case 1 pedia henoch schonlein purpura
DESCRIPTION
Henoch Schonlein purpuraTRANSCRIPT

Case presentation
Dulawe, AnneGumiran, JeffersonKotla, Chaitanya KumarMunda Cruz, Reiden Flynn

Informants: Reliability
JF, mother of patient 95%RF, the patient herself
100%

General DataPatient RF 11 year old Filipino Female, a Roman Catholic from Atulayan sur, Tuguegarao cityadmitted at Cagayan Valley Medical Center for the first time on 8:55pm of June 26, 2014. referred from People’s General Hospital on the same day.
Chief complaint:
Pain and edema of left foot.

History of present illness10 days prior to admission
4 nonpruritic flat circumscribed rashes with a diameter of 2mm on patient’s left leg No fever

Before After
Six days prior to admission pain on left ankle Confluent rashes on both legs and dorsum of both feetloss of appetite
consultation at Peoples General Hospital diagnosed with Hypersensitivity reaction Cetirizine, 10 mg per tab 1 tab bedtime for 7 days.
On the night of the same daynausea and vomiting
Mefenamic acid 1 capsule orally given by the mother.
epigastric pain


Four nights prior to admissionNauseavomiting (once) abdominal pain graded as 8 in a scale of 1 to 10 where 10 is the most intense.
Mefenamic acid given by mother with subsequent relief.

Two days prior to admissionEdema of Left footArthralgia on left ankle pain
massaged with oil with no reliefRashes on both thighs.

Few hours prior to admissionpatient’s ankle pain and foot edema worsened hence consultation was sought at People’s general Hospital but was referred to CVMC hence admission.
Past medical Historygenerally healthy as a child several episodes of fever with no associated convulsionsfew episodes of cough and colds but was never hospitalized prior to current hospitalization.Two years ago:
rashes on lower extremities with unrecalled accompanying signs and symptoms diagnosed with Urinary Tract infection given unrecalled medicines said rashes disappeared after 3 days.
no known allergies to drugs or specific foods but was advised to avoid seafoods, dairy products, coffee and junkfoods.

Personal and Social History
youngest of four childrenfather is a 49 year old government employeemother is a 53 year old elementary school teachersiblings had no history of manifesting similar signs and symptoms of current conditionActive in school organizations

Prenatal history
regular prenatal check-ups at Atulayan health center.given one dose of Tetanus toxoid intramuscularlyFerrous and folic supplementationdiet consisting mainly of rice, vegetables and meat and milk excluding coffee and soft drinksdid not smoke cigarettes nor consumed alcoholic beverages. No history of infections, fall/accident, and exposure to radiation8th month of pregnancy
mild vaginal bleeding consultation at CVMC but was referred to St. Paul Hospitalgiven unrecalled medicineadvised on bed rest after which the bleeding subsided

Birth HistoryFull termBorn to a 42 year old G4P4 (4004)Normal spontaneous delivery at home attended by a midwife

Post natal History
born with pinkish bodyminimal vernix caseosaloud cry good suckImmediate post natal care was administered by midwife.
ImmunizationsCompleted before 1 year old
single dose of BCG3 doses of DPT, OPV and Hepa-Bsingle dose of Measles
BCG booster was not given
Nutritional historybreast fed for the first 2 months mixed fed thereafter Solid foods introduced 6 months of agenormally has good appetitepreferred soft drinks and junk foods for snacks
Developmental milestones
Patient is an academic achiever ranking first in her class.
Classic theories
Age Psychosexual theory
Psychosocial theory
Cognitive theory
School age (6-12 y/o)
latency Industry vs inferiority
Concrete operational
Family historyPaternal side:
(+) HPN (+) DM (-) Asthma (-) Ca (-) TuberculosisMaternal Side:
(+) Ca- an uncle died due to liver caner(+) HPN- Both grandparents died of stroke
Review of systems Integumentary: no pruritus, no burning
sensation CNS: no convulsions, no faintness or loss of
consciousness, HEENT: no headache, no blurring of vision, no
tinnitus or ear ache Cardio-Respiratory: no cough, no difficulty of
breathing, no palpitations GIT: no dysphagia, no constipation nor diarrhea GUT: no dysuria, no hypogastric pain
Review of systems (cont.)
Musculoskeletal: No muscle weakness or muscle pain Hematology: no unexplained bruises Endocrine: no excessive sweating, no sensitivity to hot or
cold temperature Reproductive: Menarch- 10 y/oDuration of menstrual cycle: 28 to 32 daysCharacter of menstrual bleeding:
duration: 6 daysquantity : first two days- 3 almost fully soaked pads per
day then succeeding days- 3 half soaked to minimally soaked
pads per day for the

