clinical approach to neurologic disorders anatomic pathophysiologic phenomenologic symptomatic...
TRANSCRIPT

Clinical Approach to Neurologic Disorders
• GENERAL SYMPTOMS AND SIGNS
• TREATMENT
AnatomicPathophysiologicPhenomenologic
SymptomaticProtectiveCurativeSurgical

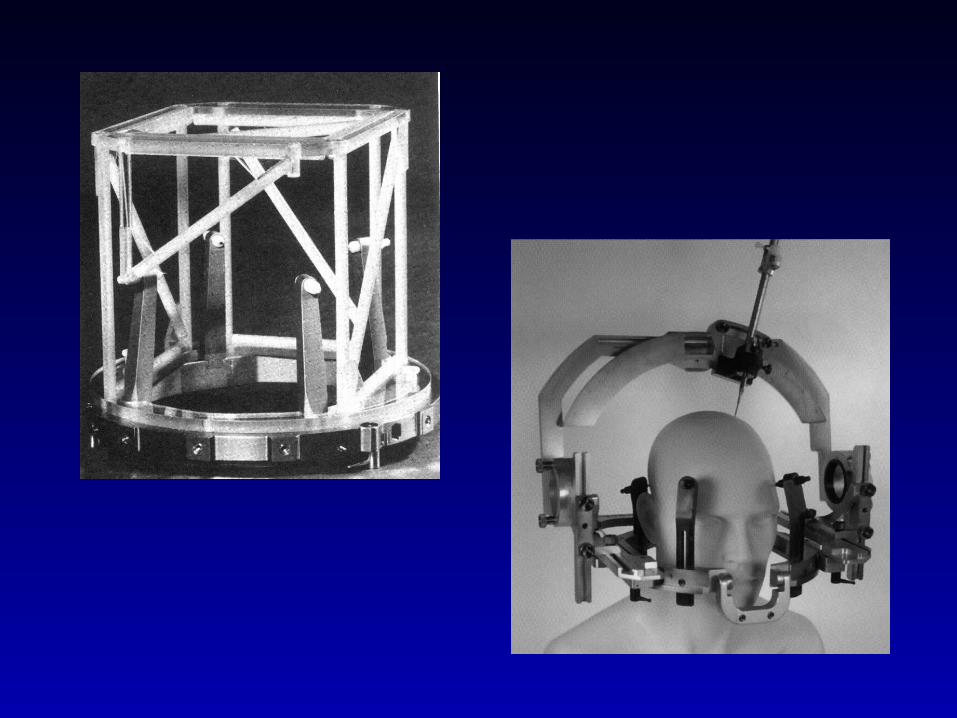
Surgical Approaches
• Ablative– thalamotomy– Pallidotomy
• Electrical stimulation (DBS) – VIM thalamus, globus pallidus internus, sub-thalamic nucleus
• Transplant– autologous adrenal, human fetal, xenotransplants, genetically
engineered transplants
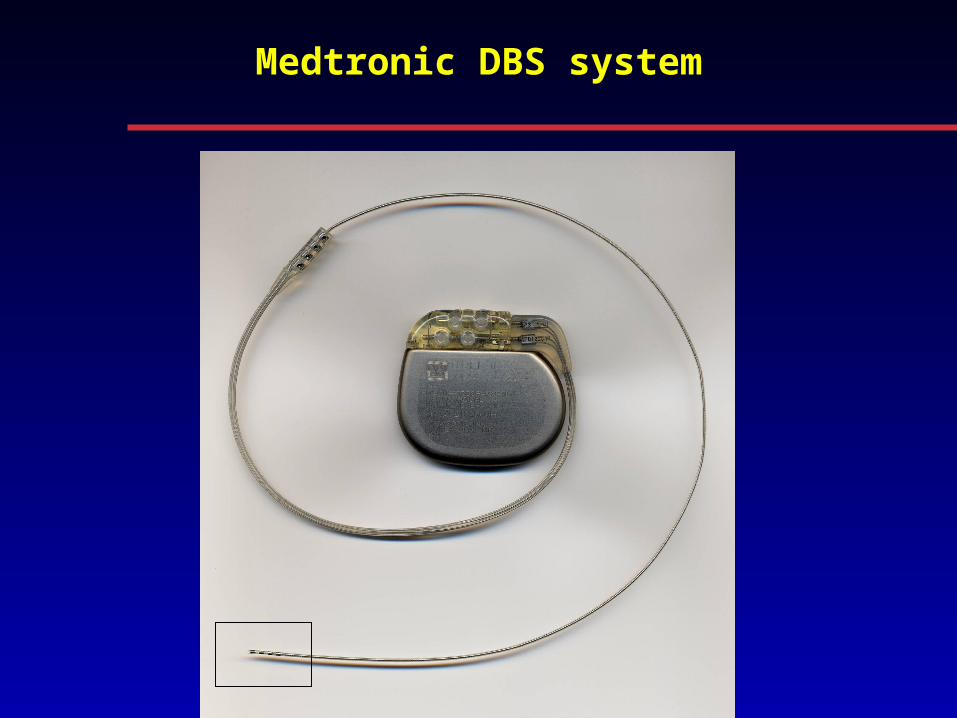
Medtronic DBS system


