plating versus intramedullary pin or conservative treatment for midshaft fracture of clavicle: a...
TRANSCRIPT
Investigational r
*Reprint req
Department of O
E-mail addre
J Shoulder Elbow Surg (2011) 20, 1008-1015
1058-2746/$ - s
doi:10.1016/j.jse
www.elsevier.com/locate/ymse
Plating versus intramedullary pin or conservativetreatment for midshaft fracture of clavicle:a meta-analysis of randomized controlled trials
Xin Duan, MD, Gang Zhong, MD, Shiqiang Cen, MD, Fuguo Huang, MD,Zhou Xiang, MD*
Department of Orthopaedics, West China Hospital, Sichuan University, Chengdu, China
Hypothesis: Clavicular fractures account for 2% to 2.6% of all fractures. Plating has been considered thegold standard for treating midshaft clavicular fracture. Intramedullary pinning and conservative treatmentshave also been commonly used. We hypothesized that intramedullary pinning and conservative treatmentshave the same treatment results compared with plating.Methods: To evaluate the effect of plating vs intramedullary pinning or conservative treatment for mid-shaft clavicular fracture, the Cochrane Central Register of Controlled Trials (CENTRAL; Wiley OnlineLibrary, October 2010), PubMed (1950 to October 2010), and EMBASE (1980 to October 2010) weresearched. Randomized and quasi-randomized controlled clinical studies evaluating plating vs intramedul-lary pinning or plating vs conservative treatment for midshaft clavicular fracture in adults were collected.After independent study selection by 2 authors, data were collected and extracted independently. The meth-odologic quality of the studies was assessed. Pooling of data was undertaken.Results: Four studies involving 305 clavicular fractures were included. There were no significant differ-ences between plating and intramedullary pinning with regard to outcome for Oxford Shoulder Score,Constant Shoulder Score, nonunion, infection, fixation failure, and hardware removal. More symptomatichardware events occurred with plating compared with intramedullary pinning. Reduced nonunion, mal-union, and neurologic symptoms, as well as more satisfaction with ultimate appearance, were associatedwith plating than with conservative treatment.Discussion: This meta-analysis supports the treatment effects reported previously with plating for mid-shaft clavicular fractures. The outcome of this meta-analysis contradicted the findings reported previouslywith conservative treatment for midshaft clavicular fractures.Conclusion: The available evidence suggests that there are no differences in treatment effects betweenplating and intramedullary pinning, but plating is associated with more side effects. Plating is associatedwith improved treatment effects when compared with conservative treatment.Level of evidence: Level II, Meta-Analysis.� 2011 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: Clavicle; fracture; plating; intramedullary pinning; conservative treatment; meta-analysis
eview board approval was not required for this study.
uests: Prof Zhou Xiang, MD, No 37 Guo Xue Xiang,
rthopaedics,West ChinaHospital, Chengdu, China 610041.
ss: [email protected] (Z. Xiang).
ee front matter � 2011 Journal of Shoulder and Elbow Surgery
.2011.01.018
Clavicular fracture is one of the most common fracturesin children and adults, representing 2% to 2.6% of allfractures. Clavicular fractures typically result from falls,motor vehicle accidents, and sporting injuries.26 The major
Board of Trustees.

Table I Search strategies
CENTRAL PubMed EMBASE
#1 MeSH descriptor Clavicle, thisterm only
#2 (clavic) or collarbone): ti, ab, kw#3 (#1 or #2)#4 MeSH descriptor Fracture Healing,
this term only#5 MeSH descriptor Fracture Fixation
explode all trees#6 MeSH descriptor Fractures, Bone
explode all trees#7 (fracture) or pseudoarthros) or
pseudarthros)): ti, ab, kw#8 (#4 or #5 or #6 or #7)#9 (#3 and #8)
(Clavicle [mh] or clavic) [tw] orcollarbone [tw]) and (FractureHealing [mh] or Fracture Fixation[mh] or Fractures, Bone [mh] orfracture) [tw] or pseudarthrosis[mh] or pseudoarthros) [tw] orpseudarthros) [tw]) and(randomized controlled trial [pt] orcontrolled clinical trial [pt] orrandomized controlled trials [mh] orrandom allocation [mh] or double-blind method [mh] or single-blindmethod [mh] OR clinical trial [pt] orclinical trials [mh] or (‘clinical trial’[tw]) or ((singl) [tw] or doubl) [tw]or trebl) [tw] or tripl) [tw]) and(mask) [tw] or blind) [tw])) or(placebos [mh] or placebo) [tw] orrandom) [tw] or research design[mh:noexp]) not (animals [mh] nothuman [mh]))
1. ‘clavicle’/exp or clavicle2. ‘fracture healing’/exp or ‘fracture
healing’3. ‘fracture treatment’/exp or
‘fracture treatment’4. ‘fracture’/exp or fracture5. #2 or #3 or #4 215,3326. ‘clinical trial’/exp or ‘clinical trial’7. ‘randomized controlled trial’/exp
or ‘randomized controlled trial’8. ‘randomization’/exp or
randomization9. ‘single blind procedure’/exp or
‘single blind procedure’10. double blind procedure’/exp or
‘double blind procedure’11. ‘placebo’/exp or placebo12. RCT13. ‘prospective study’/exp or
‘prospective study’14. #6 or #7 or #8 or #9 or #10 or #11
or #12 or #1315. #1 and #5 and #14
) To truncate a term, use an asterisk ()) at the end of a search term.
