for immediate relief of muscular pain, tension, & … · from sweden in acupuncture and physio...
TRANSCRIPT
Advanced Manual Techniques UsingTRIGGER-& ACCUPRESSURE POINTS
For Immediate Relief ofMUSCULAR PAIN, TENSION, & DYSFUNCTION
VOLUME IUPPER EXTREMITIES
BYTORBJORN M. HANSON, A.c., MANUAL THERAPIST
© T. HANSON 2012

TORBJORN HANSON, A.c. Kinesiologist & Muscle Therapist Torbjorn has 28 years of clinical experience in manual therapy for pain or dysfunction in muscles, tendons, ligaments and joints. He holds a degree from Sweden in Acupuncture and Physio Therapy, and has specialized in Trigger Point Therapy, Acupressure, Kinesiology and Sports Medicine. For 5 years he wrote a column and answered reader questions on sports injuries in B&K Sports Magazine, Scandinavia’s largest fitness publication. In 1994 Torbjorn founded Sports Performance Therapy Center, with a vision to bring together diversified therapies that would get patients Better, Faster. This state of the art physical therapy clinic is located inside Club Sport of Pleasanton, 184,000 square foot athletic club. He is also the founder of POSTU-Rx, a computer software program developed to prescribe custom made exercises, to stretch short muscles, and to strengthen elongated muscles. This program brings a new concept to sports medicine. His extensive work with professional and recreational athletes has led to the development of HandsOn Muscle Therapy. A cutting edge approach to Injury Rehabilitation and Prevention as well as Performance Enhancement. Torjorn has been teaching his techniques to therapists and physicians throughout Europe. His hands-on work is followed by a long record of success and gives instant relief and functional improvement in muscles/joint pain syndrome and sports injuries. His unique use of manual muscle testing provides feedback that assures specific therapy for each individual and every injury.

HansOn Muscle Therapy H.M.T. is an advanced manual technique using trigger and acupressure points for immediate relief of muscular pain, tension and dysfunction. H.M.T. is a diversified system that integrates Feedback from postural evaluation, range of motion assessment and specific muscle testing to pinpoint areas of myofascial tension. Muscular Imbalance Sprains, strains or micro tearing due to overuse or trauma of certain muscles leads to an accumulation of tension, i.e. muscle shortening and adhesions. Anytime there is muscle shortening, and subsequent muscle lengthening of the antagonistic muscles, there is a MUSCULAR IMBALANCE. In other words, the body is out of ALIGNMENT. The core theory in H.M.T. is that muscular imbalance is the cause of injuries and decreased performance. Muscle shortening causes: Decreased range of motion Postural imbalances Change joint positions with decreased joint space Decreased vascular circulation Inhibition of lymphatic drainage Decreased strength Friction, pressure, compression and excessive pulling over time leads to dysfunction, inflammation and pain. This pain is caused by soft tissue damage or nerve entrapment and ultimately leads to neuropathy, joint pathology and joint degeneration. Reading Body Feedback H.M.T. uses postural and range of motion assessments together with manual testing of individual muscles, the recognition of referred pain patterns, and acupressure meridian distribution to determine primary muscles with the most accumulated tension.
1

Circuit Breakers Accumulation of tension in muscles, fascia and tendons manifest as hypersensitive myofascial reflex points know as trigger points or acupressure points. Those reflex points act as circuit breakers and when overloaded with excessive tension can give rise to local or referred pain. Trigger or acupressure points are activated directly by acute overload, overwork, fatigue or direct trauma to the muscle they are located in. Those reflex points can also be activated indirectly by other reflex points, visceral disease, joint dysfunction, or emotional distress. Once a reflex point is activated, repeated muscular stress of a lesser degree can activate pain in the reference zone, especially when the muscle becomes fatigued. Research shows that a change in electrical resistance (3) and temperature (4) can be measured at the dermal location of a reflex point. This can be confirmed with ohm meters and thermograms. “Getting to the Point” There are approximately 700 acupressure points on the human body and all skeletal muscles can develop multiple trigger points. The acupressure points have definite anatomical locations while the trigger point locations are not fixed. The proper point to select for therapy is not always located at the site of pain, but rather at the site of maximal accumulated tension. Due to the number of points possibly related too an injury, the therapeutic skill lies in the ability to select the right point(s) for each specific injury. H.M.T. teaches the relationship between different reflex points, referred pain patterns and acupuncture meridian distribution. H.M.T. utilizes patient muscle feedback by the unique use of indicator muscle testing in how to select the primary point(s) for each individual condition. This muscle feedback takes away the “guesswork” or the “hit or miss” approach in the selection of appropriate reflex points for a specific condition. Re-setting The Circuit/Releasing the Tension Once a primary reflex point has been localized, it should be released of its excessive tension with deep friction massage. Deep intermittent digital pressure to a reflex point in a specific direction causes a form of “depolarization”. Digital pressure on a primary reflex point will elicit local and/or referred pain. Complete release of tension with digital pressure to a reflex point will cause all elicit pain to completely disappear.
2
Proper release of tension in a reflex point will immediately abolish readings of changed electrical resistance. Inactivation of the reflex point allows associated muscle(s) to return to proper tone and hence restore muscular balance. Releasing tension to acupressure or trigger points in shortened muscles is very effective in reducing joint pressure and restoring range of motion. Lasting results will be achieved in eliminating local or referred pain caused by muscle shortening. This also improves vascularity and lymphatic drainage which stimulates the body’s natural self-curative abilities. Due to somatovisceral effects, a release of a hypersensitive myofascial reflex point can improve tension related visceral ailments and provide emotional release. Some theories suggest that digital pressure applied to acupressure points may also stimulate the nervous system to release neuro-hormones (such as endorphins). Research has documented that this is the case with acupressure (5). This would explain the analgesic effect often experienced with the release of an acupressure point. The analgesic effect is generally short lasting in cases of joint or nerve pathology. In other cases however, endorphin release may break the pain cycle and promote lasting or permanent relief. References:
(1) Travell J. Bigelow NH: Referred somatic pain does not follow a simple “segmental” pattern. Fed Proc 5:106, 1046.
(2) Travell J. & Simons D: Myofascial pain and dysfunction. The trigger point manual,
upper extremities. Vol. 1, pg. 15, 1983. (3) Sola AE and Williams RL: Myofascial pain syndromes. Neurol 6:91-95, 1956. (4) Fisher AA: Thermography and pain. Arch Phys Med Rehabil 62:542, 1981.
(5) Mayer FJ, Price DD, Barber J, et al: Acupuncture analgesia: Evidence for activation
of pain inhibitory system as a mechanism of action. In advances in pain research and therapy, edited by J.J. Bonica, D. Albe-fessard, Vol 1 Raven press, New York 1976 (pp. 751-754).
3
Objective #1 A) Find and relieve muscular tension B) Immediate pain relief C) Restore normal range of motion, posture and strength. Muscular tension will cause muscular imbalance with uneven wear and tear to muscles, tendons and ligaments thus causing tissue damage with pain and inflammation. Muscular tension will cause a blockage of circulation with a relative oxygen deprivation as well as inhibited drainage of lymphatic waste products thus becoming the cause of muscle contraction, spasm, inflammation, pain and swelling. Excessive muscle tension can trap and pinch nerves thereby causing radiating pain patterns and neuropathy. Muscular tension results in muscular imbalance with altered posture. This misalignment will alter joint position and space, thus causing joint pathology and eventual joint degeneration. Muscular tension results in muscular imbalance with inhibited range of motion, decreased function, strength and endurance.
4
Objective #2 A) Find the underlying cause of muscular tension B) Educate to prevent recurrence of symptoms Physical cause: Direct trauma
- Impact - Sudden uncontrolled body movement
= Immediate tissue damage and tension. Microtrauma
- Repetitive movement patterns - Improper movement patterns - Poor posture - Poor sleeping position - Improper pedal foundation
= Accumulative structural stress causing tension and eventual tissue damage. Mental / Emotional cause:
- ongoing mental / emotional stress - past unresolved mental / emotional stress
= Accumulative emotional stress causing chronic muscular tension and eventual tissue damage. Nutritional / Chemical cause:
- Nutritional deficiencies - Dehydration - Toxic conditions
= Lymphatic congestion and muscular tension Environmental cause:
- Allergies = Lymphatic congestion with muscular tension.
5

Hanson Muscle Therapy
HMT Synopsis
Posture and Range of motion evaluation is used together with manual testing of individual muscles and recognition of referred pain patterns to localize muscles with accumulated tension. Indicator muscle testing is used as feedback to pinpoint the exact location of active trigger points and acupoints in muscles with accumulated tension. Digital intermittent friction massage is used to relieve tension and inactivate those points. HansOn Muscle Therapy will:
A) Relieve pain and tension immediately. B) Restore muscular balance and joint integrity. C) Improve vascularity and lymphatic drainage to
injured tissue which will initiate healing.
