surgical treatment of the symptomatic accessory navicular€¦ · navicular (figs 6,7and...
TRANSCRIPT

© 1984 British Editorial Society ofBone and Joint Surgery0301 -620X/84/2027 $2.00
218 THE JOURNAL OF BONE AND JOINT SURGERY
SURGICAL TREATMENT OF THE SYMPTOMATIC ACCESSORY
NAVICULAR
M. F. MACNICOL, S. VOUTSINAS
From Princess Margaret Rose Orthopaedic Hospital, Edinburgh
The accessory navicular is occasionally the source of pain and local tenderness over the instep. If
conservative measures fail, surgical treatment may be required and the results of 62 operations to one or bothfeet in 47 patients are reported. Twenty-six patients were treated by the Kidner operation, in which the main
insertion of the tibialis posterior is re-routed; in the remaining 21 the ossicle was merely excised. Excisionwas as effective as the Kidner technique, provided that the medial surface of the main navicular bone was
contoured to prevent any residual prominence. Both procedures were successful in relieving symptoms in the
majority of cases and failures resulted from errors in the selection of patients or in the surgical technique.Correction of any associated fiat foot was secondary to growth and maturation of the foot rather than to theoperation; hence the Kidner procedure does not confer any particular advantages over simple excision.
Pain and tenderness in relation to the medial arch of the
foot may be produced by an accessory navicular bone
(synonyms : os tibiale externum ; navicular secundum;
prehallux) which was first clearly described by Bauhin in
1605 (Froelich 1909). Whether this minor anomaly alters
the suspensory mechanism of the medial arch of the foot
has been a subject of some controversy, for although it is
often associated with pes planus, it may also present in
feet that are relatively normal apart from the character-
istic medial prominence (Giannestras 1973; Sullivan and
Miller 1979).Froelich (1909) considered that the accessory navi-
cular produced a flattened medial arch but recommended
no more than simple excision of the ossicle when it wassymptomatic. Subsequently, Kidner (1929, 1933) sug-
gested that the bony anomaly resulted in medial displace-
ment of the tendon of tibialis posterior, thus
compromising its action as an elevator of the tarsus. He
considered that adduction of the foot became pro-
nounced, and if impingement upon the deltoid ligament
or medial malleolus occurred then the peroneal muscleswould become reflexly overactive. He hypothesised that
this imbalance produced pronation of the foot, and
indeed might even lead to subluxation ofthe talonavicular
joint.
Kidner therefore advocated a more complex opera-tion in which not only was the accessory navicular shelled
M. F. Macnicol, BSc, MCh Orth, FRCS Ed(Orth) Consultant Ortho-paedic Surgeon, Part-time Senior LecturerPrincess Margaret Rose Orthopaedic Hospital, Fairmilehead, Edin-burgh EH 10 7ED, Scotland.
S. Voutsinas. MD, Research FellowI 2 Thiras, Keratsini, Piraeus, Greece.
Requests for reprints should be sent to Mr M. F. Macnicol.
out from the tibialis posterior, but the main portion ofthe tendon was also re-routed under the navicular, withthe intention of restoring the normal line of pull of the
tendon. Occasionally, a limited fusion of the cuneiform-
metatarsal or talonavicularjoints also was recommended.
The rationale and efficacy of this operation have beenquestioned(Giannestras 1973; Veitch 1978; Sullivan and
Miller 1979) although the procedure is still described in anumber of orthopaedic textbooks. Leonard et a!. (1965)
supported the use of the operation, and Chater (1962)recommended the Kidner procedure for adults, reservingsimple excision for the child.
Both the Kidner procedure and simple excision havebeen used in Edinburgh in patients whose symptomshave not responded to conservative measures. The
indications for the two operations have been comparable,
although in general the Kidner procedure has beenreserved for the more severe flat foot. In all patients the
source of symptoms was considered to be the result of aprominent accessory navicular, though flat foot was an
associated feature in a significant proportion of cases.
The results of the two operations have been reviewedand certain radiographic features will be discussed.
CLINICAL MATERIAL
Between 1962 and 1978, 76 patients with a symptomatic
accessory navicular in one or both feet were treated
surgically. Patients with a fused accessory navicular or a
prominent navicular tuberosity were not included. Thecase notes were reviewed retrospectively and 29 patients
excluded from the study as the pre-operative clinicaldetails, radiographs and photographs were considered to
be incomplete. The remaining 47 patients were all
examined at a special clinic. In 26 the Kidner procedurewas performed ; the remaining 21 were treated by excision

Localised tenderness
Fig. I
Fig. 2
SURGICAL TREATMENT OF THE SYMPTOMATIC ACCESSORY NAVICULAR 219
VOl.. 66-B. No. 2. MAR(H 984
Pain
Pain interfering with sport
Pain atthe end ofan ordinary day
Rest pain
Pain since trauma
Prominence
Shoe pressure
Frequency and characteristics of the symptoms reported by both groups of patients. Pain has been subdivided into fourcategories.
