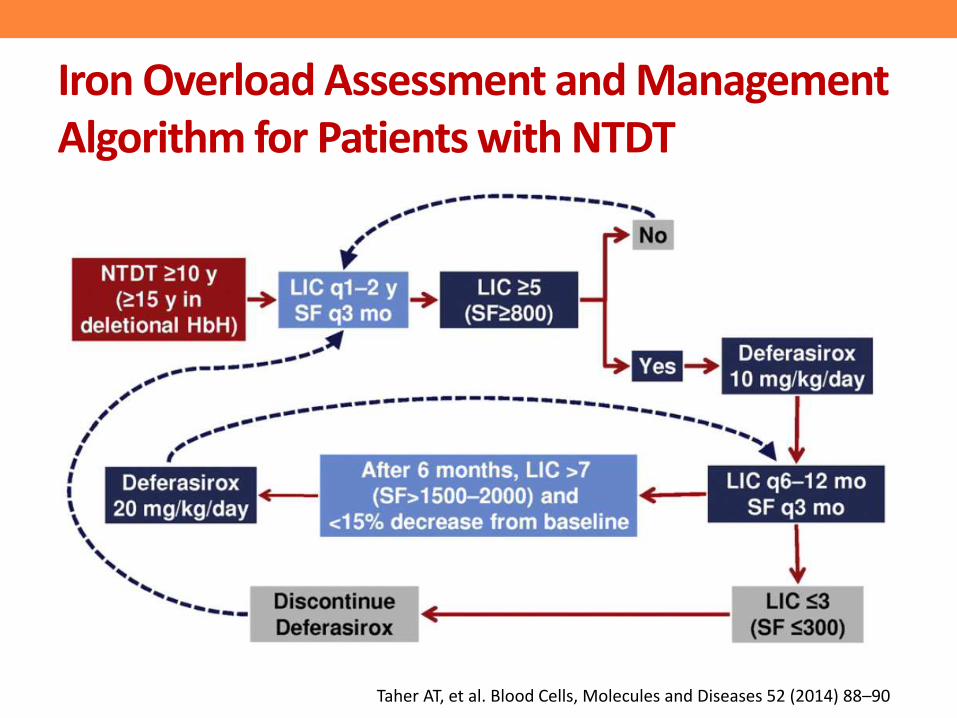
Iron Overload Assessment and Management Algorithm for Patients with NTDT
Taher AT, et al. Blood Cells, Molecules and Diseases 52 (2014) 88–90

Serum Ferritin versus LIC in TM and TI
Taher et al. AJH 2010

Taher AT, et al. BJH 2014
Using data from screened patients and those treated with deferasirox for up to 2 years in THALASSA study
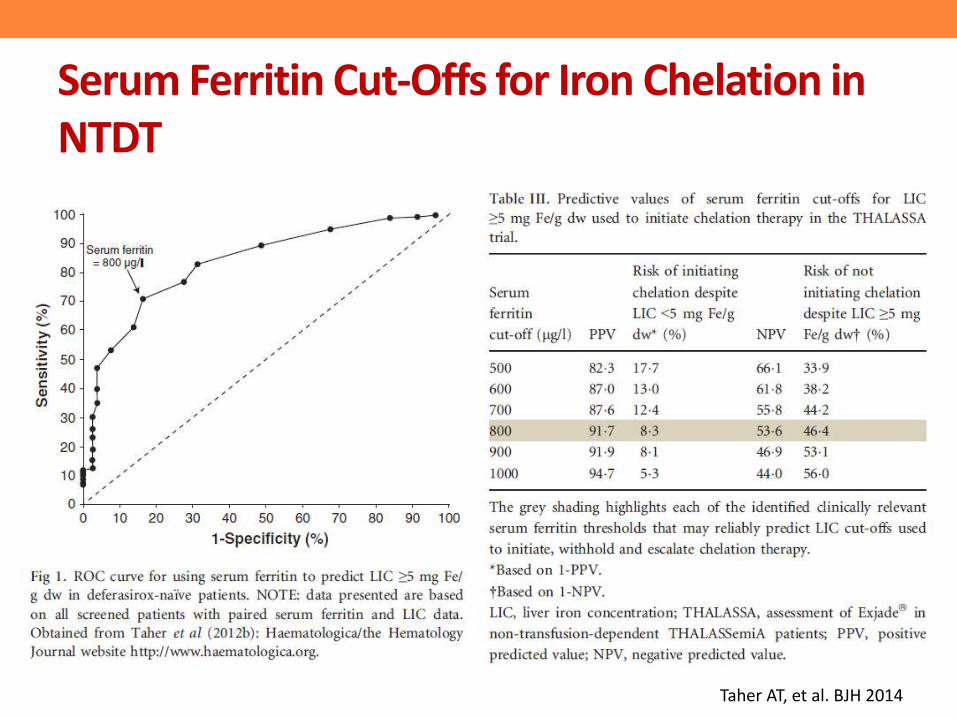
Serum Ferritin Cut-Offs for Iron Chelation in NTDT
Taher AT, et al. BJH 2014

