pathology - research and...
TRANSCRIPT

Contents lists available at ScienceDirect
Pathology - Research and Practice
journal homepage: www.elsevier.com/locate/prp
Original Article
A severe combined immunodeficiency disease mouse model of humanadenocarcinoma with lepidic-predominant growth
Ryota Tanaka1,2,⁎, Keisei Tachibana1,2, Kazuharu Suda1, Haruhiko Kondo1, Masayuki Noguchi2
1 Department of Surgery, Kyorin University School of Medicine, Tokyo, Japan2 Department of Pathology, Institute of Basic Medical Sciences, Graduate School of Comprehensive Human Sciences, University of Tsukuba, Ibaraki, Japan
A R T I C L E I N F O
Key words:SCID mouselung cancerlepidic adenocarcinomaorthotopic implantation
A B S T R A C T
Severe combined immunodeficiency disease (SCID) mice with human lepidic adenocarcinoma were establishedby the intrabronchial implantation of fresh surgically resected specimens. Human pulmonary adenocarcinomatissue from 16 different cases was transplanted into SCID mice, and SCID mouse tumors were established fromfour of these cases (25%). Among the four tumors, the tumor cells of two SCID mice showed replacement lepidicgrowth of mouse alveolar structures accompanied by multiple intrapulmonary lesions. Human lung carcinomacell lines showing lepidic growth are rare and the xenograft models using the SCID mouse model developed inthe current study will be useful for analyzing the growth and/or progression patterns and clinical behavior oflepidic adenocarcinoma, the major histological subtype of human carcinoma of the lung.
1. Introduction
Lung cancer, particularly pulmonary adenocarcinoma, has becomethe leading cause of cancer death in the world, including the UnitedStates and Japan. It is still the general consensus that the poor prognosisof pulmonary adenocarcinoma reflects its aggressive biological natureand the paucity of basic studies on its molecular carcinogenesis. Usefulin vitro and in vivo models that imitate the histological and clinicalcharacteristics of this tumor are necessary to determine the molecularmechanisms of pulmonary adenocarcinogenesis.
The conceptual validity of orthotopic models was first suggested byPaget in 1889 [1]. The organ site-specific implantation of tumor cells isessential for achieving optimal tumor growth and progression in vivo.This idea is widely supported by numerous studies using various tumormodels including lung cancer. In a previous study, the biologicalcharacteristics of representative human pulmonary adenocarcinomacell lines were investigated using the intrabronchial orthotopic propa-gation method [2]. However, existing lung cancer cell lines were es-tablished by in vitro culture or from subcutaneous xenografts. Thesedevelop into tumors in nude mice or mice with severe combined im-munodeficiency disease (SCID); however, the tumors are all moderatelyor poorly differentiated adenocarcinoma and do not mimic the basiccharacteristics of pulmonary adenocarcinoma, namely lepidic (pre-viously called bronchioloalveolar) spread.
The purpose of this study was to establish a xenograft model using
SCID mice that recapitulates the histopathological characteristics of theoriginal human lung tumor.
2. Materials and methods
2.1. Patient samples
Surgically resected tissue from 16 patients with pulmonary adeno-carcinoma who attended the University Hospital of Tsukuba (Ibaraki,Japan) or Ibaraki Prefectural Central Hospital (Ibaraki, Japan) was usedin this study. Histologically, the tumor specimens included 14 adeno-carcinomas with subtypes of lepidic (n= 2), acinar (n= 4), papillary(n= 3), micropapillary (n=1) and solid (n=4), and 1 case each ofinvasive mucinous adenocarcinoma and fetal adenocarcinoma [3]. Thepathological stages were T1aN0M0 (n=1), T1cN0M0 (n=1),T2aN0M0 (n= 3), T2bN0M0 (n= 1), T2N1M0 (n=1), T3N0M0(n= 2), T1cN2M0 (n=2), T2aN2M0 (n=1), T2bN2M0 (n=1),T4N0M0 (n=1) and T2bN0M1b (n= 2) [4]. This study was approvedby the Regional Committee for Medical Research Ethics (University ofTsukuba and Ibaraki Prefectural Central Hospital). All patients gavetheir informed consent before sample collection, in accordance with theinstitutional guidelines.
https://doi.org/10.1016/j.prp.2018.09.021Received 13 July 2018; Received in revised form 1 September 2018; Accepted 26 September 2018
⁎ Corresponding author at: Department of Surgery, Kyorin University School of Medicine, 6-20-2, Shinkawa, Mitaka-shi, Tokyo, 181-8611, Japan.E-mail address: [email protected] (R. Tanaka).
