blood transfusion, nutrition and water & electrolyte balance
TRANSCRIPT
Blood Products & TransfusionBlood Products & Transfusion Nutrition in SurgeryNutrition in Surgery
Water & Electrolyte BalanceWater & Electrolyte Balance
Dr.Ramesh ParajuliDr.Ramesh ParajuliMS (ORL-HNS)MS (ORL-HNS)
Chitwan Medical College Teaching Hospital, Bharatpur-10, chitwan, Nepal


Blood Transfusion:Blood Transfusion:
Blood Product :- Any Blood Product :- Any therapeutic substances therapeutic substances prepared from human prepared from human blood blood
Blood & Blood Products:Blood & Blood Products:
1.Whole Blood1.Whole Blood
2.Blood & Plasma 2.Blood & Plasma componentscomponents
3.Plasma Derivatives: 3.Plasma Derivatives: albumin, coagulation albumin, coagulation factors, immunoglobulinfactors, immunoglobulin

Human Blood GroupsHuman Blood Groups
23 human blood group systems23 human blood group systems
eg. ABO,MN, Duffy, Lewis, Kelleg. ABO,MN, Duffy, Lewis, Kell
ABO-most importantABO-most important
RBC Cell surface: A ,B,AB antigensRBC Cell surface: A ,B,AB antigens
Plasma : anti-B, anti-A, anti-A & anti-BPlasma : anti-B, anti-A, anti-A & anti-B
- IgM antibody- IgM antibody
HistoryHistory
1900- Karl Landsteiner discovered A,B,O1900- Karl Landsteiner discovered A,B,O
1902-Decastrello & Sturli discovered AB1902-Decastrello & Sturli discovered AB
1939-Levine & Stetson1939-Levine & Stetson
1940-Landsteiner & Weiner1940-Landsteiner & Weiner Rh system Rh system

Rh SystemRh System
Rh antigens-RBC membraneRh antigens-RBC membrane
About 15% population= Rh About 15% population= Rh NegativeNegative
Rh antibody=IgG antibodyRh antibody=IgG antibody
Anti-Rh antibody= ‘‘rhogam”Anti-Rh antibody= ‘‘rhogam”

Blood GroupingBlood Grouping
1.Before a person gets blood donation1.Before a person gets blood donation
2.Before a person donates blood2.Before a person donates blood
3.Before a person donates an organ for transplantation3.Before a person donates an organ for transplantation
4.Before surgery4.Before surgery
5.Women planning to become pregnant or has first becomes 5.Women planning to become pregnant or has first becomes pregnantpregnant
6.To show whether two people could be blood relatives6.To show whether two people could be blood relatives
7.To check identity of a person suspected of committing 7.To check identity of a person suspected of committing crimecrime
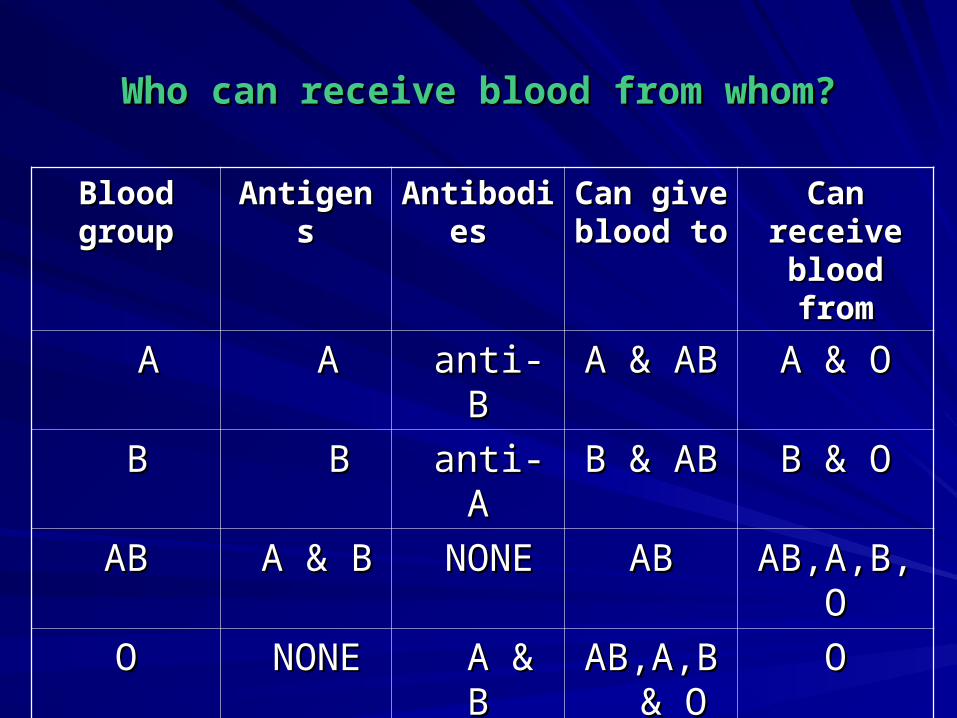
Who can receive blood from whom?Who can receive blood from whom?
Blood Blood groupgroup
AntigensAntigens AntibodieAntibodies s
Can give Can give blood toblood to
Can Can receive receive
blood fromblood from
AA A A anti-Banti-B A & ABA & AB A & OA & O
BB BB anti-Aanti-A B & AB B & AB B & OB & O
ABAB A & BA & B NONENONE ABAB AB,A,B,OAB,A,B,O
OO NONENONE A & BA & B AB,A,B AB,A,B & O& O
OO


Complications & Risks:Complications & Risks:For the Donor:For the Donor:
1.Vasovagal syncope1.Vasovagal syncope
2.Bruise at the needle site2.Bruise at the needle site
3.Hematoma at the needle site3.Hematoma at the needle site
4.Fatigue 4.Fatigue
5.Nausea & vomiting5.Nausea & vomiting
For the Patient:For the Patient:
1.Febrile non hemolytic reaction1.Febrile non hemolytic reaction
2.Vol.overload2.Vol.overload
3.Iron overload3.Iron overload
4.Graft vs host disease4.Graft vs host disease
5.Acute hemolytic reactions5.Acute hemolytic reactions

Donor unit-Donor unit-
Must be refrigerated to prevent bacterial growthMust be refrigerated to prevent bacterial growth
Must begin within 3o min after taking out of Must begin within 3o min after taking out of fridgefridge
Intravenously Intravenously
Personal details of the patients to be matched Personal details of the patients to be matched with the donorwith the donor to prevent transfusion to prevent transfusion reactionsreactions
Contraindications for being a Blood Contraindications for being a Blood DonorDonor
For Recipient SafetyFor Recipient Safety
1.Donor who recently received transfusion1.Donor who recently received transfusion2.Recent pregnancy2.Recent pregnancy3.History of cancer eg. leukemia, lymphoma3.History of cancer eg. leukemia, lymphoma
4.Current infection4.Current infection
For Donor SafetyFor Donor Safety
1.Donors not healthy enough1.Donors not healthy enough2.Nutritional status2.Nutritional status3.Age-17 to 70 yrs3.Age-17 to 70 yrs

Blood products
Platelet components
Red cell components
Plasma components &
derivatives
Apheresis

Red cell Red cell componentscomponents
Plasma Plasma componentscomponents
Plasma Plasma derivativesderivatives
Red cell Red cell concentrateconcentrate
Red cell Red cell suspension (red suspension (red cells + additive cells + additive solution)solution)
Buffy coat Buffy coat depleted red cellsdepleted red cells
Leukocyte-Leukocyte-depleted (filtered) depleted (filtered) red cellsred cells
Fresh frozen Fresh frozen plasmaplasma
Liquid plasmaLiquid plasma
Freeze-dried Freeze-dried plasmaplasma
Cryoprecipitate-Cryoprecipitate-depleted plasmadepleted plasma
Viral-inactivated Viral-inactivated plasmaplasma
CryoprecipitateCryoprecipitate
AlbuminAlbumin
Coagulation Coagulation factorsfactors
ImmunoglobulinImmunoglobulin

Centrifugation at different rpm and duration
PRP FFP Cold room
Definition :Definition : The transfusion of safe blood products to treat a condition The transfusion of safe blood products to treat a condition
leading to significant morbidity or mortality that can’t be leading to significant morbidity or mortality that can’t be prevented or managed effectively by other means.prevented or managed effectively by other means.
-Can save life-Can save life
-Improve health-Improve health

1.Homologous Transfusion1.Homologous Transfusion
2.Autologous Transfusion2.Autologous Transfusion
Blood TransfusionBlood Transfusion

Functions of anticoagulant-Functions of anticoagulant-preservativepreservativesolution in blood collection packsolution in blood collection packSolutionsSolutions FunctionsFunctions
CC Sodium citrateSodium citrate Binds with calcium ions in blood Binds with calcium ions in blood in exchange for the sodium salt in exchange for the sodium salt so the blood does not clotso the blood does not clot
PP PhosphatePhosphate Supports metabolism of the red Supports metabolism of the red cells during storage to ensure cells during storage to ensure they release oxygen readily at they release oxygen readily at tissue leveltissue level
DD DextroseDextrose Maintains the red cell Maintains the red cell membrane to increase storage membrane to increase storage lifelife
AA AdenineAdenine Provides energy sourceProvides energy source
Whole BloodWhole Blood::
1.Sterile, disposable plastic pack1.Sterile, disposable plastic pack
2.Anticoagulant-Preservative:-CPDA2.Anticoagulant-Preservative:-CPDA
3.Volume up to 510ml (63 ml anticoagulant,450ml blood)3.Volume up to 510ml (63 ml anticoagulant,450ml blood)
4.Hb-12gm/dl,Hct-35%4.Hb-12gm/dl,Hct-35%
5.No functional platelets5.No functional platelets
6.No labile coagulation factors (V & VIII)6.No labile coagulation factors (V & VIII)

Whole BloodWhole Blood
Indications Indications – Red cell replacement in acute blood loss with Red cell replacement in acute blood loss with
hypovolemiahypovolemia– Exchange transfusionExchange transfusion– Patients needing red cell transfusions where red Patients needing red cell transfusions where red
cell concentrates or suspensions are not availablecell concentrates or suspensions are not available
Contraindications Contraindications – (Risk of volume overload)– (Risk of volume overload)
– Chronic anemiaChronic anemia– Incipient cardiac failureIncipient cardiac failure

Effects of storage on whole bloodEffects of storage on whole blood
Reduction in the pHReduction in the pH
Rise in plasma potassium concentrationRise in plasma potassium concentration
Progressive reduction in the red cell content of 2,3 Progressive reduction in the red cell content of 2,3 diphosphoglycerate (2,3 DPG) diphosphoglycerate (2,3 DPG)
Loss of all platelet function in whole blood within 48 hours Loss of all platelet function in whole blood within 48 hours of donationof donation
Reduction in Factor VIII to 10–20% of normal within 48 Reduction in Factor VIII to 10–20% of normal within 48 hours of donation. Coagulation factors such as VII and IX hours of donation. Coagulation factors such as VII and IX are relatively stable in storageare relatively stable in storage

Administration Administration – Must be ABO and Rh compatible with the Must be ABO and Rh compatible with the
recipientrecipient– storage:2-6*Cstorage:2-6*C– Use within 35 days Use within 35 days – Transfuse within ½ hrs of removal from Transfuse within ½ hrs of removal from
refrigeratorrefrigerator– Complete transfusion within 4 hrs of Complete transfusion within 4 hrs of
commencementcommencement– Never add medication to a unit of bloodNever add medication to a unit of blood

Advantages:Advantages:
1.Requires only simple & inexpensive single collection pack1.Requires only simple & inexpensive single collection pack
2.Supplies all components & volume2.Supplies all components & volume
Disadvantages:Disadvantages:1.Risk of circulatory overload, transmitting infection1.Risk of circulatory overload, transmitting infection
2.No functional platelet or labile clotting factors2.No functional platelet or labile clotting factors