Plantar view of weight-hearing feet with bilateral Type IIaccessory naviculars. The medial prominences are clearly
seen. particularly on the right fot.
of the accessory bone and trimming of any residual
medial prominence of the main navicular bone. Table I
shows the composition ofeach group; females presented
approximately twice as often as males, and the Kidner
procedure was recommended bilaterally in half of the
cases operated upon, unlike simple excision where the
procedure was usually limited to one or other foot.
Figure 1 shows the symptoms in each operative
group. Pain and local tenderness over the medial
prominence (Fig. 2) was present in nearly all cases;
difficulty with shoes was less common and occurred
chiefly in women. The pain was usually described as an
ache felt over the instep or the medial prominence
towards the end of the day, although occasionally rest
pain was also present. In approximately 15 per cent of
cases a sprain of the foot was considered to be the
precipitating cause of symptoms. Other members of the
family are sometimes found to have the same condition

Mild Moderate Severe
Medial arch Slight Major (ompletc
depression
Navicular Slight Moderate Scvcrctuherositvprominence
Heel eversion 0 10 0 15 dcgrccs > I 5 degreesdegrees
Calcaneal tendon Central Slight lateral Considerabledeviation lateral des ation
Ankle Neutral Mild tilt Moderate tilt
Forefoot Neutral Mild abduction Abduction andhut no rotation pronation
Fig. 3
Three right feet : a mother (centre). her son (left) and her daughter, all of whom had bilateral accessory naviculars. The son had beensuccessfully treated for persisting foot pain by simple excision of the ossicle and surgical contouring of the main navicular.
220 M. F. MACNICOL, S. VOUTSINAS
THE JOURNAL OF BONE AND JOINT SURGERY
(Fig. 3), and McKusick (1968) considers that the
accessory navicular manifests as an autosomal dominant
trait.
The mean duration of symptoms was 33 months in
each group, ranging from 3 months to 19 years for
patients treated by the Kidner procedure, and from 6
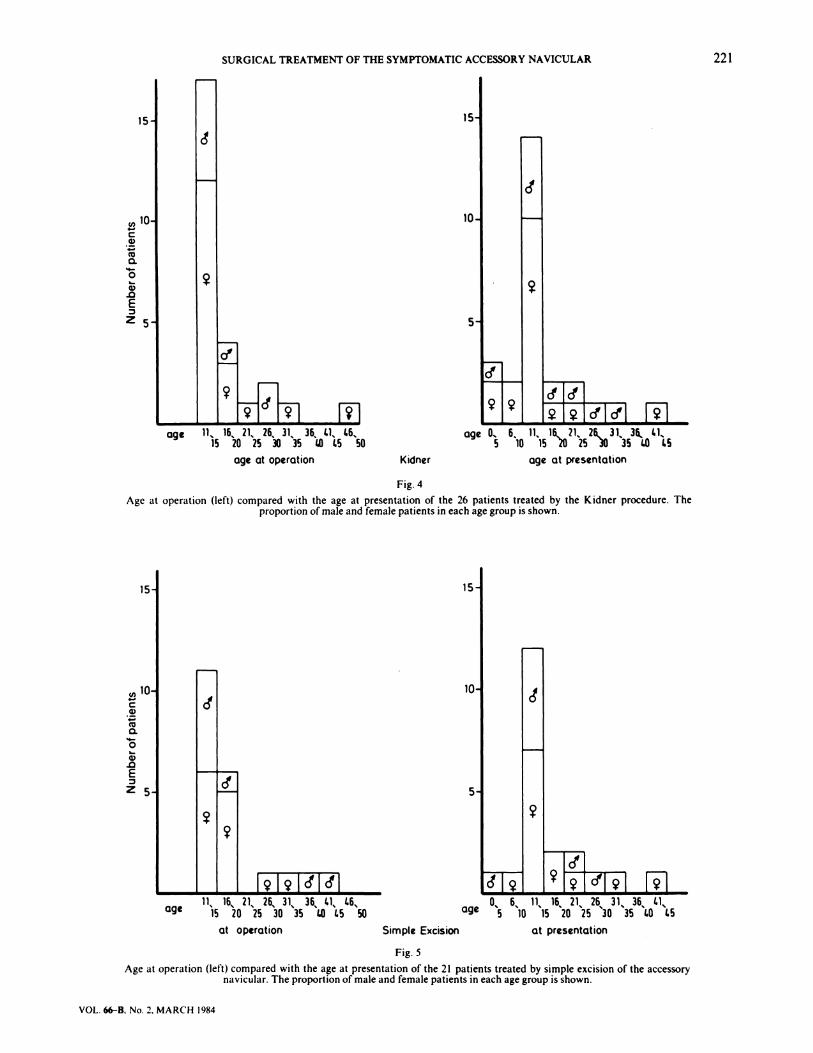
months to I 5 years for the group treated by simpleexcision. The age at operation and the age at presentation
for the two groups are shown in Figures 4 and 5. Mostpatients presented between the ages of 10 and 1 5 years
but a few were under 5 years of. age, and some were
middle-aged.