Clinically relevant serum ferritin thresholds (when MRI is unavailable):
• for initiation of chelation therapy: >800 mg/l, as well as
• chelator dose interruption: <300 mg/l
• dose escalation: >2000 mg/l
Serum Ferritin Cut-Offs for Iron Chelation in NTDT
Taher AT, et al. BJH 2014
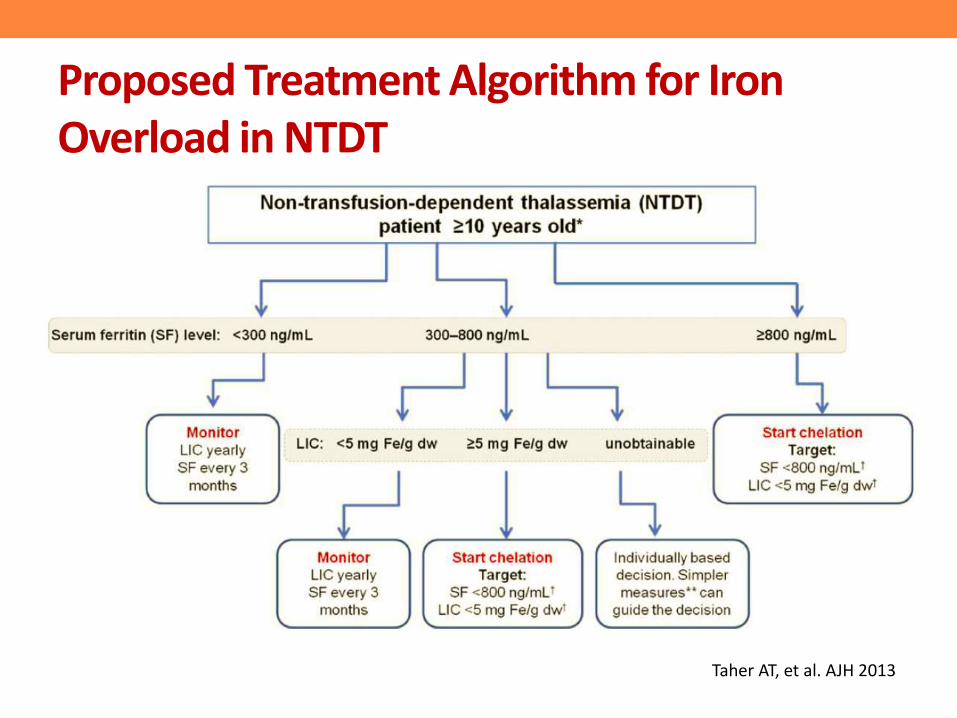
Proposed Treatment Algorithm for Iron Overload in NTDT
Taher AT, et al. AJH 2013

Iron chelation therapy in NTDT patients: DFO
• short duration and absence of assessment of tissue iron content
