mackenzie lind, epid 624 presentation, 3/30/15. affects 52.5 million adults in the us (includes...
TRANSCRIPT

Rheumatoid arthritis, osteoarthritis, and traumatic arthritis
Mackenzie Lind, EPID 624 Presentation, 3/30/15

Arthritis: Prevalence/Basic Epidemiology
Affects 52.5 million adults in the US (includes rheumatoid arthritis, gout, lupus, other arthritis, fibromyalgia) Projected to increase to 67 million by 2030
22.7% of adults- arthritis diagnosed by a doctor Jumps to ~30% for age 45-64 and ~50% for adults >
65 Most common cause of disability among US
adults!!! Many have activity limitations, work limitations, and
report lower quality of life Costs: 128 billion dollars (2003)
http://www.cdc.gov/arthritis/data_statistics/arthritis_related_stats.htm

Arthritis: Prevalene
http://www.terraclouds.com/images/Global-Arthritis-Statistics.gif

Arthritis: Prevalence
http://www.cdc.gov/arthritis/data_statistics/race.htm

Arthritis: Disability
http://www.cdc.gov/arthritis/data_statistics/national-statistics.html
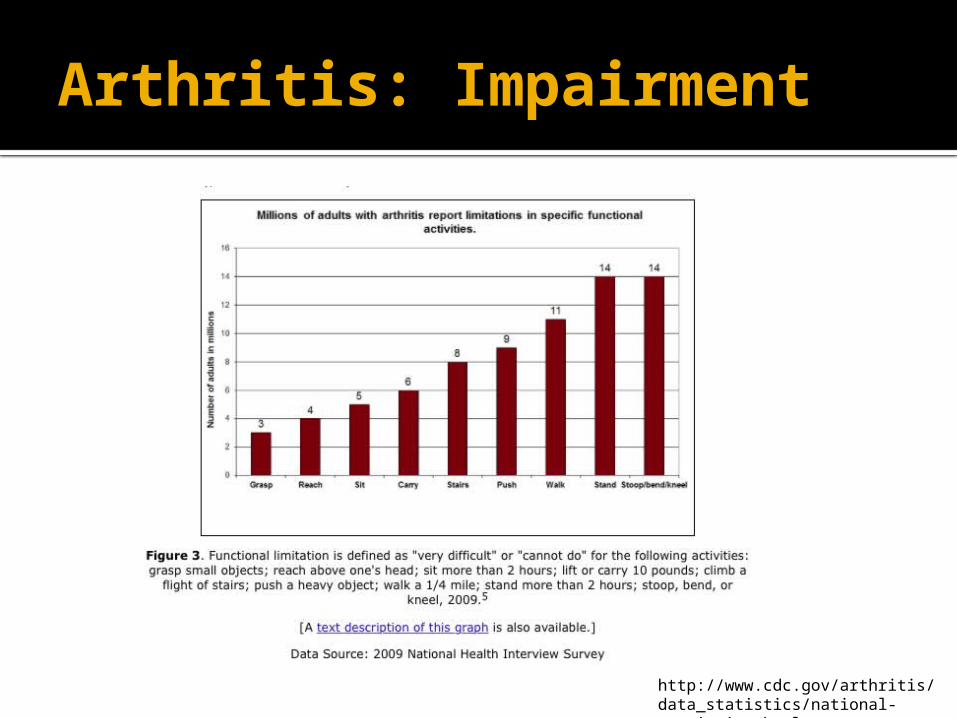
Arthritis: Impairment
http://www.cdc.gov/arthritis/data_statistics/national-statistics.html

