water, electrolyte, and acid-base balance. function of water: most of cellular activities are...
TRANSCRIPT

Water, Electrolyte, and Acid-Base Balance

Function of Water: Most of cellular activities are performed in
water solutions.

16% TBW
40% TBW4% TBW
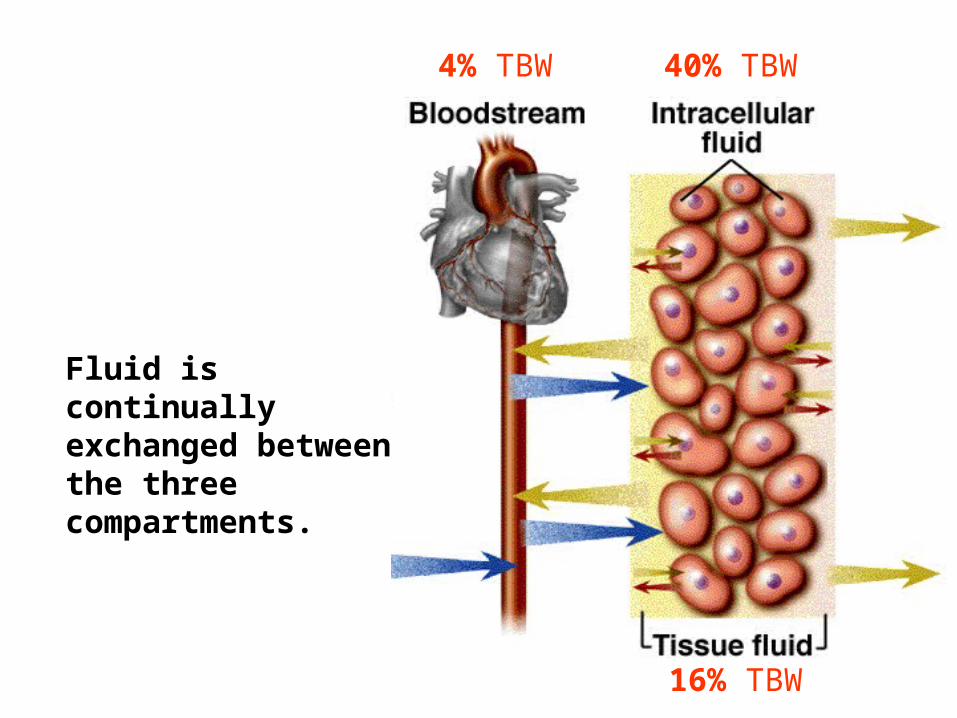
- makes up ~60% of total body weight (TBW)
- distributed in three fluid compartments.
Body Fluid
16% TBW
40% TBW4% TBW
Fluid is continually exchanged between the three compartments.

16% TBW
40% TBW4% TBWExchange between Blood & Tissue Fluid
- determined by four factors:
capillary blood pressure
plasma colloid osmotic pressure
interstitium Hydrostatic Pressure
Interstitium colloid osmotic pressure

16% TBW
40% TBW4% TBW
- not affected by electrolyte concentrations
- Edema = water accumulation in tissue fluid
Exchange between Blood & Tissue Fluid

16% TBW
40% TBW4% TBWExchange between Tissue Fluid &
Intracellular Fluid
- determined by two:
1) intracellular osmotic pressure
electrolytes
2) interstitial osmotic pressure
electrolytes

Water Gain
Water is gained from three sources.
1) food (~700 ml/day)
2) drink – voluntarily controlled
3) metabolic water (200 ml/day) --- produced as a byproduct of aerobic respiration

Routes of water loss
1) Urine – obligatory (unavoidable) and physiologically regulated, minimum 400 ml/day
2) Feces -- obligatory water loss, ~200 ml/day
3) Breath – obligatory water loss, ~300 ml/day
4) Cutaneous evaporation -- obligatory water loss, ~400 ml/day
5) Sweat – for releasing heat, varies significantly

Regulation of Water Intake
- governed by thirst.
blood volume and osmolarity
peripheral volume sensors central osmoreceptors
hypothalamus
thirst felt

Regulation of Water Output
- The only physiological control is through variations in urine volume.
- urine volume regulated by hormones

1) ADH dehydration
blood volume and/or osmolarity
hypothalamic receptors / peripheral volume sensors
posterior pituitary to release ADH
H2O reabsorption
Water retention

2) Atrial Natriuretic Factor
blood volume
atrial volume sensors
atria to release ANF
inhibits Na+ and H2O reabsorption
water output