• parenteral therapy inconvenient to patients
Taher AT, et al. Thalassaemia International Federation,2013
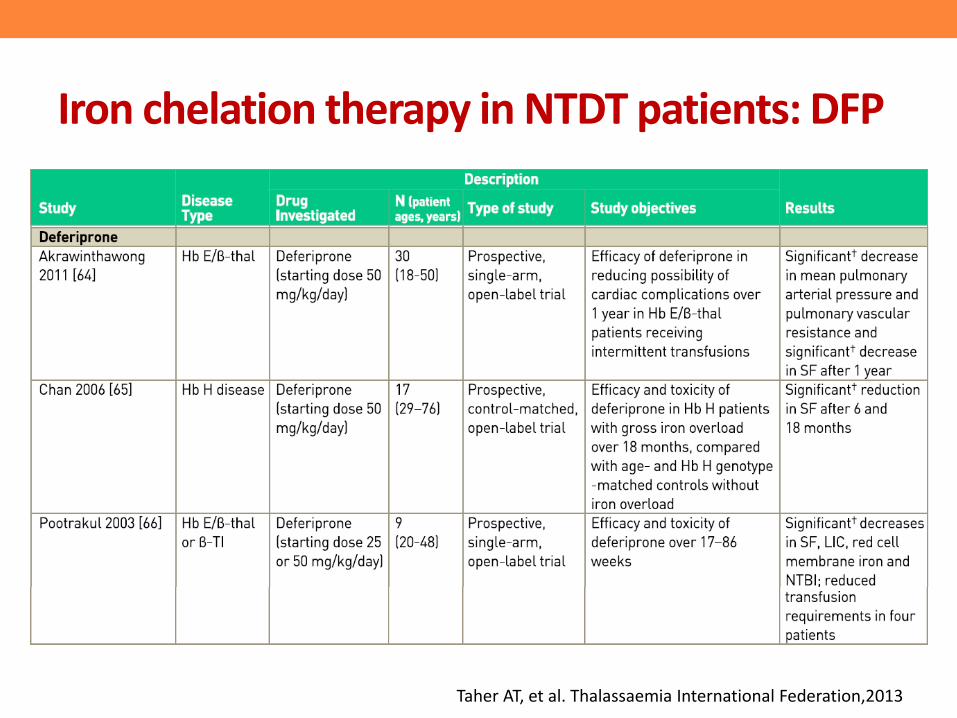
Iron chelation therapy in NTDT patients: DFP
Taher AT, et al. Thalassaemia International Federation,2013
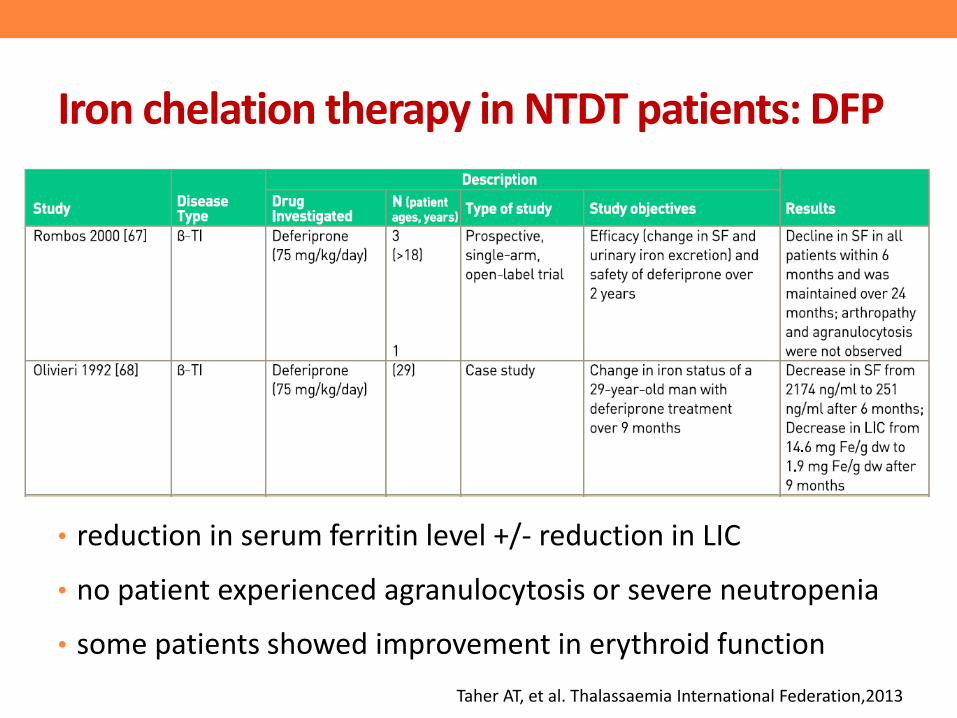
Iron chelation therapy in NTDT patients: DFP
• reduction in serum ferritin level +/- reduction in LIC
• no patient experienced agranulocytosis or severe neutropenia
• some patients showed improvement in erythroid function
