midshaft clavicle fractures in...
TRANSCRIPT

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-752
Preston CF, Egol KA. Midshaft clavicle fractures in adults. Bull NYU Hosp Jt Dis. 2009;67(1):52-7.
Abstract
Clavicle fractures remain one of the more common frac-tures encountered in the orthopaedic office. Nonoperative management remains the standard of care in most cases. However, studies have shown a higher nonunion rate and decreased patient satisfaction in fractures with increased shortening. The malunion resulting from nonoperative man-agement has been shown to be problematic in patients with significant fracture shortening. When operative reduction and fixation is indicated, there are numerous techniques to aid the surgeon patient care. This article reviews the midshaft clavicle fracture and discusses recent outcome studies on patients with fracture shortening and approaches to opera-tive management.
The clavicle is one of the most commonly fractured bones encountered by the orthopaedic surgeon. Clavicle fractures represent up to 12% of all frac-
tures and between 44% and 66% of the fractures about the shoulder.1,2 Due to its inherent anatomy, the midshaft is the most common location for these fractures accounting for ap-proximately two-thirds of cases.2,3 Historically, the treatment of these fractures has been conservative. In fact, Hippocrates noted that the physician would not be sorry for the neglect of these patients. Nonoperative management is based on
the high rate of union noted by investigators reporting on large series of patients.4,5 However, recent reports have noted lower union rates for displaced midshaft fractures treated nonoperatively and questioned the sequelae of subsequent malunion in fractures that do go on to heal.6-9 Therefore, interest in the operative management of midshaft clavicle fractures is growing and includes a recent evidence-based analysis.10 The current review will focus on the anatomy and evaluation of midshaft clavicle fractures and discuss the role of both operative and nonoperative management.
Surgical Anatomy and BiomechanicsThe clavicle is the first bone to ossify during the fifth week of gestation and is the last to fuse.11 The sternal end fuses in the early third decade. Details of the osseous anatomy become particularly important when planning operative management. Medially, the clavicle is convex forward, while laterally it is concave forward. The bone flattens out both medially and laterally at the sternoclavicular and acromio-clavicular joints. There is a central zone of transition where the clavicle is more tubular. This central area is subjected to the highest bending and torsional forces, making it vulner-able to fracture.12
Medially the clavicle is supported by strong capsular ligaments. Interclavicular ligaments run across the sterno-clavicular joint acting as static stabilizers, preventing down-ward displacement of the clavicle. Laterally, the clavicle attaches to the scapula via the coracoclavicular ligaments and acromioclavicular ligaments. The coracoclavicular liga-ments consist of the trapezoid ligament laterally and conoid ligament medially. The strong posterosuperior portion of the acromioclavicular ligaments prevent anteroposterior (AP) clavicular translation.13
The muscular attachments to the clavicle become impor-tant when considering displacement patterns of fractures. Medially, the pectoralis major and sternohyoid have their
Midshaft Clavicle Fractures in Adults
Charles F. Preston, M.D., and Kenneth A. Egol, M.D.
Charles Preston, M.D., was a Chief Resident at the NYU Hospi-tal for Joint Diseases Department of Orthopaedic Surgery and is currently in private practice with Muir Orthopaedic Specialists, Walnut Creek, California. Kenneth A. Egol, M.D., is an Associate Professor, New York University School of Medicine, and Vice Chairman for Education, Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, NYU Langone Medical Center, New York, New York.Correspondence: Kenneth A. Egol, M.D., Department of Orthopae-dic Surgery, Suite 1402, NYU Hospital for Joint Diseases, 301 East 17th Street, New York, New York 10003; [email protected].

53Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-7
origins. Superomedially, the sternocleidomastoid has its origin while running toward the inferior base of the skull. When the clavicle is fractured, the origin of the sterno-cleidomastoid acts as an insertion and the medial segment displaces accordingly. Anterolaterally, the deltoid has part of its origin on the clavicle, while the trapezius has part of its insertion posterosuperiorly. The trapezius pulls distal fracture fragments posteromedially and the fascial interval between the deltoid and trapezius is exploited during the surgical dissection. The clavicle is intimately located near the brachial plexus and subclavian vessels. The middle third is the inferior boarder of the posterior triangle of the neck. Knowledge of this anatomy is essential when planning surgical dissection and hardware placement. The clavicle functions as a strut in the sagittal plane, stabilizing the glenohumeral joint and providing a stable center of rotation for the shoulder.14 In the coronal plane, the clavicle performs a suspensory function. The shoulder girdle effectively hangs from the clavicle by the coracoclavicular ligament. This has been described as being similar to a “sign post,” whose arm, the clavicle, is dynamically stabilized by the trapezius.15
Patient EvaluationAn understanding of the mechanism of injury is essential in ruling out associated injuries. A clavicle fracture can result from both indirect and direct trauma. A fall onto the shoulder is the most common mechanism.16 A fall onto an outstretched hand is an indirect mechanism that may lead to fracture as well.17 Less common causes of fracture may include pathologic fractures following a radical neck dissection or stress fractures in laborers.3,5,16-18 Due to its subcutaneous position, open fractures of the clavicle are possible and every polytrauma patient should be examined thoroughly. Associated injuries should be evaluated and treated ac-cordingly. Rib injuries occur concomitantly 3% of the time, and a pneumothorax should be ruled out by chest radiograph if suspected. A neurovascular exam of the effected extremity should be performed and findings noted to document the in-tegrity of the brachial plexus and axillary arterial tributaries. Multiple radiographic views have been recommended for clavicle fractures. The injuries are often discovered during a routine chest radiograph. The chest film may be evaluated and associated clavicular shortening grossly as-sessed. A clavicular AP view is shot with the beam directed 15° to 30° cephalad to avoid the mediastinal contents. An apical oblique image is obtained by angling the shoulder 45° toward the beam and 20° cephalad. Due to the S-shape structure of the clavicle, the apical oblique may provide an assessment of clavicular length. Advanced imaging studies such as a computed tomography (CT) scan are reserved for cases of possible nonunion or fractures at the medial or lateral ends. Furthermore, a CT scan may be indicated
in the presence of an associated scapular neck fracture to help assess displacement. Currently, there is no role for magnetic resonance imaging (MRI) in the management of these injuries.
Nonoperative ManagementHistorically, nonoperative management has been the main-stay of treatment for midshaft clavicular fractures in adults. Investigators have cited high union rates and low associated functional deficits as a basis for such management. In 1960, Neer reported on 2,235 clavicle fractures and showed a nonunion rate of only 0.13%.4 In 1968, Rowe reported on 566 clavicle fractures and found a nonunion rate of only 0.8%.5 However, a critique of these studies may be that the pediatric population was included in the study groups. It is also notable that modern day functional assessments of outcome were not available in either study. In 1997, Hill and colleagues demonstrated a much higher nonunion rate of 15% in a study group of displaced midshaft clavicle fractures. In addition, these investigators reported 30% of the nonunion patients in this study had a poor functional result. The conclusion of this retrospective study was that an initial fracture shortening of greater than 2 cm was associated with nonunion and a high percentage of those patients went on to a poor result. Overall, the literature is clear that the majority of adults with midshaft clavicle fractures will heal their injuries. Initial immobilization in either a sling or a figure-of-eight bandage remains the norm. The patient should remain immobilized until pain allows discontinuation, typically at 2 to 4 weeks. Active motion may be initiated at that time, with light duty allowed for laborers at 6 weeks. A return to contact sport may be allowed by 3 months if the radiographs and examination allow. Anderson and associates performed a randomized study evaluating a sling versus a figure-of-eight bandage to treat clavicle fractures.19 The sling was maintained until pain allowed and the figure-of-eight bandage was worn for 3 weeks. The investigators reported on a cohort of 61 pa-tients that followed-up from the initial study group of 79. They found no difference in union rate or time to union. There was a significant increase in dissatisfaction in the patients treated in a figure-of-eight bandage. However, the reader must note that the follow-up period was 3 months in the study, and no functional outcome scores were used to evaluate treatment. In their retrospective review of 140 midclavicular fractures, Stanley and Norris also noted no difference in the radiographic outcome when comparing the sling versus figure-of-eight treatment.20 Once again, this was a short-term radiographic outcome study lacking functional outcome scores. Nonoperative treatment of midclavicular fractures in adults will likely result in a malunion with various degrees of angular, rotatory, and translational deformity (Fig. 1). The clavicle will typically lie shortened with the lateral fragment

