the science of pressure ulcers
TRANSCRIPT
1
The Science
of
Pressure Ulcers
Laurie Talarico, APRN, BC
LNHA, CDONA/LTC, CLNC
Evercare© 2006

2
Objectives
● Review components of facility skin-at-risk program
● Understand prevention assessment requirements● Discuss interdisciplinary dictates● Review components of facility wound treatment
program● Understand wound assessment requirements● Discuss standardization of wound care● Improve ability to implement positive change in
facility

3
Why is this an issue…….
● Patient care concerns◆ Pain◆ Infection◆ Quality of life◆ Death

4
Why is this an issue…….
● Quality Measure◆ Reflection to the public about the care, or lack of care, that
your facility provides◆ Residents with “low risk” shouldn’t develop pressure ulcers
● Highly publicized ◆ Read all about it◆ Lay person lacks understanding◆ Up and coming legal issue
● Expensive◆ Products cost $$◆ Nursing time cost $$◆ Bad reputation cost $$$$$◆ Legal battles cost $$$$$
5
What are the barriers to a good prevention program?
● Continuity ◆ Staffing issues ◆ Regimen
● Education◆ Lack of understanding
■ Staff■ Resident and their family
● Time ◆ Staffing levels
Evercare© 2006

6
What are the barriers to a good prevention program?
● Lack of systems◆ No consistency
● Communication ◆ Documentation◆ Speaking the “same language”
● Commitment◆ Leadership

7
Let’s discuss
Take five minutes to discuss and
list the barriers to the pressure ulcer prevention program
in your facility

8
CMS Criteria● Avoidable Pressure Ulcers
◆ The facility did not do one or more of the following:■ Evaluate the resident’s clinical condition and risk factors■ Define/implement interventions consistent with resident
goals/standards of practice■ Monitor/evaluate the impact of interventions■ Revise interventions
● Unavoidable Pressure Ulcers◆ Develop pressure ulcer even though the facility did:
■ Evaluate the resident’s clinical condition and risk factors■ Define/implement interventions consistent with resident
goals/standards of practice■ Monitor/evaluate the impact of interventions■ Revise interventions

9
Where the assessment goes wrong…..
● Who teaches who how to perform the assessment?
◆ How is competency assessed?
● What guiding principles are used when performing the assessment?
◆ Timeframes◆ “change in condition”
● Are the assessment results reproducible?● What is done with the assessment information?● Who monitors the accuracy of the information
and what is done with it?◆ When the issue of pressure ulcers is reviewed at your QI
meeting, what, other than the numbers, is examined?
10
If the facility can not guarantee the accuracy of the assessment,
how can the facility ensure that the prevention strategies are
appropriate and individualized for each resident?

11
Standards
● Ensure residents who enter the facility without pressure sores do not develop pressure sores unless the individual’s clinical condition demonstrates that they are unavoidable
● Properly assess the resident and concurrent conditions that place the individual at risk for breakdown
● Develop a plan of care that systematically assesses and identifies residents at risk for skin breakdown, presents approaches to reduce the identified risk(s) and evaluates the outcome
12
Objective
● Assessment ◆ Using medical and cognitive history, physical exam,
Braden scale (or other legitimate tool)
● Diagnosis◆ Determination of individual risk and the nature of the
specific factors that cause the risk
● Management◆ Utilizing specific skin care and early treatment
measures to maintain and improve tissue tolerance to pressure in order to prevent injury
◆ Protection against the adverse effects of the external mechanical forces of pressure, friction and shear
◆ Staff education
13
Criteria
● A comprehensive skin at risk assessment will be initiated for all residents upon admission and quarterly.
● If a resident becomes chair or bed bound or develops difficulty with repositioning outside the routine assessment time frames, an additional assessment will be done
● Contributing clinical and environmental factors will be considered when completing the Braden Scale
14
● Residents with a Braden Scale score of 15 or below and those who score below three on any individual portion of the scale are considered to be at risk for skin breakdown
● These identified residents will be placed on weekly head to toe visual examination by a licensed nurse
● Preventative measures will be implemented and addressed on the resident’s plan of care
15
Let’s talk about the tool…..
What are the barriers to using the Braden, or for that matter, the Norton Scale,
effectively in your facility?
Where does the assessment go wrong?
16
Guidelines
● Sensory Perception◆ Certain medical conditions decrease a resident’s ability
to respond meaningfully to pressure-related discomfort and contribute to the risk for skin breakdown
◆ Such factors, despite the resident’s functional mobility, contribute significantly enough to cause special consideration on the assessment
◆ Residents who have documented evidence of one contributing factor should score a minimum of three on the scale
◆ Those with two or more contributing factors will score a minimum of two on the scale
17
Contributing factors to altered sensory perception● Peripheral vascular disease● Diabetes● Anemia● Leukopenia● COPD● Paraplegia● Quadriplegia● MS or other neurological
disorder● Alzheimer’s or other
dementing disease● Altered LOC● Infection or sepsis● Terminal cancer● History of Stage II or greater
ulcer● Advanced age (>79 yo)
● Prolonged pain or discomfort● Chronic or end stage renal,
liver and/or heart disease● Dry, flaky or scaling skin
condition● Disease or drug induced
immunosuppression● Psychopharmacologic med
use● Steroid treatment● Radiation therapy● Antimetabolite therapy● Chemotherapy● Renal dialysis● Skeletal abnormalities● Restraint use