Figure 1 Flow chart shows how articles were selected. RCT, randomized controlled trial.
Meta-analysis of plating for clavicle fracture 1009
mechanism of clavicle fracture has been reported to bea direct fall on the shoulder (85%), followed by a direct blow(13%) and a fall on an outstretched hand (2%).23 Midshaftfractures account for approximately 70% to 80% of allclavicular fractures.23,26,28
Among the treatment options for midshaft clavicularfracture are nonoperation, internal fixation with plates, andinternal fixation with intramedullary pins. Plate fixation isthe standard surgical method used for the displaced mid-clavicular fracture. However, several complications have

1010 X. Duan et al.
been reported, including infection, wound breakdown,nonunion, implant failures, poor cosmetic results, and localskin numbness.2,6,31
Recently, an increasing number of surgeons haveattempted to use intramedullary pins for midshaft clavicularfracture. The use of intramedullary pins for stabilization ofclavicular fractures offers the advantages of fracture fixa-tion through smaller incisions, avoidance of significantsoft-tissue stripping at the fracture site with relativeprotection of the supraclavicular nerves, and the ability toremove the implant through a similarly small incision withthe patient under local anesthesia.5,27 Potential limitationsinclude hardware migration or failure, painful prominenthardware, refracture after hardware removal, and thedevelopment of nonunion.1,5
Nonoperation, as a traditional method, has been used totreat midshaft clavicular fracture, even when substantiallydisplaced. However, there is growing evidence and aware-ness that the outcome of such treatment is not as satisfac-tory as was previously thought. More recent studies ofdisplaced midshaft clavicular fractures have shown higherrates of nonunion, malunion, and patient dissatisfactionthan previously reported.18,21,33
This meta-analysis addresses the key question ofwhether plating produces superior results to intramedullarypinning or conservative treatment. Our objective was todetermine the effects of plating vs intramedullary pinningand plating vs conservative treatment for displaced short-ening fracture of the middle third of the clavicle.
Materials and methods
Eligibility criteria and literature search
The study included randomized and quasi-randomized controlledclinical studies, in which the method of allocating participants toa treatment group is not strictly random (eg, by date of birth,hospital record number, alternation), evaluating plating vsnonoperative methods and the plating vs intramedullary pinmethods of treatment for the middle third of the clavicle. Allskeletally mature patients with midshaft fractures of the claviclewere included. A major reason for exclusion of studies was notbeing a randomized controlled trial.
We searched the Cochrane Central Register of ControlledTrials (CENTRAL; Wiley Online Library, October 2010), PubMed(1950 to October 2010), and EMBASE (1980 to October 2010).The search strategy is summarized in Table I. The search waswithout restriction by language and collected studies conducted onhuman subjects. The reference lists of reviews and retrievedarticles were hand-searched contemporaneously.
Data extraction and quality assessment
For each trial, we gathered data on study type, interventions,randomization process, allocation concealment process, blinding,selective reporting, involved cases, lost to follow-up, and
addressed lost data. Data were extracted independently by 2authors (X.D. and Z.X.) according to the prespecified selectioncriteria. Disagreement was resolved by discussion.
The quality of the studies was assessed using the followingcriteria:
1. randomization process: assessment for selection bias;2. allocation concealment process: assessment of selection bias;3. level of blinding: assessment for performance bias and
detection bias;4. incomplete outcome data: assessment for potential bias
related to drop-out/lost to follow-up; and5. selective reporting: assessment for reporting bias.9
Based on the criteria described in the Cochrane Handbook forSystematic Reviews of Interventions, studies were broadly dividedinto the categories of (1) yes: indicating low risk of bias; (2) no:indicating high risk of bias; and (3) unclear: indicating either lackof information or uncertainty over the potential for bias.9 Eachtrial was independently assessed by 2 authors (X.D. and Z.X.). Alldisagreements were resolved by discussion.
Statistical analyses
The statistical analysis was conducted using Review Manager 5.0software (The Nordic Cochrane Centre, the Cochrane Collabora-tion, 2008, Copenhagen, Denmark). Heterogeneity was assessed byvisual inspection of the forest plot (analysis) along with consider-ation of the test for heterogeneity and the I2 statistic, with signifi-cance set at P < .05.10 Results of comparable groups of trials werepooled. Initially, we used the fixed-effect model and 95% confi-dence intervals (CI). We also considered using the random-effectsmodel where there was heterogeneity. The treatment effects wereexpressed as risk ratios (RR) with 95% CI for dichotomousoutcomes. Where appropriate, we calculated and reported numbersneeded to treat (NNT) or numbers needed to harm (NNH) foroutcomes where the RR was statistically significant. Treatmenteffects for continuous outcomes include mean differences (MD) and95% CI for single studies or for 2 or more studies with comparableoutcome measures. Standardized mean differences (SMD) and 95%CI were used for data from disparate outcome measures.
