the anatomy of the navicular and periarticular structures
TRANSCRIPT

Foot Ankle Clin N Am
9 (2004) 1–23
The anatomy of the navicular and
periarticular structures
Pau Golano, MD*, Oscar Farinas, MD, Ivan Saenz, MDLaboratory of Arthroscopy and Surgical Anatomy, Department of Human Anatomy and Embryology,
Faculty of Medicine, University of Barcelona, C/ Feixa Llarga s/n,
08907 L’Hospitalet de Llobregat, Barcelona, Spain
Bone morphology
In general, the navicular bone has a roughly pyriform shape whose major
oblique axis is oriented in the dorsoplantar and lateromedial directions, adapting
itself to the angle of rotation of the head of the talus (�45�) [1]. Its round base is
situated dorsolaterally, whereas its apex is oriented plantarmedially. From its mor-
phology, it is possible to distinguish four faces and two ends (Fig. 1).
Posterior aspect
The posterior aspect articulates with the head of the talus, although the
articular surface does not completely cover it [2]. It has a biconcave surface that
is completely covered with articular cartilage (Fig. 2). The degree of concavity is
variable; in some cases, the articular surface is nearly flat [3].
Anterior aspect
The anterior aspect has a nephroid appearance with plantar concavity. Two
slight crests divide the anterior aspect into three articular surfaces. These crests
extend dorsoplantarly and converge at the plantar margin. Although the articular
surfaces are oriented in different directions, overall, the anterior surface is convex
(Fig. 3).
The largest articular surface, the medial articular surface, is convex and
articulates with the medial cuneiform bone. It has a roughly triangular shape,
1083-7515/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/S1083-7515(03)00155-4
* Corresponding author.
E-mail address: [email protected] (P. Golano).
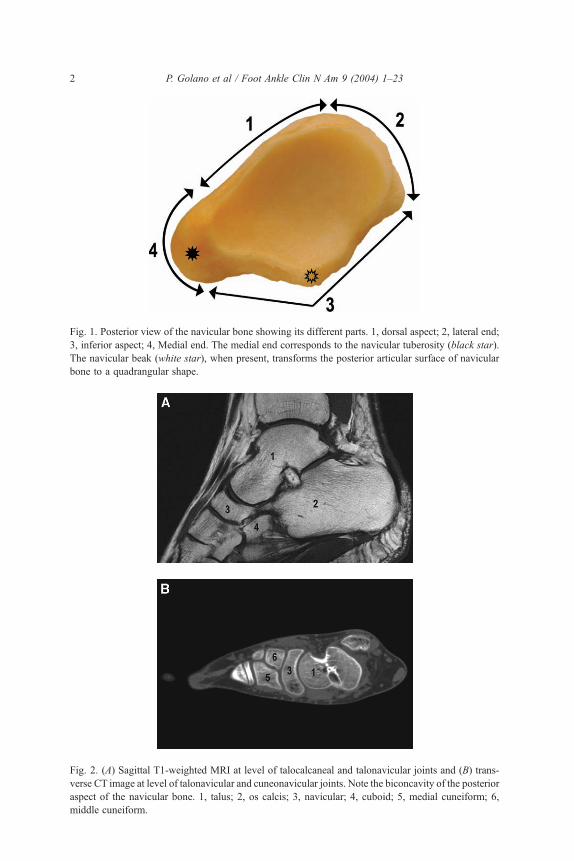
Fig. 1. Posterior view of the navicular bone showing its different parts. 1, dorsal aspect; 2, lateral end;
3, inferior aspect; 4, Medial end. The medial end corresponds to the navicular tuberosity (black star).
The navicular beak (white star), when present, transforms the posterior articular surface of navicular
bone to a quadrangular shape.
Fig. 2. (A) Sagittal T1-weighted MRI at level of talocalcaneal and talonavicular joints and (B) trans-
verse CT image at level of talonavicular and cuneonavicular joints. Note the biconcavity of the posterior
aspect of the navicular bone. 1, talus; 2, os calcis; 3, navicular; 4, cuboid; 5, medial cuneiform; 6,
middle cuneiform.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–232

Fig. 3. Transverse CT image at the level of navicular bone. Note the convexity of the anterior aspect
of the navicular bone that is formed by the convergence of the three articular surfaces of the cunei-
form bones (white arrows). 1, navicular bone; 2, Os calcis.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 3
with a dorsally convex base. The middle or intermediate articular surface, which
is flat or slightly convex, also is triangular with a dorsal base. It articulates with
the intermediate or middle cuneiform bone. The lateral articular surface, which is
flat or slightly convex, is the smallest of the three and has roughly quadrangular
morphology. The three articular surfaces converge plantarly and make up the
transverse tarsal arch of the foot.
As mentioned by Sarrafian [4], the navicular bone plays a role in the change in
direction of the medial bone column. The neck and head of the talus initiate a
medial deviation, whereas the navicular bone orients this column laterally and
plantarly. The ‘‘zigzag’’ arrangement maintains the axial alignment of the foot,
despite the initial divergence.
Dorsal aspect
Markedly convex, the dorsal aspect is wider in its medial portion. The highest
point of the convexity coincides with the intermediate or middle articular surface.
This aspect provides insertion for many capsulo-ligamentous structures.