Arthritis: Cost
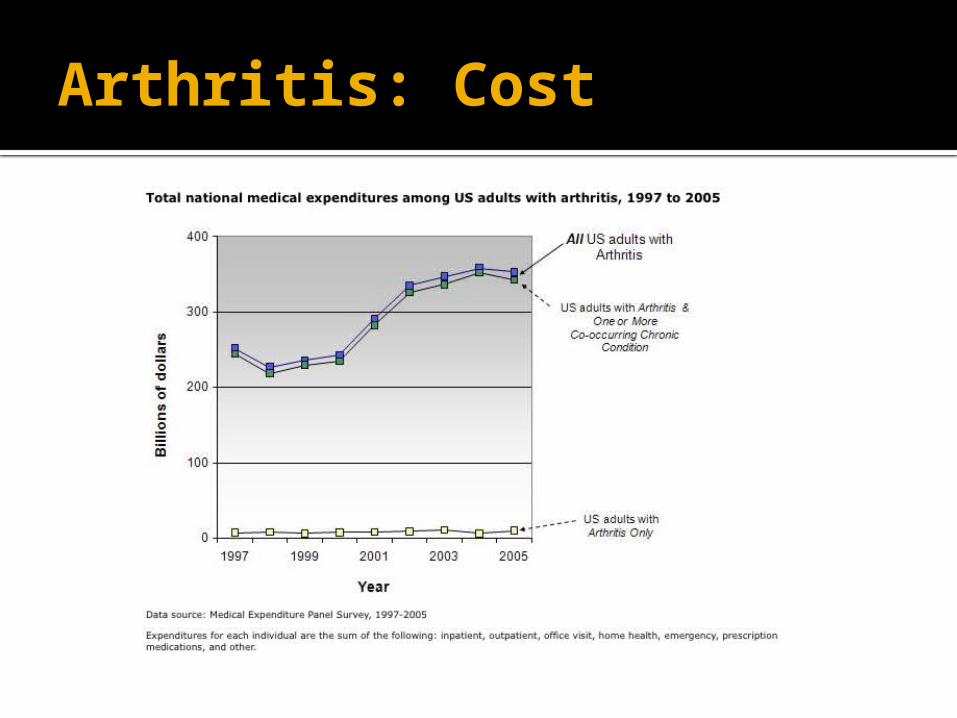
Arthritis: Cost

Arthritis: Comorbidities
http://www.cdc.gov/arthritis/data_statistics/comorbidities.htm
Rheumatoid arthritis (RA) Chronic systemic inflammatory disease Autoimmune Cause is mostly unknown, but thought to
be due to the presence of specific antibodies Antibodies to rheumatoid factor (RF), anti-
citrullinated protein antibodies (ACPA) Key features: Synovitis -> pannus
formation (thick layer of granulation tissue, releases inflammatory cytokines) -> destruction of cartilage and bone
Information from Sattar HA, Fundamentals of Pathology, 2011

RA: Pathophysiology
http://www.medical-artist.com/assets/images/Stages-of-rheumatoid-arthritis.jpg

RA: Clinical presentation
Arthritis Stiffness in the morning, improves with activity, as day
continues Symmetric involvement of joints, polyarthritis▪ Commonly the PIP joints (fingers), wrists, elbows, ankles
knees (in contrast to osteoarthritis) Systemic symptoms (e.g. fever, weight loss,
muscle pain) Rheumatoid nodules Vasculitis Baker cyst (in knee) Also: Pleural effusions, lung fibrosis,
lymphadenopathyInformation from Sattar HA, Fundamentals of Pathology, 2011

RA: Basic Epidemiology
1.5 million adults with RA (2007) 75% women! Most commonly occurs in middle age (40-60),
onset=highest in 60s Population prevalence: 0.5-1% Lifetime risk: 4% (women), 3% (men) Incidence: 41/100,000 Increased mortality in RA (2.3x)
higher in individuals with ACP and RF antibodies 40% of deaths due to heart disease
Individuals with RA have increased risk for depression, 1.7x greater (Lin et al. 2015)Information from Sattar HA, Fundamentals of Pathology, 2011
American College of Rheumatology fact sheethttp://www.cdc.gov/arthritis/data_statistics/arthritis_related_stats.htm

