level 2 pressure ulcers are a pain in the @&%! part 2 2 pressure...level 2 pressure ulcers are a...
TRANSCRIPT

Level 2 Pressure Ulcers are a Pain in the @&%!
Part 2
NPA Annual Conference
October 19-21, 2015
Presenters:
Verna Sellers, MD, MPH, AGSF, CMD
Kimberly Woodley, ASQ-CQE

Objectives
With information from this session attendees
should be able to:
• Learn how to develop a risk assessment tool that
addresses the needs of the population they serve.
• Learn from Level 2 events
• Learn to implement IDT interventions based on the risk
score
“Being ignorant is not so much a shame, as being unwilling to learn.”
- Benjamin Franklin

Centra - A regional not for profit integrated health
system serving communities in central Virginia
Acute Care
• 4 acute care
facilities
• 850 licensed beds
• 225,000 annual ER
visits
• 260 employed
physicians
• 550 active medical
staff
• 8,000 employees
• Level 2 trauma
center
• Clinical leadership
in all major service
lines
Post Acute Care
Long
Term
Acute
Care
Hsptl
Inpatient
Rehab
Facility
Palliative
Care &
Inpatient
HospiceFree
Standing
Skilled
Nursing
Facilities
Home
Health &
Hospice
Services
P.A.C.E.
Senior
Living
Facilities
Emergency
Mental Health
Inpatient
Child/Adol
Adult
Geriatric
Residential
Treatment:
Child/Adol
Chemical Dep
Rivermont
Schools
Outpatient
Psychiatric
Services
Centra PACE
• In February 2009, Centra PACE, opened
its first site in Lynchburg, Virginia.
• Service area includes urban and rural
areas of central Virginia.
• ~110 Participants

Centra PACE Expansion
• In January 2013, Centra PACE, opened its
second site in Farmville, Virginia, approximately
an hour away from Lynchburg.
• Service area is a rural area in the center of
Virginia.
• ~ 70 participants

Level 2
• Unusual incidents that result in serious adverse
participant outcomes OR negative media coverage
related to the PACE organization.
• Incidents meet reporting thresholds as defined by July
2015 Guidance
• Require reporting to CMS (DMAO), Regional Office, and
State Administrating Agency
• Majority require an internal investigation of the
occurrence, with the goal of identifying failures and
improvement opportunities.(RCA)

Background
“An investment in knowledge always pays the best interest”.
- Benjamin Franklin
• How are pressure ulcers staged?
• What is a level 2 pressure ulcer?

Level 2 Pressure Ulcers
Acquired while enrolled in PACE (includes a
pressure ulcer that is present upon enrollment, but
worsens after enrollment):
• Unstageable
• Stage IV
• Stage III

Stage 1
Stage 2
Stage 3
Stage 4
DTI
Unstagable
9


Braden Scale Challenges
“Tis a great confidence in a friend to tell him your faults; greater to tell him his.”
- Benjamin Franklin
• Subjective: “always”, “occasionally”, “limited”
• Moisture: “linen changes”
• Activity: “majority of shift”
• Nutrition: “every meal”
• Friction: “bed or chair”
Warner-Maron, Annals of Long Term Care, May 2015