18
Moisture
● Certain clinical conditions increase the degree to which a resident's skin is exposed to moisture and contribute to the risk for skin breakdown
● Such factors, despite the resident's functional mobility, contribute significantly enough to cause special consideration on the assessment
● The amount of time and the degree of exposure to moisture need to be considered
● Sources of moisture include incontinence of urine or stool, perspiration and wound drainage

19
Contributors to scoring for “Moisture”
● Residents who are exposed to excess moisture sufficient enough to require at least one change of linen, clothing or incontinence device in a 24 hour period should be scored at a minimum of three on the scale
● Residents who are exposed to excess moisture sufficient enough to require more than one change of linen, clothing or incontinence device in a 24 hour period should be scored at a minimum of two on the scale
● Residents who experience frequent exposure to excess moisture, requiring staff intervention and changing of linen, clothing or incontinence device every two hours should be scored a one on the scale
20
Activity
● Certain clinical and environmental conditions alter a resident’s ability to be active and contribute to the risk for skin breakdown
● The degree of activity the resident is capable of expending contributes significantly enough to cause special consideration on the assessment
● Activity issues to be considered include physical, cognitive and environmental contributions
● The primary risk factors for pressure ulcers are immobility and limited activity levels
● Residents whose activity is limited to bed or in any chair are at greater risk than those who ambulate freely

21
Considerations for scoring Activity
● Among the clinical conditions that limit resident ability to move freely are:
◆ Arthritic conditions◆ Muscle weakening conditions◆ Advanced age◆ Pain◆ Respiratory conditions◆ Restraints◆ Altered levels of awareness◆ Neurological disorders

22
Scoring “Activity”● Residents who spend greater than 75% of wakeful time
ambulating freely are scored four on the Braden Scale◆ Do not spend the majority of their time in a chair
● Residents who ambulate freely 50-75% of the time are scored three on the Braden Scale
◆ Sit more of the day than stand, increasing the time pressure is not relieved
● Residents who require staff assistance to ambulate, are transferred from bed to chair, or cannot bear their own weight are scored two on the scale
● Residents who do not leave the bed or are transferred from bed to any chair only are scored one on the scale
◆ It is as though they never left the bed

23
Mobility
● Certain clinical and environmental conditions alter a resident’s ability to mobilize and contribute to the risk for skin breakdown
● The degree of mobilization the resident is capable of performing contributes significantly enough to cause special consideration in the assessment
● Mobility issues to be considered include physical, cognitive and environmental contributors
● Primary risk factors for pressure ulcers are immobility and limited activity levels

24
Mobility● Residents with impaired ability to reposition
themselves are at greater risk than those who move freely and purposefully in bed or in a chair
● Mobility includes considerations of postural alignment, distribution of weight, balance, stability and pressure relief
● Some clinical conditions limit resident ability to move freely
•Muscle weakening conditions
•Advanced age
•Pain
•Respiratory conditions
•Dementing disorders
•Restraints
•Altered levels of awareness
•Neurological disorders
•Parkinson’s disease
•Arthritic conditions
•Disorders which affect tone

25
Mobility
● Important to consider both the ability to position and the purposefulness of the position change
● Bedfast, elderly patients are less likely to move spontaneously
If the position change does not create a situation where pressure is moved from
one area to another,
then it is not purposeful.
26
Let’s score “Mobility”
● Residents who require no assistance to reposition and can demonstrate that their position change is purposeful – is major enough to notice the resident redistributes weight evenly by turning side to side, side to back, etc. – score four on the Braden Scale
● If the resident makes only slight changes, where it is not apparent that the resident repositions frequently enough to avoid redness, or if the resident has one of the concomitant conditions which affect ability to position, score three.
27
● If the resident requires assist of any level, including positioning devices, to ensure repositioning occurs, score two
● Should the resident’s physical or cognitive ability be such that the resident makes no change in position, score one
28
Nutrition
● The Braden Scale refers to consumption
● Consumption patterns alone do not dictate the role of nutrition in the development of pressure ulcers
● Need to consider the intake of calories, protein and iron
● Vitamins C, A, D, K, B-complex and minerals Magnesium, Copper, Zinc and Calcium all play important roles
● Infection resistance, factors that lead to healing, digestion and synthesis
29
Clinical signs and symptoms● Pale skin● Red, swollen lips● Swollen and or dry tongue
with scarlet or magenta hue● Poor skin turgor● Cachexia
● Bilateral edema● Muscle wasting● Calf tenderness● Reduced urinary output● Weight loss of more than
10% in the previous month
Lab values, although not routinely ordered for the resident with intact skin, require consideration if available
•Serum albumin below 3.4 g/dl
•Serum transferrin level below 180 mg/dl
•Hemoglobin less than 12 mg/dl