Results
Patient selection and characteristics
The search strategy retrieved 266 studies: 31 fromCENTRA, 80 from PubMed, and 155 from EMBASE.After deduplication and examination of the titles andabstracts of these references, 9 studies were identi-fied.3,4,7,11,12,14,16,24,32 A reading of the full text of 5 studiesindicated they were not randomized controlled trials andthey were excluded.3,11,14,16,24 Thus, 4 studies matched ourinclusion criteria (Fig. 1),4,7,12,32 of which 3 were reportedto be randomized controlled trials,4,7,32 and 1 study wasa quasi-randomized controlled trial.12
Sample sizes of the studies ranged from 32 to 111. Fourtrials with 305 clavicle fractures were included in theanalysis. Of those, 157 clavicle fractures were randomized
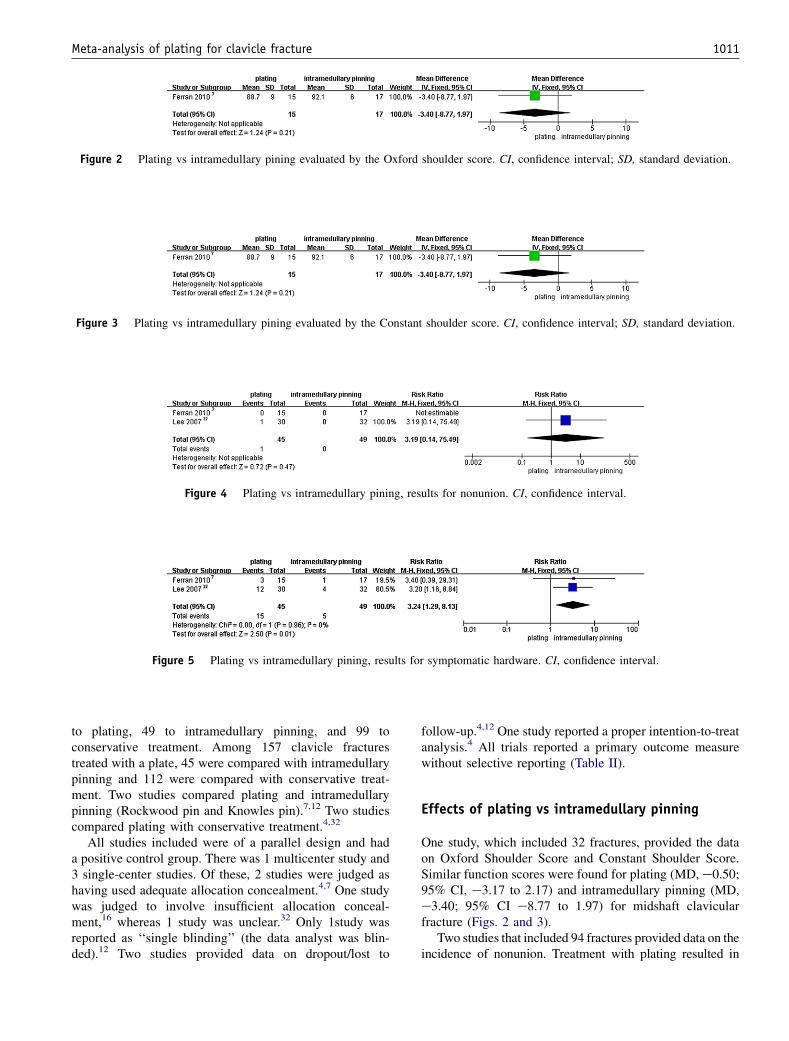
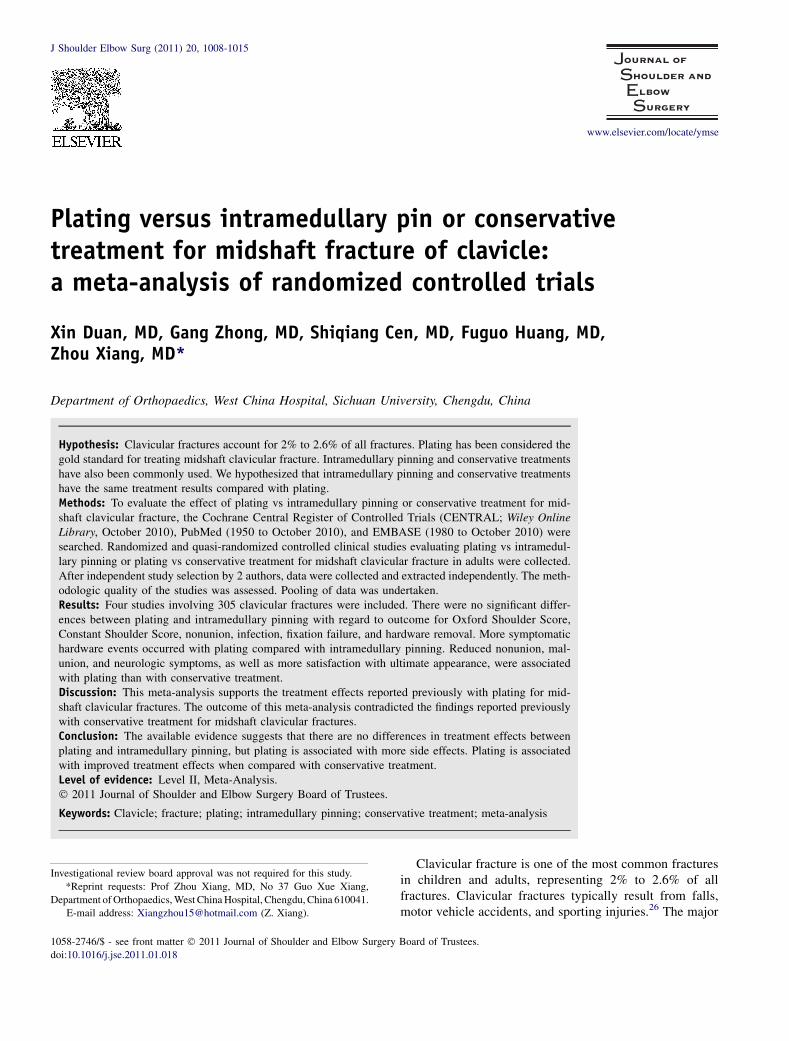
Figure 2 Plating vs intramedullary pining evaluated by the Oxford shoulder score. CI, confidence interval; SD, standard deviation.