Disease Classification
Congenital
Genetic
Demyelinating
Vascular
Immunologic
Neoplastic/ Para-neoplastic
To xic/ Nutritive
Metabolic
Mitochondrial/ Sub-cellular systems
Infectious/ Post-infectious
Traumatic
Degenerative
Idiopathic
Iatrogenic

Physical Exam
• Vital signs• Appearance• Emotional state
General medical Brief comments on relevant pulmonary,cardiovascular (murmurs, bruits),musculo-skeletal (deformities,asymmetries) and skin (rashes, othermarkings).
In neurology, asymmetric or focal findings are typically most important

Neurologic
Mental status orientation, level of alertness, speech, memory,cognitive state (mini-mental exam is helpful).
Cranial nerves I important really if asymmetric, particularly with achange in personality or suspected frontal lobe disease.II - fundus exam, visual acuity (should be documented),visual fields, and relative afferent pupillary defect(RAPD).III, IV and VI - pupil and eye movements, optokineticnystagmus (OKN), other forms of nystagmus andrelated findings.V sensory: cornea, skin to vertex of head, not angleof mandible.
motor: muscles of mastication (chewing).VII should clarify peripheral vs central issues.VIII important in hearing, balance. IX - XII - speech quality, swallowing, tonguemovements, tongue atrophy.
Physical Exam

Physical Exam
Motor examStrength e.g. MRC 5/5 point scaleMuscle massToneReflexes deep tendon (can be elicited in the jaw)
cutaneous (Babinski, abdominals)Rapid alternating movements speed, decrement rhythmInvoluntary movements
tremormyoclonuschoreaathetosisticsdystoniaballismusdyskinesia
Motor apraxiasdressing, combing hair, brushing teeth
Physical Exam
Sensory exam
Cranial divisions of V
Other head and neck Angle of jawSpinal levelsNerve or root
Primary modalities Light touchTwo point discriminationPainVibrationPosition sense
Higher cortical modalitiesGraphesthesiaStereognosis
Physical Exam
CoördinationUsually, but not always, tests for cerebellar dysfunction
Targeted voluntary movementsfinger-to-noseheel-shin
Rapid alternating movementsfine hand, finger control
Gait and posture
Stride, stancetruncal sway, arm swing
Posturestooped, falling forward, backward
Freezingin doorson or off medicationat start of walking
Disorders of muscle tone
I. HYPERTONICITY
a. Upper motor neuron syndrome
1. Loss of strength - paresis or paralysis2. Loss of fine distal movements3. Spasticity
clasp-knife (velocity-dependent) toneincreased (velocity-dependent) deep tendon
reflexes4. Release of flexor reflex afferents, eg Babinski sign
b. Extrapyramidal rigidity
1. Plastic, lead-pipe, equally increased tone throughout2. Normal deep tendon reflexes3. No paralysis of movement

Disorders of muscle tone
II. HYPOTONICITY
a. Cerebellar disease - acuteb. Deep coma
III. GEGENHALTEN
Resistance to passive manipulation, unable to relax, confusion,
frontal lobe disease