Pathology - Research and Practice xxx (xxxx) xxx–xxx
0344-0338/ © 2018 Elsevier GmbH. All rights reserved.
Please cite this article as: Tanaka, R., Pathology - Research and Practice, https://doi.org/10.1016/j.prp.2018.09.021
2.2. Experimental animals
Five-week-old female SCID mice, with a CB-17 genetic background,were obtained from CLEA Japan, Inc. (Tokyo, Japan). The mice werefree of known pathogens at the time of the study, and were housed insterilized filter-topped cages with ad libitum access to autoclaved foodand water. The animal experiments were carried out humanely afterreceiving approval from the Institutional Animal ExperimentCommittee of the University of Tsukuba and were in accordance withthe Regulations for Animal Experiments of our university and theFundamental Guidelines for Proper Conduct of Animal Experiments.
2.3. Fresh tumor cell implantation and histopathological studies
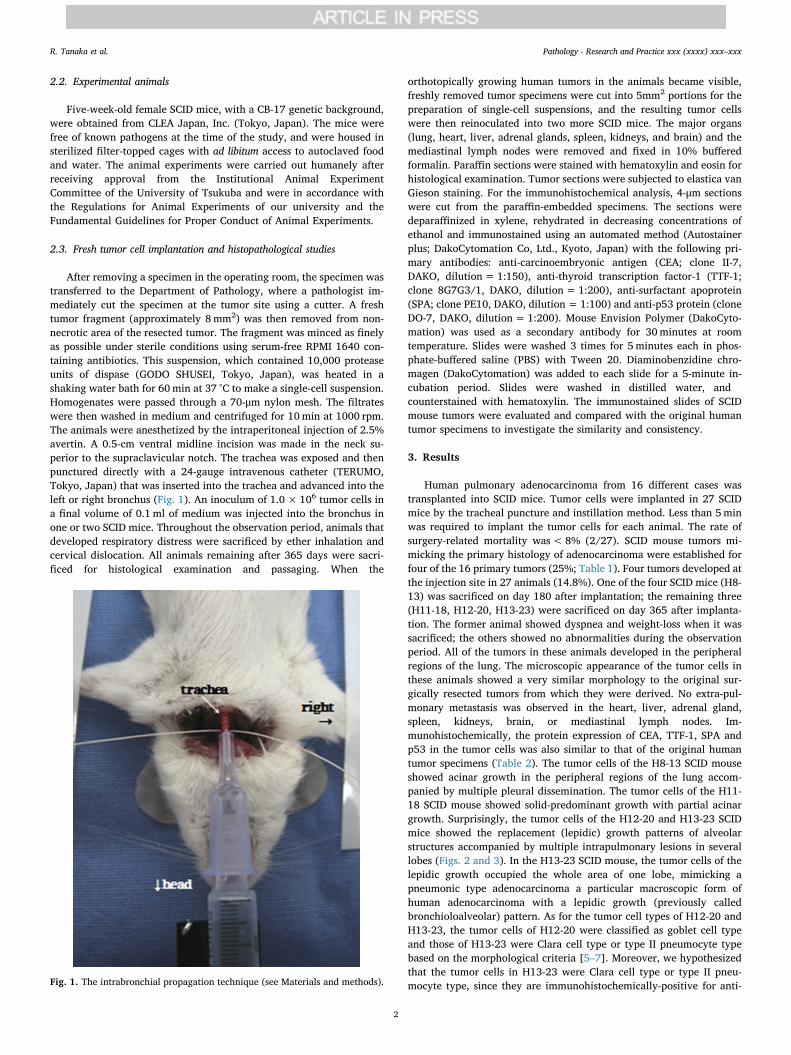
After removing a specimen in the operating room, the specimen wastransferred to the Department of Pathology, where a pathologist im-mediately cut the specimen at the tumor site using a cutter. A freshtumor fragment (approximately 8mm2) was then removed from non-necrotic area of the resected tumor. The fragment was minced as finelyas possible under sterile conditions using serum-free RPMI 1640 con-taining antibiotics. This suspension, which contained 10,000 proteaseunits of dispase (GODO SHUSEI, Tokyo, Japan), was heated in ashaking water bath for 60min at 37 °C to make a single-cell suspension.Homogenates were passed through a 70-μm nylon mesh. The filtrateswere then washed in medium and centrifuged for 10min at 1000 rpm.The animals were anesthetized by the intraperitoneal injection of 2.5%avertin. A 0.5-cm ventral midline incision was made in the neck su-perior to the supraclavicular notch. The trachea was exposed and thenpunctured directly with a 24-gauge intravenous catheter (TERUMO,Tokyo, Japan) that was inserted into the trachea and advanced into theleft or right bronchus (Fig. 1). An inoculum of 