Production of Whole BloodProduction of Whole Blood
Donor –whole blood-ABO & RhD testingDonor –whole blood-ABO & RhD testing
II
Test for infectious diseases markersTest for infectious diseases markers
II
Negative positiveNegative positive
I II I
Quarentine refrigerator discardQuarentine refrigerator discard
II
releaserelease
II
Blood bank refrigeratorBlood bank refrigeratorcompatibility testcompatibility testcompatiblecompatible pts pts
Red cell Concentrate Red cell Concentrate (Packed Red cells)(Packed Red cells)
Prepared by allowing the blood to Prepared by allowing the blood to separate under gravity in refrigerator at separate under gravity in refrigerator at 2-6*C overnight2-6*C overnight
oror
By centrifugingBy centrifuging
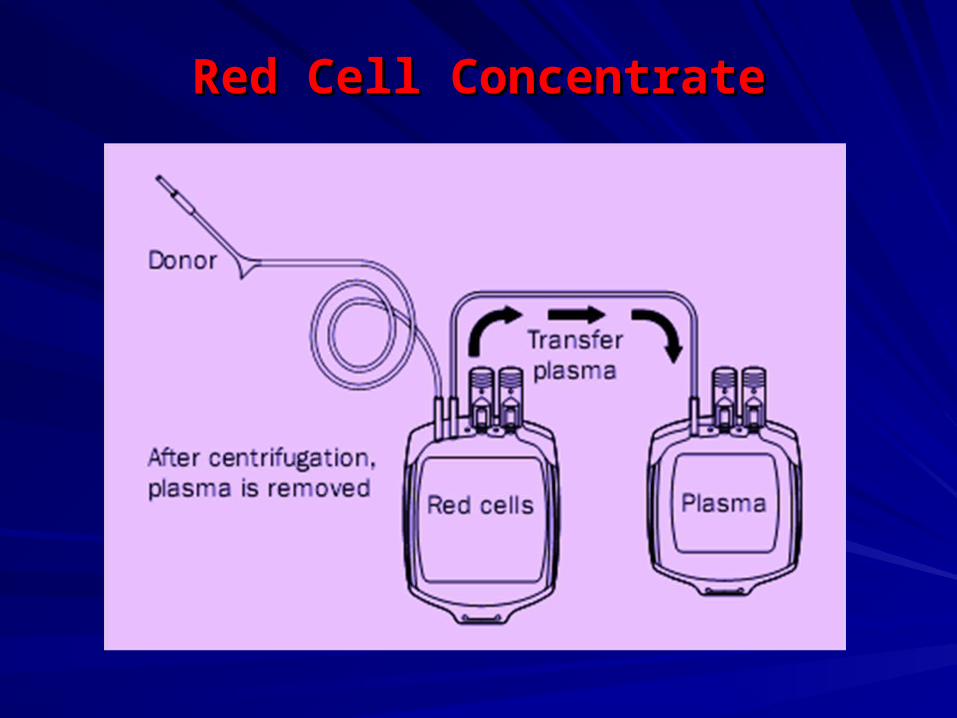
Red Cell ConcentrateRed Cell Concentrate
150-200ml red cells150-200ml red cells
Hb approx. 20gm/dl(not<45gm per unit)Hb approx. 20gm/dl(not<45gm per unit)
Hct 55 -75%Hct 55 -75%
Indications Indications – Replacement of red cells in anemic patientsReplacement of red cells in anemic patients– Use with crystalloid replacement fluids or colloid Use with crystalloid replacement fluids or colloid
solution in acute blood losssolution in acute blood loss
Administration Administration – Same as whole bloodSame as whole blood– To improve transfusion flow, normal saline (50–To improve transfusion flow, normal saline (50–
100 ml) may be added using a Y-pattern infusion 100 ml) may be added using a Y-pattern infusion setset

Advantages:Advantages:
simple, cheapersimple, cheaper
Disadvantages:Disadvantages:
--Increases viscosityIncreases viscosity
-Febrile Non haemolytic Transfusion Reaction-Febrile Non haemolytic Transfusion Reaction

Red cell SuspensionRed cell Suspension

150–200 ml red cells with minimal residual plasma150–200 ml red cells with minimal residual plasma
110 ml normal saline, adenine, glucose, mannitol 110 ml normal saline, adenine, glucose, mannitol solution (SAG-M) or an equivalent red cell nutrient solution (SAG-M) or an equivalent red cell nutrient solution addedsolution added
Hb approximately 15 g/dL (not < 45 g per unit)Hb approximately 15 g/dL (not < 45 g per unit)
Hct – 50–70%Hct – 50–70%
Indications – Same as red cell concentrateIndications – Same as red cell concentrate
Contraindications – exchange transfusion of Contraindications – exchange transfusion of neonatesneonates

Administration Administration – Same as whole bloodSame as whole blood– Better flow rates than red cell concentrate Better flow rates than red cell concentrate
or whole bloodor whole blood
Advantages:Advantages:-Reduces viscosity-Reduces viscosity-Better preservation of the red cells-Better preservation of the red cells-Permits separated use of platelets & plasma-Permits separated use of platelets & plasma
Disadvantages:Disadvantages:-Cost a special blood collection set-Cost a special blood collection set-Expensive equipment (refrigerated centrifuge)-Expensive equipment (refrigerated centrifuge)

Red cell suspension or concentrate containing < 5 x 10Red cell suspension or concentrate containing < 5 x 1066 white cells per packwhite cells per pack
Preparation – filtration through a leucocyte-depleting filterPreparation – filtration through a leucocyte-depleting filter
Leucocyte depletion removes the risk of transmission of Leucocyte depletion removes the risk of transmission of cytomegalovirus (CMV)cytomegalovirus (CMV)
Leucocyte-Depleted (Filtered) Red cells Leucocyte-Depleted (Filtered) Red cells or Whole Bloodor Whole Blood
IndicationsIndications– Minimizes white cell immunization in Minimizes white cell immunization in
patients receiving repeated transfusionpatients receiving repeated transfusion– Reduces risk of CMV transmissionReduces risk of CMV transmission– Patients who have experienced two or Patients who have experienced two or
more previous febrile reactions to red cell more previous febrile reactions to red cell transfusiontransfusion
ContraindicationsContraindications– Will not prevent graft-vs-host diseaseWill not prevent graft-vs-host disease
Advantages:Advantages:
--Decreases development of immunity to Decreases development of immunity to white cellswhite cells
-Decreased transfusion reaction-Decreased transfusion reaction
-Decreases chance of transmitting viral -Decreases chance of transmitting viral infection eg; CMVinfection eg; CMV
Disadvantages:Disadvantages:
--Special instrument & blood pack neededSpecial instrument & blood pack needed
-Skilled & trained operator needed-Skilled & trained operator needed

Buffy Coat Depleted Red CellsBuffy Coat Depleted Red Cells
--White cells & platelets are removed by White cells & platelets are removed by controlled centrifugationcontrolled centrifugation
Advantages:Advantages:
-Red cells & only about 10% of the -Red cells & only about 10% of the white cells remains in concentratewhite cells remains in concentrate
-Use to prepare platelets concentrates-Use to prepare platelets concentrates
DisadvantagesDisadvantages
--Expensive procedureExpensive procedure
-More skilled manpower needed-More skilled manpower needed
Platelet ConcentratesPlatelet Concentrates
Single donor unit in a volume of 50–60 ml of Single donor unit in a volume of 50–60 ml of plasma should contain:plasma should contain:– At least 55 x 10At least 55 x 1099 platelets platelets– <1.2 x 10<1.2 x 1099 red cells red cells– <0.12 x 10<0.12 x 1099 leucocytes leucocytes
Single donor unit : platelets prepared from one Single donor unit : platelets prepared from one donationdonation
Pooled unit : platelets prepared from 4 to 6 donor Pooled unit : platelets prepared from 4 to 6 donor units ‘pooled’ into one pack to contain an adult units ‘pooled’ into one pack to contain an adult dose of at least 240 x 10dose of at least 240 x 1099 platelets platelets
Bacterial contamination affects about 1% of Bacterial contamination affects about 1% of pooled unitspooled units
Indications Indications
Treatment of bleeding due to:Treatment of bleeding due to:ThrombocytopeniaThrombocytopeniaPlatelet function defectsPlatelet function defectsPrevention of bleeding due to Prevention of bleeding due to thrombocytopenia, such as in bone marrow thrombocytopenia, such as in bone marrow failurefailure

Contraindications Contraindications
– Not generally indicated for prophylaxis of Not generally indicated for prophylaxis of bleeding in surgical patients, unless known bleeding in surgical patients, unless known to have significant pre-operative platelet to have significant pre-operative platelet deficiencydeficiency
– Not indicated in:Not indicated in:ITPITPTTPTTPDICDICThrombocytopenia associated with Thrombocytopenia associated with septicemia, until treatment has septicemia, until treatment has commenced or in cases of commenced or in cases of hypersplenismhypersplenism

DosageDosage– 1 unit of platelet concentrate/10 kg body 1 unit of platelet concentrate/10 kg body
weight : in a 60 or 70 kg adult, 4–6 single weight : in a 60 or 70 kg adult, 4–6 single donor units containing at least donor units containing at least 240 x 10240 x 1099 platelets should raise the platelet count by platelets should raise the platelet count by 20–40 x 1020–40 x 1099/L/L
– Increment will be less if there is:Increment will be less if there is:SplenomegalySplenomegalyDICDICSepticemiaSepticemia
Contd.
AdministrationAdministration
-After pooling, platelet concentrates should be -After pooling, platelet concentrates should be infused as infused as
soon as possible generally within 4 hourssoon as possible generally within 4 hours
– Must not be refrigerated before infusion as this Must not be refrigerated before infusion as this reduces platelet functionreduces platelet function
– 4–6 units of platelet concentrates should be 4–6 units of platelet concentrates should be infused through a fresh standard blood infused through a fresh standard blood administration setadministration set
– Special platelet infusion sets are not requiredSpecial platelet infusion sets are not required

– Platelet concentrates should be Platelet concentrates should be infused over about 30 minutesinfused over about 30 minutes
– Platelet concentrates prepared from Platelet concentrates prepared from Rh D positive donors should not be Rh D positive donors should not be given to a Rh D negative potential given to a Rh D negative potential child-bearing femalechild-bearing female
– Platelet concentrates that are ABO Platelet concentrates that are ABO compatible should be given compatible should be given whenever possiblewhenever possible

ComplicationsComplications
– Febrile Non-hemolytic ReactionsFebrile Non-hemolytic Reactions– Allergic Urticarial ReactionsAllergic Urticarial Reactions– Pooling increases transmission of infectionPooling increases transmission of infection

FRESH FROZEN PLASMAFRESH FROZEN PLASMA
Fresh Frozen PlasmaFresh Frozen Plasma
Pack containing the plasma separated from one Pack containing the plasma separated from one whole blood donation within 6 hours of collection and whole blood donation within 6 hours of collection and then rapidly frozen to –25°C or colderthen rapidly frozen to –25°C or colder
Contains normal plasma levels of stable Contains normal plasma levels of stable clotting clotting factors, albumin and immunoglobulinfactors, albumin and immunoglobulinFactor VIII level at least 70% of normal fresh plasma Factor VIII level at least 70% of normal fresh plasma levellevel
Usual volume of pack is 200–300 mlUsual volume of pack is 200–300 ml
Smaller volume packs may be available for childrenSmaller volume packs may be available for children
Very low risk of infection if treated with methylene Very low risk of infection if treated with methylene blue/ultraviolet light inactivationblue/ultraviolet light inactivation

IndicationsIndications
– Replacement of multiple coagulation factor Replacement of multiple coagulation factor deficiencies, e.g: -deficiencies, e.g: -
Liver diseaseLiver disease
Warfarin overdoseWarfarin overdose
Depletion of coagulation factors in pts Depletion of coagulation factors in pts receiving large volume transfusionsreceiving large volume transfusions
DICDIC
TTPTTP
Dosage – Dosage – Initial dose of 15 ml/kgInitial dose of 15 ml/kg
AdministrationAdministration --Must normally be ABO compatible to avoid risk of Must normally be ABO compatible to avoid risk of hemolysis in recipienthemolysis in recipient
– No cross matching neededNo cross matching needed– Before use, should be thawed in water which is Before use, should be thawed in water which is
between 30°C and 37°C.between 30°C and 37°C.– Higher temperatures will destroy clotting factors and Higher temperatures will destroy clotting factors and
proteinsproteins– Infuse using a standard blood infusion set as soon Infuse using a standard blood infusion set as soon
as possible after thawingas possible after thawing– Labile coagulation factors rapidly degrade; Labile coagulation factors rapidly degrade; use use
within 6 hours of thawingwithin 6 hours of thawing– Cant be refrozen for further storageCant be refrozen for further storage

CryoprecipitateCryoprecipitate
CryoprecipitateCryoprecipitate
Prepared from FFP by collecting the Prepared from FFP by collecting the precipitate formed during controlled thawing precipitate formed during controlled thawing and re suspending it in 10–20 ml plasmaand re suspending it in 10–20 ml plasma
Contains about half of the Factor VIII and Contains about half of the Factor VIII and fibrinogen in the donated whole blood: e.g. fibrinogen in the donated whole blood: e.g. Factor VIII: 80–100 I.U./pack; fibrinogen: Factor VIII: 80–100 I.U./pack; fibrinogen: 150–300 mg/pack150–300 mg/pack
Usually supplied as a single donor pack or a Usually supplied as a single donor pack or a pack of 6 or more single donor unitspack of 6 or more single donor units
CryoprecipitateCryoprecipitate
IndicationsIndications
– As an alternative to Factor VIII As an alternative to Factor VIII concentrate in the treatment of inherited concentrate in the treatment of inherited deficiencies of:deficiencies of:
Von Willebrand Factor (von Von Willebrand Factor (von Willebrand’s disease)Willebrand’s disease)
Factor VIII (haemophilia A)Factor VIII (haemophilia A)
Factor XIIIFactor XIII
As a source of fibrinogen in acquired As a source of fibrinogen in acquired coagulopathies: e.g. (DIC)coagulopathies: e.g. (DIC)

Factor VIII ConcentrateFactor VIII ConcentratePartially purified Factor VIII prepared from large Partially purified Factor VIII prepared from large pools of donor plasmapools of donor plasma
Vials of freeze-dried protein usually about 250 i.u. Vials of freeze-dried protein usually about 250 i.u. of Factor VIIIof Factor VIII
IndicationsIndications– Treatment of hemophilia ATreatment of hemophilia A– Treatment of von Willebrand’s diseaseTreatment of von Willebrand’s disease
Factor VIII prepared in vitro using recombinant Factor VIII prepared in vitro using recombinant DNA methods is commercially availableDNA methods is commercially available

