goals the accessory navicular - podiatry management · by atrophied fin rays.10 the accessory...
TRANSCRIPT
SEPTEMBER 2013 | PODIATRY MANAGEMENT | 143www.podiatrym.com
The accessory navicular hasbeen reported to occur inup to 21% of the non-pa-tient adult population;however, its incidence in
clinical practice is markedly higher.Some have erroneously consideredthis entity as an anatomic androentgenographic variant; however,certain types are associated withpathologic conditions such as posteri-or tibial tendon dysfunction and tears,navicular enthesopathy, and painfulnavicular syndrome. Its identification,
clinical significance, bio—and patho-mechanics, as well as conservativeand surgical management, will hereinbe discussed and illustrated.
Incidence, Significance andSynonyms
The accessory navicular was firstdescribed by Bauhin in 1605.1,2 It is anautosomal dominant congenitalanomaly in which a tuberosity devel-ops from a secondary center of ossifi-cation.3,4 This frequently bilateral con-dition has been reported to occur in
4-21% of the population; however, itsincidence in a patient population maybe markedly and significantly higher.5-8 A recent radiographic study of 100consecutive adult patients revealedthe presence of an accessory navicu-lar in almost every instance.9
Synonyms for this condition in-clude: os tibiale externum, os navicu-laris, os naviculare secundarium,hooked navicular, gorilloid navicular,cornuate navicular, prehallux, and bi-furcate navicular. It is an atavistic
Continued on page 144
Continuing
Medical Education
Goalsand Objectives
1) To present an overview ofthe incidence, identification,and clinical significance of theaccessory navicular.
2) To discuss its attendantbio—and patho-mechanics.
3) To review its relationshipto flatfoot deformity.
4) To establish a rationale forits conservative as well as sur-gical management.
5) To enable the astute prac-titioner to resolve discomfort,improve dysfunction, and re-store quality of life for patients.
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $22.00 per topic) or 2) per year, for the special rate of $169 (you save $51).You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. You can also takethis and other exams on the Internet at www.podiatrym.com/cme.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earnedcredits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake thetest at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 152. Other than those en-tities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be ac-ceptable by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best ef-forts to ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of thisprogram is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts bynoted authors and researchers. If you have any questions or comments about this program, you can write or call us at:Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (pg. 152).—Editor
TheAccessoryNavicular
Identification, clinicalsignificance,
and management
BY JOSEPH C D’AMICO, DPM
TheAccessoryNavicular
Identification, clinicalsignificance,
and management
BY JOSEPH C D’AMICO, DPM
www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
144 | SEPTEMBER 2013 | PODIATRY MANAGEMENT
trait or reversion, ren-dering this hypermobile
foot type better suited toprehensile tasks than toambulation. Monahan con-sidered the accessory nav-icular a dormant center ofossification left in all feetby atrophied fin rays.10 Theaccessory navicular is anexample of Hoeckle’s lawof recapitulation in whichontogeny recapitulatesphylogeny.
The EctomorphConnection
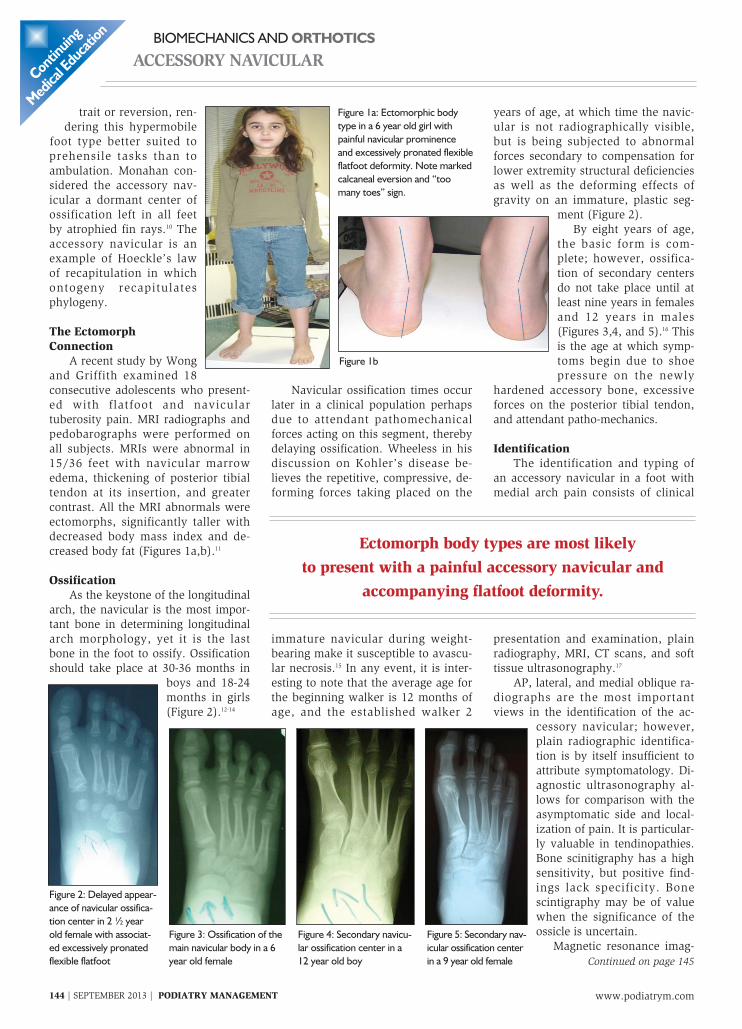
A recent study by Wongand Griffith examined 18consecutive adolescents who present-ed with flatfoot and naviculartuberosity pain. MRI radiographs andpedobarographs were performed onall subjects. MRIs were abnormal in15/36 feet with navicular marrowedema, thickening of posterior tibialtendon at its insertion, and greatercontrast. All the MRI abnormals wereectomorphs, significantly taller withdecreased body mass index and de-creased body fat (Figures 1a,b).11
OssificationAs the keystone of the longitudinal
arch, the navicular is the most impor-tant bone in determining longitudinalarch morphology, yet it is the lastbone in the foot to ossify. Ossificationshould take place at 30-36 months in
boys and 18-24months in girls(Figure 2).12-14
Navicular ossification times occurlater in a clinical population perhapsdue to attendant pathomechanicalforces acting on this segment, therebydelaying ossification. Wheeless in hisdiscussion on Kohler’s disease be-lieves the repetitive, compressive, de-forming forces taking placed on the
immature navicular during weight-bearing make it susceptible to avascu-lar necrosis.15 In any event, it is inter-esting to note that the average age forthe beginning walker is 12 months ofage, and the established walker 2
years of age, at which time the navic-ular is not radiographically visible,but is being subjected to abnormalforces secondary to compensation forlower extremity structural deficienciesas well as the deforming effects ofgravity on an immature, plastic seg-
ment (Figure 2).By eight years of age,
the basic form is com-plete; however, ossifica-tion of secondary centersdo not take place until atleast nine years in femalesand 12 years in males(Figures 3,4, and 5).16 Thisis the age at which symp-toms begin due to shoepressure on the newly
hardened accessory bone, excessiveforces on the posterior tibial tendon,and attendant patho-mechanics.
IdentificationThe identification and typing of
an accessory navicular in a foot withmedial arch pain consists of clinical
presentation and examination, plainradiography, MRI, CT scans, and softtissue ultrasonography.17
AP, lateral, and medial oblique ra-diographs are the most importantviews in the identification of the ac-
cessory navicular; however,plain radiographic identifica-tion is by itself insufficient toattribute symptomatology. Di-agnostic ultrasonography al-lows for comparison with theasymptomatic side and local-ization of pain. It is particular-ly valuable in tendinopathies.Bone scinitigraphy has a highsensitivity, but positive find-ings lack specificity. Bonescintigraphy may be of valuewhen the significance of theossicle is uncertain.