1.0×106 tumor cells ina final volume of 0.1ml of medium was injected into the bronchus inone or two SCID mice. Throughout the observation period, animals thatdeveloped respiratory distress were sacrificed by ether inhalation andcervical dislocation. All animals remaining after 365 days were sacri-ficed for histological examination and passaging. When the
orthotopically growing human tumors in the animals became visible,freshly removed tumor specimens were cut into 5mm2 portions for thepreparation of single-cell suspensions, and the resulting tumor cellswere then reinoculated into two more SCID mice. The major organs(lung, heart, liver, adrenal glands, spleen, kidneys, and brain) and themediastinal lymph nodes were removed and fixed in 10% bufferedformalin. Paraffin sections were stained with hematoxylin and eosin forhistological examination. Tumor sections were subjected to elastica vanGieson staining. For the immunohistochemical analysis, 4-μm sectionswere cut from the paraffin-embedded specimens. The sections weredeparaffinized in xylene, rehydrated in decreasing concentrations ofethanol and immunostained using an automated method (Autostainerplus; DakoCytomation Co, Ltd., Kyoto, Japan) with the following pri-mary antibodies: anti-carcinoembryonic antigen (CEA; clone II-7,DAKO, dilution=1:150), anti-thyroid transcription factor-1 (TTF-1;clone 8G7G3/1, DAKO, dilution= 1:200), anti-surfactant apoprotein(SPA; clone PE10, DAKO, dilution= 1:100) and anti-p53 protein (cloneDO-7, DAKO, dilution= 1:200). Mouse Envision Polymer (DakoCyto-mation) was used as a secondary antibody for 30minutes at roomtemperature. Slides were washed 3 times for 5minutes each in phos-phate-buffered saline (PBS) with Tween 20. Diaminobenzidine chro-magen (DakoCytomation) was added to each slide for a 5-minute in-cubation period. Slides were washed in distilled water, and counterstained with hematoxylin. The immunostained slides of SCIDmouse tumors were evaluated and compared with the original humantumor specimens to investigate the similarity and consistency.