Taher AT, et al. Thalassaemia International Federation,2013
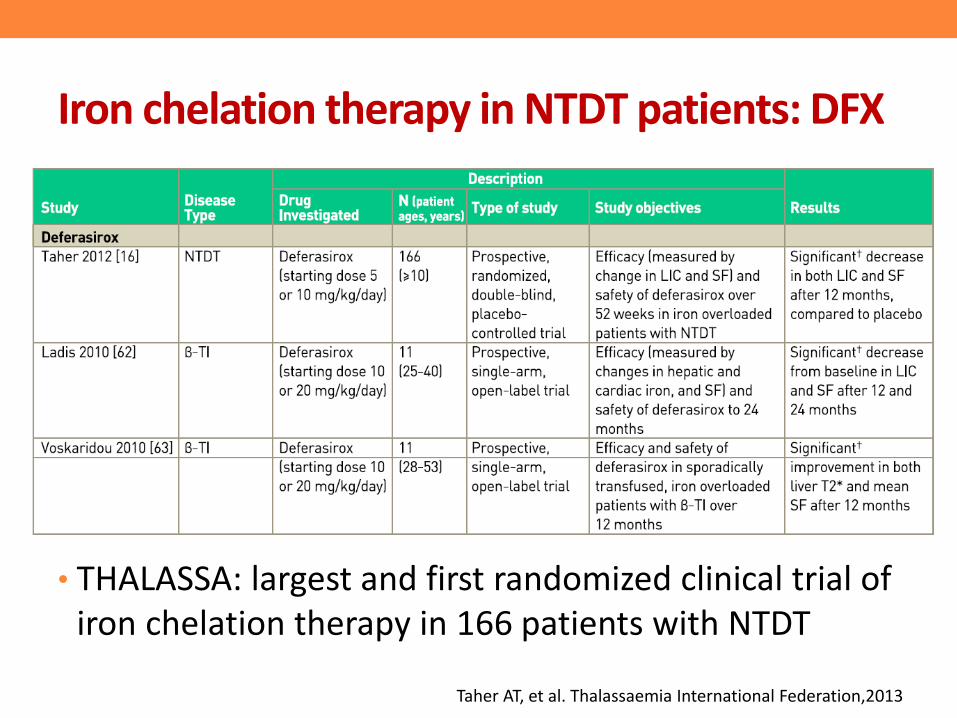
Iron chelation therapy in NTDT patients: DFX
• THALASSA: largest and first randomized clinical trial of iron chelation therapy in 166 patients with NTDT
Taher AT, et al. Thalassaemia International Federation,2013
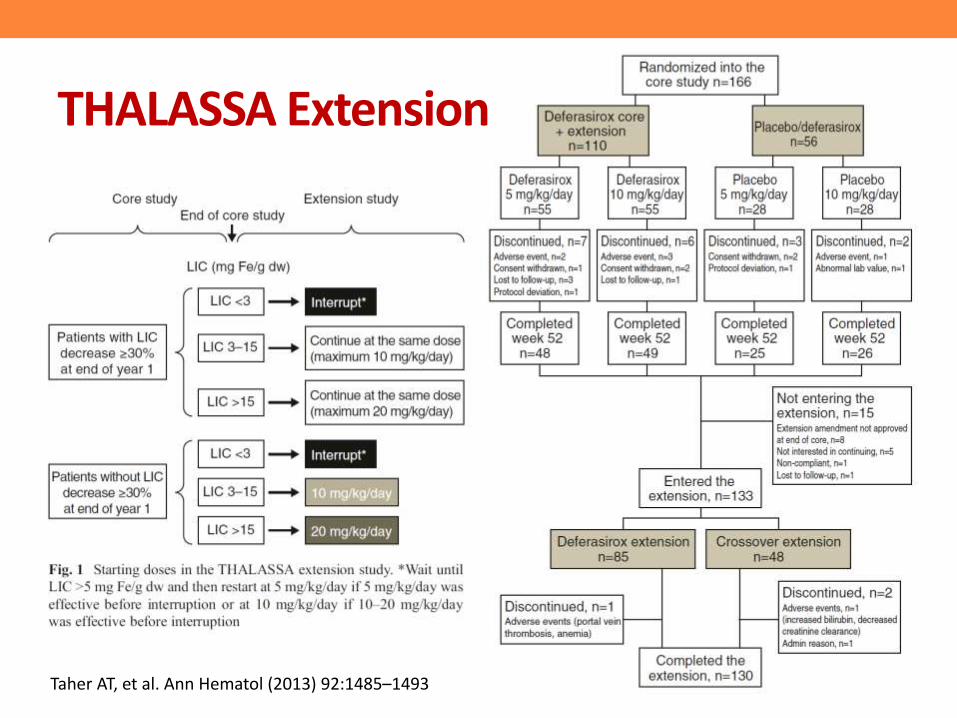
• Patients with NTDT who completed the THALASSA core study randomized to deferasirox or placebo continued with deferasirox or crossed from placebo to deferasirox
