thoracic outlet syndrome caused by malunion of a midshaft clavicle fracture
TRANSCRIPT

Injury Extra 40 (2009) 159–161
Case report
Thoracic outlet syndrome caused by malunion of a midshaft clavicle fracture
Chen Yunfeng, Ao Rongguang, Zeng Bingfang*
Department of Orthopaedic Surgery, Shanghai Sixth People’s Hospital, Jiaotong University, 600 Yishan Rd, Shanghai 200233, PR China
Contents lists available at ScienceDirect
Injury Extra
journal homepage: www.elsev ier .com/ locate / inext
A R T I C L E I N F O
Article history:
Accepted 30 April 2009
1. Introduction
Thoracic outlet syndrome (TOS) refers to a collection of clinicalsyndromes caused by various anatomic anomalies of the anteriorand medial scalenus and the first rib, resulting in compression ofthe brachial plexus or subclavian arteries and veins. Clinicalmanifestations vary and, currently, there is no laboratoryexamination available to make a definitive diagnosis.
Malunion of a midshaft clavicle fracture can cause narrowing ofthe thoracic outlet, with resultant compression of the brachialplexus and/or subclavian nerves and vessels; however, TOS causedby malunion of a clavicular fracture is rarely reported in theliterature.6,11 This paper describes the diagnosis and treatment of acase of TOS caused by the malunion of a fracture of the middle thirdof the clavicle.
2. Case report
A 57-year-old woman was hospitalised 5 months afterreceiving conservative treatment for a fracture of the left clavicle.The original injury had occurred after the patient had accidentallyfallen off her bicycle, directly hitting her left shoulder on theground. The fall left her with left shoulder pain and limited range ofmotion. At the local hospital, an X-ray showed a fracture of themiddle third of the left clavicle. A figure-eight bandage fixation wasapplied at the emergency room (Fig. 1).
The patient then revisited the outpatient department of ourhospital 5 months after the injury, with a complaint of pain in theleft shoulder and left forearm, and sleep disruption due to pain.Pain was intensified with movement, and the range of motion ofthe left shoulder was limited. Physical examination showedshoulder asymmetry with a non-tender prominence at the siteof the left clavicle fracture; left upper limb anteflexion angle <808and abduction angle <508. The Constant score was 55 and theDASH score was 31.5. The X-ray showed malunion of the left
* Corresponding author. Tel.: +86 21 64856083; fax: +86 21 64856083.
E-mail address: [email protected] (B. Zeng).
1572-3461/$ – see front matter � 2009 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2009.04.012
clavicle. Bilateral tangential radiographs of the clavicle wereperformed to assess the width of the costoclavicular space. Thebilateral tangential radiographs showed narrowing of the leftcostoclavicular space (Fig. 2).
EMG was performed and showed damage to the left brachialplexus.
Three-dimensional CT reconstruction of the left shoulder andangiography were performed to assess the malunion of the fractureand to learn whether the subclavian vessels were compressed ordamaged. However, no obvious vascular compression or damagewas seen.
These studies, in light of the clinical history, established thediagnosis of malunion of a midshaft clavicular fracture andresultant thoracic outlet syndrome.
2.1. Treatment
Left clavicle osteotomy and plate fixation were performed asfollows: the patient received brachial plexus block and cervicalplexus block anaesthesia, and was placed in the beach-chairposition. A long, curved incision was made at the upper edge ofthe original fracture and the skin flap was pulled open.Precautions were taken to protect the branches of the supracla-vicular nerves, and the healing site of the original fracture wasexposed. Malunion of the original fracture and an osteophytewere observed (Fig. 3). A bone chisel was used to separatethe bone along the original fracture line, and the bone marrowcavity was exposed. The external bone callus was removedcompletely and the fracture was reduced. An 8-hole reconstruc-tion plate was selected, and was placed at the antero-superiorportion of the clavicle fracture line. Screws of appropriate lengthswere selected for the fixation. Once a satisfactory position wasdemonstrated by C-arm fluoroscopy, the field was rinsed, theincision sutured, and negative pressure drainage was positionedaccordingly.