Human Albumin SolutionsHuman Albumin SolutionsPrepared by fractionation of large pools of donated Prepared by fractionation of large pools of donated human plasmahuman plasma
PreparationsPreparations– Albumin 5%: contains 50 mg/ml of albuminAlbumin 5%: contains 50 mg/ml of albumin– Albumin 20%: contains 200 mg/ml of albuminAlbumin 20%: contains 200 mg/ml of albumin– Albumin 25%: contains 250 mg/ml of albuminAlbumin 25%: contains 250 mg/ml of albumin– Stable plasma protein solution (SPPS) and plasma Stable plasma protein solution (SPPS) and plasma
protein fraction (PPF): similar albumin content to protein fraction (PPF): similar albumin content to albumin 5%albumin 5%
IndicationsIndications– Replacement fluid in therapeutic plasma exchange Replacement fluid in therapeutic plasma exchange
ContraindicationsContraindications - Not for use as IV nutrition - Not for use as IV nutrition

Volume of Blood ProductsVolume of Blood Products
Blood productBlood product VolumeVolume
Whole blood (CPDA-1)Whole blood (CPDA-1) 350 ml350 ml
Whole blood for component Whole blood for component separationseparation
450 ml450 ml
Packed red blood cells (CPD)Packed red blood cells (CPD) 150-200 ml150-200 ml
Packed red blood cells (SAGM)Packed red blood cells (SAGM) 200-250 ml200-250 ml
Fresh frozen plasmaFresh frozen plasma 100-150 ml100-150 ml
Cryo poor plasmaCryo poor plasma 100-150 ml100-150 ml
Platelet rich plasmaPlatelet rich plasma 100-150 ml100-150 ml
Platelet concentratePlatelet concentrate 50-70 ml50-70 ml
CryoprecipitateCryoprecipitate 15-20 ml15-20 ml
Buffy coatBuffy coat 50-70 ml50-70 ml
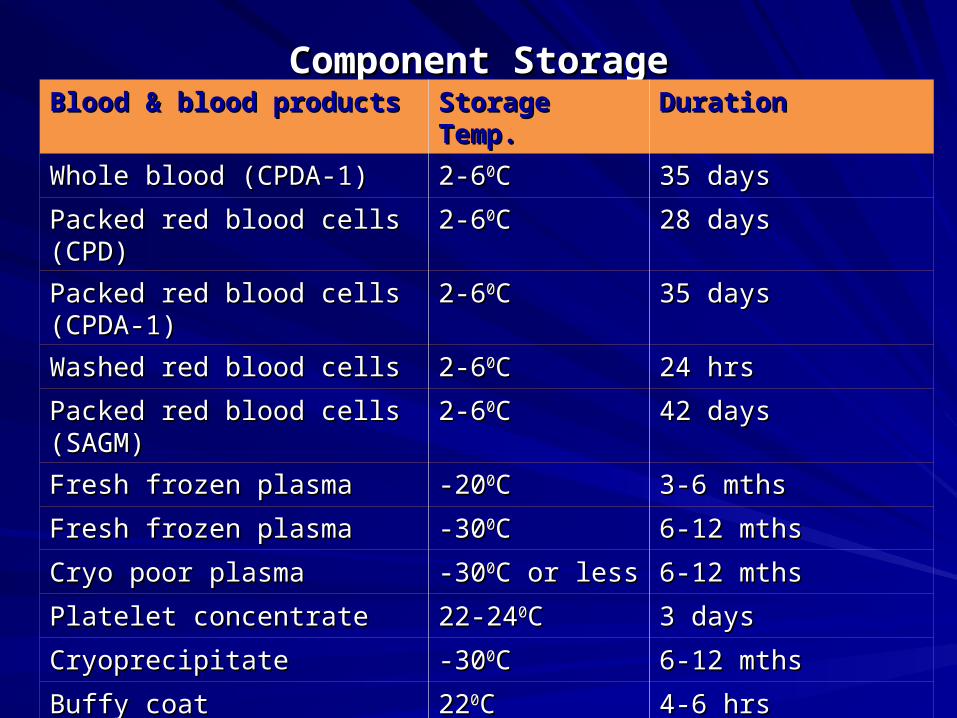
Component StorageComponent StorageBlood & blood productsBlood & blood products Storage Temp.Storage Temp. Duration Duration
Whole blood (CPDA-1)Whole blood (CPDA-1) 2-62-600CC 35 days35 days
Packed red blood cells (CPD)Packed red blood cells (CPD) 2-62-600CC 28 days28 days
Packed red blood cells (CPDA-Packed red blood cells (CPDA-1)1)
2-62-600CC 35 days35 days
Washed red blood cellsWashed red blood cells 2-62-600CC 24 hrs24 hrs
Packed red blood cells Packed red blood cells (SAGM)(SAGM)
2-62-600CC 42 days42 days
Fresh frozen plasmaFresh frozen plasma -20-2000CC 3-6 mths3-6 mths
Fresh frozen plasmaFresh frozen plasma -30-3000CC 6-12 mths6-12 mths
Cryo poor plasmaCryo poor plasma -30-3000C or lessC or less 6-12 mths6-12 mths
Platelet concentratePlatelet concentrate 22-2422-2400CC 3 days 3 days
CryoprecipitateCryoprecipitate -30-3000CC 6-12 mths6-12 mths
Buffy coatBuffy coat 222200CC 4-6 hrs4-6 hrs
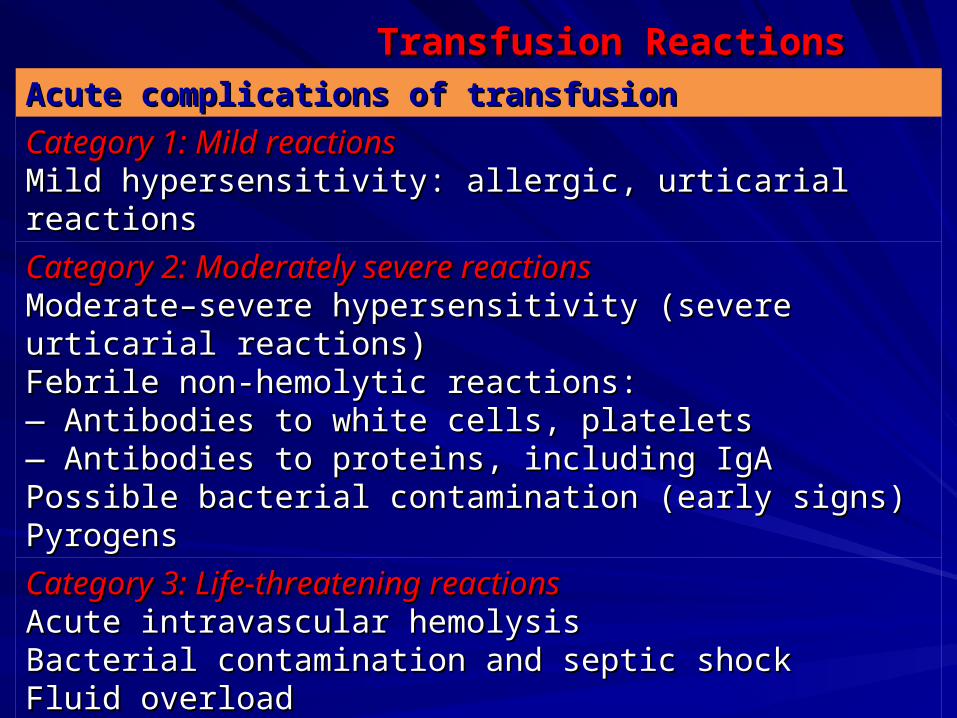
Transfusion ReactionsTransfusion ReactionsAcute complications of transfusionAcute complications of transfusion
Category 1: Mild reactionsCategory 1: Mild reactionsMild hypersensitivity: allergic, urticarial reactionsMild hypersensitivity: allergic, urticarial reactions
Category 2: Moderately severe reactionsCategory 2: Moderately severe reactionsModerate–severe hypersensitivity (severe urticarial reactions)Moderate–severe hypersensitivity (severe urticarial reactions)Febrile non-hemolytic reactions:Febrile non-hemolytic reactions:— — Antibodies to white cells, plateletsAntibodies to white cells, platelets— — Antibodies to proteins, including IgAAntibodies to proteins, including IgAPossible bacterial contamination (early signs)Possible bacterial contamination (early signs)PyrogensPyrogens
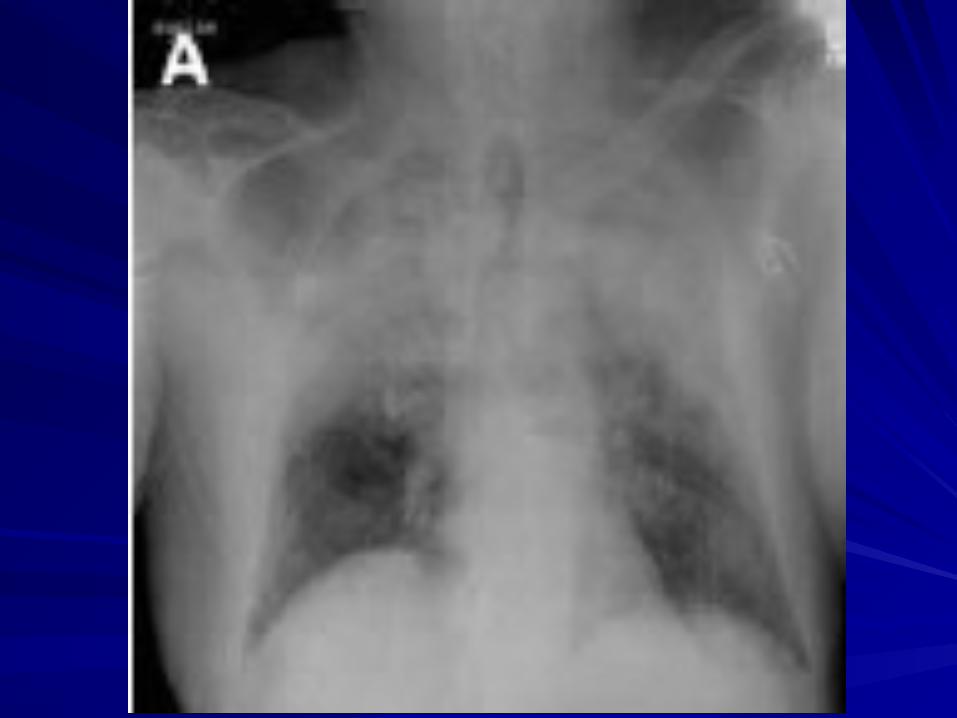
Category 3: Life-threatening reactionsCategory 3: Life-threatening reactionsAcute intravascular hemolysisAcute intravascular hemolysisBacterial contamination and septic shockBacterial contamination and septic shockFluid overloadFluid overloadAnaphylactic reactionsAnaphylactic reactionsTransfusion-associated Acute lung injury (TRALI)Transfusion-associated Acute lung injury (TRALI)
Delayed complications of transfusionDelayed complications of transfusion
Transfusion-transmitted infections :Transfusion-transmitted infections :HIV-1 and HIV-2HIV-1 and HIV-2HTLV-I and IIHTLV-I and IIViral hepatitis B and CViral hepatitis B and CSyphilisSyphilisChagas diseaseChagas diseaseMalariaMalariaCytomegalovirusCytomegalovirusOther rare infections: e.g. human parvovirus B19 and Other rare infections: e.g. human parvovirus B19 and
hepatitis Ahepatitis A
Other delayed complications of transfusion :Other delayed complications of transfusion :Delayed hemolytic reactionDelayed hemolytic reactionPost-transfusion PurpuraPost-transfusion PurpuraGraft-vs-host diseaseGraft-vs-host diseaseIron overload Iron overload

Management of Transfusion ReactionsManagement of Transfusion Reactions
CategoryCategory SignsSigns SymptomsSymptomsCategory 1: Category 1: Mild reactionsMild reactions
Localized cutaneousLocalized cutaneousreactions: Urticaria, Rashreactions: Urticaria, Rash
Pruritus (itching)Pruritus (itching)
Category 2: Category 2: Moderately Moderately severe severe reactionsreactions
FlushingFlushingUrticariaUrticariaRigorsRigorsFeverFeverRestlessnessRestlessnessTachycardiaTachycardia
AnxietyAnxietyPruritus (itching)Pruritus (itching)PalpitationsPalpitationsMild dyspnoeaMild dyspnoeaHeadacheHeadache
Category 3: Category 3: Life-Life-threatening threatening reactionsreactions
RigorsRigorsFeverFeverRestlessnessRestlessnessHypotension (fall of ≥20% in Hypotension (fall of ≥20% in SBP)SBP)Tachycardia (rise of ≥20% in HR)Tachycardia (rise of ≥20% in HR)Haemoglobinuria (red urine)Haemoglobinuria (red urine)Unexplained bleeding (DIC)Unexplained bleeding (DIC)
AnxietyAnxietyChest painChest painPain near infusion sitePain near infusion siteRespiratory Respiratory distress/SOBdistress/SOBLoin/back painLoin/back painHeadacheHeadacheDyspnoeaDyspnoea