RA: Epidemiology
RA=19th most common for years lost to disability
Individuals with RA report more loss of function, worse functional status (even more than OA),worse quality of life
RA accounts for ~22% of all arthritis-related deaths
Costs: $2785/year (US 2000) (more than OA) Lifetime $61,000-122,00 (US 1995)
http://www.cdc.gov/arthritis/basics/rheumatoid.htm
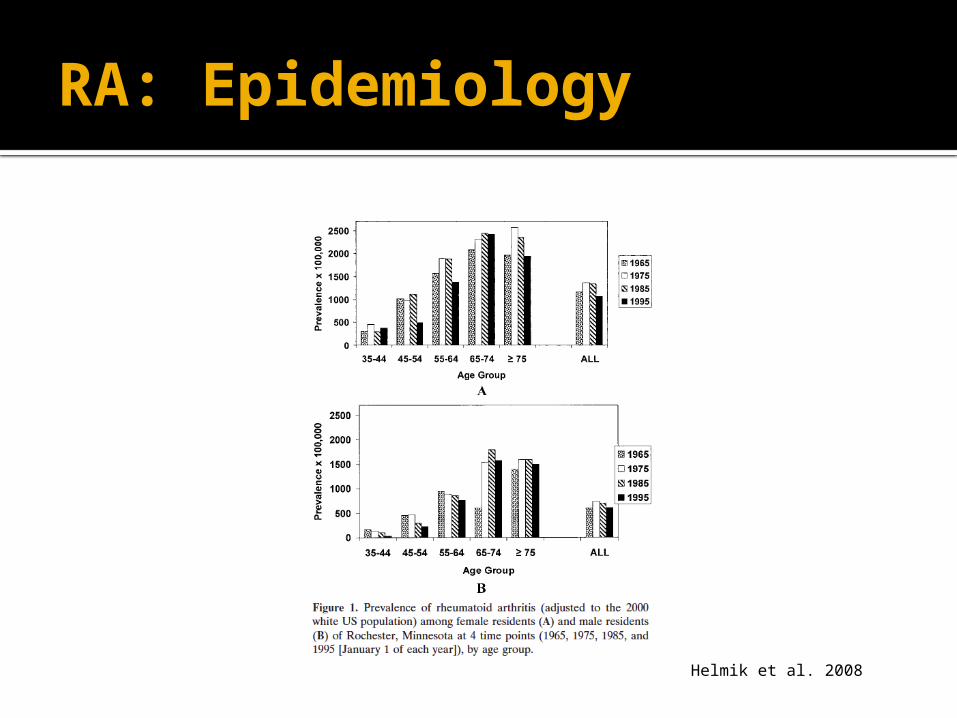
RA: Epidemiology
Helmik et al. 2008
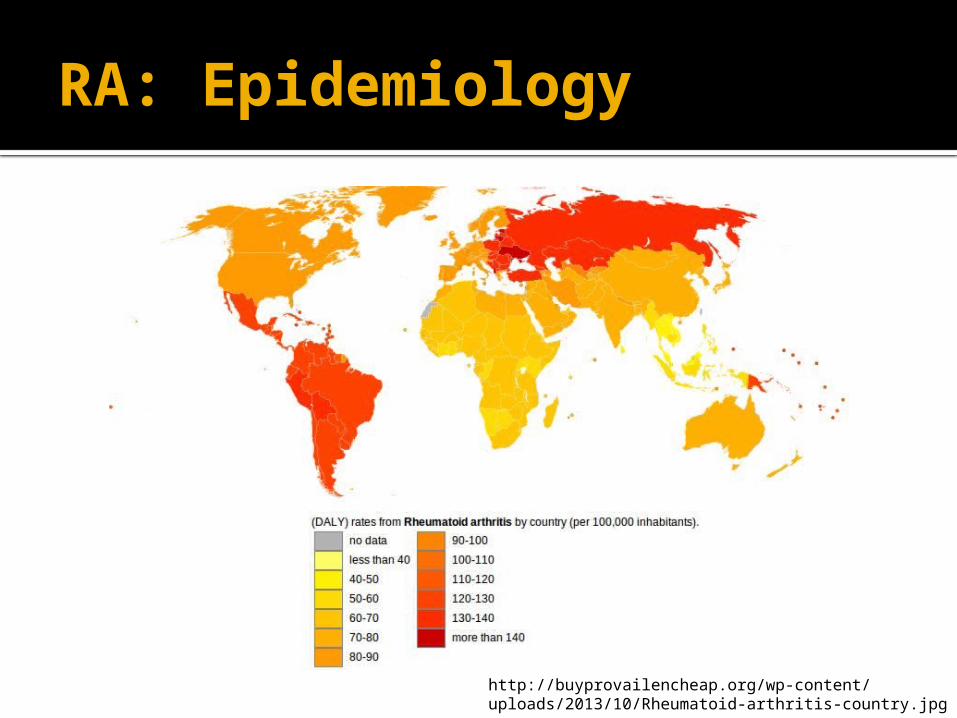
RA: Epidemiology
http://buyprovailencheap.org/wp-content/uploads/2013/10/Rheumatoid-arthritis-country.jpg

