pathophysiologic aspects, clinical manifestation a nd management of
TRANSCRIPT

PATHOPHYSIOLOGIC ASPECTS,CLINICAL MANIFESTATION AND
MANAGEMENT OF CERVICAL RADICULOPATHY
By
DR SUSHANT YADAV
RESIDENT IN DEPARTMENT OF MEDICINE
MGM MEDICAL COLLEGE, AURANGABAD
ANATOMYParts of a Typical Vertebra
• Vertebrae in different regions of the spinal column vary in size, shape,
and details.
• Vertebrae typically consist:
1. Body
2. Vertebral arch
3. Processes
Hermizan Halihanafiah

Body
• Thick, Disc shape anterior portion
• Weight bearing part of the vertebrae.
• Superior & inferior surface are roughened – attachment of cartilaginous
intervertebral disc.
• Anterior and lateral surface contain nutrient foramina, opening for blood vessels
deliver nutrient and O2 and remove CO2 and wastes from bone tissues.

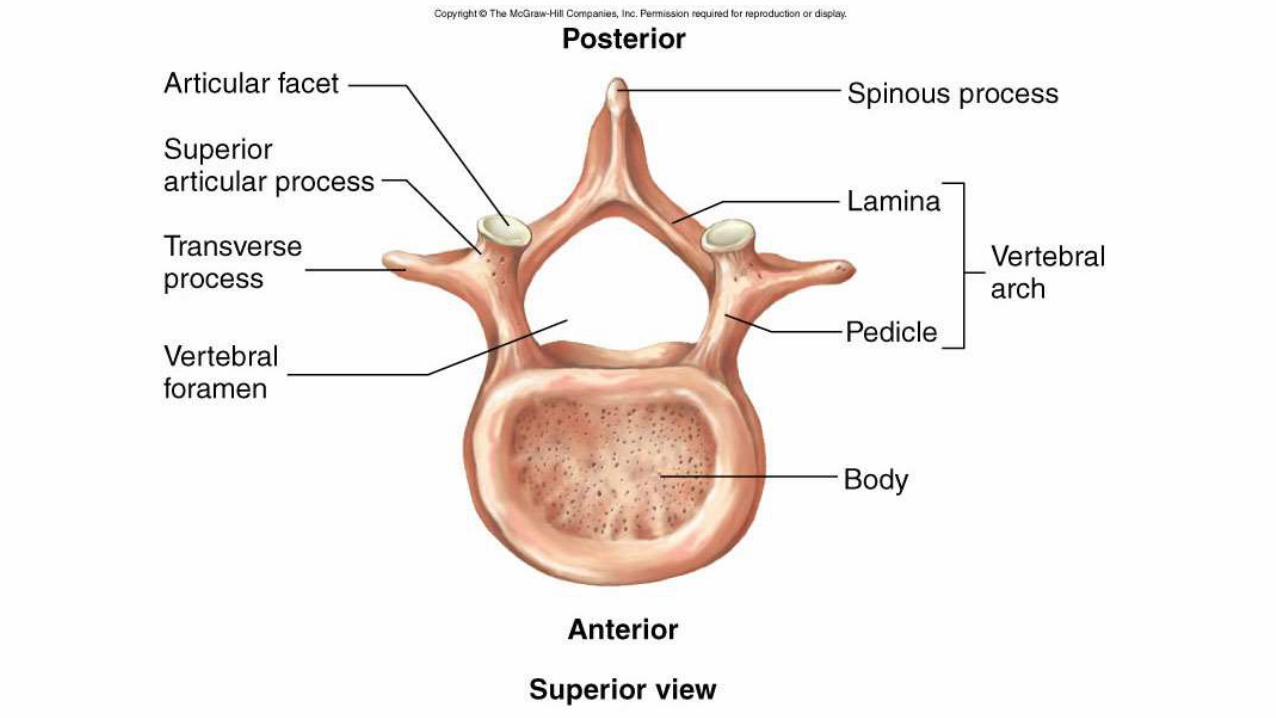
Vertebral Arch• 2 short, thick processes called the pedicles, project posteriorly from the
vertebrae body to unite with the flat laminae, to form the vertebrae arch.
• Vertebral arch extend posteriorly from the body of the vertebra, together with
the body and vertebral arch surround the spinal cord by forming the vertebral
foramen.
• Vertebral foramen contain spinal cord, adipose tissue and areolar connective
tissue and blood vessels.
Vertebral Arch
• Collectively, the vertebral foramina of all vertebrae form the vertebral
(spinal) cavity.
• The pedicles exhibit superior and inferior indentation called vertebral
notches.
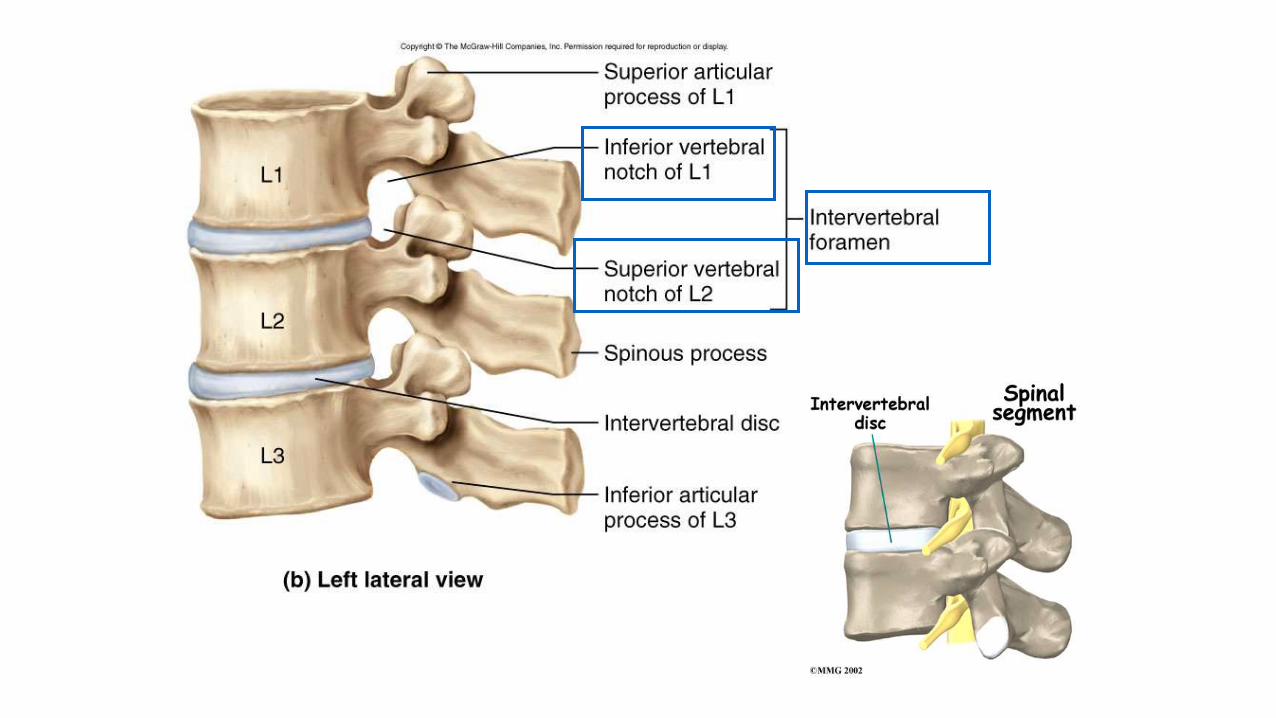
• Superior and inferior vertebral notch are stacked on top of ones another
to form intervertebral foramen.
• Intervertebral foramen permits the passage of single spinal nerve that
passes to a specific region of the body.
Processes• 7 processes arise from the vertebral arch.
• At the point where lamina and pedicle join, a transverse process extends
laterally on each side.
• A single spinous process projects posteriorly from the junction of the
laminae.
• These 3 processes serve as points of attachments for muscles.

