acute gastroenteritis: a case discussion
DESCRIPTION
Ryan Em C. Dalman MD MBA - 070070. Acute Gastroenteritis: A Case Discussion. Outline. Objectives Case Presentation Case Discussion. Objectives. Present a case of Acute Gastroenteritis Discuss the pathophysiology and management of Acute Gastroenteritis. Case Presentation. - PowerPoint PPT PresentationTRANSCRIPT
Acute Gastroenteritis: A Case Discussion
Ryan Em C. Dalman MD MBA - 070070
Outline
Objectives Case Presentation Case Discussion
Objectives
Present a case of Acute Gastroenteritis
Discuss the pathophysiology and management of Acute Gastroenteritis
Case PresentationPatient History
General Data
JM 1-year-old born on July 9, 2009 Female Admitted for the first time Roman Catholic Pasig City
Chief Complaint
Vomiting
History of Present Illness
Vomiting 1x ingested food Non-projectile Non-bilous Non-bloody
3 days PTA
1 day PTA Loose bowel movement 3x
Watery Non-bloody Non-mucoid Non-foul smelling
No associated symptoms, no medications, no consults
History of Present Illness Symptoms persisted 12 hours PTA
Consult at the
ER
Sent home after successful trial feeds
History of Present Illness
Vomiting 3x ingested food Post-prandial Non-projectile Non-bilous Non-bloody
Few hours PTA
Consult at the
ER
Admitted
Review of Systems
General: no weight loss, no change in appetite
Cutaneous: no lesions, no pigmentation, no hair loss, no pruritus
