acute gastroenteritis (meta)
DESCRIPTION
dadfafdadsadsadsaTRANSCRIPT

1
A Case Study On
Acute Gastroenteritis
In Partial Fulfillment of the Requirements
In NCM103N- Related Learning Experience
Metabolism Concept
Submitted to:
Ms. Trina S. Domanais RN MN MAN
Clinical Instructor
Submitted by:
FsCrestine N. Buga-ay St.N
Cyrus Jean S. DestorSt.N
Marigold Anne Diaz St.N
Nada A. PaguitalSt.N
Ramon Bien E. PatrataSt.N
July 04, 2013

2
TABLE OF CONTENTS
Introduction 3
Objectives 5
Initial Data Base 7
Biographic Data 7
Clinical Data 7
Family Health History 8
Past Health History 8
History of Present Illness 9
Definition of Diagnosis 10
Physical Assessment 12
Anatomy and Physiology 15
Pathophysiology 26
Etiology
Symptomatology 26
Schematic Tracing of the Disease 27
Narrative 29
Medical Management 33
Diagnostic Exam 33
Actual
Laboratory Test
Diagnostic Exams
Possible Laboratory & Diagnosis
Therapeutics 62
Drug Study 72
Nursing Care 80
3
Nursing Care Plan 80
Discharge Planning 91
Nursing Theory 93
Prognosis 94
References 96

4
INTRODUCTION
Metabolism is an integral part of the physical and chemical processes in the body that convert
or use energy for bodily functions such breathing, circulating blood, controlling body
temperature, contracting muscles, digesting food and nutrients, eliminating waste through urine
and feces and functioning of the brain and nerves (ADAM, 2011).
We students nurses were task to look for a patient with metabolic problem in accordance to our
metabolism concept. This task involves having the permission of the client to be a part or our
subject for our case study as well as the required consent from the higher authorities. During
our exposure on St. Luke’s ward which mostly handles patients with metabolic problems, we’ve
seen and known patient experiencing different types of metabolic diseases that gives us the
knowledge on what is the actual picture of that certain disease or complication. Also, we’ve
experience alot of complication on that clinical experience because some patient we’re not
cooperating and wants their privacy during their stay on that certain hospital and we have to
accept it because it is a part of their privileges being a client of that institution.
We, the BSN 3B, group 4 subgroup 1 had our 3 weeks and 1 day experience at St. Luke’s Ward
of San Pedro Hospital. Our client is Mr. M.Q, 31 years old who is admitted due to fever and LBM
on June 19, 2013 at 10:15 PM. We chose him as our client since He is fit to be our subject in
our case study for having an Acute Gastroenteritis which is one of the metabolic problems. Also,
He is willing and has the cooperation to answer our queries in accordance with his condition.
Gastroenteritisis also known asgastro, gastric flu, andstomach flu, although unrelated to
influenza. It is the inflammation of the gastrointestinal tract, involving both the stomach and the
small intestine and resulting in acute diarrhea . The inflammation is caused most often by
infection with certain viruses, less often by bacteria or their toxins, parasites, or adverse reaction
to something in the diet or medication.
According to the Centers for Disease Control and Prevention that Worldwide, inadequate
treatment of gastroenteritis kills 5 to 8 million people per year. The Philippine Health Statistics
reported that 971 infants out of 1000 live births died due to Gastroenteritis in the year 2009. And
in Davao City, we have 4, 862 numbers in all ages which is rank as 3rd leading cause of
morbidity in the year 2011 according to City Health Office of Davao City. Gastroenteritis occurs
on individuals in all ages.
5
This case study aims to gather all necessary data that can help provide useful
information for health workers who are interested in learning epilepsy. This study can be used
as data for further nursing research on the topic.
In nursing education we are given the chance to enhance our knowledge with regards on the
disease process and we have also the chance to impart our knowledge on our patient through
giving of health teachings. In nursing research, we are oblige to search more about the disease
as well as its possible causes, it’s treatment and some possible modification of lifestyle. And
finally in nursing practice, our skills were enhance and guided by our clinical instructor to give
the proper medical care that the patient should get to lessen his burdens. Through rendering the
appropriate interventions and management to the client.

6
OBJECTIVES
General Objectives:
That within our 4 weeks span of duty at St. Luke’s Ward, we will be able to present a
comprehensive case study and enhance our skills in developing our nursing capabilities.
Specific Objectives:
The group specifically aims to:
o find a patient that will serve as our subject for our case study;
o establish rapport with the patient and his significant others to gain their trust and
cooperation;
o gather all necessary data through conducting an interview and through reviewing the
patient’s chart;
o perform a thorough cephalocaudal assessment on the client to determine any
abnormalities;
o identify the normal and abnormal findings taken during the cephalocaudal assessment;
o construct an introduction that will serve as an overview of the rotation, case and client;
o formulate general, specific, measurable, attainable, realistic and time-bounded
objectives to serve as our guide;
o collect pertinent personal causes of the client’s present condition specifically the client’s
family lineage, family history, past health history and present health illnesses;
o explain the anatomy and physiology of the affected system of our client’s case;
o trace the pathophysiology of our client’s case along with its predisposing factors,
precipitating factors, etiology and symptomatology;
o explain the medical management for our client’s case which includes the diagnostic and
laboratory examinations, doctor’s orders and the medications administered;
o make five nursing care plans composing of three actual problems and two risk problems;
o render suitable health teachings to the client regarding his conditions;
o discuss the discharge plan and the prognosis on our client’s case; and
o enumerate all the references that we used during the case study.

7
INITIAL DATA BASE
PERSONAL DATA
NAME: Marvin Quinsaat SEX: Male
ADDRESS:B21, L12 Rosalina Village 2, Puan BIRTHDAY: August 17, 1981
AGE: 31 years old BIRTHPLACE: Manila
RELIGION: Agnostic CIVIL STATUS: Single
NATIONALITY: Filipino OCCUPATION: None
MOTHER’S NAME: NenitaQuinsaat FATHER’S NAME: Mario Quinsaat
Live-in partner: Lanee Gonzales
CLINICAL DATA
DATE OF ADMISSION: June 19, 2013 TIME OF ADMISSION: 10:15PM
HOSPITAL: San Pedro Hospital WARD: Sta. Rosa Ward transferred
to St. Luke’s Ward
ATTENDING PHYSICAIN:Dr. Marjorie B. Guillermo CHIEF COMPLAINT: Fever and
LBM
ADMITTING DIAGNOSIS: ADMISSION VS:
Temp. – 38.9˚C
PR- 95 bpm
CR- 101 bpm
RR- 20
BP-110/70
Acute gastroenteritis with moderate dehydration
8
FAMILY HEALTH HISTORY
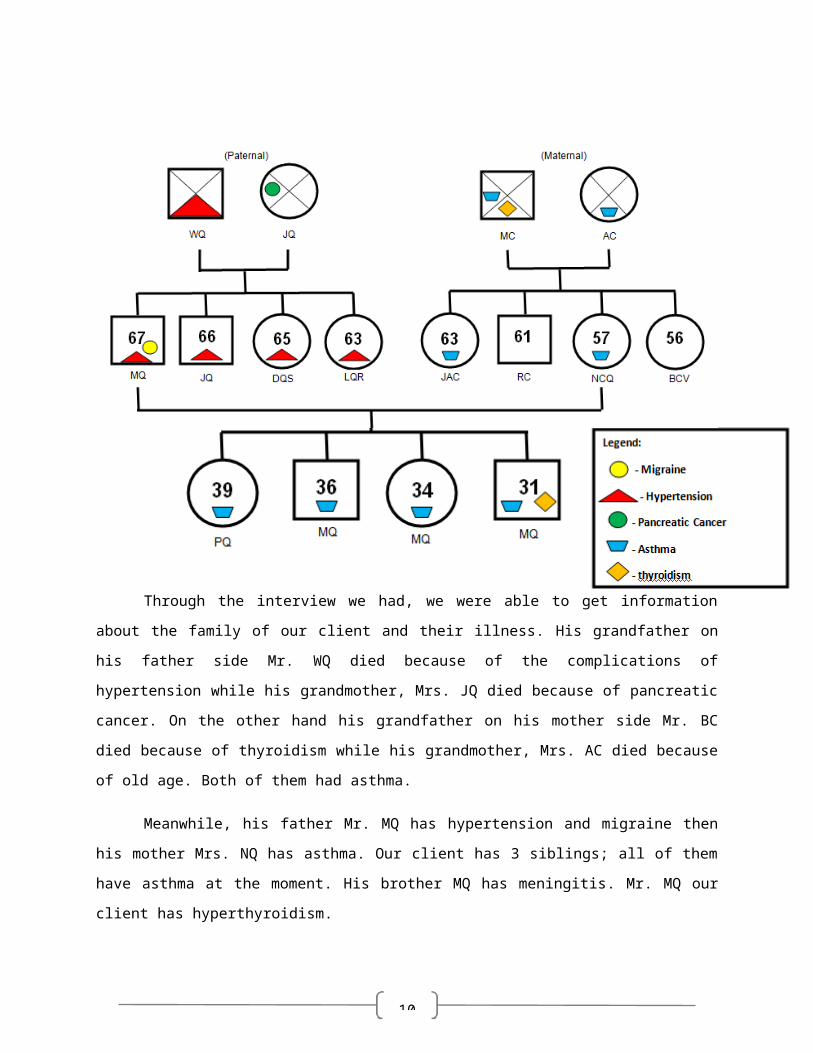
Through the interview we had, we were able to get information about the family of our
client and their illness. His grandfather on his father side Mr. WQ died because of the
complications of hypertension while his grandmother, Mrs. JQ died because of pancreatic
cancer. On the other hand his grandfather on his mother side Mr. BC died because of
thyroidism while his grandmother, Mrs. AC died because of old age. Both of them had asthma.
Meanwhile, his father Mr. MQ has hypertension and migraine then his mother Mrs. NQ
has asthma. Our client has 3 siblings; all of them have asthma at the moment. His brother MQ
has meningitis. Mr. MQ our client has hyperthyroidism.
PAST HEALTH HISTORY
Quinsaat - Cruz