2.2. Postoperative treatment
The affected limb was suspended with a forearm sling, and a2-week program of passive range of motion functional trainingwithout shoulder joint load was initiated immediately. Func-tional shoulder training was carried out at the rehabilitationdepartment for 4 weeks after surgery. The range of shoulderabduction was increased gradually from the initial session oftherapy.
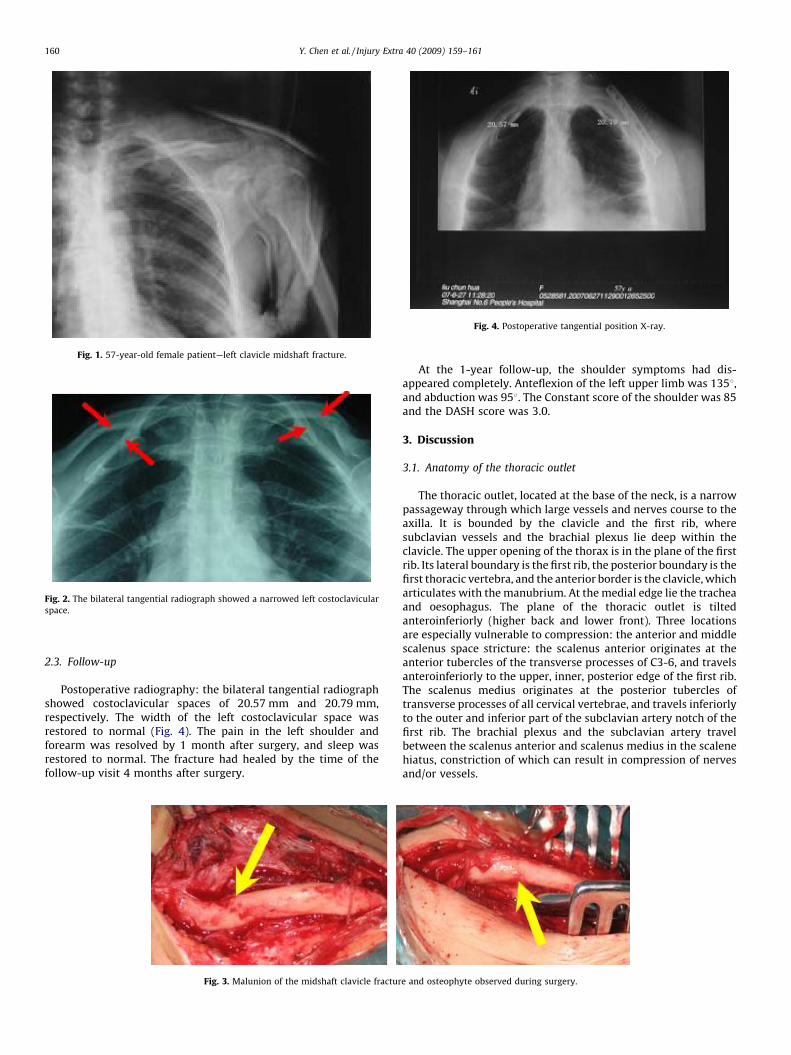
Fig. 1. 57-year-old female patient—left clavicle midshaft fracture.
Fig. 2. The bilateral tangential radiograph showed a narrowed left costoclavicular
space.
Fig. 4. Postoperative tangential position X-ray.
Y. Chen et al. / Injury Extra 40 (2009) 159–161160
2.3. Follow-up
Postoperative radiography: the bilateral tangential radiographshowed costoclavicular spaces of 20.57 mm and 20.79 mm,respectively. The width of the left costoclavicular space wasrestored to normal (Fig. 4). The pain in the left shoulder andforearm was resolved by 1 month after surgery, and sleep wasrestored to normal. The fracture had healed by the time of thefollow-up visit 4 months after surgery.
Fig. 3. Malunion of the midshaft clavicle fractur
At the 1-year follow-up, the shoulder symptoms had dis-appeared completely. Anteflexion of the left upper limb was 1358,and abduction was 958. The Constant score of the shoulder was 85and the DASH score was 3.0.
