neurology news from the inaugural european ispor meeting
TRANSCRIPT
6 I_n_t_e_r_n_a_t1_'o__n_a_l__R_e_s_e_a__rc__h_a_n_d__O.....p_i_n_i.o_ns_
1I
Neurology news from the inaugural European ISPOR meeting[Cologne, Gennany December 1998]
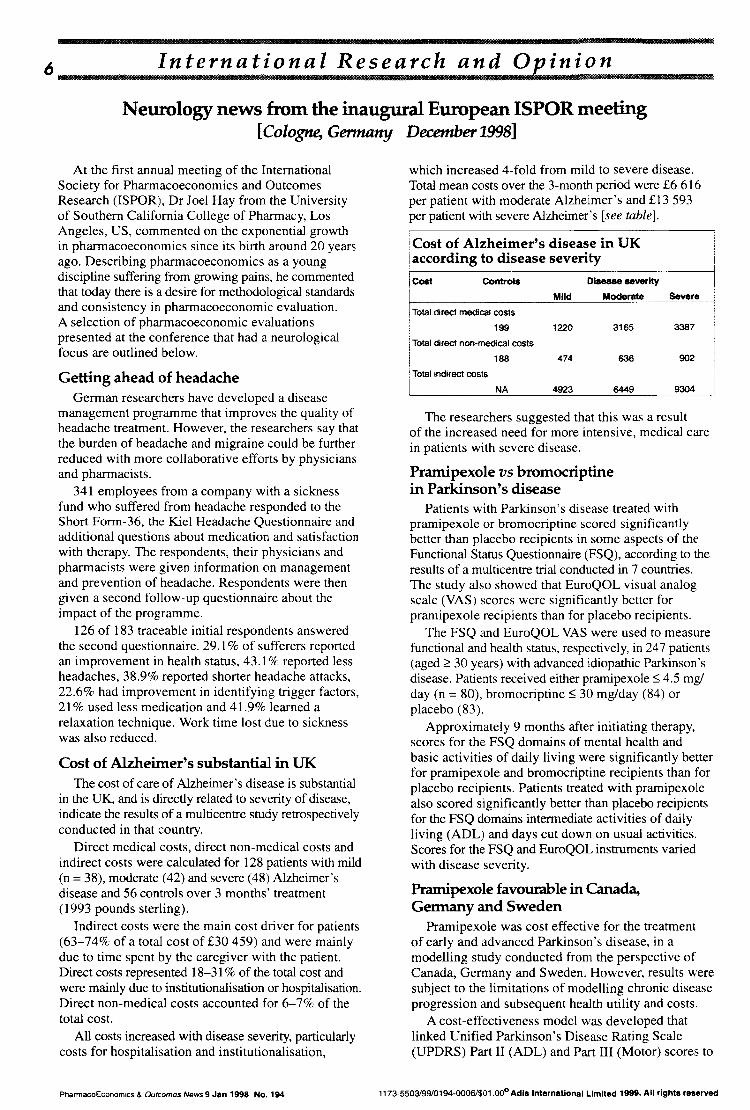
which increased 4-fold from mild to severe disease.Total mean costs over the 3-month period were £6 616per patient with moderate Alzheimer's and £13593per patient with severe Alzheimer's [see table].
:Cost of Alzheimer's disease in UKi according to disease severity
ITotal direct medical costs
199
902
3387
Severe
636
3165
Disease severity
Moderate
474
Mild
1220
188
Contro"ICost
iTotal direct non-medical costsI!
At the first annual meeting of the InternationalSociety for Pharmacoeconomics and OutcomesResearch (ISPOR), Dr Joel Hay from the Universityof Southern California College of Pharmacy, LosAngeles, US, commented on the exponential growthin pharmacoeconomics since its birth around 20 yearsago. Describing pharmacoeconomics as a youngdiscipline suffering from growing pains, he commentedthat today there is a desire for methodological standardsand consistency in pharmacoeconomic evaluation.A selection of pharmacoeconomic evaluationspresented at the conference that had a neurologicalfocus are outlined below.
Pramipexole favourable in Canada,Gennanyand Sweden
Pramipexole was cost effective for the treatmentof early and advanced Parkinson's disease, in amodelling study conducted from the perspective ofCanada, Germany and Sweden. However, results weresubject to the limitations of modelling chronic diseaseprogression and subsequent health utility and costs.
A cost-effectiveness model was developed thatlinked Unified Parkinson's Disease Rating Scale(UPDRS) Part II (ADL) and Part III (Motor) scores to
The researchers suggested that this was a resultof the increased need for more intensive, medical carein patients with severe disease.
Pramipexole vs bromocriptinein Parkinson's disease
Patients with Parkinson's disease treated withprarnipexole or bromocriptine scored significantlybetter than placebo recipients in some aspects of theFunctional Status Questionnaire (FSQ), according to theresults of a multicentre trial conducted in 7 countries.The study also showed that EuroQOL visual analogscale (VAS) scores were significantly better forprarnipexole recipients than for placebo recipients.