Plan CheckCurrent Metrics
March 2015
Goals:
2014 FMV Rate: 2.6% per month
2014 LYN Rate: 2.1% per month
Team Members
Dawn Stanley, FMV Int Ctr Mgr Kendra Kerr, Int LYN Ctr Mgr
Renee Gilliam, FMV Clinic Coord Jenny Link, LYN Clinic Coord,
Cassandra Hurt, FMV HCC Carol Arthur,LYN HCC
Meagan Waller, FMV Dietician Brenda Meredith, LYN Dietician
Verna Sellers, MD Kimberly Woodley, Facilitator
Carol Emerson, CODA Chrissette Brooks, Outcomes Specialist
Do● Print hard copies of graph and Treatment/Prevention Research -Complete
● Review graph and research prior to next meeting. - Complete
● Add Therpy Rep to Team - Complete
● Assure Clinic Nurse Can Attend - Complete
● Determine scoring - Continues
● Deveiop interventions - Continues
● Steps required for implementation - Continues
ACT:
● Review PACE Pressure Ulcer Policy prior to next meeting - Team● Evaluate wording for mobility and moisture - make "frequent" less subjective - Kim
● Because Moisture is so key; calculate total score using a weighted score of
0,1,2, 4 - Kim
Pressure Ulcer Reduction
Mission Statement: Reduce the percertange of participants, who acquire any
pressure ulcer after enrollment into the PACE program or a pressure ulcer that
is present upon enrollment worsens. This rate includes all pressure ulcers
regardless of the location or stage when it is initially identified.
2015 Goal is to reduce the Centra rate to ≤ 1.5% of PACE participants will
acquire a pressure ulcer in any given month or have a pressure ulcer present on
admission worsen. This is a stretch goal.
FMV 1.8% 1.8%
LYN 1.0% 1.9%
Centra PACE 1.3% 1.9%
Site
Percentage of Participants w/
Acquired Pressure Ulcers
during month.
Prevelence of Participants
w/ Acquired Pressure
Ulcers.
Risk Score Low n=11
Low/Mod
n=5 Mod n=13 High n=13
11 1
12 0
13 0
14 1
15 1 2
16 1
17 0
18 2 1
19 2
20 1
21 1
22 1 1
23 6 2
24 1 1 1
25 3 3 1
26 2 0 1
27 5 1
11 5 13 13
Propose:
High: ≤ 21
Moderate 22 to 24
Low ≥ 25
0
1
2
3
4
5
6
7
11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Numb
er of
Parti
cipan
t
Risk Scores
Risk Assessment Score
Low n=11
Low/Mod n=5
Mod n=13
High n=13

Centra PACE’s Risk
Assessment“He that can have patience can have what he will”.
- Benjamin Franklin
• Project has been active for 18 months
• SIXTH Revision
• Has not been clinically proven
• Has not been statistically determined to be
repeatable and reliable
• Numeric scores cannot be compared to Braden

Centra PACE’s Risk
Assessment• Scoring is weighted in relationship to the
“importance” of criteria as determined by the
team.
• Developed using stratified or selected sample to
assure inclusion of participants at a variety of
risk levels
• Has not yet replaced the Braden (but will when
team has ‘buy in’).