Fig. 4. Fluoroscan image of two different navicular bones: (A) with navicular beak (black arrow) and
(B) without it.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–234
Plantar aspect
The plantar aspect is irregular and is continuous medially with the navicular
tuberosity. It often presents an osseous prominence called the ‘‘navicular beak’’
(Fig. 4). Some investigators consider this prominence to be a fused os cuboides
secundarium [5,6]. When this prominence is present, the posterior articular
surface of the navicular bone extends downwards, thus adopting a quadrangular
morphology. Like the dorsal aspect, the plantar aspect provides insertion for
many capsulo-ligamentous structures.
Medial end
The medial end is made up of an osseous prominence, the navicular tuber-
osity. The plantar and medial avicular ligaments, as well as the tendon of the pos-
terior tibialis muscle, insert into the navicular tuberosity.
The size of this osseous prominence is variable. When it is separated from the
rest of the bone, it is known as the ‘‘naviculare secundarium’’ or ‘‘accessory
navicular bone.’’
Lateral end
The lateral end is convex and has two discernible segments—the inferior or
plantar segment and the superior or dorsal segment. The superior segment pro-
vides insertion for the medial component of the bifurcate ligament or lateral
calcaneonavicular ligament. A small, inconstant articular surface [3] for the
cuboid occupies nearly all of the inferior segment and is continuous with the
articular surface for the lateral cuneiform bone.
Joints and ligaments
From a functional and anatomical point of view, the subtalar articular com-
plex is formed by the posterior talocalcaneal joint and the acetabulum pedis [7],
which contains the head of the talus. The talocalcaneonavicular joint, or ace-
tabulum pedis, thus named for its morphologic similarity to the hip joint [8], is
made up of a series of skeletal and ligamentous structures. The skeletal elements

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 5
include the posterior articular surface of the navicular and the anterior and mid-
dle calcaneal articular surfaces, which articulate with the head and the antero-
medial surface of the anterior aspect of the talus. These osseous structures are
joined or stabilized by the inferior or plantar and superomedial calcaneonavicular
ligaments. The lateral calcaneonavicular ligament, a component of the bifurcate
ligament, provides the lateral limit (Fig. 5).
There is a lot of confusion and disagreement in the literature [9–13] regard-
ing the description of the plantar calcaneonavicular ligament, also known as
the spring ligament. According to Testut and Jacob [8], the plantar calcaneona-
vicular ligament is made up of a fibrocartilaginous and a fibrous component in
which it is possible to differentiate two types of fascicles, an anterior fascicle that
is inserted into the plantar aspect of the navicular and a transverse fascicle that is
Fig. 5. Dorsal view of the acetabulum pedis after removing the talus. The components of the
acetabulum pedis are classified as osseous (posterior articular surface of navicular bone, anterior and
middle calcaneal articular surface) and ligamentous (superomedial, inferior, and lateral calcaneona-
vicular ligaments). 1, posterior articular surface of navicular bone; 2, anterior calcaneal articular
surface; 3, middle calcaneal articular surface, 4; posterior calcaneal articular surface; 5, superomedial
calcaneonavicular ligament; 6, inferior calcaneonavicular ligament; 7, lateral calcaneonavicular
ligament (component of bifurcate ligament).