6
How to LOCALIZE MUSCLES with ACCUMULATED TENSION Evaluate posture of pain area Use form A:1-3 for Anterior, Posterior and Lateral view Posture Evaluation. Reference; “Postu-Rx Manual for Muscle Imbalance” or DVD to establish standard for normal posture. Each postural imbalance indicates which muscles are tense / shortened or elongated. Evaluate range of motion of the joints proximal to the pain area. Use form B:1 for the upper extremities, form B:2 for lower extremities and spine to establish standard for normal range of motion. Reference; “Postu-Rx Manual for Muscular Imbalance” or DVD to establish standards for normal range of motion. Each range of motion imbalance indicates which muscles are tens / shortened or elongated. Perform manual muscle testing of muscles in pain area Use form C:1, for testing upper extremity muscles #1-35 or form C:2 for lower extremity and spine muscles #36-72. Each muscle will test either normal, hypotonic/weak/elongated, or hypertonic/tense/shortened. Reference; HMT Manual Muscle Testing manual I (upper extremity, muscles # 1-35), and II (lower extremity and spine, muscles #36-72). “Muscle Testing and Function” by Kendall or “Applied Kinesiology, Synopsis” by Walther, can also be used. Ask the Patient where the pain is felt and fill in the appropriate pain zones Use form D:1, For the patient to indicate pain patterns on anterior, posterior or lateral illustration.
7
How to prioritize which muscle to treat first
Postural Evaluation, Range of Motion Assessment, Manual Muscle Testing, Referred Pain Patterns and Acu-Meridians is what determines which muscles have an accumulation of tension and harbor active trigger points or AcuPoints. Use the Priority sheet (Form E) to determine which muscle(s) are indicated the most.
Example I:A patient presents with a right shoulder promlem.
Postural Exam:
Anterior view show a medially rotated right arm. See exam form A-1 on page #11This indicares that the muscles that medially rotate the arms are relatively shorter (morecontracted) than the muscies that laterally rotate the arms. This also indicates that the muscles that laterally rotate the arms are relatively elongated compared to the musclesthat medially rotate the arms.
Shortened muscles Elongated musclesMedial rotators of arm Lateral rotators of arm#8 Pectoralis Major Clavicular #16 Infraspinatus#9 Pectoralis Major Sternal #17 Teres Minor#10 Latissimus Dorsi #20 Deltoid Posterior#12 Teres Major#14 Subscapularis#18 Deltoid Anterior Posterior view shows and elevated right scapula. See exam form A-2 on page #12This indicates that the muscles that elevate the scapula are shortened and the muscles that depress the scapula are elongated Shortened muscles Elongated muscles#1 Trapezius Upper #3 Trapezius Lower#5 Levator Scapulae (#10 Latissimus Dorsi)#6 Rhomboids#7 Pectoralis Minor
8
Lateral view shows a right anterior humeral head. See exam form A-3 on page #13This indicates that the muscles that pull the humeral head anterior are shortened, and the musclesthat pull the humeral head posterior are elongated.Shortened Muscles Elongated MusclesPull humeral head anterior Humeral head posterior#1 Trapezius Upper #2 Trapezius Middle#4 Serratus Anterior #3 Trapezius Lower#7 Pectoralis Minor #20 Deltoid Posterior#8 Pectoralis Major Clavicular#9 Pectoralis Major Sternal#18 Deltoid Anterior#27 Coracobrachialis
Mark form E:1 with the muscles that are shortened and elongated in the Postural Evaluation.See example page 23.
9

PAIN
MA
PP
ING
Hav
e p
atie
nt
use
a c
olo
red
pen
. “St
rip
e” z
on
es w
ith
mo
der
ate
pai
n.
“Ch
ecke
r” z
on
es w
ith
sev
ere
pai
n.
D1
PATI
ENT’
S N
AM
E: _
____
____
____
____
____
____
____
____
____
____
____
____
_ PAT
IEN
T ID
NO
: __
____
____
____
____
__JO
E D
EM
O
123
-45
-67
89
10
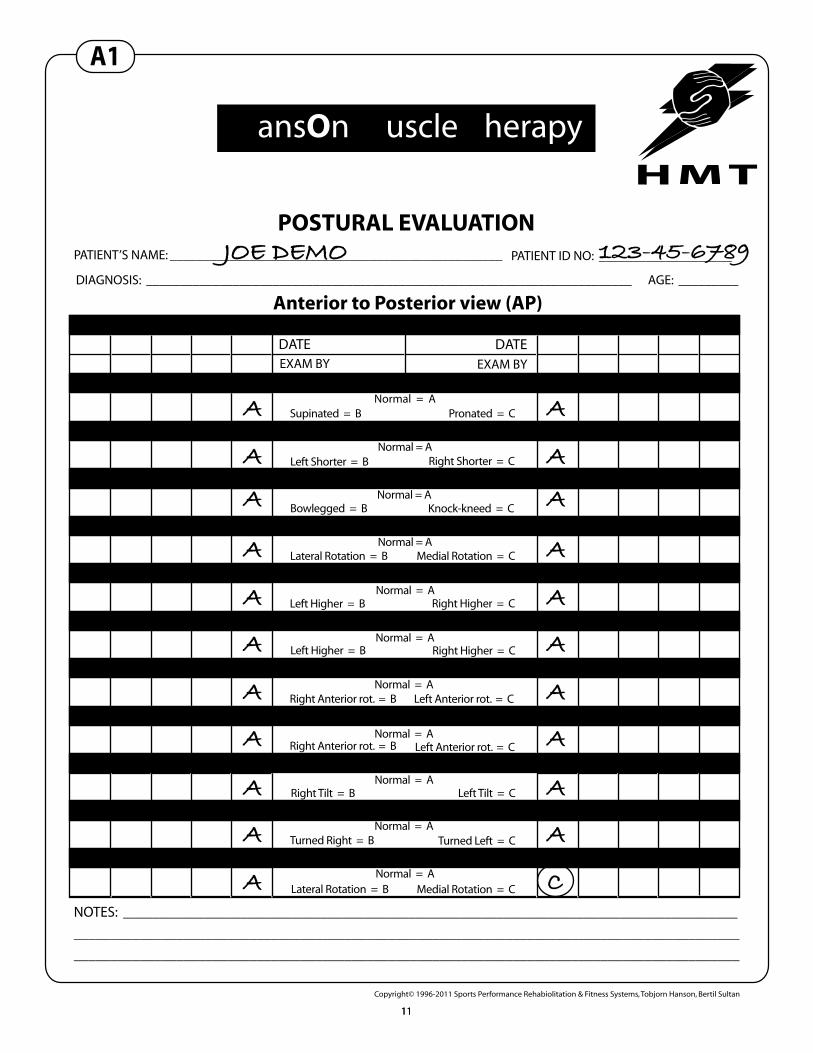
POSTURAL EVALUATIONPATIENT’S NAME: __________________________________________________ PATIENT ID NO: ____________________
DIAGNOSIS: _________________________________________________________________________ AGE: _________
Anterior to Posterior view (AP)LEFT RIGHT
DATE DATEEXAM BY EXAM BY
NO. 1:1 NO. 1:2
NO. 1:6
NO. 1:9
NO. 1:10NO. 1:10
NO. 1:10NO. 1:10
NO. 1:13 NO. 1:14
NO. 1:12 NO. 1:12
NO. 1:11 NO. 1:11
NO. 1:9
NO. 1:8 NO. 1:8
NO. 1:7
NO. 1:5NO. 1:4
NO. 1:3 NO. 1:3
1. FEET
2. LEG LENGTH
3. KNEES
4. FEMUR
5. HIPS
6. SHOULDERS
7A. TORSO ROTATION
7B. HIP ROTATION
8A. HEAD TILT
8B. HEAD ROTATION
9. ARMS
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Supinated = B Pronated = C
Left Shorter = B Right Shorter = C
Bowlegged = B Knock-kneed = C
Lateral Rotation = B Medial Rotation = C
Left Higher = B Right Higher = C
Right Higher = CLeft Higher = B
Right Anterior rot. = B
Right Anterior rot. = B
Left Anterior rot. = C
Left Anterior rot. = C
Right Tilt = B Left Tilt = C
Turned Right = B Turned Left = C
Lateral Rotation = B Medial Rotation = C