Magnetic resonance imag-Continued on page 145
Conti
nuing
Medica
l Edu
cation
Figure 1a: Ectomorphic bodytype in a 6 year old girl withpainful navicular prominenceand excessively pronated flexibleflatfoot deformity. Note markedcalcaneal eversion and “toomany toes” sign.
Figure 1b
Figure 2: Delayed appear-ance of navicular ossifica-tion center in 2 ½ yearold female with associat-ed excessively pronatedflexible flatfoot
Figure 3: Ossification of themain navicular body in a 6year old female
Figure 4: Secondary navicu-lar ossification center in a12 year old boy
Figure 5: Secondary nav-icular ossification centerin a 9 year old female
Ectomorph body types are most likelyto present with a painful accessory navicular and
accompanying flatfoot deformity.

SEPTEMBER 2013 | PODIATRY MANAGEMENT | 145www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
ing is of high diagnosticvalue for demonstratingbone marrow and tissueedema as well as abnor-malities in tendon inser-tion.18,19 MRI tendinopathyis characterized by a con-tour deformity with intra-substance signal intensityalterations. CT examina-tion easily reveals corticalirregularity in type II casesalong with fragmentationof the accessory navicular.Sclerosis involving bothsides of the synchondrosiscan also be observed. MRIdemonstrates bone mar-row edema within the ac-cessory bone and occa-sionally the adjacent nav-icular, suggesting pseu-doarthrosis.7 There may be high sig-nal intensity within the synchondrosisof T-2 weighted images.
TypesThree types of accessory navicular
have been described in the literature.Type I is a small, round separate ossi-cle, actually a sesamoid bone imbed-ded into the distal aspect of the poste-
rior tibial tendon. The dis-tance between the ossicleand the main navicularbody is usually less than 3mm.20 It has been reportedthat only 2% persist, withthe rest fusing to the navic-ular body. This type israrely associated withsymptomatology (Figure 6).
First described by Geist,type II is a larger (8-12mm), triangular ossifica-tion adjacent to the navicu-lar tuberosity and connect-ed by a sysostosis.5,6 Thistype has been called the os
tibiale externum. Fusion with thenavicular body takes place in 50% ofthe cases. It is subject to traction andshear forces from the altered mechan-ics of the posterior tibial tendon (Fig-ures 7,8).
Type III is an enlarged medialhorn of the navicular itself. It wasfirst described by Sella, et al. in 1986and is better referred to as a cornuate,
hooked, or gorilloid navicular(Figure 9).21 In a recent MRI andCT study of 148 patients, (11.5% typeI, 4.11% type II and 4.74% type III),multiple ossicle appearance wasnoted in 14.7% of the cases studied.7
The dilemma with identificationof these types is that they are not ra-diographically visible in younger chil-dren and do not become visible untilossification has been completed dur-ing early adolescence (Figures10,11,12). Clinically, there may ormay not be a palpable navicular pro-trusion, but many times, this mayalso be due to a severely adductedtalus in an excessively pronated foot.
SymptomsAs previously
mentioned, symptomsbegin in early adoles-cence as the sec-ondary navicular ossi-fication center solidi-fies. Clinically, pa-tients can presentwith an associatedflatfoot deformity withsignificant calcanealeversion and “toomany toes” sign.22
There is acute midfootpain, especially in un-
yielding footwear. Discomfort is notonly due to direct shoe pressure butalso from the medially displaced pos-terior tibial tendon insertion into theos navicularis instead of the mainbody of the navicular (Figures 13,14).There may be an associated enthe-sopathy as well.
Continued on page 146
Continuing
Medical Education
Figure 6: Type I accessory navic-ular with small ossicle within ten-don sheath
Figure 7: Type II accessorynavicular with syndesmoticattachment of the accessorybone to the native navicular
Figure 8: MRI revealing bilateral type II ac-cessory navicular with syndesmotic attach-ment and TPT enthesopathy
Figure 9: Type III cornuate, gorilloid, orhooked accessory navicular in which thesecondary ossification center has fused tothe native navicular.
Figure 10: 7 yr old female with normal navicularossification
Figure 11: Same patient at 10 ½ years of age.Note beginning ossification of secondary center
Figure 12: Again at age 13. Note full ossificationof secondary center revealing a type III accesso-ry navicular
www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
146 | SEPTEMBER 2013 | PODIATRY MANAGEMENT
Clinical examination may re-veal a localized point of maximum
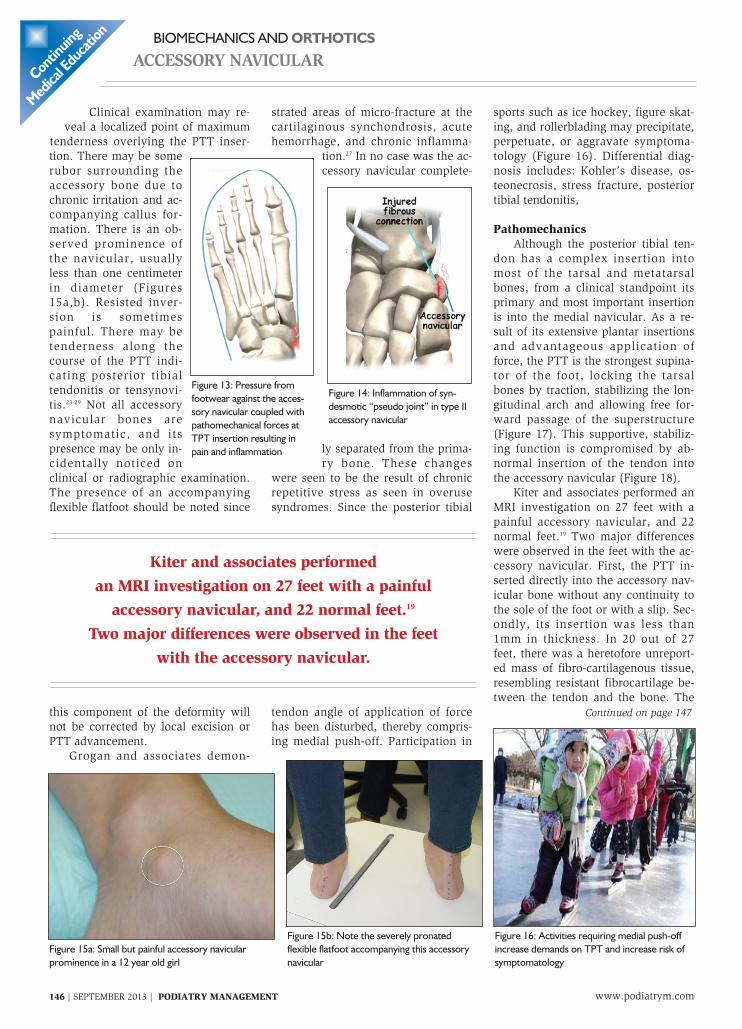
tenderness overlying the PTT inser-tion. There may be somerubor surrounding theaccessory bone due tochronic irritation and ac-companying callus for-mation. There is an ob-served prominence ofthe navicular, usuallyless than one centimeterin diameter (Figures15a,b). Resisted inver-sion is sometimespainful. There may betenderness along thecourse of the PTT indi-cating posterior tibialtendonitis or tensynovi-tis.23-29 Not all accessorynavicular bones aresymptomatic, and itspresence may be only in-cidentally noticed onclinical or radiographic examination.The presence of an accompanyingflexible flatfoot should be noted since
this component of the deformity willnot be corrected by local excision orPTT advancement.