PHYSICAL EXAMINATIONGeneral Survey:
Patient is awake, conscious, coherent and afebrile, not irritable, active and not in respiratory distress.Vital Signs:
Temperature: 36.5 ᵒ CHeart rate: 76bpmRespiratory rate: 18 cpm
Anthropometric Measurements: Weight: 35kgsHead Circumference : 53cms
Skin: (+) pallor, (-) jaundice, moist and cold to touch.

HEENT:Head : normocephalic with moist scalp, abundant and
evenly distributed dark hairEyes : pale conjunctiva, pupils equally round and reactive
to light accommodation, no periorbital edemaEars: symmetrical and no discharges Nose: no discharges and (-) nasal flaringMouth: no hyper salivationNeck: no cervical lymphadenopathy, no mass and no
nuchal rigidity

Lungs: Breathing spontaneously with symmetrical chest expansion, no rales on all lung fields
Heart: adynamic precordium, PMI at 5th intecostal left midclavicular line,normal rate, regular rhythm a no murmur.
Abdomen: soft, globular abdomen with normoactive bowel sound, no tenderness , (-) palpable mass
Genitalia: Tunner stage III Extremities: no edema, pinkish nail beds, CRT 1-
2 seconds, full and equal pulses, 10 toes and hand digits

Neurological ExaminationCerebral: conscious and coherentCerebellar: (-) nystagmus

Cranial Nerves:CN1: able to smellCN2: pupils equally round and
reactive to lightCN3,4, and 6: no ptosisCN5: grimacesCN7: no facial symmetryCN8: respond to verbal
commands and inquiries appropriately CN9 and 10: good gag reflexCN11: can shrug her shoulder
and turn face against resistance CN12: no tongue deviation

Motor System: (Muscle bulk, tone, and strength)
Able to move extremities in all directions (grade 5/5)Sensory System: (pain, temperature, light touch, vibration, discrimination)
All fours 100%

SALIENT FEATURES:General Data:
Adolescent (11 years old), femaleHistory:
Skin: Macular rashesGI: Abdominal pain, nausea
and vomitingMuskuloskeletal: (+)
arthralgia, edema of dorsum left foot