NOTES: ____________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Copyright© 1996-2011 Sports Performance Rehabiolitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
JOE DEMO 123-45-6789
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
C
HansOn Muscle Therapy
A1
1111
POSTURAL EVALUATIONPATIENT’S NAME: __________________________________________________ PATIENT ID NO: ____________________
DIAGNOSIS: _________________________________________________________________________ AGE: _________
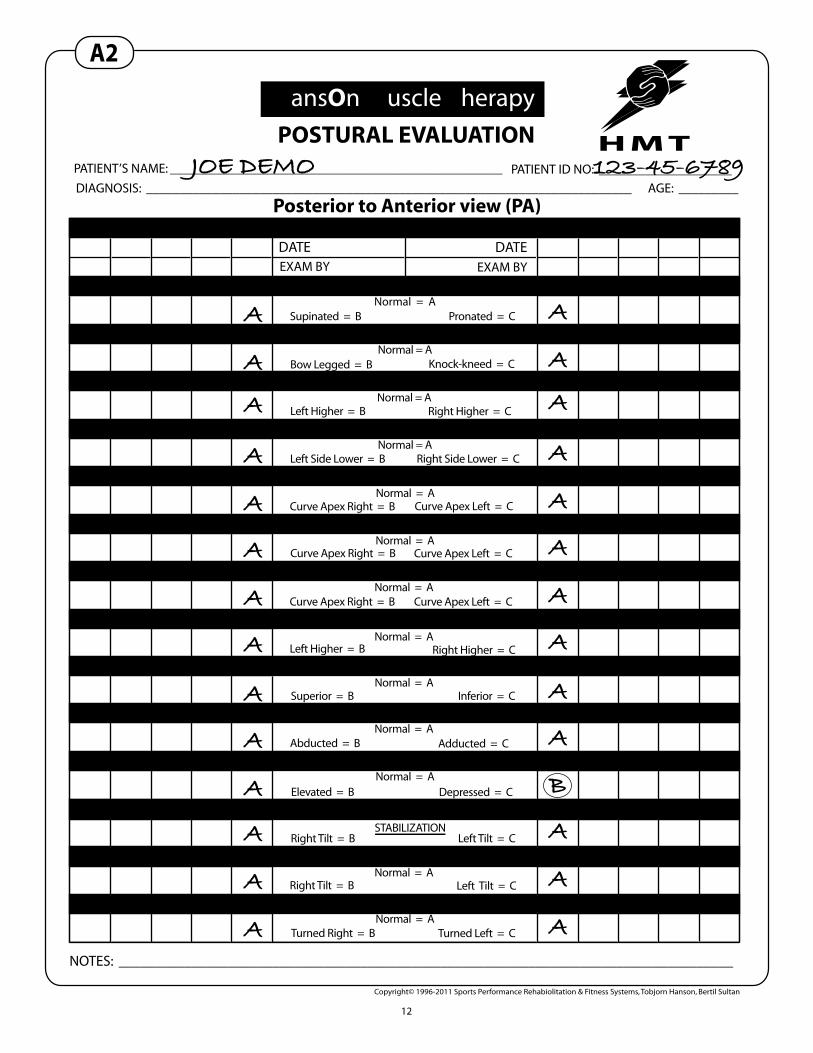
Posterior to Anterior view (PA)LEFT RIGHT
DATE DATEEXAM BY EXAM BY
NOTES: ____________________________________________________________________________________
Copyright© 1996-2011 Sports Performance Rehabiolitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
HansOn Muscle Therapy
NO. 2:1 NO. 2:2
NO. 2:3
NO. 2:5
NO. 2:6NO. 2:6
NO. 1:9NO. 1:9
NO. 2:9 NO. 2:13
NO. 2:8 NO. 2:12
NO. 2:7 NO. 2:11
NO. 2:5
NO. 2:4 NO. 2:4
NO. 2:3
NO. 1:8NO. 1:8
NO. 1:4 NO. 1:5
1. ACHILLES TENDON
2. KNEES
3. HIPS
4. RIB CAGE
5A. ENTIRE SPINE CURVATURE
5B. THORACIC SCOLIOSIS
5C. LUMBER SCOLIOSIS
6. SHOULDERS
7A. SCAPULA ROTATION
7B. SCAPULA HOR. LEVEL
7C. SCAPULA VERT. LEVEL
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Normal = A
Supinated = B Pronated = C
Bow Legged = B Knock-kneed = C
Left Higher = B Right Higher = C
Left Side Lower = B Right Side Lower = C
Curve Apex Right = B Curve Apex Left = C
Curve Apex Left = CCurve Apex Right = B
Curve Apex Right = B
Left Higher = B
Curve Apex Left = C
Right Higher = C
Superior = B Inferior = C
Abducted = B Adducted = C
Elevated = B Depressed = C
NO. 1:12 NO. 1:12
NO. 1:11 NO. 1:11
NO. 2:10 NO. 2:147D. SCAPULA THORACIC
8A. HEAD TILT
8B. HEAD ROTATIONNormal = A
Normal = A
STABILIZATIONRight Tilt = B Left Tilt = C
Right Tilt = B Left Tilt = C
Turned Right = B Turned Left = C
A2
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
A
B
A
A
A
JOE DEMO 123-45-6789
12

JOE DEMO 123-45-6789
A
A
A
A
A
A
A
A
A
A
A
A
A
C
POSTURAL EVALUATION
PATIENT’S NAME: __________________________________________________ PATIENT ID NO: ____________________
DIAGNOSIS: _________________________________________________________________________ AGE: _________
Lateral ViewLEFT RIGHT
DATE DATEEXAM BY EXAM BY
NO. 3:1 NO. 3:2
NO. 3:5
NO. 3:7
NO. 3:10NO. 3:9
NO. 3:8
NO. 3:6 NO. 3:6
NO. 3:5
NO. 3:4NO. 3:4
NO. 3:3 NO. 3:3
1. KNEES
2. PELVIS & LUMBER SPINE
3. THORAX & HEAD POSITION
4. ABDOMEN
5. HEAD TILT
6. HUMERAL HEAD
7A. ELBOW FLEXION
Normal = A
Normal = A
Normal = A
Normal = A
Normal / flat = A
Normal = A
Normal = AHyperextended = B Flexed = C
Posterior tilt / lack of lumber curve = BAnterior tilt / excess lordosis = C
Excess kyphosis / head forward = BLack of thoracic curve / head posterior = C
Protruding = B
Posterior tilt / excess lordosis = BAnterior tilt / straight neck = C
Anterior = CPosterior = B
Excessive = B Deficient = C
NOTES: ____________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Copyright© 1996-2011 Sports Performance Rehabiolitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
HansOn Muscle Therapy
A3
1313
Range of Motion (ROM) Exam
Upper extremity ROM show limited and painful abduction on the right. See exam form B-1 on page #16This indicates The muscles responsible for the antagonistic (opposite) range of motion, theadductors, are shortened and therefore limiting abduction. The muscles responsible for theabduction are relatively elongated. Shortened muscles Elongated musclesShoulder adductors Shoulder abductors#8 Pectoralis Major Clavicular #11 Supraspinatus#9 Pectoralis Major Sternal #18 Deltoid Anterior#10 Latissimus Dorsi #19 Deltoid Middle #12 Teres Major #20 Deltoid Posterior#24 Triceps Long Head#27 Coracobrachialis
Upper Extremity ROM shows limited and painful lateral rotation (with 90 degreesof abduction) on the right. See exam form B-1 on page #16This inidcates that the medial rotators of the arm are shortened and the lateral rotators are elongated which would limit lateral rotation.Shortened muscles Elongated musclesMedial rotators Lateral rotators#8 Pectoralis Major Clavicular #16 Infraspinatus#9 Pectoralis Major Sternal #17 Teres Minor#10 Latissimus Dorsi #20 Deltoid Posterior #12 Teres Major #14 Subscapularis#18 Deltoid Anterior
14
Cervical ROM shows that lateral flexion to the left is limited. See exam form B-3 on page #17This indicates that the muscles responsible for lateral flexion to the left are elongated.Muscles responsible for the antagonistic (opposite) movement, lateral flexion to the rightare shortened.Shortened muscles Elongated musclesRight lateral Flexors Left lateral flexors#1 Trapezius Upper #1 Trapezius Upper#36 Sternocleidomastoid #36 Sternocleidomastoid#37 Scalenes #37 Scalenes #39 Neck Extensors #39 Neck Extensors
Mark form E:1 with the muscles that are tested shortened and elongated in the Range OfMotion Assessment. See example page 23.