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–236
fused with the deltoid ligament. Weitbreck [14] differentiated two fascicles of the
plantar calcaneonavicular ligament. The main one, plantar and rounded, inserts
into the plantar aspect of the navicular; the second, medial and flat, inserts into
the medial end of the navicular bone. Moreover, in 1993, Sarrafian [4] described
two differentiated ligaments: the superomedial and inferior calcaneonavicular
ligaments. It is possible that the confusion about the description of these struc-
tures lies in their indivisibility; the medial margin of the inferior calcaneonavicu-
lar ligament is continuous with the superomedial calcaneonavicular ligament
[15]. Also it is difficult to dissecting these ligaments because of their fibrocarti-
laginous characteristics, although they can be delimited artificially. Some inves-
tigators speak of a spring ligament complex that includes the superomedial and
inferior calcaneonavicular ligaments, as well as the talonavicular fascicle of the
superficial component of the deltoid ligament [2,16].
Fig. 6. (A) Medial view of an osseous rearfoot and midfoot. Note the origin and insertion sites of
superomedial calcaneonavicular ligament (dark green lines). This ligament joins laterally with fibers of
the tibionavicular component of the deltoid ligament (pink lines), and plantarly with the inferior
calcaneonavicular ligament (light green lines). (B) Medial view of navicular and os calcis. The
superomedial calcaneonavicular ligament attaches to the superior, medial, and inferior articular
margins of the medial third of the navicular bone and sustentaculum tali. 1, navicular tuberosity;
2, sustentaculum tali.
Superomedial calcaneonavicular ligament
The superomedial calcaneonavicular ligament, also known as the ‘‘ligamen-
tum neglectum,’’ was initially described as a component of the tibiocalcaneona-
vicular ligament [17], but was later classified by Lane [18] as a separate ligament.
It has a quadrangular shape and its fibers intermingle with those of the inferior
calcaneonavicular ligament. Its origin is at the anterior and medial margins of
the sustentaculum tali, as well as at the anterior margin of the anterior articular
surface of the os calcis. This ligament shares its origin with the tibiocalcaneal part
of the superficial deltoid ligament. From its origin, the superomedial calcaneo-
navicular ligament follows the perimeter of the margin of the anterior calcaneal
articular surface, fans out anteriorly, dorsally, and laterally, with a lateral con-
cavity, and ends in a broad insertion at the margin of the posterior articular
surface of the navicular. Its insertional surface covers the superior, medial, and
inferior articular margins of the medial third of the navicular (Figs. 6 and 7) [16].
There are discrepancies in the anatomical studies concerning the insertion of
this ligament into the navicular tuberosity [2,4,16]. This ligament is fused along
its course with the different components of the deltoid ligament, as well as with
the superior talonavicular ligament. At its dorsal aspect, it is in intimate relation
with a thick fibrous or fibrocartilaginous layer that forms the floor of the fibrous
tunnel of the tendon of the posterior tibialis muscle (see Fig. 7). Its articular
surface presents a triangular fibrocartilaginous surface that corresponds in size
and shape to the triangular plantar-medial articular surface of the head of the talus
(Figs. 8 and 9). The fibrocartilaginous surface occasionally is ossified, which may
be one of the reasons for confusion about the existence of a possible accessory
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 7
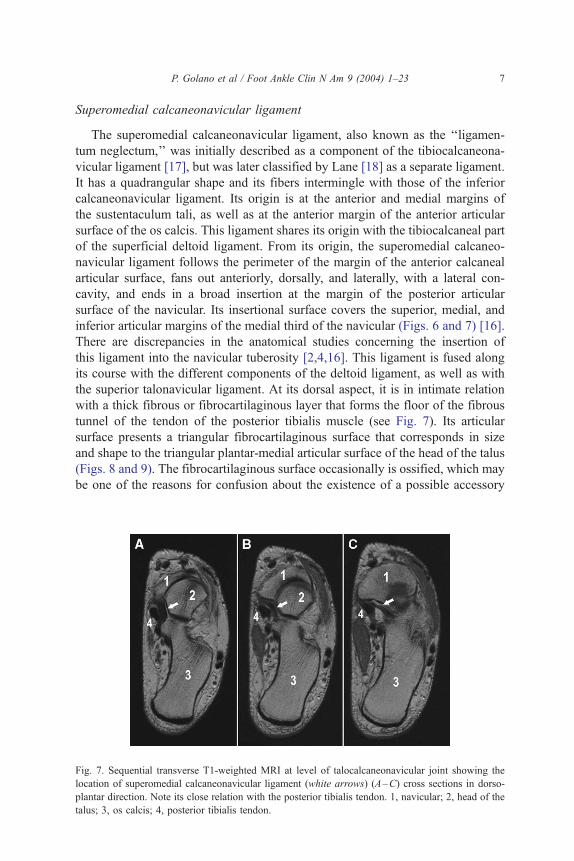
Fig. 7. Sequential transverse T1-weighted MRI at level of talocalcaneonavicular joint showing the
location of superomedial calcaneonavicular ligament (white arrows) (A–C) cross sections in dorso-
plantar direction. Note its close relation with the posterior tibialis tendon. 1, navicular; 2, head of the
talus; 3, os calcis; 4, posterior tibialis tendon.