HEENT: no rednessno aural dischargeno neck massesno sore throat
Review of Systems
Cardiovascular: no easy fatigability, or fainting spells
Gastrointestinal: no constipationGenitourinary: no genital discharge, no
pruritusno problems in
urinationEndocrine: polydypsia, no heat/cold
intolerance
Review of Systems
Muskuloskeletal: no joint or muscle swelling, no limitation of movement, no stiffness
Hematopoietic: no easy bruisability, or bleeding
Maternal and Birth History Born full term via NSD to a 31 year
old G4P3 (3013) by an obstetrician at PCGH
with complete prenatal consults No intake of any medications except
for multivitamins No maternal illnesses No complications at birth
Nutritional History
Breastfed from birth to 3 months old Bona Supplementary foods were given at
6 month old Current diet
Milk 4-5 bottles a day Rice + (chicken, vegetables, w/ soup) 3x
a day Bread every morning
Immunizations
BCG – 1 dose DPT – 3 doses Hep B – 3 doses Measles – 1 dose
Developmental History
Stands alone Throws toys Obeys commands or requests Attempts to use a spoon
Past Medical History
No Tuberculosis, Asthma, TraumaNo previous surgeriesNo previous hospitalizationsNo Allergies
Family History
Diabetes, Hypertension – father No heart disease, cancer, stroke,
kidney disease, asthma, or allergies
Personal and Social History Father works for Reagent Mother is a housewife Private Subdivision in Pasig City
Environmental