Grogan and associates demon-
strated areas of micro-fracture at thecartilaginous synchondrosis, acutehemorrhage, and chronic inflamma-
tion.27 In no case was the ac-cessory navicular complete-
ly separated from the prima-ry bone. These changes
were seen to be the result of chronicrepetitive stress as seen in overusesyndromes. Since the posterior tibial
tendon angle of application of forcehas been disturbed, thereby compris-ing medial push-off. Participation in
sports such as ice hockey, figure skat-ing, and rollerblading may precipitate,perpetuate, or aggravate symptoma-tology (Figure 16). Differential diag-nosis includes: Kohler’s disease, os-teonecrosis, stress fracture, posteriortibial tendonitis,
PathomechanicsAlthough the posterior tibial ten-
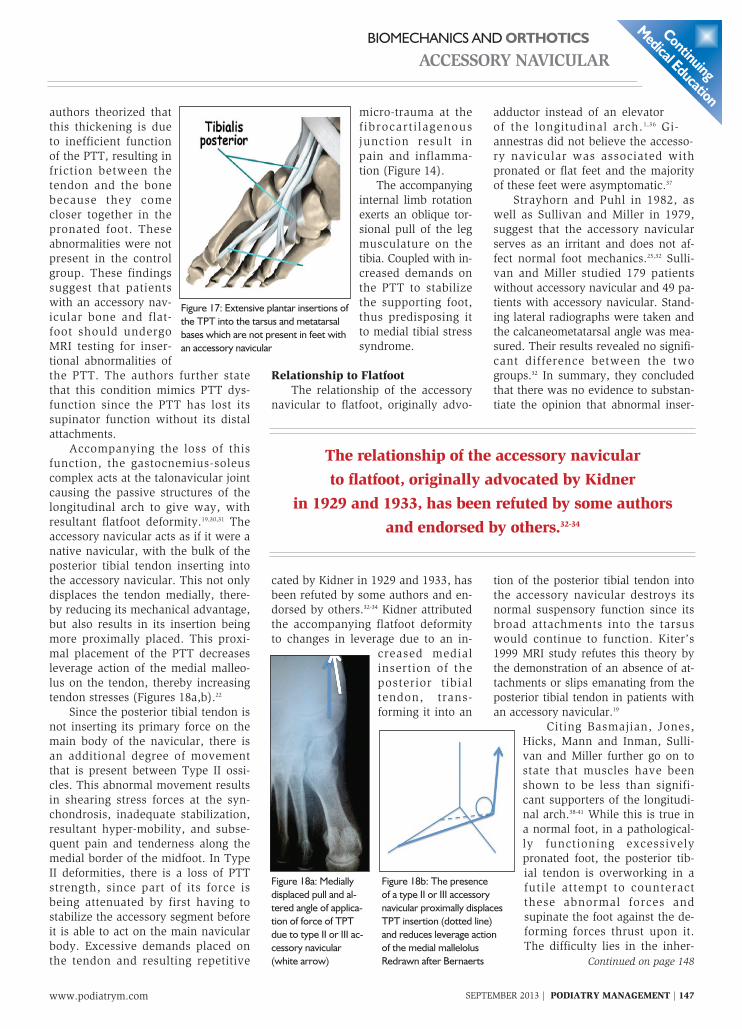
don has a complex insertion intomost of the tarsal and metatarsalbones, from a clinical standpoint itsprimary and most important insertionis into the medial navicular. As a re-sult of its extensive plantar insertionsand advantageous application offorce, the PTT is the strongest supina-tor of the foot, locking the tarsalbones by traction, stabilizing the lon-gitudinal arch and allowing free for-ward passage of the superstructure(Figure 17). This supportive, stabiliz-ing function is compromised by ab-normal insertion of the tendon intothe accessory navicular (Figure 18).
Kiter and associates performed anMRI investigation on 27 feet with apainful accessory navicular, and 22normal feet.19 Two major differenceswere observed in the feet with the ac-cessory navicular. First, the PTT in-serted directly into the accessory nav-icular bone without any continuity tothe sole of the foot or with a slip. Sec-ondly, its insertion was less than1mm in thickness. In 20 out of 27feet, there was a heretofore unreport-ed mass of fibro-cartilagenous tissue,resembling resistant fibrocartilage be-tween the tendon and the bone. The
Continued on page 147
Conti
nuing
Medica
l Edu
cation
Figure 13: Pressure fromfootwear against the acces-sory navicular coupled withpathomechanical forces atTPT insertion resulting inpain and inflammation
Figure 14: Inflammation of syn-desmotic “pseudo joint” in type IIaccessory navicular
Figure 15a: Small but painful accessory navicularprominence in a 12 year old girl
Figure 15b: Note the severely pronatedflexible flatfoot accompanying this accessorynavicular
Figure 16: Activities requiring medial push-offincrease demands on TPT and increase risk ofsymptomatology
Kiter and associates performedan MRI investigation on 27 feet with a painfulaccessory navicular, and 22 normal feet.19
Two major differences were observed in the feetwith the accessory navicular.
SEPTEMBER 2013 | PODIATRY MANAGEMENT | 147www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
authors theorized thatthis thickening is dueto inefficient functionof the PTT, resulting infriction between thetendon and the bonebecause they comecloser together in thepronated foot. Theseabnormalities were notpresent in the controlgroup. These findingssuggest that patientswith an accessory nav-icular bone and flat-foot should undergoMRI testing for inser-tional abnormalities ofthe PTT. The authors further statethat this condition mimics PTT dys-function since the PTT has lost itssupinator function without its distalattachments.
Accompanying the loss of thisfunction, the gastocnemius-soleuscomplex acts at the talonavicular jointcausing the passive structures of thelongitudinal arch to give way, withresultant flatfoot deformity.19,30,31 Theaccessory navicular acts as if it were anative navicular, with the bulk of theposterior tibial tendon inserting intothe accessory navicular. This not onlydisplaces the tendon medially, there-by reducing its mechanical advantage,but also results in its insertion beingmore proximally placed. This proxi-mal placement of the PTT decreasesleverage action of the medial malleo-lus on the tendon, thereby increasingtendon stresses (Figures 18a,b).22
Since the posterior tibial tendon isnot inserting its primary force on themain body of the navicular, there isan additional degree of movementthat is present between Type II ossi-cles. This abnormal movement resultsin shearing stress forces at the syn-chondrosis, inadequate stabilization,resultant hyper-mobility, and subse-quent pain and tenderness along themedial border of the midfoot. In TypeII deformities, there is a loss of PTTstrength, since part of its force isbeing attenuated by first having tostabilize the accessory segment beforeit is able to act on the main navicularbody. Excessive demands placed onthe tendon and resulting repetitive
micro-trauma at thefibrocarti lagenousjunction result inpain and inflamma-tion (Figure 14).
The accompanyinginternal limb rotationexerts an oblique tor-sional pull of the legmusculature on thetibia. Coupled with in-creased demands onthe PTT to stabilizethe supporting foot,thus predisposing itto medial tibial stresssyndrome.