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-754
posterior to the medial fragment.21 The effect of subsequent malunion and the possible sequelae have been the subjects of recent study. As stated previously, Hill and coworkers had a greater than 30% dissatisfaction rate in 52 malunited clavicle frac-tures.7 Thirty-seven percent of the patients had difficulty with overhead activities and 25% required the use of an analgesic for pain at an average follow-up of 38 months. When using the contralateral clavicle as a comparison, another study found a 25% dissatisfaction rate in shortened clavicle fractures. The investigators defined a threshold of acceptable shortening to be 18 mm in males and 14 mm in females.22 Muscular dysfunction has recently been demon-strated in shortened malunions of the clavicle as well.23 In 2006, McKee and colleagues reported on the functional out-come of healed displaced midshaft clavicle fractures.8 The investigators reported on the results of 30 healed displaced clavicle fractures at an average of 55 months. In this study, Constant and DASH outcome measures were utilized as was objective strength testing of the effected shoulder.24,25 The range of motion of the injured shoulder was similar to the contralateral side. However, the injured shoulder had strength and endurance scores 60% to 80% in various planes of motion when compared to the opposite side. The Constant and DASH scores were significantly worse than for contralateral shoulder, signifying a relative disability in the malunited clavicle fractures. The recent malunion literature is countered by the 17-year follow-up reported by Nordqvist and associates, which concluded that acceptable results can be expected with non-operative management.26 The study investigators reported on 225 midshaft clavicle fractures treated nonoperatively and reported outcomes as good, fair, or poor, based on pain or functional deficit. There were 185 good results in such a classification. It has been noted that, although the majority of patients with nondisplaced fractures had a good result,
the percentage decreased to 83% of those with displaced two-part fractures and 73% of those with displacement and comminution.27
Operative ManagementThe options for surgical management include external fixa-tion, intramedullary fixation, and osteosynthesis with a plate and screws. The technique used depends on surgeon prefer-ence and the “personality” of the fracture. Patient positioning is either supine or beach chair. Supine positioning can help to facilitate intramedullary screw placement and provide easier access for the image machine. We prefer the beach chair position with a folded towel underneath the ipsilateral scapula when using plate and screw techniques. Incisions are typically placed along Langers lines, and thick skin flaps are developed to aid in covering a plate. Supraclavicular nerves should be identified and preserved in order to avoid the development of painful neuromas (Fig. 2).
Figure 1 Injury radiograph (A) and 6-month follow-up radiograph (B), demonstrating an anticipated malunion of a displaced midshaft clavicle fracture.
B
A
Figure 2 Intraoperative view demonstrating the preservation of supraclavicular nerves during the superior plating of a clavicle fracture.
55Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-7
External fixation is effective in the setting of open frac-tures and has been reported for use in nonunions.28 Further-more, external fixation may be considered in certain open fractures or fractures with vascular injury to allow access to the neurovascular anatomy. When external fixation is utilized, typically 3.0 mm half pins are used. The medial pins should be placed in an anterior to posterior direction to avoid the apex of the lung. The lateral pins are then placed in a superior to inferior direction. Schuind and coworkers reported the healing of 20 out of 20 clavicular nonunions treated in such a manner.28 The advocates of intramedullary fixation cite the ease of the procedure, the limited exposure involved, and satisfac-tory rates of healing. The technique is variable and may
involve the use of K-wires, threaded screws, Knowles pins, Hagie pins, or elastic titanium nails. Intramedullary fixa-tion typically should be avoided in the setting of fracture comminution where a plate will better maintain clavicular length. Only a small skin incision is needed for intramedullary fixation. The clavicle’s medial and lateral ends are prepared sequentially with drill bits until a good fit is obtained. The appropriate sized pin is then placed in a retrograde fashion. The pin will exit the lateral fragment under the skin posteromedial to the acromioclavicular joint. A small stab incision can then be made to pull the pin back prior to advancing into the medial fragment. Reduction forceps are used to hold the fracture in place while this is performed. Historically, excellent healing rates have been observed using intramedullary fixation. Neviaser in 1975 reported a 100% healing rate using Knowles pins.29 In 1981, Zenni and colleagues reported on a mix of intramedullary fixation techniques, but had a 100% healing rate.30 The investiga-tors, however, did note one instance of wire breakage and one refracture following hardware removal. More recently Chu and associates reported on the healing of 77 of 78 clavicle fractures treated with a Knowles pin.31 Elastic titanium nails were used by Jubel and coworkers to treat 58 acute midshaft clavicle fractures, and only one nonunion was encountered.32 With these excellent healing rates have come concerns about associated complications. In a retrospective com-parison study, Grassi and colleagues had a 35% compli-cation rate with intramedullary fixation.33 The majority of complications were superficial infections. However, delayed union, nonunion, and refractures occurred as well.