Not exposed to environmental hazards like chemicals, pollution, cigarette smoking, etc
Generally clean environment Has their own toilet Water comes from Manila Waters
Drinking water mineral water
Case PresentationPhysical Exam
General Survey
awake, active, with good cry but consolable
Not in cardiorespiratory distress
Vital Signs/ Anthropometrics
Vital signsTemperature – 36.5oCCR – 112 (70-110) RR – 28
(20-30)
Weight: 10.4 kg (50-75th) Length: 75cm (50th) HC: 45.5cm (50-75th) CC: 45 cmAC: 42 cm
Skin
Light brown No rashes, hemorrhages, scars Moistgood skin turgorCRT 1-2 seconds
HEENTHead
normocephalicno lesions, fontanels closed
Eyesanicteric sclerae, pink palpebral conjunctiva, not sunkenpupils 2-3mm
Earscone of light present inferomedially on both earsno discharge noted
Noseseptum medline, moist mucosa
Throatmouth and tongue moistno TPC
Chest and LungsNeck
no cervical lymphadonapathySupple
Chestadynamic precordiumno heaves, thrills, or lifts, PMI at 4th ICS MCLslightly tachycardic, normal rhythm, distinct S1 and S2no murmurs
Lungssymmetrical chest expansion, no retractionsEqual vocal fremitiClearbreath sounds
Abdomen/ Perineum
AbdomenDistended, no scars, no lesionsHyperactive bowel soundstympanitic on all quadrantsno tenderness on all quadrantsno masses, no organomegallyliver edge palpatedkidneys and spleen not appreciated
Neurologic Examination
Glasgow Coma Scaleverbal response: 5eye opening: 4motor response: 6total: 15