Processes
• The remaining 4 processes forms joints with other vertebrae above and
below.
• 2 superior articular processes articulate with the 2 inferior articular
processes of vertebrae above them.
• The articulating surfaces of articular processes called facets.
• Articulation between the bodies and articular facets of successive
vertebrae are called intervertebral joint.

• Neural foramen
• Notches between adjacent
vertebrae.
• Allows for the passage of the
spinal nerve roots, spinal artery,
veins, nerve plexus, and
ligaments
Intervertebral Foramen

Intervertebral Discs
• Fibrocartilage.
• Lie between adjacent
vertebrae in the spine.
• Each disc forms a
cartilaginous joint to allow
slight movement of the
vertebrae
• Acts as a ligaments to hold
the vertebrae together.
Hermizan Halihanafiah
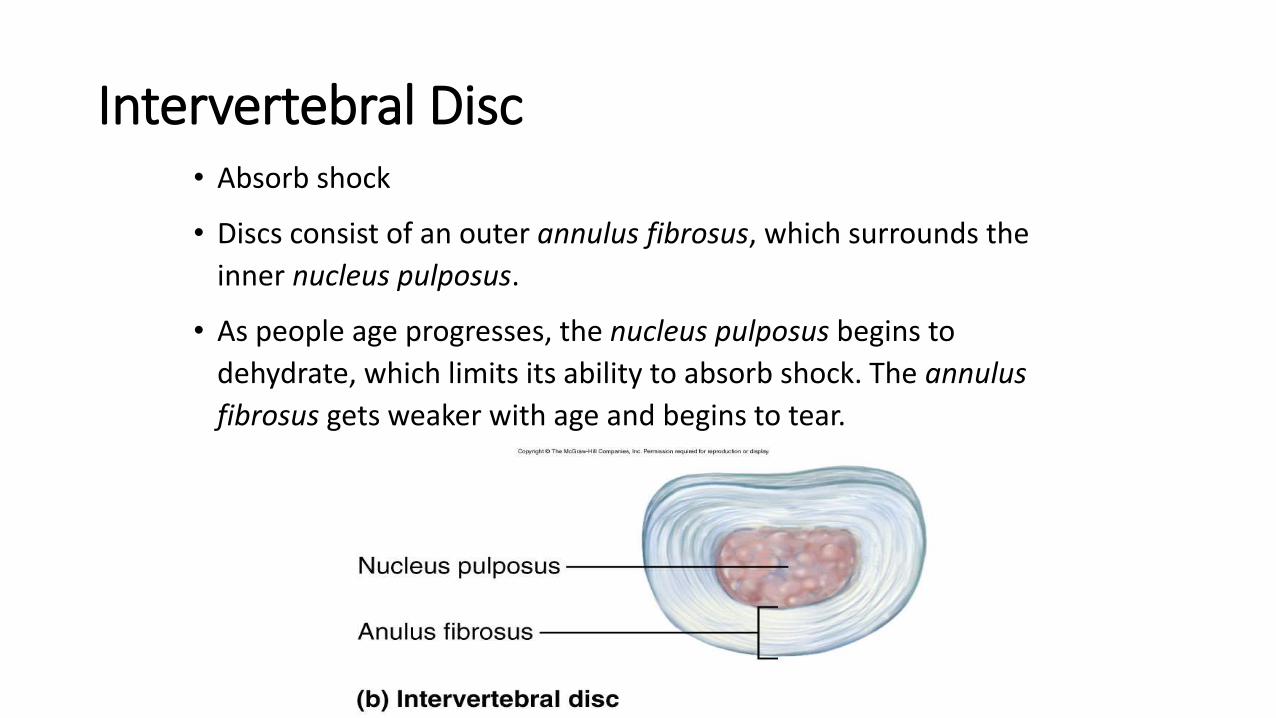
Intervertebral Disc• Absorb shock
• Discs consist of an outer annulus fibrosus, which surrounds the
inner nucleus pulposus.
• As people age progresses, the nucleus pulposus begins to
dehydrate, which limits its ability to absorb shock. The annulus
fibrosus gets weaker with age and begins to tear.

Cervical Vertebrae▪ Seven vertebrae (C1-C7) are the smallest, lightest vertebrae
▪ C1, C2 and C7 are atypical
▪ C3-C6 are typical
▪ Oval body & wider side to side
▪ short spinous processes and is bifid
▪ vertebral foramina is large and triangular
▪ Each transverse process contains a transverse foramen through which the vertebral arteries pass to the brain
▪ C7 spinous process is larger and not bifid
▪ C7 vertebra prominence (can be seen through the skin) is the landmark for counting.
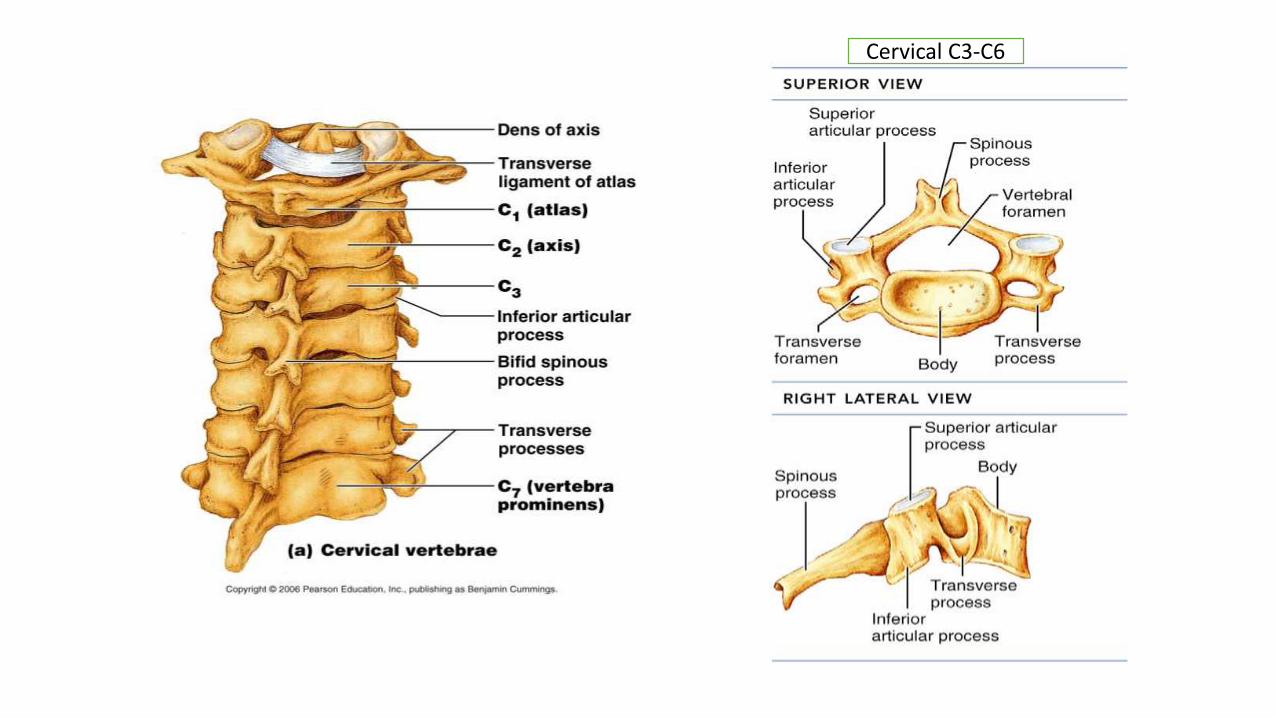
Cervical C3-C6
Cervical Vertebrae: The Atlas (C1)
▪ No intervertebral disc between C1 &C2
▪ The atlas has no body and no spinous process
▪ It consists of anterior and posterior arches, and two lateral masses.
▪ Each lateral mass has articular facets on both its superior and inferior surfaces
▪ The superior surfaces of lateral masses articulate with the occipital condyles of occipital bone to form atlanto – occipital joint.
▪ These articulation permits the movement for “YES”.
▪ The inferior surfaces articulate with the Axis (C2) to form atlanto-axial joint
▪ These articulation permits the movement for “NO”.

