trauma muskuloskeletal - info medical ya-ha · mechanism of injury •penetrating trauma –gsw...
TRANSCRIPT

Trauma muskuloskeletal
Arterial injuries associated with fractures or dislocations
Clavicle fracture subclavian artery
Shoulder fxdislocation axillary artery
Supracondylar humerus fx brachial artery
Elbow dislocation brachial artery
Pelvic fracture gluteal arteries
Femoral shaft fx femoral artery
Distal femur fracture popliteal artery
Knee dislocation popliteal artery
Tibial shaft fx tibial arteries
Incidence
Overall uncommon
bull 3 of long bone fractures
Specific circumstances
bull Fractures with GSW (up to 38)
bull Knee dislocations (16-40)
Mechanism of Injury
bull Penetrating trauma
ndash GSW
ndash Stab
bull Blunt trauma
ndash High energy
ndash Low energy
bull iatrogenic
Consequences of vascular injury
bull Blood loss
bull Ischemia
bull Compartment syndrome
bull Tissue necrosis
bull Amputation
bull Death
Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Arterial injuries associated with fractures or dislocations
Clavicle fracture subclavian artery
Shoulder fxdislocation axillary artery
Supracondylar humerus fx brachial artery
Elbow dislocation brachial artery
Pelvic fracture gluteal arteries
Femoral shaft fx femoral artery
Distal femur fracture popliteal artery
Knee dislocation popliteal artery
Tibial shaft fx tibial arteries
Incidence
Overall uncommon
bull 3 of long bone fractures
Specific circumstances
bull Fractures with GSW (up to 38)
bull Knee dislocations (16-40)
Mechanism of Injury
bull Penetrating trauma
ndash GSW
ndash Stab
bull Blunt trauma
ndash High energy
ndash Low energy
bull iatrogenic
Consequences of vascular injury
bull Blood loss
bull Ischemia
bull Compartment syndrome
bull Tissue necrosis
bull Amputation
bull Death
Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Incidence
Overall uncommon
bull 3 of long bone fractures
Specific circumstances
bull Fractures with GSW (up to 38)
bull Knee dislocations (16-40)
Mechanism of Injury
bull Penetrating trauma
ndash GSW
ndash Stab
bull Blunt trauma
ndash High energy
ndash Low energy
bull iatrogenic
Consequences of vascular injury
bull Blood loss
bull Ischemia
bull Compartment syndrome
bull Tissue necrosis
bull Amputation
bull Death
Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Mechanism of Injury
bull Penetrating trauma
ndash GSW
ndash Stab
bull Blunt trauma
ndash High energy
ndash Low energy
bull iatrogenic
Consequences of vascular injury
bull Blood loss
bull Ischemia
bull Compartment syndrome
bull Tissue necrosis
bull Amputation
bull Death
Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Consequences of vascular injury
bull Blood loss
bull Ischemia
bull Compartment syndrome
bull Tissue necrosis
bull Amputation
bull Death
Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Prognostic factors
bull Level and type of vascular injury
bull Collateral circulation
bull Shockhypotension
bull Tissue damage (crush injury)
bull Warm ischemia time
bull Patient factorsmedical
conditions
Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Speed is crucial
bull Rapid resuscitation
bull Complete rapid
evaluation
bull Urgent surgical
treatment
PROTOCOL IS ESSENTIAL
Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Immediate treatment
bull Control bleeding
bull Replace volume loss
bull Cover wounds
bull Reduce
fracturesdislocations
bull Splint
bull Re-evaluate
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration
Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Diagnosis
bull Physical exam
bull Doppler pressure (Anklebrachial
systolic pressure index)
bull Duplex scanning
bull Arteriogram
bull Exploration Careful physical exam and
high index of suspicion are
most important
Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Physical exam
bull Major hemorrhagehypotension
bull Arterial bleeding
bull Expanding hematoma
bull Altered distal pulses
bull Pallor
bull Temperature differential between extremities
bull Injury to anatomically-related nerve
bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull Asymmetric pulses warrant doppler examination (determine ABI)
