hepatic visceral larva migrans presenting as a pseudotumor
TRANSCRIPT
mbtwnam
Electronic Image of the Month
Hepatic Visceral Larva Migrans Presenting as a Pseudotumor
LOIC RAFFRAY,* BRIGITTE LE BAIL,‡ and DENIS MALVY*‡
*Travel Clinics and Tropical Diseases Unit, University Hospital Center of Bordeaux; and Pathology Department, Pellegrin University Hospital,Bordeaux, France
hcdlfni
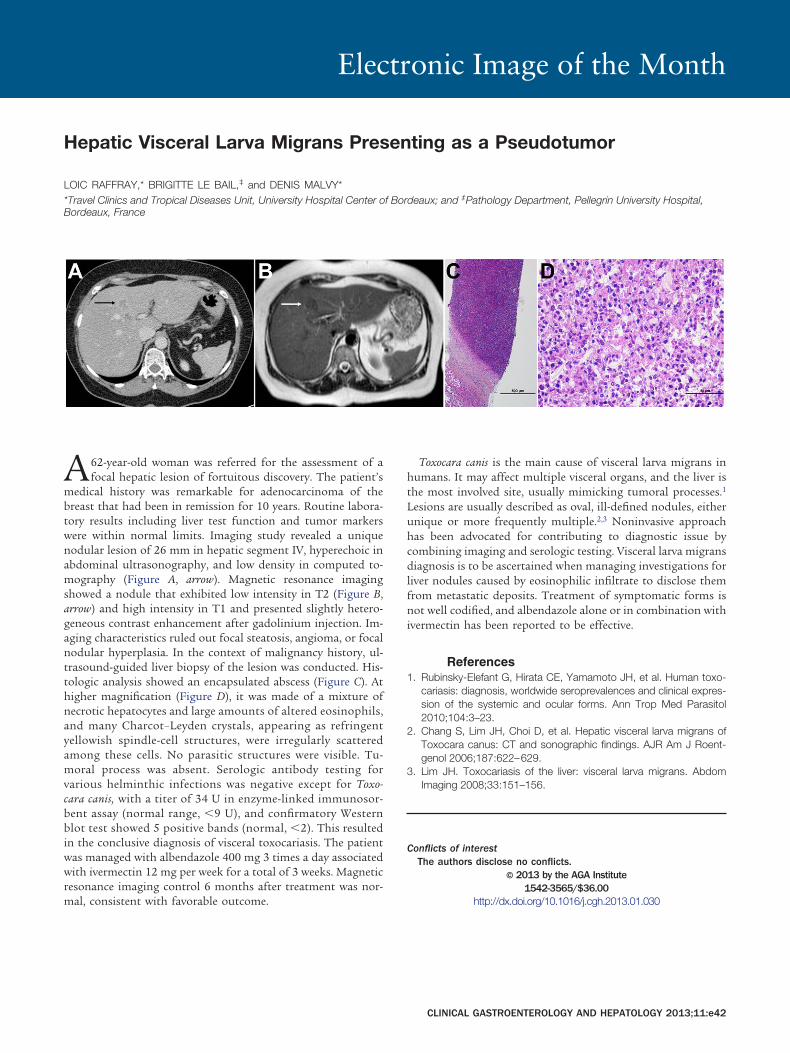
A62-year-old woman was referred for the assessment of afocal hepatic lesion of fortuitous discovery. The patient’s
edical history was remarkable for adenocarcinoma of thereast that had been in remission for 10 years. Routine labora-ory results including liver test function and tumor markersere within normal limits. Imaging study revealed a uniqueodular lesion of 26 mm in hepatic segment IV, hyperechoic inbdominal ultrasonography, and low density in computed to-ography (Figure A, arrow). Magnetic resonance imaging
showed a nodule that exhibited low intensity in T2 (Figure B,arrow) and high intensity in T1 and presented slightly hetero-geneous contrast enhancement after gadolinium injection. Im-aging characteristics ruled out focal steatosis, angioma, or focalnodular hyperplasia. In the context of malignancy history, ul-trasound-guided liver biopsy of the lesion was conducted. His-tologic analysis showed an encapsulated abscess (Figure C). Athigher magnification (Figure D), it was made of a mixture ofnecrotic hepatocytes and large amounts of altered eosinophils,and many Charcot–Leyden crystals, appearing as refringentyellowish spindle-cell structures, were irregularly scatteredamong these cells. No parasitic structures were visible. Tu-moral process was absent. Serologic antibody testing forvarious helminthic infections was negative except for Toxo-cara canis, with a titer of 34 U in enzyme-linked immunosor-bent assay (normal range, �9 U), and confirmatory Westernblot test showed 5 positive bands (normal, �2). This resultedin the conclusive diagnosis of visceral toxocariasis. The patientwas managed with albendazole 400 mg 3 times a day associatedwith ivermectin 12 mg per week for a total of 3 weeks. Magneticresonance imaging control 6 months after treatment was nor-
mal, consistent with favorable outcome.Toxocara canis is the main cause of visceral larva migrans inhumans. It may affect multiple visceral organs, and the liver isthe most involved site, usually mimicking tumoral processes.1
Lesions are usually described as oval, ill-defined nodules, eitherunique or more frequently multiple.2,3 Noninvasive approach
as been advocated for contributing to diagnostic issue byombining imaging and serologic testing. Visceral larva migransiagnosis is to be ascertained when managing investigations for
iver nodules caused by eosinophilic infiltrate to disclose themrom metastatic deposits. Treatment of symptomatic forms isot well codified, and albendazole alone or in combination with
vermectin has been reported to be effective.
References1. Rubinsky-Elefant G, Hirata CE, Yamamoto JH, et al. Human toxo-
cariasis: diagnosis, worldwide seroprevalences and clinical expres-sion of the systemic and ocular forms. Ann Trop Med Parasitol2010;104:3–23.
2. Chang S, Lim JH, Choi D, et al. Hepatic visceral larva migrans ofToxocara canus: CT and sonographic findings. AJR Am J Roent-genol 2006;187:622–629.
3. Lim JH. Toxocariasis of the liver: visceral larva migrans. AbdomImaging 2008;33:151–156.
Conflicts of interestThe authors disclose no conflicts.
© 2013 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2013.01.030
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:e42