9
Our client had a history of asthma which started at the age of 3. He also told us that he
is a non-alcoholic beverage drinker. But he is a smoker for 15 years with 15-20 sticks/day that
probably one of the causes of his hypothyroidism aside, from his genetic history of thyroidism.
His hyperthyroidism occur 3-4 years ago. His live in partneer Ms. LG told us that our client
doesn’t have any allergies from food and drugs.
PRESENT HEALTH HISTORY
It started 2 days prior to his admission he has an intermittent fever that riches 39+0C.
This was associated with loose stools which is 5 episodes/dayLast June 19, . He took
paracetamol as a temporary relief. 2013 at 10:15pm, our client was admitted at San Pedro
Hospital via wheelchair. Few hours prior to admission our client was having persistent
symptoms with body malaise, dizziness and positive smoker’s cough.
DEFINITION OF DIAGNOSIS
10
Gastroenteritis
An acute inflammation of the gastric and intestinal mucosa which is most commonly due
to bacterial,viral,protozoal, or parasitic infection. It may also be caused by irritation due to
chemical or toxin exposure or allergic response. Viral exposure is more likely in winter; bacterial
exposure is more common in summer when food-borne illness exposure is likely.
Reference:
DiGuilio, M. et al. (2007). Medical-Surgical Nursing Demystified. New York. McGraw Hill.
Gastroenteritis is a condition that causes irritation and inflammation of the stomach and
intestines (the gastrointestinal tract). An infection may be caused by bacteria or parasites in
spoiled food or unclean water. Some foods may irritate your stomach and cause gastroenteritis.
Lactose intolerance to dairy products is one example.
Reference:
WebMD - Better information. Better health. Gastroenteritis (Stomach Flu) Symptoms, Causes,
Treatments. Retrieved July 2, 2013,
fromhttp://www.webmd.com/digestive-disorders/gastroenteritis.
Gastroenteritis (better known as the stomach flu) is an inflammation of the GI tract.
Although gastroenteritis can occur at any age, infants and older adults are at risk of having more
severe symptoms.
Reference:
Hurst, M. (2008). Hurst Reviews: Pathophysiology Reviews. New York. McGraw Hill.
PHYSICAL ASSESSMENT

11
General Survey
During the assessment, the client was wearing a loose t-shirt and baggy pants.
He is in anectomorphic body build. He stands to(height in cm) and weighs (weight in kg). And
his BMI is (bmi). Level of consciousness is alert and oriented. He was in an appropriate mood
and was cooperative during the assessment. He also had and IVF of PNSS 1L @ 140cc/hr
infusing well at left metacarpalvein.
Vital Signs
Vital sign Normal range Result
Blood pressure 10/70-120-80 120/80
Cardiac Rate 60-100 87
Pulse Rate 70-80 80
Respiratory Rate 16-20 20
Skin, Hair, and Nails
His hair was evenly distributed and was well groomed. He had silver strands of hair on
his head. His skin was warm to touch and had good skin turgor, with no discolorations noted.
His finger and toe nails were long and uncut. Capillary bedsrefilledat 2 seconds.
Head and Neck
His head was symmetrical and round in shape, erect and is midline. And also, neither
lesions nor masses were noted upon palpation. His neck was symmetrical with head centered.
(add thyroid assessment here). Lymph nodes were not palpable.
Eyes
His pupils were equally round and reactive to light stimulation and accommodation. His
eyes move symmetrically. Visual acuity of 150 - 100, he was wearing glasses.
Ears
12
His ears had the same color as the facial skin, symmetrical in position, firm and
not tender. Pinna recoils after it is folded. Presence swelling or odorous discharges were not
noted on both ears. Hearing acuity is normal.
Nose and Sinuses
The color of the nose is the same with as the rest of the face; nasal structure is
smooth and symmetrical; and the client reports no tenderness upon palpation. Sinuses were not
tender upon palpation.
Mouth and Pharynx
His lips appeared dry and pale. He has 28 teeth light yellowish in color with no
dental carries. Gums are pink, moist, and firm with tight margins to the teeth. No lesion noted.
The buccal area was also pink and moist with no lesion. The tongue was able to move freely,
with sublingual frenulum intact and midline. The uvula was fleshy, and hangs freely in midline.
Neck?
Breasts and Axillae
The areolar area and nipples were not inspected due to client’s refusal. According to
patient’s verbalization, the nipples were symmetrical with negative inversion, discharges,
crusting, and masses. Both axillas were noted to be free from rashes and infections.
Thorax and Lungs
His anteroposterior transverse ratio was 1:2. He had a (tattoo description here) on his
chest. Clear breath sounds upon auscultation of both lung fields with no adventitious sounds
noted. Upon palpation, vocal fremitus was symmetrical.
Heart
No murmurs skip beats, noted upon auscultation. (add other assessment here).
Abdomen
(add abdominal Assessment here). Hndikokasinakia nag tyannya.:D
Genitourinary
13
Client refused visualization of the genitalia.
Musculoskeletal
The muscles on both sides of the body had no contractures and tremors. Muscle
weaknesses were not noted on both lower and upper extremities.

14
ANATOMY AND PHYSIOLOGY
The GI System
The gastro-intestinal system is essentially a long tube running right through the body, with
specialised sections that are capable of digesting material put in at the top end and extracting
any useful components from it, then expelling the waste products at the bottom end. The whole
system is under hormonal control, with the presence of food in the mouth triggering off a
cascade of hormonal actions; when there is food in the stomach, different hormones activate
acid secretion, increased gut motility, enzyme release etc. etc.
Nutrients from the GI tract are not processed on-site; they are taken to the liver to be broken
down further, stored, or distributed.
The Esophagus

15
Once food has been chewed and mixed with saliva in the mouth, it is swallowed and
passes down the oesophagus. The oesophagus has a stratified squamous epithelial
lining (SE) which protects the oesophagus from trauma; the submucosa (SM) secretes
mucus from mucous glands(MG) which aid the passage of food down the oesophagus.
The lumen of the oesophagus is surrounded by layers of muscle (M)- voluntary in the top
third, progressing to involuntary in the bottom third- and food is propelled into the
stomach by waves of peristalisis.
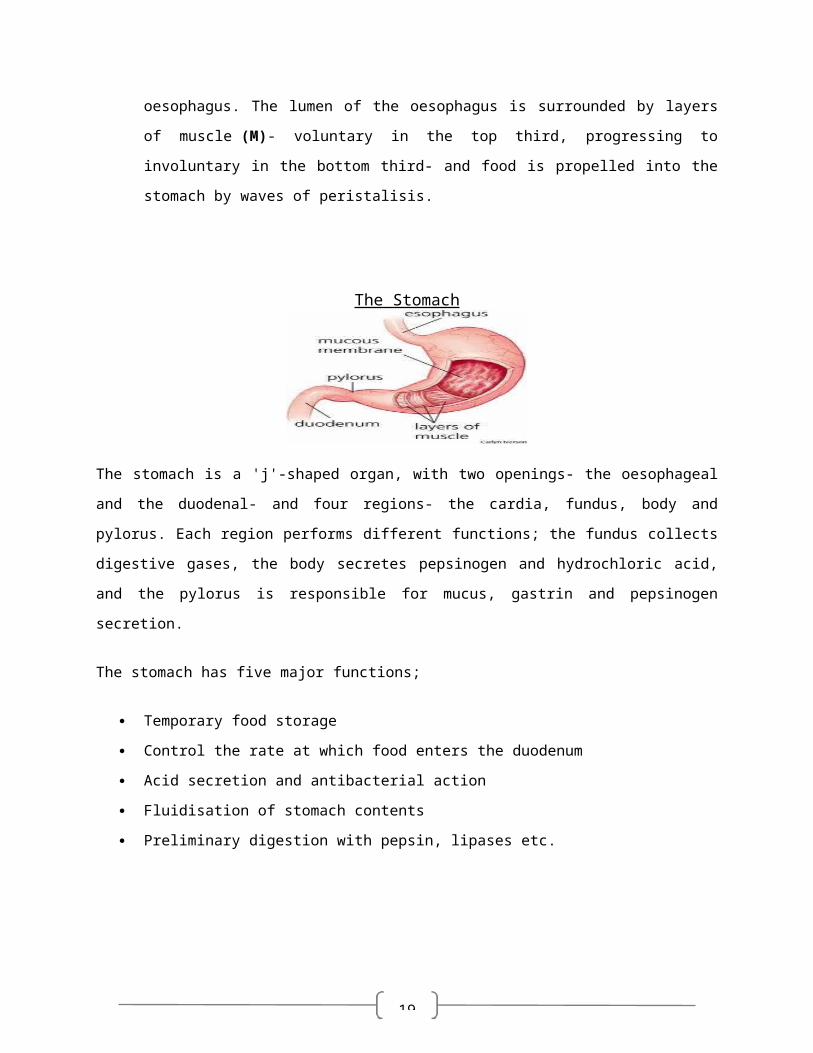
The Stomach
The stomach is a 'j'-shaped organ, with two openings- the oesophageal and the duodenal- and
four regions- the cardia, fundus, body and pylorus. Each region performs different functions; the
fundus collects digestive gases, the body secretes pepsinogen and hydrochloric acid, and the
pylorus is responsible for mucus, gastrin and pepsinogen secretion.
The stomach has five major functions;
Temporary food storage
Control the rate at which food enters the duodenum
Acid secretion and antibacterial action
Fluidisation of stomach contents
Preliminary digestion with pepsin, lipases etc.
G- mucosa containing glandular tissue; different areas of the stomach contain different
types of cells which secrete compounds to aid digestion. The main types involved are:
o parietal cells which secrete hydrochloric acid
o chief cells which secrete pepsin
16
o enteroendocrine cells which secrete regulatory hormones.
MM- muscularis mucosae
SM- submucosa
The stomach contains three layers of involuntary smooth muscle which aid
digestion by physically breaking up the food particles;
o OM- inner oblique muscle
o CM- circular muscle
o LM- outer longitudinal muscle
The Small Intestine
The small intestine is the site where most of the chemical and mechanical digestion is carried
out, and where virtually all of the absorption of useful materials is carried out. The whole of the
small intestine is lined with an absorptive mucosal type, with certain modifications for each
section. The intestine also has a smooth muscle wall with two layers of muscle; rhythmical
contractions force products of digestion through the intestine (peristalsis). There are three main
sections to the small intestine;
Duodenum forms a 'C' shape around the head of the pancreas. Its main function is to
neutralize the acidic gastric contents (called 'chyme') and to initiate further
digestion; Brunner's glands in the submucosa secrete an alkaline mucus which
neutralizes the chyme and protects the surface of the duodenum.
Jejunum where most chemical digestion takes place

17
Ileum. The jejunum and the ileum are the greatly coiled parts of the small intestine, and
together are about 4-6 metres long; the junction between the two sections is not well-
defined. The mucosa of these sections is highly folded (the folds are called plicae),
increasing the surface area available for absorption dramatically.
The epithelial surface of the plicae (P) is further folded to form villi(V). These increase
the surface area of the small intestine still further, and the surface of each villus is
covered in small microvilli to maximise surface area- the area available for absorption is
vast. Each villus has its own blood supply- the vessels can be seen in the
submucosa (SM)- and blood containing digestive products from the small intestine is
taken to the liver via the hepatic portal system. The double muscle layer (M) moves food
through the intestine by peristalsis.
The Large Intestine
By the time digestive products reach the large intestine, almost all of the
nutritionally useful products have been removed. The large intestine removes
water from the remainder, passing semi-solid feces into the rectum to be
expelled from the body through the anus. The mucosa (M) is arranged into
tightly-packed straight tubular glands (G) which consist of cells specialized for
water absorption and mucus-secreting goblet cells to aid the passage of feces.
The large intestine also contains areas of lymphoid tissue (L); these can be
found in the ileum too (called Peyer's patches), and they provide local
immunological protection of potential weak-spots in the body's defenses. As the
gut is teeming with bacteria, reinforcement of the standard surface defenses
seems only sensible.