Fig. 8. Fluoroscan dorsoplantar view of an osteoarticular fresh-frozen cadaveric specimen. The
talus has been removed to show the osseous components of the acetabulum pedis. Note the presence
of a fibrocartilaginous tissue (black star) that corresponds with the superomedial calcaneonavicu-
lar ligament.
Fig. 9. Medial (A), dorsal (B), and anterior (C) view of the talus. Note the triangular plantarmedial
articular surface of the head of the talus (arrows) for the superomedial calcaneonavicular ligament.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–238

Fig. 10. Dorsal view of spring ligament. The spring ligament is composed of the superomedial and
inferior calcaneonavicular ligament. Note the two fascicles of the inferior calcaneonavicular liga-
ment. 1a, Medial fascicle; 1b, lateral fascicle; 2, superomedial calcaneonavicular ligament; 3, pos-
terior articular surface of navicular bone; 4, anterior calcaneal articular surface; 5, middle calcaneal
articular surface.
Fig. 11. Medial view of the os calcis. The inferior calcaneonavicular ligament arises from coronoid
fossa (arrow). This fossa corresponds to a small depression that is located between the anterior and
middle calcaneal articular surface, just anterior to the sustentaculum tali.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 9

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2310
navicular bone. The concave structure of this ligament provides a gentle tran-
sitional surface for the head of the talus.
Inferior calcaneonavicular ligament
The inferior calcaneonavicular ligament is trapezoidal in shape. It is in relation
with the inferior segment of the head of the talus, which is not supported by
articular surfaces (Fig. 10). It arises from the most superior part of the coronoid
fossa, located in the space between the anterior and middle calcaneal articular
surfaces, at the level of the anterior aspect of the sustentaculum tali (Fig. 11). This
ligament inserts into the plantar aspect of the navicular bone, laterally to the
navicular beak, and just lateral to the insertion of the superomedial calcaneona-
vicular ligament (Fig. 12).
This ligament has a fascicular morphology; the lateral fascicle, which inserts
into the navicular beak, is the strongest. Between the fiber bundles there is a series
Fig. 12. (A) Plantar view of an osseous rearfoot and midfoot. The inferior calcaneonavicular ligament
(light green lines) arises from the coronoid fossa and attaches to the plantar aspect of the navicular
bone. There is a confluence of fibers with the superomedial calcaneonavicular ligament (dark green
lines) medially. (B) Plantar view of fresh-frozen cadaveric specimen showing the inferior
calcaneonavicular ligament after the posterior tibialis tendon has been removed. 1, coronoid fossa;
2, navicular bone; 3, inferior calcaneonavicular ligament; 4, plantar cubonavicular ligament.

Fig. 12 (continued).
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 11
of longitudinal intervals, with an adipose layer spread through them that covers
the plantar aspect of this ligament (Fig. 13). This fat pad is located intra-articularly
but extrasynovially.
The medial margin of this ligament is continuous with the superomedial cal-
caneonavicular ligament; in most cases, a small triangular space that is occupied
by fatty tissue, separates the two ligaments at their navicular attachments [16].
Its dorsal surface is fibrocartilaginous for the support of the head of the talus
and appears a triangular morphology. Medially, its plantar surface is in contact
with the tendon of the posterior tibialis muscle, and, laterally, with the tendons of
the flexor hallucis longus and flexor digitorum longus muscles [12].
Together with the anterior superficial fibers of the deltoid ligament, the long
plantar ligament, and the plantar fascia, the inferior calcaneonavicular ligament is
one of the main static stabilizers of the longitudinal arch of the foot [16].
Bifurcate ligament
The bifurcate ligament (or Chopart’s ligament) is made up of the lateral cal-
caneonavicular ligament and the medial calcaneocuboid ligament, which are
arranged in a ‘‘Y’’ or ‘‘V’’ with different origins at the os calcis.