Relationship to FlatfootThe relationship of the accessory
navicular to flatfoot, originally advo-
cated by Kidner in 1929 and 1933, hasbeen refuted by some authors and en-dorsed by others.32-34 Kidner attributedthe accompanying flatfoot deformityto changes in leverage due to an in-
creased medialinsertion of theposterior tibialtendon, trans-forming it into an
adductor instead of an elevatorof the longitudinal arch.1,36 Gi-annestras did not believe the accesso-ry navicular was associated withpronated or flat feet and the majorityof these feet were asymptomatic.37
Strayhorn and Puhl in 1982, aswell as Sullivan and Miller in 1979,suggest that the accessory navicularserves as an irritant and does not af-fect normal foot mechanics.25,32 Sulli-van and Miller studied 179 patientswithout accessory navicular and 49 pa-tients with accessory navicular. Stand-ing lateral radiographs were taken andthe calcaneometatarsal angle was mea-sured. Their results revealed no signifi-cant difference between the twogroups.32 In summary, they concludedthat there was no evidence to substan-tiate the opinion that abnormal inser-
tion of the posterior tibial tendon intothe accessory navicular destroys itsnormal suspensory function since itsbroad attachments into the tarsuswould continue to function. Kiter’s1999 MRI study refutes this theory bythe demonstration of an absence of at-tachments or slips emanating from theposterior tibial tendon in patients withan accessory navicular.19
Citing Basmajian, Jones,Hicks, Mann and Inman, Sulli-van and Miller further go on tostate that muscles have beenshown to be less than signifi-cant supporters of the longitudi-nal arch.38-41 While this is true ina normal foot, in a pathological-ly functioning excessivelypronated foot, the posterior tib-ial tendon is overworking in afutile attempt to counteractthese abnormal forces andsupinate the foot against the de-forming forces thrust upon it.The difficulty lies in the inher-
Continued on page 148
Continuing
Medical Education
Figure 17: Extensive plantar insertions ofthe TPT into the tarsus and metatarsalbases which are not present in feet withan accessory navicular
Figure 18a: Mediallydisplaced pull and al-tered angle of applica-tion of force of TPTdue to type II or III ac-cessory navicular(white arrow)
Figure 18b: The presenceof a type II or III accessorynavicular proximally displacesTPT insertion (dotted line)and reduces leverage actionof the medial mallelolusRedrawn after Bernaerts
The relationship of the accessory navicularto flatfoot, originally advocated by Kidner
in 1929 and 1933, has been refuted by some authorsand endorsed by others.32-34

www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
148 | SEPTEMBER 2013 | PODIATRY MANAGEMENT
ent inability of oneextrinsic muscle to be
able to achieve this taskwhile pitted against thedeforming effects of gravi-ty, which are dynamicallybeing imposed on it by anadvancing super-structure(Figure 19).
Prichasuk also differedwith Sullivan’s findingsnoting a distinct lowering ofcalcaneal pitch in 28 symp-tomatic accessory navicularpatients versus 200 non-af-fected individuals.33
Whether or not there isa one-to-one direct causalrelationship between thepresence of an accessorynavicular and the develop-ment of a pathologicallyfunctioning flexible flatfootcan be debated; however, there is nodoubt that the additional pathome-chanical demands placed on the footand ankle by its presence certainly donot benefit foot function.
Conservative ManagementConservative management of the
painful accessory navicular beginswith the identification of its specifictype, attendant pathology, and accom-panying patho-mechanics. Non-surgi-cal measures can provide relief andmay obviate the need for surgical in-tervention. Acute care would includeactivity modification or cessation,NSAIDs, local peritendinous, intersyn-chondrosis or insertional short to in-termediate acting corticosteroid injec-tions, ultrasound, strapping, immobi-lization, footwear modifications, andneutralization of structural deficien-cies via prescription foot orthoses. Theuse of night splints with the foot andankle held at 90 degrees is also helpfulespecially in those cases where dis-comfort is present upon arising.
The use of prescription foot or-thoses with appropriate modificationsis a mainstay in the conservative man-agement of the symptomatic accessorynavicular. Since the presence of an ac-cessory navicular by itself disrupts thenormal biomechanics of the foot andankle, it is of paramount importancethat existing structural deficiencies
and their secondary com-pensatory patho-mechan-ics be addressed as well.The goal of mechanicaltherapy is re-alignment ofthe osseous and soft tissuestructures, reduced PTTforces, and establishmentof optimum foot functionduring all weight-bearingactivities. Should this regi-men prove unsuccessful,then short-leg cast or bootimmobilization for up sixto eight weeks should beconsidered.25,42 Useful mod-ifications to enhance con-trol as well as allow adap-tation to the device in-clude: deepened heel seat,extended rearfoot post, re-duced undercut, medialand lateral flanges, navicu-
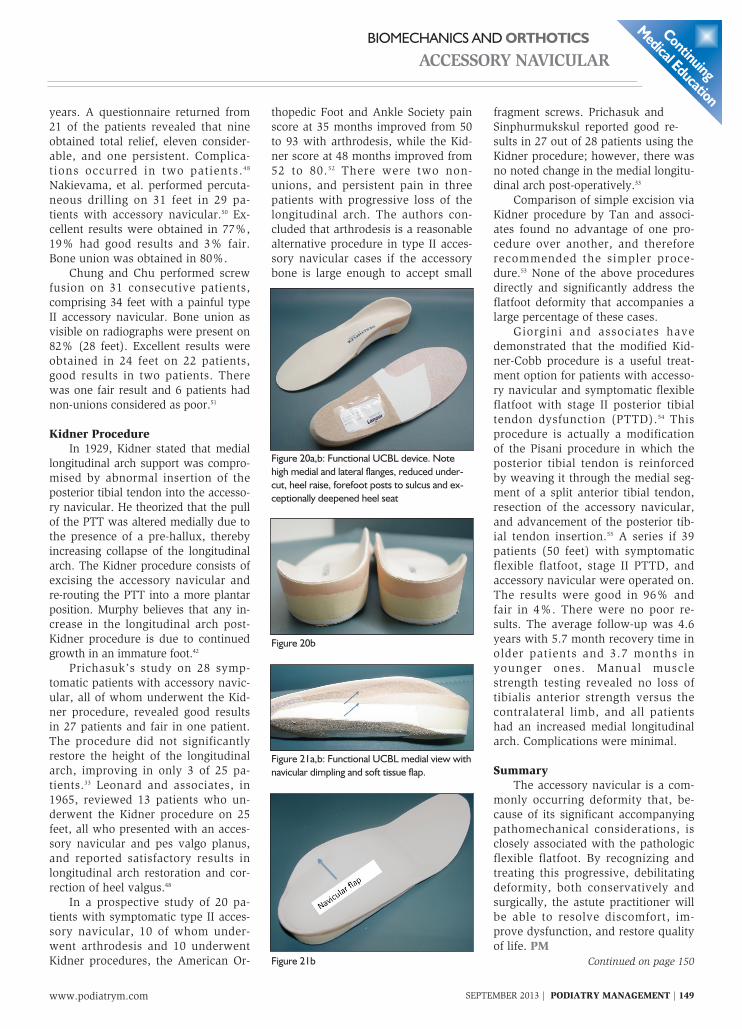
lar flap, navicular dimple, aggressiverearfoot posting, Kirby skive, andBlake inverted cast correction (Figures20a,b 21a,b).43,44
The shell or module for control ofpatho-mechanical foot function in pa-tients with an accessory navicularshould be non-compressible and non-
deformable. This does not mean thatthe device has to be completely inflexi-ble, but rather be sufficiently rigid tomaintain control during all weight-bearing activities, including sports par-ticipation. Materials that possess thesecharacteristics include: graphite com-posites, ortholene, subortholene, andhigh-density polyethylene (HDPE).Particularly useful, well-tolerated, andhighly controlling is a sub-ortholenedevice with high medial and lateralflanges, aggressive rearfoot posting,forefoot posting extended to the sul-cus, reduced undercut, heel raise andbutadiene rubber longitudinal arch re-inforcement (Figures 20 a,b)
Except for its increased length dueto the extended forefoot posts, the re-
sulting orthotic outwardly resemblesthe UCBL; however, functionallythere is a crucial difference. The origi-nal UCBL functions by blocking allsubtalar joint motion, whereas thefunctional UCBL acts as a true Root-type functional orthoses by optimallyrealigning the osseous and soft tissuesegments of the foot and ankle duringeach segment of the gait cycle, there-by promoting normal function. I referto this device as a functional UCBL(Figures 20a,b).45
Should conservative therapy fail toprovide definitive relief within a fourto six month period of time then surgi-cal intervention should be considered.