RA: Genetics
RA is heritable Estimate from twin and family studies is ~60% due to additive
genetic effects (Frisell et al. 2013, MacGregor et al. 2000, van der Woude et al. 2009)
Identification of specific genes that confer risk First genes were in the Human Leukocyte Antigen (HLA) group
of the Major Histocompatibility Complex (MHC) (Kochi, Suzuki, & Yamamoto 2014)
Most well known= HLADR-4, HLADRB-1 Many others, also involved in immunological functions: PTPN4,
CTLA-4, PADI4, MIF (Orozco, Rueda, & Martin, 2006)
Genome-Wide Association Studies (GWAS) have identified 101 risk loci for RA (Kochi, Suzuki, & Yamamoto 2014)
Also, some genetic overlap with other autoimmune disorders as well as chronic diseases (psoriatric arthrtis, cancer, diabetes, heard disease)
RA: Environmental risk factors Smoking *Most widely accepted*
Accounts for 1 of every 6 new cases of RA▪ Also have gene x environment interactions (complex)
1.3-2.4x increased risk to develop arthritis Relationship is most significant among individuals with the
ACPA antibody Other air pollutants
Occupation exposures, silica Reproductive
Oral contraceptives, breast feeding (decreased risks) Alcohol
Moderate amounts protective Socioeconomic status
Will discuss more at the end!Hoovestol and Mikuls, 2011

RA: Prevention
Primary prevention: This is challenging for RA, since genetics
play a significant role but many specific RFs are unknown
Don’t smoke Secondary prevention??? Tertiary prevention
Medication to control/delay the progression of the disease

RA: Treatment
NSAIDs and corticosteroids Disease-modifying anti-rheumatoid
drugs (DMARDs) [non-biologic] Biologic drugs: e.g. anti-TNF alpha
drugs (adalimumab, infliximab, etanercept)
Also PT and OT
http://www.cdc.gov/arthritis/basics/rheumatoid.htm

Osteoarthritis (OA)
Most common! Also known as degenerative joint
disease Generally develops after age 40 Cause unknown
“wear and tear” Defined by changes on radiography
as well as symptoms (pain/swelling)
Information from Sattar HA, Fundamentals of Pathology, 2011

OA: Clinical Presentation
Arthritis Joint stiffness in the morning, gets worse
throughout the day Oligoarticular Knees, hips, lumbar spine, distal interphalangeal
joints (DIPs), proximal interphalangeal joints (PIPs) Progression: disruption of cartilage,
eburnation- bone on bone, osteophytes (bony growths) can form, often in fingers (Heberden nodes in DIPs, Bouchard nodes in PIPs)
Information from Sattar HA, Fundamentals of Pathology, 2011

OA: Pathology
http://arthro.wpengine.netdna-cdn.com/wp-content/uploads/2014/01/image001-1.jpg

OA: Pathology
http://img.webmd.com/dtmcms/live/webmd/consumer_assets/site_images/media/medical/hw/h9991469_003.jpg
http://upload.wikimedia.org/wikipedia/commons/9/9c/Heberden-Arthrose.JPG

OA: Epidemiology
Affects 27 million Americans >25 y/o (Lawrence et al. 2008)
<50 y/o- more common in men, then switches to women
13.9% (25 or older), 33.6% (65 or older)
Approximately 1 in 2 people develop OA in knee by age 85
For obese individuals: 2/3 risk of lifetime knee OA
1 in 4 develop hip OA
http://www.niams.nih.gov/Health_Info/Osteoarthritis/default.asp
http://www.cdc.gov/arthritis/basics/osteoarthritis.htm