CATEGORY 1: MILDCATEGORY 1: MILD1.Slow the transfusion1.Slow the transfusion
2.Administer antihistamine IM (e.g. 2.Administer antihistamine IM (e.g. chlorpheniramine 0.1 mg/kg or chlorpheniramine 0.1 mg/kg or equivalent).equivalent).
3.If no clinical improvement within 30 3.If no clinical improvement within 30 minutes or if signs and symptoms minutes or if signs and symptoms worsen, worsen, treat as Category 2.treat as Category 2.
CATEGORY 2: MODERATELY SEVERECATEGORY 2: MODERATELY SEVERE1. Stop the transfusion. Replace the infusion set and keep 1. Stop the transfusion. Replace the infusion set and keep
IV line open with normal salineIV line open with normal saline
2. Notify the doctor and the blood bank immediately.2. Notify the doctor and the blood bank immediately.
3. Send blood unit with infusion set, freshly collected urine 3. Send blood unit with infusion set, freshly collected urine and new blood samples (1 clotted and 1 anticoagulated) and new blood samples (1 clotted and 1 anticoagulated) from vein opposite infusion site to blood bank and from vein opposite infusion site to blood bank and laboratory for investigations.laboratory for investigations.
4. Administer antihistamine IM (e.g. chlorpheniramine 0.1 4. Administer antihistamine IM (e.g. chlorpheniramine 0.1 mg/kg or equivalent) and oral or rectal antipyretic (e.g. mg/kg or equivalent) and oral or rectal antipyretic (e.g. paracetamol 10 mg/kg: 500 mg – 1 g in adults). Avoid paracetamol 10 mg/kg: 500 mg – 1 g in adults). Avoid aspirin.aspirin.
5.5. Give IV corticosteroids and bronchodilators if there are Give IV corticosteroids and bronchodilators if there are anaphylactoid features (e.g. bronchospasm, stridor).anaphylactoid features (e.g. bronchospasm, stridor).
6.6. Collect urine for next 24 hours for evidence of Collect urine for next 24 hours for evidence of hemolysis and send to laboratory.hemolysis and send to laboratory.
7.7. If clinical improvement, restart transfusion slowly with If clinical improvement, restart transfusion slowly with new blood unit and observe carefully.new blood unit and observe carefully.
8.8. If no clinical improvement within 15 minutes or if S/S If no clinical improvement within 15 minutes or if S/S worsen, worsen, treat as Category 3.treat as Category 3.

CATEGORY 3: LIFE-THREATENINGCATEGORY 3: LIFE-THREATENING1.1. Stop the transfusion. Replace the infusion set and keep Stop the transfusion. Replace the infusion set and keep
IV line openIV line open
2.2. Infuse NS (initially 20–30 ml/kg) to maintain SBP. If Infuse NS (initially 20–30 ml/kg) to maintain SBP. If hypotensive, give over 5 minutes and elevate patient’s hypotensive, give over 5 minutes and elevate patient’s legs.legs.
3.3. Maintain airway and give high flow oxygen by mask.Maintain airway and give high flow oxygen by mask.
4.4. Give adrenaline (as 1:1000 solution) 0.01 mg/kg body Give adrenaline (as 1:1000 solution) 0.01 mg/kg body weight by slow intramuscular injection.weight by slow intramuscular injection.
5.5. Give IV corticosteroids and bronchodilators if there are Give IV corticosteroids and bronchodilators if there are anaphylactoid features (e.g. bronchospasm, stridor).anaphylactoid features (e.g. bronchospasm, stridor).
6.6. Give diuretic: e.g. frusemide 1 mg/kg IV or equivalent.Give diuretic: e.g. frusemide 1 mg/kg IV or equivalent.
7.7. Notify the doctor and the blood bank immediately.Notify the doctor and the blood bank immediately.

8.8. Send blood unit with infusion set, fresh urine sample and Send blood unit with infusion set, fresh urine sample and new blood samples (1 clotted and 1 anticoagulated) from new blood samples (1 clotted and 1 anticoagulated) from vein opposite infusion site to blood bank and laboratory vein opposite infusion site to blood bank and laboratory for investigations.for investigations.
9.9. Check a fresh urine specimen visually for signs of Check a fresh urine specimen visually for signs of haemoglobinuria (red or pink urine)haemoglobinuria (red or pink urine)
10.10. Start a 24-hour urine collection and I/O charting. Maintain Start a 24-hour urine collection and I/O charting. Maintain fluid balance.fluid balance.
11.Assess for bleeding from puncture sites or wounds. If 11.Assess for bleeding from puncture sites or wounds. If there is evidence of DIC, give platelets (adult: 5–6 units) there is evidence of DIC, give platelets (adult: 5–6 units) and either cryoprecipitate (adult: 12 units) or FFP (adult: and either cryoprecipitate (adult: 12 units) or FFP (adult: 3 units). Use virally-inactivated plasma coagulation 3 units). Use virally-inactivated plasma coagulation products, wherever possible.products, wherever possible.
12.12. Reassess. If hypotensive:Reassess. If hypotensive:
Give further saline 20–30 ml/kg over 5 minutesGive further saline 20–30 ml/kg over 5 minutes
Give ionotrope, if availableGive ionotrope, if available
13.13. If urine output falling or laboratory evidence of acute If urine output falling or laboratory evidence of acute renal failure : renal failure :
Maintain fluid balance accuratelyMaintain fluid balance accurately
Give further frusemideGive further frusemide
Consider dopamine infusion, if availableConsider dopamine infusion, if available
Seek expert help: the patient may need renal dialysisSeek expert help: the patient may need renal dialysis
14.14. If bacteremia is suspected, start broad-spectrum If bacteremia is suspected, start broad-spectrum antibiotics IV, to cover pseudomonas and gram antibiotics IV, to cover pseudomonas and gram positives.positives.

Massive Blood TransfusionMassive Blood TransfusionDefined as the replacement of blood loss Defined as the replacement of blood loss equivalent to or greater than the patient’s total equivalent to or greater than the patient’s total blood volume with stored blood in < 24 hours blood volume with stored blood in < 24 hours (70 ml/kg in adults, 80–90 ml/kg in children or (70 ml/kg in adults, 80–90 ml/kg in children or infants)infants)
ComplicationsComplications– AcidosisAcidosis– HyperkalemiaHyperkalemia– Citrate toxicity and hypocalcaemiaCitrate toxicity and hypocalcaemia– Depletion of fibrinogen and coagulation factorsDepletion of fibrinogen and coagulation factors– Depletion of plateletsDepletion of platelets– DICDIC– HypothermiaHypothermia– Reduced 2,3 diphosphoglycerate (2,3 DPG)Reduced 2,3 diphosphoglycerate (2,3 DPG)– MicroaggregatesMicroaggregates

(1)Preoperative Blood Deposit (PAD)(1)Preoperative Blood Deposit (PAD)
(2)Acute Normovolaemic Haemodilution(2)Acute Normovolaemic Haemodilution
(3)Blood salvage(3)Blood salvage– Gauze filtrationGauze filtration– Simple suction collection systemsSimple suction collection systems– Automated suction collection systemsAutomated suction collection systems– Modified drain Modified drain
Autologous Blood TransfusionAutologous Blood Transfusion

Artificial Oxygen CarrierArtificial Oxygen Carrier
(1)Hemoglobin-based Oxygen Carriers (HBOC) (1)Hemoglobin-based Oxygen Carriers (HBOC)
(2)Products based on Perfluorocarbons (PF)(2)Products based on Perfluorocarbons (PF)
AdvantageAdvantage– Can be sterilizedCan be sterilized– Do not have any blood group Do not have any blood group – Could be stored for a long timeCould be stored for a long time
DisadvantageDisadvantage
-Very short half life=around 24 hrs-Very short half life=around 24 hrs
-High flow O2 required-High flow O2 required

Other Methods to Reduce Red Blood Cell Other Methods to Reduce Red Blood Cell TransfusionTransfusion
1.Recombinant Erythropoietin1.Recombinant Erythropoietin
2.Fibrin Glue:2.Fibrin Glue:
11stst Syringe-calcium & human thrombin Syringe-calcium & human thrombin
22ndnd Syringe- human fibrinogen Syringe- human fibrinogen
Injected simultaneously over the minor cutaneous bleeding Injected simultaneously over the minor cutaneous bleeding sitessitesfibrin clot(glue)fibrin clot(glue)hemostasishemostasis
3.Tranexamic acid3.Tranexamic acid

Transfusions of blood products Transfusions of blood products can save lives, but are not without can save lives, but are not without risks or costsrisks or costs
Safe blood is a scarce and Safe blood is a scarce and valuable resource that is valuable resource that is expensive to collect, process and expensive to collect, process and administeradminister
Limiting Transfusion to patientsLimiting Transfusion to patients
whose chance of survival or quality of life is whose chance of survival or quality of life is improved with blood will help to decrease improved with blood will help to decrease the high demand for blood products and the high demand for blood products and will reduce unnecessary exposure of will reduce unnecessary exposure of patients to the risks of transfusion.patients to the risks of transfusion.

Maximum Blood Ordering ScheduleMaximum Blood Ordering Schedule
Elective Surgical ProcedureElective Surgical Procedure
Agreement between Surgeons, Agreement between Surgeons, Anaesthesiologists & HaematologistsAnaesthesiologists & Haematologists
ProcedureProcedure Blood OrderBlood Order
Tumor of palateTumor of palate G & S G & S
LaryngectomyLaryngectomy 2 units2 units
RNDRND 2 units2 units
CommandoCommando 4 units4 units
Getting The Right Blood to the RightGetting The Right Blood to the RightPatient at the Right TimePatient at the Right Time
Nutrition in Nutrition in SurgerySurgery

30% – 50% of hospitalized patients – malnourished30% – 50% of hospitalized patients – malnourished
Malnutrition a/w increased morbidity and mortalityMalnutrition a/w increased morbidity and mortality
Most healthy patients can tolerate 7 days of starvation (with Most healthy patients can tolerate 7 days of starvation (with adequate glucose and fluid replacement)adequate glucose and fluid replacement)
Preoperative nutritional support can significantly reduce Preoperative nutritional support can significantly reduce perioperative morbidity and mortality in patients with severe perioperative morbidity and mortality in patients with severe malnutrition malnutrition
Protein RequirementsProtein Requirements– Avg. healthy adult : approximately Avg. healthy adult : approximately 0.8 g/kg 0.8 g/kg
body weightbody weight– Physiologically stressed : Physiologically stressed : 1.2 – 2.5 g/kg/day1.2 – 2.5 g/kg/day– protein intake of 6.25 g equivalent to 1 g of protein intake of 6.25 g equivalent to 1 g of
nitrogennitrogen– 15% of normal energy expenditure15% of normal energy expenditure– 1 gm of protein = 4 kcal1 gm of protein = 4 kcal
Carbohydrate RequirementsCarbohydrate Requirements– 40-60 % of normal energy expenditure40-60 % of normal energy expenditure– 400 kcal of CHO/day minimizes protein 400 kcal of CHO/day minimizes protein
breakdown, particularly after adaptation to breakdown, particularly after adaptation to starvationstarvation
– 1 gm of Enteral CHO = 4 kcal & 1 gm of Enteral CHO = 4 kcal &
1gm of Parenteral CHO = 3.4 kcal/g1gm of Parenteral CHO = 3.4 kcal/g
Lipid Requirements :Lipid Requirements :– 25% to 45% of normal energy expenditure25% to 45% of normal energy expenditure– 1 gm of lipid = 9 kcal1 gm of lipid = 9 kcal
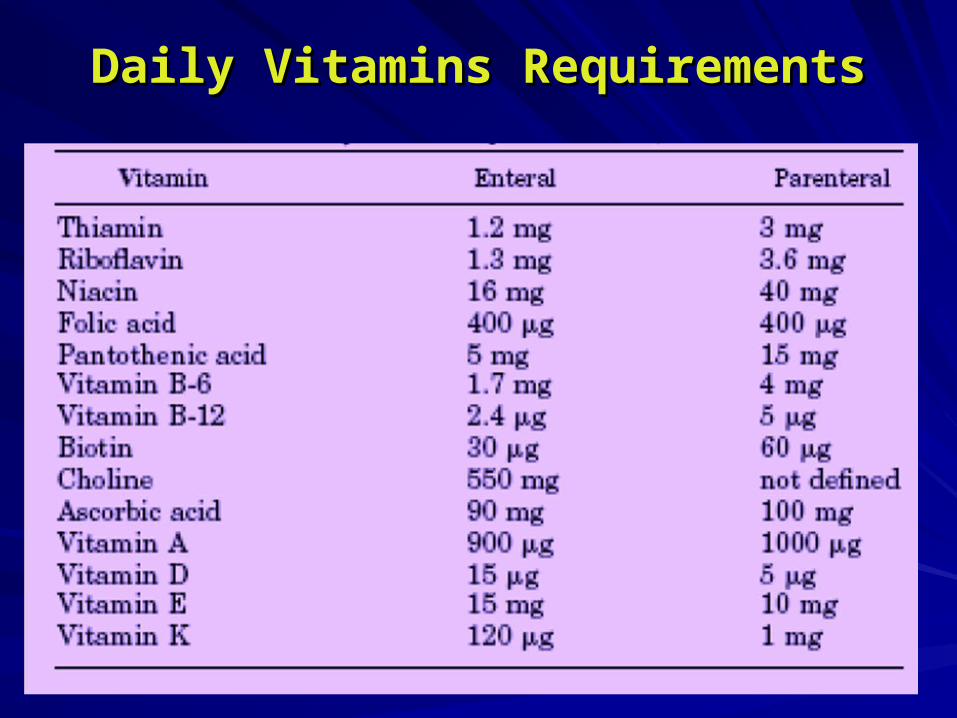
Daily Vitamins RequirementsDaily Vitamins Requirements
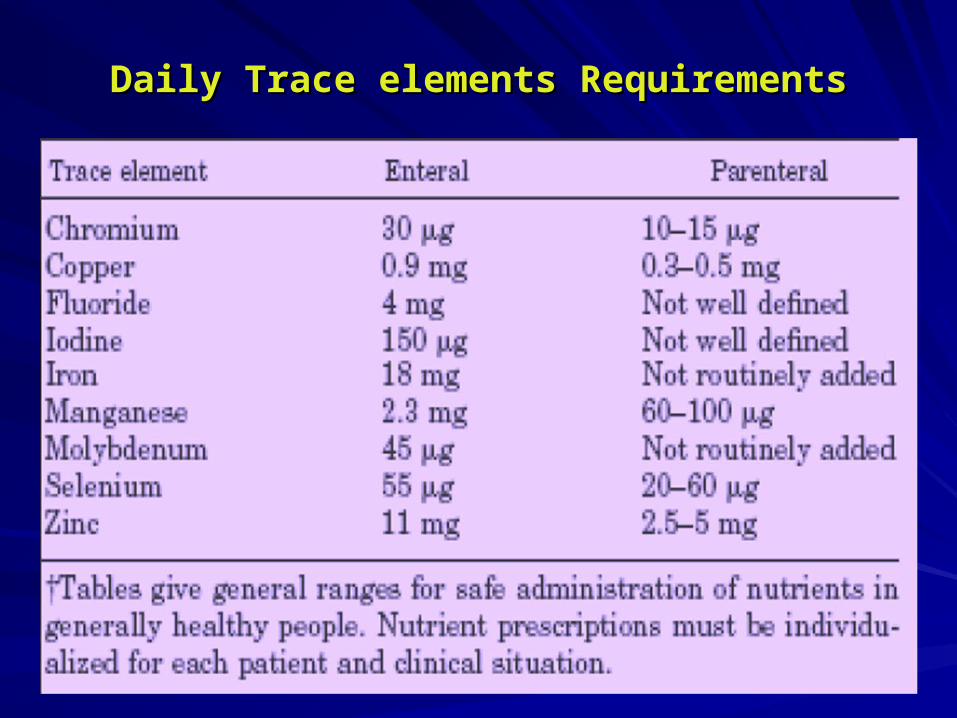
Daily Trace elements RequirementsDaily Trace elements Requirements