Surgical Decision-MakingA variety of surgical procedures for
treatment of the painful accessory nav-icular yield good results. Not only dothese procedures address subjectiveconcerns, but each one of them to agreater or lesser extent improves pos-terior tibial tendon function by at theleast reducing slip, slide, and play atits insertion, thereby improving its me-chanical advantage. These proceduresinclude: ossicle excision, percutaneousdrilling, Kidner procedure and its mod-
ifications, and arthrodesis of the ossi-cle to the main navicular body.
Grogan and associates reportedcomplete relief in 16 out of 17 feettreated by simple excision, while Ben-nett reported good results in 45 (70feet) of 50 patients (90%) operatedon.27,46 Simple excision of small ossi-cles and segmental fusion after re-moval of the synchondrosis for largeossicles yield good results.47,49 A studyof 22 adolescent patients comprising34 feet with a diagnosis of symp-tomatic accessory navicular was per-formed. Five individuals had type I,17 type II and 11 type III deformities.All subjects underwent simple exci-sion. The mean follow-up was 5.6
Continued on page 149
Conti
nuing
Medica
l Edu
cation
Figure 19: The inability ofone extrinsic muscle to stabi-lize the longitudinal arch andsupinate the foot as bodyweight is being dynamicallyimposed on it
A variety of surgical proceduresfor treatment of the painful accessory navicular
yield good results.
SEPTEMBER 2013 | PODIATRY MANAGEMENT | 149www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
years. A questionnaire returned from21 of the patients revealed that nineobtained total relief, eleven consider-able, and one persistent. Complica-tions occurred in two patients.48
Nakievama, et al. performed percuta-neous drilling on 31 feet in 29 pa-tients with accessory navicular.50 Ex-cellent results were obtained in 77%,19% had good results and 3% fair.Bone union was obtained in 80%.
Chung and Chu performed screwfusion on 31 consecutive patients,comprising 34 feet with a painful typeII accessory navicular. Bone union asvisible on radiographs were present on82% (28 feet). Excellent results wereobtained in 24 feet on 22 patients,good results in two patients. Therewas one fair result and 6 patients hadnon-unions considered as poor.51
Kidner ProcedureIn 1929, Kidner stated that medial
longitudinal arch support was compro-mised by abnormal insertion of theposterior tibial tendon into the accesso-ry navicular. He theorized that the pullof the PTT was altered medially due tothe presence of a pre-hallux, therebyincreasing collapse of the longitudinalarch. The Kidner procedure consists ofexcising the accessory navicular andre-routing the PTT into a more plantarposition. Murphy believes that any in-crease in the longitudinal arch post-Kidner procedure is due to continuedgrowth in an immature foot.42
Prichasuk’s study on 28 symp-tomatic patients with accessory navic-ular, all of whom underwent the Kid-ner procedure, revealed good resultsin 27 patients and fair in one patient.The procedure did not significantlyrestore the height of the longitudinalarch, improving in only 3 of 25 pa-tients.33 Leonard and associates, in1965, reviewed 13 patients who un-derwent the Kidner procedure on 25feet, all who presented with an acces-sory navicular and pes valgo planus,and reported satisfactory results inlongitudinal arch restoration and cor-rection of heel valgus.48
In a prospective study of 20 pa-tients with symptomatic type II acces-sory navicular, 10 of whom under-went arthrodesis and 10 underwentKidner procedures, the American Or-
thopedic Foot and Ankle Society painscore at 35 months improved from 50to 93 with arthrodesis, while the Kid-ner score at 48 months improved from52 to 80.52 There were two non-unions, and persistent pain in threepatients with progressive loss of thelongitudinal arch. The authors con-cluded that arthrodesis is a reasonablealternative procedure in type II acces-sory navicular cases if the accessorybone is large enough to accept small
fragment screws. Prichasuk andSinphurmukskul reported good re-sults in 27 out of 28 patients using theKidner procedure; however, there wasno noted change in the medial longitu-dinal arch post-operatively.33
Comparison of simple excision viaKidner procedure by Tan and associ-ates found no advantage of one pro-cedure over another, and thereforerecommended the simpler proce-dure.53 None of the above proceduresdirectly and significantly address theflatfoot deformity that accompanies alarge percentage of these cases.
Giorgini and associates havedemonstrated that the modified Kid-ner-Cobb procedure is a useful treat-ment option for patients with accesso-ry navicular and symptomatic flexibleflatfoot with stage II posterior tibialtendon dysfunction (PTTD).54 Thisprocedure is actually a modificationof the Pisani procedure in which theposterior tibial tendon is reinforcedby weaving it through the medial seg-ment of a split anterior tibial tendon,resection of the accessory navicular,and advancement of the posterior tib-ial tendon insertion.55 A series if 39patients (50 feet) with symptomaticflexible flatfoot, stage II PTTD, andaccessory navicular were operated on.The results were good in 96% andfair in 4%. There were no poor re-sults. The average follow-up was 4.6years with 5.7 month recovery time inolder patients and 3.7 months inyounger ones. Manual musclestrength testing revealed no loss oftibialis anterior strength versus thecontralateral limb, and all patientshad an increased medial longitudinalarch. Complications were minimal.