Fig. 13. Dorsal view of acetabulum pedis. The talus has been removed. (A) A fat pad covers the inferior
calcaneonavicular ligament. (B) After the fat tissue has been removed the different fascicles of the
inferior calcaneonavicular ligament can be seen. Note that the anterior and middle calcaneal articular
surfaces can be fused. 1, posterior articular surface of navicular bone; 2, anterior and middle calcaneal
articular surface; 3, superomedial calcaneonavicular ligament; 4a and 4b, inferior calcaneonavicular
ligament; 5, lateral calcaneonavicular ligament (component of bifurcate ligament).
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2312
The lateral calcaneonavicular ligament arises from the anteromedial angle of
the sinus tarsi, just lateral to the anterior talar articular surface, and reaches the
lateral aspect of the intermediary tubercle [19]. It extends anteriorly, dorsally, and
medially to its insertion in the superior segment of the lateral end of the navicular
(see Figs. 5 and 13). Barclay-Smith [20] described this ligament as being formed
by two fiber bundles. The inferior fibers are short and are separated from the most
lateral portion of the inferior calcaneonavicular ligament by a fatty interval. The
superior fibers, which are the most superficial, are long and resistant and
constitute the main part of this ligament.
The medial calcaneocuboid ligament arises from the anterior aspect of the
intermediary tubercle, lateral to the origin of the lateral calcaneonavicular
ligament. It runs anteriorly and slightly inferiorly and attaches into the dorsal
aspect of the cuboid (approximately 1.5 cm anterior to the posterior margin of the
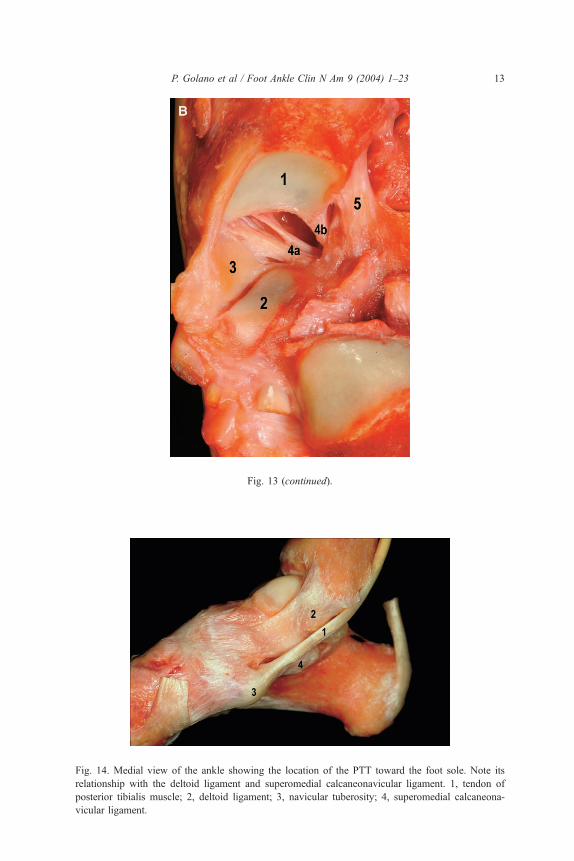
Fig. 13 (continued).
Fig. 14. Medial view of the ankle showing the location of the PTT toward the foot sole. Note its
relationship with the deltoid ligament and superomedial calcaneonavicular ligament. 1, tendon of
posterior tibialis muscle; 2, deltoid ligament; 3, navicular tuberosity; 4, superomedial calcaneona-
vicular ligament.
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 13

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2314
cuboid). The two components of the bifurcate ligament form an angle of
approximately 30� in the transverse plane and 20� in the sagittal plane [21].
Tibialis posterior tendon
The navicular bone provides tendinous insertion only to the posterior tibialis
muscle. The posterior tibialis muscle is located in the deep compartment of the leg,
Fig. 15. Plantar view of the foot. Drawing (A) and fresh-frozen cadaveric specimen dissection
(B). The anterior component of the PTT, continuity of the main tendon, attaches to the navicular
tuberosity (1), the inferior aspect of the medial cuneiform, and the inferior capsule of the medial
cuneonavicular joint (2).

Fig. 15 (continued).
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 15
between the flexor hallucis longus and flexor digitorum longus muscles. From its
broad surface of origin, it runs distally, forming a long tendon. At the level of the
inferior third of the leg, the posterior tibialis tendon (PTT), which initially runs
laterally to the flexor digitorum longus muscle, crosses this muscle and runs
medially, forming the sural decussation. With respect to the ankle joint, the PTT is
located just behind the medial malleolus, within an osteofibrous groove, and on
top of the deltoid ligament (Fig. 14).
With respect to the foot, the PTT is in contact with the inferior aspect of the
inferior calcaneonavicular ligament. Here, the tendon becomes flattened and
acquires fibrocartilaginous characteristics, or, may even have a sesamoid bone
within it; this sesamoid bone represents one of the possible types of accessory
navicular bones.
Right at the navicular tuberosity, the tendon of the posterior tibialis muscle is
divided into three components: anterior, middle, and posterior. The anterior
component is the largest of the three and is the continuation of the main tendon.

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2316
It inserts into the navicular tuberosity and the inferior capsule of the medial
cuneonavicular joint, as well as the inferior aspect of the medial cuneiform bone
(Fig. 15). The middle component is attached into the middle and lateral cuneiform
bones, the cuboid, and the bases of the second to fifth metatarsal bones (metatarsal
extension) (Fig. 16). In all specimens, a bursa was found in relation to the
metatarsal extension of the PTT. This bursa is independent of the synovial sheath
of the tendon of the posterior tibialis muscle and a small fibrous septum sepa-
rates them [22]. Its proximal limit of the bursa is located near the insertion of the
tendon into the navicular tuberosity. Finally, the posterior component, with its
recurrent path, inserts into the sustentaculum tali [23].
Fig. 16. Plantar view of the foot. Drawings showing themiddle component attachments at the level of the
middle and lateral cuneiform and cuboid (A) and to the bases of the second to fifth metatarsal bones
(B). (C) Fresh-frozen cadaveric specimen dissection of the attachments of the middle component of
the PTT. 1, attachment to middle cuneiform bone; 2, attachment to lateral cuneiform bone; 3, attachment
to cuboid; 4–6, metatarsal extension (attachments to the bases of second to fifth metatarsal bones).