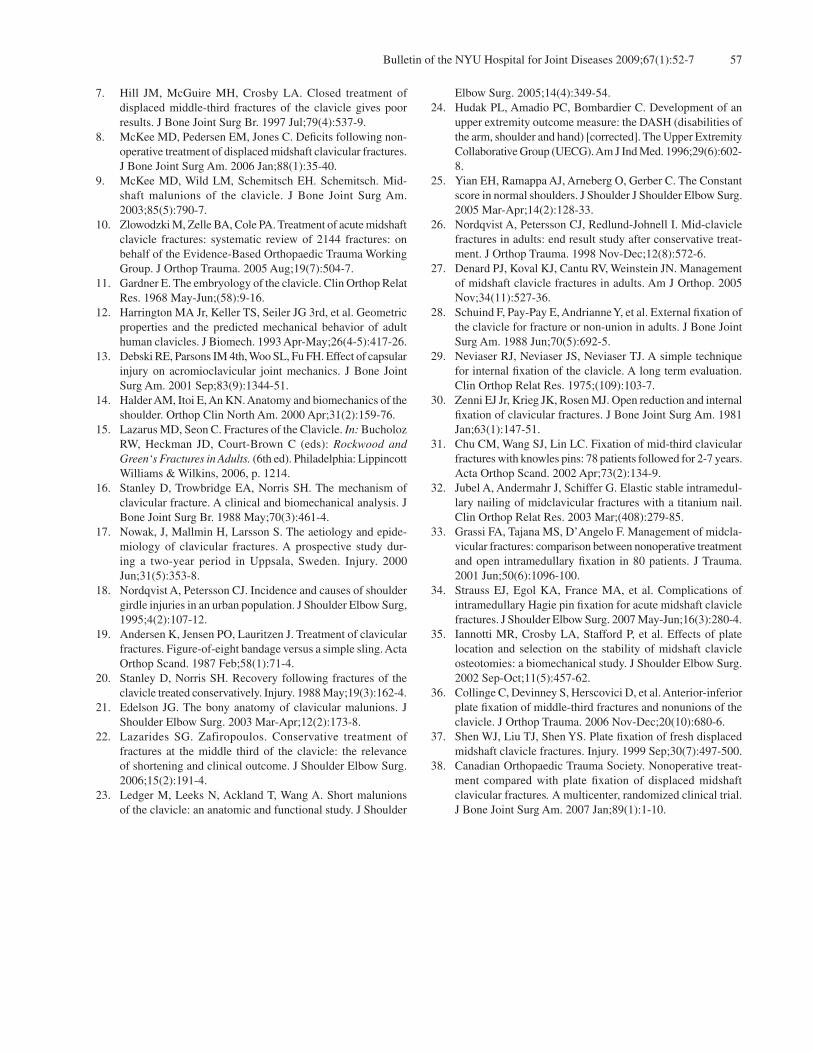
Figure 4 Injury radiograph (A) and 1-year follow-up radiograph (B), demonstrating the successful application of a 3.5 mm reconstruc-tion plate in an anteroinferior fashion.