3. Discussion
3.1. Anatomy of the thoracic outlet
The thoracic outlet, located at the base of the neck, is a narrowpassageway through which large vessels and nerves course to theaxilla. It is bounded by the clavicle and the first rib, wheresubclavian vessels and the brachial plexus lie deep within theclavicle. The upper opening of the thorax is in the plane of the firstrib. Its lateral boundary is the first rib, the posterior boundary is thefirst thoracic vertebra, and the anterior border is the clavicle, whicharticulates with the manubrium. At the medial edge lie the tracheaand oesophagus. The plane of the thoracic outlet is tiltedanteroinferiorly (higher back and lower front). Three locationsare especially vulnerable to compression: the anterior and middlescalenus space stricture: the scalenus anterior originates at theanterior tubercles of the transverse processes of C3-6, and travelsanteroinferiorly to the upper, inner, posterior edge of the first rib.The scalenus medius originates at the posterior tubercles oftransverse processes of all cervical vertebrae, and travels inferiorlyto the outer and inferior part of the subclavian artery notch of thefirst rib. The brachial plexus and the subclavian artery travelbetween the scalenus anterior and scalenus medius in the scalenehiatus, constriction of which can result in compression of nervesand/or vessels.
e and osteophyte observed during surgery.

Y. Chen et al. / Injury Extra 40 (2009) 159–161 161
The insertion of the pectoralis minor muscle on the coracoidprocess: when the arm is abducted, the vessels and nerves may beentrapped by the coracoid process and be forced upwards. At thesame time, the pectoralis minor muscle contracts, squeezing thenerves and blood vessels under the tendons, thus causingsymptoms of TOS.
3.2. Diagnosis of TOS
The clinical manifestations of TOS: at present, the diagnosisrelies mainly on the clinical symptoms7; however, provocativemaneuvers for eliciting symptoms constitute the most usefulmethod for early diagnosis. The skin pain threshold test and thetwo-point discrimination test are used for the diagnosis of patientsin intermediate and advanced stages.8 Adson’s maneuver andHalsted’s maneuver diagnose TOS by the effects of the maneuvers(involving arm and neck position) on the radial pulse, but thereliability of these tests is limited by high rates of false positive andfalse negative results. Provocation of symptoms often employs theRoos test, in which the arm is abducted 908 in external rotationwith the elbow flexed 908. This position is maintained for 3 min,with repetitive opening and closing of the hand. Thompson andJannsen12 reported that this test was positive in 92 percent ofpatients with TOS subsequently confirmed by surgery, but only 62percent of patients with TOS had diminution of the radial pulse.
Currently, there is no effective laboratory diagnostic test forTOS. Somatosensory evoked potential is a sensitive method, andthe sensitivity can be improved through the determination of thesomatosensory evoked potential in specific positions. Imaging (CTand X-ray) can help identify anatomical abnormalities such as anexcessively long C7 transverse process. Some researchers havefound that 85% of TOS patients have anatomic abnormalitiesdetectable with these imaging techniques. The diagnosis of thiscase was established on the basis of clinical symptoms anddiagnostic studies. The clinical symptoms of the patient werehighly suggestive, with pain in the left shoulder and left forearm,and sleep disturbance. Pain was intensified with movement of theupper limb. The tangential radiograph of the clavicle demonstratedthat the left costoclavicular space was narrowed; therefore,compression of the subclavian vessels and nerves was suspected.Three-dimensional CT reconstruction of the left shoulder did notshow any obvious vascular compression, so the possibility of thesubclavian vascular compression was excluded. However, EMGsuggested left brachial plexus injury, thus establishing thediagnosis of brachial plexus compression.