Fig. 16 (continued).
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 17
The posterior tibialis muscle-tendon unit is the main dynamic stabilizer of the
rearfoot; it maintains the structure formed by the longitudinal arch of the foot [24].
Many factors are implicated as causes of failure of the PTT, including: (1) im-
pingement in the osteofibrous groove, (2) compression by the flexor retinaculum,
(3) presence of an accessory navicular bone, (4) weakening in the area of inser-
tion, (5) hypovascularization of the tendon at the level of the medial malleolus
[25], (6) inflammatory arthropathy, (7) acute traumatism [26], (8) corticosteroid
injection, and (9) chronic mechanical overload [27,28].
A dysfunction of the tendon of the posterior tibialis muscle causes an inver-
sion of the rearfoot which blocks the transverse tarsal joint (Chopart’s joint) during
the middle and late phases of gait. As a result, the contractive force of the triceps
surae must act through the talonavicular joint instead of the metatarsal heads. In
this situation, the head of the talus acts repeatedly on the spring ligament. A
lengthening or rupture of this ligament enables the talus to carry out plantar flexion
with a valgus alignment of the os calcis which results in an adult acquired flat-
foot deformity [8,29–34].

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2318
Accessory navicular bone
At the posterior margin of the posteromedial navicular tuberosity, a supernu-
merary ossiculum, that serves as insertion for the PTT, along with the navicular
bone, is found occasionally [35].
Initially described by Bahuin in 1605, the accessory navicular bone is
considered to be a radiographic and anatomical variant present in 4% to 21% of
the population [36], although the highest rates are found in patients who have flat
foot (19%) [37]. It is more frequent in women and is visible radiographically from
the age of 9 years [35].
Depending on the accessory navicular bone’s morphology and position, as
well as on whether there is synchondrosis with the navicular bone, Weitch in
1978, divided it into three types [38]:
Type I. Os tibiale externum, naviculare secundarium or accessory navicular.
This type represents 30% of the total. Located within the tendon of the posterior
tibialis muscle, this sesamoid bone presents an ovoid morphology of about 2 mm
to 3 mm (Fig. 17).
Fig. 17. Posteroanterior (PA) radiograph of bilateral type I accessory navicular (arrows).

Fig. 18. PA radiograph of type III accessory navicular (arrows).
P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 19
Type II. Prehallux or bifurcate hallux. This type is found in 50% to 60% of
cases and shows a triangular morphology of about 12 mm at its major axis.
Formed from a secondary ossification center of the navicular bone, it is found
joined to this bone by fibrocartilage or hyaline cartilage [39,40], which creates
a synchondrosis.
Type III. The accessory navicular bone is a prominent navicular tuberosity
known as a cornuated navicular [41] and is considered to be the last stage in the
fusion of type II (Fig. 18) [36]. This bone is considered to be an asymptomatic
variant, although when it suffers trauma, it can cause painful symptoms.
Fig. 19. Lateral radiograph of type II accessory navicular (arrow).

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2320
In 1986, Sella et al [40] divided type II into two subtypes (IIa and IIb)
depending on its localization with respect to the navicular and on the angle formed
between the synchondrosis and the lateral process of the talus (the SOT angle). In
subtype IIa, the SOT angle is an average of 56.3� and the ossiculum is located
dorsally. In subtype IIb, the SOT angle is much more acute and the ossiculum is
situated more plantarly (Figs. 19 and 20). When the fibrocartilage of the
synchondrosis of types IIa and IIb is subjected to tension or compressive forces,
it can present histologic findings that are similar to bone fractures [40,41].
Radiographically, the changes are imperceptible and require 99mTc (99mtechnetium
methylene diphosphonate) in follow-up testing to detect the increase in activity.
Occasionally, surgery is necessary in symptomatic cases of this supernumerary
bone when orthopedic treatments have failed [36,42]. The presence of an
accessory navicular has been associated with several pathologies, such as flatfoot
[43,44], or, more recently, hallux limitus [45].
Fig. 20. PA radiograph of type II accessory navicular (arrows).