OA: Disease Impact
Increased mortality (~2x) But only ~6% of all arthritis deaths Significant effect on quality of life
Knee OA among top 5 leading causes of disability in adults
High in DALYs and YLDs 80% of patients with OA have limitations to movement Poor health, lost work
70% of all arthritis hospitalizations! Cost: in part due to high cost of surgery
28.5 billion (knee replacements), 13.7 billion (hip) 13 million in job-related costs
http://www.cdc.gov/arthritis/basics/osteoarthritis.htm

OA: Risk factors
Age Trauma (joint injury),
overuse/repetitive use Occupational
Construction, cleaning…hard labor Obesity (for knee especially)
Excess pressure on joints Certain deformities *Hand RA=risk for knee RA
http://www.rheumatology.org/Practice/Clinical/Patients/Diseases_And_Conditions/Osteoarthritis/

OA: Genetics
Genetic contributions to OA Heritability estimated at 35-65% Genes implicated:
Collagen genes (joint structure) for early onset▪ E.g. COL11A1/A2, Col1A1
Immune system▪ Interleukins, e.g. IL-1, IL-6, IL-4
Estrogen (women)▪ Estrogen receptor
Vitamin D▪ Vitamin D receptor
New findings: novel loci (NCOA3, ALDH1A2), in regulatory genes, alters gene expression (Loughlin, 2015)
Fernandez-Moreno, Rego, Carreira-Garcia, & Blanco, 2008

OA: Prevention
Primary: Diet/exercise▪ Obesity and knee OA
Secondary: Diet/exercise
Tertiary Pain management Exercise Weight control Surgery (if severe) *Treatment primarily consists of managing pain,
maintaining activity, and weight control

Post-traumatic arthritis (PTA) Form of osteoarthritis
~12% of individuals with OA have PTA 5.5 million people
Occurs following joint injury (e.g., sports, accident, etc)
The injury damages cartilage/bone Need to prevent injuries! Treatment- exercise, medicine, maintain
proper weight Possibly surgery- for debriding, reconstruction,
or replacement, if severe.http://my.clevelandclinic.org/health/diseases_conditions/hic_Arthritis/hic-post-traumatic-arthritis
Other types of arthritis and related disorders
Ankylosing spondylitis Involves axial skeleton
Psoriatic arthritis Psoriasis and joint pain
Reactive arthritis Develops after STI (Chlamydia), GI infection (e.g. Salmonella,
Campylobacter) Can’t see, can’t pee, can’t climb a tree
Infectious arthritis Bacterial infection- N. gonorrhoae (sexually active young
adults), S. aureus (kids) Gout
Deposits of monosodium urate crystals in joints Due to hyperuriciemia, often pain in big toe
Information from Sattar HA, Fundamentals of Pathology, 2011
Osteoporosis
Defined as a reduction in bone mass (trabecular), as compared to a reference group’s bone mineral density (BMD) Measured via DXA scans
Instead, bone is porous- which increases the risk of fracture (compression fractures)
‘Silent Disease’ Often undetected until a broken bone occurs
After age 30: lose bone mass each year (~1%) Accelerated with poor diet, no weight-bearing
exercise, low estrogenSattar HA, Fundamentals of PathologyCDC
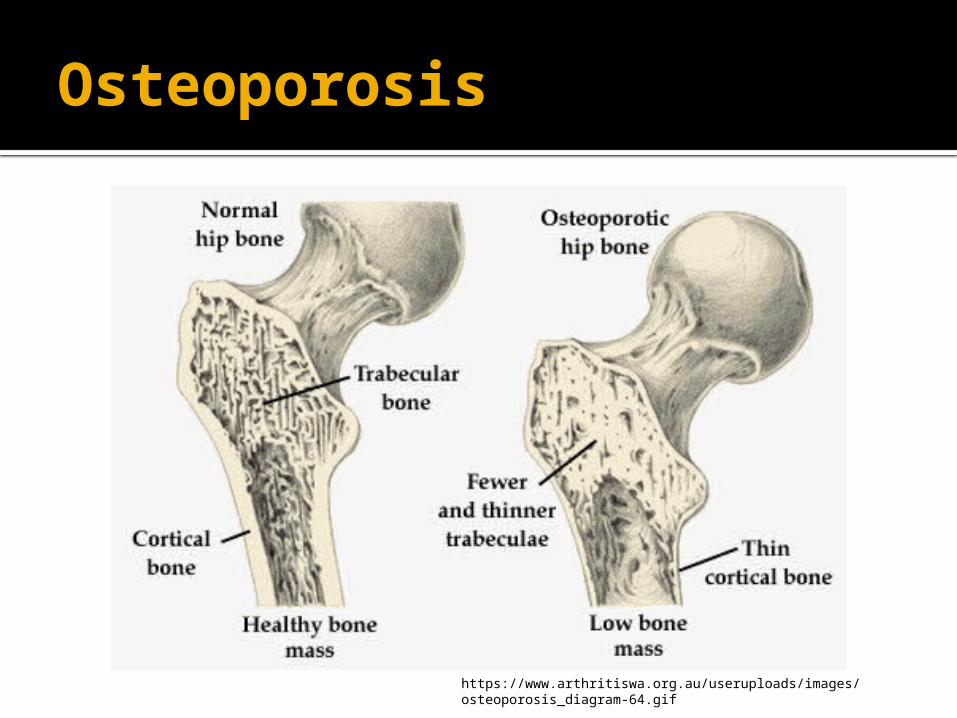
Osteoporosis
https://www.arthritiswa.org.au/useruploads/images/osteoporosis_diagram-64.gif