15
PATIENT'S NAME: __________________________________________________
DIAGNOSIS : _________________________________________________________________________ _________
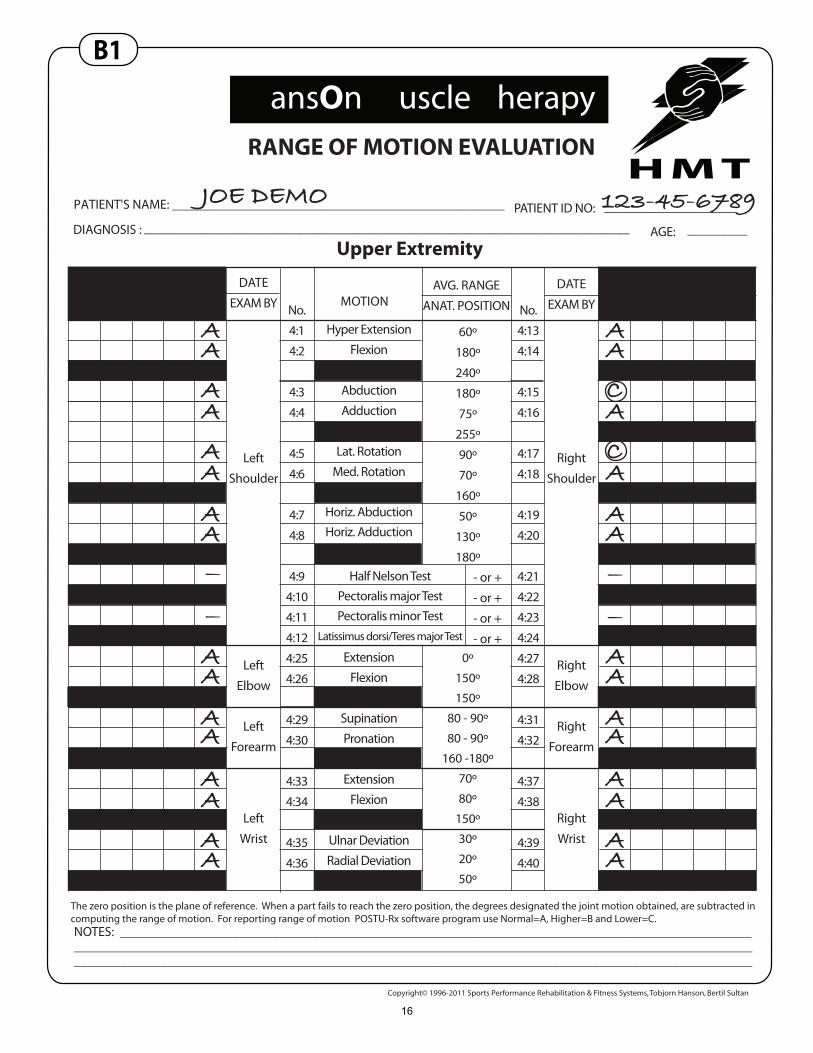
Upper Extremity
JOE DEMO 123-45-6789
RANGE OF MOTION EVALUATION
ExtensionFlexionRange
SupinationPronation
RangeExtension
FlexionRange
Ulnar DeviationRadial Deviation
Range
Hyper Extension
Flexion
Range
Abduction
Adduction
Range
Lat. Rotation
Med. Rotation
RangeHoriz. AbductionHoriz. Adduction
Range
No.
4:1
4:2
4:3
4:4
4:5
4:6
4:7
4:8
4:9
4:10
4:11
4:12
4:25
4:26
4:29
4:30
4:33
4:34
4:35
4:36
No.
4:13
4:14
4:15
4:16
4:17
4:18
4:19
4:20
4:21
4:22
4:23
4:24
4:27
4:28
4:31
4:32
4:37
4:38
4:39
4:40
DATE
EXAM BYDATE
EXAM BYMOTIONAVG. RANGE
ANAT. POSITION
Right
Shoulder
Right
Elbow
Right
Forearm
Right
Wrist
Left
Shoulder
Left
Elbow
Left
Forearm
Left
Wrist
60º
180º
240º
180º
75º
255º
90º
70º
160º
50º
130º
180º
0º
150º
150º
80 - 90º
80 - 90º
160 -180º
70º
80º
150º
30º
20º
50º
- or +
- or +
- or +
- or +
The zero position is the plane of reference. When a part fails to reach the zero position, the degrees designated the joint motion obtained, are subtracted incomputing the range of motion. For reporting range of motion POSTU-Rx software program use Normal=A, Higher=B and Lower=C.NOTES: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Copyright© 1996-2011 Sports Performance Rehabilitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
____________________
HansOn Muscle Therapy
B1
Half Nelson TestPectoralis major TestPectoralis minor Test
Latissimus dorsi/Teres major Test
AGE:
PATIENT ID NO:
AA
AA
AA
AA
AA
AA
AA
AA
AA
CA
AC
AA
----
----
AA
AA
AA
AA
16

PATIENT'S NAME: __________________________________________________ PATIENT ID NO:
DIAGNOSIS : _________________________________________________________________________ AGE: _________
SPINE
RANGE OF MOTION EVALUATION
The zero position is the plane of reference. When a part fails to reach the zero position, the degrees designated the joint motion obtained, are subtracted incomputing the range of motion. For reporting range of motion POSTU-Rx software program use Normal=A, Higher=B and Lower=C.
NOTES: _______________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
Copyright© 1996-2011 Sports Performance Rehabilitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
____________________
HansOn Muscle Therapy
B3
No.
6:1
6:2
6:3
6:4
6:5
6:6
6:7
6:8
6:9
6:10
6:11
6:12
DATE
EXAM BYMOTION AVG.RANGE
45º
45º
90º
45º
45º
90º
70º
70º
140º
80º
20-30º
100-110º
35º
35º
70º
45º
45º
90º
FlexionExtension
RangeLateral bending left
Lateral bending rightRange
Rotation/Turning leftRotation/Turning right
RangeFlexion
ExtensionRange
Lateral bending leftLateral bending right
RangeAnterior rotation left
Anterior rotation rightRange
Cervical
Spine
Thoracic &Lumber
Spine
JOE DEMO 123-45-6789
AA
AA
A
AA
AA
AA
C
17
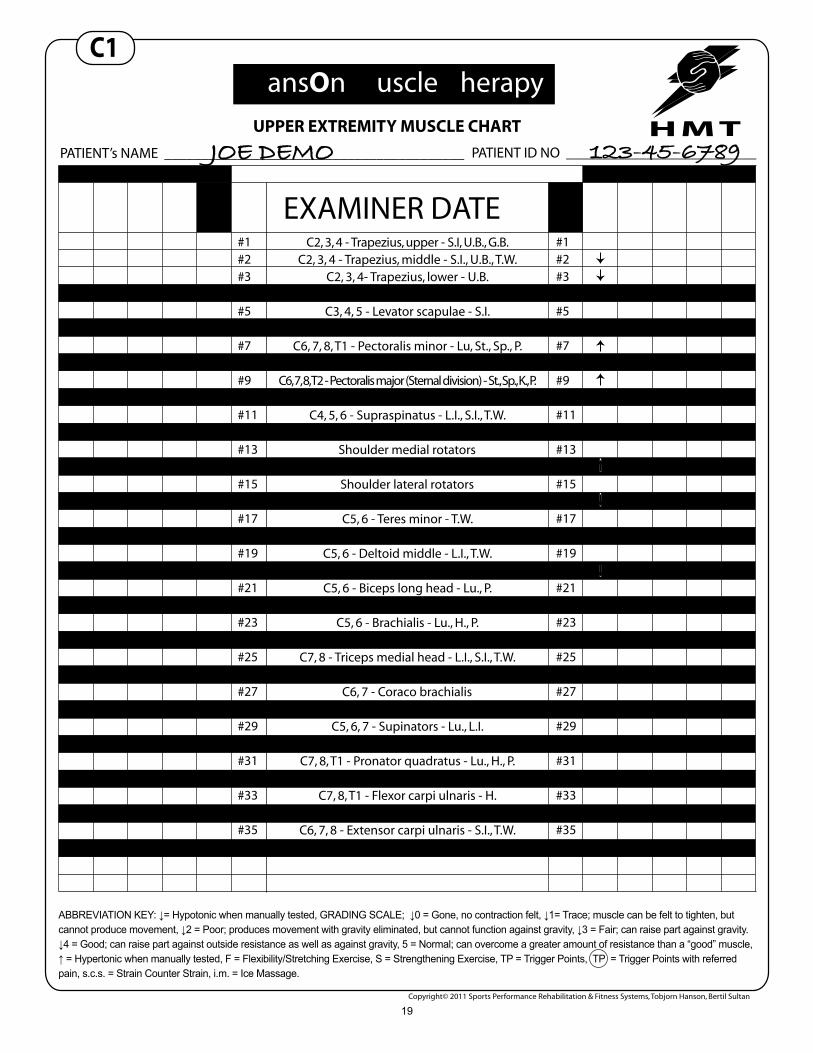
Manual Muscle Testing Manual muscle testing revealed weakness/hypotonicity in #2 Trapezius Middle. #3Trapezius Lower, #16 Latissimus Dorsi, and #20 Deltoid Posterior on the right side.See exam form C-1 on page #19 Weakness/hypotonicity means that the person is unable to sustain a contraction of themuscle being tested, it also means that the muscle is elongated.Manual muscle testing revealed hypertonicity in #7 Pectoralis Minor, #9 Pectoralis Major Sternal, and #14 Subscapularis on the right side.Hypertonicity is indicated when a patient is able to sustain a contraction of the musclebeing tested, but unable to sustain the same contraction following a passive stretch.Hypertonicity means that the muscle is shortened.Shortened muscles Elongated musclesTesting weak after stretch Testing weak#7 Pectoralis Minor #2 Trapezius Middle#9 Pectoralis Major Sternal #3 Trapezius Lower#14 Subscapularis #16 Infraspinatus #20 Deltoid Posterior
Mark form E:1 with the muscles that tested shortened/Hyper Tonic or Elongated /Hypotonic on Manual Muscle Testing. See example page 23.