Cerebrumawake and active
Cerebellumno nystagmus, tremors, or abnormal movements
Neurologic Examination
Sensoryresponds to pain
MotorSymmetrical general movement with good activity
DTR++ on all extremities
Neurologic Examination
Cranial NervesI: not elicited II: 2-3mm pupils, equally reactive to lightIII,IV,VI: EOM’s intactV: corneal reflex presentV1, V2, V3 intact (responds to touch)VII: no facial asymmetry VIII: turns to soundIX, X: gag reflex presentXI: turns head from side to sideXII: tongue midline
Case PresentationSalient Features, Admitting Impression, Differentials, Course in the Ward
Salient Features
1 year month old, female Vomiting Acute Loose watery stools
Non-bloody, non-mucoid, non-foul smelling Distended abdomen Skin – good turgor, CRT 1-2 sec Eyes not sunken Moist oral mucosa Hyperactive bowel sounds
Admitting Impression
Acute Gastroenteritis, probably viral, with no signs of dehydration
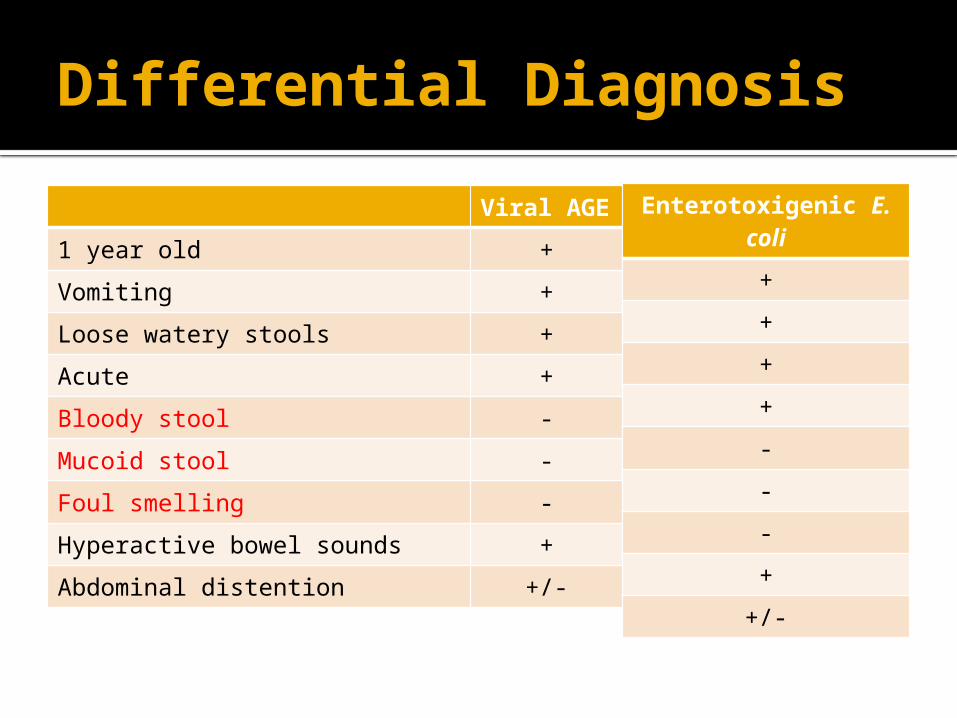
Differential DiagnosisViral AGE
1 year old +Vomiting +Loose watery stools +Acute +Bloody stool -Mucoid stool -Foul smelling -Hyperactive bowel sounds +Abdominal distention +/-
Enterotoxigenic E. coli++++---+
+/-
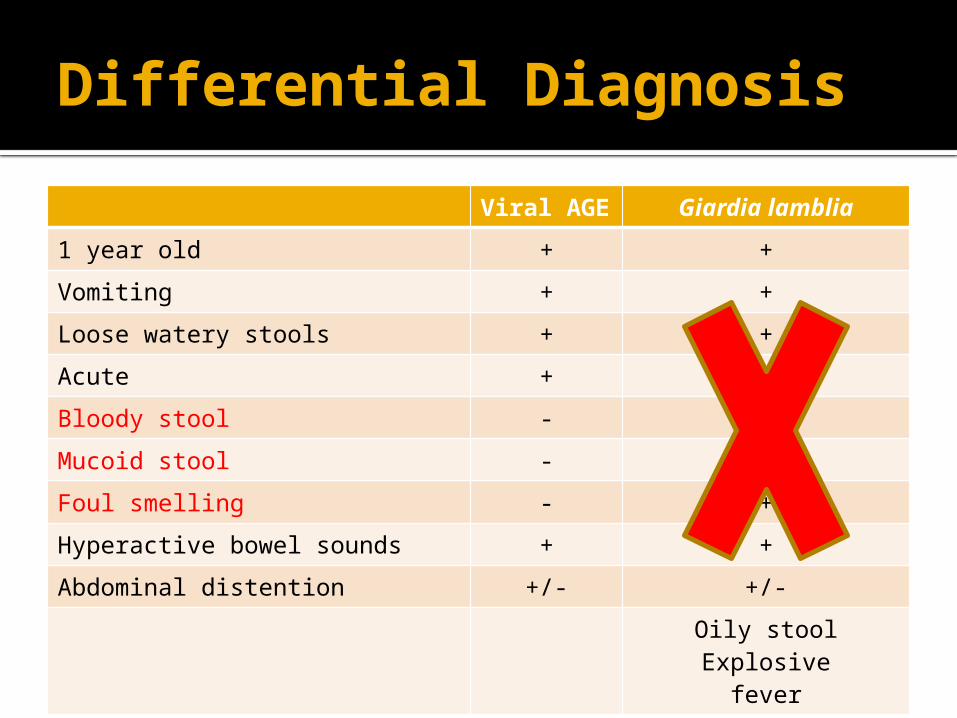
Differential DiagnosisViral AGE Giardia lamblia
1 year old + +Vomiting + +Loose watery stools + +Acute + +Bloody stool - -Mucoid stool - +Foul smelling - +Hyperactive bowel sounds + +Abdominal distention +/- +/-