18
Ascending Colon - The ascending colon is comprised of strong muscles that
motor waste products upward and onward out of the body. As part of the larger
gastrointestinal tract, the ascending colon connects and continues the work of
the small intestine in moving food along on its journey through the body.
Transverse Colon - helps stabilize fluid levels and prepare the body for the
expulsion of waste
Descending Colon - to store food that will be emptied into the rectum;
its function is primarily the absorption of water from fecal matter
Rectum - store your feces and provide force to force feces out of your body
through the anus
19
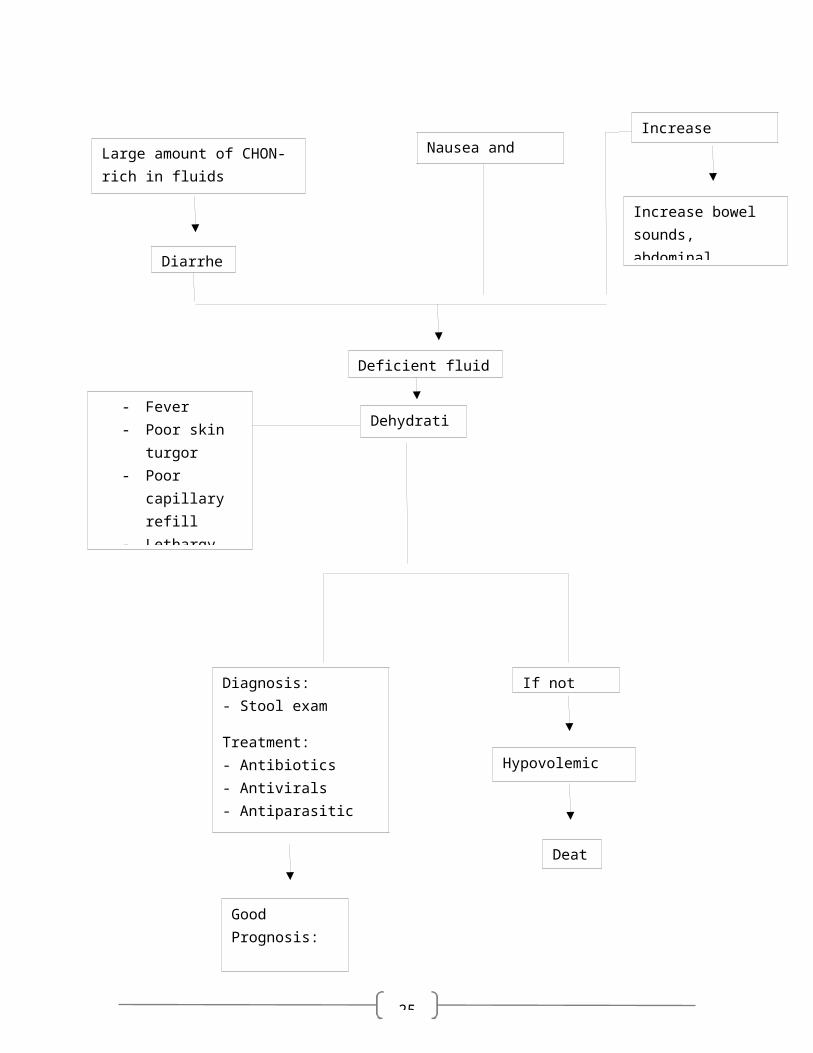
Release of enterotoxins and attachment of microorganisms to mucosal epithilium
Increase secretion of water and electrolytes
Inhibits Sodium reabsorption
Large amount of CHON-rich in fluids
Diarrhea
Decrease intestinal wall integrity
Parasympathetic and sympathetic stimulation
Decrease intestinal absorption
Stimulation of the emetic center
Nausea and vomiting
Increase gastrocolic reflex
Increase peristalsis
Increase bowel sounds, abdominal cramping and abdominal pain
PREDISPOSING FACTORS
- Age- Geographical Location
PRECIPITATING FACTORS
- Unsanitary food handling - Poor environmental condition- Lifestyle (habitual eating of street
foods)
PATHOPHYSIOLOGY
Ingestion of food contaminated with bacteria (Salmonella, Shigella,Campylobacter, Clostridium, E. coli and Aeromonas species), viruses (rotavirus, norovirus, adenovirus) or parasites

20
PATHOPHYSIOLOGY OF ACUTE GASTROENTERITIS
Viruses and bacteria spread from person to person by means of the fecal-oral route or
by direct ingestion of contaminated foods cause gastroenteritis. Some viruses such as
the norovirus may be transmitted by an airborne route. Once these microorganisms have
been ingested, they will release enterotoxins that may damage and outnumber normal
bacteria and attach themselves in the bowel wall causing a decrease in intestinal wall
integrity and would cause inflammation in the stomach and intestine. Once this will
Dehydration
Good Prognosis:
RECOVERY
If not treated
Hypovolemic Shock
Death
Deficient fluid volume
- Fever- Poor skin turgor- Poor capillary
refill- Lethargy- Weakness- Weight loss
Diagnosis:- Stool exam
Treatment:- Antibiotics- Antivirals- Antiparasitic- ORS

21
happen, there would be a stimulation of the emetic center in the brain caused by the
parasympathetic and sympathetic stimulation which would eventually lead to vomiting.
There would also be a decrease intestinal absorption and increase gastrocolic reflex
which would result to an increase peristaltic movement causing abdominal bowel
sounds, abdominal pain and cramping. In relation to the release of enterotoxins, there
would be an increase secretion of water and electrolytes and Sodium would not
reabsorbed back. Proteins would also increase in the lumen and would lead to greater
chances of dehydration (proteins also play a vital role in holding fluids intracellularly by
oncotic pressure). All of these factors would lead to fluid volume deficiency and
dehydration marked by signs and symptoms such as fever, poor skin turgor, poor
capillary refill, lethargy, weakness and weight loss.
If the patient will not be treated, he/she may undergo hypovolemic shock and
death. If treated, patient will have a good prognosis and will have a better chance of
recovering.
LABORATORY EXAMINATION
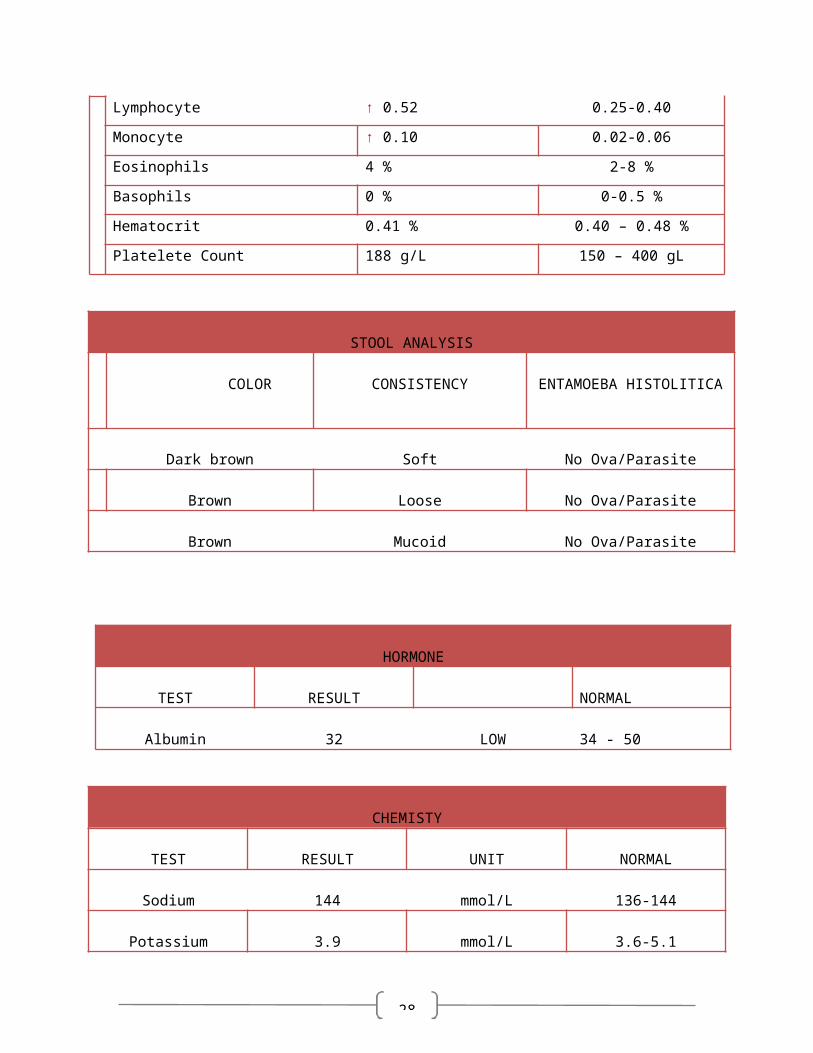
HEMATOLOGY
TEST RESULT NORMAL