SummaryThe accessory navicular is a com-
monly occurring deformity that, be-cause of its significant accompanyingpathomechanical considerations, isclosely associated with the pathologicflexible flatfoot. By recognizing andtreating this progressive, debilitatingdeformity, both conservatively andsurgically, the astute practitioner willbe able to resolve discomfort, im-prove dysfunction, and restore qualityof life. PM
Continued on page 150
Continuing
Medical Education
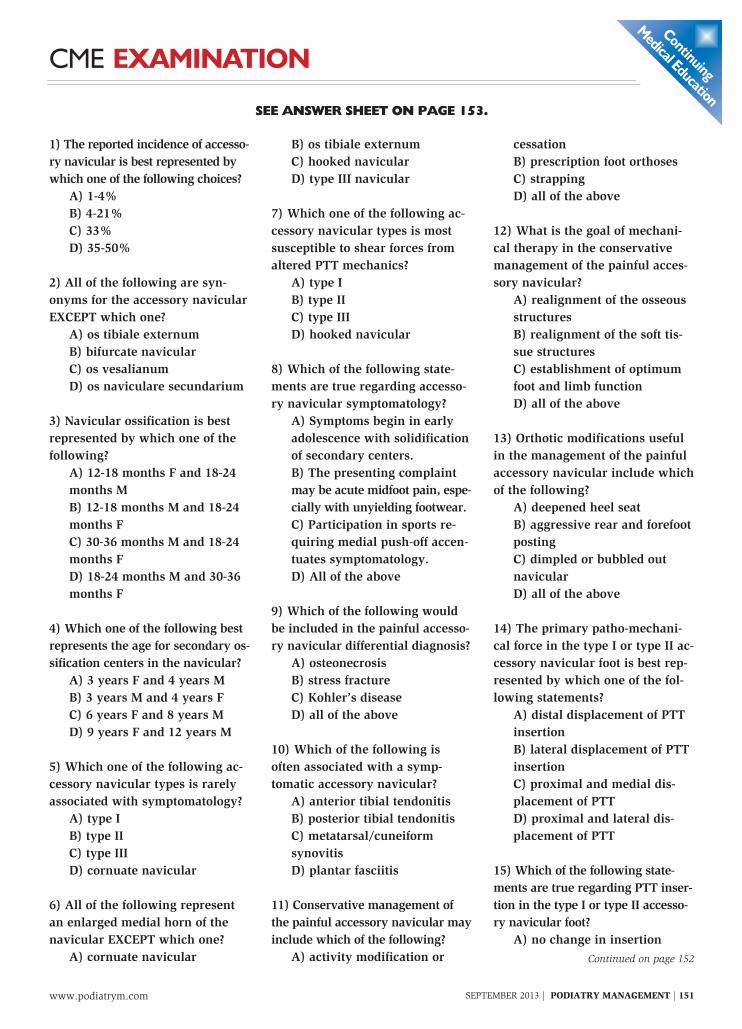
Figure 20a,b: Functional UCBL device. Notehigh medial and lateral flanges, reduced under-cut, heel raise, forefoot posts to sulcus and ex-ceptionally deepened heel seat
Figure 20b
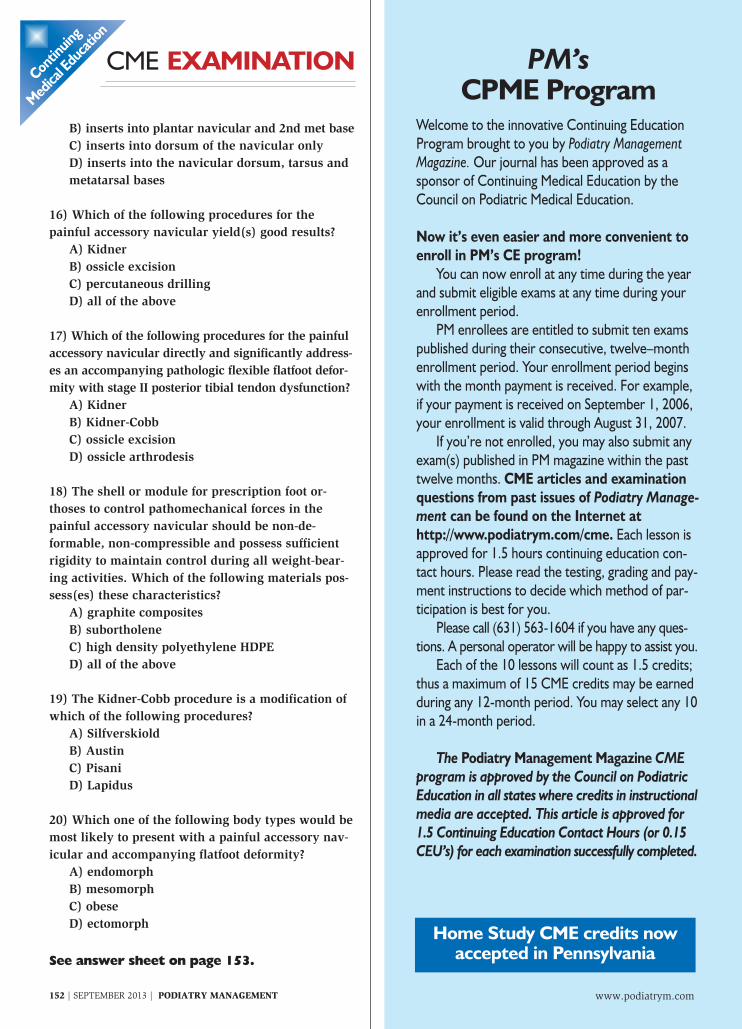
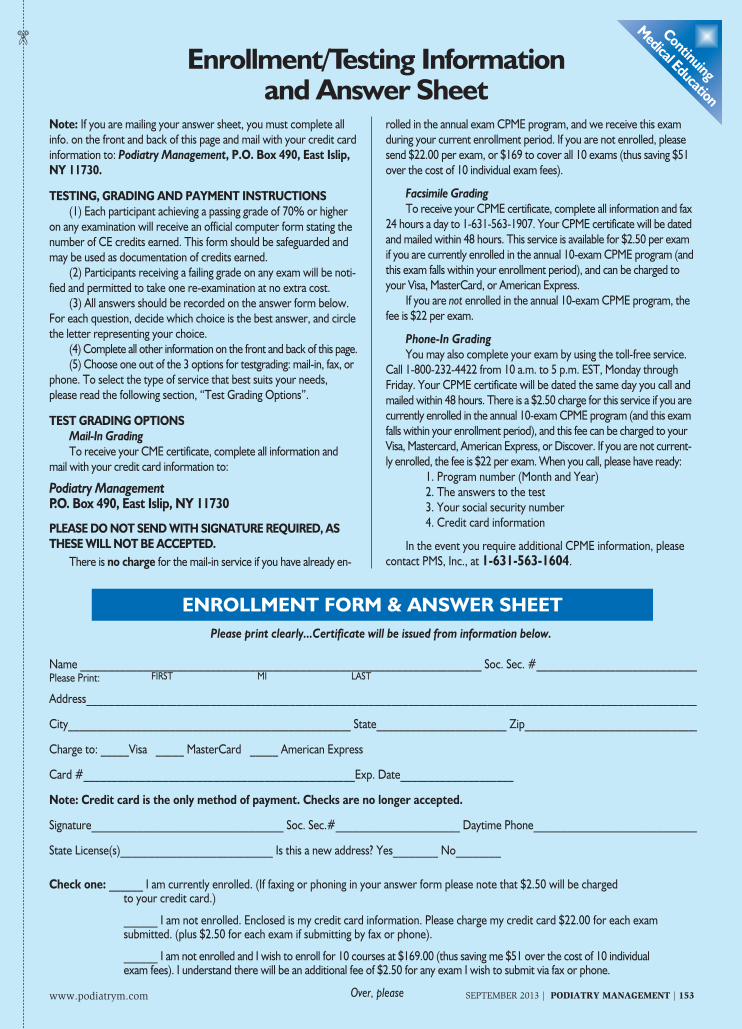
Figure 21a,b: Functional UCBL medial view withnavicular dimpling and soft tissue flap.
Figure 21b

www.podiatrym.com
BIOMECHANICS AND ORTHOTICS
ACCESSORY NAVICULAR
150 | SEPTEMBER 2013 | PODIATRY MANAGEMENT
References1 Kidner FC. The pre-hallux (accessory
scaphoid) in its relation to flat-foot. J Bone JointSurg 1929:11:831.
2 Zadek I, Gold AM The accessory tarsalscaphoid. J Bone Joint Surg 1948;30-A:1948.
3 Dobbs MB, Walton T. Autosomal domi-nant transmission of accessory navicular. IowaOrthop J. 2004;24:84-5.
4 McKusic VA. Mendelian inheritance inman. 2nd ed Balitimore, MD: The Johns Hop-kins University Press 1968.
5 Geist ES. Supernumerary bone of the foot-a roentgen study of the feet in one hundred nor-mal individuals. Am J Orthop Surg 1914:12;403-414.
6 Geist ES. The accessory scaphoid bone. JBone Joint Surg 1925:7;570.
7 Perdikakis E, Grigoraki E, Karantanas A.Os naviculare: the multiple-ossicle configurationof a normal variant. Skeletal Radiol. 2011Jan;40(1)85-8.
8 Keles Coskun N, Arican RY et al. The inci-dence of accessory navicular bones in Turkishsubjects. Surg Radio Anat. Nov;31(9):675-9.
9 D’Amico JC. Incidence and significance ofaccessory navicular in an adult patient popula-tion. Unpublishedmanuscript 2013.
10 Monahan JJ. Human pre-hallux. Am JMed Sci 1920 160:708.
11 Wong MW, Griffith JW. MRI in adoles-cent painful flatfoot. Foot and Ankle IntApr;30(4):303-8.
12 Waugh W. The ossification and vascular-ization of the tarsal navicular and their relationto Kohler’s disease. J Bone Joint Surg 1958;40-B:765.