IMPRESSION
Henoch- Schonlein Purpura
RULE IN RULE OUT
arthralgia biphasic fever
Macular purpura/ rash
myalgia
Abdominal pain
Lymphadenopathy
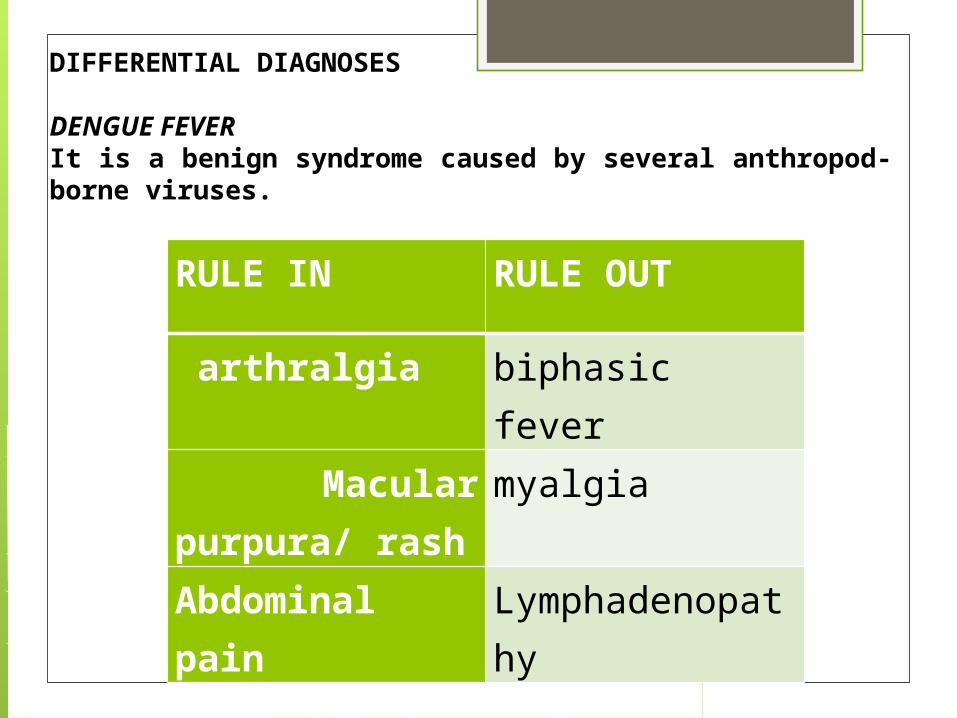
DIFFERENTIAL DIAGNOSES
DENGUE FEVERIt is a benign syndrome caused by several anthropod- borne viruses.
RULE IN RULE OUT
abdominal pain Weight loss
purpura painful nodules
Arthralgias myalgias
testicular pain
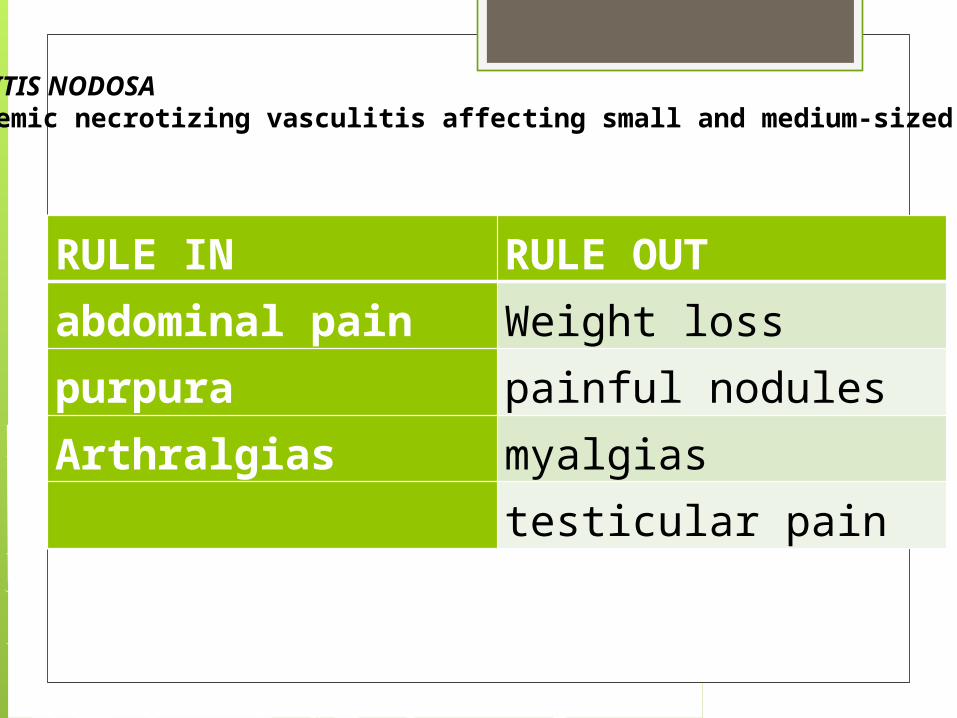
POLYARTERITIS NODOSAis a systemic necrotizing vasculitis affecting small and medium-sized arteries.
RULE IN RULE OUTAge at onset <16 years old