3. Results
Human pulmonary adenocarcinoma from 16 different cases wastransplanted into SCID mice. Tumor cells were implanted in 27 SCIDmice by the tracheal puncture and instillation method. Less than 5minwas required to implant the tumor cells for each animal. The rate ofsurgery-related mortality was<8% (2/27). SCID mouse tumors mi-micking the primary histology of adenocarcinoma were established forfour of the 16 primary tumors (25%; Table 1). Four tumors developed atthe injection site in 27 animals (14.8%). One of the four SCID mice (H8-13) was sacrificed on day 180 after implantation; the remaining three(H11-18, H12-20, H13-23) were sacrificed on day 365 after implanta-tion. The former animal showed dyspnea and weight-loss when it wassacrificed; the others showed no abnormalities during the observationperiod. All of the tumors in these animals developed in the peripheralregions of the lung. The microscopic appearance of the tumor cells inthese animals showed a very similar morphology to the original sur-gically resected tumors from which they were derived. No extra-pul-monary metastasis was observed in the heart, liver, adrenal gland,spleen, kidneys, brain, or mediastinal lymph nodes. Im-munohistochemically, the protein expression of CEA, TTF-1, SPA andp53 in the tumor cells was also similar to that of the original humantumor specimens (Table 2). The tumor cells of the H8-13 SCID mouseshowed acinar growth in the peripheral regions of the lung accom-panied by multiple pleural dissemination. The tumor cells of the H11-18 SCID mouse showed solid-predominant growth with partial acinargrowth. Surprisingly, the tumor cells of the H12-20 and H13-23 SCIDmice showed the replacement (lepidic) growth patterns of alveolarstructures accompanied by multiple intrapulmonary lesions in severallobes (Figs. 2 and 3). In the H13-23 SCID mouse, the tumor cells of thelepidic growth occupied the whole area of one lobe, mimicking apneumonic type adenocarcinoma a particular macroscopic form ofhuman adenocarcinoma with a lepidic growth (previously calledbronchioloalveolar) pattern. As for the tumor cell types of H12-20 andH13-23, the tumor cells of H12-20 were classified as goblet cell typeand those of H13-23 were Clara cell type or type II pneumocyte typebased on the morphological criteria [5–7]. Moreover, we hypothesizedthat the tumor cells in H13-23 were Clara cell type or type II pneu-mocyte type, since they are immunohistochemically-positive for anti-Fig. 1. The intrabronchial propagation technique (see Materials and methods).
R. Tanaka et al. Pathology - Research and Practice xxx (xxxx) xxx–xxx
2

TTF-1 antibody, which is a relatively specific marker for a Clara celltype or a type II pneumocyte type [8]. Moreover, the tumors that werepropagated in animals H12-20 and H13-23 were remarkably similar tothe lepidic adenocarcinoma component of the original human tumor.Staining of elastic fibers showed that tumor growth replaced the pul-monary alveolar structures of the mouse (lepidic growth) (Fig. 3E). Thetumors did not show stromal vascular or pleural invasion. The SCIDmouse tumors were diagnosed as lepidic adenocarcinoma.
4. Discussion
For many years, implantation of subcutaneous xenografts has been astandard method for establishing animal tumors for human cancer re-search. Although such tumors have helped us to understand the biolo-gical nature of human cancer, they do not truly represent the histolo-gical characteristics of human cancer [9]. Many previous reports havesuggested that the organ site-specific microenvironment is an importantfactor for the growth of implanted human cancer cells in im-munodeficient animals [10,11].
In this study, the orthotopic implantation method was modified forhuman pulmonary adenocarcinoma of the peripheral regions using thelungs of SCID mice. Tumor cells from two of the four human cases were
successfully implanted in SCID mice and developed into lepidic ade-nocarcinoma in the SCID mouse lung. It is very interesting that the twoSCID mouse tumors showed lepidic growth, while the original tumorsincluded an acinar component beside a lepidic component. We hy-pothesized that the method of orthotopic implantation influenced thetumorigenicity of the lepidic and acinar components. When adeno-carcinomas developing in the peripheral lung tissue are subdivided intotwo groups showing lepidic or non-lepidic growth, approximately 75%of tumors are considered to show total or partial lepidic growth of pure“bronchioloalveolar carcinoma (previously called BAC [12])” or “ade-nocarcinoma of mixed subtype with a BAC component” [13]. It istherefore extremely important to understand the growth and/or pro-gression patterns and the molecular carcinogenesis of lepidic growthadenocarcinoma. However, to date there have been no reports onhuman lung cancer cell lines that show lepidic growth. This method oforthotopic implantation using SCID mice allows us to develop cell linesshowing lepidic growth, which is the main characteristic of peripheraltype lung carcinoma. Some limitations associated with the presentstudy warrant mention. First, lepidic pulmonary adenocarcinoma showsa gradient of atypia, with milder atypia in the peripheral region than inthe central region. However, the tumor cells in the xenograft mono-tonously spread over the alveolar walls, in the same manner as that
Table 1Clinicopathological features of original human tumors and growth patterns of SCID mouse tumors
Case SCID Number of i.p. lesion e
Number Differentiation Histological subtype a pTNM Diameter b Number Day c Growth pattern Diameter d
H8 G2 Acinar (+papillary) T2bN0M1a 43 mm 13 180 Acinar 4 mm 3H11 G2 Solid (+Acinar) T1cN2M0 27 mm 18 365 Solid (+Acinar) 9 mm 1H12 G1 Invasive mucinous T1cN0M0 29 mm 20 365 Lepidic (mucinous) 2 mm 6H13 G1 Acinar (Lepidic) T3(pm1)N0M0 37 mm 23 365 Lepidic (non-mucinous) 10 mm 16
SCID, severe combined immunodeficiency disease; G1, well differentiated; G2, moderately differentiated; pm1, separate tumor nodules in the same lobe as theprimary tumor.