The The MetabolicMetabolic Response to Critical Response to Critical IllnessIllness

Nutritional AssessmentNutritional AssessmentHistory History – Weight fluctuation or a change in dietary habitsWeight fluctuation or a change in dietary habits– Recent weight lossRecent weight loss
5% in the last month5% in the last month10% over 6 months10% over 6 monthsCurrent body weight of 80% to 85% (or less) Current body weight of 80% to 85% (or less) of ideal body weightof ideal body weight
Physical ExaminationPhysical Examination– Muscle wasting (especially thenar, temporal & Muscle wasting (especially thenar, temporal &
gluteal muscles)gluteal muscles)– Loose or flabby skinLoose or flabby skin– Peripheral edema and/or ascitesPeripheral edema and/or ascites– Skin rash, pallor, glossitis, gingival lesions, hair Skin rash, pallor, glossitis, gingival lesions, hair
changes, hepatomegaly, neuropathy, and changes, hepatomegaly, neuropathy, and dementia dementia
Anthropometric measurementsAnthropometric measurements– Triceps skinfold thicknessTriceps skinfold thickness– Mid-upper arm circumferenceMid-upper arm circumference– BMIBMI
Laboratory testsLaboratory tests– Serum albumin < 3.5 g/dL Serum albumin < 3.5 g/dL – Half-life is 14 to 20 days.Half-life is 14 to 20 days.– Serum Prealbumin (indicator of acute changes) : Serum Prealbumin (indicator of acute changes) :
10 to 17 mg/dL – mild depletion10 to 17 mg/dL – mild depletion5 to 10 mg/dL – moderate depletion5 to 10 mg/dL – moderate depletion< 5 mg/dL – severe depletion < 5 mg/dL – severe depletion half-life is 2 to 3 days.half-life is 2 to 3 days.
– Serum transferrin < 200 mg/dLSerum transferrin < 200 mg/dLhalf-life is 8 to 10 days.half-life is 8 to 10 days.
Immune FunctionImmune Function– Delayed-type hypersensitivity (anergy Delayed-type hypersensitivity (anergy
to common skin antigens)to common skin antigens)– Total lymphocyte count (TLC)Total lymphocyte count (TLC)
1,500 to 1,800/mm1,500 to 1,800/mm33 – mild – mild depletiondepletion
900 to 1,500/mm900 to 1,500/mm33 – moderate – moderate depletiondepletion
< 900/mm< 900/mm33 – severe depletion – severe depletion

Nutritional IndicesNutritional Indices
Body Mass Index (BMI)Body Mass Index (BMI)BMI = weight (kg)/[height (m)]BMI = weight (kg)/[height (m)]22 BMI: Normal 18.5–24.9BMI: Normal 18.5–24.9 Overweight 25–29.9Overweight 25–29.9 Obese 30–40Obese 30–40 Morbid Obesity >40Morbid Obesity >40Prognostic Nutritional Index (PNI)Prognostic Nutritional Index (PNI)PNI = 158 - 16.6 (Alb) - 0.78 (TSF) - 0.2 (TFN) - 5.8 (DH)PNI = 158 - 16.6 (Alb) - 0.78 (TSF) - 0.2 (TFN) - 5.8 (DH)DH: >5 mm induration = 2; 1–5 mm induration = 1; anergy DH: >5 mm induration = 2; 1–5 mm induration = 1; anergy = 0= 0PNI: >50% = high risk for complicationsPNI: >50% = high risk for complications 40%–49% = intermediate risk40%–49% = intermediate risk <40% = low risk<40% = low risk
Alb, albumin (g/dL); DH, delayed cutaneous hypersensitivity; TFN, transferrin (mg/dL); TSF, triceps skinfold thickness (mm); UUN, 24-hr urine urea nitrogen excretion (g)

Estimation of Caloric Estimation of Caloric RequirementsRequirements
TEE = BEE + EEA + EETTEE = BEE + EEA + EET
TEE : Total Daily Energy ExpenditureTEE : Total Daily Energy Expenditure
BEE : Basal Energy ExpenditureBEE : Basal Energy Expenditure
EEA : Energy Expenditure of Activity (25 %)EEA : Energy Expenditure of Activity (25 %)
EET : Energy Expenditure of Thermogenesis (10%)EET : Energy Expenditure of Thermogenesis (10%)
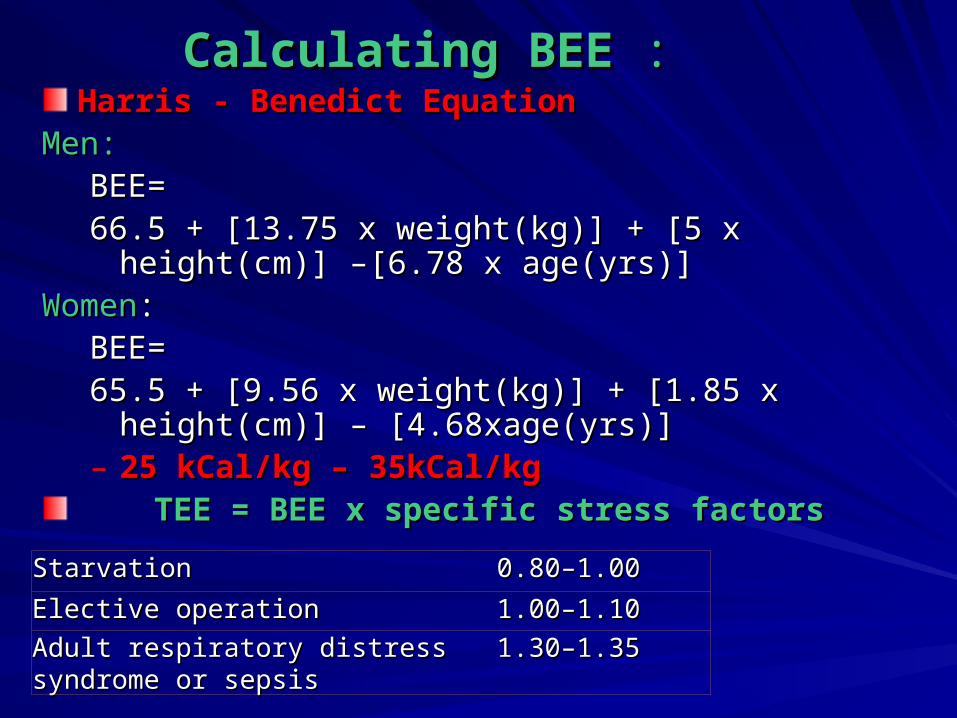
Calculating BEECalculating BEE : :Harris - Benedict EquationHarris - Benedict Equation
Men:Men:BEE= BEE= 66.5 + [13.75 x weight(kg)] + [5 x height(cm)] –[6.78 x 66.5 + [13.75 x weight(kg)] + [5 x height(cm)] –[6.78 x
age(yrs)]age(yrs)]WomenWomen::
BEE= BEE= 65.5 + [9.56 x weight(kg)] + [1.85 x height(cm)] – 65.5 + [9.56 x weight(kg)] + [1.85 x height(cm)] –
[4.68xage(yrs)][4.68xage(yrs)]– 25 kCal/kg – 35kCal/kg25 kCal/kg – 35kCal/kg
TEE = BEE x specific stress factorsTEE = BEE x specific stress factors
StarvationStarvation 0.80–1.000.80–1.00
Elective operationElective operation 1.00–1.101.00–1.10
Adult respiratory distress syndrome or Adult respiratory distress syndrome or sepsissepsis
1.30–1.351.30–1.35
Caloric requirements may be 150% more than the basal Caloric requirements may be 150% more than the basal energy expenditure in pts undergoing major surgeryenergy expenditure in pts undergoing major surgery
Phases following SurgeryPhases following Surgery(1)Phase I: Catabolic phase lasting 3-7 days, increased (1)Phase I: Catabolic phase lasting 3-7 days, increased
protein consumptionprotein consumption
(2)Phase II: Protein consumption & production are equal(2)Phase II: Protein consumption & production are equal
(3)Phase III: Anabolic phase, protein production exceeds (3)Phase III: Anabolic phase, protein production exceeds consumptionconsumption
(4)Phase IV: Restoration of lipid stores(4)Phase IV: Restoration of lipid stores