Clinical appearances. Of the 26 patients treated by theKidner procedure, 22 (85 per cent) presented with mobileflat feet, of similar severity bilaterally. Flat feet were
classified as mild, moderate or severe according to the
criteria in Table II. Two patients had severe flat feet, 12
moderate flat feet and 8 mild flat feet. Of the remaining
four patients, three presented with clinically normal feetand one with rigid spastic flat feet secondary to
calcaneonavicular bars. In none ofthe patients was there
clinical evidence of a neuromuscular disorder.
In the group of 21 patients treated by excision of the
accessory navicular, the majority had normally shaped
medial arches apart from the medial prominence.
However, five were classified as having bilateral mobileflat foot (one severe, three moderate and one mild), and
one further case had a severe, more rigid flat foot. None
was found to have tarsal coalition or neuromuscular
abnormalities.
Radiographic appearances. At the time of operationradiographs showed that 1 3 out of the 26 patients
admitted for the Kidner procedure had bilateral accessorynavicular bones, whereas only 2 of the 21 treated by
simple excision had bilateral ossicles. The accessory
navicular has been classified into two types (Dwight
1907) both of which may present in the same patient.
Type I is small, round and discrete from the main
navicular (Figs 6, 7 and 8); it should be distinguished
from the posterior tibial sesamoid which is rarely visible
radiographically (Wood l949� O’Rahilly 1953). Type II,
originally described by Geist (1925), is closely related to
the body of the navicular but separated by an irregular
plate of dense fibrocartilage (Figs 9 and 10). Various
stages of bony union may be apparent, and traumatic or
degenerative features are known to develop both macro-
Table I. A comparison of the two groups
Operation Total M F Bilateral 1. RTotal numberof operations
Kidner 26 8 IS I) S S 39
Excision 21 8 13 2 5 14 23
scopically (Fig. 1 1 ) and microscopically (Zadek and Gold
1948). There were three Type I and 36 Type II accessory
naviculars in the Kidner group and two and 21
respectively in the group treated by excision alone.
Although pre-operative radiographs were retrieved
forall patients, only standinglateral views were considered
to be ofdiagnostic value; 17 were available in the Kidner
group and five in the group treated by simple excision.
Table II. Clinical grading of hat toot. tccording to the appcaranccswhen weight-hearing
15
U)
C
0.
0
.0
E
2
of
15 15-
1o�
5
2
19191tflc5’l
SURGICAL TREATMENT OF THE SYMPTOMATIC ACCESSORY NAVICULAR 221
VOL. 66-B, No. 2, MARCH 1984
age 1l� l6� 21� 26� 31% 36 61. 46.. age O� 6. 11� l6�. ?1. 31% 3� 1.1�15202530351.04550 5 1O�52Ol5 1351.045
age at operation Kidner age at presentation
Fig. 4
Age at operation (left) compared with the age at presentation of the 26 patients treated by the Kidner procedure. Theproportion of male and female patients in each age group is shown.
U)
C
0.
0
.0
E
Z5
�ki�i [�111% 16� 2l� 26� 31 36 6�. 66� 0� 6 11� � � 26 � 35� 61�
age � � � 30 35 1.0 65 50 age � �o 15 20 25 30 35 60 45
at operation Simple Excision at presentation
Fig. 5
Age at operation (left) compared with the age at presentation of the 21 patients treated by simple excision of the accessorynavicular. The proportion of male and female patients in each age group is shown.