Oily stoolExplosive
fever
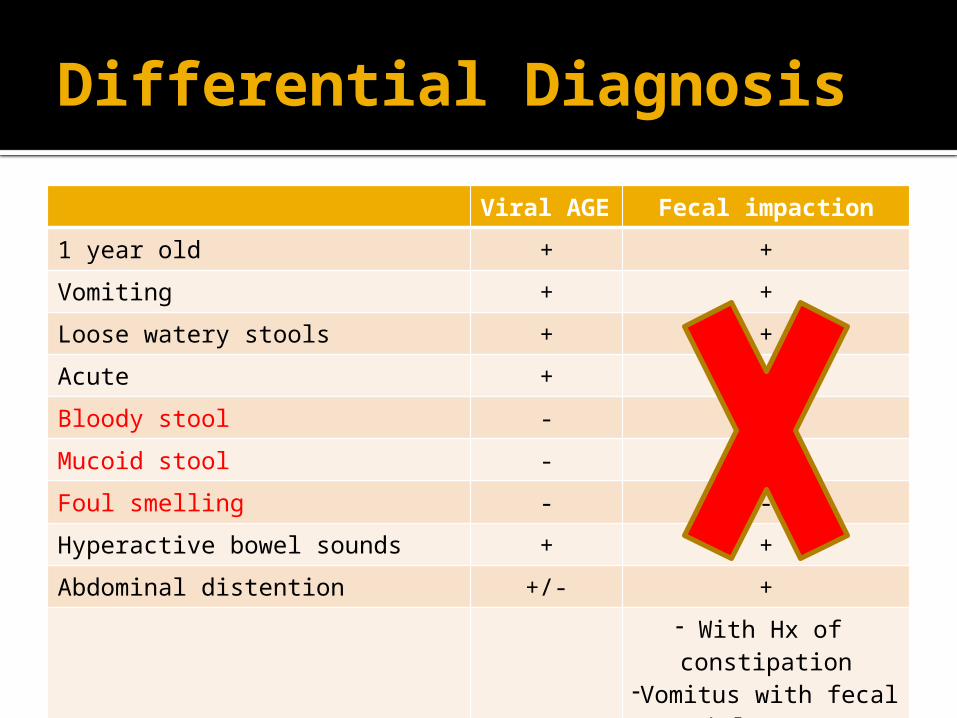
Differential DiagnosisViral AGE Fecal impaction
1 year old + +Vomiting + +Loose watery stools + +Acute + -Bloody stool - -Mucoid stool - -Foul smelling - -Hyperactive bowel sounds + +Abdominal distention +/- +
- With Hx of constipation
-Vomitus with fecal material
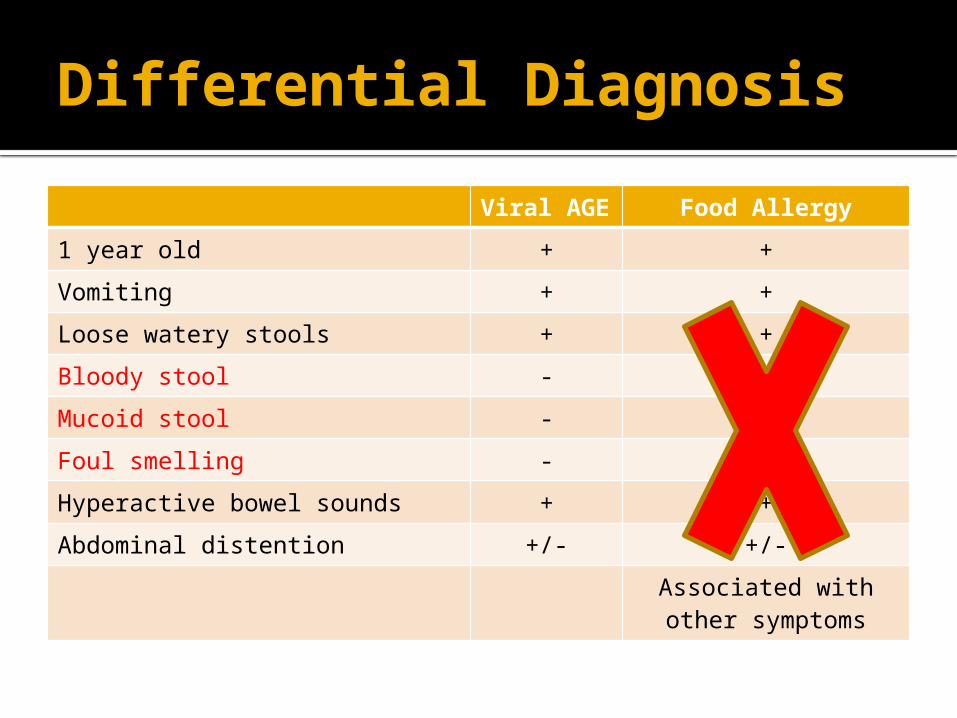
Differential DiagnosisViral AGE Food Allergy
1 year old + +Vomiting + +Loose watery stools + +Bloody stool - +/-Mucoid stool - -Foul smelling - -Hyperactive bowel sounds + +Abdominal distention +/- +/-
Associated with other symptoms
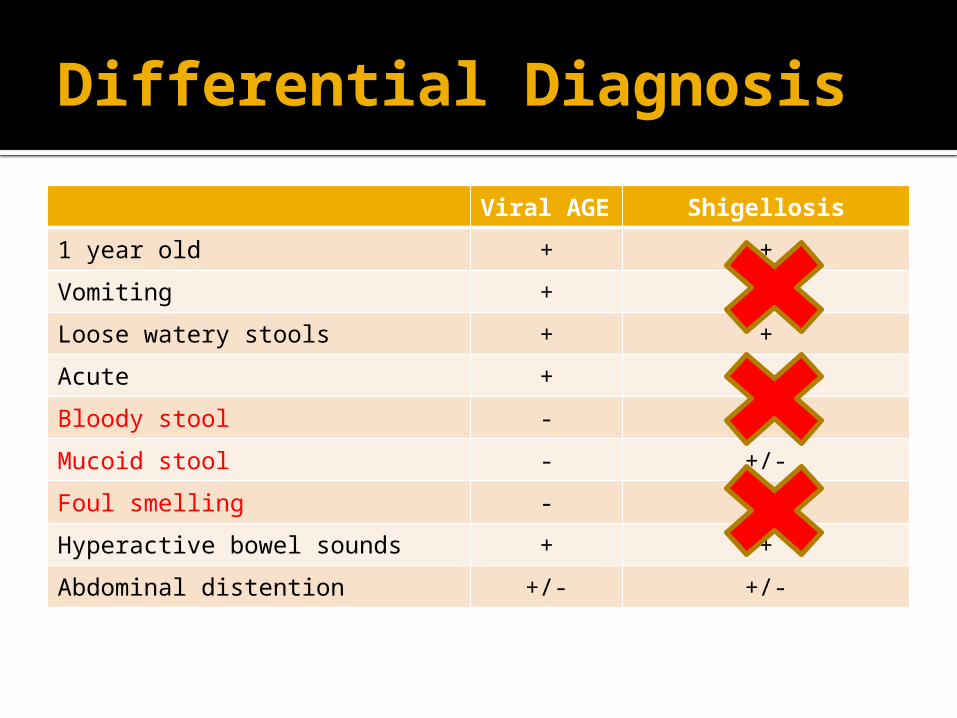
Differential DiagnosisViral AGE Shigellosis
1 year old + +Vomiting + +Loose watery stools + +Acute + -Bloody stool - +Mucoid stool - +/-Foul smelling - +Hyperactive bowel sounds + +Abdominal distention +/- +/-
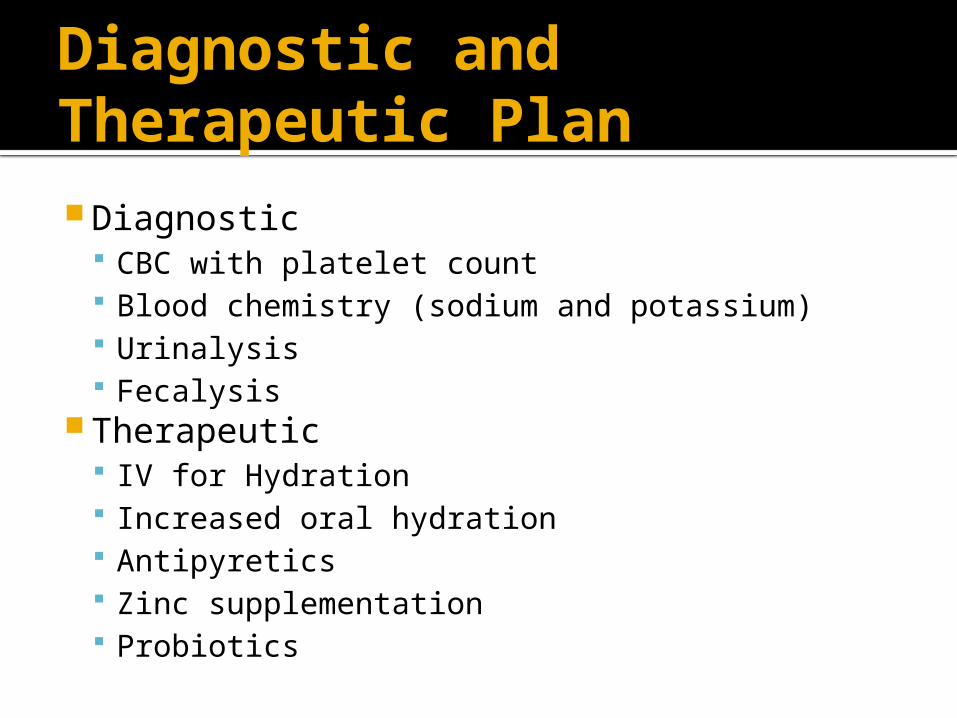
Diagnostic and Therapeutic Plan Diagnostic
CBC with platelet count Blood chemistry (sodium and potassium) Urinalysis Fecalysis
Therapeutic IV for Hydration Increased oral hydration Antipyretics Zinc supplementation Probiotics
Course in the Ward
1st Hospital DayS O A P
Poor suckComfortableNo vomiting3 BM-2x watery with some formed-soft
T: 36oC CR: 104 RR: 30-U/O: 1.84 cc/hr-Awake, with good cry-Good activity-Eyeballs not sunken-With tears-Clear breath sounds-Regular cardiac rate with normal rhythm-Normoactive bowel sounds-Soft and non-tender abdomen