B
A
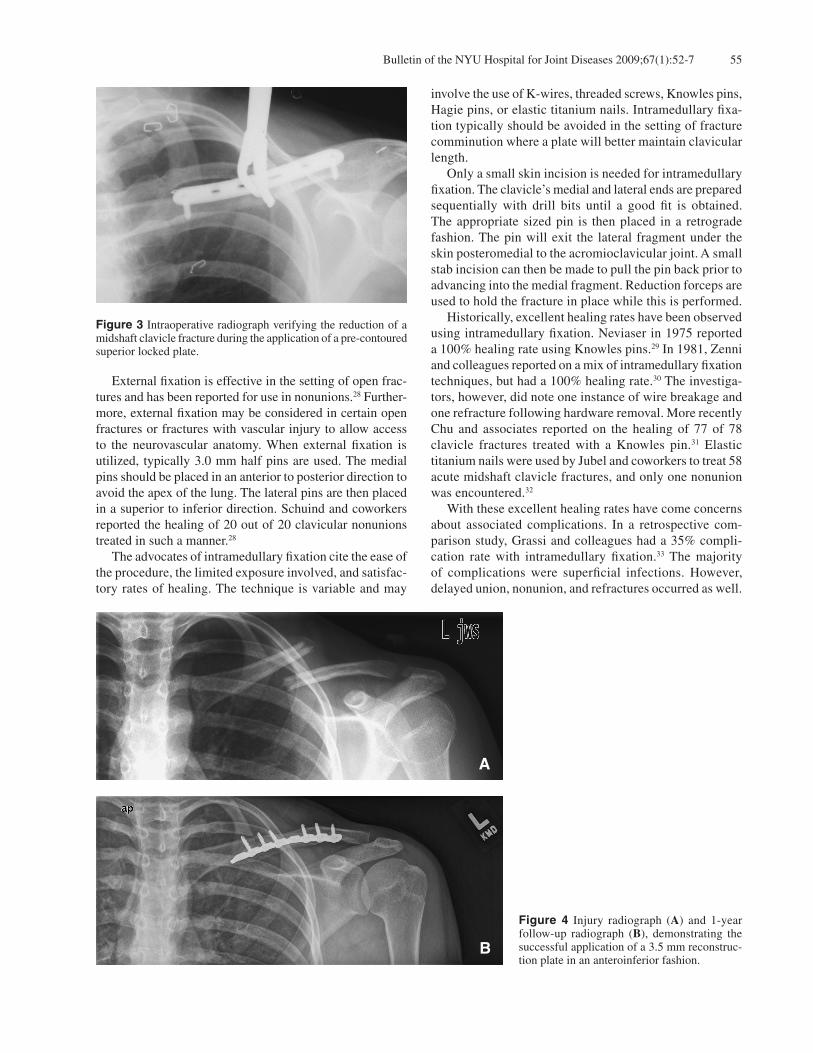
Figure 3 Intraoperative radiograph verifying the reduction of a midshaft clavicle fracture during the application of a pre-contoured superior locked plate.

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-756
In a recent study, Strauss and associates reported on the complications associated with the use of intramedullary pins for the treatment of midshaft clavicle fractures.34 The investigators found that while the ultimate union rate was 100% and shoulder range of motion was largely preserved, there was a 50% complication rate. As with the previously mentioned study, most complications were related to su-perficial skin breakdown. Plate osteosynthesis carries the benefit of more rigid fixation, the ability for cortical compression, and more rotational control of the fracture. Plating options include small fragment implants, such as 3.5 mm LDC plates and 3.5 mm reconstruction plates. Furthermore, mini fragment fixation such as 2.7 mm plates and screws or smaller may also be utilized in small or thin patients, or both, as well as in extensively comminuted fractures. Pre-contoured plates with locking and nonlocking options are available as well (Fig. 3). A compression plating technique can be used for transverse or short oblique fractures. Long oblique or comminuted fractures should be amenable to neutralization plating with lag screws. Autogenous bone grafting may be considered in the setting of highly comminuted fractures.27
Plates are applied in a superior or anteroinferior posi-tion across the midclavicle. The wide anterior to posterior expanses of the clavicle allow ample room for a superior plate to be applied. The dissection for superior plating may also avoid the neurovascular structures beneath the clavicle. In a 2002 study, Iannotti and coworkers found the superior position to have more axial and rotational rigidity.35 Anteroinferior plating on the other hand has four major advantages. First, it allows for a longer length of screws in the anterior to posterior direction. Second, there is a decreased risk to neurovascular injury when plunging with the drill bit. Third, hardware should be less promi-nent as opposed to the superior plate which would lie just beneath the subcutaneous tissue. Lastly, an anteroinferior plate will theoretically buttress the lateral fragment and prevent inferior displacement (Fig. 4).36 In 1999, Shen and colleagues reported their results of plating for displaced midclavicular fractures.37 The inves-tigators routinely plated all displaced fractures presenting to their institution. The study cohort included 232 fractures that underwent a mixture of plating techniques dependent on the fracture characteristics. The union rate was 97% with a single deep infection and four superficial infec-tions. Patients were followed-up with a phone interview documenting any residual symptoms and their overall satisfaction rate. No patients had a perceived deformity or deficit in strength or range of motion, and the satisfaction rate with the procedure was 94%. More recently, a multicenter randomized clinical trial comparing nonoperative treatment with plate fixation of displaced midshaft clavicle fractures was performed.38 One hundred eleven of the 132 patients randomized completed the one year follow-up. There were 62 patients in the