SENSORY PERCEPTION
ability to respond meaningfully
to pressure- related discomfort
1.Comple te ly Limite d
● Unresponsive (does not moan flinch or
grasp to painful stimuli due to diminished
level of consciousness or sedation
OR
● Limited ability to feel pain over most of
body
2 . Ve ry Limite d
● Responds only to painful stimuli. Cannot
communicate discomfort except by
moaning or restlessness
OR
● Has a sensory impairment which limits
the ability to feel pain or discomfort.
3 . S lightly Limite d
● Responds to verbal commands but
cannot always communicate discomfort
or the need to be turned.
OR
● Has some sensory impairment which
limits the ability to feel pain or discomfort
in 1 or 2 extremities.
4 . No Impa irme nt
● Responds to verbal commands. Has no
sensory defic it which would limit ability to
feel or voice pain or discomfort.
COGNITIVE IMPAIRMENT 1.La te , Se ve re Impa irme nt
● Nearly unintelligible verbal output
● Remote memory gone
● Unable to copy or write
● No longer grooming or dressing
● Motor or verbal agitation
● MMSE 0 to 10
2 . Middle , Mode ra te Cognitive
Impa irme nt
● Disoriented to date, place
● Comprehension difficulties (aphasia)
● Impaired new learning
● Getting lost in familiar places
● Delusions, agitation, aggression
● MMSE 11 to 20
3 . Ea rly, Mild Cognitive Impa irme nt
● Disoriented to date
● Naming difficulties (anomia)
● Recent recall problems
● Mild difficulty copying figures
● Decreased insight
● Problems managing finances
● MMSE 21 to 25
4 . Mild Cognitive Impa irme nt
●Report by patient or caregiver of memory
loss
● Objective signs of memory impairment.
● Mild construction, language, or
executive dysfunction.
● MMSE 26 to 30
MOISTURE
degree to which skin is exposed
to moisture (include feet)
0 . Inc ontine nt of Bla dde r a nd/or
Bowe l
● R equires changing every two hours.
1. Ve ry Moist
●Skin is often moist (socks/shirt are moist
to touch at changing ~ once a week)
●Incontinent at times (~ once a week)
●Requires assistance changing
●BMI ≥ 40 w/ multiple skin folds
2 . Oc c a siona lly moist.
● Skin is occasionally moist.(socks/shirt
are moist to touch at changing ~ once a
month)
● Two or fewer skin folds
● Moisture between toes
4 . Contine nt of bla dde r a nd bowe l
● Toilet self OR
● Able to change self w/o assistance
ACTIVITY
degree of physical activity
1. Be dfa st
● Confined to bed.
2 . Cha irfa st
●Ability to walk severely limited or non-
existent.
● Cannot bear own weight and/or must be
assisted into chair or wheelchair.
3 . Wa lks Oc c a siona lly
●Walks occasionally during day but for
very short distances with or without
assistance.
●Spends majority of time in bed or in
chair.
4 . Wa lks Fre que ntly
● Walks at least once every two hours
during waking hours.
NUTRITIONNutrition risk assessment w ill be
assessed by RD in semiannual/ annual
assessment. Rated on a scale of 1-4
as a skin core under "other" in skin
part of nutritional assessment.
1. Ne e ds proba bly not be ing me t
(two or more of the following
fa c tors)
● Weight loss or BMI ≤ 23
● Poor/ fair intake in Center
● No appetite; poor intake
● Interventions in place to meet nutritional
needs, but status remains compromised
● Totally dependent for feeding
/hydrating
2 . High Risk (two or more of the
following fa c tors)
● Weight loss due to insuffic ient calories
● Dependent and/or refuses
supplements/food
● Intake is primarily "empty calorie food"
● BMI ≤ 23
● Takes > 40 minutes to eat
● Upper GI or mouth issue effecting PO
3 . Mode ra te Risk (one or more of
the following fa c tors)
● Weight stable but questionable protein
intake.
● Dependent on supplements
● Intake is primarily "empty calorie food"
● BMI ≤ 23
● Upper GI or mouth issue effecting PO
● Weight Loss Pattern
4 .Low Risk
● Weight stable indicative of calories to
spare protein.
● Intake is primarily balanced diet from
"My Plate"
● Adequate food resources
● Able to feed self without problems
FRICTION & SHEER 1. Ma ximum Assista nc e
● Requires moderate to maximum
assistance in moving.
● Complete lifting without sliding against
sheets is impossible.
● Frequently slides down in bed requiring
frequent repositioning with maximum
assistance.
2 . Ne e ds Assista nc e
●Maintains relatively good position in
chair or bed most of the time but
occasionally slides down, and needs
assistance for repositioning.
4 . No Assista nc e
●Maintains relatively good position in
chair or bed most of the time .
● Needs no assistance in repositioning.
Scoring:
5 to 11 High Risk of developing a Pressure Ulcer
12 to 17 Moderate Risk of developing a Pressure Ulcer
18 to 24 Mild Risk of developing a Pressure Ulcer
Centra PACE Pressure Ulcer Risk Assessment

Braden Risk Assessment
• Five Risk Categories
– Very High Risk: Total Score 9 or less
– High Risk: Total Score 10-12
– Moderate Risk: Total Score 13-14
– Mild Risk: Total Score 15-18
– No Risk: Total Score 19-23
– Sample of n=36: 92% of Participants scored
“mild” or “no risk”; which means only 8%
identified as moderate or greater.