bull Absent pulses warrant emergent vascular consultationsurgical exploration
Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Doppler ultrasound
bull Determine presenceabsence of arterial
supply
bull Assess adequacy of flow
PRESENCE OF SIGNAL DOES NOT
EXCLUDE ARTERIAL INJURY
Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Angiography
bull Locates site of injury
bull Characterizes injury
bull Defines status of vessels
proximal and distal
bull May afford therapeutic
intervention
Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Angiography
Identify and control bleeding from pelvic fractures
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
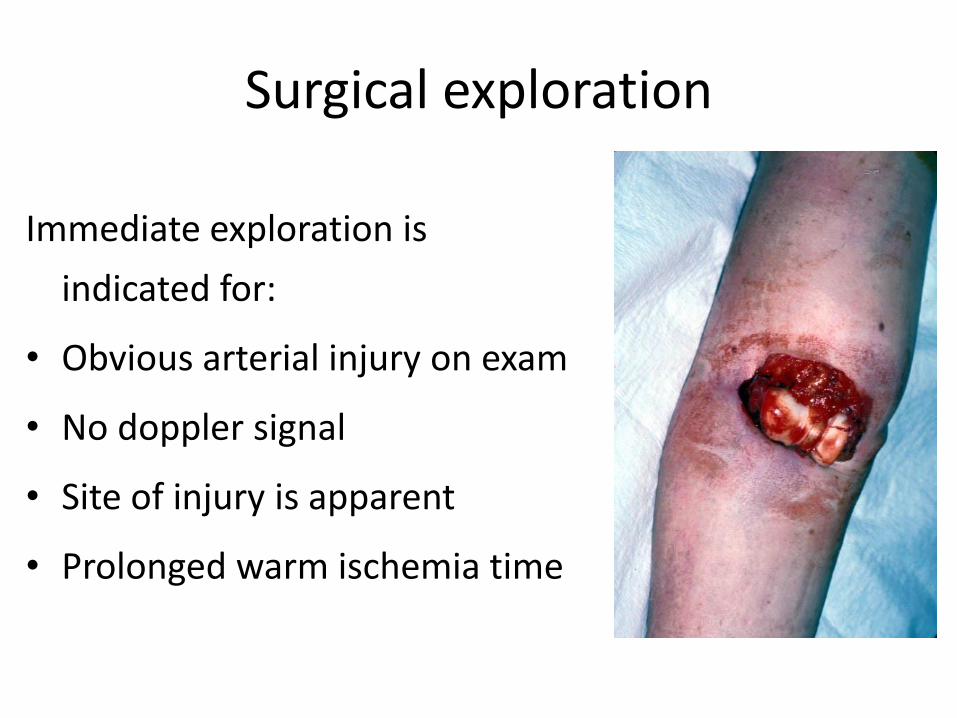
Surgical exploration
Immediate exploration is
indicated for
bull Obvious arterial injury on exam
bull No doppler signal
bull Site of injury is apparent
bull Prolonged warm ischemia time
Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Crush syndrome
Crush Syndrome is a reperfusion injury as a result of traumatic rhabdomyolysis
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Spitak earthquake in Armenia in 1988
Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Great Hanshin earthquake in Japan in 1995
Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Marmara earthquake in Turkey in 1999
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
bull First described in the English language literature by Bywaters and Beal (1941)
bull Several patients who had been trapped under rubble of buildings bombed subsequently died of acute renal failure
bull A severe often fatal condition that follows a severe crushing injury particularly involving large muscle masses
bull Characterized by fluid and blood loss shock hematuria and renal failure
Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Crush Syndrome
1048708Building collapse
1048708Earthquakes
1048708Landslides
1048708Bombings
1048708Construction accidents
1048708Heavy snow on roof
1048708Mine or trench collapse
Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Signs and Symptoms of Crush Injury
bull Skin injury bull Swelling bull Paralysis ndash may cause to be mistaken as a spinal cord
injury bull Paresthesias numbness ndash may mask the degree of
damage bull Pain bull Pulses ndash distal pulses may or may not be present bull Myoglobinuria ndash the urine may become dark red or
brown indicating the presence of myoglobin
Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Compartment Syndrome
bull Severe pain in the involved extremity
bull Pain on passive stretching of the muscles involved
bull Decreased sensation in branches of the involved peripheral nerves
bull Elevated intracompartmental pressures on direct manometry
Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Treatment
bull The airway must be secured and protected from dust impaction
bull Adequate ventilation must be ensured and maintained along with adequate oxygenation
bull Intravenous Fluid
preexisting dehydration or fluid loss should be corrected
bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull Intravenous (IV) fluids containing potassium (eg lactated Ringers solution) should be avoided
bull Normal saline is a good initial choice
bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull formula that can be used to maintain an alkaline urine output of 8 Ld is the infusion of 12 Ld of Normal Saline Solution (NSS) with 50 mEq of sodium bicarbonate per liter of fluid plus 120 grams of mannitol daily to maintain this urine output
Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Sodium Bicarbonate
bull reverse the preexisting acidosis
bull first steps in treating hyperkalemia
bull increase the urine pH to decrease the amount of myoglobin precipitated in the kidneys
bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull 50 to 100 mEq of bicarbonate depending on severity of injury to be given prior to release from compression
Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Treatment of Hyperkalemia
bull Insulin and glucose
bull Calcium ndash intravenously for life-threatening dysrhythmias
bull Beta-2 agonists ndash albuterol metaproterenol sulfate (Alupent) etc