Dehydration
- decrease in body fluid
- Causes
1) the lack of drinking water
2) excessive loss of body fluid due to:
overheat
diabetes
overuse of diuretics
diarrhea

Edema
- the accumulation of fluid in the interstitial spaces
caused by:
1) increased capillary filtration, or
2) reduced capillary reabsorption, or
3) obstructed lymphatic drainage

ELECTROLYTE BALANCE

Electrolytes = small ions that carry charges

Major cations
Na+
K+
Ca++
H+
Major anions
Cl-
HCO3-
PO4---

Na+
K+Ca++
Cl-PO4
---
Distribution of Electrolytes
Cell
Extracellularspace

Sodium Na+
Functions
- involved in generating action membrane potential of cells
- make a major contribution to extracellular osmolarity.
Na+
K+Ca++
Cl- PO4---
Cell

Regulation of plasma Na+
1) Aldosterone
plasma Na+
aldosterone
renal Na + excretion
plasma Na +
Na+
plasma

2) Renin-angiotensin-II
renin
angiotensin-II
aldosterone
renal Na+ excretion
plasma Na+
Na+
plasma
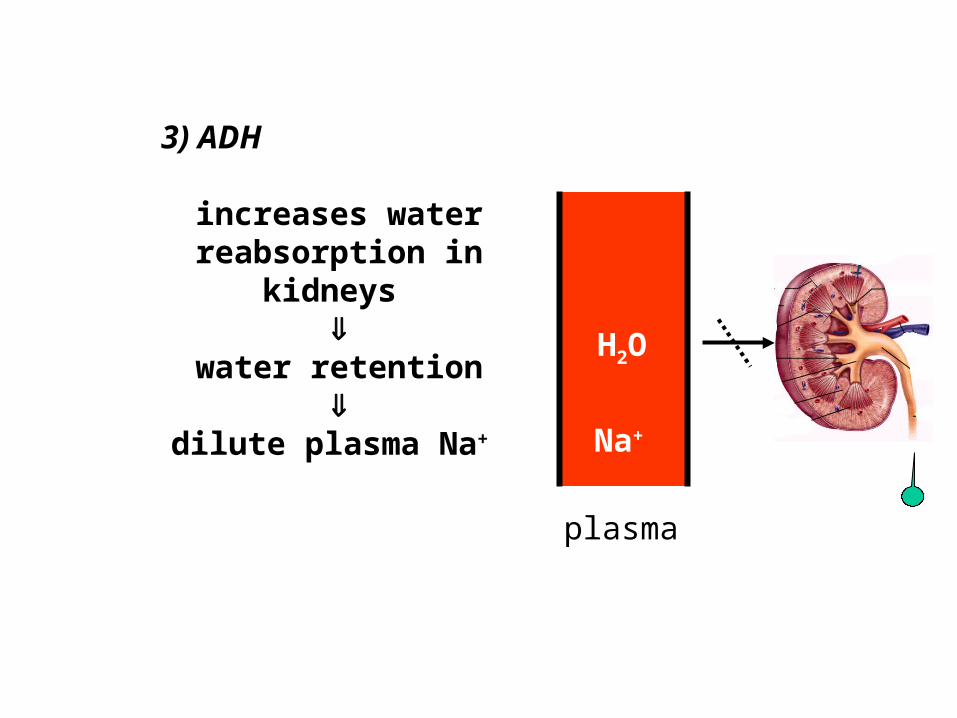
3) ADH
increases water reabsorption in
kidneys
water retention
dilute plasma Na+
plasma
Na+
H2O

4) Atrial Natriuretic Factor
inhibits renal reabsorption of Na+ and H2O and
the excretion of renin and ADH
eliminate more sodium
and water
plasma Na +
Na+
plasma Na+

Sodium imbalance
hypernatremia plasma sodium > 145 mEq/L,
hyponatremia plasma sodium < 130 mEq/L

Potassium
Functions
- the greatest contributor to intracellular osmosis and cell volume
- determines the resting membrane potentials
- an essential cofactor for protein synthesis and some other metabolic processes.
K+Na+
K+Ca++
Cl- PO4---
Cell

Regulation of Potassium
- by aldosterone
Aldosterone
stimulates K+
secretion by the kidneys
Plasma K+
K+
plasma K+

Potassium Imbalance
hyperkalemia (> 5.5 mEq/L)
hypokalemia (< 3.5 mEq/L)

Chloride
- makes a major contribution to extracellular osmolarity
- required for the formation of stomach acid (HCl)
Na+
K+Ca++
Cl- PO4---
Cell
Regulation of Cl–
- No direct regulation
- indirectly regulated as an effect of Na+ homeostasis. As sodium is retained or excreted, Cl– passively follows.
Chloride Imbalance
hyperchloremia (> 105 mEq/L)
hypochloremia (< 95 mEq/L).