plate group and 49 patients in the sling group. Outcome measures included radiographic union, Constant shoulder scores, DASH scores, and an overall satisfaction survey.24,25 The mean time to union was significantly improved in the operative group as was the nonunion rate (3% vs 15%). The Constant scores were significantly superior in the operative group at all time points utilized in the study. The DASH scores were also significantly superior in the operative group. The investigators’ conclusion supported plating of displaced fractures and citied the significance of the patient-based outcomes used in their study. However, these results may be influenced by the fact that outcomes were not further stratified according to the patient’s healing status. Simply stated, the poor outcomes of the nonunion patients in the nonoperative group may have led to the overall difference in comparing the two groups.
ConclusionClavicle fractures continue to be a common injury encoun-tered by the orthopaedic surgeon and have received much attention recently. Overall, the union rate of minimally dis-placed fractures treated nonoperatively is acceptable. The management of the displaced midshaft clavicle fractures remains somewhat controversial as patient-based outcome measures have revealed the possible sequelae of clavicular malunion. Currently, there is momentum growing toward the operative management of displaced midclavicular fractures. While nonoperative care remains the standard for the major-ity of minimally displaced clavicle fractures, there may be a subset of patients with significant displacement who benefit from surgical intervention.
Disclosure StatementCharles F. Preston, M.D., has no financial or proprietary interest in the subject matter or materials discussed, includ-ing, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony. Kenneth A. Egol, M.D., is an unpaid consultant to Exactech, Inc., has received institutional support from Biomet, Smith & Nephew, Stryker, and Synthes, and participates in stock ownership of Johnson & Johnson.
References1. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology
of clavicle fractures. J Shoulder Elbow Surg. 2002 Sep-Oct;11(5):452-6.
2. Robinson CM. Fractures of the clavicle in the adult. Epi-demiology and classification. J Bone Joint Surg Br. 1998 May;80(3):476-84.
3. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994(300):127-32.
4. Neer CS 2nd. Nonunion of the clavicle. JAMA. 1960;172:1006-11.
5. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res. 1968;(58):29-42.
6. Chan KY, Jupiter JB, Leffert RD, Marti R. Clavicle malunion. J Shoulder Elbow Surg. 1999 Jul-Aug;8(4):287-90.
57Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):52-7
7. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997 Jul;79(4):537-9.
8. McKee MD, Pedersen EM, Jones C. Deficits following non-operative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am. 2006 Jan;88(1):35-40.
9. McKee MD, Wild LM, Schemitsch EH. Schemitsch. Mid-shaft malunions of the clavicle. J Bone Joint Surg Am. 2003;85(5):790-7.
10. Zlowodzki M, Zelle BA, Cole PA. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005 Aug;19(7):504-7.
11. Gardner E. The embryology of the clavicle. Clin Orthop Relat Res. 1968 May-Jun;(58):9-16.
12. Harrington MA Jr, Keller TS, Seiler JG 3rd, et al. Geometric properties and the predicted mechanical behavior of adult human clavicles. J Biomech. 1993 Apr-May;26(4-5):417-26.
13. Debski RE, Parsons IM 4th, Woo SL, Fu FH. Effect of capsular injury on acromioclavicular joint mechanics. J Bone Joint Surg Am. 2001 Sep;83(9):1344-51.
14. Halder AM, Itoi E, An KN. Anatomy and biomechanics of the shoulder. Orthop Clin North Am. 2000 Apr;31(2):159-76.
15. Lazarus MD, Seon C. Fractures of the Clavicle. In: Bucholoz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green‘s Fractures in Adults. (6th ed). Philadelphia: Lippincott Williams & Wilkins, 2006, p. 1214.