18
UPPER EXTREMITY MUSCLE CHART
LEFT RIGHT
PATIENT’s NAME _________________________________________ PATIENT ID NO __________________________
EXAMINER DATE#1 #1#2 #2#3 #3#4 #4#5 #5#6 #6#7 #7#8 #8#9 #9#10 #10#11 #11#12 #12#13 #13#14 #14#15 #15#16 #16#17 #17#18 #18#19 #19#20 #20#21 #21#22 #22#23 #23#24 #24#25 #25#26 #26#27 #27#28 #28#29 #29#30 #30#31 #31#32 #32#33 #33#34 #34#35 #35
ABBREVIATION KEY: ↓= Hypotonic when manually tested, GRADING SCALE; ↓0 = Gone, no contraction felt, ↓1= Trace; muscle can be felt to tighten, but cannot produce movement, ↓2 = Poor; produces movement with gravity eliminated, but cannot function against gravity, ↓3 = Fair; can raise part against gravity. ↓4 = Good; can raise part against outside resistance as well as against gravity, 5 = Normal; can overcome a greater amount of resistance than a “good” muscle, ↑ = Hypertonic when manually tested, F = Flexibility/Stretching Exercise, S = Strengthening Exercise, TP = Trigger Points, TP = Trigger Points with referred pain, s.c.s. = Strain Counter Strain, i.m. = Ice Massage.
Copyright© 2011 Sports Performance Rehabilitation & Fitness Systems, Tobjorn Hanson, Bertil Sultan
C2, 3, 4 - Trapezius, upper - S.I, U.B., G.B.C2, 3, 4 - Trapezius, middle - S.I., U.B., T.W.
C2, 3, 4- Trapezius, lower - U.B.C5, 6, 7, 8 - Serratus anterior - Lu, Sp, P., G.B.
C3, 4, 5 - Levator scapulae - S.I.C4, 5 - Rhomboids - U.B.
C6, 7, 8, T1 - Pectoralis minor - Lu, St., Sp., P.C6, 7, 8, T2 - Pectoralis major (Clavicular division) - Lu., St., Sp., K.
C6, 7, 8, T2 - Pectoralis major (Sternal division) - St., Sp., K., P.C6, 7, 8 - Latissimus dorsi - U.B., G.B.C4, 5, 6 - Supraspinatus - L.I., S.I., T.W.
C5, 6, 7 - Teres major - S.I.Shoulder medial rotators
C5, 6, 7 - Subscapularis - H.Shoulder lateral rotators
C4, 5, 6 - Infraspinatus - S.I.C5, 6 - Teres minor - T.W.
C5, 6 - Deltoid anterior - L.I.C5, 6 - Deltoid middle - L.I., T.W.
C5, 6 - Deltoid posterior - S.I., T.W.C5, 6 - Biceps long head - Lu., P.C5, 6 - Biceps short head - Lu., P.
C5, 6 - Brachialis - Lu., H., P.C7, 8 - Triceps long head - S.I., T.W.
C7, 8 - Triceps medial head - L.I., S.I., T.W.C7, 8 - Triceps lateral head - T.W.
C6, 7 - Coraco brachialisC5, 6 - Brachioradialis - Lu., L.I.C5, 6, 7 - Supinators - Lu., L.I.
C6, 7 - Pronator teres - P.C7, 8, T1 - Pronator quadratus - Lu., H., P.
C6, 7, 8 - Flexor carpi radialis - P.C7, 8, T1 - Flexor carpi ulnaris - H.
C5, 6, 7, 8 - Extensor carpi radialis - T.W.C6, 7, 8 - Extensor carpi ulnaris - S.I., T.W.
C1 HansOn Muscle Therapy
JOE DEMO 123-45-6789
19
Primary Pain Zone
This manual uses Travell & Simons “Myofascial pain syndromes” Vol. I and II as a reference for trigger points and their Local and Referred Pain Patterns (RPP).
Since there are so many trigger points and muscles to take into account plus the fact that so manyof those pain patterns overlap each other, there is a need for a helping tool.
HMT uses 7 Pain Zones. The patient mark where they experience their pain on form D:1 (seeexample page 10). On this form there is an outline drawing of a man seen in Front, Bank, Rightand Left view. The drawings has been divided into 7 zones (see page 21). A key for each zonewill indicate all muscles who has trigger points that refer pain into that zone. The zone or zonesthe patient has marked on form D:1 will give an indication on muscles that should be checked andcleared of trigger points. The patient fill in where their greatest pain is felt. They are instructedto mark strips for moderate pain and checkered for severe pain in the appropriate zones.
In the example the patient has marked the posterior pain zone “II”, the posterior portion of shoulder.This pain could be caused by local trigger points or acu-points in the muscles located in thiszone or by remote trigger points referring pain into this zone.Trigger points in muscles #5 Levator scapulae, #11 Superspinatus, #12 Teres Major, #14 Subscapularis,#17 Teres Minor, #20 Deltoid Posterior, #24 Triceps Long Head, and #37 Scalenes can all causepain into the posterior shoulder of zone “II” (See pages 30-41)
20

7 P
AIN
ZO
NES
III
III
IVV
VI
VII
21
Prioritizing Muscles to TreatPrimary or active trigger points and acu-points are more frequently found in theshortened/hypertonic muscles.
After examining posture, assessing range of motion and manually testing the muscles ofthe shoulder and taken the patients marked pain zones with muscles that refer pain intothe same area as the patients complaint is taken under consideration. Eight muscles wereindicated as shortened (hypertonic) with higher frequency than others.
#9 Pectoralis Major Sternal was indicated 5 times. #9 IIII#12 Teres Major was indicated 4 times. #12 IIII#14 Subscapularis was indicated 4 times. #14 IIII#8 Pectoralis Major Clavicular was indicated 4 times. #8 IIII #10 Latissimus Dorsi was indicated 4 times. #10 IIII #1 Trapezius Upper was indicated 3 times. #1 lll#7 Pectoralis Minor was indicated 3 times. #7 lll
See pages 23 and 24 showing Priority Form E:1 and E:2.
This example shows how integration of postural evaluation, range of motion assessment,manual muscle testing, recognition of referred pain patterns and acu puncture meridianswill help us prioritize which muscles to check and clear from trigger and acu-points.Primary active trigger points or acu-points will be found in one of those muscles.
In HMT all muscles that have been indicated as shortened or hypertonic can be treated.Treatment consist of releasing trigger and acu-points in shortened muscles as well asgiving the patient the home stretching (Flexibility) exercise to prevent the muscles fromshortening again and hence help the treatment last.
22

UPPER EXTREMITY
#9 – PECTORALIS MAJOR STERNAL
▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬ Origin: Anterior surface of the sternum, cartilage of the first six or seven ribs, aponeurosis of the External Oblique. Insertion: Crest of the greater tubercle of the humerus. The fibers twist on themselves and are more posterior and cranial in comparison to the clavicular fibers. Action: Adducts and medially rotates humerus. Horizontally adducts humerus towards the contralateral anterior superior iliac spine. Reversed origin-insertion and change of action: The Pectoralis Major Sternal may assist in elevating the thorax as in forced inspiration. In crutch walking or in parallel bar work, it will assist in supporting the weight of the body. Myotatic unit / Synergists & Antagonists: Adduction of humerus: Synergists: #8 Pectoralis Major Clavicular, #10 Latissimus Dorsi, #12 Teres Major, #24 Triceps Long Head, #27 Coracobrachialis. Antagonists: #11 Superspinatus, #18 Anterior Deltoid, #19 Middle Deltoid, #20 Posterior Deltoid. Medial rotation of humerus: Synergists: #8 Pectoralis Major Clavicular, #10 Latissimus Dorsi, #12 Teres Major, #14 Subscapularis, #18 Anterior Deltoid. Antagonists: #16 Infraspinatus, #17 Teres Minor, #20 Posterior Deltoid. Horizontal adduction of the humerus: Synergists: #8 Pectoralis Major Clavicular. Antagonists: #2 Middle Trapezius, #3 Lower Trapezius. Nerve Suppy: Lateral and medial pectoral, C6, C7, C8, T1
9:1
9:2
I
II II
II
TP III22
TP IV
#9 Pectoralis Major Sternal
I
IIIII
9:3
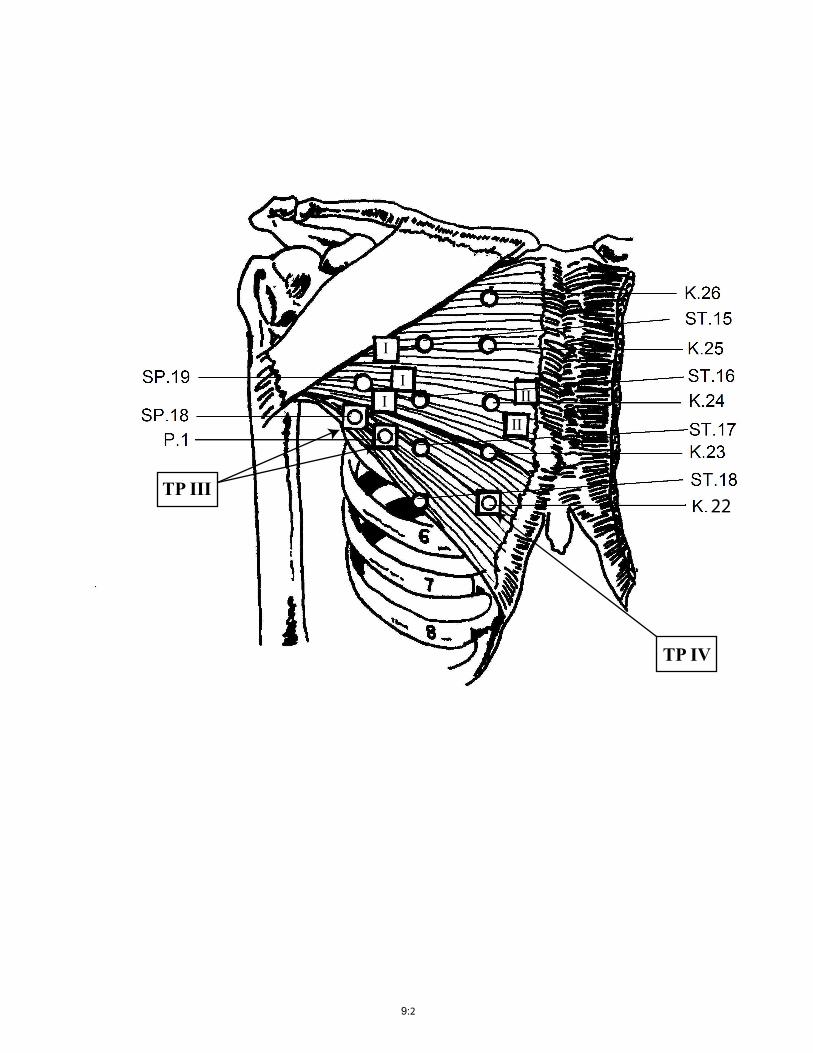
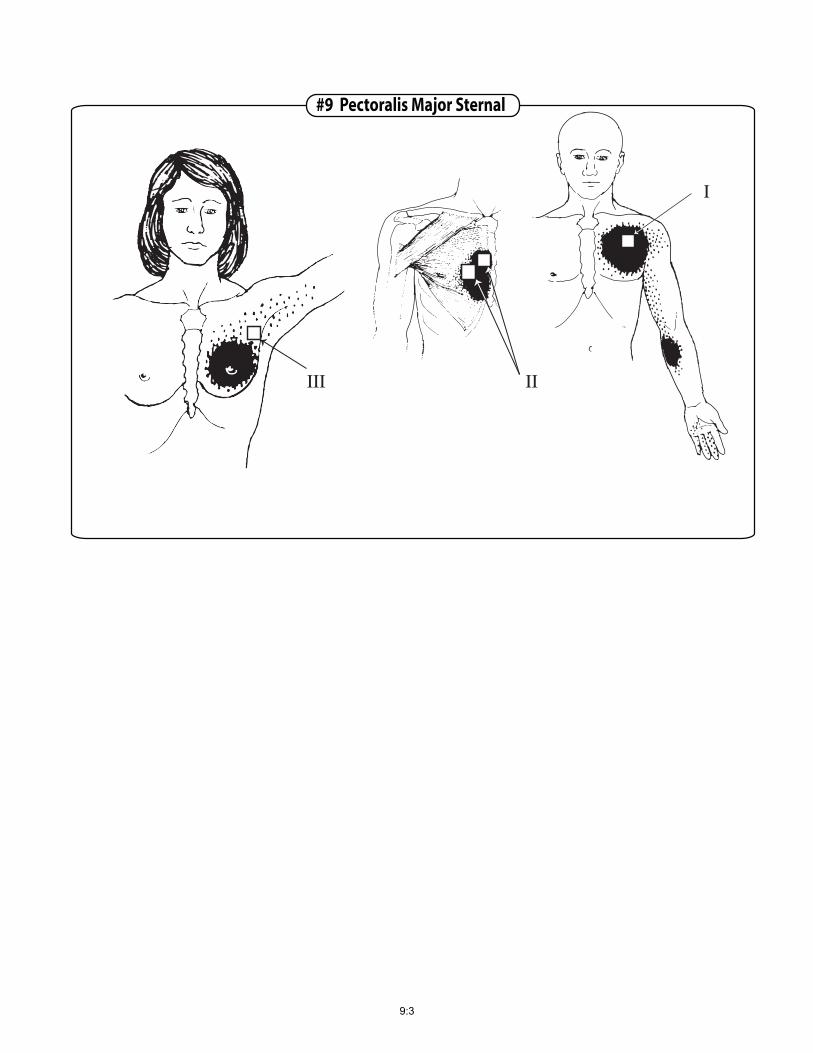
Entrapments: Entrapment of a lymph duct by passage between tense, shortened fibers of an involved Pectoralis Major Sternal may cause edema of the breast. These signs of entrapped lymphatic drainage and breast tenderness are relieved by extinction of the related TP’s. Pectoralis Major Sternal Trigger Points: TP’s are localized through the Pectoralis Minor against the chest wall. Trigger points in the Pectoralis Minor may be distinguished from Pectoralis Major by the fiber direction of palpable bands (TP’s). TP I : Location: Three trigger points are found in the lateral portion of the muscles sternal division. Between the 2nd and 4th ribs approximately 4.5-5.5 cun lateral to the center of the sternum. Referred Pain Pattern: Anterior chest, down the inner aspect of the arm, accented pain in the area of the medial epicondyle. In severe cases the pain will travel to the volar aspect of the forearm and the ulnar side of the hand, the last 2 of 2½ digits usually innervated by the sensory fibers of the ulnar nerve. TP II: Location: Two trigger points are found in the medial sternal section, 0.5-1.5 cun lateral to the center of the sternum, between the 3rd and 4th rib. Referred Pain Pattern: Locally in the medial portion of the muscle, and over the sternum without crossing the midline. TP III: Location: Two trigger points are found in the costal/abdominal section of the muscle at the lateral free margin of the muscle approximately 5-6 cun lateral to the center of the sternum in the region of the 4th intercostals space. Referred Pain Pattern: Pain in the lower anterior chest, breast tenderness with hypersensitivity of the nipple, intolerance to clothing and often breast pain. TP IV: Location: One trigger point is located medially in the costal/abdominal section of the muscle. The same location or nearby the K. 22 acupuncture point, in the 5th intercostals space, 2 cun lateral to the center of the sternum. Referred Pain Pattern: Local spot tenderness associated with ectopic cardiac rhythms, but not with any pain complaint. When active trigger points occur in the left pectoralis major, the referred pain can easily be confused with coronary insufficiency. All patients with those symptoms should be checked by their physician to clear any cardiac disease or dysfunction. It is possible for coronary artery insufficiency or other intrathoracic organ diseases/dysfunctions to create viscerosomatic satellite trigger points in the skeletal muscles of the anterior chest wall. Caution must be taken so that release of trigger points in this area are not masking any organ pathology, always refer to the patients physician when in doubt.
9:4
On the other hand it is possible for active trigger points to mimic pai patterns of cardiac or gallbladder pathology without any organ dysfunction to be found. Release of those trigger points will permanently relieve symptoms. Associated Trigger Points: #2 Middle Trapezius, #4 Serratus Anterior, #6 Rhomboids, #7 Pectoralis Minor, #8 Pectoralis Major Clavicular, #10 Latissimus Dorsi, #14 Subscapularis, #17 Teres Minor, #18 Anterior deltoid, #20 Posterior deltoid, #27 Coracobrachialis, #36 Sternocleidomastoid, #37 Scalenes. Satellite Trigger Points: #7 Pectoralis Minor, #8 Pectoralis Clavicular, #10 Latissimus Dorsi, #14 Subscapularis, #30 Pronator Teres, #32 Flexor Carpi Radialis, #33 Flexor Carpi Ulnaris. These muscles lie within the zones of referred pain from TP’s in the Pectoralis Major Sternal. Pain experienced in the Pectoralis major clavicular can be of a referred nature from trigger points in the following muscles: #4 Serratus Anterior, #7 Pectoralis Minor #37 Scalenes. Acupuncture Meridians: Stomach (St.), Spleen (Sp.), Kidney (K.), Pericardium (P.) Pectoralis Major sternal Local Acupuncture points: St. 15: Location: In the 2nd intercostal space on the mammillary line. Indications: Cough, asthma, fullness in the chest, mastitis. St. 16: Location: In the 3rd intercostals space on the mammillary line. Indications: Cough, asthma, fullness of the chest, mastitis. St. 17: Location: In the center of the nipple, in the 4th intercostals space. Indications: Therapy is contraindicated. St. 18: Location: In the 5th intercostals space on the mammillary line. Indications: Cough, Asthma, mastitis, lactation deficiency, pain in the chest. Sp. 18/TP: Location: 2 cun lateral to the nipple, in the 4th intercostals space. Indications: Sensation of fullness and pain in the chest, cough, mastitis, lactation deficiency.