Cervical Vertebrae: The Atlas (C1)

Cervical Vertebrae: The Axis (C2)
▪ The axis has a body, spine, and vertebral arches as do
other cervical vertebrae
▪ Unique to the axis is the dens, or odontoid process,
which projects superiorly from the body and is cradled
in the anterior arch of the atlas
▪ The dens fuses with axis during embryonic
development
▪ The dens is a pivot for the rotation of the atlas

Anterior View Posterior View Lateral View
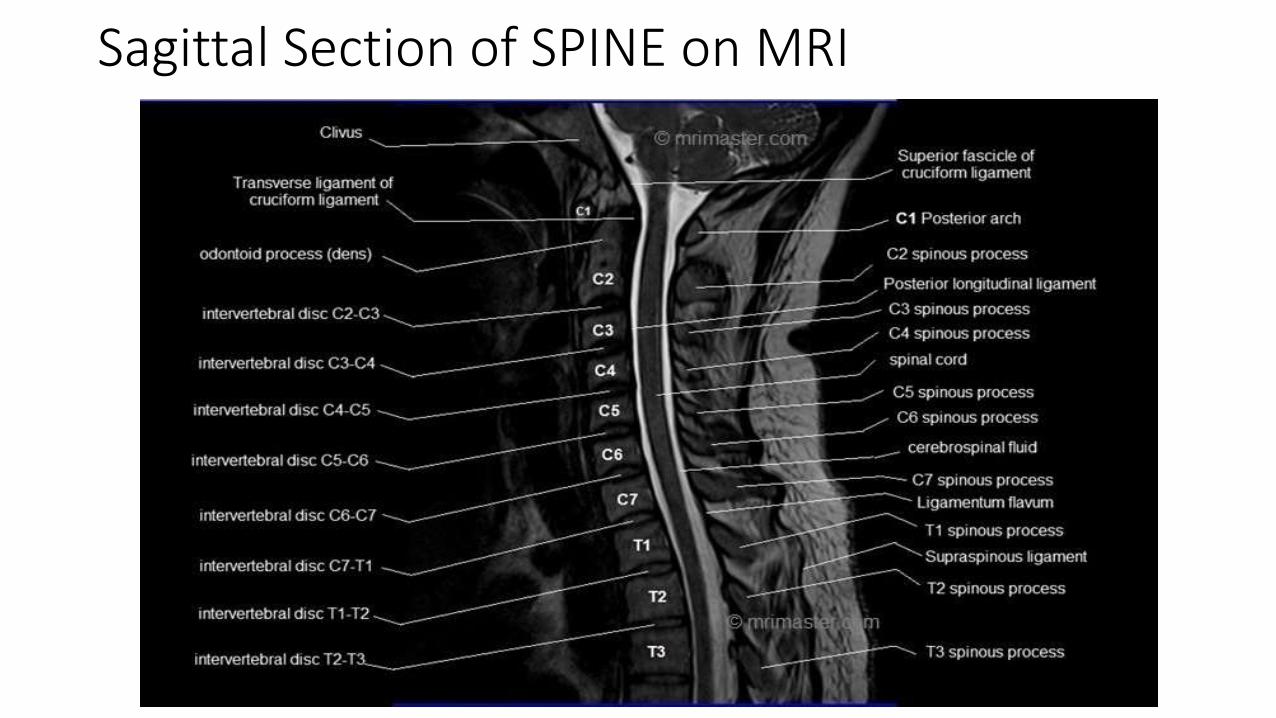
Sagittal Section of SPINE on MRI

Transverse Section of SPINE at C7 level on MRI
Cervical Nerve Roots• Eight pairs of cervical nerve roots are formed directly from multiple tiny rootlets that
originate directly from the spinal cord.
• These tiny rootlets coalesce immediately within the intraspinal canal and form the dorsal (sensory) and the ventral (motor) roots.
• These join together just before passing through the intervertebral foramen and form the spinal nerve root.
• On exiting the foramen, the nerve root splits into the small posterior ramus and the larger anterior ramus.
• In contrast to the roots, there are only seven cervical vertebra whereas the eight root exits below the seventh cervical vertebra and above the first thoracic vertebra.

Cervical Nerve Roots• The neuroforamen are bordered anteromedially by the uncovertebral joint,
posterolaterally by the facet joint, superiorly by the pedicle of the vertebral body immediately above, and inferiorly by the pedicle of the vertebral body immediately below.
• The medial section of the foramen is derived from the intervertebral discs and the vertebral endplates.
• The roots originate in close proximity to the level at which they exit the intraspinalcanal.
• The cervical roots generally pass through the canal and in a somewhat more horizontal fashion.
• This arrangement causes the neuroforamen to originate more medially and the cervical root and the cervical spinal cord to be in close proximity, thereby susceptible to abnormalities of these medial structures such as osteophytes or disc herniations, leading to the symptoms of cervical radiculopathy.

Definition
•Radiculopathy• Functional disturbance of spinal nerve root
•Myelopathy• Functional disturbance of the spinal cord

Cervical radiculopathy
• Cervical radiculopathy is the term that describes compression of a cervical nerve root which results in pain and/or sensorimotor deficit in the upper extremity. It can be caused by disc herniation, spondylosis, instability, trauma and rarely, tumors.
• The C7 (60%) and C6 (25%) cervical nerve roots are the most commonly affected.
Risk Factors
• Heavy lifting > 25pounds
• Smoking
• Driving
• Operating vibrating equipment
• Previous trauma 15%

Epidemiology
• Annual incidence 0.85 cases/1000• Peak 4th & 5th decades
• Prevalence 3.3/1000• Less frequent than lumbar spine
• Male > Female
• C6 & C7 roots are most commonly affected
• Young Population- Disc Herniation or Acute injury causing foraminalimpingement of exiting nerve.• Older Population- Degenerative changes (Foraminal narrowing from
osteophytes, More axial neck & interscapular pain) > Disc herniation

CAUSES
• Disc herniation
• Degeneration, spondylosis, hypertrophy of Zygapophyseal joint or uncovertebral joint
• Spinal instability
• Trauma
• Tumors


PATHOPHYSIOLOGY• Beginning in the third decade of life, a progressive decline in the water content of the
intervertebral disc occurs and continues with age. The nucleus pulposus becomes an indistinct fibrocartilaginous mass.
• In patients younger than 30 years, the water content of the intervertebral disc approaches 90%, and it decreases to less than 70% by the eighth decade of life.
• The basic structural unit of the nucleus pulposus is glycosaminoglycan protein, which consists of a proteoglycan protein core and bulky, sterically active polysaccharide attachments of chondroitin sulfate and keratin sulfate.
• Because of their high molecular weight and overall negative charge, glycosaminoglycan proteins have a strong attraction for water molecules.
PATHOPHYSIOLOGY• With aging, these large, sterically active glycosaminoglycan proteins gradually diminish in
size and number.
• As a result, the intervertebral disc’s ability to retain water also diminishes. These age-related changes in the chemical composition of the nucleus pulposus and annulus fibrosuscause the degenerated disc to become more compressible and less elastic.
• Consequently, the disc loses height and bulges dorsally into the spinal canal. As the vertebral bodies drift toward one another, the ligamentum flavum and facet joint capsule fold in dorsally, causing a further decrease in the canal and foraminal dimensions.
• This approximation of adjacent vertebral bodies leads to a reactive process that produces osteophytes around the disc margins and at the uncovertebral and facet joints.