a Histological subtype is based on the new WHO classification [3]. (+ Subtype) indicates a non-predominant histological component.b The maximum diameter of the main tumor in a given case.c The day that an animal was sacrificed after the implantation.d The maximum diameter of the main tumor in a SCID mouse.e The number of intrapulmonary lesions, including the main tumor.
Table 2Immunohistochemical analyses of the protein expressions in original human tumors and SCID mouse tumors.
Case number H8 H11 H12 H13
IHC Original SCID(H8-13)
Original SCID(H11-18)
Original SCID(H12-20)
Original SCID(H13-23)
CEA ± - + + - - - -TTF-1 + + + + - - + +SPA ± + ± + - - + +p53 protein + + - - + + - -
SCID, severe combined immunodeficiency disease; IHC, immunohistochemical staining; CEA, carcinoembryonic antigen; TTF-1, thyroid transcription factor-1; SPA,surfactant apoprotein; +, positive; -, negative;± , including some part of areas with none of tumor cells with positive.
Fig. 2. The microscopic appearance of (A) the original tumor(H & E staining, × 200), and (B) the H12-20 SCID mousetumor (H & E staining, × 200). (A) The tumor cells of theoriginal tumor resembled bronchial epithelial cells with gobletcell-like morphology and showed lepidic spread. (B) The H12-20 tumor cells also showed goblet cell-like morphology andlepidic spread.
R. Tanaka et al. Pathology - Research and Practice xxx (xxxx) xxx–xxx
3

observed in H13-23 SCID mouse tumor. Tumor cells of the SCID mousemodels might be characterized as a metastatic tumor with alveolarspreading similar to a micropapillary subtype with a malignant poten-tial against lepidic adenocarcinoma. Second, there were only two le-pidic adenocarcinomas in the resected specimens, and none of thetumor cells were established in the SCID mouse investigated in thisstudy. In a future study, to establish tumor cells with mild atypia oflepidic adenocarcinoma, many lepidic adenocarcinoma cells obtainedfrom original human specimens may be required to establish cellswhich mimic human lepidic adenocarcinoma in the SCID mouse.
5. Conclusions
SCID mouse models with human pulmonary adenocarcinoma tu-mors showing lepidic spread were established using an orthotopic in-trabronchial implantation method. The method provides a useful modelof lepidic carcinoma, the major histological type of human lung cancer.
Conflict of interest
The authors declare no conflicts of interest in association with thepresent study. This research did not receive any specific grant fromfunding agencies in the public, commercial, or not-for-profit sectors.
References
[1] S. Paget, Secondary growths in cancer of the breast, Lancet 1 (1889) 571–573.[2] K. Mase, T. Iijima, N. Nakamura, T. Takeuchi, M. Onizuka, T. Mitsui, M. Noguchi,
Intrabronchial orthotopic propagation of human lung adenocarcinoma-character-izations of tumorigenicity, invasion and metastasis, Lung Cancer 36 (2002)
271–276.[3] W.D. Travis, E. Brambilla, A.P. Burke, A. Marx, Nicholson AG, WHO Classification
of Tumours of the Lung, Pleura, Thymus and Heart, fourth ed., IARC Press, Lyon,France, 2015.