Quotidian fever for at least 3 days andaccompanied by ≥1 of the following:1. Evanescent (nonfixed) erythematous rash.2. Generalized lymph node enlargement.3. Hepatomegaly or splenomegaly or both.4. Serositis.
Arthritis Easy fatigabilityNonpruritic rash
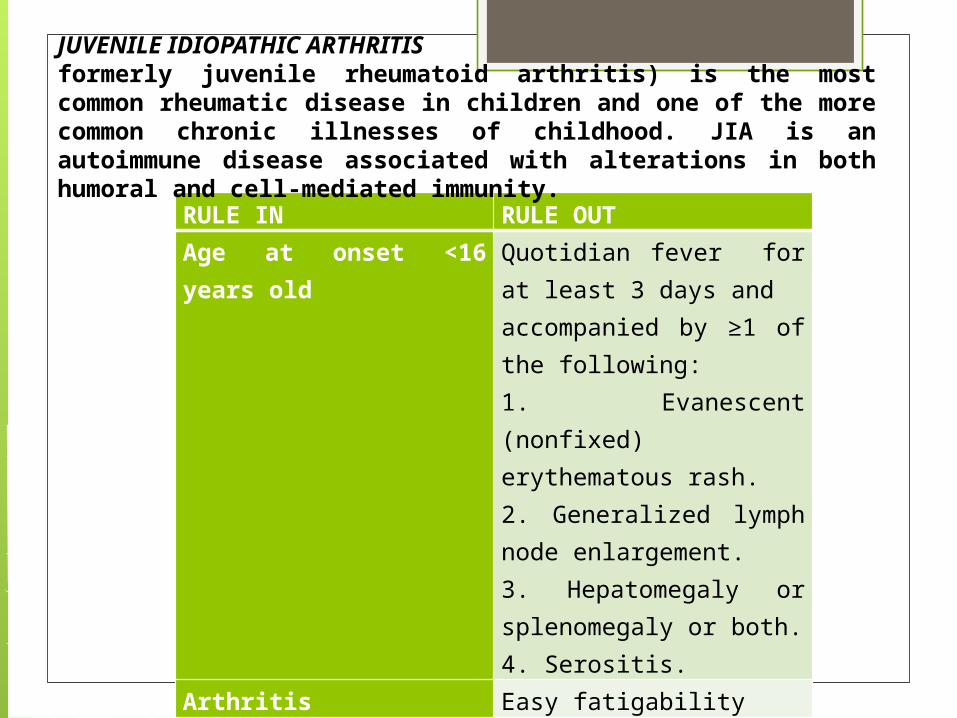
JUVENILE IDIOPATHIC ARTHRITISformerly juvenile rheumatoid arthritis) is the most common rheumatic disease in children and one of the more common chronic illnesses of childhood. JIA is an autoimmune disease associated with alterations in both humoral and cell-mediated immunity.