Calcium
Na+
K+Ca++
Cl- PO4---
Cell

Functions of Ca++
- lends strength to the skeleton
Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
Excitation Contraction[ Ca++ ]i
(Action Potentials) (shortening)

Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
- serves as a second messenger for some hormones and neurotransmitters

Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
- serves as a second messenger for some hormones and neurotransmitters
- activates exocytosis
of neurotransmitters and
other cellular secretions

Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
- serves as a second messenger for some hormones and neurotransmitters
- activates exocytosis of neurotransmitters and other cellular secretions
- essential factor
in blood clotting.

Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
- serves as a second messenger for some hormones and neurotransmitters
- activates exocytosis of neurotransmitters and other cellular secretions
- essential factor in blood clotting.
- activates many cellular
enzymes

Dynamics of Calcium
Ca++
plasma
Ca++
Ca++
Ca++

Regulation of calcium
1) parathyroid hormone (PTH):

Regulation of calcium
1) parathyroid hormone (PTH):
- dissolving Ca++ in bones
- reducing renal excretion of Ca++
plasma
Ca++
Ca++

2) calcitonin (secreted by C cells in thyroid gland):

2) calcitonin (secreted by C cells in thyroid gland):
depositing Ca++ in bones
plasma
Ca++
Ca++

3) calcitrol (derivative of vitamin D):
- enhancing intestinal absorption of Ca++ from food
plasma
Ca++
Ca++
Ca++

Calcium imbalances
hypocalcemia (< 4.5 mEq/L)
hypercalcemia (> 5.8 mEq/L).

Phosphates
- needed for the synthesis of:
ATP, GTP
DNA, RNA
phospholipids

Regulation of Phosphate
- by parathyroid hormone
PTH
increases renal excretion of phosphate
decrease plasma
phosphate
- no real phosphate
imbalances
PO4---
plasma PO4---
ACID-BASE BALANCE

Acid An acid is any chemical that releases H+ in
solution.
Base A base is any chemical that accepts H+.

pH
is the negative logarithm of H+ concentration, and an indicator of acidity.
pH = - log [H+ ]
Example: [H+ ] = 0.1 M = 10 –7 M

pH
is the negative logarithm of H+ concentration, and an indicator of acidity.
pH = - log [10 –7 ]
Example: [H+ ] = 0.1 M = 10 –7 M
= 7 log 10 = 7

pH
is the negative logarithm of H+ concentration, and an indicator of acidity.
pH = - log [10 –8 ]
Example: [H+ ] = 0.01 M = 10 –8 M
= 8 log 10 = 8
[ H+ ] = pH
[ H+ ] = pH 0.01 M [ H+ ] = pH 8
0.1 M [ H+ ] = pH 7

Normal functions of proteins (especially
enzymes) heavily depend on an optimal pH.
pH7.35-pH7.45

Regulation of acid-base balance
1) Chemical Buffers
2) Respiratory Control of pH
3) Renal Control of pH