PATHOPHYSIOLOGY• Compressive radiculopathies occur as a result of mechanical distortion of the nerve
root by either the hypertrophied facet joint or uncovertebral joints, disc protrusion, spondylotic spurring of the vertebral body, or a combination of these factors.
• Pressure on the nerve root may lead to sensory deficits, motor weakness, or radicular pain.
• When a nerve is compressed changes occur in and around the nerve which include: an inflammatory response, changes in vascular flow, and intra-neural edema. A combination of these three events are thought to result in the development of radicular pain.

Clinical Presentation
• Radiculopathy can be divided into acute, subacute, and chronic.
• Acute cervical radiculopathy occurs in relatively young patients in the setting of a tear in the annulus fibrosus and subsequent prolapse of the nucleus pulposus.
• Subacute radiculopathy occurs in patients with pre-existing cervical spondylosis, without persistent symptoms except for occasional neck pain. Patients develop insidious symptoms, which are often polyradicular in nature.
• Chronic radiculopathies materialize from acute or subacute radiculopathies that have failed to respond to treatment.
• Pain is most prominent in acute cervical radiculopathy and diminishes as the condition becomes more chronic.
• It may be described as sharp, achy, or burning and may be located in the neck, shoulder, arm, or chest, depending on the nerve root involved.
• Classically, an acute radiculopathy presents with pain radiating in a myotomaldistribution.
• Sensory symptoms, predominantly parasthesias and numbness, are more common than motor loss and diminished reflexes.
Physical Exam
• Sensation
•Motor strength
• Range of motion
•Deep tendon reflexes
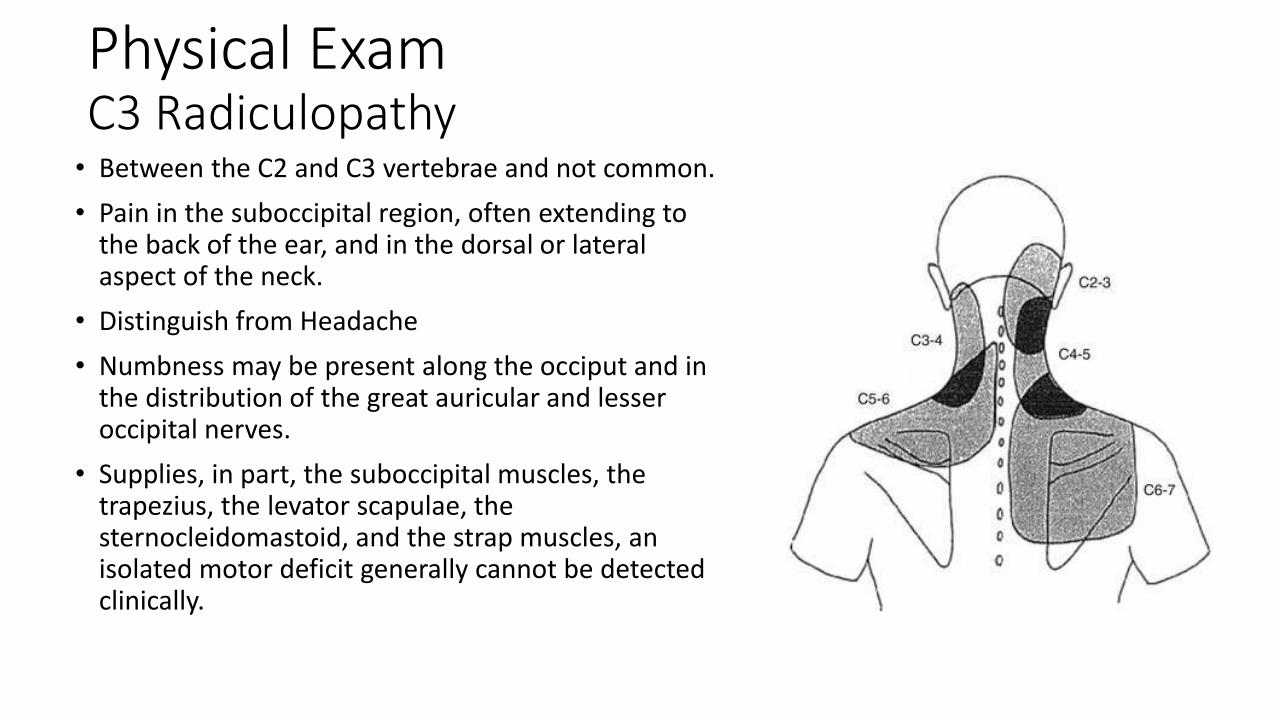
Physical ExamC3 Radiculopathy• Between the C2 and C3 vertebrae and not common.
• Pain in the suboccipital region, often extending to the back of the ear, and in the dorsal or lateral aspect of the neck.
• Distinguish from Headache
• Numbness may be present along the occiput and in the distribution of the great auricular and lesser occipital nerves.
• Supplies, in part, the suboccipital muscles, the trapezius, the levator scapulae, the sternocleidomastoid, and the strap muscles, an isolated motor deficit generally cannot be detected clinically.