Centra PACE’s Risk
Assessment• Three Risk Categories
– High
– Moderate
– Mild
• Sample of n=36: 25% score moderate

Centra PACE’s Risk
Assessment Sample (n=36)
Braden
• 92% Mild or Very Mild
• 8% Moderate
• 55% Participants score 17
Centra
• 75% Mild
• 25% Moderate

Centra PACE’s Level 2
“By failing to prepare, you are preparing to fail.”
- Benjamin Franklin
• 83 year old Male
• Participant lived alone at home, and was receiving end of life/ palliative care
services in home. Participant’s wishes were that he die in his home, which
he did.
• Significant diagnoses include CAD, Dementia, Depression, Diverticulosis,
Esophageal stricture, Gait disturbance, Hemiplegia, Hyperlipidemia, HTN,
MI old, PVD, PHB, Anemia, Anxiety, Atherosclerosis, A-fib, Cataract, CVD,
CKD stage 3,
• IDT team’s main concerns related to participant prior to event: Fall with
injury, Impaired skin integrity, End of life/palliative care in home (includes,
minimally weekly visits by PACE Nurse Navigator), Assist participant and
family with end of life process, and Adverse reactions to medications
Centra PACE’s Level 2
In home Personal Care Aide called Nurse Navigator and described wound on
hand near palm protector. PACE Nurse Navigator made home visit and found
stage III pressure ulcer in the area between the pointer finger and the thumb.
Identification of risk points and their potential contribution to the event:
•No documentation of education being provided to family or Personal Care Aide
on use of Palm Protector which potentially may have led to improper use of the
Palm Protector
•OT assessment did not list palm protector as a brace or splint in 06/08/15 OT
assessment which potentially may have led to improper use of the Palm
Protector. Assessment had been done in person prior to 06/08/15, but was not
documented until that time.
•Home Care 06/10/15 assessment did not list Palm Protector in DME list and it
was not addressed in POC for skin which may have led to skin breakdown.

Centra PACE’s Level 2
• Therapy will develop a log that will list DME, date issued, participant name,
education conducted (check off), and documented in EMR (check off) which
should include with whom education occurred and date. Outcomes
Specialist will audit process from July to December to assure
implementation.
• A question will be added to Home Care Assessments regarding the
participant using a brace or splint. The EMR has been updated with fields
for the device and for education that is provided to family/PCA, etc.
• The EMR has been updated with fields for education provided by Therapy
to family/PCA etc. Outcomes Specialist will audit to assure compliance.
• Educate Therapy to notify Dayroom C.N.A. if nail care needs to be
performed.

Centra PACE’s Level 2
• Develop a Therapy specific email list.
• Therapy will utilize the “Daily to Do List” to better communicate within
Therapy.
• When an assessment is done off site or away from a computer, down time
form will be used.
• Develop an education module for skin assessment.
• Active Performance Improvement Team Pressure is working to reduce
Acquired Pressure Ulcers. Currently, the team is working to develop a Risk
Assessment Tool that addresses the PACE population. Other future work
will involve revision of current policy and assure appropriate interventions
for risk levels.
IDT Approach to Prevention
“Instead of cursing the darkness, light a candle.”
- Benjamin Franklin
• Providers/ Clinic
– Skin assessment using a risk assessment tool,
minimally during annual/semi annual, but more if
participant is at high risk.
– Pre/Post Respite skin assessments
– Recommendation of skin barriers ointments
– Treatments to prevent worsening if breakdown
occurs

IDT Approach to Prevention
• Dietician: Nutrition– Hepatic proteins (albumin/pre-albumin) are not markers of malnutrition but do correlate with
mortality & morbidity and thus are useful indicators of illness severity
– Protein intake should be 1.25-1.5 gm/kg; severe illness or injury may need 2.0 gm/kg
– Energy intake should be 30-35 cal/kg
– Arginine stimulates insulin secretion, promotes the transport of amino acids into cells, and
supports the formation of protein in the cells. “There is growing body of moderate-quality
evidence supporting the positive effect of supplementation with additional protein, arginine,
and micronutrients to promote pressure ulcer healing.”
– Vitamin C can be met usually with diet.
– Zinc deficiency may cause loss of appetite, abnormal taste, impaired immune function, and
impaired wound healing. On the other hand, “high-serum zinc levels may inhibit healing,
impair phagocytosis, interfere with copper metabolism and induce a copper deficiency
(copper is essential for collagen cross-linking.)”
2015 White Paper from the National Pressure Ulcer Advisory Panel.