3.3. Clavicular fracture and TOS
The mechanisms of TOS caused by the common condition ofclavicle fracture include: early compression by subclavianhematoma; hyperplastic bone callus; and scapular instabilitycaused by clavicular nonunion. When the shoulder is abducted orlifted, the costoclavicular space narrows and compresses thesubclavian vessels or nerves, which is a common cause of TOS.Malunion of a midshaft clavicle fracture is common, but it seldomcauses TOS.2,10 Theoretically, if there is malunion of a midshaftclavicle fracture, the distal end of the clavicle may rotateanteroinferiorly, resulting in clavicular shortening and strictureof the costoclavicular space, thus compressing the subclavianvessels or nerves, and causing TOS. Connolly and Dehne1 followed15 patients with clavicular nonunion, seven of whom werediagnosed with TOS. Jupiter and Leffert3 reported 23 cases of
nonunion, four of whom were diagnosed with TOS. Rowe9 reportedthat vessel and nerve compression symptoms in two patients werecaused by hyperplasia of the bone callus after clavicular fracture.Mulder et al.5 reported one case of TOS caused by malunion of amidshaft clavicle fracture. Currently, there is no other publishedreport detailing midshaft clavicular fracture and resultant thoracicoutlet syndrome.
3.4. TOS treatment
Conservative treatment is usually preferable for TOS. Thesymptoms in approximately 60% of the patients can be completelyalleviated, and the discomfort in the cervical and scapular regionscan be alleviated in 90% of patients. The mainstay of conservativetreatment is physical exercise, whose main objective is to restoremuscle balance in the cervical and scapular regions, that is, torestore normal muscle length, scope of activity, and strength.When the symptoms seriously affect the work and life of thepatient, and conservative treatment has had no significant effect,surgical treatment must be considered.
Surgical treatment for TOS includes resection of the scalenusanterior, resection of the first rib, or partial or total resection of theclavicle in order to alleviate compression of the affected vesselsand/or nerves. Rowe9 observed that removal of hyperplastic bonecallus relieved the symptoms of TOS. Because partial or totalresection of the clavicle may cause instability of the scapula, thecurrently favoured surgical procedure for clavicular malunioncausing TOS symptoms is resection of the hyperplastic part of theclavicle to relieve the compression of the injured vessels and/ornerves. Our patient presented with malunion of the left clavicle,and external bone callus. Surgery was performed to realign thefractured clavicle and remove the external bone callus. At 1-yearfollow-up, her shoulder and forearm were free of symptoms, andshe had full range of motion and normal use of her shoulder.
The traditional view that the vast majority of clavicularfractures heal with good functional outcomes following non-operative treatment is no longer valid.4 All displaced fractures thatare treated nonoperatively heal with some degree of malunion dueto angulation or shortening. TOS can be caused by chronicmalunion associated with hyperplastic bone callus. Correctiveosteotomy and plate fixation can improve function in patients inwhom symptomatic malunion has produced neurovascularcompression.
References
1. Connolly JF, Dehne R. Nonunion of clavicle and thoracic outlet syndrome. JTrauma 1989;29:1127–33.
2. Daskalakis MK. Thoracic outlet syndrome. Int Surg 1983;68:337–44.3. Jupiter JB, Leffert RD. Non-union of the clavicle: associated complications and
surgical management. J Bone Joint Surg Am 1987;69:753–60.4. Kashif Khan LA, Bradnock TJ, Caroline Scott, Michael Robinson C. Fractures of
the clavicle. J Bone Joint Surg Am 2009;91:447–60.5. Mulder DS, Greenwood FAH, Brooks CE. Posttraumatic thoracic outlet syn-
drome. J Trauma 1973;13:706–15.6. Nahum R, Lars N, Angus WW. Functional outcome of surgical treatment of
symptomatic nonunion and malunion of midshaft clavicle fractures. J ShoulderElbow Surg 2007;16:510–4.
7. Novak CB, Mackinnon SE. Orthop Clin North Am 1996;27:747–62.8. Novak CB, Mackinnon SE, Patterson GA. J Hand Surg Am 1993;18:292–9.9. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin
Orthop 1968;58:29–42.10. Roos DB. Congenital anomalies associated with thoracic outley syndrome:
anatomy, syndrome, diagnosis and treatment. Am J Surg 1976;132:771–8.11. Richard JS, Sharon LH, Neal MR. Thoracic outlet syndrome. The Neurologist
2008;14:365–73.12. Thompson JF, Jannsen F. Br J Surg 1996;83:435–6.