9:5
Sp. 19: Location: In the 3rd intercostal space, 6 cun lateral to the center of the sternum. Indications: Sensation of fullness and pain in the chest and hypochondriac region. K. 22/TP Location: In the 5th intercostals space, 2 cun lateral to the center of the sternum. Indications: Cough, Asthma, local point tenderness associated with ectopic cardiac rhythms. K. 23 Location: In the 5th intercostals space, 2 cun lateral to the center of the sternum. Indications: Cough, Asthma, sensation of fullness in the chest and hypochondriac region, mastitis. K. 24 Location: In the 4th intercostals space, 2 cun lateral to the center of the sternum. Indications: Cough, Asthma, sensation of fullness in the chest and hypochondriac region, mastitis. K. 25 Location: In the 3rd intercostals space, 2 cun lateral to the center of the sternum. Indications: Cough, Asthma, chest pain. K. 26 Location: In the 1st intercostals space, 2 cun lateral to the center of the sternum. Indications: Cough, Asthma, sensation of fullness in the chest and hypochondriac region. P. 1/TP Location: 1 cun lateral to the nipple in the 4th intercostals space. Indications: Suffocating sensation in the chest, pain in the hypochondriac region, swelling and pain of the axillary region.
9:6
UPPER EXTREMITY
#12 - TERES MAJOR
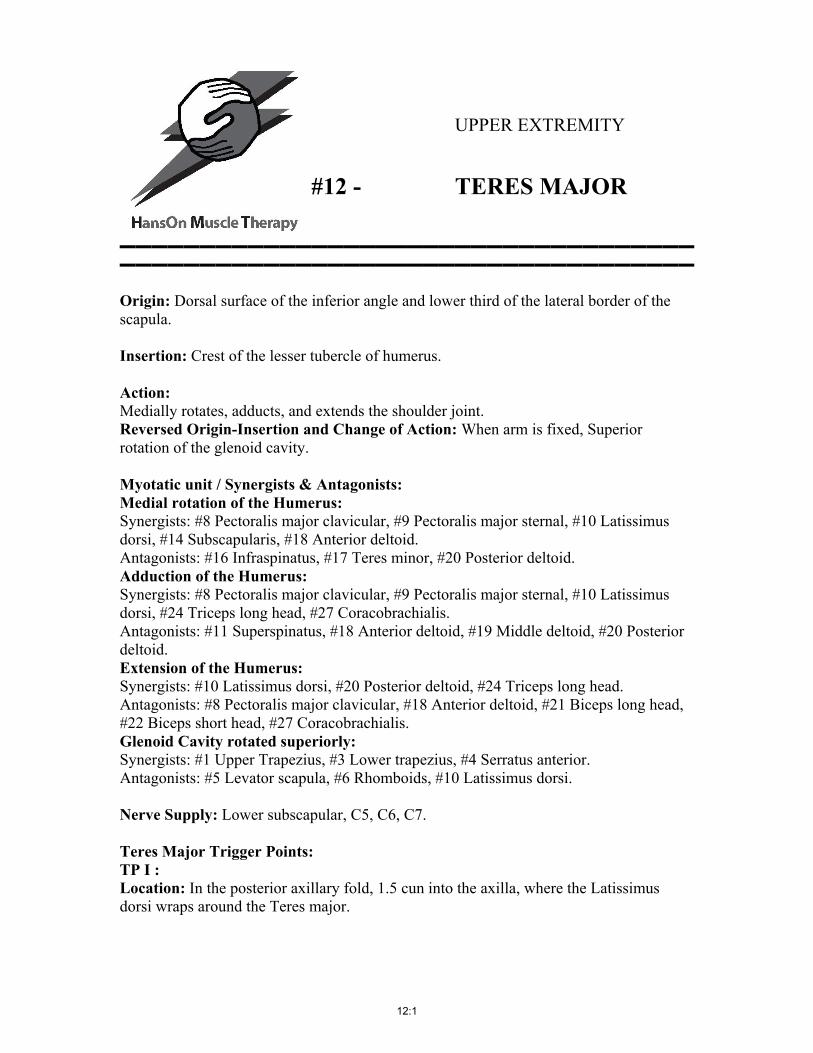
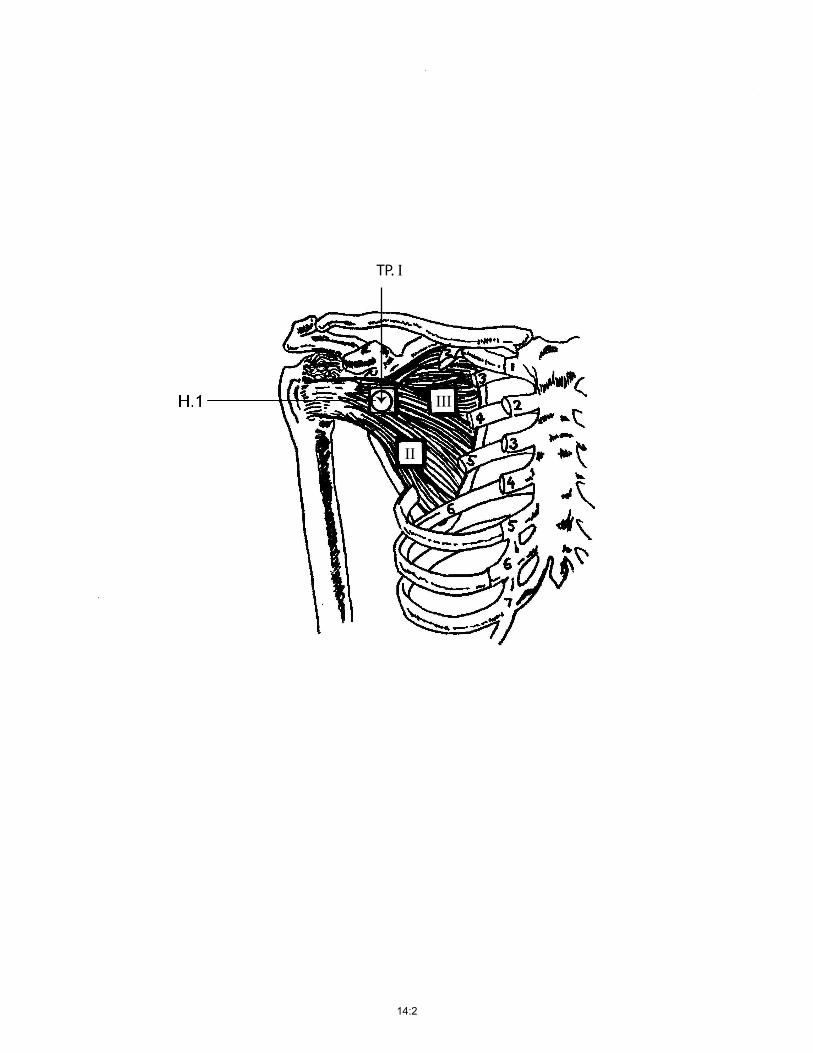
▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬ Origin: Dorsal surface of the inferior angle and lower third of the lateral border of the scapula. Insertion: Crest of the lesser tubercle of humerus. Action: Medially rotates, adducts, and extends the shoulder joint. Reversed Origin-Insertion and Change of Action: When arm is fixed, Superior rotation of the glenoid cavity. Myotatic unit / Synergists & Antagonists: Medial rotation of the Humerus: Synergists: #8 Pectoralis major clavicular, #9 Pectoralis major sternal, #10 Latissimus dorsi, #14 Subscapularis, #18 Anterior deltoid. Antagonists: #16 Infraspinatus, #17 Teres minor, #20 Posterior deltoid. Adduction of the Humerus: Synergists: #8 Pectoralis major clavicular, #9 Pectoralis major sternal, #10 Latissimus dorsi, #24 Triceps long head, #27 Coracobrachialis. Antagonists: #11 Superspinatus, #18 Anterior deltoid, #19 Middle deltoid, #20 Posterior deltoid. Extension of the Humerus: Synergists: #10 Latissimus dorsi, #20 Posterior deltoid, #24 Triceps long head. Antagonists: #8 Pectoralis major clavicular, #18 Anterior deltoid, #21 Biceps long head, #22 Biceps short head, #27 Coracobrachialis. Glenoid Cavity rotated superiorly: Synergists: #1 Upper Trapezius, #3 Lower trapezius, #4 Serratus anterior. Antagonists: #5 Levator scapula, #6 Rhomboids, #10 Latissimus dorsi. Nerve Supply: Lower subscapular, C5, C6, C7. Teres Major Trigger Points: TP I : Location: In the posterior axillary fold, 1.5 cun into the axilla, where the Latissimus dorsi wraps around the Teres major.