Pre-operative PreparationPre-operative Preparation
In patients with severe nutritional risk, start nutrition In patients with severe nutritional risk, start nutrition supplement 2 wks prior to surgerysupplement 2 wks prior to surgery
Solid foods allowed up to 6 hrsSolid foods allowed up to 6 hrs
Liquid foods allowed up to 4hrsLiquid foods allowed up to 4hrs
Clear liquid allowed up to 2 hrsClear liquid allowed up to 2 hrs
Preoperative carbohydrate loading, the night before and Preoperative carbohydrate loading, the night before and 2 hr before surgery recommended2 hr before surgery recommended
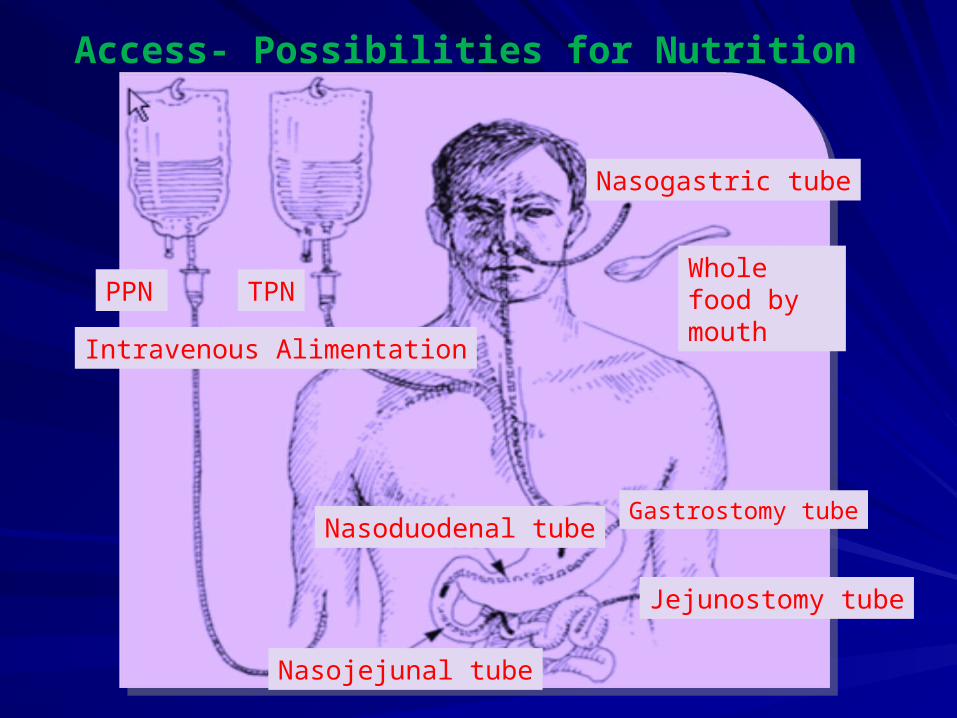
Access- Possibilities for Nutrition
Nasogastric tube
Whole food by mouth
Gastrostomy tube
Jejunostomy tube
Nasoduodenal tube
Nasojejunal tube
PPN
TPN
Intravenous Alimentation
Preferred over the Parenteral routePreferred over the Parenteral route
Simple, physiologic, relatively inexpensive, and well Simple, physiologic, relatively inexpensive, and well tolerated by most patientstolerated by most patients
Maintains the GI tract cytoarchitecture and mucosal integrity Maintains the GI tract cytoarchitecture and mucosal integrity (via trophic effects), absorptive function, and normal (via trophic effects), absorptive function, and normal microbial flora microbial flora
IndicationsIndications : patients who have a functional GI tract but are : patients who have a functional GI tract but are unable to sustain an adequate oral dietunable to sustain an adequate oral diet
ContraindicationsContraindications : intestinal obstruction, ileus, GI : intestinal obstruction, ileus, GI bleeding, severe diarrhea, vomiting, enterocolitis, or a high-bleeding, severe diarrhea, vomiting, enterocolitis, or a high-output enterocutaneous fistulaoutput enterocutaneous fistula
Enteral NutritionEnteral Nutrition

Enteral Feeding ProductsEnteral Feeding Products
– Standard Solutions – 1 kcal/mlStandard Solutions – 1 kcal/ml
- Calorically concentrated solutions – >1 kcal/ml- Calorically concentrated solutions – >1 kcal/ml
-Dietary Formulations -Dietary Formulations
Nutritionally complete formulas (standard Nutritionally complete formulas (standard enteral diets)enteral diets)
Chemically defined formulas (elemental Chemically defined formulas (elemental diets)diets)
Modular formulations (in specific clinical Modular formulations (in specific clinical situations)situations)

Bolus FeedingsBolus Feedings– Reserved for patients with nasogastric or gastrostomy Reserved for patients with nasogastric or gastrostomy
feeding tubesfeeding tubes– Administered by gravityAdministered by gravity– Begin at 50 to 100 mL every 4 hours, and increased in Begin at 50 to 100 mL every 4 hours, and increased in
50-mL increments until goal intake reached (usually 240 50-mL increments until goal intake reached (usually 240 to 360 mL every 4 hours)to 360 mL every 4 hours)
– Tracheobronchial aspiration is a potentially serious Tracheobronchial aspiration is a potentially serious complicationcomplication
Enteral Feeding Protocols
Continuous InfusionContinuous Infusion
– Administered by a pumpAdministered by a pump
– Generally required for nasojejunal, gastrojejunal, Generally required for nasojejunal, gastrojejunal, or jejunal tubesor jejunal tubes
– Initiated at 20 mL/hour and increased in 10 to Initiated at 20 mL/hour and increased in 10 to 20mL/hour increments every 4 to 6 hours until 20mL/hour increments every 4 to 6 hours until the desired goal reachedthe desired goal reached
– Can be infused over 8 to 12 hours at nightCan be infused over 8 to 12 hours at night

Conversion to Oral FeedingConversion to Oral Feeding– Resumed graduallyResumed gradually– Enteral Feeding modified asEnteral Feeding modified as
Providing fewer feedingsProviding fewer feedings
Holding daytime feedingsHolding daytime feedings
Decreasing the volume of feedingsDecreasing the volume of feedings
When oral intake provides approximately 75% of When oral intake provides approximately 75% of the required calories, tube feedings can be the required calories, tube feedings can be stoppedstopped

Administration of medicationsAdministration of medications– Many oral medications can be administeredMany oral medications can be administered– Not suitable for administration through a feeding Not suitable for administration through a feeding
tube includetube include
Enteric-coated medicationsEnteric-coated medications
Drugs in gelatinous capsulesDrugs in gelatinous capsules
Medications that are designed for sublingual Medications that are designed for sublingual useuse
Most sustained-release medicationsMost sustained-release medications

Complications of Enteral Complications of Enteral NutritionNutrition
Metabolic ComplicationsMetabolic Complications
Clogging Clogging (prevented by careful routine flushing of the (prevented by careful routine flushing of the feeding tube)feeding tube)
Tracheobronchial AspirationTracheobronchial Aspiration
High Gastric ResidualsHigh Gastric Residuals
DiarrheaDiarrhea

Parenteral NutritionParenteral Nutrition
Indicated for patients Indicated for patients – Who cannot meet their needs through oral intake Who cannot meet their needs through oral intake – Enteral feeding is contraindicated or not toleratedEnteral feeding is contraindicated or not tolerated
Peripheral parenteral nutrition (PPN)Peripheral parenteral nutrition (PPN)– Osmolarity of PPN solutions limited to 1,000 mOsm Osmolarity of PPN solutions limited to 1,000 mOsm
(approximately 12% dextrose solution)(approximately 12% dextrose solution) to avoid phlebitis to avoid phlebitis– Unacceptably large volumes (>2,500 ml) necessaryUnacceptably large volumes (>2,500 ml) necessary– Temporary nutritional supplementationTemporary nutritional supplementation
Total parenteral nutrition (TPN)Total parenteral nutrition (TPN)– Complete nutritional support Complete nutritional support – Central venous catheter requiredCentral venous catheter required– Replaced for unexplained fever or bacteremiaReplaced for unexplained fever or bacteremia

TPN SolutionsTPN Solutions
– 3-in-1 admixture3-in-1 admixture
Protein, as amino acids (10%; 4 kcal/g)Protein, as amino acids (10%; 4 kcal/g)
Carbohydrate, as dextrose (70%; 3.4 kcal/g)Carbohydrate, as dextrose (70%; 3.4 kcal/g)
Fat, as a lipid emulsion of soybean or safflower oil Fat, as a lipid emulsion of soybean or safflower oil (20%; 9 kcal/g)(20%; 9 kcal/g)
– Alternatively, the lipid emulsion can be administered Alternatively, the lipid emulsion can be administered as a separate intravenous infusionas a separate intravenous infusion
– Standard preparations availableStandard preparations available

AdditivesAdditives– Electrolytes : sodium, potassium, chloride, acetate, Electrolytes : sodium, potassium, chloride, acetate,
calcium, magnesium, phosphate adjusted dailycalcium, magnesium, phosphate adjusted daily– Number of cations and anions must balanceNumber of cations and anions must balance– Calcium : Phosphate ratio must be monitored to Calcium : Phosphate ratio must be monitored to
prevent salt precipitationprevent salt precipitation
Medications Medications
– Albumin, HAlbumin, H22-receptor antagonists, heparin, iron, -receptor antagonists, heparin, iron,
dextran, insulin, and Metoclopramidedextran, insulin, and Metoclopramide– Regular Insulin after adjusting doseRegular Insulin after adjusting dose

Other additivesOther additives– Trace elements added daily eg. commercially Trace elements added daily eg. commercially
prepared mixtureprepared mixture– Multivitamins generally added daily using a Multivitamins generally added daily using a
commercially prepared mixture commercially prepared mixture (e.g., 10 mL MVI-12)(e.g., 10 mL MVI-12)– Vitamin K not included in most multivitamin mixtures Vitamin K not included in most multivitamin mixtures
and must be added separately and must be added separately (10 mg once a week)(10 mg once a week)– Vitamins A and C and zinc essential for proper wound Vitamins A and C and zinc essential for proper wound
healing.healing.

Routine Physiologic and Laboratory MonitoringRoutine Physiologic and Laboratory Monitoring– On a scheduled basisOn a scheduled basis
– More frequently whose postoperative course has not More frequently whose postoperative course has not stabilizedstabilized
– Vital signs and serum glucose Vital signs and serum glucose every 6 hoursevery 6 hours
– Weight, serum electrolytes, and blood urea nitrogen Weight, serum electrolytes, and blood urea nitrogen dailydaily
– Triglycerides, CBC, PT, liver enzymes, and bilirubin Triglycerides, CBC, PT, liver enzymes, and bilirubin weeklyweekly
Administration of TPNAdministration of TPNIntroduction of TPNIntroduction of TPN– Gradual. e.g. approximately 1,000 kcal in 1Gradual. e.g. approximately 1,000 kcal in 1stst day day– Caloric goal achieved over 1 to 2 daysCaloric goal achieved over 1 to 2 days
TPN solutionsTPN solutions– Continuous infusionContinuous infusion
Cyclic administration of TPN solutionsCyclic administration of TPN solutions– Useful for selected patientsUseful for selected patients
Discontinuation of TPNDiscontinuation of TPN– Satisfies 75% of his or her caloric and protein needs Satisfies 75% of his or her caloric and protein needs
with oral intake or enteral feedingwith oral intake or enteral feeding
Complications Associated Complications Associated with TPNwith TPN
Catheter-Related ComplicationsCatheter-Related Complications
Metabolic Complications – Na overload, CHF, Metabolic Complications – Na overload, CHF, electrolyte imbalance, hyperglycemia and electrolyte imbalance, hyperglycemia and hyperosmolarity hyperosmolarity
(hyperglycemia may be the first indication of occult (hyperglycemia may be the first indication of occult infection)infection)
Refeeding Syndrome – in severely malnourished Refeeding Syndrome – in severely malnourished patientpatient
Hepatic Dysfunction – steatosis, raised AST, Hepatic Dysfunction – steatosis, raised AST, ALT, ALP & Bil. finally cirrhosisALT, ALP & Bil. finally cirrhosis
Cholecystitis – Acalculous type d/t CholestasisCholecystitis – Acalculous type d/t Cholestasis
Adverse Effects and RisksAdverse Effects and Risks
Parenteral NutritionParenteral Nutrition
OverfeedingOverfeeding
HyperglycemiaHyperglycemia
Infectious ComplicationsInfectious Complications
Gut Mucosal Atrophy?Gut Mucosal Atrophy?
Bacterial translocation?Bacterial translocation?
Early Enteral NutritionEarly Enteral Nutrition
Procedure-related Procedure-related complications complications High gastric residualsHigh gastric residualsBacterial colonization of Bacterial colonization of the stomachthe stomachAspiration PneumoniaAspiration Pneumonia
Water & Electrolyte BalanceWater & Electrolyte Balance
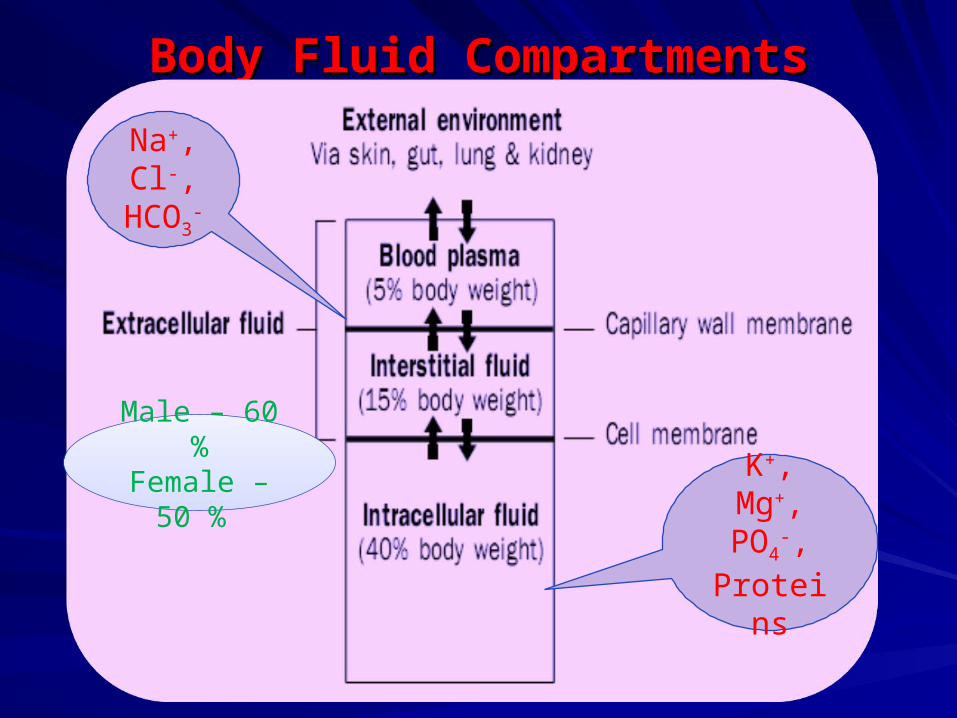
Body Fluid CompartmentsBody Fluid Compartments
K+, Mg+, PO4
-, Proteins
Na+, Cl-,
HCO3-
Male – 60 %Female – 50
%
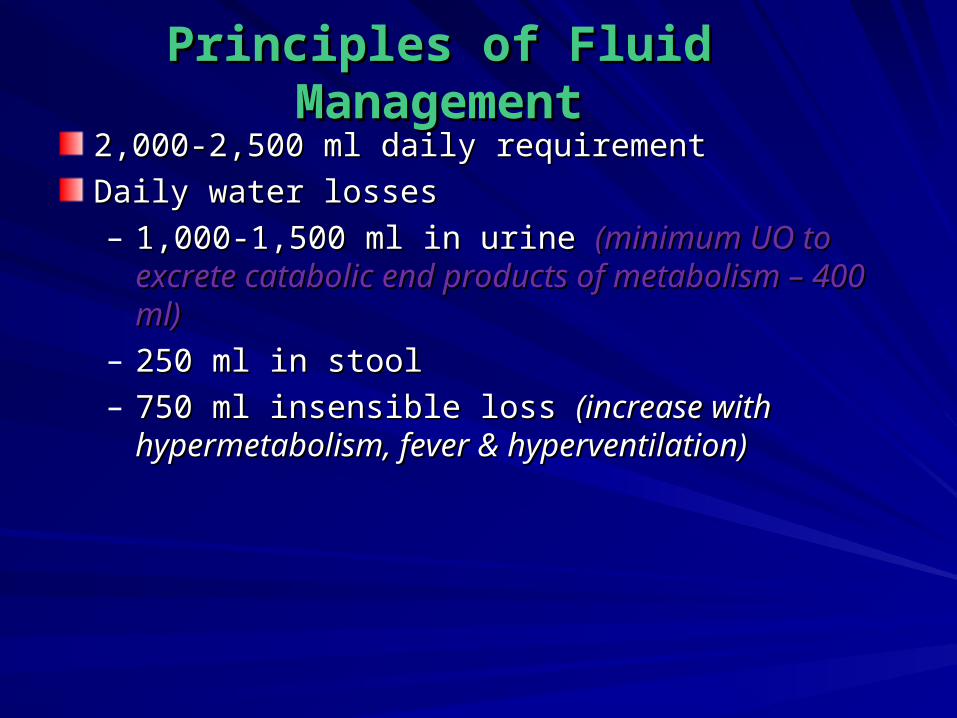
Principles of Fluid Principles of Fluid ManagementManagement
2,000-2,500 ml daily requirement2,000-2,500 ml daily requirement
Daily water losses Daily water losses – 1,000-1,500 ml in urine 1,000-1,500 ml in urine (minimum UO to excrete (minimum UO to excrete
catabolic end products of metabolism – 400 ml)catabolic end products of metabolism – 400 ml)– 250 ml in stool250 ml in stool– 750 ml insensible loss 750 ml insensible loss (increase with hypermetabolism, (increase with hypermetabolism,
fever & hyperventilation)fever & hyperventilation)