RULE IN RULE OUTArthritis, arthralgias,
Fatigue, anorexia, weight loss, fever, lymphadenopathy
tendonitis, myositis, myalgias, avascular necrosis, osteoporosis
Nonpruritic rash Malar rash, discoid rash
SYSTEMIC LUPUS ERYTHEMATOSUSis a chronic autoimmune disease characterized by multisystem inflammation and the presence of circulating autoantibodies directed against self-antigens.

Case Discussio
n
HENOCH SCHONLEIN PURPURAis the most common vasculitis of childhood and is characterized by leukocytoclastic vasculitis and immunoglobulin (Ig) A deposition in the small vessels in the skin, joints, gastrointestinal tract, and kidney. EPIDEMIOLOGY- HSP occurs worldwide and affects all ethnic groups. - incidence of HSP is estimated at 14-20/100,000 children per year and affects males more than females, with a 1.2-1.8 : 1 male: female ratio. usually - - between the ages of 3 and 10 yr. - more common in the fall, winter, or spring and is unusual in summer months. - Many cases of HSP follow a documented upper respiratory infection.
PATHOLOGY - In all tissues, immunofluorescence identifies IgA deposition in walls of small vessels, accompanied to a lesser extent by deposition of C3, fibrin, and IgM.

PATHOGENESISThe exact pathogenesis of HSP remains unknown.Given the frequency of preceding upper respiratory infections, including group A streptococcal infections, an infectious trigger is suspected. The common finding of deposition of IgA, specifically IgA1, suggests that HSP is a disease mediated by IgA and IgA immune complexes.Suggestive of genetic components
CLINICAL MANIFESTATIONSThe hallmark of HSP is its rash: palpable purpura starting as pink macules or wheals and developing into petechiae, raised purpura, or larger ecchymoses. Occasionally, bullae and ulcerations develop. The skin lesions are usually symmetric and occur in gravity-dependent areas (lower extremities) or on pressure points (buttocks). The skin lesions often evolve in groups, typically lasting 3-10 days, and may recur up to 4 mo after initial presentation. Subcutaneous edema localized to the dorsa of hands and feet, periorbital area, lips, scrotum, or scalp is also common. Musculoskeletal involvement, including arthritis and arthralgias, is common, occurring in up to 75% of children with HSP. The arthritis tends to be self-limited and oligoarticular, with a predilection for the lower extremities, and does not lead to deformities.

DIAGNOSISThe diagnosis of HSP is a clinical one and is often straightforward when the typical rash is present. However, in at least 25% of cases, the rash appears after other manifestations, making early diagnosis challenging. The differential diagnosis for HSP depends on specific organ involvement but usually includes other small vessel vasculitides, infections, coagulopathies, and other acute intra-abdominal processes.
LABORATORY FINDINGSNo laboratory finding is diagnostic of HSP. Common but nonspecific findings include leukocytosis, thrombocytosis, mild anemia, and elevations of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Occult blood is frequently found in stool specimens. Autoantibody testing is not useful diagnostically except to exclude other diseases. Serum IgA values are often elevated but are not routinely measured. Assessment of renal involvement with blood pressure, urinalysis, and serum creatinine is necessary. Ultrasound is often used in the setting of gastrointestinal complaints to look for bowel wall edema or the rare occurrence of an associated intussusception. Barium enema can also be used to both diagnose and treat intussusception. Although often unnecessary in typical HSP, biopsies of skin and kidney can provide important diagnostic information, particularly in atypical or severe cases.
TREATMENTTreatment of HSP is supportive, with an emphasis on assuring adequate hydration, nutrition, and analgesia. Controversy continues concerning the appropriate use of glucocorticoids in the management of HSP, but steroids are most often used to treatsignificant gastrointestinal involvement or other life-threatening manifestations. Empiric use of prednisone (1 mg/kg/day for 1 to 2 wk, followed by taper) reduces abdominal and joint pain but does not alter overall prognosis nor prevent renal disease. Chronic HSP renal disease is managed with a variety of immunosuppressants, including azathioprine, cyclophosphamide, and mycophenolate mofetil. End-stage renal disease develops in up to 8% of children with HSP nephritis.

COMPLICATIONSAcutely, serious gastrointestinal involvement such as intestinal perforation imparts significant morbidity and mortality. Renal disease is the major long-term complication, occurring in 1-2% of children with HSP. Renal disease can develop up to 6 mo after diagnosis but rarely does so if the initial urinalyses findings are normal. It is recommended that children with HSP undergo serial monitoring of blood pressure and urinalyses for 6 mo after diagnosis, especially those who presented with hypertension or urinary abnormalities.

PROGNOSISOverall, the prognosis for childhood HSP is excellent, and most children experience an acute, self-limited course. About 30% of children with HSP experience one or more recurrences, typically within 4-6 mo of diagnosis. With each relapse, symptoms are usually milder than at presentation. Children with a more severe initial course are at higher risk for relapse. Chronic renal disease develops in 1-2% of children with HSP, and approximately 8% of those with HSP nephritis go on to have end-stage renal disease.

THANK YOUPo..