The FSQ and EuroQOL VAS were used to measurefunctional and health status, respectively, in 247 patients(aged ~ 30 years) with advanced idiopathic Parkinson'sdisease. Patients received either prarnipexole ~ 4.5 mg/day (n = 80), bromocriptine ~ 30 mg/day (84) orplacebo (83).
Approximately 9 months after initiating therapy,scores for the FSQ domains of mental health andbasic activities of daily living were significantly betterfor pramipexole and bromocriptine recipients than forplacebo recipients. Patients treated with prarnipexolealso scored significantly better than placebo recipientsfor the FSQ domains intermediate activities of dailyliving (ADL) and days cut down on usual activities.Scores for the FSQ and EuroQOL instruments variedwith disease severity.
Getting ahead of headacheGerman researchers have developed a disease
management programme that improves the quality ofheadache treatment. However, the researchers say thatthe burden of headache and migraine could be furtherreduced with more collaborative efforts by physiciansand pharmacists.
341 employees from a company with a sicknessfund who suffered from headache responded to theShort Form-36, the Kiel Headache Questionnaire andadditional questions about medication and satisfactionwith therapy. The respondents, their physicians andpharmacists were given information on managementand prevention of headache. Respondents were thengiven a second follow-up questionnaire about theimpact of the programme.
126 of 183 traceable initial respondents answeredthe second questionnaire. 29.1 % of sufferers reportedan improvement in health status, 43.1 % reported lessheadaches, 38.9% reported shorter headache attacks,22.6% had improvement in identifying trigger factors,21 % used less medication and 41.9% learned arelaxation technique. Work time lost due to sicknesswas also reduced.
Cost of Alzheimer's substantial in UKThe cost of care of Alzheimer's disease is substantial
in the UK, and is directly related to severity of disease,indicate the results of a multicentre study retrospectivelyconducted in that country.
Direct medical costs, direct non-medical costs andindirect costs were calculated for 128 patients with mild(n = 38), moderate (42) and severe (48) Alzheimer'sdisease and 56 controls over 3 months' treatment(1993 pounds sterling).
Indirect costs were the main cost driver for patients(63-74% of a total cost of £30459) and were mainlydue to time spent by the caregiver with the patient.Direct costs represented 18-31 % of the total cost andwere mainly due to institutionalisation or hospitalisation.Direct non-medical costs accounted for 6-7% of thetotal cost.
All costs increased with disease severity, particularlycosts for hospitalisation and institutionalisation,
!Total indirect costs
NA 4923 6449 9304
PharmacoEconomics & Outcomes News 9 Jan 1998 No. 194 1173-5503199/0194-0006/$01.00°Adlslnternational Limited 1999. All rights reserved

INTERNATIONAL RESEARCH & OPINION7
disease progression, costs and quality-adjusted lifeyears (QALYs). Data were derived from the medicalliterature, clinical trials and a survey of resource useand health utility for 193 patients.
The incremental cost effectiveness of pramipexole,relative to baseline treatment, was estimated usingcost and QALY estimates from the model. Early andadvanced Parkinson's patients were analysedseparately and sensitivity analyses were performed.
In Sweden, pramipexole treatment had lowercosts and was more effective than baseline treatment.In Germany and Canada, pramipexole treatment hadhigher costs but was more effective than baselinetreatment.
CE ratios relatively lowCost-effectiveness ratios were lower than those
used for many commonly used medical therapies.TI:e incremental cost-effectiveness ratios for patientsWIth early-stage Parkinson's disease in Sweden,Germany and Canada were -SEK41 161, DM26 780and $Can28 097, respectively (1997 values). Ratiosfor patients with advanced-stage Parkinson's diseasewere -SEK27 386, DM49 168 and $Can25 090respectively. Pramipexole is also a favourable o~tionin Parkinson's disease in thc US.*
milSltl!:!
1173.5503199/0194-00071$01.00°Adlalnternatlonal Llmltecl1999. All rlghta reaerved
Cost and mortality of Parkinson's disease
Healthcare costs and mortality in Parkinson'sdisease are significant and emphasise the need forimproved treatment, say researchers in Scotland.
A controlled study was conducted using 2 populations in Tayside, Scotland; a 7-year cohort (19891995; n = 30 (00) and an ll-year cohort (1985-1995;10000). Incident cases were identified, and thosewho had taken antipsychotics were excluded, usingthe first 6 months of data. Each case was matchedto 9 controls.
The incidence of Parkinson's disease was 108 and33 in the 7- and II-year cohorts, respectively. Mediancosts of hospitalisation were significantly higher inParkinson's disease compared with controls (£14 119vs £5077, respectively). The relative risk of mortalityin patients with Parkinson's disease was similarbetween the 2 cohorts (2.5 after 7 years and 2.25 afterII years). This risk was significantly greater than thatfor controls.
The researchers said that the robustness of thecosting methods indicated that these results could begeneralised to the population of the United Kingdom.* see PharmacoEconomics & Outcomes News 189:8,21 Nov1998; 800683126
llii
PharmacoEconomics & Outcomes News 9 Jan 1998 No. 194