MaintenanceMaintenance– Maintain urine output of 0.5 to 1 ml/kg/hour in Maintain urine output of 0.5 to 1 ml/kg/hour in
adult & 1 to 2 ml/kg/hr in childrenadult & 1 to 2 ml/kg/hr in children
eg. in adult UO at least 30 ml/hreg. in adult UO at least 30 ml/hr
– Estimation of Maintenance FluidEstimation of Maintenance FluidFirst 10 kg – 100 ml/kg/day First 10 kg – 100 ml/kg/day
Second 10 kg – 50 ml/kg/daySecond 10 kg – 50 ml/kg/day
Then for subsequent kg – 20 ml/kg/dayThen for subsequent kg – 20 ml/kg/day
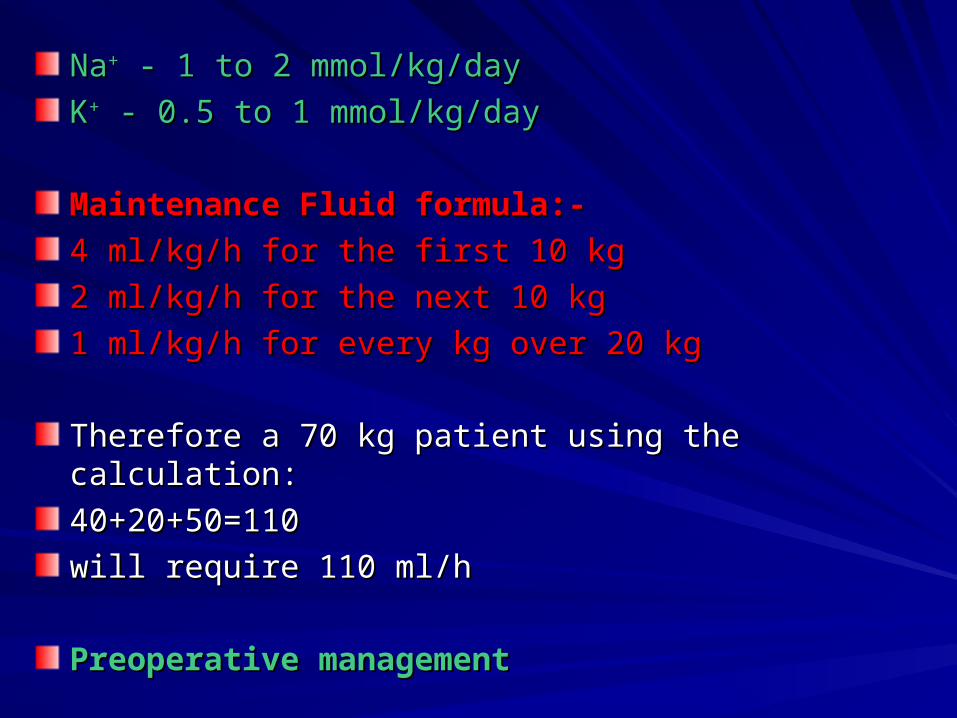
NaNa++ - 1 to 2 mmol/kg/day - 1 to 2 mmol/kg/day
KK++ - 0.5 to 1 mmol/kg/day - 0.5 to 1 mmol/kg/day
Maintenance Fluid formula:-Maintenance Fluid formula:-
4 ml/kg/h for the first 10 kg4 ml/kg/h for the first 10 kg
2 ml/kg/h for the next 10 kg2 ml/kg/h for the next 10 kg
1 ml/kg/h for every kg over 20 kg1 ml/kg/h for every kg over 20 kg
Therefore a 70 kg patient using the calculation:Therefore a 70 kg patient using the calculation:
40+20+50=11040+20+50=110
will require 110 ml/hwill require 110 ml/h
Preoperative managementPreoperative management

Intraoperative fluid managementIntraoperative fluid management– duration of the caseduration of the case– hemorrhagehemorrhage– third-space lossesthird-space losses
Estimation of Intraoperative Fluid Loss and Guide for Estimation of Intraoperative Fluid Loss and Guide for ReplacementReplacement
Preoperative deficitPreoperative deficit Maintenance IVF × hr NPO, plus Maintenance IVF × hr NPO, plus preexisting deficit related to preexisting deficit related to disease statedisease state
Maintenance fluidsMaintenance fluids Maintenance IVF × duration of Maintenance IVF × duration of casecase
Third-space and Third-space and insensible lossesinsensible losses
1–3 mL/kg/hr for minor procedure 1–3 mL/kg/hr for minor procedure (small incision)(small incision)3–7 mL/kg/hr for moderate 3–7 mL/kg/hr for moderate procedure (medium incision)procedure (medium incision)9–11 mL/kg/hr for extensive 9–11 mL/kg/hr for extensive procedure (large incision)procedure (large incision)
Blood lossBlood loss 1 mL blood or colloid per 1 mL 1 mL blood or colloid per 1 mL blood loss, or 3 mL crystalloid per blood loss, or 3 mL crystalloid per 1 mL blood loss1 mL blood loss

Postoperative Fluid Postoperative Fluid ManagementManagement
– Sequestration of ECF can continue for > 12 Sequestration of ECF can continue for > 12 hours after operationhours after operation
– Maintain Urine OutputMaintain Urine Output– GI lossesGI losses from NG or Gastrostomy tube suction from NG or Gastrostomy tube suction
Replaced with an equal volume ofReplaced with an equal volume of CrystalloidCrystalloid– Mobilization of Peri-operative third-space fluid Mobilization of Peri-operative third-space fluid
losses typically begins 2 to 3 days after losses typically begins 2 to 3 days after operationoperation

Commonly Used Parenteral SolutionsCommonly Used Parenteral Solutions
IV IV solutionsolution
Osmolality Osmolality (mOsm/L)(mOsm/L)
[Glucose] [Glucose] (g/L)(g/L)
[Na[Na++] ] (mEq/L)(mEq/L)
[Cl[Cl--] ] (mEq/L)(mEq/L)
[HCO[HCO33--] ]
equivalents equivalents (mEq/L)(mEq/L)
DD55WW 278278 5050 00 00 00
DD1010WW 556556 100100 00 00 00
DD5050WW 27782778 500500 00 00 00
0.225% 0.225% NaClNaCl
7777 00 38.538.5 38.538.5 00
0.45% NaCl0.45% NaCl 154154 00 7777 7777 00
0.9% NaCl0.9% NaCl 308308 00 154154 154154 00
3% NaCl3% NaCl 10261026 00 513513 513513 00
Lactated* Lactated* Ringer'sRinger's
274274 00 130130 109109 2828
*Also contains 4 mEq/l K+, 1.5 mEq/l Ca++, and 28 mEq/l lactate.
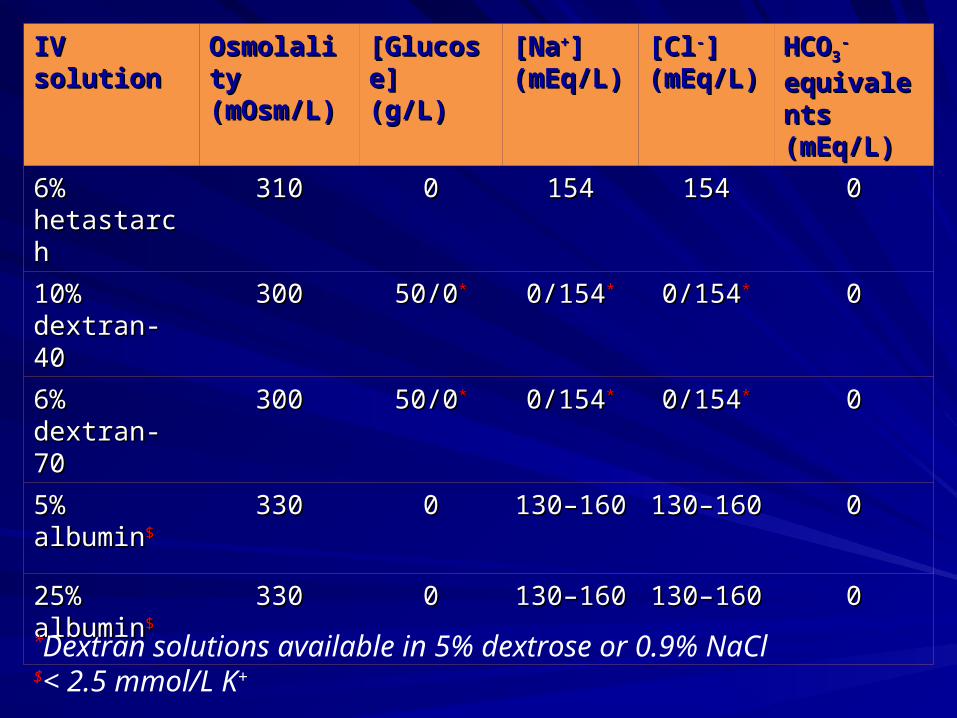
IV solutionIV solution Osmolality Osmolality (mOsm/L)(mOsm/L)
[Glucose] [Glucose] (g/L)(g/L)
[Na[Na++] ] (mEq/L)(mEq/L)
[Cl[Cl--] ] (mEq/L)(mEq/L)
HCOHCO33--
equivalentequivalents (mEq/L)s (mEq/L)
6% 6% hetastarchhetastarch
310310 00 154154 154154 00
10% 10% dextran-40dextran-40
300300 50/050/0** 0/1540/154** 0/1540/154** 00
6% 6% dextran-70dextran-70
300300 50/050/0** 0/1540/154** 0/1540/154** 00
5% albumin5% albumin$$ 330330 00 130–160130–160 130–160130–160 00
25% 25% albuminalbumin$$
330330 00 130–160130–160 130–160130–160 00
*Dextran solutions available in 5% dextrose or 0.9% NaCl$< 2.5 mmol/L K+
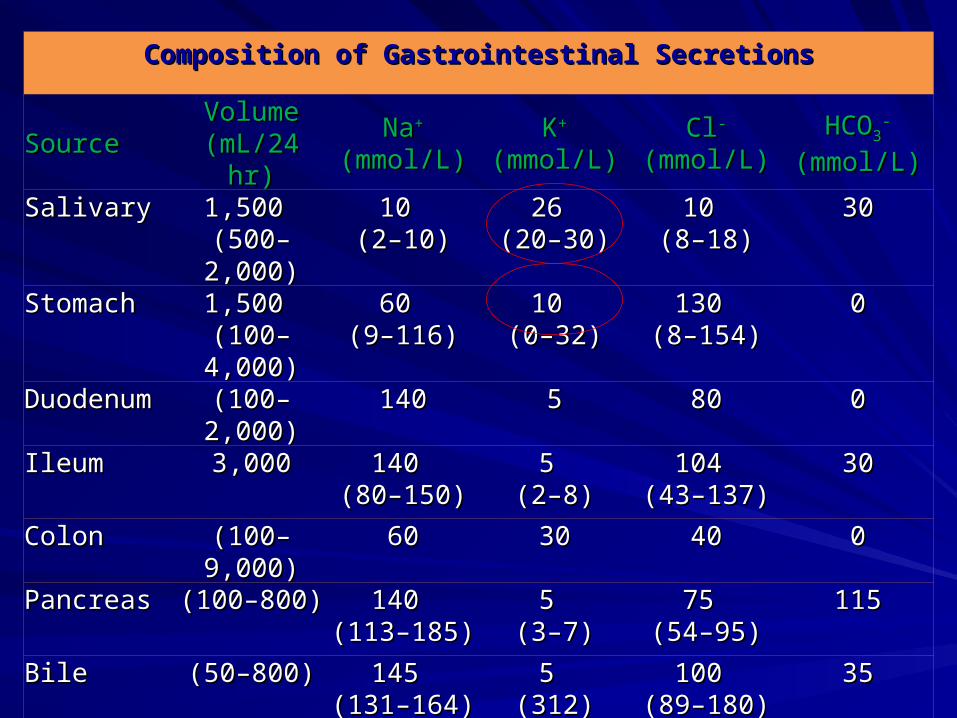
Composition of Gastrointestinal SecretionsComposition of Gastrointestinal Secretions
SourceSource Volume Volume (mL/24 hr)(mL/24 hr)
NaNa++ (mmol/L)(mmol/L) KK++ (mmol/L) (mmol/L) ClCl-- (mmol/L) (mmol/L)
HCOHCO33--
(mmol/L)(mmol/L)
SalivarySalivary 1,500 1,500 (500–2,000)(500–2,000)
10 10 (2–10)(2–10)
26 26 (20–30)(20–30)
10 10 (8–18)(8–18)
3030
StomachStomach 1,500 1,500 (100–4,000)(100–4,000)
60 60 (9–116)(9–116)
10 10 (0–32)(0–32)
130 130 (8–154)(8–154)
00
DuodenumDuodenum (100–2,000)(100–2,000) 140140 55 8080 00
IleumIleum 3,0003,000 140 140 (80–150)(80–150)
5 5 (2–8)(2–8)
104 104 (43–137)(43–137)
3030
ColonColon (100–9,000)(100–9,000) 6060 3030 4040 00
PancreasPancreas (100–800)(100–800) 140 140 (113–185)(113–185)
5 5 (3–7)(3–7)
75 75 (54–95)(54–95)
115115
BileBile (50–800)(50–800) 145 145 (131–164)(131–164)
5 5 (312)(312)
100 100 (89–180)(89–180)
3535
SodiumSodium
Serum conc. – 135 to 145 mmol/LSerum conc. – 135 to 145 mmol/L
Potential sources of significant NaPotential sources of significant Na++ loss – sweat, urine, loss – sweat, urine, and GI secretionsand GI secretions
PPosmosm – 290 to 310 mOsm/L – 290 to 310 mOsm/L
• Hyponatremia – [Na+] <135 mEq/L• Hypernatremia – [Na+] >145 mEq/L