Course in the Ward
1st Hospital DayS O A P
Poor suckComfortableNo vomiting3 BM-2x watery with some formed-soft
Fecalysis-negative
Blood Chemistry-Normal Na and K+
Urinalysis -normal
CBC-normal
Acute gastroenteritis with no signs of dehydration-resolving
IVF D5LR 1L 42-43ml/hr-Small frequent feeding-avoid oily and fatty food-encourage apples and bananas-continue hydration-monitor input and output
Course in the Ward
2nd Hospital DayS O A P
Good suckComfortableNo vomiting1 BM, soft
T: 36.7oC CR: 103 RR: 28-U/O: 1.77 cc/hr-Awake, with good cry-Good activity-Eyeballs not sunken-With tears-Clear breath sounds-Regular cardiac rate with normal rhythm-Normoactive bowel sounds-Soft and non-tender abdomen
Acute Gastroenteritis with no signs of dehydration-resolved
-May go home tomorrow-consume IVF then switch to oral hydration-home medications:Zinc sulfite syrupProbiotics

Case Discussion
Definition
Infections of the gastrointestinal tract caused by bacterial, viral, or parasitic pathogens
Diarrheal disorders Term used in public health setting
Diarrhea 3 or more unusually watery stools
passed in 24 hours
WHO – Treatment of Diarrhea
Etiology
> 3 years old Viral
Rotavirus Enteric adenovirus Astrovirus Norovirus Calicivirus
E. coli, Salmonella
Epidemiology
18% of childhood deaths >700 million episodes of diarrhea
annually < 5 years old (WHO)