13 Karp M. Kohler’s disease of the tarsalscaphoid. J Bone Joint Surg 1937;19-84.
14 Morrissy RT, Weinstein SL. Lovell andWinter’s pediatric orthopedics Philadelphia, PALippincottWilliams andWilkins 2006; 2:1318.
15 Wheeless CR. Wheeless textbook of or-thopedics. Duke Health Data Trace Internet2011.
16 Baker BJ, Dupras L, Tocheri W. Bones ofthe hand and feet. in The osteology of infantsand children 9:142 Texas AMUniv Press 2005.
17 Chuang YW, Tsai WS, Chen KH, HsuHC. Clinical use of high-resolution ultrasonogra-phy for the diagnosis of posterior tibial ten-donitis in a type II accessory navicular bone.Am J PhysMed Rehabil. 2012 Feb;91(2):177-81.
18 Mosel LD, Kat E, Voyvodic F. Imaging ofthe symptomatic accessory navicular bone. Aus-tralas Radiol. 2004 Jun;48(2):267-71.
19 Kiter E, Erdag N, Karatosun Y. Tibialisposterior tendon abnormalities in feet with ac-cessory navicular bone and flatfoot. Acta OrthopScand. 1999 Dec;70(6):618-21.
20 Bareither DJ, Muehleman CH, FeldmanNJ. Os tibial externum of sesamoid in the ten-don of the tibialis posterior. J Foot Ankle Surg1995;34:429.
21 Sella EJ, Lawson JP. The accessory navic-
ular synchondritis. Clin Orthop., 209:280-285,1986.
22 Bernaerts A, Vanhoenacker S, Van dePerre AM. Accessory navicular bone:not such anormal variant. JBR-BTR.2004 Sep-Oct;87(5):250-2.
23 Burman MS, Lapidus PW. The functionaldisturbances caused by the inconstant bonesand sesamoids of the foot. Arch Surg1931;22:936-751931;22:936-75.
24 Myergind HB. The accessory tarsalscaphoid. Clinical features and treatment. ActaOrthop Scand 1953;23:142-51.
25 Strayhorn G, Puhl J. The symptomatic ac-cessory navicular bone. J Fam Pract 1982;15:59-64.
26 Lawson JP, Ogden JA et al. The painfulaccessory navicular. Skeletal Radiol1984;12:250-62.
27 Grogan DP, Gasser SI, Ogden JA. Thepainful accessory navicular:a clinical andhistopathological study. Foot Ankle1989;10:164-69.
28 Chen YJ, Hsu RW et al. Degeneration ofthe accessory navicular synchondrosis present-ing as rupture of the posterior tibial tendon. JBone Joint Surg (Am)1997;79:1791-8.
29 Dyal CM, Feder J, Deland JT, andThompson FM. Pes planus in patients with pos-terior tibial tendon insufficiency:Asymptomaticversus symptomatic foot. Foot Ankle1997;18:85-8.
30 Funk DA, Cass JR, Johnson KA. Ac-quired adult flatfoot secondary to posterior tib-ial-tendon pathology. J Bone Joint Surg (Am)1986;68:95-102.
31 Navarez J, Navarez JA et al. Posterior tib-ial tendon dysfunction as a cause of acquiredflatfoot in the adult:value of magnetic resonanceimaging. Br J Rheumatol 1997;36:136-9.
32 Sullivan JA, Miller WA.The relationshipof the accessory navicular to the development ofthe flat foot. Clin Orthop 1979;144:233.
33 Prichasuk S, Sinphurmsukskul B. Kidnerprocedure for symptomatic accessory navicularand its relation to pes planus. Foot Ankle1995;16(8):500-03.
35 Chater EH. Foot pain and the accessorynavicular bone. Irish JMed Sci 1962;442:471-75.
36 Kidner FC. Pre-hallux in relation to flat-foot. JAMA 1933;101:1539-42.
37 Giannestras NJ. Foot disorders: medicaland surgical management, 2nd edition, Philadel-phia, 1973,Lea & Febiger.
38 Basmajian JV, Stecko G. The role of mus-cles in arch support of the foot: an electromyo-graphic study. J Bone Joint Surg 1963;45A:1184.
39 Hicks JH. The mechanics of the foot II.The plantar aponeurosis and the arch. J Anat.88:25, 1954.
40 Jones RL. The human foot. An experi-mental study of its mechanics and the role of itsmuscles and ligaments in the support of thearch. Am J Anat 68:1, 1941.
41 Mann R, Inman VT. Phasic activity of the
intrinsic muscles of the foot. J Bone Joint Surg46A:469,1964.
42 Canale ST, Beaty JH.Pes planus in Camp-bell’s operative orthopedics. 79; 4601 2007Mosby.
43 Blake R. Inverted functional orthosis. JAm Podiatr Med Assoc. 1986;76(50):275-276.
44 Kirby KA. The medial heel skive tech-nique. J am Podiatr Med Assoc 1992;84(4):177-188.
45 Mereday C, Dolan CM, Lusskin R. Evalu-ation of the University of California Biomechan-ics Laboratory shoe insert in “flexible” pesplanus. Clin Orthop 1972;82:45-48.
46 Bennett GL, Weiner DS, Leighey B. Surgi-cal treatment of symptomatic accessory tarsalnavicular. J Pediatr Orthop 1978;131:210-13.
47 Leonard ZC, Fortin PT. Adolescent acces-sory navicular. Foot Ankle Clin 15(2):337-47(2010).
48 Leonard MH, Gonzales, S. Lateral trans-fer of the posterior tibial tendon in certain select-ed cases of pes plano-valgus(kidner operation).Clin Orhop 40:139,1965.
49 Jasiewicz B, Pataczek KT. Results of sim-ple excision technique in surgical treatment ofaccessory navicular. Foot Ankle Surg2008;14(2):57-61.
50 Nakieyama S, Suginoto K, Takakura Y.Surgical drilling of the symptomatic accessorynavicular in young athletes. Am J Sports Med.2005 Apr;334):531-5.
51 Chung JW, Chu IT. Outcome of fusion ofa painful accessory navicular to the primarynavicular. Foot Ankle Int. 2009 Feb;30(2):106-9.
52 Scott AT, Sabesan VJ, Saluta JR. Fusionvs excision of the symptomatic type II accessorynavicular: a prospective study. Foot Ankle Int.2009 Jan;30(1):10-5.
53 Tan SM, Chin TW, Mitra AK. Surgicaltreatment of symptomatic accessory navicular.Ann AcadMed Singapore 1995;24:379.
54 Giorgini RJ, Giorgini T, Calderaro M. Themodified Kidner-Cobb procedure for symp-tomatic flexible pes valgoplanus and posteriortibial tendon dysfunction stage II: review of 50feet in 39 patients.Jrn Foot Ankle Surg49(2010)411-16.
55 Pisani G Peritalar destabilization syn-drome (adult flatfoot with degenerativemyelopathy). Foot Ankle Surg. 2010Dec;16(4):183-8.
Dr. D’Amico is Profes-sor and past chairman ofthe Division of Orthope-dic Sciences at NYCPM,and a Diplomate ofAmerican Board of Po-diatric Orthopedics anda Distinguished Practi-tioner in the NationalAcademies of Practice.
He is a nationally recognized author and lecturer.
Conti
nuing
Medica
l Edu
cation
CME EXAMINATION
1) The reported incidence of accesso-ry navicular is best represented bywhich one of the following choices?
A) 1-4%B) 4-21%C) 33%D) 35-50%
2) All of the following are syn-onyms for the accessory navicularEXCEPT which one?