Figure 3 Plating vs intramedullary pining evaluated by the Constant shoulder score. CI, confidence interval; SD, standard deviation.
Figure 4 Plating vs intramedullary pining, results for nonunion. CI, confidence interval.
Figure 5 Plating vs intramedullary pining, results for symptomatic hardware. CI, confidence interval.
Meta-analysis of plating for clavicle fracture 1011
to plating, 49 to intramedullary pinning, and 99 toconservative treatment. Among 157 clavicle fracturestreated with a plate, 45 were compared with intramedullarypinning and 112 were compared with conservative treat-ment. Two studies compared plating and intramedullarypinning (Rockwood pin and Knowles pin).7,12 Two studiescompared plating with conservative treatment.4,32
All studies included were of a parallel design and hada positive control group. There was 1 multicenter study and3 single-center studies. Of these, 2 studies were judged ashaving used adequate allocation concealment.4,7 One studywas judged to involve insufficient allocation conceal-ment,16 whereas 1 study was unclear.32 Only 1study wasreported as ‘‘single blinding’’ (the data analyst was blin-ded).12 Two studies provided data on dropout/lost to
follow-up.4,12 One study reported a proper intention-to-treatanalysis.4 All trials reported a primary outcome measurewithout selective reporting (Table II).
Effects of plating vs intramedullary pinning
One study, which included 32 fractures, provided the dataon Oxford Shoulder Score and Constant Shoulder Score.Similar function scores were found for plating (MD, e0.50;95% CI, e3.17 to 2.17) and intramedullary pinning (MD,e3.40; 95% CI e8.77 to 1.97) for midshaft clavicularfracture (Figs. 2 and 3).
Two studies that included 94 fractures provided data on theincidence of nonunion. Treatment with plating resulted in
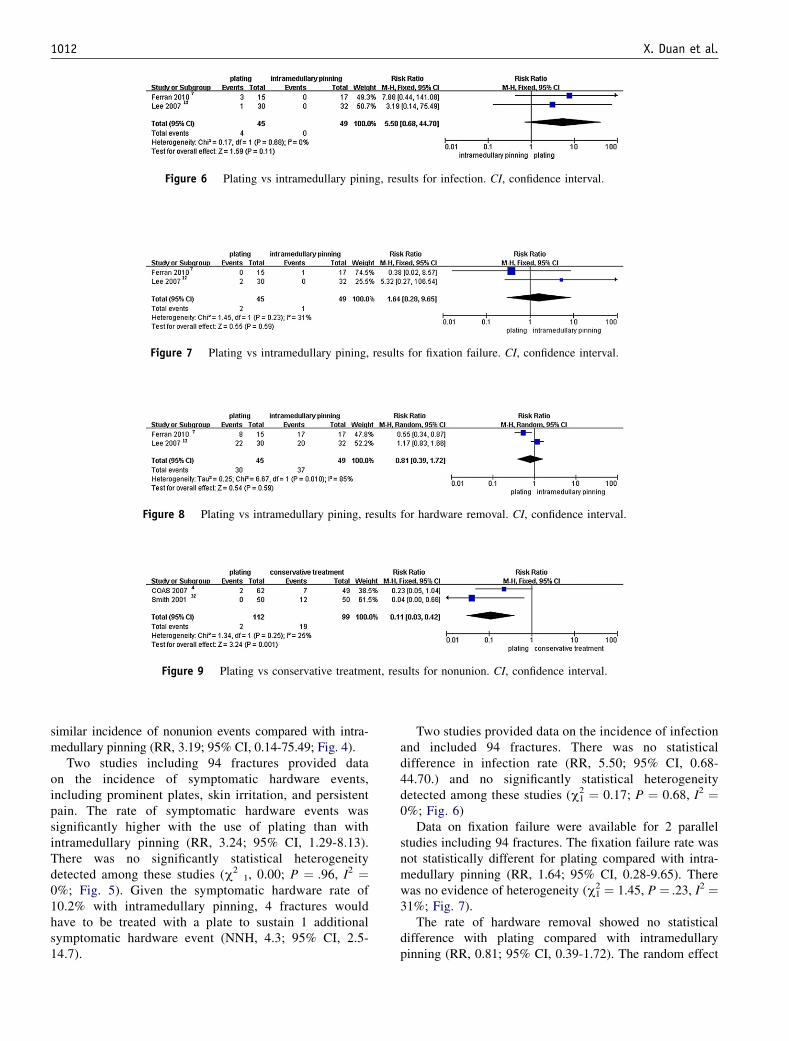
Figure 6 Plating vs intramedullary pining, results for infection. CI, confidence interval.