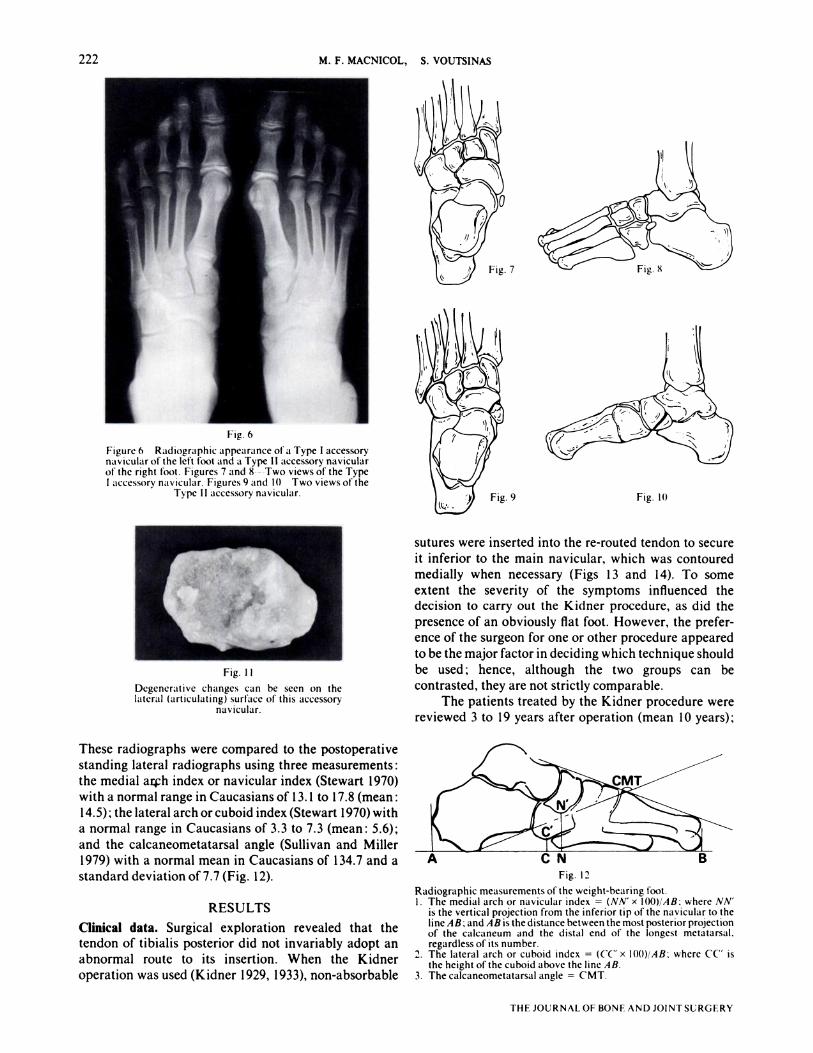
Fig. I I
Degenerative changes can be seen on thelateral (articulating) surface of this accessory
navicular.
Fig. 12
222 M. F. MACNICOL, S. VOUTSINAS
THE JOURNAL OF BONE AND JOINT SURGERY
Fig. 6
Figure 6 Radiographic appearance ofa Type I accessorynavicularofthe left foot and a Type II accessory navicularof the right foot. Figures 7 and 8--Two views of the TypeI accessory navicular. Figures 9 and 10 Two views of the
Type II accessory navicular.
These radiographs were compared to the postoperative
standing lateral radiographs using three measurements:
the medial arch index or navicular index (Stewart 1970)with a normal range in Caucasians of 1 3. 1 to 17.8 (mean:
14.5); the lateral arch or cuboid index (Stewart 1970) with
a normal range in Caucasians of 3.3 to 7.3 (mean: 5.6);
and the calcaneometatarsal angle (Sullivan and Miller
1979) with a normal mean in Caucasians of 134.7 and a
standard deviation of7.7 (Fig. 12).
RESULTS
Clinical data. Surgical exploration revealed that thetendon of tibialis posterior did not invariably adopt anabnormal route to its insertion. When the Kidner
operation was used (Kidner 1929, 1933), non-absorbable
7�s�j�
Fig. 9 Fig. 10
sutures were inserted into the re-routed tendon to secure
it inferior to the main navicular, which was contouredmedially when necessary (Figs 13 and 14). To some
extent the severity of the symptoms influenced thedecision to carry out the Kidner procedure, as did the
presence of an obviously flat foot. However, the prefer-ence of the surgeon for one or other procedure appeared
to be the major factor in deciding which technique shouldbe used; hence, although the two groups can be
contrasted, they are not strictly comparable.
The patients treated by the Kidner procedure werereviewed 3 to 19 years after operation (mean 10 years);
Radiographic measurements of the weight-bearing foot.I. The medial arch or navicular index = (NN’ x I00)/AB: where NN’
is the vertical projection from the inferior tip of the navicular to theline AB: and AB is the distance between the most posterior projectionof the calcaneum and the distal end of the longest metatarsal,regardless of its number.