A) os tibiale externumB) bifurcate navicularC) os vesalianumD) os naviculare secundarium
3) Navicular ossification is bestrepresented by which one of thefollowing?
A) 12-18 months F and 18-24months MB) 12-18 months M and 18-24months FC) 30-36 months M and 18-24months FD) 18-24 months M and 30-36months F
4) Which one of the following bestrepresents the age for secondary os-sification centers in the navicular?
A) 3 years F and 4 years MB) 3 years M and 4 years FC) 6 years F and 8 years MD) 9 years F and 12 years M
5) Which one of the following ac-cessory navicular types is rarelyassociated with symptomatology?
A) type IB) type IIC) type IIID) cornuate navicular
6) All of the following representan enlarged medial horn of thenavicular EXCEPT which one?
A) cornuate navicular
B) os tibiale externumC) hooked navicularD) type III navicular
7) Which one of the following ac-cessory navicular types is mostsusceptible to shear forces fromaltered PTT mechanics?
A) type IB) type IIC) type IIID) hooked navicular
8) Which of the following state-ments are true regarding accesso-ry navicular symptomatology?
A) Symptoms begin in earlyadolescence with solidificationof secondary centers.B) The presenting complaintmay be acute midfoot pain, espe-cially with unyielding footwear.C) Participation in sports re-quiring medial push-off accen-tuates symptomatology.D) All of the above
9) Which of the following wouldbe included in the painful accesso-ry navicular differential diagnosis?
A) osteonecrosisB) stress fractureC) Kohler’s diseaseD) all of the above
10) Which of the following isoften associated with a symp-tomatic accessory navicular?
A) anterior tibial tendonitisB) posterior tibial tendonitisC) metatarsal/cuneiformsynovitisD) plantar fasciitis
11) Conservative management ofthe painful accessory navicular mayinclude which of the following?
A) activity modification or
cessationB) prescription foot orthosesC) strappingD) all of the above
12) What is the goal of mechani-cal therapy in the conservativemanagement of the painful acces-sory navicular?
A) realignment of the osseousstructuresB) realignment of the soft tis-sue structuresC) establishment of optimumfoot and limb functionD) all of the above
13) Orthotic modifications usefulin the management of the painfulaccessory navicular include whichof the following?
A) deepened heel seatB) aggressive rear and forefootpostingC) dimpled or bubbled outnavicularD) all of the above
14) The primary patho-mechani-cal force in the type I or type II ac-cessory navicular foot is best rep-resented by which one of the fol-lowing statements?
A) distal displacement of PTTinsertionB) lateral displacement of PTTinsertionC) proximal and medial dis-placement of PTTD) proximal and lateral dis-placement of PTT
15) Which of the following state-ments are true regarding PTT inser-tion in the type I or type II accesso-ry navicular foot?
A) no change in insertionContinued on page 152
SEE ANSWER SHEET ON PAGE 153.
SEPTEMBER 2013 | PODIATRY MANAGEMENT | 151www.podiatrym.com
Continuing
Medical Education
Continued on page <None>
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenient toenroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Manage-ment can be found on the Internet athttp://www.podiatrym.com/cme. Each lesson isapproved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of par-ticipation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may be earnedduring any 12-month period. You may select any 10in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instructionalmedia are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
Home Study CME credits nowaccepted in Pennsylvania
Conti
nuing
Medica
l Edu
cation
CME EXAMINATION
www.podiatrym.com152 | SEPTEMBER 2013 | PODIATRY MANAGEMENT
B) inserts into plantar navicular and 2nd met baseC) inserts into dorsum of the navicular onlyD) inserts into the navicular dorsum, tarsus andmetatarsal bases
16) Which of the following procedures for thepainful accessory navicular yield(s) good results?
A) KidnerB) ossicle excisionC) percutaneous drillingD) all of the above
17) Which of the following procedures for the painfulaccessory navicular directly and significantly address-es an accompanying pathologic flexible flatfoot defor-mity with stage II posterior tibial tendon dysfunction?
A) KidnerB) Kidner-CobbC) ossicle excisionD) ossicle arthrodesis
18) The shell or module for prescription foot or-thoses to control pathomechanical forces in thepainful accessory navicular should be non-de-formable, non-compressible and possess sufficientrigidity to maintain control during all weight-bear-ing activities. Which of the following materials pos-sess(es) these characteristics?
A) graphite compositesB) subortholeneC) high density polyethylene HDPED) all of the above
19) The Kidner-Cobb procedure is a modification ofwhich of the following procedures?
A) SilfverskioldB) AustinC) PisaniD) Lapidus
20) Which one of the following body types would bemost likely to present with a painful accessory nav-icular and accompanying flatfoot deformity?
A) endomorphB) mesomorphC) obeseD) ectomorph
See answer sheet on page 153.
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________ Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________ State_______________________ Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________ Soc. Sec.#______________________ Daytime Phone_____________________________
State License(s)___________________________ Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be chargedto your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $22.00 for each examsubmitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $169.00 (thus saving me $51 over the cost of 10 individualexam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must complete allinfo. on the front and back of this page and mail with your credit cardinformation to: Podiatry Management, P.O. Box 490, East Islip,NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or higher
on any examination will receive an official computer form stating thenumber of CE credits earned. This form should be safeguarded andmay be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will be noti-fied and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer form below.For each question, decide which choice is the best answer, and circlethe letter representing your choice.
(4) Complete all other information on the front and back of this page.(5) Choose one out of the 3 options for testgrading: mail-in, fax, or
phone. To select the type of service that best suits your needs,please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information and
mail with your credit card information to:
Podiatry ManagementP.O. Box 490, East Islip, NY 11730
PLEASE DO NOT SEND WITH SIGNATURE REQUIRED, ASTHESE WILL NOT BE ACCEPTED.
There is no charge for the mail-in service if you have already en-
ENROLLMENT FORM & ANSWER SHEET
� Continuing
Medical Education
rolled in the annual exam CPME program, and we receive this examduring your current enrollment period. If you are not enrolled, pleasesend $22.00 per exam, or $169 to cover all 10 exams (thus saving $51over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and fax
24 hours a day to 1-631-563-1907. Your CPME certificate will be datedand mailed within 48 hours. This service is available for $2.50 per examif you are currently enrolled in the annual 10-exam CPME program (andthis exam falls within your enrollment period), and can be charged toyour Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME program, thefee is $22 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free service.
Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Monday throughFriday. Your CPME certificate will be dated the same day you call andmailed within 48 hours. There is a $2.50 charge for this service if you arecurrently enrolled in the annual 10-exam CPME program (and this examfalls within your enrollment period), and this fee can be charged to yourVisa, Mastercard, American Express, or Discover. If you are not current-ly enrolled, the fee is $22 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information, pleasecontact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
Over, please SEPTEMBER 2013 | PODIATRY MANAGEMENT | 153www.podiatrym.com
�
ENROLLMENT FORM & ANSWER SHEET (continued)Co
ntinu
ing
Medica
l Edu
cation
Medical Education Lesson Evaluation
Strongly Stronglyagree Agree Neutral Disagree disagree
[5] [4] [3] [2] [1]
1) This CME lesson was helpful to my practice ____
2) The educational objectives were accomplished ____
3) I will apply the knowledge I learned from this lesson ____
4) I will makes changes in my practice behavior based on thislesson ____
5) This lesson presented quality information with adequatecurrent references ____
How long did it take you to complete this lesson?
______hour ______minutes
What topics would you like to see in future CME lessons ?
Please list :
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
EXAM #6/13The Accessory Navicular
(D’Amico)
www.podiatrym.com154 | SEPTEMBER 2013 | PODIATRY MANAGEMENT