Taher AT, et al. Ann Hematol (2013) 92:1485–1493
Taher AT, et al. Ann Hematol (2013) 92:1485–1493
THALASSA Extension
THALASSA Extension
THALASSA Extension
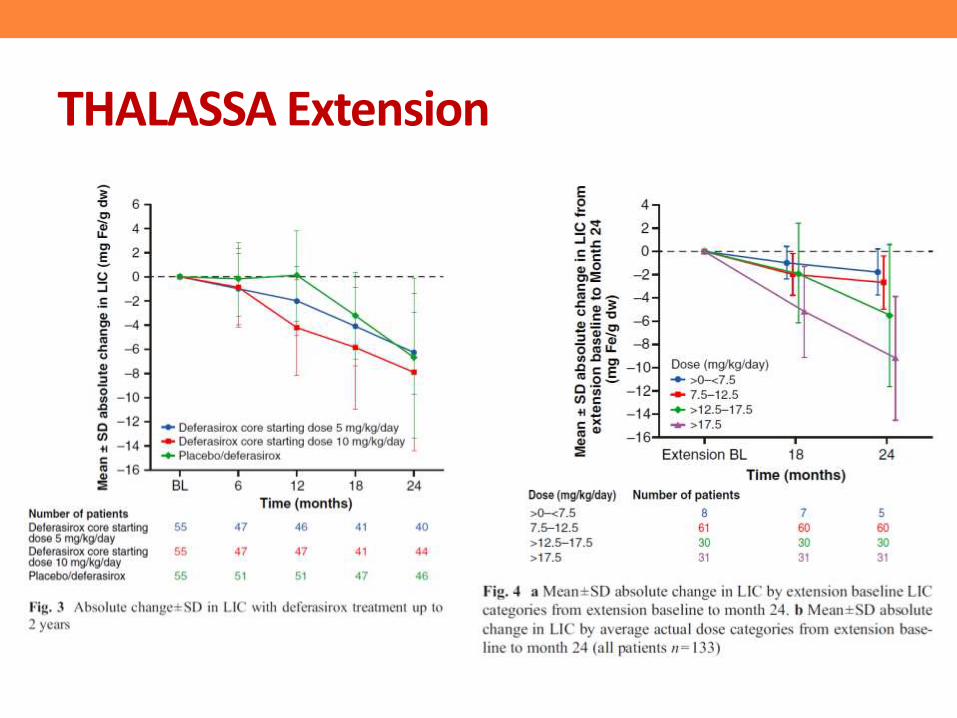
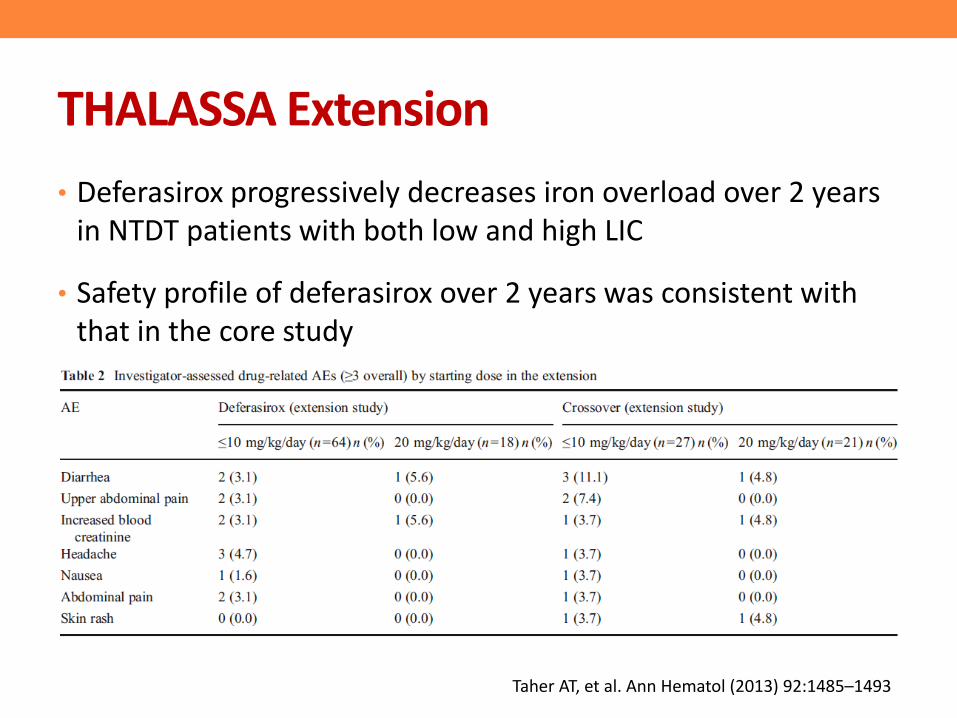
• Deferasirox progressively decreases iron overload over 2 years in NTDT patients with both low and high LIC
• Safety profile of deferasirox over 2 years was consistent with that in the core study
Taher AT, et al. Ann Hematol (2013) 92:1485–1493
Summary
• MRI techniques allow more precise quantitation of body iron burden and differential tissue deposition.
• Serum ferritin response can help predict LIC response
• Combination therapy allows for intensification of chelation in those with higher iron burdens, as well as allowing for adequate chelation in those who have dose-limiting toxicity with a monotherapy
• Patients with NTDT also require regular monitoring of body iron status and chelation therapy should be commenced if there is evidence of overload
The End
Thank you