Figure 7 Plating vs intramedullary pining, results for fixation failure. CI, confidence interval.
Figure 8 Plating vs intramedullary pining, results for hardware removal. CI, confidence interval.
Figure 9 Plating vs conservative treatment, results for nonunion. CI, confidence interval.
1012 X. Duan et al.
similar incidence of nonunion events compared with intra-medullary pinning (RR, 3.19; 95% CI, 0.14-75.49; Fig. 4).
Two studies including 94 fractures provided dataon the incidence of symptomatic hardware events,including prominent plates, skin irritation, and persistentpain. The rate of symptomatic hardware events wassignificantly higher with the use of plating than withintramedullary pinning (RR, 3.24; 95% CI, 1.29-8.13).There was no significantly statistical heterogeneitydetected among these studies (c2
1, 0.00; P ¼ .96, I2 ¼0%; Fig. 5). Given the symptomatic hardware rate of10.2% with intramedullary pinning, 4 fractures wouldhave to be treated with a plate to sustain 1 additionalsymptomatic hardware event (NNH, 4.3; 95% CI, 2.5-14.7).
Two studies provided data on the incidence of infectionand included 94 fractures. There was no statisticaldifference in infection rate (RR, 5.50; 95% CI, 0.68-44.70.) and no significantly statistical heterogeneitydetected among these studies (c2
1 ¼ 0.17; P ¼ 0.68, I2 ¼0%; Fig. 6)
Data on fixation failure were available for 2 parallelstudies including 94 fractures. The fixation failure rate wasnot statistically different for plating compared with intra-medullary pinning (RR, 1.64; 95% CI, 0.28-9.65). Therewas no evidence of heterogeneity (c2
1 ¼ 1.45, P ¼ .23, I2 ¼31%; Fig. 7).
The rate of hardware removal showed no statisticaldifference with plating compared with intramedullarypinning (RR, 0.81; 95% CI, 0.39-1.72). The random effect

Figure 10 Plating vs conservative treatment, results for malunion. CI, confidence interval.
Figure 11 Plating vs conservative treatment, results for neurologic symptoms. CI, confidence interval.
Figure 12 Plating vs conservative treatment, results for satisfaction with appearance. CI, confidence interval.
Meta-analysis of plating for clavicle fracture 1013
model was used because substantial heterogeneity existed(c2
1¼ 6.67, P ¼ .01, I2 ¼ 85%; Fig. 8).
Effects of plating vs conservative treatment
Two studies that included 211 cases provided data onnonunion. Treatment with a plate resulted in lower inci-dence of nonunion compared with conservative treatment(RR, 0.11; 95% CI. 0.03-0.42). No statistically significantheterogeneity was detected among these studies (c2
1 ¼ 1.34,P ¼ .25). Based on union rate of 19.2% with conservativetreatment, 6 fractures would have to be treated with a plateto reduce the number of nonunion cases by 1 (NNT, 5.7;95% CI, 3.9-10.8; Fig. 9).
One study that included 111 cases provided data onmalunion. The malunion rate was significantly lower withthe use of plating compared with conservative treatment(RR, 0.04; 95% CI, 0.00-0.70). The NNT was 5.4 (95% CI,3.4-13.2; Fig. 10).
Two studies reported data on neurologic symptoms,including 211 cases. Fractures receiving plating showedfewer neurologic symptoms than those receiving conser-vative treatment (RR, 0.44; 95% CI, 0.22-0.88). There wasno statistical heterogeneity (c2
1 ¼ 3.96, P ¼ .05, I2 ¼ 75%;Fig. 11).
In 2 studies with 211 patients, there was significantlymore satisfaction with appearance (RR, 1.64; 95% CI, 1.36-1.99). There was no statistically significant heterogeneity(c2
1 ¼ 0.64, P ¼ .42). Based on the 54.5% rate of satis-faction with ultimate cosmetic appearance achieved withconservative treatment, plating would achieve a singleadditional satisfactory result for every 3 fractures treated(NNT, 2.9; 95% CI, 2.3-4.3, I2 ¼ 0%; Fig. 12).