Physical ExamC4 Radiculopathy
• C3-C4 level
• Unexplained pain along the base of the neck that radiates to the superior aspect of the shoulder and posteriorly to the scapula
• The rhomboid, trapezius, and levatorscapulae muscles are supplied, in part, by the fourth nerve root, but a motor deficit may be hard to detect.
• Sensory loss along anterolateral aspect of the neck, along the distribution of the transverse cervical and supraclavicular nerves
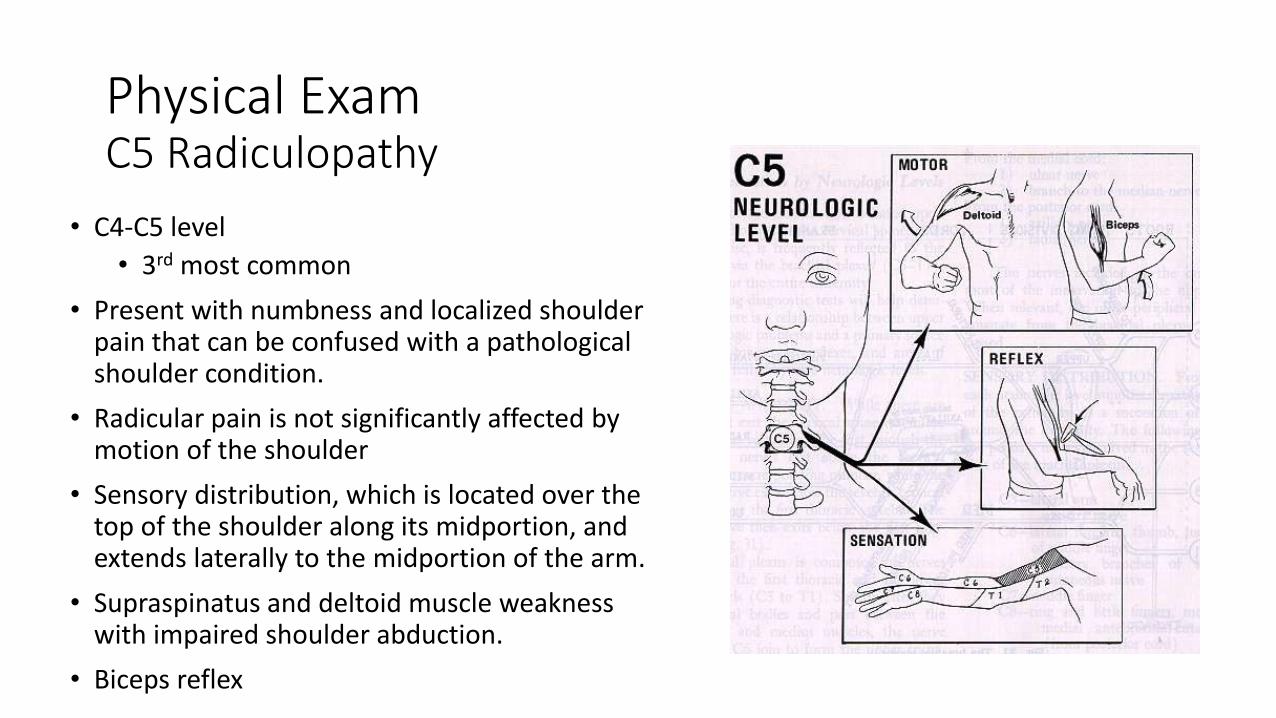
Physical ExamC5 Radiculopathy
• C4-C5 level
• 3rd most common
• Present with numbness and localized shoulder pain that can be confused with a pathological shoulder condition.
• Radicular pain is not significantly affected by motion of the shoulder
• Sensory distribution, which is located over the top of the shoulder along its midportion, and extends laterally to the midportion of the arm.
• Supraspinatus and deltoid muscle weakness with impaired shoulder abduction.
• Biceps reflex
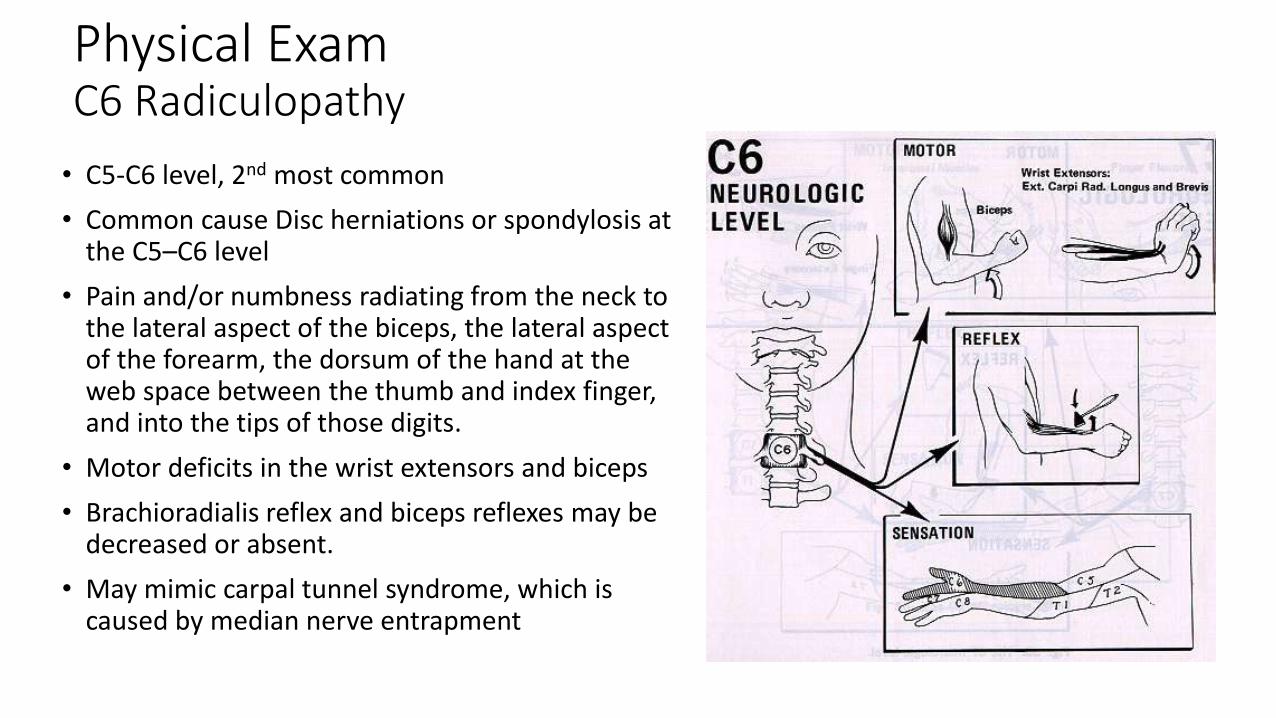
Physical ExamC6 Radiculopathy
• C5-C6 level, 2nd most common
• Common cause Disc herniations or spondylosis at the C5–C6 level
• Pain and/or numbness radiating from the neck to the lateral aspect of the biceps, the lateral aspect of the forearm, the dorsum of the hand at the web space between the thumb and index finger, and into the tips of those digits.
• Motor deficits in the wrist extensors and biceps
• Brachioradialis reflex and biceps reflexes may be decreased or absent.
• May mimic carpal tunnel syndrome, which is caused by median nerve entrapment
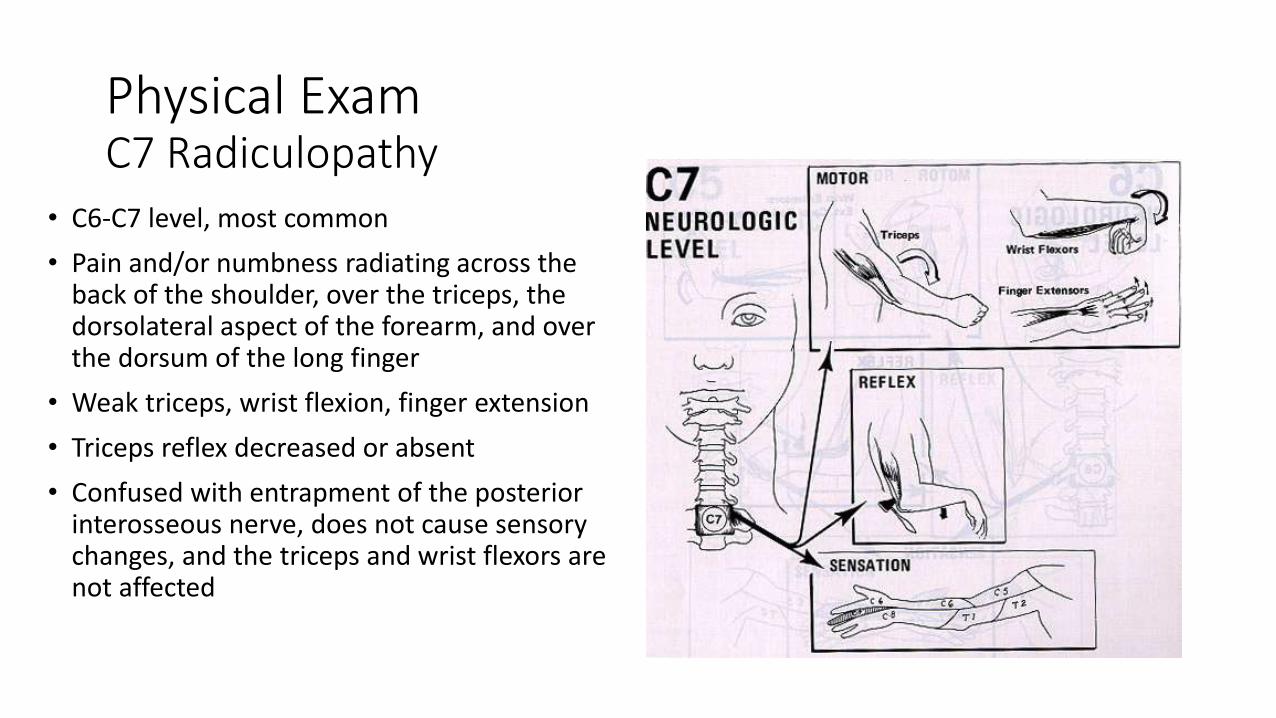
Physical ExamC7 Radiculopathy
• C6-C7 level, most common
• Pain and/or numbness radiating across the back of the shoulder, over the triceps, the dorsolateral aspect of the forearm, and over the dorsum of the long finger
• Weak triceps, wrist flexion, finger extension
• Triceps reflex decreased or absent
• Confused with entrapment of the posterior interosseous nerve, does not cause sensory changes, and the triceps and wrist flexors are not affected

Physical ExamC8 Radiculopathy
• C7-T1 level, Infrequent
• The medial aspect of the arm and forearm and into the medial hand and the last two digits.
• Numbness usually involves both the dorsal and volar aspects of the digits and hand and may extend proximal to the wrist over the medial aspect of the forearm
• Weak grip
• Mimic ulnar entrapment at the elbow.