IDT Approach to Prevention
• Home Care:
– Educating Participants/Families/Caregivers:• Proper hygiene
• Keeping participants dry
• Changing Pads pull ups
• Changing positions
• Use of skin barriers ointments
• Notifying PACE at the first sign of skin breakdown
• Well fitting shoes
• Brace/splint fit
– Assuring pressure release devices are in use
– In home/facility skin assessments

IDT Approach to Prevention
• Activities/Dayroom:
– Keeping participants dry
– Changing Pads pull ups
– Toileting Schedule
– Use of skin barriers ointments
– Notifying Clinic at the first sign of skin breakdown
– Assuring pressure release cushions are in use

IDT Approach to Prevention
• Therapy:
– Well fitting shoes
– Brace/splint fit
– Pressure release devices- cushions,
mattresses, etc.

IDT Approach to Prevention
• Transportation:
– Evaluation of routes, if possible LIFO (Last in,
first off)
– Cushions/ Dysum mats

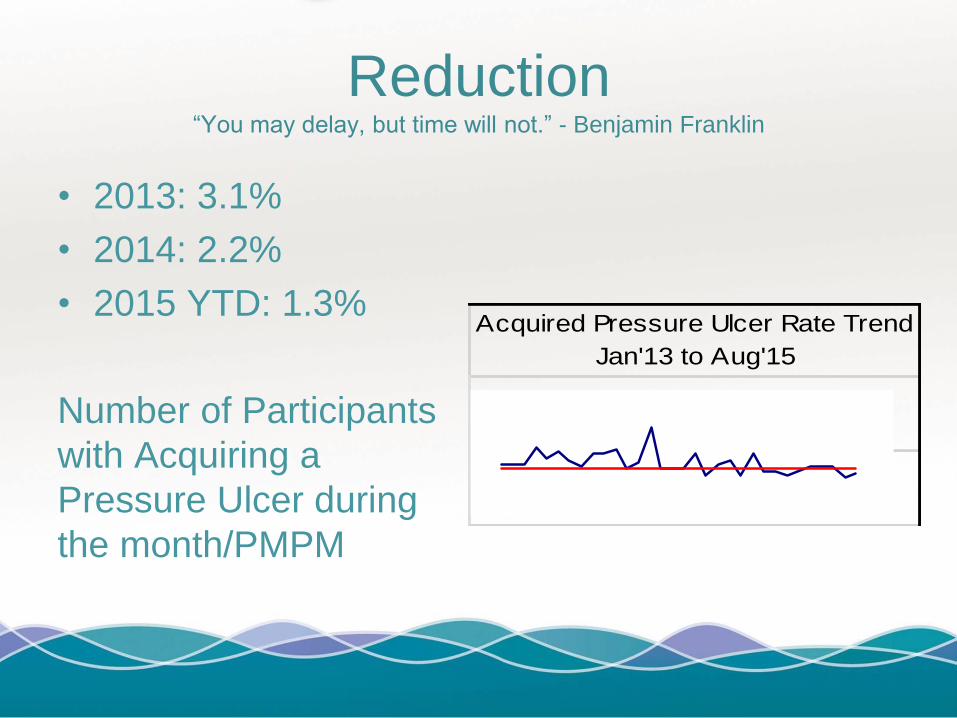
Reduction“You may delay, but time will not.” - Benjamin Franklin
• 2013: 3.1%
• 2014: 2.2%
• 2015 YTD: 1.3%
Number of Participants
with Acquiring a
Pressure Ulcer during
the month/PMPM
Acquired Pressure Ulcer Rate Trend
Jan'13 to Aug'15
Final Thoughts
• Pressure Ulcer Risk Assessment should be a part of the
semi annual/annual/ and unscheduled assessments
• Developing a Risk Assessment tool to address the
PACE population may be beneficial
• Regardless of the tool used, an IDT approach to
prevention is necessary for success.