bull Potassium-binding resins such as sodium polystyrene sulfonate (Kayexalate)
bull Dialysis especially in patients with acute renal failure
Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Alkaline Diuresis
bull maintain a urine output of at least 300 mlh with a pH higher than 65
bull intravenous fluids mannitol and sodium bicarbonate (44 to 50 mEqliter)
Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Intravenous Mannitol
bull protects the kidneys from the effects of rhabdomyolysis
bull increases extracellular fluid volume
bull increases cardiac contractility
bull relief symptoms and reduction of swelling of compartment syndrome
bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull Mannitol can be given in doses of 1 gmkg or added to the patients intravenous fluid as a continuous infusion
bull The maximum dose is 200 gmd
bull Mannitol should be given only after good urine flow has been established
bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull Wounds should be cleaned deacutebrided and covered with sterile dressings
bull Splinting and elevation of the limb will help to limit edema and maintain perfusion
bull Intravenous antibiotics
bull Medications for pain control can be given as appropriate
bull Tourniquets are controversial and usually not necessary
bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

bull Amputation should be used only as a last resort
bull Fasciotomy
CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

CONCLUSIONS
bull The development of Crush injury syndrome is preventable and treatable
bull The mainstay of treatment is the prevention of renal failure by adequate rehydration and alkalinization of urine
bull The traditional treatment of compartment syndrome is fasciotomy
bull The complication rate is high with the most serious hemorrhage and sepsis
Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Amputations
bull Amputations are classified at the level where the amputation takes place
Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Types and levels
bull congenital
bull Acquired
bull lower extremity
bull upper extremity
bull Forequarter
bull Intrascapulothorasic
bull shoulder disarticulation
bull Transhumeral ndash above elbow
ndash Elbow Disarticulation
bull Transradial
ndash below elbow
bull wrist disarticulation
bull Transcarpal
bull Metacarpal phalangeal
bull Transphalangeal
bull partial hand
Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Types of Amputations (according to soft tissues cutting)
1 Flap amputations
- single-flap amputation
- double-flap amputation
2 Circular amputations
- one-step (guillotine) amputation
- two-step amputation (variety ndash ldquocuffrdquo
method of forearm amputation)
- three-step (conical-circular)
amputation
Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Sites of Election for Amputations of Upper
Extremity
Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Finger Amputation
Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Osteo-plastic Amputations
(Gritti-Stokes and Sabanajeff amputations)
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
Pirogoff Amputation
Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Callander Amputation (this gives an excellent end-bearing stump)
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
Below-knee Amputation
Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Amputation in Middle Third of Leg
Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Schemes of Foot Amputations
Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Syme Amputation
Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Phantom limb sensationpain
bull The sensation that the amputated extremity is still there
bull Pain treated with TENS desensitization fluidotherapy US nerve blocks or surgery
Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Other complications SP amputation
bull Depression is common
bull Falls
ndash stand on side of LE amputation
bull balance is greatly disturbed
ndash body center of gravity is changed
ndash balance must be relearned
ndash protective reactions must be changed
Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Stump Management