Philippines 2nd leading cause of morbidity 6th leading cause of mortality for all ages 3rd leading cause of infant deaths Predominance of rotavirus and
enterotoxigenic E. coliNelson/ Carlos and Saniel, Etiology and Epidemiology of Diarrhea (1990)
Manifestation
Most common Diarrhea Vomiting
May also have systemic symptoms Abdominal pain fever
Clinical types of Diarrhea Acute watery diarrhea
Several hours to days Acute bloody diarrhea Persistent diarrhea
> 14 days Diarrhea with severe malnutrition
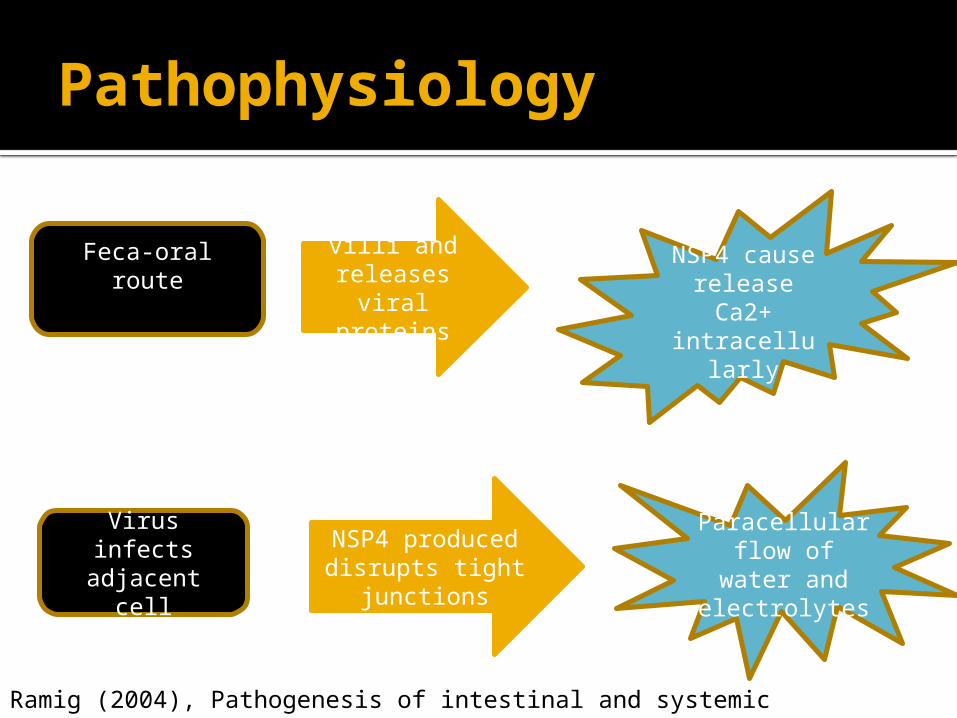
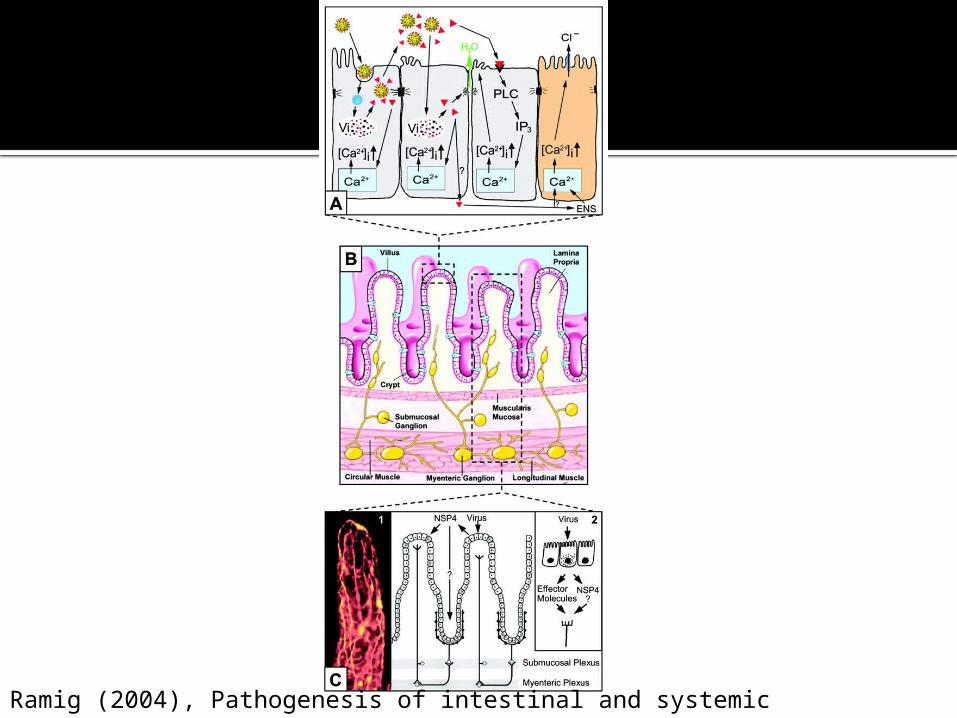
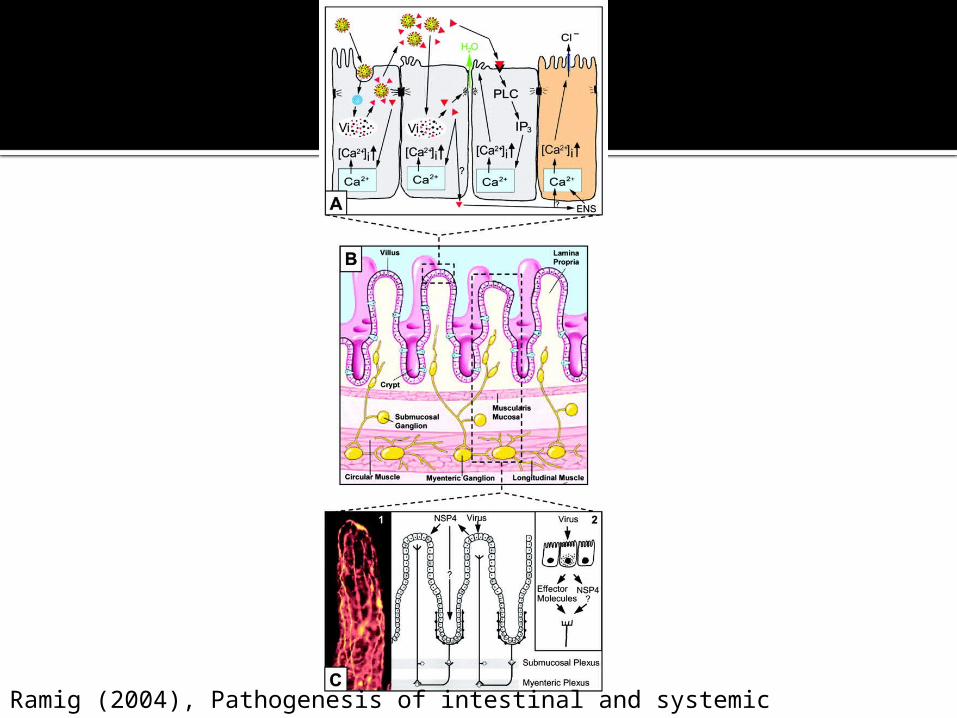
Pathophysiology
Enters villi and releases viral proteins
(NSP4)
Feca-oral route NSP4 cause release Ca2+
intracellularly
Virus infects adjacent cell
NSP4 produced disrupts tight
junctions
Paracellular flow of water
and electrolytes
Ramig (2004), Pathogenesis of intestinal and systemic rotavirus infection
Ramig (2004), Pathogenesis of intestinal and systemic rotavirus infection
Pathophysiology
Intracellular Ca2+
cascade
NSP4 causes release of more
Ca2+
Disruption of
microvillar cytoskeleton
Intracellular Ca2+ cascade
Induces chloride secretion
Ramig (2004), Pathogenesis of intestinal and systemic rotavirus infection
Ramig (2004), Pathogenesis of intestinal and systemic rotavirus infection
Diagnostics
Clinical evaluation Fecalysis
Suspected amoebiasis or giardiasis Acute watery diarrhea▪ Very young/elderly▪ Immuno-compromised▪ Severely dehydrated