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 21
Vascularization of the navicular bone
The navicular bone has vascular branches at its dorsal and plantar aspects, as
well as its tuberosity. The dorsal vascularization arises from a vascular branch of
the dorsalis pedis artery which, upon crossing the dorsum of the navicular, divides
into three to five branches [46]. Branches that arise directly from the dorsalis pedis
artery also are found occasionally. The plantar vascularization depends on vessels
that arise from the medial plantar artery, whereas the navicular tuberosity receives
vessels from an anastomotic network that is formed by the dorsalis pedis and
medial plantar arteries. This arterial network provides a rich vascularization to the
medial and lateral portions of the navicular, although the central portion of the
bone shows a lower level of vascularization [47].
As described by Zchakaja [48], with increasing age, there is a decrease in the
number of supplementary arteries that supply the navicular bone. This may be a
cause of osteonecrosis or stress fractures at the middle third of this bone, as
described initially by Torg et al [47] and, later, by other investigators [49–53].
Acknowledgments
We would like to thank to Joan Angel Clavero, MD from Diagnosis Medica
(Barcelona, Spain) for his support and the use of the MR and CT images that
appear in this article.
References
[1] Kamina P. Anatomie. Introduction a la clinique. Osteologie des membres (Anatomy: introduction
to the clinic, osteology of limbs). Paris: Editeur Maloine; 1986 [in French].
[2] Myerson MS. Foot and ankle disorders, vol 2. Philadelphia: W.B. Saunders Company; 2000.
[3] Manners-Smith T. A study of the navicular in the human and anthropoid foot. J Anat Physiol
1907;41:261.
[4] Sarrafian SK. Anatomy of the foot and ankle. Descriptive, topographic and functional. 2nd
edition. Philadelphia: J.B. Lippincott Company; 1993.
[5] Dwight R. Os intercuneiforme tarsi, os paracuneiforme tarsi, calcaneus secundarius. Anat Anz
1902;20:465.
[6] Dwight T. Variations of the bones of the hands and feet: a clinical atlas. Philadelphia: JB
Lippincott; 1907.
[7] Pisani G. La coxa pedis ed i movimenti torsionali astragalici (The coxa pedis and the torsional
movement of the talus (in Italian)). Chir Piede 1988;12:35–44.
[8] Testut L, Jacob O. 9th edition. Tratado de anatomıa humana (Human anatomy treaty), vol 1.
Barcelona (Spain): Salvat Editores, S.A.; 1985.
[9] Yao L, Gentili A, Cracchiolo A. MR imaging findings in spring ligament insufficiency. Skeletal
Radiol 1999;28:245–50.
[10] Rule J, Yao L, Seeger LL. Spring ligament of the ankle: normal MR anatomy. AJR 1993;
161:1241–4.
[11] Hardy RH. Observations on the structure and properties of the calcaneonavicular ligament in
man. J Anat 1951;85:135–9.
[12] Borton DC, Saxby TS. Tear of the plantar calcaneonavicular (spring) ligament causing flatfoot: a
case report. J Bone Joint Surg Br 1997;79B:641–3.