2. The lateral arch or cuboid index = (CC x l00)/AB: where C(’ isthe height of the cuboid above the line AB.
3. The calcaneometatarsal angle = CMT.
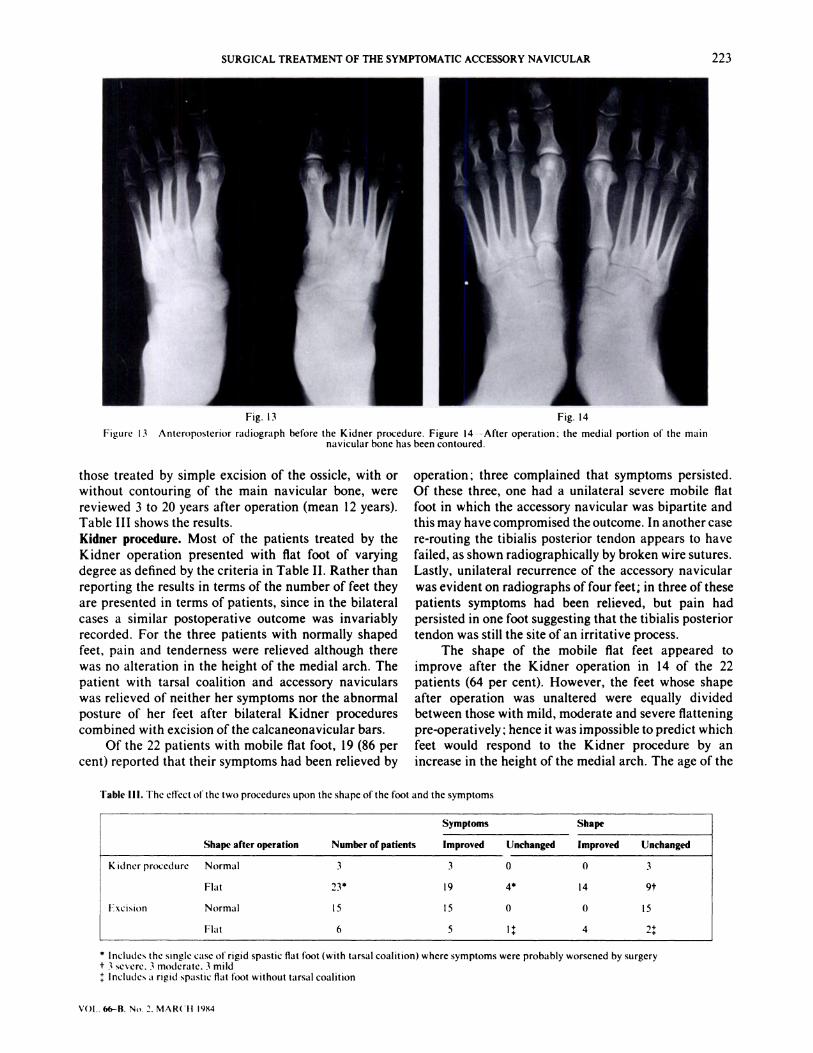
Fig. 13 Fig. 14
Figure 13 Anteroposterior radiograph before the Kidner procedure. Figure 14--After operation: the medial portion of the mainnavicular bone has been contoured.
Symptoms Shape
Shape after operation Number of patients Improved Unchanged Improved Unchanged
Kidnerprocedure Normal 3 3 0 0 3
Flat 23* 19 4* 14 9t
Excision Normal 15 15 0 0 15
Flat 6 5 l� 4 2�
SURGICAL TREATMENT OF THE SYMPTOMATIC ACCESSORY NAVICULAR 223
VOl.. 66-8. No. 2. MARCH 984
those treated by simple excision of the ossicle, with or
without contouring of the main navicular bone, were
reviewed 3 to 20 years after operation (mean 12 years).
Table III shows the results.
Kidner procedure. Most of the patients treated by the
Kidner operation presented with flat foot of varyingdegree as defined by the criteria in Table II. Rather than
reporting the results in terms of the number of feet they
are presented in terms of patients, since in the bilateral
cases a similar postoperative outcome was invariably
recorded. For the three patients with normally shaped
feet, pain and tenderness were relieved although there
was no alteration in the height of the medial arch. The
patient with tarsal coalition and accessory naviculars
was relieved of neither her symptoms nor the abnormal
posture of her feet after bilateral Kidner procedures
combined with excision of the calcaneonavicular bars.
Of the 22 patients with mobile flat foot, 19 (86 percent) reported that their symptoms had been relieved by
operation ; three complained that symptoms persisted.Of these three, one had a unilateral severe mobile flatfoot in which the accessory navicular was bipartite andthis may have compromised the outcome. In another case
re-routing the tibialis posterior tendon appears to have
failed, as shown radiographically by broken wire sutures.