16. Stanley D, Trowbridge EA, Norris SH. The mechanism of clavicular fracture. A clinical and biomechanical analysis. J Bone Joint Surg Br. 1988 May;70(3):461-4.
17. Nowak, J, Mallmin H, Larsson S. The aetiology and epide-miology of clavicular fractures. A prospective study dur-ing a two-year period in Uppsala, Sweden. Injury. 2000 Jun;31(5):353-8.
18. Nordqvist A, Petersson CJ. Incidence and causes of shoulder girdle injuries in an urban population. J Shoulder Elbow Surg, 1995;4(2):107-12.
19. Andersen K, Jensen PO, Lauritzen J. Treatment of clavicular fractures. Figure-of-eight bandage versus a simple sling. Acta Orthop Scand. 1987 Feb;58(1):71-4.
20. Stanley D, Norris SH. Recovery following fractures of the clavicle treated conservatively. Injury. 1988 May;19(3):162-4.
21. Edelson JG. The bony anatomy of clavicular malunions. J Shoulder Elbow Surg. 2003 Mar-Apr;12(2):173-8.
22. Lazarides SG. Zafiropoulos. Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg. 2006;15(2):191-4.
23. Ledger M, Leeks N, Ackland T, Wang A. Short malunions of the clavicle: an anatomic and functional study. J Shoulder
Elbow Surg. 2005;14(4):349-54.24. Hudak PL, Amadio PC, Bombardier C. Development of an
upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29(6):602-8.
25. Yian EH, Ramappa AJ, Arneberg O, Gerber C. The Constant score in normal shoulders. J Shoulder J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):128-33.
26. Nordqvist A, Petersson CJ, Redlund-Johnell I. Mid-clavicle fractures in adults: end result study after conservative treat-ment. J Orthop Trauma. 1998 Nov-Dec;12(8):572-6.
27. Denard PJ, Koval KJ, Cantu RV, Weinstein JN. Management of midshaft clavicle fractures in adults. Am J Orthop. 2005 Nov;34(11):527-36.
28. Schuind F, Pay-Pay E, Andrianne Y, et al. External fixation of the clavicle for fracture or non-union in adults. J Bone Joint Surg Am. 1988 Jun;70(5):692-5.
29. Neviaser RJ, Neviaser JS, Neviaser TJ. A simple technique for internal fixation of the clavicle. A long term evaluation. Clin Orthop Relat Res. 1975;(109):103-7.
30. Zenni EJ Jr, Krieg JK, Rosen MJ. Open reduction and internal fixation of clavicular fractures. J Bone Joint Surg Am. 1981 Jan;63(1):147-51.
31. Chu CM, Wang SJ, Lin LC. Fixation of mid-third clavicular fractures with knowles pins: 78 patients followed for 2-7 years. Acta Orthop Scand. 2002 Apr;73(2):134-9.
32. Jubel A, Andermahr J, Schiffer G. Elastic stable intramedul-lary nailing of midclavicular fractures with a titanium nail. Clin Orthop Relat Res. 2003 Mar;(408):279-85.
33. Grassi FA, Tajana MS, D’Angelo F. Management of midcla-vicular fractures: comparison between nonoperative treatment and open intramedullary fixation in 80 patients. J Trauma. 2001 Jun;50(6):1096-100.
34. Strauss EJ, Egol KA, France MA, et al. Complications of intramedullary Hagie pin fixation for acute midshaft clavicle fractures. J Shoulder Elbow Surg. 2007 May-Jun;16(3):280-4.
35. Iannotti MR, Crosby LA, Stafford P, et al. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: a biomechanical study. J Shoulder Elbow Surg. 2002 Sep-Oct;11(5):457-62.
36. Collinge C, Devinney S, Herscovici D, et al. Anterior-inferior plate fixation of middle-third fractures and nonunions of the clavicle. J Orthop Trauma. 2006 Nov-Dec;20(10):680-6.
37. Shen WJ, Liu TJ, Shen YS. Plate fixation of fresh displaced midshaft clavicle fractures. Injury. 1999 Sep;30(7):497-500.
38. Canadian Orthopaedic Trauma Society. Nonoperative treat-ment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10.