Discussion
This meta-analysis was based on 4 randomized or quasi-randomized studies that included 49 fractures treated withintramedullary pinning, 99 treated conservatively, and 157fractures treatedwith plating. The outcomes investigatedwereshoulder function (Oxford Shoulder Score and ConstantShoulder Score), nonunion, hardware removal, infection, andfixation failure. The outcomes were similar regardless ofwhether plating or intramedullary pinningwas used.However,plating caused more symptomatic hardware events thanintramedullary pinning. Our results demonstrated a lower rateof nonunion, reduced rate of malunion, fewer neurologicsymptoms, and increased satisfaction with cosmetic appear-ance for plating compared with conservative treatment.
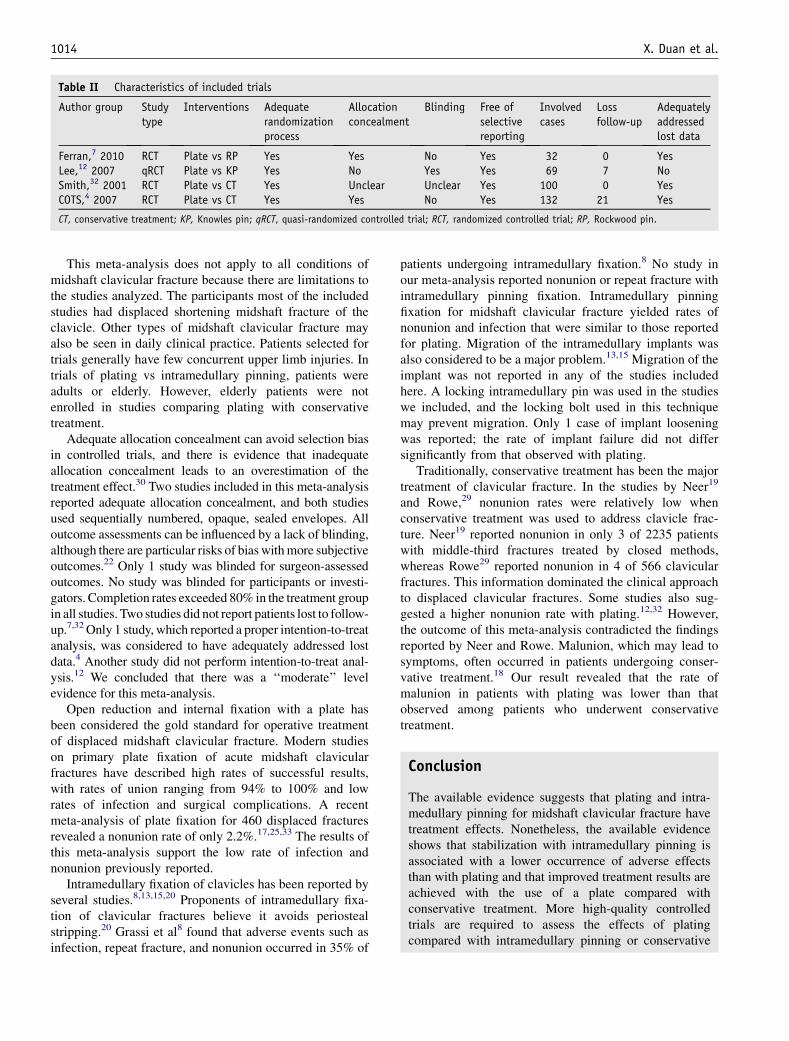
Table II Characteristics of included trials
Author group Studytype
Interventions Adequaterandomizationprocess
Allocationconcealment
Blinding Free ofselectivereporting
Involvedcases
Lossfollow-up
Adequatelyaddressedlost data
Ferran,7 2010 RCT Plate vs RP Yes Yes No Yes 32 0 YesLee,12 2007 qRCT Plate vs KP Yes No Yes Yes 69 7 NoSmith,32 2001 RCT Plate vs CT Yes Unclear Unclear Yes 100 0 YesCOTS,4 2007 RCT Plate vs CT Yes Yes No Yes 132 21 Yes
CT, conservative treatment; KP, Knowles pin; qRCT, quasi-randomized controlled trial; RCT, randomized controlled trial; RP, Rockwood pin.
1014 X. Duan et al.
This meta-analysis does not apply to all conditions ofmidshaft clavicular fracture because there are limitations tothe studies analyzed. The participants most of the includedstudies had displaced shortening midshaft fracture of theclavicle. Other types of midshaft clavicular fracture mayalso be seen in daily clinical practice. Patients selected fortrials generally have few concurrent upper limb injuries. Intrials of plating vs intramedullary pinning, patients wereadults or elderly. However, elderly patients were notenrolled in studies comparing plating with conservativetreatment.