Physical ExamT1 Radiculopathy
• T1-T2 level, Very uncommon
• Weak hand intrinsic muscles
• Axillary numbness is common, and Horner’s syndrome can occur ipsilaterally


Physical ExamProvocative Tests• Reduced cervical rotation <60 degrees to the affected side.
• Reduction of symptoms with shoulder abduction
• Reduction of symptoms with cervical distraction
• Provocation of symptoms with the Spurling test
• Provocation of symptoms with the median nerve biased neurodynamic test which is done by performing Upper Limb Neural Tension Test (ULNTT).
• Provocation of symptoms with the Valsalva maneuver – less commonly included.
• L’hermitte’s Sign – less commonly included
• Spurling test, distraction test, ipsilateral rotation <60 degrees and ULNTT have a 99% specificity when all four items are positive and 94% specificity when 3 items are positive (Waldrop, 2006)


Physical ExamSpurling Test/Foraminal compression test/Neck compression test/ Quadrant test
• Extending the neck
• Rotating head
• Downward pressure on head
• Positive finding eliciting reproduction of radicular pain into ipsilateral arm of headrotation
• 92% sensitive, 95% specific
• Low sensitivity but high specificity- not useful as a screening tool, but it does help confirm the diagnosis
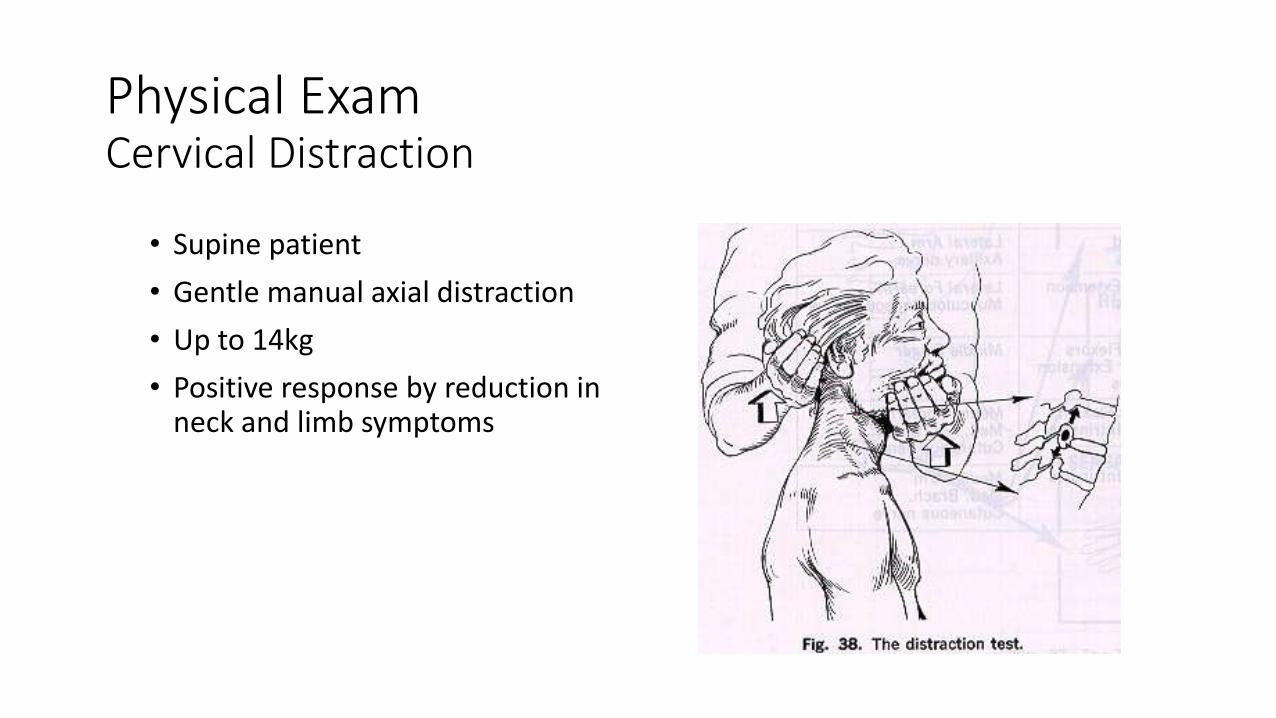
Physical ExamCervical Distraction
• Supine patient
• Gentle manual axial distraction
• Up to 14kg
• Positive response by reduction in neck and limb symptoms

Physical ExamUpper Limb Neural Tension Test (ULNTT)
• The patient is positioned in supine. During the ULNTT that places a bias towards testing the patient’s response to tension placed on the median nerve
• Scapular depression
• Shoulder abduction to approximately 90 degrees with the elbow flexed
• Shoulder external rotation
• Forearm supination, wrist and finger extension
• Elbow extension
• Contralateral then ipsilateral cervical side-bending
• A positive test is indicated by
• Reproduction of all or part of the patient’s symptoms
• On the symptomatic side, contralateral cervical side-bending increases the patient’s symptoms, or ipsilateral side-bending decreases the patient’s symptoms
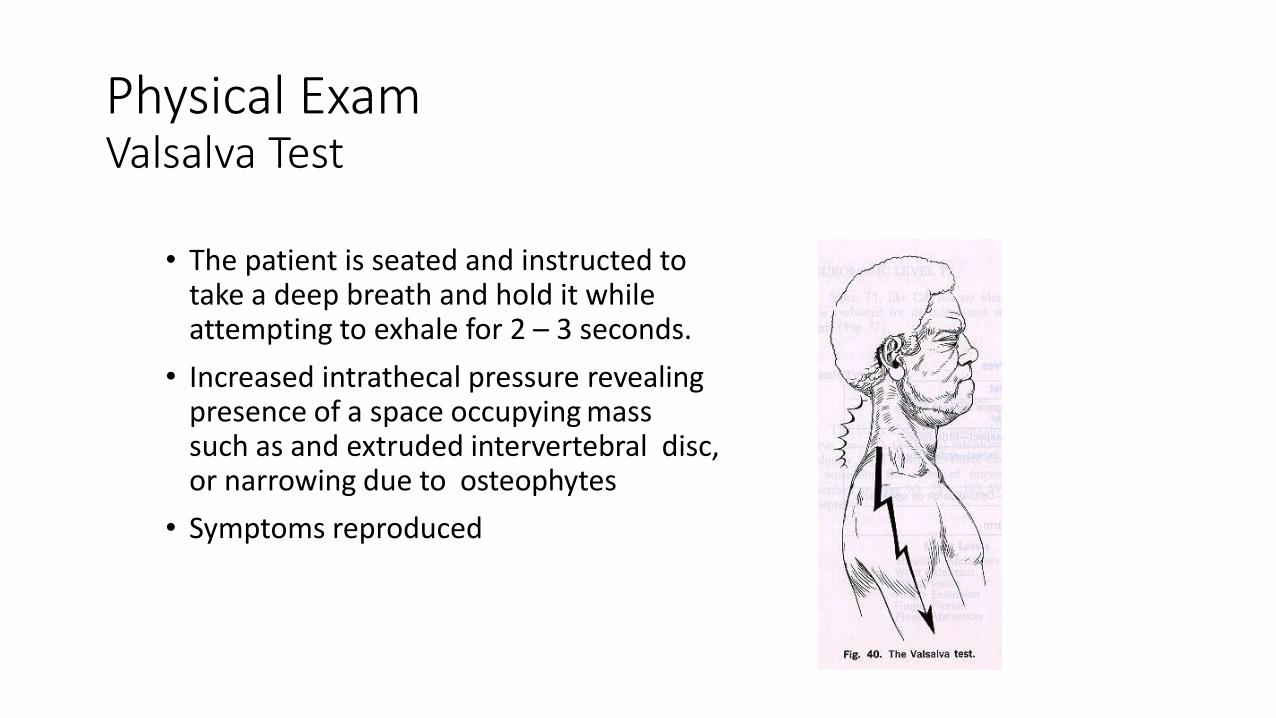
Physical ExamValsalva Test
• The patient is seated and instructed to take a deep breath and hold it while attempting to exhale for 2 – 3 seconds.
• Increased intrathecal pressure revealing presence of a space occupying mass such as and extruded intervertebral disc, or narrowing due to osteophytes
• Symptoms reproduced