Hip fractures
Common with osteoporosis (from falls, etc)
Dangerous- public health concern! Increased risk of death during 12 months
following hip fracture Afterwards- hard to get around, lose mobility,
etc Costly
Most expensive of all osteoporosis fractures
Info from NHANES fact sheethttp://www.cdc.gov/nchs/data/nhanes/databriefs/osteoporosis.pdf

Osteoporosis: Epidemiology 54 million Americans have low bone mass and
osteoporosis 43.4 million: low bone mass 10.2 million: osteoporosis The total number is estimated to increase to 64.4
million by 2030 1 in 2 women and 1 in 4 men > 50 y/o will
break a bone due osteoporosis Costs: $19 billion dollars every year, up to 25.3
billion by 2010 Medicare pays for 80% of broken bones due to
osteoporosisInfo from National Osteoporosis Association
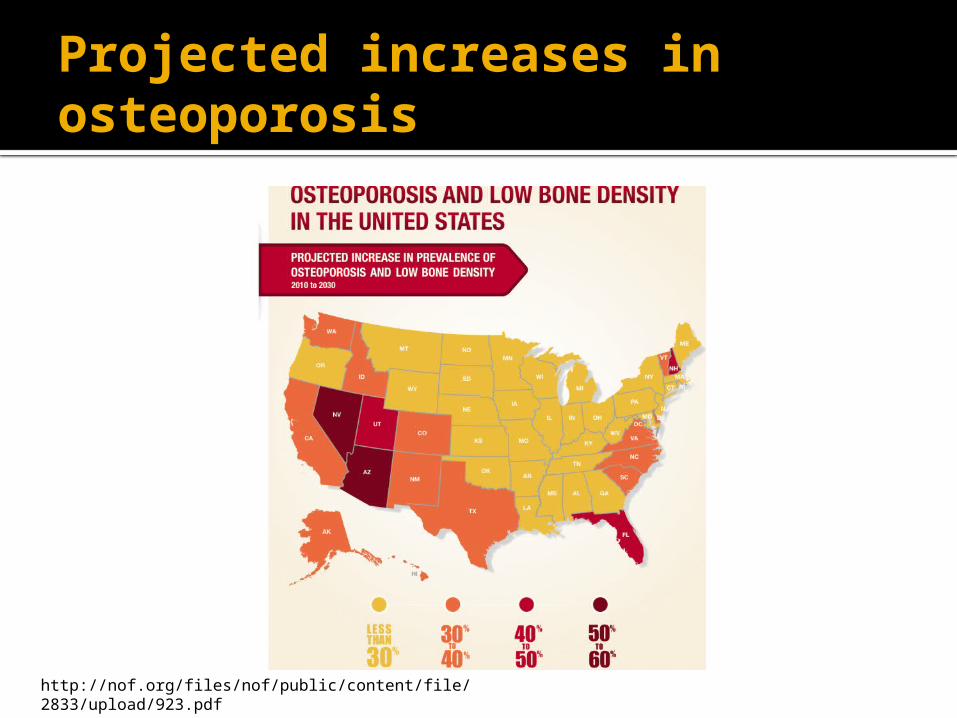
Projected increases in osteoporosis
http://nof.org/files/nof/public/content/file/2833/upload/923.pdf