bull Shape residual limb so it is tapered at the distal end to allow for prosthetic fit
bull Figure 8 ace bandage wrap ndash wrapped distal to proximal
ndash more pressure distally
ndash never wrap circular direction because of tourniquet effect
ndash pt wears wrap continually
ndash check skin 3-4 times each day
Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Common Traumatic Injuries of the Hand
Bone and Soft Tissue
ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

ndash Extensor and flexor tendons insert into the base of the distal phalanx
ndash Routinely not a deforming fracture
Applied Anatomy
Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Nailbed Injury
bull Nailbed lacerations need to be repaired
ndash Use 6-0 absorbable to repair matrix
ndash Prevents nail growth problems
bull Reinsert nail and secure
Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Subungual Hematoma
bull Results from blunt trauma to nail
bull Very painful
bull Relieved by
ndash Cautery
ndash Heated paperclip
ndash 18g needle
Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Subungual Hematoma
bull Clean with alcohol
bull Instrument of choice
bull Pierce nail
bull Gauze for 24 hours
Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Mallet Fingers (soft tissue and bony)
bull Applied Anatomy ndash Terminal extensor tendon
inserts into the dorsum of the distal phalanx
bull Mechanism of injury ndash Occurs with a sudden
flexion force against an extended digit
ndash Results in flexion deformity of the DIP joint
Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Mallet Fingers (soft tissue and bony)
bull History and Physical Exam ndash Pain and deformity of
the DIP joint after bumping the end of the finger
ndash Inability to straighten the end joint
ndash Test for tendon function
Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Mallet Fingers (soft tissue and bony)
bull Radiographs ndash 2 views looking for dorsal
avulsion fragment
ndash May be negative
bull Classification ndash Soft tissue (- x-ray)
ndash Bony (+ x-ray) bull Fleck
bull Dorsal articular piece
bull Subluxation of DIP joint
Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Mallet Fingers (soft tissue and bony)
bull Treatment ndash Closed reduction
ndash Continuously splint DIP in full extension for 6 to 10 weeks
bull Only immobilize the DIP
ndash Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Flexor Tendon Avulsion
bull Applied Anatomy
ndash Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Flexor Tendon Avulsion
bull Mechanism of Injury ndash Hyperextension
against a flexed DIP joint
ndash Relatively uncommon but devastating is missed
ndash Ring finger most commonly involved
Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Flexor Tendon Avulsion
bull Associated injuries ndash None
bull History and Physical Exam ndash Pain on volar surface of digit
bull May extend into palm with eccymosis
ndash Cannot flex tip
ndash Resting hand has extension of DIP joint
ndash No active flexion
Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Flexor Tendon Avulsion
bull Radiographs
ndash DIP to look for avulsion but also hand to look for retracted segment
ndash Most are normal
bull Classification
ndash Pure tendon avulsion
ndash Bony avulsion
Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Flexor Tendon Avulsion
bull Treatment
ndash Should be splinted and referred in a semi-urgent fashion
ndash Surgery is required
bull Outcomes
ndash Results correlate with delay in treatment
bull Early do well
bull Postoperative hand therapy is important
Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Boutonniere
bull Applied Anatomy
ndash When the central slip insertion at the base of the middle phalanx is disrupted active PIP joint extension may be limited
Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Boutonniere
bull Applied Anatomy ndash The flexed position of the
PIP joint then allows the lateral bands to fall volar to the axis
ndash These lateral bands then act to flex the PIP joint further
ndash Tension pulls the DIP joint into extension
Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Boutonniere