Adequate allocation concealment can avoid selection biasin controlled trials, and there is evidence that inadequateallocation concealment leads to an overestimation of thetreatment effect.30 Two studies included in this meta-analysisreported adequate allocation concealment, and both studiesused sequentially numbered, opaque, sealed envelopes. Alloutcome assessments can be influenced by a lack of blinding,although there are particular risks of bias withmore subjectiveoutcomes.22 Only 1 study was blinded for surgeon-assessedoutcomes. No study was blinded for participants or investi-gators. Completion rates exceeded 80% in the treatment groupin all studies. Two studies did not report patients lost to follow-up.7,32Only 1 study, which reported a proper intention-to-treatanalysis, was considered to have adequately addressed lostdata.4 Another study did not perform intention-to-treat anal-ysis.12 We concluded that there was a ‘‘moderate’’ levelevidence for this meta-analysis.
Open reduction and internal fixation with a plate hasbeen considered the gold standard for operative treatmentof displaced midshaft clavicular fracture. Modern studieson primary plate fixation of acute midshaft clavicularfractures have described high rates of successful results,with rates of union ranging from 94% to 100% and lowrates of infection and surgical complications. A recentmeta-analysis of plate fixation for 460 displaced fracturesrevealed a nonunion rate of only 2.2%.17,25,33 The results ofthis meta-analysis support the low rate of infection andnonunion previously reported.
Intramedullary fixation of clavicles has been reported byseveral studies.8,13,15,20 Proponents of intramedullary fixa-tion of clavicular fractures believe it avoids periostealstripping.20 Grassi et al8 found that adverse events such asinfection, repeat fracture, and nonunion occurred in 35% of
patients undergoing intramedullary fixation.8 No study inour meta-analysis reported nonunion or repeat fracture withintramedullary pinning fixation. Intramedullary pinningfixation for midshaft clavicular fracture yielded rates ofnonunion and infection that were similar to those reportedfor plating. Migration of the intramedullary implants wasalso considered to be a major problem.13,15 Migration of theimplant was not reported in any of the studies includedhere. A locking intramedullary pin was used in the studieswe included, and the locking bolt used in this techniquemay prevent migration. Only 1 case of implant looseningwas reported; the rate of implant failure did not differsignificantly from that observed with plating.
Traditionally, conservative treatment has been the majortreatment of clavicular fracture. In the studies by Neer19
and Rowe,29 nonunion rates were relatively low whenconservative treatment was used to address clavicle frac-ture. Neer19 reported nonunion in only 3 of 2235 patientswith middle-third fractures treated by closed methods,whereas Rowe29 reported nonunion in 4 of 566 clavicularfractures. This information dominated the clinical approachto displaced clavicular fractures. Some studies also sug-gested a higher nonunion rate with plating.12,32 However,the outcome of this meta-analysis contradicted the findingsreported by Neer and Rowe. Malunion, which may lead tosymptoms, often occurred in patients undergoing conser-vative treatment.18 Our result revealed that the rate ofmalunion in patients with plating was lower than thatobserved among patients who underwent conservativetreatment.
Conclusion
The available evidence suggests that plating and intra-medullary pinning for midshaft clavicular fracture havetreatment effects. Nonetheless, the available evidenceshows that stabilization with intramedullary pinning isassociated with a lower occurrence of adverse effectsthan with plating and that improved treatment results areachieved with the use of a plate compared withconservative treatment. More high-quality controlledtrials are required to assess the effects of platingcompared with intramedullary pinning or conservative

Meta-analysis of plating for clavicle fracture 1015
treatment. Future studies should be large and multi-centered, including participants of all ages.
Disclaimer
The authors, their immediate families, and any researchfoundations with which they are affiliated have notreceived any financial payments or other benefits fromany commercial entity related to the subject of thisarticle.
References
1. Boehme D, Curtis RJ Jr, DeHaan JT, Kay SP, Young DC,
Rockwood CA Jr. The treatment of nonunion fractures of the midshaft
of the clavicle with an intramedullary Hagie pin and autogenous bone
graft. Instr Course Lect 1993;42:283-90.
2. Bostman O, Manninen M, Pihlajamaki H. Complications of plate
fixation in fresh displaced midclavicular fractures. J Trauma 1997;43:
778-83.
3. Bravo CJ, Wright CA. Displaced, comminuted diaphyseal clavicle
fracture. J Hand Surg Am 2009;34:1883-5. doi:10.1016/j.jhsa.2009.
10.012
4. Canadian Orthopaedic Trauma Society. Nonoperative treatment
compared with plate fixation of displaced midshaft clavicular frac-
tures. A multicenter, randomized clinical trial. J Bone Joint Surg Am
2007;89:1-10. doi:10.2106/JBJS.F.00020
5. Denard PJ, Koval KJ, Cantu RV, Weinstein JN. Management of
midshaft clavicle fractures in adults. Am J Orthop (Belle Mead NJ)
2005;34:527-36.
6. Duncan SF, Sperling JW, Steinmann S. Infection after clavicle frac-
tures. Clin Orthop Relat Res 2005;439:74-8. doi:10.1097/01.blo.
0000183088.60639.05
7. Ferran NA, Hodgson P, Vannet N, Williams R, Evans RO. Locked
intramedullary fixation vs plating for displaced and shortened mid-
shaft clavicle fractures: a randomized clinical trial. J Shoulder
Elbow Surg 2010;19:783-9. doi:10.1016/j.jse.2010.05.002
8. Grassi FA TM, D’Angelo F. Management of midclavicular fractures:
comparison between conservative treatment and open intramedullary
fixation in 80 patients. J Trauma 2001;50:1096-100.