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–2322
[13] Chen JP, Allen AM. MR diagnosis of traumatic tear of the spring ligament in a pole vaulter.
Skeletal Radiol 1997;26:310–2.
[14] Weitbreck J. Syndesmology. Philadelphia: WB Saunder; 1969.
[15] De Palma L, Santucci A, Ventura A, et al. Anatomy and embryology of the talocalcaneal joint.
Foot Ankle Surg 2003;9:7–18.
[16] Davis WH, Sobel M, DiCarlo EF, et al. Gross, histological, and microvascular anatomy and
biomechanical testing of the spring ligament complex. Foot Ankle 1996;17:95–102.
[17] Henle J. Handbuch der systematischen anatomie des menschen (Handbook of the human sys-
tematic anatomy), vol 3. Braunschweig (Germany): Von Friedrich Vieweg und John; 1868.
[18] Lane AS. The causation, pathology and physiology of several of the deformities wich develop
during young life. Guys Hosp Rep 1887;44:254.
[19] Kokturk C. Remarques sur le ligament de Chopart (lig. Bifurcatum) [Remarks on Chopart’s
ligament (lig. bifurcatum)]. Comptes-Rendus Assoc Anat 1957;44:380 [in French].
[20] Barclay-Smith E. The astragalo-calcaneo-navicular joint. J Anat Physiol 1896;30:390.
[21] Hovelacque A, Sourdin A. Note au sujet de quelques ligaments de l’articulation medio-tarsienne
[Note on the subject of some ligements of mediotrsal articulation]. Ann Anat Pathol Anat
Normal 1933;10:469.
[22] Jones FW. Structure and function as seen in the foot. London: Bailliere, Tindall & Cox; 1944.
[23] Martin BF. Observations on the muscles and tendons of the medial aspect of the sole of the foot.
J Anat 1964;98:437–53.
[24] Kitaoka HB, Luo ZP, An K-A. Effect of the posterior tibial tendon on the arch of the foot during
simulated weightbearing: biomechanical analysis. Foot Ankle 1997;18:43–6.
[25] Frey C, Shereff M, Greenidge N. Vascularity of the posterior tibial tendon. J Bone Joint Surg Am
1990;72A:884–8.
[26] Marks RM, Schon JC. Posttraumatic posterior tibialis tendon insertional elongation with incom-
petency: a case report. Foot Ankle 1998;19:180–3.
[27] Rosenberg ZS. Chronic rupture of the posterior tibial tendon. Magn Reson Imaging Clin North
Am 1994;2:279–86.
[28] Pomeroy GC, Pike RH, Beals TC, et al. Acquired flatfoot in adults due to dysfunction of the
posterior tibial tendon. J Bone Joint Surg Am 1999;81-A:1173–82.
[29] Jahss MH. Tendons disorders of the foot and ankle. In: Jahss MH, editor. Disorders of the foot
& ankle: medical & surgical management. 2nd edition. Philadelphia: W.B. Saunders; 1991.
p. 1321–71.
[30] Mann RA. Flatfoot in adults. In: Coughlin MJ, Mann RA, editors. Surgery of the foot & ankle.
6th edition. St. Louis (MO): Mosby-Year Book; 1999. p. 733–67.
[31] Funk DA, Cass JR, Johnson KA. Acquired adult flatfoot secondary to posterior tibial tendon
pathology. J Bone Joint Surg Am 1986;68A:95–102.
[32] Goldner JL, Geats PK, Bassett FH, et al. Progressive talipes equinovalgus due to trauma or
degeneration of the posterior tibial tendon and medial plantar ligaments. Orthop Clin North
America 1974;5:39–49.
[33] Balen PF, Helms CA. Association of posterior tibial tendon injury with spring ligament injury,
sinus tarsi abnormality, and plantar fasciitis on MR imaging. AJR 2001;176:1137–43.
[34] Gazdag AR, Cracchiolo A. Rupture of the posterior tibial tendon. Evaluation of injury of the
spring ligament and clinical assessment of tendon transfer and ligament repair. J Bone Joint Surg
Am 1997;79A:675–81.
[35] Sever JW. Clinical importance of the os tibiale externum, or accessory tarsal scaphoid. JAMA
1927;89:359–61.
[36] Miller TT, Staron RB, Feldman F, et al. The symptomatic accessory tarsal navicular bone:
assessment with MR imaging. Radiology 1995;195:849–53.
[37] Wood WA, Spencer AM. Incidence of os tibiale externum in clinical pes planus. JAPA
1970;60:276–7.
[38] Weitch JM. Evaluation of the Kidner procedure in treatment of syntomatic accessory tarsal
scaphoid. Clin Orthop 1978;131:210–3.

P. Golano et al / Foot Ankle Clin N Am 9 (2004) 1–23 23
[39] Zadek I, Gold AM. The accessory tarsal scaphoid. J Bone Joint Surg Am 1948;30:957.
[40] Lawson JP, Ogden JA, Sella EJ, et al. The painful accessory navicular. Skeletal Radiol 1984;12:
250–62.
[41] Sella EJ, Lawson JP, Ogden JA. The accessory navicular synchondrosis. Clin Orthop 1986;
209:280–5.
[42] Ray S, Goldberg VM. Surgical treatment of the accessory navicular. Clin Orthop Rel Res 1983;
177:61–6.
[43] Kidner FC. The prehallux (accesorie scaphoid), in its relation with flat foot. J Bone Joint Surg
Am 1929;11A:831–7.
[44] Hatoff A. Bipartite navicular bone as a cause of flat foot. Am J Dis Child 1950;80:991.
[45] Lee Evans RD, Averett R. The association of hallux limitus with the accessory navicular. J Am
Podiatr Med Assoc 2002;92:359–65.
[46] Velluda C. Sur la vascularisation du scaphoid du tarse [[On the vascularization of the tarsal
scaphoid]]. Ann Anat Pathol 1928;5:1016 [in French].
[47] Torg J, Pavlov H, Cooley L, et al. Stress fractures of the tarsal navicular. J Bone Joint Surg Am
1982;64A:700–12.
[48] Zchakaja MJ. Blutversorgung der knochen des fusses (Vascularisation of the feb bones) (ossa
pedis). Fortschr Gebiete Rontgenol 1932;45:160.
[49] Fitch K, Blackwell J, Gilmour W. Operation for non-union of stress fracture of the tarsal
navicular. J Bone Joint Surg Br 1989;71B:105–10.
[50] Haller J, Sartoris DJ, Resnick D, et al. Spontaneous osteonecrosis of the tarsal navicular in
adults. AJR 1988;151:355–8.
[51] Kiss ZS, Khan KM, Fuller PJ. Stress fractures of the tarsal navicular bone: CT findings in 55
cases. AJR 1993;160:111–5.
[52] Gunal I, Yorukoglu K. Osteonecrosis of the accessory navicular bone. Arch Orthop Trauma Surg
2001;121:546–7.
[53] Coughlin MJ. Tarsal navicular stress fractures. Tech Foot Ankle Surg 2002;1:112–22.