bull Mechanism of Injury ndash Acute flexion force to PIP
joint
ndash PIP does not immediately fall into a flexed position
ndash Several weeks after the injury the digit assumes a buttonhole posture
ndash Other mechanism include PIP dislocation and central slip lacerations
bull History and Physical Exam ndash Pain and swelling about PIP
ndash Inability to fully extend PIP
ndash DIP flexion is limited
ndash Longstanding cases
bull PIP flexion
bull Passive extension not possible
Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Boutonniere
bull Radiographs ndash Most often negative
ndash Occasionally small fragments dorsally off middle phalanx
bull Classifications ndash Acute
ndash Chronic bull Stiff
bull supple
Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Boutonniere
bull Treatment
ndash If not sure of central slip assume it is and splint the PIP in full extension
ndash Acute boutonnieres bull 4 weeks of full extension splinting of PIP with active DIP flexion
exercises
bull Occasionally need surgery
ndash Chronic boutonnieres bull Hand therapy
bull Possible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash PIP is a hinge
ndash Ligaments along palmar aspect - volar plate
bull Prevents hyperextension
ndash Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Applied Anatomy
ndash Each PIP joint has a radial and ulnar collateral ligament
bull Tethers the PIP joint in its side-to-side motion
ndash Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Mechanism of Injury
ndash Sudden force directed to tip of digit results in hyperextension
bull Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
bull Associated Injury ndash If the skin tears open it is an
open dislocation
bull History and Physical Exam ndash Joint swollen and tender
ndash Test collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Radiographs ndash 2 views to check for
fractures
ndash Post-reduction films if done
bull Classifications ndash I ndash do not compromise
stability
ndash II ndash partial compromise at risk for complete disruption
ndash III- complete disruption can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
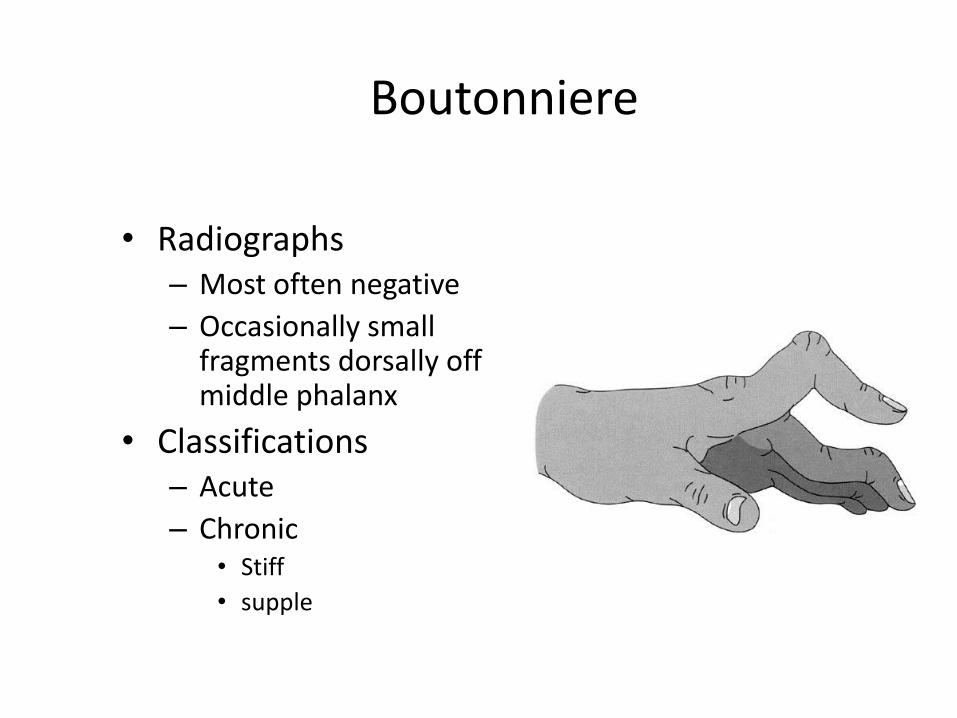
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
bull Treatment ndash Early mobilization after a few days of splinting
bull Buddy tape for 4 weeks
ndash A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
bull Outcomes ndash These injuries can heal with some permanent fusiform
swelling from scar tissue
ndash Long term problem is not recurrent instability but stiffness bull For this reason early range of motion program is most often
recommended
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull The ulnar collateral ligament of the thumb is important for pinch strength and stability
bull Because of its location it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Mechanism of Injury
ndash Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over ulnar side of MP joint
ndash In complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeperrsquos Thumb)
bull Radiographs ndash Typically negative
ndash Possible avulsion fragment off proximal phalanx or metacarpal
bull Treatment ndash Incomplete ndash non-
operatively (splint)
ndash Complete - surgically
Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Bennetts Fracture Dislocation
bull Most frequent of all thumb fracture
bull Described in 1882 by Dr Edward Bennet
bull It is a fracture dislocation intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Bennetts Fracture Dislocation
bull Mechanism of Injury
ndash Results from axial blow directed against the partially flexed metacarpal (ie from fist fights)
bull History and Physical Exam
ndash Moderate swelling and eccymosis over the CMC joint
ndash Pain with ROM or palpation
Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning

Bennetts Fracture Dislocation
bull Radiographs ndash Oblique fracture line with a
triangluar fragment at ulnar base of metacarpal
ndash Triangular fragment remains attached to trapezium w proximal displacement of the metacarpal
bull Treatment ndash Immobilization
ndash Referral for surgical pinning