22
Hemoglobin ↓132 g/dL 140-180 g/dL
Erythrocytes 5.41/L 4.5-5.0 L
MCH ↓ 24.4 pg 28-33 pg
MCV ↓ 74 fl 82-98 fl
MCHC 34.1 g/dL 33-36 g/L
Leukocyte 5.9 g/L 4.8-10.8 g/L
Neutrophil ↓ 0.33 0.55-0.65
Lymphocyte ↑ 0.52 0.25-0.40
Monocyte ↑ 0.10 0.02-0.06
Eosinophils 4 % 2-8 %
Basophils 0 % 0-0.5 %
Hematocrit 0.41 % 0.40 – 0.48 %
Platelete Count 188 g/L 150 – 400 gL
STOOL ANALYSIS
COLOR CONSISTENCY ENTAMOEBA HISTOLITICA
Dark brown Soft No Ova/Parasite
Brown Loose No Ova/Parasite
Brown Mucoid No Ova/Parasite
HORMONE
TEST RESULT NORMAL
Albumin 32 LOW 34 - 50
CHEMISTY
23
TEST RESULT UNIT NORMAL
Sodium 144 mmol/L 136-144
Potassium 3.9 mmol/L 3.6-5.1
Calcium 2.44 mmol/L 2.23-2.58
ULTRASOUND
THYROID LEFT RIGHT
LENGTH 6.9 cm 5.6 cm
WIDTH 2.9 cm 3.0 cm
THICKNESS 2.8 cm 2.6 cm
THYROID FUNCTION TEST
TEST RESULT INTERPRITATION NORMAL
FT4 > 100 HIGH 12-22
THYROID STIM < 0.005 LOW 0.27-4.2