Physical ExamShoulder abduction test/ Shoulder abduction relief sign/Bakody’s sign
• Active/passive abduction of ipsilateralshoulder
• Relief of radicular symptoms
• takes stretch off of the affected nerve rootand may decrease or relieve radicularsymptoms

• Flexion of neck producing electric shock like sensations that extend down the spine and shoot into the limbs
• Usefulness is limited
• Indicates spinal canal stenosis,disc impingement, multiplesclerosis, or tumor
Physical ExamLhermitte sign/ Barber chair phenomenon

Others
• NAFFZIGER'S TEST(for nerve rootcompression)
• Manual compression of the jugular veinsbilaterally
• An increase or aggravation of pain or sensory disturbance over the distribution of the involved nerve root confirms the presence of an extruded intervertebral disk or other mass
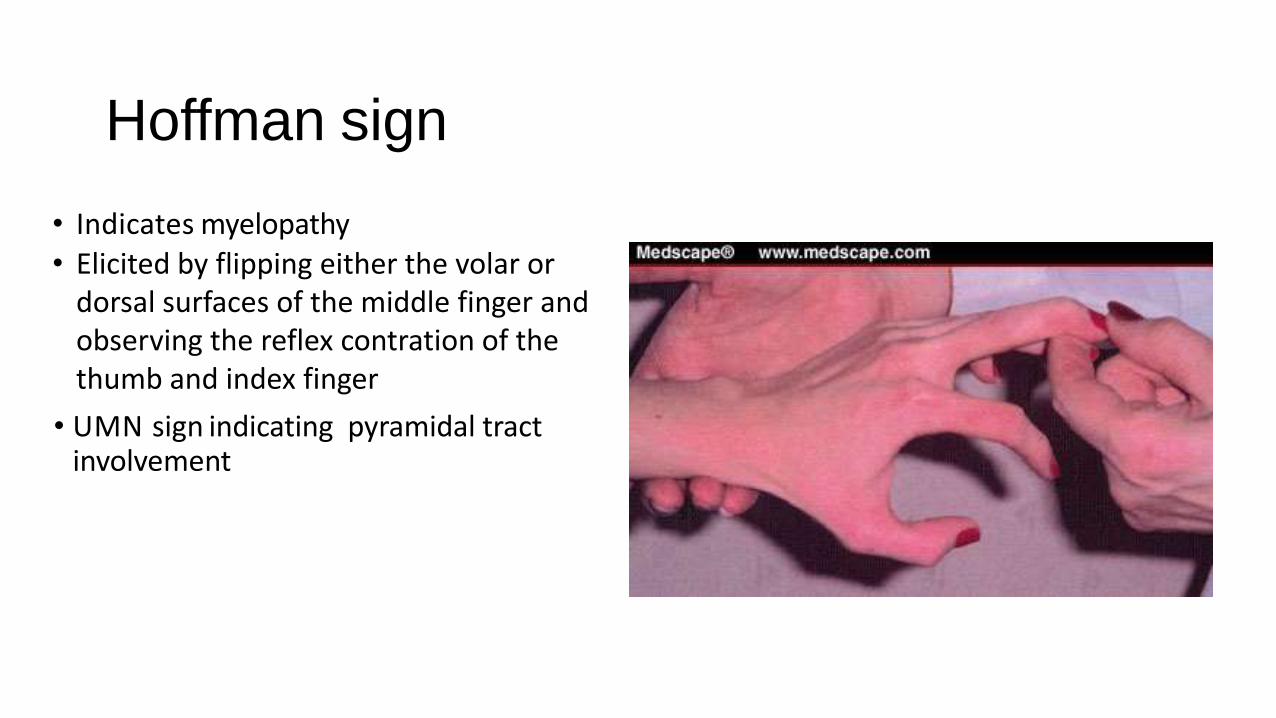
Hoffman sign
• Indicates myelopathy• Elicited by flipping either the volar or
dorsal surfaces of the middle finger and observing the reflex contration of the thumb and index finger
• UMN sign indicating pyramidal tract involvement

Differential Diagnosis

Plain radiographyRole somewhat limited in evaluation of nerve rootsInitial study to rule out instability,congenital abnormalities, fractures, deformity or pathologic changes in bone
Oblique views can show narrowing of the neuroforamina secondary to degenerative changes
INVESTIGATIONS

MRI
MRI has become the method of choice for imaging the neck to detect significant soft-tissue pathology, such as disc herniation and spinal stenosis is due to the intrinsic contrast and good spatial resolution
The American College of Radiology recommends routine MRI as the most appropriate imaging study in patients with chronic neck pain who have neurologic signs or symptoms but normal radiographs
Sagittal T1 - Hypointense signal is common for herniated degenerative disks,calcified ligaments, and bone spurs, making differentiation of these structuresmore difficult
Axial T1 - Insight into both intraspinal and extraspinal disorders, as well as the intrathecal nerve root anatomy
T2-weighted sequence or variants - “myelo-graphic” view

T1- Weighted image T2- Weighted imageCSF is Dark CSF is Bright
Mid Sagittal View is the Optimal view to visualize the spinal cord, CSF and Vertebral Bones. But it may not be optimal view the disk herniation as most are posterolateral as opposed to straight posterior.

T1-weighted-MRI-of-the-cervical-spine-Large-posterior-disc



Cervical myelogram• Outlines Spinal Cord and exiting nerve roots with
radiopaque dye
• Water-soluble agent may be injected via the C1-2interval, allowing the dye pool to gravitate caudally
• Accuracy has been estimated 67% to 92%. For this reason, cervical myelography is often accompanied by CT
• Excellent visualization of nerves in relation to surrounding osseous structures
• Because the diagnosis of neural compression is inferred only indirectly, the exact nature of the compression is not always clear. For example, with myelography alone, it can be difficult to distinguish between a “hard disc” with bony osteophytes and a “soft disc” herniation

Computed Tomography
• CT allows for the direct visualization of pathology causing compression of neural structures
• CT also has a high spatial resolution and is especially helpful in visualizing the foraminal region.
• Distinguish neural compression caused by soft tissue from compression related to bony structures