HyponatremiaHyponatremia

C/F :C/F :
– Predominantly Neurologic Predominantly Neurologic – Lethargy, confusion, nausea, vomiting, seizures, and Lethargy, confusion, nausea, vomiting, seizures, and
comacoma– Chronic hyponatremia often asymptomatic until serum Chronic hyponatremia often asymptomatic until serum
NaNa++ concentration < 110 to 120 mEq/L concentration < 110 to 120 mEq/LRx :Rx :
– Correct the underlying disorderCorrect the underlying disorder– Fluid Restriction (1,000 mL/day)Fluid Restriction (1,000 mL/day)– Hypovolemic hyponatremia – administer 0.9% NaCl to Hypovolemic hyponatremia – administer 0.9% NaCl to
correct volume deficits and replace ongoing losses.correct volume deficits and replace ongoing losses.Rapid correction should be avoidedRapid correction should be avoided

HypernatremiaHypernatremia

C/F :C/F :– Primarily NeurologicPrimarily Neurologic– Lethargy, weakness, & irritabilityLethargy, weakness, & irritability– Fasciculations, seizures, coma, & irreversible Fasciculations, seizures, coma, & irreversible
neurologic damageneurologic damage
Rx :Rx :– Water deficit (L) = 0.60 × total body weight (kg) × Water deficit (L) = 0.60 × total body weight (kg) ×
[(serum Na[(serum Na++ in mmol/L/140) – 1] in mmol/L/140) – 1]– Gradual correction Gradual correction – Treat specific causeTreat specific cause

PotassiumPotassium
Serum conc. – 3.5 to 5 mmol/LSerum conc. – 3.5 to 5 mmol/L
90 % of K90 % of K++ excreted renally, remainder in stools excreted renally, remainder in stools
HypokalemiaHypokalemia – – [K[K++] <3.5 mEq/L] <3.5 mEq/L
Hyperkalemia – [KHyperkalemia – [K++] >5.0 mEq/L] >5.0 mEq/L

Causes :Causes :– Inadequate intake Inadequate intake
– GI losses (e.g., diarrhea, persistent vomiting, GI losses (e.g., diarrhea, persistent vomiting, Nasogastric suctioning)Nasogastric suctioning)
– Renal losses (e.g., diuretics, fluid mobilization)Renal losses (e.g., diuretics, fluid mobilization)– Cutaneous losses (e.g., burns)Cutaneous losses (e.g., burns)
– Acute intracellular KAcute intracellular K++ uptake (insulin excess, metabolic uptake (insulin excess, metabolic alkalosis, hypothermia, theophylline toxicity)alkalosis, hypothermia, theophylline toxicity)
– Refeeding Syndrome – in malnourished patient after Refeeding Syndrome – in malnourished patient after initiation of TPNinitiation of TPN
HypokalemiaHypokalemia
C/F :C/F :– Mild hypokalemia [KMild hypokalemia [K++ >3 mmol/L] generally >3 mmol/L] generally
asymptomaticasymptomatic– Severe KSevere K++ deficiency [K deficiency [K++ <3 mmol/L] – primarily <3 mmol/L] – primarily
cardiovascular cardiovascular (ECG manifestations – ectopy, T-wave (ECG manifestations – ectopy, T-wave depression, and prominent U waves)depression, and prominent U waves)
– Fatigue, myalgias, and muscular weakness or cramps Fatigue, myalgias, and muscular weakness or cramps of the lower extremitiesof the lower extremities
– Constipation ,paralytic ileusConstipation ,paralytic ileus– Complete paralysis, hypoventilation, or Complete paralysis, hypoventilation, or
rhabdomyolysisrhabdomyolysisRx :Rx :– Oral replacement (40 to 100 mmol)Oral replacement (40 to 100 mmol)– Parenteral therapy (not exceeding 40 mmol/L & not Parenteral therapy (not exceeding 40 mmol/L & not
exceeding 20 mmol/hour)exceeding 20 mmol/hour)

HyperkalemiaHyperkalemia
Causes :Causes :– PseudohyperkalemiaPseudohyperkalemia– Abnormal redistribution of KAbnormal redistribution of K++
Insulin deficiencyInsulin deficiency
β-β-adrenergic receptor blockadeadrenergic receptor blockade
Acute acidosisAcute acidosis
RhabdomyolysisRhabdomyolysis
Cell lysis (after chemotherapy)Cell lysis (after chemotherapy)
Digitalis intoxicationDigitalis intoxication
Reperfusion of ischemic limbsReperfusion of ischemic limbs
Succinylcholine Succinylcholine

C/F :C/F :– Mild Hyperkalemia [KMild Hyperkalemia [K++ = 5 to 6 mmol/L] generally = 5 to 6 mmol/L] generally
asymptomaticasymptomatic– Severe Hyperkalemia [KSevere Hyperkalemia [K++ >6.5 mmol/L] – arrhythmia >6.5 mmol/L] – arrhythmia
(ECG abnormalities : symmetric peaking of T waves, (ECG abnormalities : symmetric peaking of T waves, reduced P-wave voltage, and widening of the QRS reduced P-wave voltage, and widening of the QRS complex, ultimately sinusoidal ECG pattern)complex, ultimately sinusoidal ECG pattern)
– Weakness, flaccid paralysis & hypoventilationWeakness, flaccid paralysis & hypoventilation
Rx :Rx :– Mild Hyperkalemia :Mild Hyperkalemia :
Reduction of daily KReduction of daily K++ intake intake
Loop diureticLoop diuretic
Withdrawal of drugs impairing KWithdrawal of drugs impairing K++ homeostasis homeostasis
-Severe Hyperkalemia-Severe HyperkalemiaTemporizing MeasuresTemporizing Measures
– Calcium gluconateCalcium gluconate– Insulin with dextroseInsulin with dextrose
– Inhaled βInhaled β22-agonists-agonists
– NaHCONaHCO33
Therapeutic MeasuresTherapeutic Measures– Sodium polystyrene sulfonate (Kayexalate), a Sodium polystyrene sulfonate (Kayexalate), a
NaNa++-K-K++ exchange resin exchange resin– Hydration in combination with a loop diuretic Hydration in combination with a loop diuretic – DialysisDialysis

CalciumCalcium
Serum Calcium – 2.23 to 2.57 mmol/L (8.9 to 10.3 Serum Calcium – 2.23 to 2.57 mmol/L (8.9 to 10.3 mg/dL), exists in three formsmg/dL), exists in three forms– Ionized (45%)Ionized (45%)– Protein bound (40%)Protein bound (40%)– Complexed to freely diffusible compounds (15%)Complexed to freely diffusible compounds (15%)
Free ionized CaFree ionized Ca2+2+ (4.6 to 5.1 mg/dL) is physiologically (4.6 to 5.1 mg/dL) is physiologically activeactive
Calcium Homeostasis – PTH, Vit. D & CalcitoninCalcium Homeostasis – PTH, Vit. D & Calcitonin

HypocalcemiaHypocalcemia
Serum Calcium <8.4 mg/dL with a normal serum albumin Serum Calcium <8.4 mg/dL with a normal serum albumin or an ionized calcium <4.2 mg/dLor an ionized calcium <4.2 mg/dL
Causes :Causes :– Calcium sequestration (acute pancreatitis, Calcium sequestration (acute pancreatitis,
rhabdomyolysis, or rapid administration of blood)rhabdomyolysis, or rapid administration of blood)– Vitamin D deficiencyVitamin D deficiency– Total thyroidectomy Total thyroidectomy – Parathyroidectomy Parathyroidectomy – Acute alkalemiaAcute alkalemia

C/F :C/F :– Perioral Numbness and TinglingPerioral Numbness and Tingling– TetanyTetanyECG - QT-interval prolongation and ventricular ECG - QT-interval prolongation and ventricular
arrhythmiasarrhythmias
Rx :Rx :– Parenteral therapy (overt tetany, laryngeal spasm, or Parenteral therapy (overt tetany, laryngeal spasm, or
seizures)seizures)– Oral therapy (Ca & vit. D)Oral therapy (Ca & vit. D)

HypercalcemiaHypercalcemia
Serum Calcium >10.3 mg/dl with a normal serum albumin Serum Calcium >10.3 mg/dl with a normal serum albumin or an ionized calcium >5.2 mg/dl or an ionized calcium >5.2 mg/dl
Causes :Causes :– MalignancyMalignancy– HyperparathyroidismHyperparathyroidism– HyperthyroidismHyperthyroidism– Vitamin D intoxicationVitamin D intoxication– ImmobilizationImmobilization– Long-term total parenteral nutritionLong-term total parenteral nutrition– Thiazide diureticsThiazide diuretics– Granulomatous diseaseGranulomatous disease

C/F :C/F :– Mild Hypercalcemia (Calcium <12 mg/dl) is generally Mild Hypercalcemia (Calcium <12 mg/dl) is generally
asymptomaticasymptomatic– Altered mental status, diffuse weakness, dehydration, Altered mental status, diffuse weakness, dehydration,
adynamic ileus, nausea, vomiting, and severe adynamic ileus, nausea, vomiting, and severe constipationconstipation
– Hypercalcemia of hyperparathyroidism –associated Hypercalcemia of hyperparathyroidism –associated infrequently with classic parathyroid bone disease and infrequently with classic parathyroid bone disease and nephrolithiasis.nephrolithiasis.
ECG - QT-interval shortening and arrhythmiasECG - QT-interval shortening and arrhythmias
Rx :Rx :– NaCl 0.9% and loop diuretics mayNaCl 0.9% and loop diuretics may– Salmon calcitoninSalmon calcitonin– Pamidronate disodiumPamidronate disodium

Thank youThank you
Cooperation Cooperation is the Key is the Key to Success!!!to Success!!!