Osteoporosis: Epidemiology
Data from NHANEShttp://www.cdc.gov/nchs/data/nhanes/databriefs/osteoporosis.pdf

Osteoporosis: Epidemiology
Data from NHANEShttp://www.cdc.gov/nchs/data/nhanes/databriefs/osteoporosis.pdf

Osteoporosis: Risk factors
Age Gender (women more than men) Ethnicity (White/Asian) Body type/size Family history (genetics) Other
Alcohol, smoking, activity level, medications, calcium/Vit D levels, low estrogen, anorexia
Info from NIH fact sheethttp://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/osteoporosis_ff.asp

Osteoporosis: Prevention (and treatments)
Primary prevention Diet- adequate calcium and Vitamin D Exercise Avoid smoking and excess alcohol consumption Bone density scans at appropriate age
Secondary prevention Also diet/exercise Medications, such as bisphosphonates like Alendronate
(antiresorptive) or anabolic drugs like Teriparatide (similar to parathyroid hormone), that can increase bone formation
Tertiary prevention Taking measures to prevent falls, important in the elderly Medications

Vitamin D Recommendations
http://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/

Calcium recommendations
http://ods.od.nih.gov/factsheets/Calcium-HealthProfessional/

Research

Research
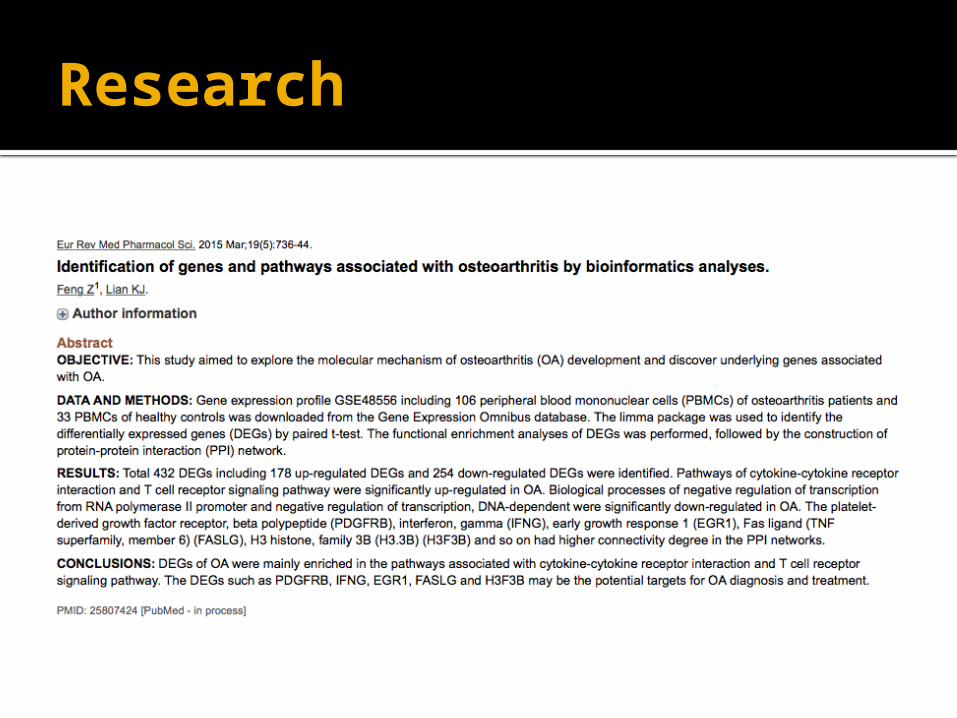
Research

Research

Research