Electrodiagnosis plays a critical role• Referred to as an extension of neurologic examination, as it is able to provide physiologic evidence of nerve dysfunction
1. EMG
2. Motor and sensory nerve conduction studies
ELECTROMYOGRAPHY (EMG)• Localize lesions to a particular root level
• The goal -- find a pattern of spontaneous and/or chronic motor unit changes in a clear myotomal pattern
• The needle electrode portion of the EMG is performed by analyzing multiple muscles within the same myotome and in adjacent myotomes.
• The presence of fibrillation potentials and positive sharp waves at rest is indicative of denervation, but these changes may not occur until 3 weeks after the onset of neural injury.
• Limitations –can only detect change in the motor nervous system
• To diagnose radiculopathy electrodiagnostically, needle study of 2 muscles that receive innervation from the same nerve root, preferably via different peripheral nerves, should beabnormal.
• Adjacent nerve roots should be unaffected unless a multilevel radiculopathy is present
NERVE CONDUCTION STUDIES• Nerve conduction studies are performed to exclude peripheral nerve pathology.
• The amplitude, distal latency, and conduction velocity can be measured.
• The amplitude corresponds to the number of intact axons.
• The distal latency and conduction velocity reflect the degree of myelination.
• The primary role -- determine if other neurologic processes exist as an explanation for a patient’s clinical picture, or if another process coexists with a root level problem
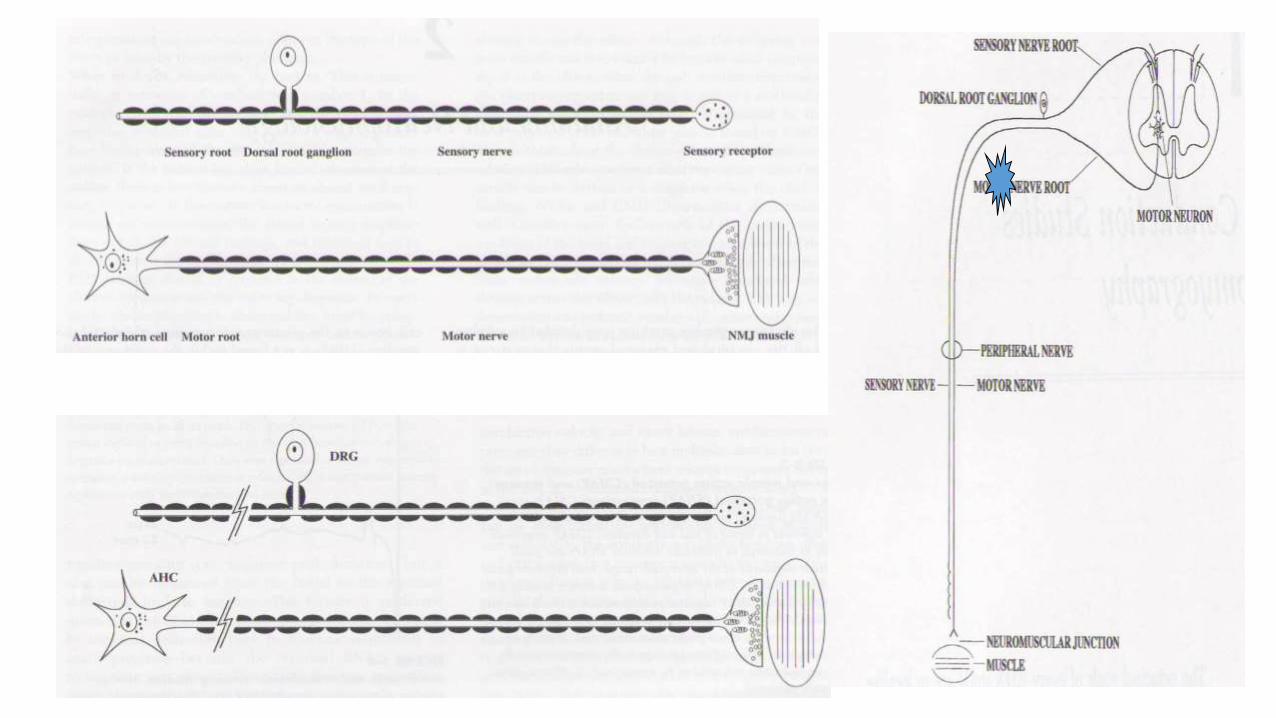
• In pure radiculopathy, the sensory nerve studies should be normal.
• Pathologic lesion in radiculopathy typically occurs proximal to the dorsal root ganglion(DRG). Since the DRG houses the cell bodies for the sensory nerves, the sensory nerve studies should be normal.
• Common nerve entrapments such as median neuropathy at the wrist or ulnar neuropathy at the elbow

Treatment Algorithm


ImmobilizationSoft Collar
• The aim is to reduce pressure on the nerve rootand improve the pathophysiology resulting fromcompression i.e. the health of the nerve
• Some advocate short course (one week) of neckimmobilization may reduce symptoms in theinflammatory phase
• Cervical collar has not been proven to alter thecourse or intensity of the disease process
• Adverse effects - especially when used for longerperiods of time. It is feared that a long period ofimmobilization, can result in atrophy-relatedsecondary damage
PATIENT EDUCATION
• Minimal driving as it will continue aggravating their neck from turning too far into painful range.
• Educate about typical aggravating and easing factors as well as appropriate positions for rest and sleeping.
• Follow the guidelines given by doctor for each medication and not to stray from the dosage.

Traction• Distracts neural foramen and decompresses nerve root
• Typically, 8 to 12 lb of traction at approximately 24 degrees of flexion for 15- to
20-minute intervals
• Most beneficial when acute muscular pain has subsided
• Not be used in patients who have signs of myelopathy!
• “Some studies have shown mechanical traction to be effective within the first 6
weeks of injury” (Caridi, Pumberger & Hughes., 2011, p. 268).
• “Five studies have looked at traction as a treatment for radiculopathy. Traction
was temporarily efficacious in relieving patient’s symptoms; however, none of
the studies included standardized outcome measures” (Caridi, Pumberger &
Hughes., 2011, p. 268).

Physical therapy
• Aerobic exercise
• Postural awareness
• Spinal extensor strengthening
• Thermotherapy
• Acupuncture

SPINAL MANIPULATIVE THERAPY & MOBILIZATIONDescrbed as external force applied to the patient by the hand, an instrumental device resulting in movement and/or separation of the joint articular surfaces with high or low velocity of joint movement
Evidence low in quality

Pharmacological management
NSAIDs - effects on pain and inflammation
In general, 10-14 days of regular dosing is all that is needed tocontrol pain and inflammationMUSCLE RELAXANTS Cyclobenzaprine and Chlorzoxazone
Oral steroids - reduce the associated inflammation from compression
No controlled study exists
Longer-term use is not recommended
Tricyclic antidepressants - adjunct in controlling radicular pain
Opioid medications - generally not necessary for pain relief, but can be used when other medications fail to provide adequate relief

The Neuropathic Pain Special Interest Group. (NeuPSIG) Pharma Recommendations Finnerup et al 2015

Epidural Steroid injection
Principle- steroid decreases pain andinflammation at the site, decreases PG
Indication –◦ Radicular pain unresponsive to non-
interventional care for 1-2 months
◦ Patients without progressive neurological deficit or cervical myelopathy can be considered before sx
Complications◦ Dural puncture, vasovagal reaction, facial
flushing, fever, nerve root injury, pneumocephalus, epidural hematoma, subdural hematoma, stiff neck, transient paresthesias, hypotension, respiratory insufficiency, transient blindness and
Surgery
Disabling motor weakness of 6 weeks duration or less (i.e., deltoid palsy, wrist drop)
Progressive neurologic deficit
Static neurologic deficit + radicular or referred pain
Instability or deformity of functional spinal unit + radicular symptoms
Surgical Management of Cervical Radiculopathy, Todd J. Albert, MD, and Samuel E. Murrell, MD, J Am Acad Orthop Surg 1999;7:368-376
RED FLAGS!!!
Persistent or recurrent radicular symptoms unresponsive to non-operativemanagement for at least 6 weeks

Posterior lamino-foraminotomy (with or without diskectomy)
◦ Burr thins lamina over nerve root
◦ Nerve root exposed
◦ Angled curette can remove additional bone & expand foraminotomy
◦ Disk material can be exposed & removed

Anterior cervical diskectomy and fusion (ACDF)
• Most widely used• Removes ventral compressive
lesion WITHOUT need for retraction of SC
• Disc removed and iliac crest bone autograft placed to ENCOURAGE FUSION
• Nowadays, allografts (no donor sitemorbidity)
• In 1990s, cervical plates wereadded to INCREASE stability and decrease post op bracing

Anterior cervical diskectomy without fusion
• Because of high incidenceof pseudarthrosis afterACDF
• Reported outcomes comparable
• Disk-space collapse and osseous fusion
• There is stress on removal of PLL (buckling of ligament as disk space collapses produces compression of the neural elements) but removes another stabilizing structure
Post anterior cervical diskectomy without fusion Lateral cervical radiograph shows increase in kyphosis. T2-weighted MRI - stenosis, ligamentum and disk bulging, spondylosis, and cord compression

Cervical Disc Arthroplasty
Bryan cervical disk (Medtronic, USA)FlexicoreProDisc-C (Synthes Spine Company, USA)