12:1
. I
II
PT
12:2
#12 Teres Major
III
12:3
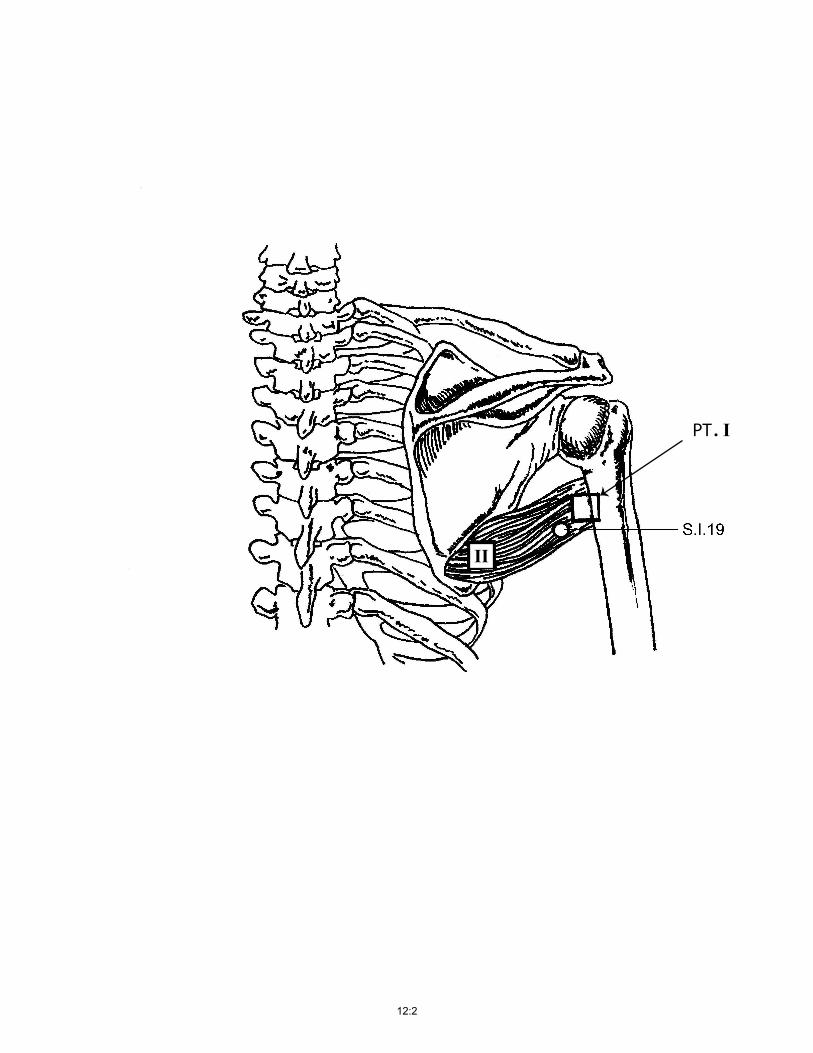
TP II: Location: Close to the origin of the muscle on the inferior angle of the scapula. Referred Pain Pattern: Posteriorly into the shoulder joint, occasionally to the dorsal forearm. Associated Trigger Points: #10 Latissimus dorsi, #14 Subscapularis, #16 Infraspinatus, #17 Teres minor, #18 Anterior deltoid, #24 Triceps long head. Satellite Trigger Points: #11 Supraspinatus, #16 Infraspinatus, #17 Teres minor, #18 Anterior deltoid, #34 Extensor carpi radialis, #35 Extensor carpi ulnaris. Pain experienced in the Teres Major can be of a referred nature from trigger points in the following muscles: #4 Serratus anterior, #5 Levator scapula, #10 Latissimus dorsi, #11 Supraspinatus, #14 Subscapularis, #16 Infraspinatus, #17 Teres minor, #20 Posterior deltoid, #24 Triceps long head, #37 Scalenes. Acupuncture Meridians: Small Intestine (S.I.) Teres Major Local Acupuncture points: S.I. 9: Location: Posterior and inferior to the shoulder joint. When the arm is adducted, the point is 1 cun above the posterior end of the axillary fold. Indications: Pain in the scapular region, pain and motor impairment of the hand and arm.
12:4

UPPER EXTREMITY
#14 - SUBSCAPULARIS
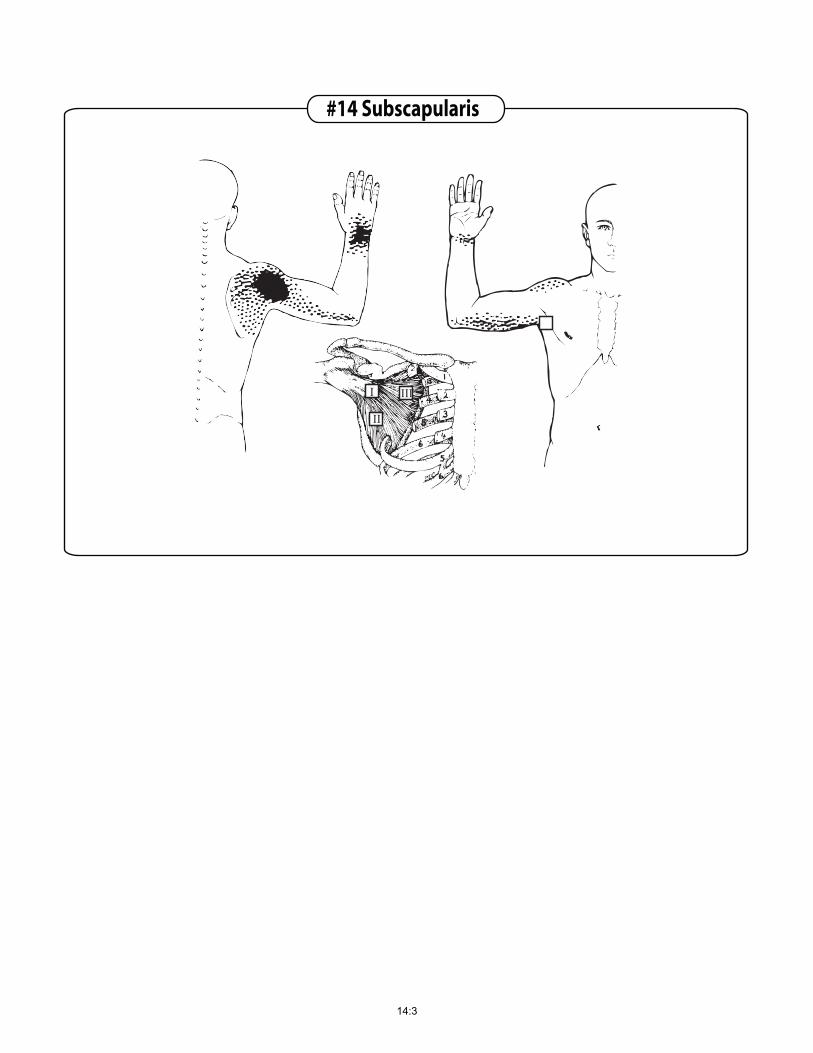
▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬ Origin: Subscapular fossa of the scapula. Insertion: Lesser tubercle of the humerus and shoulder joint capsule. Action: Medially rotates the shoulder joint, and stabilizes the head of the humerus in the glenoid cavity, preventing it from subluxating anteriorly during movements of this joint. Myotatic unit / Synergists & Antagonists: Medial rotation of the Humerus: Synergists: #8 Pectoralis major clavicular, #9 Pectoralis major sternal, #10 Latissimus dorsi, #12 Teres major, #18 Anterior deltoid. Antagonists: #16 Infraspinatus, #17 Teres minor, #20 Posterior deltoid. Nerve Supply: Upper and lower subscapular, C5, C6, C7. Subscapular Trigger Points: TP I: Location: Deep in the posterior axillary fold on the anterior portion of the scapula, close to its lateral border and the muscle insertion. It lies 3 fingers into the axilla. TP II: Location: Deep in the axilla, on the anterior portion of the scapula, approximately at the mid-scapular level. TP III: Location: On the anterior portion of the scapula, real deep, medial to TP I. To palpate those TP’s, the arm must be abducted as much as possible (in involved cases the patient may only be able to abduct the arm to 30 degrees). The scapula must be abducted by the therapist causing traction by pulling the arm or scapula laterally. Referred Pain Pattern: Severe pain both at rest and on motion. The essential zone lies over the posterior aspect of the shoulder, spillover reference zones cover the scapula and extends down the posterior aspect of the arm to the elbow, frequently the pain refers like a strap around the wrist.
14:1
Insert Subscapularis Picture
TP. I
II
III
14:2
#14 Subscapularis
I III
II
14:3
Associated Trigger Points: #8 Pectoralis major clavicular, #9 Pectoralis major sternal, #10 Latissimus dorsi, #12 Teres major, #16 Infraspinatus, #18 Anterior deltoid, #20 Posterior deltoid, #24 Triceps long head. Satellite Trigger Points: #10 Latissimus dorsi, #12 Teres major, #16 Infraspinatus, #17 Teres minor, #19 Middle deltoid, #20 Posterior deltoid, #24 Triceps long head, #25 Triceps medial head, #26 Triceps lateral head, #31 Pronator quadratus. Those muscles lie within the zones of referred pain from TP’s in the subscapularis. Pain experienced in the Subscapularis can be of a referred nature from trigger points in the following muscles: #4 Serratus anterior, # 7 Pectoralis minor, #9 Pectoralis major sternal, #10 Latissimus dorsi, #16 Infraspinatus. Acupuncture Meridians: Heart (H.) Subscapularis Local Acupuncture points: H. 1: Location: In the center of the axilla, on the medial side of the axillary artery. Indications: Pain in the costal and cardiac regions, scapula, cold and pain in the elbow and arm.
14:4