Lastly, unilateral recurrence of the accessory navicular
was evident on radiographs of four feet; in three of these
patients symptoms had been relieved, but pain had
persisted in one foot suggesting that the tibialis posterior
tendon was still the site of an irritative process.The shape of the mobile flat feet appeared to
improve after the Kidner operation in 14 of the 22patients (64 per cent). However, the feet whose shape
after operation was unaltered were equally dividedbetween those with mild, moderate and severe flatteningpre-operatively; hence it was impossible to predict which
feet would respond to the Kidner procedure by anincrease in the height of the medial arch. The age of the
Table Ill. The efrect ofthe two procedures upon the shape ofthe foot and the symptoms
* Includes the single case of rigid spastic flat foot (with tarsal coalition) where symptoms were probably worsened by surgery
t 3 severe. 3 moderate. 3 mild
�: Includes a rigid spastic flat foot without tarsal coalition
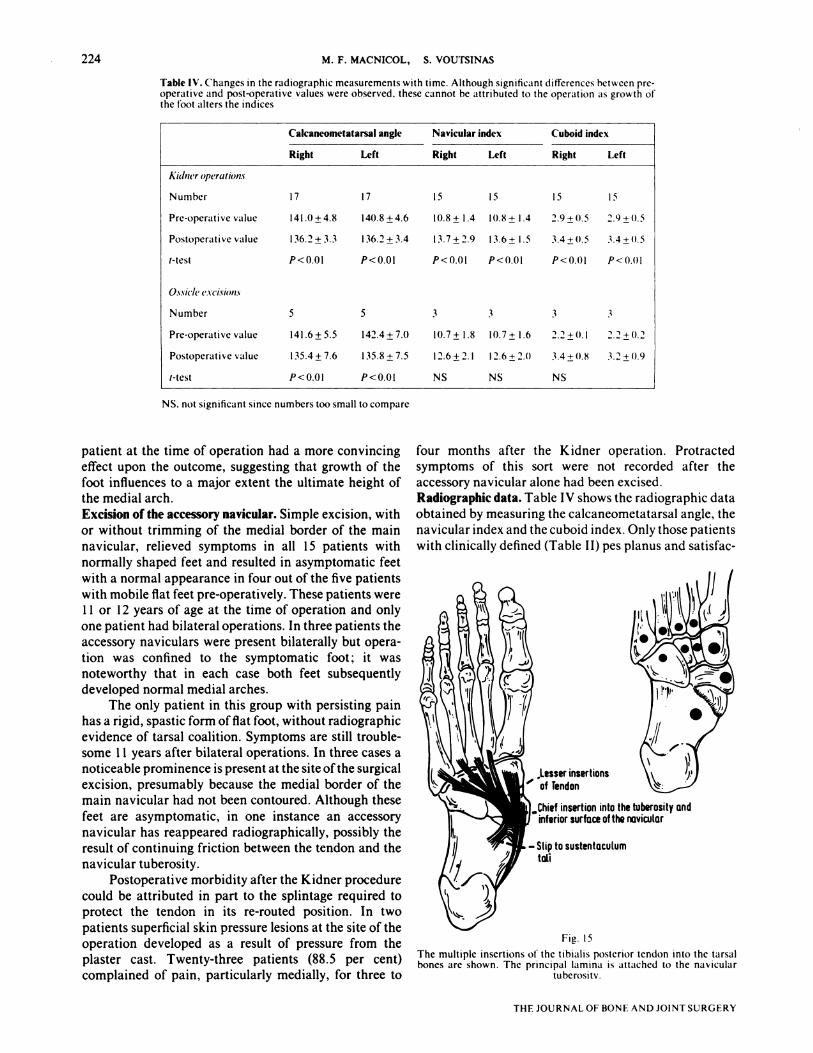
Calcaneometatarsal angle Navicular index Cuboid index
Right left Right left Right Left
Aulnt’r operations
Number 17 17 15 IS 15 15
Pre-operative value 141.0±4.8 140.8±4.6 10.8± 1.4 10.8± 1.4 2.9±0.5 2.9±0.5
Postoperative value 136.2±3.3 136.2±3.4 13.7±2.9 13.6± 1.5 3.4±0.5 3.4±0.5
t-test P < 0.01 P< 0.01 P < 0.01 P < 0.01 P < 0.0 I P <0.01
O.5.sl(l(’ e.vci.sion.s
Number 5 5 3 3 3 3
Pre-operativevalue 141.6±5.5 142.4±7.0 10.7± 1.8 10.7± 1.6 2.2±0.1 2.2±0.2
Postoperative value 135.4± 7.6 1 35.8 ± 7.5 12.6 ± 2. 1 I 2.6 ± 2.0 3.4 ±11.8 3.2 ± 0.9
t-test P<0.01 P<0.Ol NS NS NS
ond
- Slip to sustentacuLumtaLl
Fig. 15
The multiple insertions of the tibialis posterior tendon into the tarsalbones are shown. The principal lamina is attached to the navicular
tuberositv.
224 M. F. MACNICOL, S. VOUTSINAS
TI-IF JOURNAL OF BONE AND JOINT SURGERY
Table IV. Changes in the radiographic measurements with time. Although significant differences between pre-operative and post-operative values were observed, these cannot be attributed to the operation as growth ofthe foot alters the indices
NS. not significant since numbers too small to compare
patient at the time of operation had a more convincing
effect upon the outcome, suggesting that growth of the
foot influences to a major extent the ultimate height ofthe medial arch.
Excision of the accessory navicular. Simple excision, withor without trimming of the medial border of the main
navicular, relieved symptoms in all 15 patients with
normally shaped feet and resulted in asymptomatic feet
with a normal appearance in four out of the five patients
with mobile flat feet pre-operatively. These patients were1 1 or 12 years of age at the time of operation and only
one patient had bilateral operations. In three patients the
accessory naviculars were present bilaterally but opera-
tion was confined to the symptomatic foot ; it wasnoteworthy that in each case both feet subsequentlydeveloped normal medial arches.