Basal ganglia disease
NEGATIVE symptoms
a. Primary functional deficits -
1. Akinesia or bradykinesiaunderactivity or poverty of movement (hypokinesia)
2. Loss of postural reflexesfailure to make small adjustments walking, standing up, etc
3. Difficulty with rapid alternating movements
POSITIVE symptoms
b. Secondary effects -
1. Lead pipe rigidityincreased tone
2. Involuntary movements (hyperkinetic disorders or dyskinesias)tremordystoniachoreaathetosisballismakathisia

Basal Ganglia
• Subcortical forebrain structures connected to sensorimotor and limbic systems
• Crucial part of the “control circuitry” that allows for the smooth execution of voluntary movement

Basal Ganglia
• Multiple cortico-basal ganglia-thalamo-cortical circuits
• Help program and carry out motor plans
• Scale the amplitude and effort of the execution of tasks with relation to requirements
• Incorporate motivation and emotional drives

D1
SNc
D2
GPe
DA
+-
GABA -
Brainstem/spinal cord
Glu +
Glu +
Glu +
-GABASPDyn
STN
GABAEnk -
Ventralthalamus
GPi/SNr
GABA -
GABA -
Parkinson’s disease
D1
SNc
D2
GPe
DA
+-
GABA -
Normal
Glu +
Glu +
-GABASPDyn
STN
GABAEnk -
Ventralthalamus
GPi/SNr
GABA -
Brainstem/spinal cord
GABA -
Glu +
Cerebral cortex
Striatum
Cerebral cortex
Striatum
D1
SNc
D2
GPe
DA
+-
GABA -
Brainstem/spinal cord
Glu +
Glu +
Glu +
-GABASPDyn
STN
GABAEnk -
Ventralthalamus
GPi/SNr
GABA -
GABA -
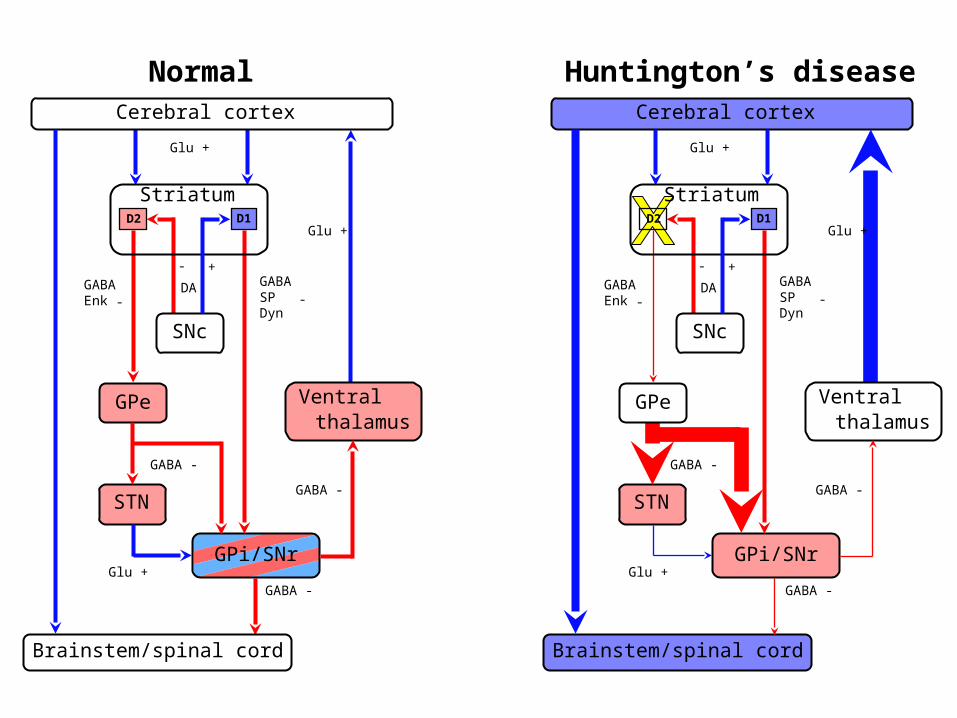
Huntington’s disease
D1
SNc
D2
GPe
DA
+-
GABA -
Normal
Glu +
Glu +
-GABASPDyn
STN
GABAEnk -
Ventralthalamus
GPi/SNr
GABA -
Brainstem/spinal cord
GABA -
Glu +
Cerebral cortex
Striatum
Cerebral cortex
Striatum