24
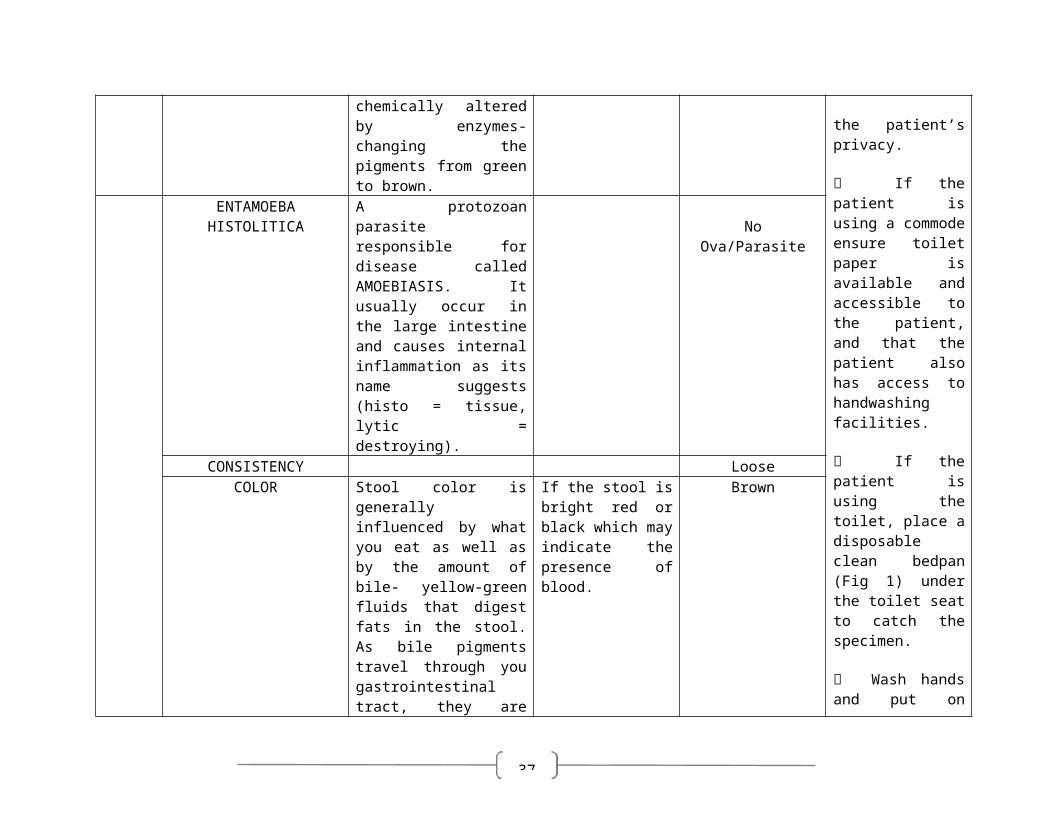
STOOL ANALYSIS
DATE COMPONENTS DEFENITION RATIONALE RESULTNURSING
RESPONSIBILITYENTAMOEBA HISTOLITICA
A protozoan parasite responsible for disease called AMOEBIASIS. It usually occur in the large intestine and causes internal inflammation as its name suggests (histo = tissue, lytic = destroying).
No Ova/Parasite Explain the procedure and the reason it is required clearly and privately to the patient. Obtain informed consent and document that it has been given.
Where appropriate, offer the patient the choice of using either a commode at the bedside or a toilet.
Ensure the bedside curtains are pulled tight or the toilet door is completely shut to protect the patient’s privacy.
If the patient is using a commode ensure toilet paper is available and accessible to the patient, and that the patient also has access to handwashing facilities.
If the patient is using the toilet, place a disposable clean bedpan (Fig 1) under the toilet seat to catch the specimen.
Wash hands and put on gloves (Fig 2).
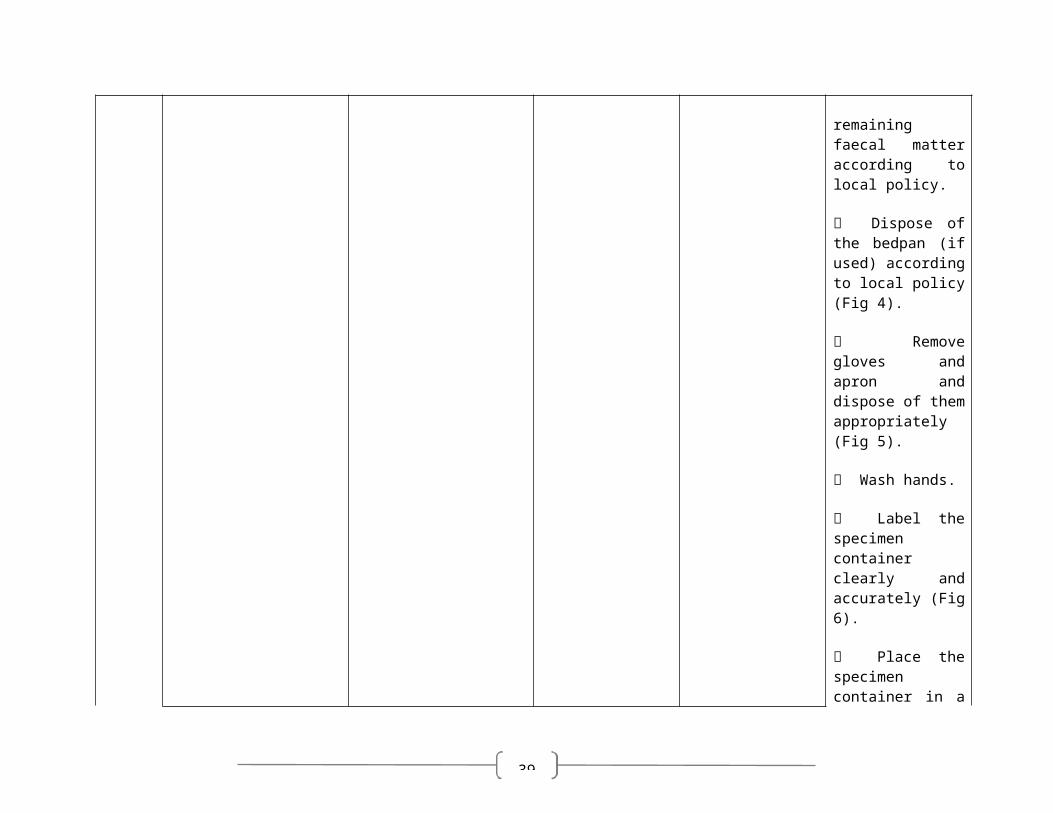
When the patient has produced the sample, examine the stool for consistency, colour, blood or any other abnormality.
Unscrew the top of the specimen
CONSISTENCY softCOLOR Stool color is generally
influenced by what you eat as well as by the amount of bile- yellow-green fluids that digest fats in the stool. As bile pigments travel through you gastrointestinal tract, they are chemically altered by enzymes- changing the pigments from green to brown.
If the stool is bright red or black which may indicate the presence of blood.
Dark Brown
ENTAMOEBA HISTOLITICA
A protozoan parasite responsible for disease called AMOEBIASIS. It usually occur in the large intestine and causes internal inflammation as its name suggests (histo = tissue, lytic = destroying).
No Ova/Parasite
CONSISTENCY LooseCOLOR Stool color is generally
influenced by what you eat as well as by the amount of bile- yellow-green fluids that digest fats in the stool. As bile pigments travel through you gastrointestinal tract, they are chemically altered by enzymes- changing the pigments from green to brown.
If the stool is bright red or black which may indicate the presence of blood.
Brown
ENTAMOEBA HISTOLITICA
A protozoan parasite responsible for disease called AMOEBIASIS. It usually occur in the large
No Ova/Parasite
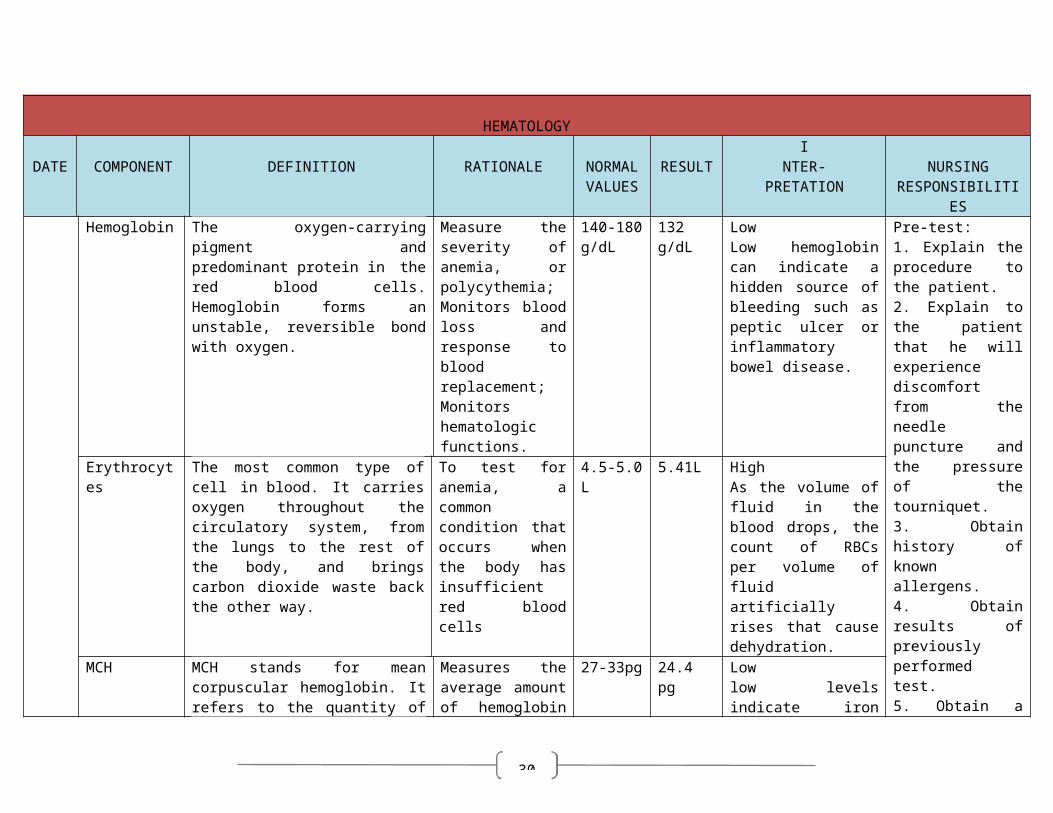
HEMATOLOGY
COMPONENT DEFINITION RATIONALE NORMAL VALUES
RESULTI
NTER-PRETATION
NURSING RESPONSIBILITIE
Hemoglobin The oxygen-carrying pigment and predominant protein in the red blood cells. Hemoglobin forms an unstable, reversible bond with oxygen.
Measure the severity of anemia, or polycythemia; Monitors blood loss and response to blood replacement; Monitors hematologic functions.
140-180 g/dL
132 g/dL LowLow hemoglobin can indicate a hidden source of bleeding such as peptic ulcer or inflammatory bowel disease.
Pre-test: 1. Explain the procedure to the patient. 2. Explain to the patient that he will experience discomfort from the needle puncture and the pressure of the tourniquet. 3. Obtain history of known allergens. 4. Obtain results of previously performed test. 5. Obtain a list of medications the patient is taking. 6. Note any recent procedures that can interfere with the result. 7. Tell the patient and the watcher that there are no fluid, food or medication restrictions, unless by medical direction.
Post-test: 1. Observe venipuncture site for bleeding or hematoma formation.
2. Apply pressure at the site of the venipuncture because bleeding may occur.
3. If hematoma develops, apply warm soaks.
4. Evaluate the results in relation to the patient’s symptoms and
Erythrocytes The most common type of cell in blood. It carries oxygen throughout the circulatory system, from the lungs to the rest of the body, and brings carbon dioxide waste back the other way.
To test for anemia, a common condition that occurs when the body has insufficient red blood cells
4.5-5.0 L 5.41L High As the volume of fluid in the blood drops, the count of RBCs per volume of fluid artificially rises that cause dehydration.
MCH MCH stands for mean corpuscular hemoglobin. It refers to the quantity of hemoglobin in red corpuscles This is a calculated value derived from the measurement of hemoglobin and the red cell count.
Measures the average amount of hemoglobin in the average red cell.
27-33pg 24.4 pg Low low levels indicate iron deficiency or anaemia
MCV Mean corpuscular volume is the average volume of a red blood cell. This is a calculated value derived from the hematocrit and red cell count.
Measures the average volume of a red blood cell.
85-96Fl 74fL LowWhen the number is smaller than normal, the cell is too small and this is a condition that causes microcytic anemia or microcytosis
MCHC Mean corpuscular hemoglobin concentration (MCHC) is the average concentration of hemoglobin in red blood cells
.
MCHC is used to help diagnose the type (cause) and severity of anemia. When MCHC is low, this can mean a person has iron-deficiency anemia. This type of anemia can be caused by insufficient iron in the diet or by blood loss. Blood loss, such as what might occur with tumors in the colon and other parts of gastrointestinal tract can cause low iron levels and a low MCHC.
33-36 g/L 34.1 g/dL
NormalIf the levels fall
between the normal range, the person
does not have to worry about being anemic.
Leukocytes A colorless blood corpuscle capable To count WBC 4.8- 5.9 g/L Normal
25
COLOR Stool color is generally influenced by what you eat as well as by the amount of bile- yellow-green fluids that digest fats in the stool. As bile pigments travel through you gastrointestinal tract, they are chemically altered by enzymes- changing the pigments from green to brown.
If the stool is bright red or black which may indicate the presence of blood.
Brown
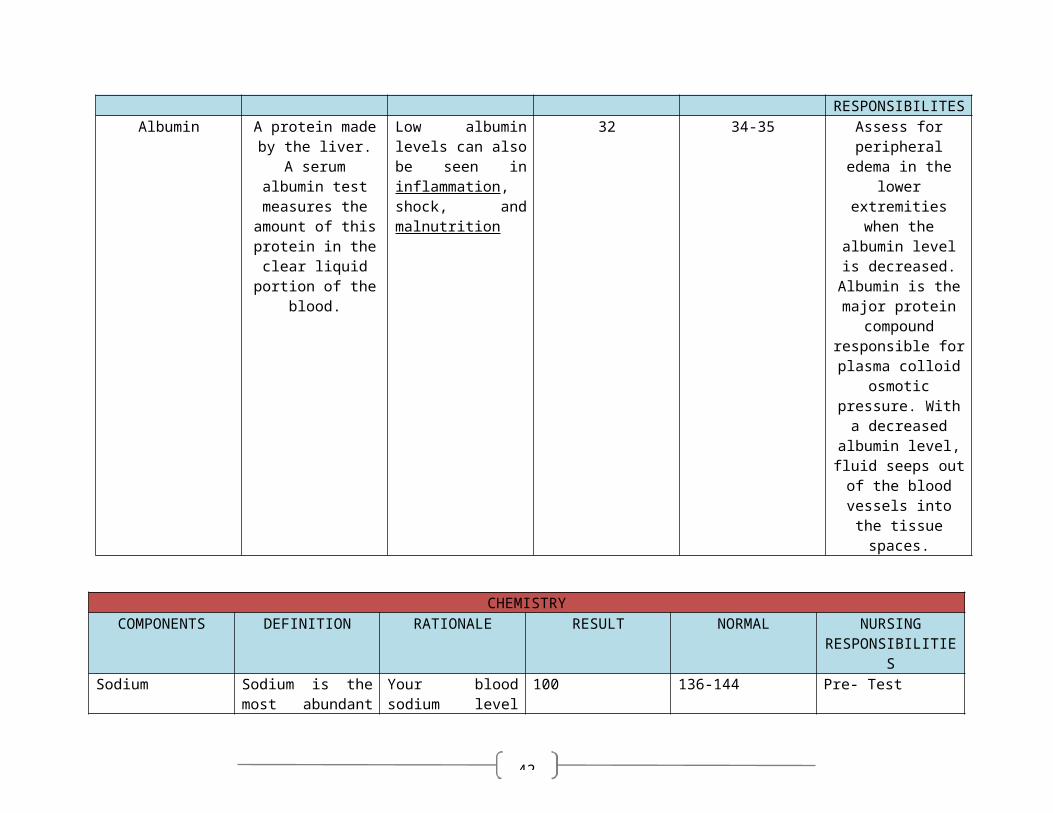
CHEMISTRYCOMPONENTS DEFINITION RATIONALE RESULT NORMAL
Sodium Sodium is the most abundant cation (pronounced cat-ion) in the blood and its chief base. It functions in the body to maintain osmotic pressure, acid-base balance and to transmit nerve impulses.
Your blood sodium level represents a balance between the sodium and water in the food and drinks you consume and the amount in urine
100 136-144
HORMONECOMPONETS DEFINITION RATIONALE RESULT NORMAL NURSING
RESPONSIBILITESAlbumin A protein made by
the liver. A serum albumin test
measures the amount of this
protein in the clear liquid portion of the
blood.
Low albumin levels can also be seen in inflammation, shock, and malnutrition
32 34-35 Assess for peripheral edema in
the lower extremities when
the albumin level is decreased. Albumin is the major protein
compound responsible for plasma colloid
osmotic pressure. With a decreased albumin level, fluid
seeps out of the blood vessels into the tissue spaces.
26
Potassium Potassium regulates the heart and function of the muscle. And he major positive ion (cation) found inside of cells.
The proper level of potassium is essential for normal cell function.
3.9 3.5-5.1
Calcium Calcium is bound to the proteins in the bloodstream, so the level of calcium is related to the patient's nutrition as well as the calcium intake in the diet.
It is important in the transmission of nerve impulses across synapses, the clotting of blood and the contraction of muscles
2.44 2.23-2.58
THYROID FUNCTION TESTCOMPONENTS DEFINITION RATIONALE RESULT NORMAL
FT4 Free T4 measures the free, unbound thyroxine levels in your bloodstream
Free T4 is typically elevated in hyperthyroidism
> 100 12-22

27
THYROID STIMULATING
HORMONE (TSH)
A special messenger hormone that stimulate the thyroid to release more thyroid hormone
TSH that is elevated, or above normal, is considered indicative of hypothyroidism.
<0.005 0.27-4.2
ULTRASOUND
THYROID LEFT RIGHT
LENGTH 6.9 cm 5.6 cm
WIDTH 2.9 cm 3.0 cm
THICKNESS 2.8 cm 2.6 cm*Both thyroid lobes enlarged. Both show heterogeneous parenchymal echopattern. External outline is smooth. No pathologic classification
*Bilateral carotid spaces are intact
*No cervical lymphadenopathy demonstrated
*Impression: thyromegaly with diffuse thyroid parechymal disease
28