Buffer
is any mechanism that resists changes in
pH.
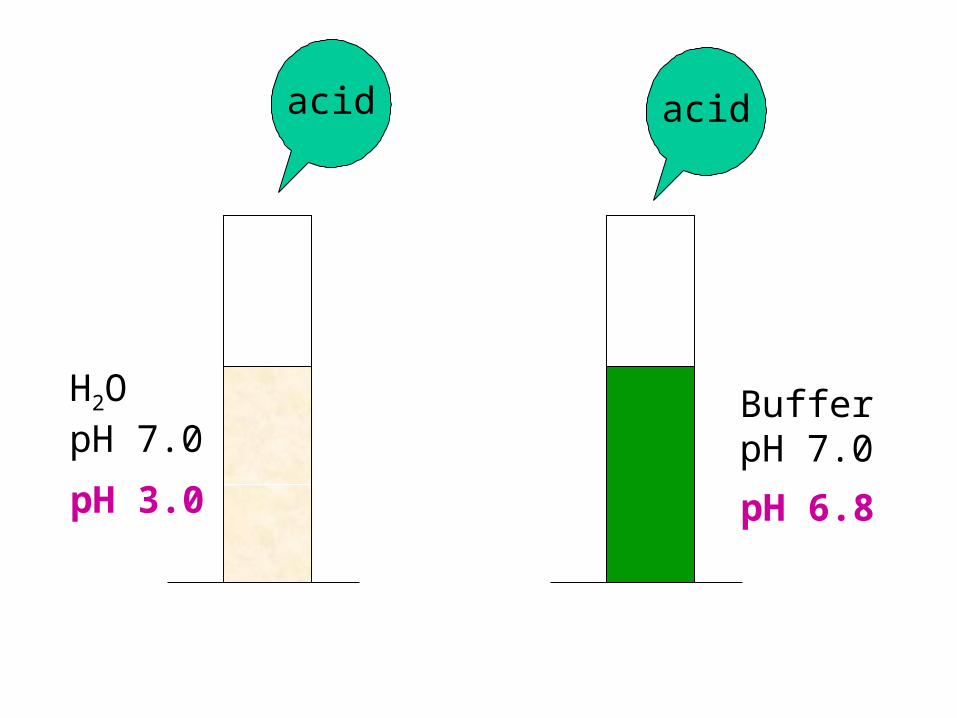
H2OpH 7.0
BufferpH 7.0
acid
pH 3.0 pH 6.8
acid

H2OpH 7.0
BufferpH 7.0
base
pH 11.0 pH 7.2
base

3) The Protein Buffer
There are three major buffers in body fluid.
1) The Bicarbonate (HCO3-) Buffer
2) The Phosphate Buffer
Chemical Buffers

1) The Bicarbonate (HCO3-) Buffer System
H + HCO3- H2CO3 H2O + CO2
- reversible depending on the equilibrium between the substrates and products.
- The lungs constantly remove CO2.

2) The Phosphate Buffer System
H + HPO42– H2PO4
– + H H3PO4

3) The Protein Buffer System
- more concentrated than either bicarbonate or phosphate buffers
- accounts for about three-quarters of all chemical buffering ability of the body fluids.
- The carboxyl groups release H+ when pH rises and amino groups bind H+ when pH falls.
NH2-CH2-CH2 CH2-CH2-COOH
H+ H+

Properties of Chemical Buffers
- respond to pH changes within a fraction of a second.
- Bind to H but can not remove H out of the body
- Limited ability to correct pH changes

H2CO3 H2O + CO2
10 20 20
H + HCO3- H2CO3 H2O + CO2
10 10 10 10 10
1)
20 10 10 10 10
2) H + HCO3- H2CO3 H2O + CO2
10 0 20 10 10
3) H + HCO3- H2CO3 H2O + CO2

Respiratory Control of pH
H + HCO- H2CO3 CO2 + H2O
H + HCO- H2CO3 CO2 + H2O

pH
stimulate peripheral/central chemoreceptors
pulmonary ventilation
removal of CO2 and pH
H2CO3
H + HCO3- H2O + CO2

Limit to respiratory control of pH
The respiratory regulatory mechanism cannot remove H+ out of the body. Its efficiency depends on the availability of HCO3
- .
H + HCO3- H2CO3 H2O + CO2

Renal Control of pH
1. The kidneys can neutralize more acid or base than both the respiratory system and chemical buffers.
a. Renal tubules secrete hydrogen ions into the tubular fluid, where most of it combines with bicarbonate, ammonia, and phosphate buffers.
b. Bound and free H+ are then excreted in urine.

2. The kidneys are the only organs that actually expel H+ from the body. Other buffering systems only reduce its concentration by binding it to another chemical.
3. Tubular secretion of H+ continues as long as a sufficient concentration gradient exists between the tubule cells and the tubular fluid.

Disorders of Acid-Base Balance
Acidosis: < pH 7.35 , Alkalosis: > pH 7.45
- Mild acidosisdepresses CNS, causing
confusion, disorientation, and coma.
- Mild alkalosis CNS becomes hyperexcitable. Nerves fire spontaneously and overstimulate skeletal muscles.
- Severe acidosis or alkalosis is lethal.

Respiratory vs Metabolic Cause
Respiratory acidosis / alkalosis - caused by hypoventilation or hyperventilation
H + HCO- H2CO3 H2O + CO2
Initial change
Emphysema

Respiratory acidosis / alkalosis - caused by hypoventilation or hyperventilation
Metabolic acidosis or alkalosis
- result from any causes but respiratory problems
Diabetes
production of organic acids
metabolic acidosis
Chronic vomiting
loss of stomach acid
metabolic alkalosis