Basal ganglia disease
Tremor♦ Rhythmic oscillation about a joint
1. Physiologi c and exaggerated physiologic
2. Rest (parkinsonia )n
3. Kinetic or action
4. Postural
5. Int ent ion (cerebellar)
6. Task-relat ed: writ ing tr emor, ortho st at ic tr emor
Dystonia♦ Sust ained and/ or semi-rhyth mic muscle spasms, oft en worse with a
part icular t ask or po stur e♦ Persist ent att itud e in ext remes o f po sit ion, eg hyper- f lexed or hyper-
ext ended♦ Irregular tr emors
♦ “ Occupat ional” cramps (w rit er’s c ramps, musician’ cramps, et c)
♦ Meige’s syndro me: blepharospasm and o ro- facial dyskinesias/ dysto nia.

Photo by James Parkinson from his paper "An Essay on the Shaking Palsy” 1817
Normal PD

Basal ganglia disease
Chorea♦ Rapi ,d arrhythmi ,c jerk , y equa l distally and proximally
Athetosis♦ Slow, sinuous movements
♦ Movement s fro m on e postur e to another
♦ Inability to kee p limb i n one position
Ballism♦ Wil ,d flingin g movements o f limbs
♦ Associated with lesio ns o f the subthalami c nucleus

Basal ganglia disease
Myoclonus♦ Shoc -k like fast muscle jerks - faste r than chorea, less sinuous th an tremor
♦ Irregular
♦ May hav e sensor y relationship
♦ Cortical, su -b cortical, spinal
♦ Unusual variants: palata l myoclonus
Tics♦ Stereotyp ed movements
♦ Simple, e g eye blinking, o r complex involving many bo dy regions
♦ Associated with “inner feeling” to releas e tension
♦ May be vocal, eg barkin , g sniffing
♦ Gilles de la Tourett e syndrome
Akathisia♦ restlessness
♦ unab le to sit fo r more than a few seconds
Neurologic Issues Relevant to Dentistry
Bell’s palsy
Inflammation of the facial (VII) nerve - weakness of all parts of theface – the forehead movements , eye closure, mouth movements.
Often is mistaken for a “stroke” with slurred speech except thatlanguage and cognitive functions are preserved.
Never results in double vision, can affect taste on one side of thetongue, can occur at any age, and can be preceded by pain in oraround the ear.

Bell’s palsy
Initial presentation After 6 months
Neurologic Issues Relevant to Dentistry
Disorders affecting the face, jaw, mouth and neck
• Trigeminal neuralgia• Temporo-mandibular joint disorders• Other facial pains• Jaw tremors• Bruxism• Tardive dyskinesia• Meige’s syndrome• Other oro-buccal facial dystonias• Torticollis
Other Neurologic Issues Relevant to Dentistry
Complications of anesthesia
♦ Coma
♦ Maligna nt hyperthermia

Malignant Hyperthermia
Sudden onset of high fever, muscle rigidity and autonomic signs.
♦ Temperature rise → 42 -4 3° C
♦ Tachypnea, tachycardia
♦ Los s o f brainstem reflexes
♦ Circulator y collapse
♦ Rigidit y in all muscles → high C K a nd myoglobinuria
♦ J aw clenching - unexpected after relaxation fro m anesthesia
♦ Anesthetic agents
halothanesuccinylcholineether

Malignant Hyperthermia
Pathogenesis: a. anesthesia lead to increase in O2 consumption
b. depletion of ATPc. muscles unable to relax (muscles require energy to relax)
Treatment: D/C anesthesia at first sign
IV dantrolene - inhibits Ca++ releaseCooling, hydration, sodium bicarbonate
Susceptible patients: Family history of anesthetic-related problemsMusculo-skeletal abnormalitiesShort stature, ptosis, high arched palate