29
Medical orders
30
DRUGSTUDY
Date Ordered: June 19, 2013
Generic Name: Propylthiouracil (PTU)
Brand Name:
Classification: Anti-thyroid drug
Mechanism of Action:
Inhibits conversion of the synthesis of thyroid hormones; partially inhibits the peripheral T4 to T3, the more potent form of thyroid hormone.
Indication: Hyperthyroidism
Contraindication:
Allergy Pregnancy
Ordered Dose: 50mg tab BID
Adverse Effects:
CNS: Paresthisias, neuritis, vertigo, neuropaties, depression CV: Vasculitis, periarteritis Dermatologic: Urticaria, pruritus, skin pigmentation, exfoliative dermatitis, lupus-like
syndrome GI: Epigastric distress, loss of taste, jaundice, hepatitis GU: Nephritis Hematologic: Agranulocytosis, granulocytopenia, thrombocytopenia,
hypoprothrombinemia, aplastic anemia
Side Effects:
Nausea Vomiting Skin rash Headache Drowsiness Weakness
Drug Interaction:

31
Increased risk of bleeding with oral anticoagulants Alterations in the ophylline, metoprolol, propranolol, digitalis glycoside clearance, serum
levels and effects as patient moves from hyperthyroid state to eurothyroid state
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug.2. Assess allergy to antithyroid products3. Administer drug in 3 equally divided doses at 8 hour interval 4. Inform patient of the possible side effects of the drug5. Instruct patient to take drug with meals todecrease risk of adverse GI reactions.6. Urge patient to report signs and symptomsof infection, such as fever and
sorethroat, or signs and symptoms that couldreflect hepatic dysfunction, such as anorexia and right-upper-quadrant pain.
7. Advise patient to notify prescriber immediately if he has fatigue, weakness, and vagueabdominal pain, loss of appetite, itching,easy bruising, or yellowing of eyes or skin.
8. Monitor CBC, PT, and liver and thyroidfunction test results in patientstakingpropylthiouracil. Elevated serum triiodothyronine(T3) level may be the soleindicator of inadequate treatment.
Date Ordered: June 19, 2013

32
Generic Name:Paracetamol
Brand Name:Boigesic
Classification: Non-opioid analgesics, Antipyretics
Mechanism of Action:
Inhibits the synthesis of prostaglandins that may serve as mediators of pain and fever, primarily in the CNS.
Reduces fever by acting directly on the hypothalamic heat-regulating center to cause vasodilation and sweating which helps dissipate heat.
Indication:
Mild pain Fever
Contraindication:
Hypersensitivity to acetaminophen or its components Use cautiously with impaired hepatic function, chronic alcoholism, pregnancy, lactation.
Ordered Dose:500mg tab every 4 hours for fever
Adverse Effects:
CV: chest pain, dyspnea, myocardial damage GI: heaptic toxicity and failure, jaundice GU: Acute renal failure, renal tubular necrosis Hematologic: Methemoglobinemia-cyanosis, haemolytic anemia- hematuria, anuria,
neutropenia, hypoglycaemia, leukopenia Hypersensitivity: Rash, urticarial
Side Effects:
Headache Nausea vomiting
Drug Interactions:
Increased toxicity with long term, excessive ethanol ingestion Increased hypoprothrombinemic effect of oral anticoagulants Increased risk of hepatotoxicity Possible decreased therapeutic effects with barbiturates, carbamazepine, hydantoins, rifampin,
sulfinpyrazone

33
Possible delayed or decreased effectiveness with anticholinergics Possible reduced absorption of acetaminophen with activated charcoal Possible decreased effectiveness of zidovudine
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug2. Assess temperature of the patient before giving the medicine.3. Use liquid form for children and patients who have difficulty swallowing.4. Administer with water. 5. Give drug with food if GI upset occurs.6. Discontinue drug if hypersensitivity occurs.7. Ensure patient is not allergic to Paracetamol8. Assess allergic reactions: rash, urticaria; if these occur, drug may have to be discontinued.
Date Ordered: June 19, 2013
Generic Name: Racecadotril

34
Brand Name:Hidrasec
Classification: Antidiarrheal
Mechanism of Action:
Racecadotril is an antihypersecretory agent. It inhibits the enzyme enkephalinase in the small intestine, thereby reducing the intestinal hypersecretion of water and electrolytes induced by cholera toxin or inflammation. Racecadotril does not affect basal secretory activity and exerts rapid antidiarrhoeal action without modifying intestinal transit time
Indication: Treatment of acute diarrhea
Contraindication:
Allergy Renal impairment Liver impairment Pregnancy and lactation
Ordered Dose: 100g/ tab BID
Side Effects:
Drowsiness nausea and vomiting dizziness headaches
Drug Interactions:
No interaction with other drugs have been described in humans to date. In humans, the concomitant treatment of racecadotril with loperamide or nifuroxazide does not modify the kinetics of racecadotril.
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug.2. Assess if patient is hypersensitive to the drug.3. Advise patient to increase oral fluid intake4. Instruct patient to eat foods rich in fiber such as green leafy vegetables5. Instruct to report episodes of loose bowel movement6. Educate about the possible side effects og the drug7. Observe for the amount & consistency of the stool8. Instruct patient to report any unusualities

35
Date Ordered:
Generic Name:Methimazole

36
Brand Name:Tapdin
Classification: Antithyroid agent
Mechanism of Action: Inhibits the synthesis of thyroid hormones and thus is effective in the treatment of hyperthyroidism
Indication:
Management of hyperthyroidism,goiter, Graves’ disease and psoriasis. It is also used before thyroid surgery or radioactive iodine treatment.
Contraindication:Allergy, pregnancy, lactation
Ordered Dose: 5mg/tab
Adverse Effects:
CNS: Paresthisisas, neuritis, vertigo, neuropathies Dermatologic: Uricaria, pruritus, lupus-like syndrome, skin pigmentation GI: Epigastric distress, sialadenopathy, jaundice, hepatitis GU: Nephritis Hematologic: Agranulocytosis, granulocytopenia, thrombocytopenia, vasculitits
Side Effects:
Nausea & vomiting Gastric discomfort Headache Skin rashes Drowsiness
Drug Interaction:
Increased theophylline clearance and decreased effectiveness if given to hyperthyroid patients; clearance will change as patient approaches euthyroid state
Altered effects of oral anticoagulants with methamizole Increased therapeutic effectsand toxicity of digitalis glycosides,metoprolol, propranolol
when hyperthyroid patients become euthyroid
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug2. Give drug in three equally divided doses at 8 hour interval
37
3. Inform patient that the drug should be taken for a prolonged period to achieve the desired effects.
4. Educate patient of the possible side effects5. Instruct patient to take the drug with food6. Instruct to report if patient experiences fever, sore throat, unusual bleeding or bruising,
headache or general malaise.
Date Ordered: June 19, 2013
Generic Name: Ciprofloxacin

38
Brand Name:Cipro
Classification: Antibacterial
Mechanism of Action:
Bactericidal; Interferes with DNA replication in susceptible bacteria preventing cell reproduction.
Indication: For treatment of infections
Contraindication:
Allergies Pregnancy Lactation
Ordered Dose: 500 mg tab BID
Adverse Effects:
CNS: insomnia, fatigue, somnolence, depression, blurred vision CV:Arrhytmias, hypotension, angina EENT: Dry eye, eye pain, keratopathy GI:diarrhea, abdominal pain Hematologic: Elevated BUN, AST, ALT, serum creatinine and alkaline phosphatase;
decreased WBC, neutrophil count, Hct
Side effects:
Headache Dizziness Nausea Vomiting dry mouth
Drug Interaction:
decreased therapeutic effect with iron salts, sucralfate decreased absorption withantacids, didanosine increased serum levels and toxic effects of theophyllines if taken concurrently with
ciprofloxacin increased effects of coumarin or its derivatives
Nursing Responsibilities:
1. Assess allergy to ciprofloxacin.2. Observe 10 rights in giving the drug.3. Drink plenty of water when taking the drug.
39
4. Monitor vital signs.5. Give antacids at least 2 hours after dosing.6. Inform about the possible side effects of the drugs.7. Educate patient about the ways to prevent infection such as handwashing.8. Advise to eat foods rich in Vitamin C to boost immune system.
Date Ordered: June 20, 2013
Generic Name:Propranolol

40
Brand Name:Inderal
Classification:
Beta-adrenergic blocker Antianginal Antiarrhytmic Antihypertensive
Mechanism of Action:
Through beta-blocking action, propranolol:o Prevents arterial dilation and inhibits renin secretion, resulting in decreased blood pressure
(in hypertension and pheochromocytoma) and relief of migraine headacheso Decreases heart rate, which helps resolve tachyarrhythmiaso Improves myocardial contractility, which helps ease symptoms of hypertrophic
cardiomyopathyo Decreases myocardial oxygen demand, which helps prevent anginal pain and death of
myocardial tissue.
Indication:
To manage hypertension To treat chronic angina To treat supraventricular arrhythmias and ventricular tachycardia To control tremor To prevent vascular migraine headaches As adjunct to treat hypertrophic cardiomyopathy As adjunct to manage pheochromocytoma To prevent MI
Contraindication:
Asthma Cardiogenic shock Greater thanfirst-degree AV block Sick sinus syndrome Heart failure (unless secondary totachyarrhythmia responsive to propranolol) Hypersensitivity to propranolol or itscomponents
Ordered Dose:
Adverse Effects:

41
Allergic reactions: Pharyngitis, erythematous rash, laryngospasm CNS: Vertigo, tinnitus, paresthesias CV: CHF, cardiac arrhythmias , pulmonary edema Dermatologic: Pruritus EENT: Conjunctivitis GI: Ischemic cholitis, renal and mesenteric arterial thrombosis, retroperitoneal fibrosis,
hepatomegaly, acute pancreatitis GU: Impotence, decreased libido, dysuria
Side Effects:
Dizziness Headache Nausea Vomiting Eye irritation sweating
Drug Interaction:
Increased effects with verapamil Decreased effects with indomethacin, ibuprofen, piroxicam, sulindac, barbiturates Prolonged hypoglycemic effects of insulin Initial hypertensive episode followed by bradycardia with epinephrine Increased first-dose response to prazosin Increased serum levels and toxic effects with lidocaine, cimetidine
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug.2. Assess if there is allergy to the drug.3. Take with meals to facilitate absorption.4. Monitor vital signs.5. Inform patient about the possible side effects of the drug
Date Ordered: June 20, 2013
Generic Name: Probiotics
42
Brand Name:HexBio
Classification: Anti-diarrheal
Mechanism of Action:
Suppressing the growth of pathogens through secretion of antimicrobial substances Competing for attachment sites/nutrients with the pathogens.
Indication:Treatment of diarrhea
Contraindication:
allergy
Ordered Dose: 1 sachet OD
Adverse Effects:
Side Effects:
Nursing Responsibilities:
1. Observe the 10 rights in giving the drug.2. Assess if patient is hypersensitive to the drug.3. Dissolve 1 sachet in ½ cup of water4. Advise patient to increase oral fluid intake5. Instruct patient to eat foods rich in fiber such as green leafy vegetables6. Instruct to report episodes of loose bowel movement7. Educate about the possible side effects og the drug8. Observe for the amount & consistency of the stool9. Instruct patient to report any unusualities
Date Ordered:
Generic Name: Verapamil hydrochloride
Brand Name:Isoptin
Classification:

43
Calcium channel blocker Antianginal Antiarrhytmic antihypertensive
Mechanism of Action:
Inhibits calcium movement into coronaryand vascular smooth-muscle cells by blockingslow calcium channels in cell membranes.The resulting decrease in intracellularcalcium level has the following effects:o inhibits smooth-muscle cell contractions decreases myocardial oxygen demand byo relaxing coronary and vascular smootho muscle, reducing peripheral vascularo resistance, and decreasing systolic ando diastolic pressureso slows AV conduction time and prolongso AV nodal refractorinesso Interrupts reentry circuit in AV nodalreentranttachycardias.
Indication:
To treat chronic angina pectoris To manage hypertension To prevent or treat supraventriculartachycardia
Contraindication:
Allergy Hypotension Pregnancy & lactation Heart-block Sick sinus syndrome except with ventricular pacemaker
Ordered Dose: 40mg/tab
Adverse Effects:
CNS: Vertigo CV: Peripheral edema, hypotension, arrhythmias, bradycardia, AV heart block
Side Effects:
Nausea Constipation Dizziness Headache

44
Sleepiness
Drug Interaction:
Risk of serious cardiac effects with IV beta-adrenergic blocking agents; do not give these drugs within 48 hour before or 24 hour after IV verapamil.
Increased cardiac depression with beta-adrenergic blocking agents Additive effects of verapamil and digoxin to slow AV conduction Increased serum levels of digoxin carbamazepine, prazosin, quinidine Increased respiratory depression with atracurium, gallamine, pancoronium, tubocurarine,
vecuronium Decreased effects with calcium, rifampin
Nursing Responsibilities:
1. Observe the 10 rights2. Ensure that the patient swallows SR tablets whole; patient should not cut, crush or chew
them.3. Monitor vital signs, especially BP very carefully with concurrent doses of antihypertensives.4. Administer SR form in the morning with food to decrease GI upset.5. Do not take the drug with grape or grapefruit.6. Inform about the possible side effects of the drug.

45
Cues Need Nursing Diagnosis Objective of Care Nursing Intervention Evaluation
D/T CUES NEED NURSING DIAGNOSIS OBJECTIVES OF CARE NURSING INTERVENTIONS EVALUATION
J
U
N
E
20,
2
0
1
3
@
7am
Subjective:
“Ginakalibanga man
gudko. “
“Gahaponnisugodakong
kalibanga.”
Objective:
Vital signs as taken:
-T: 36.6oC
-PR: 80 bpm
-RR: 20 cpm
-CR: 87 bpm
-BP: 120/80 mmHg
dry lips
sunken eyes
loose watery stool
history of loose
watery stools,
5episode/day with
100cc/episode
IVF of PNSS 1L @
140cc/hr
Drugs as ordered:
-Ciprofloxacin 500
mg tab BID
-Paracetamol
500mg tab q4 PRN
for fever
-Propylthiouracil
50mg BID
-Isoptin 40mg/tab
-Tapdin 5mg/tab
-Propranolol
E
L
I
M
I
N
A
T
I
O
N
P
A
T
T
E
R
N
Diarrhea r/t infectious
processes secondary to
acute gastroenteritis
®Diarrhea means loose
bowel movements,
usually causing to move
his or her bowels
frequently. Vomiting
may bepresent as well.
Acute diarrhea means
the diarrhea lasts for
only a limited time; this
is also called
gastroenteritis. There
are manypossible causes
of gastroenteritis,
including infections with
bacteria, viruses, or
parasites. Diarrhea may
also be asymptom of
other diseases, but this is
less common.
Reference:
Hurst, M. (2008). Hurst
Reviews:
Pathophysiology
Reviews. New York.
McGraw Hill.
At the end of my 8 hours span
of nursing care, the patient
will be able to:
1. Report decrease in the
frequency of bowel
movements
2. Learn ways to prevent
diarrhea
3. Verbalize
understanding of the
interventions
4. Demonstrate ways to
prevent infection
1. Obtain vital signs
® to have baseline data
2. Assess the medications being
taken by patient
® some drugs may cause
diarrhea
3. Observe and record number
and consistency of stools per
day
®Documentation of output
provides a baseline and helps
direct replacement fluid
therapy
4. Secure stool sample
® to test the sample and
identify the possible causative
agent
5. Emphasize importance of
handashing
® to prevent spread of
microorganisms
6. Monitor input and output of the
patient
®Diarrhea can lead to
profound dehydration and
electrolyte imbalance.
7. Administer drugs as ordered
June 20, 2013 @ 3pm
GOAL MET
After the 8 hours span of care, the
patient was be able to:
1. Report decrease in
frequency of bowel
movements as evidenced
by:
Less than 3 bowel
movements during the
shift with semi-
formed stool
2. Learned ways to prevent
diarrhea such as ensuring
that the food he eats is
safe and not spoiled
3. Verbalized understanding
of the condition,
“Muinomnakougdaghanng
atubigugmukaonugmgagul
ayparamarehydratekougm
ugahiakonglibang”.
4. Demonstrated ways to
prevent infection such as
handwashing

46
Date&
Time
J
U
N
E
2
2,
2
0
1
3
@
7
am
Subjective:
“pakiramdamko
, hinanghina
ako, at madali
lang ako
mapagod.
Parati lang nga
ako natutulog.”
As verbalized
by the patient.
Objective:
- Lack of
energy
- Irritable
- VS taken as
follows:
A
C
T
I
V
I
T
Y
E
X
E
R
C
I
S
E
P
Fatigue related to
hypermetabolic
state with
increased energy
requirements.
R: Hyperthyroidism
is an over
production of
thyroid hormone,
which creates far
reaching metabolic
effects.
Hypertrophy and
hyperplasia of the
thyroid gland occur
with increased
vascularity. Most
of the clinical
After the 8 hours span of
care, the patient will be
able to:
1. Show decrease, or
absence of
irritability
2. Verbalize
increased
knowledge
regarding fatigue
and management
of high energy
consuming
activities.
3. Verbalize proper
understanding of
1. Monitor vital
signs, noting pulse
rate or cardiac rate at
rest and when active.
R: Pulse or Cardiac
rates are typically
elevated, and even at
rest, tachycardia up to
160 bpm may be
noted.
2. Note daily energy
patterns.
R: Helpful in
determining
pattern/timing of
activity.
@ 3pm
Goal Met
After the 8 hours span
of care, the patient will
be able to:
1. Showed
decrease, or
absence of
irritability.
2. Verbalized
increased
knowledge
regarding fatigue
and
management of

47
T: 36.6
P: 80
CR: 87
BP: 120/80
RR: 20
A
T
T
E
R
N
manifestations
result from
increased
metabolic rate,
excessive heat
production,
increase
neuromuscular
and cardiovascular
activity, and
hyperactivity of the
sympathetic
nervous system.
his medical illness
and the
management
required.
4. Demonstrate
relaxation
techniques that
can decrease the
presence of fatigue
such as: massage
and cold or hot
showers.
3. Advise patient to
report development of
tachypnea, dyspnea,
pallor, and cyanosis.
R: O2 demand and
consumption are
increased in
hypermetabolic state,
potentiating risk of
hypoxia with activity.
4. Provide quiet
environment, cool
room, decreased
sensory stimuli,
soothing colors, and
quiet music.
R: Reduces stimuli
that may aggravate
high energy
consuming
activities.
3. Verbalized
proper
understanding of
his medical
illness and the
management
required.
4. Demonstrated
relaxation
techniques that
can decrease the
presence of
fatigue such as:
massage and
cold or hot
showers.

48
agitation,
hyperactivity, and
insomnia.
5. Encourage client to
rest in bed as much
as possible.
R: Helps counteract
effects of increased
metabolism.
6. Provide comfort
measures like
massages and hot or
cold showers.
R: May decrease
nervous energy,
promoting relaxation.
7. Provide for calming

49
diversional activities
such as reading,
listening to the radio,
and watch television.
R: Allows for use of
nervous energy in a
constructive manner,
serves as a
distraction, and may
reduce anxiety.
8. Avoid topics that
irritate or upset client.
Discuss ways to
respond to these
feelings.
R: Increased irritability
of the CNS may
cause client to be
easily excited,

50
agitated, and prone to
emotional outbursts.
9. Discuss with
Significant Others
reasons for fatigue
and emotional ability.
R: Understanding that
the behavior is
physically based may
enhance coping with
current situation and
encourage Significant
Other to respond
positively and provide
support for client.
10. Administer
medications, as
indicated, such as
anti-anxiety agents.