The only patient in this group with persisting pain
has a rigid, spastic form offlat foot, without radiographic
evidence of tarsal coalition. Symptoms are still trouble-
some I I years after bilateral operations. In three cases a
noticeable prominence is present at the site ofthe surgical
excision, presumably because the medial border of the
main navicular had not been contoured. Although these
feet are asymptomatic, in one instance an accessory
navicular has reappeared radiographically, possibly the
result of continuing friction between the tendon and the
navicular tuberosity.
Postoperative morbidity after the Kidner procedure
could be attributed in part to the splintage required to
protect the tendon in its re-routed position. In two
patients superficial skin pressure lesions at the site of the
operation developed as a result of pressure from the
plaster cast. Twenty-three patients (88.5 per cent)
complained of pain, particularly medially, for three to
four months after the Kidner operation. Protracted
symptoms of this sort were not recorded after the
accessory navicular alone had been excised.
Radiographic data. Table IV shows the radiographic data
obtained by measuring the calcaneometatarsal angle, thenavicular index and the cuboid index. Only those patients
with clinically defined (Table II) pes planus and satisfac-

SURGICAL TREATMENT OF THE SYMPTOMATIC ACCESSORY NAVICULAR 225
VOL. 66-B. No. 2. MARCH 1984
tory pre-operative standing radiographs are included and
hence the numbers are small. Irrespective of the nature
of the operation, or whether the surgical procedure was
bilateral or unilateral, the same changes in the various
indices were evident in both feet at review.
If these radiographic measurements of the arch of
the foot are accepted as valid, they show that re-routing
the tibialis posterior tendon has no effect upon the
radiographic indices; similar changes occur after simple
excision. Changes in the navicular index were most
marked when there was an obvious flat foot before
operation, but this effect was no different from that seenin the few such cases subjected to simple excision.
DISCUSSION
The multiple insertions of the tibialis posterior tendoninto the tarsal bones (Fig. 15) suggests that the action of
the muscle is to elevate the medial arch. A major portion
of the tendon is inserted into the body and tuberosity of
the navicular and it has often been observed that
flattening of the foot follows traumatic severance or
attrition rupture. Kidner presumed that any deviation in
the insertion of tibialis posterior would diminish its
suspensory action, although it can equally be argued that
the accessory navicular may enhance the tendon function
by a pivot effect. The theory that an accessory navicular
produces reflex overactivity of the peroneal muscles was
also not substantiated from this review.
Recurrence ofthe ossicle after excision only occurredwith Type I ossicles and suggests that this variant mayresult from stress applied to the tibialis posterior tendon
as it passes over the medial surface of the navicular. It
was notable that recurrence of the ossicle occurred only
when the prominence of the medial border of the main
navicular had not been trimmed.
A symptomatic accessory navicular presents as
commonly in flat feet as in feet with a normal medial
arch ; hence it is unproven whether the appearance of the
accessory navicular causes flat foot or is produced by it.
Probably the ossicle is part ofthe configuration of certain
pronated feet thereby contributing to any symptoms; butit is also clear that after simple excision of the accessory
navicular alone, a foot may be left with an entirely
normal medial arch radiographically.
Symptoms from the accessory navicular develop in
approximately one per thousand of the population
according to Harris and Beath (1947), being more
common in women (Specht 1973) and sometimes mani-
festing quite late in life. The ossicle is probably the most
common accessory bone in the foot, becoming radio-
graphically apparent between the ages of 9 and 1 1 years
in approximately 19 per cent of the population (Geist
1925). It persists as a distinct, separate bone in two per
cent (Zadek and Gold 1948), normally fusing completely
or incompletely to the navicular. Trauma may precipitatesymptoms and was felt to be contributory in 1 5 per cent
of cases in this review. Pain is produced by friction or
pressure over the medial prominence, by degenerative
changes in the synchondrosis, or by an associated foot
strain in cases with pes planus. Women present twice as
commonly as men, possibly because the type of shoe
worn and the greater incidence of ligamentous laxitypredispose towards the onset of symptoms.
Operation is advised only if symptoms persist after
conservative measures have been tried. Alterations to
footwear, and exercises for the intrinsic foot muscles and
lateral thigh rotators may prevent or delay the need foroperation, but once symptoms have become establishedoperation was felt to be justified. The Kidner procedure
did not confer any advantages when compared to simple
excision of the ossicle although the two series are not
strictly comparable, as the radiographic incidence of flat
foot pre-operatively was greater in the former group.Simple excision was highly successful as long as it was
combined with contouring the navicular tuberosity;
patients could be encouraged to take weight without
splintage as soon as the wound had healed, whereas after
the Kidner procedure a plaster cast for six weeks isrecommended.