[4] P. Goldstraw, K. Chansky, J. Crowley, R. Rami-Porta, H. Asamura, W.E. Eberhardt,A.G. Nicholson, P. Groome, A. Mitchell, V. Bolejack, The IASLC Lung CancerStaging Project: Proposals for Revision of the TNM Stage Groupings in theForthcoming (Eighth) Edition of the TNM Classification for Lung Cancer, J ThoracOncol. 11 (2016) 39–51.
[5] Y. Kimula, A histochemical and ultrastructural study of adenocarcinoma of thelung, Am. J. Surg. Pathol. 2 (1978) 253–264.
[6] Y. Shimosato, M. Noguchi, Pulmonary neoplasms, in: S.E. Mills (Ed.),Sternberg’diagnostic surgical pathology, 4th edition, Lippincott Williams & WilkinsInc., Philadelphia, 2004, pp. 1173–1222.
[7] R. Tanaka, Y. Nakazato, H. Horikoshi, S. Tsuchida, T. Yoshida, Y. Nakazato,K. Tachibana, H. Kondo, T. Goya, Diffusion-weighted imaging and positron emis-sion tomography in various cytological subtypes of primary lung adenocarcinoma,Clinical Imaging 37 (2013) 876–883.
[8] A.M. Maeshima, M. Omatsu, K. Tsuta, H. Asamura, Y. Matsuno,Immunohistochemical expression of TTF-1 in various cytological subtypes of pri-mary lung adenocarcinoma, with special reference to intratumoral heterogeneity,Pathology International 58 (2008) 31–37.
[9] F. Toshiharu, F. Xinyu, K. Tetsuro, W. Masahiko, K. Masaki, M.H. Robert, Nudemouse metastatic models of human stomach cancer constructed using orthotopicimplantation of histologically intact tissue, Cancer Res. 53 (1993) 1204–1208.
[10] T.L. McLemore, M.C. Liu, P.C. Blacker, M. Gregg, M.C. Alley, B.J. Abbott,R.H. Shoemaker, M.E. Bohlman, C.C. Litterst, W.C. Hubbard, R.H. Brennan,J.B. McMahon, D.L. Fine, J.C. Eggleston, J.G. Mayo, Novel intrapulmonary modelfor orthotopic propagation of human lung cancers in athymic nude mice, CancerRes. 47 (1987) 5132–5140.
[11] C. Manzotti, R.A. Audisio, G. Pratesi, Importance of orthotopic implantation forhuman tumors as model systems: relevance to metastasis and invasion, Clin. Exp.Metastasis. 11 (1993) 5–14.
[12] W.D. Travis, T.V. Colby, B. Corrin, Y. Shimosato, E. Brambilla, Histological typingof lung and pleural tumours, Springer Verlag Inc., Berlin, 1999.
[13] M. Noguchi, A. Morikawa, M. Kawasaki, Y. Matsuno, T. Yamada, S. Hirohashi,H. Kondo, Y. Shimosato, Small adenocarcinoma of the lung - histologic character-istics and prognosis, Cancer 75 (1995) 2844–2852.
Fig. 3. The macroscopic and microscopic appearance of (A)the original tumor (H & E staining, × 200) and (B, C, D, E)H13-23 SCID mouse tumor (C: H & E staining, × 100; D: H & Estaining, × 200; E: elastica van Gieson staining, × 200). (A)The original tumor cells resembled type II pneumocytes andshowed lepidic spread. (B) The H13-23 tumor cells occupiedthe whole lobe of an SCID mouse lung, mimicked the originaltumor cells and showed lepidic spread (C, D), along the fra-mework (elastic fiber: arrow) of the mouse alveolar structure(E).
R. Tanaka et al. Pathology - Research and Practice xxx (xxxx) xxx–xxx
4