51
R: May be prescribed
to help combat
nervousness,
hyperactivity, and
insomnia.
Date and Time
Cues Need Nursing Diagnosis Objectives of Care
Nursing Interventions Evaluation
52
JUNE
22,
2013
@
7 AM
Subjective:
“Sakitakongtiyanpabalikbalikunyamagsigesiyaugtingog”, as verbalized by the patient.
Objective:
Facial grimace
Irritability
Reduced interaction with people
Appears weak
Pain scale of 3 out of 5
COGNITIVE/PERCEPTUAL
PATTERN
Acute pain r/t inflammatory
process
Rationale:Gastroenteritis is the inflammation of the stomach and the intestinal tracts that primarily affects the bowel. One manifestation of gastroenteritis is abdominal pain. During the course of inflammation, the body’s immune response is to release cytokines and prostaglandin causing an increase in vascular permeability and causes pain in the abdomen.(Black, J.M. 2010)
That within my 8 hours span of
care, my patient will be able to:
a. Verbalize less pain felt;
b. enumerate ways on how to deal with pain during its occurrence;
c. pain scale of 1-2 out of 5.
1. Establish rapport with the patient.Rationale: To gain trust and cooperation.
2. Check vital signs.Rationale: To serve as baseline data.
3. Assess level of pain using pain scale.Rationale: To determine the degree of pain felt by the client.
4. Provide diversional activities such as watching television or listening to music.Rationale: To divert his/her attention from the pain felt.
5. Instruct client to perform deep breathing exercise.
June 22, 2013@ 3pm
“Goal Met”
a. “Okay okaynamanakongpaminawkaysaganiha. Medyoniarang-arangnaakongpaminaw”, as verbalized by the patient.
b. “Mag-facebooknalangkoaniarunmedyomahuwasanko. Mag-inompudkoganalgesic paramawalaangsakit”, as verbalized by the

53
Rationale: Deep breathing exercises may reduce pain sensation/ used in pain management.
6. Provide a calm environment.Rationale: Lessens patient’s irritability.
7. Administer prescribed analgesics.Rationale: To decrease pain.
8. Monitor effectiveness of pain medications.Rationale: To promote timely intervention.
client.
c. Pain scale of 2 out of 5.

54
Reference:
Date &
Time
Cues
Needs Nursing DiagnosisObjectives
of Care
Nursing Interventions
Evaluation
J
U
N
E
21,
2
0
1
3
@
7 AM
TO
3PM
Subjective:“nag papalpitatesiyakanina miss” as verbalized by the watcher
Objective: CR: 120 bpm Palpitation Short
breathlessness Irritability Irregular heart rate Medication:
Propanolol 10g
ACTIVITY-EXCERCISE
PATT
ERN
Risk for decrease cardiac output ( systemic) r/t increasing workload of the heart as manifested by hyperthyroidism
R: patients with hyperthyroidism usually have the symptoms of palpitation. With the increasing workload of the heart this may lead to decrease cardiac output due to excessive pumps of the heart.
Reference:Smeltzer,
S. C. EdD,
RN, FAAN.
Brunner
&Suddarth’s
Textbook of
Medical –
Surgical
Nursing.
That with my 2 hours span of care, the patient will be able to have normal cardiac output as evidenced by:
a. Enumerate causative factors affecting his normal breathing.
b. Identify situations that would worsen the level of heart rate.
c. identify and use appropriate support system.
1. Establish rapport.®To gain the trust and the cooperation of the client.
2. Monitor vital signs.®For baseline data.
3. Increase oral fluid intake.
®water helps regulate the body’s cardiac rate.
4. Record the heart sounds.
® Know of any changes in heart rhythm.
5. Limit your activities adequately.
®adequate rest is needed to improve the efficiency of cardiac contraction and oxygen consumption and reduce redundant work.
6. Emphasized the importance of adequate rest in elevation of cardiac output.
®This will help the client understand ways
December 21, 2013@ 11 am
“GOAL MET”Patient was able to have normal Cardiac rate as evidenced by client was able to:
a. verbalized “angpaggalawgalawkosiguro at pagiisipngsobraangdahilan kaya akohinihingalkokaninaperongayon okay okayna”
b. verbalized “angdilikopaginomsatamanggamotkopagnasabahayangdahilan kaya ako nag papalpitate”
c. identify his support system and that is his family. “ginabadlong man konilalabinaakong partner”
d. have a cardiac rate of 90bpm after rechecking.

55

56
D/T CUES NEED NURSING DIAGNOSIS OBJECTIVES OF CARE NURSING INTERVENTIONS EVALUATION
J
U
N
E
20,
2
0
1
3
@
7am
Subjective:
“Naga sigarilyo man
gudkomaongluspadnia
kungngabil” as
verbalized by the
patient.
Objective:
(+)
hyperthyroidism
for 3-4 years
Consumes 15-20
sticks/ day
Vital signs as
taken:
-T: 36.6oC
-PR: 80 bpm
-RR: 20 cpm
-CR: 87 bpm
-BP: 120/80
mmHg
With a capillary
refill of 2sec.
Dry pale lips
history of loose
watery stools,
5episode/day with
100cc/episode
Diagnostic and
Lab:
+ Hematology:
-hemoglobin
132g/dl (140-180
M
E
T
A
B
O
L
I
C
P
A
T
T
E
R
N
Impaired tissue
perfusion r/t decreased
hemoglobin in the blood
as evidenced by anemia
® Thyroid gland is
responsible for the
secretion of the
hormones that controls
the metabolic rate of the
body which the body
burns energy to
maintain the normal
functions of life and the
rate of growth or
replacement of body
tissue. Individuals with
hyperthyroidism tends
to have an overactive
thyroid gland which
increases the
production of hormones
that exceeds the normal
metabolic rate causing
increase peristaltic
movement that may
result to gastroenteritis.
Reference:
Timothy Secomb.
January 26, 2009.
Quantitative
Analysis of
At the end of my 8 hours
span of nursing care, the
patient will be able to:
5. Demonstrates adequate tissue perfusion as evidenced by warm and dry skin, and the absence of respiratory distress
6. Verbalizes knowledge
of treatment regimen,
including appropriate
exercise and
medications and their
actions and possible
side effects
7. Identifies changes in
lifestyle that are
needed to increase
tissue perfusion such
as gradually stop
smoking by consuming
at least 2-3 sticks/ day.
14. Obtain vital signs
® To have baseline data
15. Assess patient’s condition
® To render appropriate
interventions
16. Monitor vital signs, capillary
refill and nail beds.
® Provides information
about the degree /
adequacy of tissue
perfusion and help
determine the need for
intervention.
17. Observe for skin color on the
sick.
® The skin color typically
occurs when cyanosis,
cold skin. During the
color change, the sick to
be cool then throbbing
and tingling sensations.
18. Check respirations and
absence of work of breathing.
® Cardiac pump
malfunction and/or
ischemic pain may result
to respiratory distress.
Nevertheless, abrupt or
continuous dyspnea may
signify thromboembolic
June 20, 2013 @ 3pm
GOAL MET
After the 8 hours span of care,
the patient was be able to:
5. Demonstrated adequate
tissue perfusion as
evidenced by skin is
warm, in normal skin
turgor and respiration is
on normal range of 20-25
bpm.
6. Patient verbalize
knowledge of treatment
regimen as “kabalona
man
kosamgaepektosatambal
kaymga 4 kona nah
katuigginatumarug kung
naa may
mgadilinakubationkaynag
a pa check-up man
dayonko”.
7. Identifies changes in
lifestyle that are needed
not to provoke the
disease process
“gitestingan man naku
mag
undangdatiugsigarilyoper
57
58

59
METHOD Health Teachings RationaleMedication Medications should
be taken regularly as prescribed, on exact dosage, time and frequency, making sure that the purpose of medications is fully disclosed by the health care provider.
Instruct the family to report the occurrence of any adverse effects and refer them immediately to the physician.
For a better and effective management of the condition which would provide optimum health for the patient and prevent lethal complications that that they would encounter.
To maximize the optimum health of the patient whenever the patient has taken the drugs.
Exercise Exercise should be
promoted in a way by stretching hand and feet every morning.
Encourage the patient to keep active to adhere to exercise program and to remain as self-sufficient as possible.
To promote muscle strength and enhance circulatory processes.
Treatment Comply to the treatment regimen such as taking medications as prescribed by the physician.
Discuss to the watcher and significant others the dangers of noncompliance to doctor’s order
It necessary to take the prescribed take home medications and to follow the given instructions exactly as they are told
To let the patient and significant others recognize the possible efffects if compliance to the Doctor’s order is not attained
Hygiene Instruct patient for proper body hygiene such as routine handwashing.
To deter the spread of microorganisms
60
Where is your nursing theory??
PROGNOSIS

61
Our patient no longer has fever and LBN and could be discharged the next day;
we rated the duration of illness as good prognosis. He eats fruits and vegetables with
good appetite, drinks at least 8 glasses of water every day. The patient readily compiled
with the treatment regimen, so we therefore conclude that our patient has a good
prognosis.
References

62
Deglin, J. H., PharmD. Davis’s DRUG GUIDEFOR NURSES. F. A. Davis Company.
2011, 12th edition.
Deglin, J.H. &m Vallerand, A.H. (2009). Davis’s Drug Guide for NURSES (Eleventh
Doenges, M. E., APRN, BC–retired Nurse’s Pocket Guide Diagnoses, Prioritized
Interventions, and Rationales.Saunders ©2011.10th edition.
Elsevier, M. (2007). Maternity & Women’s Health Care (9th Edition). Elsevier Inc. 11 830
Gulanick, M. et al.(2007). Nursing Care Plan. Elsevier Inc. Singapore
James,SRPhd, Ashwill, JW RN, MSN, Medical Disability Advisor, Mosby ©2010
Jonas MS: Mosby's Dictionary of Complementary and Alternative Medicine. Elsevier (c)
2009, 6th edition.
Klossner, N. J., MSN, RNC. Introductory Maternity &Pediatric Nursing.Williams &
Wilkins, Philadelphia.2010, 2nd edition.
Linton, A. D., Phd. Mayo Foundation for Medical Education and Research
(MFMER)W.B .
Newfield S. A., PhD, RN, APRN. BC.COX’S CLINICAL APPLICATIONS OF NURSING
DIAGNOSIS: Adult, Child, Women’s, Mental Health,Gerontic, and Home Health
Considerations F. A. Davis Company. 2009, 7th edition.
Smeltzer, S. C. EdD, RN, FAAN. Brunner &Suddarth’s Textbook of Medical – Surgical
Nursing.Williams & Wilkins, Philadelphia.2010, 12th edition.
Tortora, G. J., Derrickson, B. H. PRINCIPLES OF ANATOMY AND PHYSIOLOGY.
John Wiley & Sons, Inc, Hoboken. 2012, 12thedition.Westline Industrial Drive, St.
Louis, Missouri 63146Wilkins. 323 Norristown Road, Suite 200, Ambler, PA 19002-
2756.York: Lippincott, Williams, & Wilkins

63