Although the effects of the two procedures upon theshape of the foot was assessed radiographically the
interpretation of these results was hampered by several
factors. Pre-operative standing lateral radiographs were
not always available, and alterations in lower limbrotation and the degree of weight-bearing affected theaccuracy ofthe assessment. Furthermore, ifthe sesamoid
underlying the first metatarsophalangeal joint was not
ossified, measurement ofthe medial arch by the navicular
index proved impossible and therefore the calcaneo-
metatarsal angle (Sullivan and Miller 1979) became the
only assessment possible. Nevertheless it was clear that
the few cases of radiographically flat foot treated by
simple excision responded with an increase in the
navicular index similar to the larger number of cases of
pes planus treated by the Kidner procedure (Fig. 14).
The outcome was unpredictable, however, and Veitch(1978), who reviewed 15 patients with clinical pes planus
before the Kidner procedure, did not find any withpostoperative improvement in the arch. On the other
hand, Leonard et al. (1965) reported satisfactory results
in 25 feet subjected to the Kidner procedure, with the
postoperative production of a good medial arch. In this
present series an improvement in the navicular indexwas evident in virtually all cases.
Significantly, half of the non-operated feet, particu-
larly in the younger patients, improved with time. Thus,
12 out of 22 Kidner procedures produced a normal pair
of feet radiographically, but in five of these I 2 patients
operation had been performed on only one foot. This
confirms the well-established fact that the growing foot
develops a higher medial arch as it matures (Jones 1975)
and casts further doubt on the validity of altering the
tibialis posterior tendon insertion. The Kidner procedure
does not appear to offer any advantages over simple

226 M. F. MACNICOL, S. VOUTSINAS
THE JOURNAL OF BONE AND JOINT SURGERY
excision of the ossicle, and the postoperative care is and the parent bone. Contouring of any residual medialcertainly more elaborate. While the two series in this prominence is an important addition to either operationreview are not strictly comparable, symptoms were as it not only improves the shape of the medial border ofrelieved equally by either procedure, suggesting that pain the foot but decreases both the likelihood of recurrent
is produced by pressure over the prominent accessory symptoms and the radiographic reappearance of annavicular and the resultant friction between the ossicle ossicle within the tibialis posterior tendon.
REFERENCES
Chater EH. Foot pain and the accessory navicular bone. IrJ MedSci 1962:422:471-5.
Dwight T. Variations of the hones o/the hands andj#{232}et: a c/mica/atlas. Philadelphia : JB Lippincott Co., 1907.
Froelich R. Des osselets surnum#{233}raires du tarse et de leur importance pratique. Ret’ Med de lEst I 909 : 41 : 433-6.
Geist ES. The accessory scaphoid bone. J Bone Joint Surg 1925 : 7 : 570-4.
Giannestras NJ. Foot disorders: medicalandsurgicalmanagement. 2nd ed. Philadelphia : Lea and Febiger. 1973.
Harris RI, Beath T. Army foot survey: an investigation offoot ailments in Canadian soldiers. Ottawa : National Research Council. 1947.
Jones BS. Flat-foot : a preliminary report of an operation for severe cases. J Bone Joint Surg [Br] 1975 : 57-B : 279-82.
Kidner FC. The prehallux (accessory scaphoid) in its relation to flat-foot. J Bone Joint Surg 1929 : II : 831 7.Kidner FC. Pre-hallux in relation to flatfoot. JAMA 1933; 101 : 1539-42.
Leonard MH, Gonzales S, Breck 1W, Basom C, Palafox M, Kosicki ZW. Lateral transfer of the posterior tibial tendon in certain selected cases ofpes pIano valgus (Kidner operation). C/in Orthop 1965 :40: 139-44.
McKusick VA. Mende/ian inheritance in man : catalogs o/autosomaldominant. autosoma/recessire and X-/inkedphenotipe.s. 2nd ed. Baltimore : JohnsHopkins Press, 1968.
O’Rahilly R. A survey ofcarpal and tarsal anomalies. J Bone Joint Surg [Am] 1953 : 35-A : 626-42.
Specht EE. Minor congenital deformities and anomalies of the foot. In : Inman VT, ed. Du Vries’ surger� ofthe/#{243}ot, 3rd ed. St Louis : CV Mosby1973: 54-8.
Stewart SF. Human gait and the human foot : an ethnological study of the flatfoot. Part I. C/in Orthop 1970: 70: 1 I 1-23.
Sullivan JA, Miller WA. The relationship ofthe accessory navicular to the development ofthe flat foot. C/in Orthop 1979: 144: 233-7.
Veitch JM. Evaluation ofthe Kidner procedure in the treatment of symptomatic accessory tarsal scaphoid. C/in Orthop 1978 :131 : 2 10-3.
Wood JF. Structure andfunction as seen in thefbot. 2nd ed. London : Balli#{234}re,Tindall & Cox, 1949.
Zadek I, Gold AM. The accessory tarsal scaphoid. J Bone Joint Surg [Am] 1948 : 30-A : 957-68.