Clinical presentation is atypical
UMED Acute infectious diarrhea and common intestinal parasitism workbook
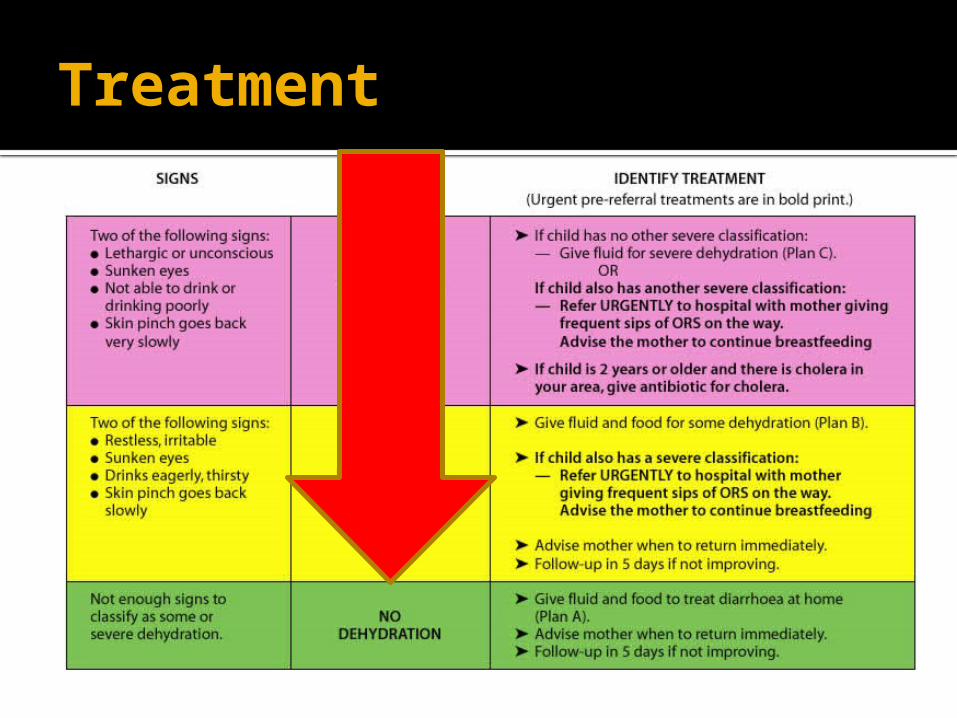
Treatment
Assess for the level of dehydration
Treatment
Treatment
No signs of dehydration Home therapy to prevent
dehydration More fluids than usual▪ ORS, salted drinks (salted rice water), chicken
soup with salt▪ Add salt (3g/L) for unsalted drinks and food▪ Usual milk feed every 3 hours▪ As much as the child wants
Frequent small feedings every 3-4 hours
Failure of oral
rehydration
Treatment
For failure of ORT ORS via nasogastric tube IV Ringer’s Lactate Solution
75 ml/kg in 4 hours Reassess
Treatment
Some signs of Dehydration Oral rehydration therapy with ORS
solution 75 ml/kg/hour
If a child wants more than the estimated amount of ORS solution, and there are no signs of over-hydration, give more
Teaspoonful every 1-2minutes Reassess
Treatment
Severe signs of Dehydration Admit in the Hospital If patient can still drink poorly, give ORS
until IV drip is running 5 ml/kg for 3-4 hours
IV Ringer’s lactate Solution (100 ml/kg) 1st 30ml/kg in 1 hour Then 70 ml/kg in 5 hours
Reassess every 15-30 minutes until strong radial pulse is present, then 1-2 hours
Prevention
Promotion of exclusive breast-feeding
Improved complementary feeding practices
Rotavirus immunization Proper food preparation/ hygiene
Prognosis
Good prognosis as long as adequate hydration has been given