9. Higgins JP, Green S, editors. Cochrane handbook for systematic
reviews of interventions version 5.0.2 [updated September 2009]. The
Cochrane Collaboration, 2009. www.cochrane-handbook.org. Last
accessed: Feb 20, 2011.
10. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring incon-
sistency in meta-analyses. BMJ 2003;327:557-60. doi:10.1136/bmj.
327.7414.557
11. Jeray KJ. Acute midshaft clavicular fracture. J Am Acad Orthop Surg
2007;15:239-48.
12. Lee Y, Lin C, Huang C, Chen C, Liao W. Operative treatment of
midclavicular fractures in 62 elderly patients: Knowles pin versus
plate. Orthopedics 2007;30:959-64.
13. Leppilahti J, Jalovaara P. Migration of Kirschner wires following
fixation of the clavicleea report of 2 cases. Acta Orthop Scand 1999;
70:517-9.
14. Liu PC, Chien SH, Chen JC, Hsieh CH, Chou PH, Lu CC. Minimally
invasive fixation of displaced midclavicular fractures with titanium
elastic nails. J Orthop Trauma 2010;24:217-23. doi:10.1097/BOT.
0b013e3181b8ba33
15. Lyons FA, Rockwood CA Jr. Migration of pins used in operations on
the shoulder. J Bone Joint Surg Am 1990;72:1262-7.
16. McKee MD. Clavicle fractures in 2010: sling/swathe or open reduc-
tion and internal fixation? Orthop Clin North Am 2010;41:225-31. doi:
10.1016/j.ocl.2009.12.005
17. McKee MD, Seiler JG, Jupiter JB. The application of the limited
contact dynamic compression plate in the upper extremity: an analysis
of 114 consecutive cases. Injury 1995;26:661-6.
18. McKeeMD,WildLM,SchemitschEH.Midshaftmalunionsof the clavicle.
J Bone Joint Surg Am 2003;85:790-7. doi:10.2106/JBJS.H.00034
19. Neer CS 2nd. Nonunion of the clavicle. JAMA 1960;5(172):1006-11.
20. Ngarmukos C, Parkpian V, Patradul A. Fixation of fractures of the
midshaft of the clavicle with Kirschner wires. Results in 108 patients.
J Bone Joint Surg Br 1998;80:106-8.
21. Nordqvist A, Petersson CJ, Redlund-Johnell I. Mid-clavicle fractures
in adults: end result study after conservative treatment. J Orthop
Trauma 1998;12:572-6.
22. Noseworthy JH, Ebers GC, Vandervoort MK, Farquhar RE, Yetisir E,
RobertsR.The impact of blinding on the results of a randomized, placebo-
controlled multiple sclerosis clinical trial. Neurology 1994;44:16-20.
23. Nowak J, Mallmin H, Larsson S. The aetiology and epidemiology of
clavicular fractures. A prospective study during a two-year period in
Uppsala, Sweden. Injury 2000;31:353-8.
24. Pearson AMTA, Koval KJ, McKeeMD, Cantu RV, Bell JE, Vicente M. Is
surgery for displaced, midshaft clavicle fractures in adults cost-effective?
Results based on a multicenter randomized, controlled trial. J Orthop
Trauma 2010;24:426-33. doi:10.1097/BOT.0b013e3181c3e505
25. Poigenfurst J, Rappold G, Fischer W. Plating of fresh clavicular
fractures: results of 122 operations. Injury 1992;23:237-41.
26. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of
clavicle fractures. J Shoulder Elbow Surg 2002;11:452-6. doi:10.1067/
mse.2002.126613
27. Ring D, Holovacs T. Brachial plexus palsy after intramedullary fixa-
tion of a clavicular fracture. A report of three cases. J Bone Joint Surg
Am 2005;87:1834-7. doi:10.2106/JBJS.D.02919
28. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and
classification. J Bone Joint Surg Br 1998;80:476-84.
29. Rowe CR. An atlas of anatomy and treatment of midclavicular frac-
tures. Clin Orthop Relat Res 1968;58:29-42.
30. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of
bias. Dimensions of methodological quality associated with estimates
of treatment effects in controlled trials. JAMA 1995;273:408-12.
31. Shen WJ, Liu TJ, Shen YS. Plate fixation of fresh displaced midshaft
clavicle fractures. Injury 1999;30:497-500.
32. Smith CA RJ, Crosby LA, editor. Results of operative versus non-
operative treatment for 100% displaced mid-shaft clavicle fractures:
a prospective randomized trial. The 68th Annual Meeting of the
American Academy of Orthopaedic Surgeons; 2001.
33. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Treatment of
acute midshaft clavicle fractures: systematic review of 2144 fractures:
on behalf of the Evidence-Based Orthopaedic Trauma Working Group.
J Orthop Trauma 2005;19:504-7. doi:10.1097/01.bot.0000172287.
44278.ef