30
Scoring “Nutrition”● When scoring, acknowledge that even when a
resident consumes 100% of their diet, should any of the clinical signs, symptoms or lab data discussed be present, there may be other considerations affecting overall nutrition
● When assigning a score, first estimate the usual consumption
● Subtract one point from the overall score if 1-2 considerations exist
● Subtract two points from the overall score if 3-4 considerations exist
● Subtract three points from the overall score is more than 5 considerations exist

31
Friction and Shear
● Assess the resident’s ability to properly position, transfer and turn
● Friction injuries occur when a resident's skin moves across a surface such as bed linens
● Shearing occurs when skin remains stationary and the underlying tissue shifts, such as when the head of the bed is elevated
● These injuries occur then voluntary or involuntary movements are altered by physical or cognitive factors and when they are positioned improperly

32
Clinical conditions that can cause friction and shear
● Muscle weakening conditions
● Advanced age● Pain● Respiratory conditions● Dementing disorders● Restraints● Altered levels of
awareness● Neurological disorders
● Parkinson’s disease● Arthritic conditions● Disorders that affect tone● Disorders that require the
head of the bed be elevated for significant periods of time

33
Scoring “Friction and Shear”
● Residents who present with movement or positioning difficulties are scored at a minimum of two
● Those who are dependent for positioning or movement are scored one

34
Who are the most appropriate people in your facility to
assess risk of skin breakdown?
35
Remember….
● Residents with a Braden Scale score of 15 or below and those who score below three on any individual portion of the scale are considered to be at risk for skin breakdown
● Use a weekly assessment tool◆ Place in the treatment book◆ Educate staff on head to toe assessment and form
completion◆ Use as a time to ensure preventative measures are in
place

36
Example of
“Weekly Skin Assessment”
format

37
Don’t forget the care plan….
38
Pressure relief measures
● Pressure relief mattress/gel mattress● Pressure relief chair cushion● Turning and repositioning on a regular schedule
individualized for each resident● Rehabilitation services assessment as indicated
for mobility and positioning● Maximize mobility through ambulating if possible
and range of motion

39
Relief of friction/shear
● Use of elbow/heel protectors or other devices as appropriate (“floating” the heels)
● Proper transfer/positioning techniques● Use of lifting devices such as a draw sheet● Use of transparent film dressing when
appropriate● Avoid massage over bony prominence● Avoid position over trochanter● Maintain the head of the bed at the lowest degree
of elevation consistent with medical conditions and other restrictions – limit the amount of time the head of the bed is elevated

40
Nutritional intervention
● Assure appropriate dietary intake through assessment of ability and provision of necessary assistance
● Dietary consult to assess beneficial increase of protein or other dietary assessment
● Maintain adequate hydration by offering fluid frequently unless contraindicated by medical condition
41
Reduce skin contact with moisture/bacteria
● Toilet every two hours, if appropriate
● Frequent incontinent checks and care
● Use of moisture barrier creams
● Incontinent management program
● Minimize force and friction applied to the skin during cleansing
42
Relieve dry skin
● Use moisturizing creams
● Use bath oils
● Avoid hot water
● Use mild cleansing agent that minimizes irritation and dryness
43
Monitor
● Food consumption
● Weight
● Weekly skin assessment
● Requests for NP/MD evaluation and or intervention for identified problems
● Labs as needed per NP/MD order

44
Example of care plan

45
Who needs to be on the “Skin Prevention Team”??
● Nursing (licensed and para) – clinical assessment
● PT – mobility assessment
● OT – positioning and feeding assessment
● Dietician – nutritional/hydration assessment
Don’t be afraid to physically look at the resident as a group.

46
Documentation
● Braden ● Nurses notes● MDS, RAP and quarterly● Nursing assistant documentation (could be where
preventative measures are indicated)● Positioning schedules● Treatment records indicating prevention measures and
their outcome● Care plan● Monthly summary● Weekly Skin Assessment
47
Education
● Structured, organized and comprehensive
● Direct at all levels of providers
● Stress the importance of interdisciplinary input for prevention
● Gear QA efforts toward increasing awareness of risk factors, assessment, prevention and early treatment

48
Educational program
● Etiology and risk factors● Risk assessment and contributing factors● Skin assessment● Selection and/or use of support surfaces● Development and implementation of an
individualized program of skin care● Demonstration of positioning to decrease risk of
tissue breakdown (take pictures)● Instruction on accurate documentation of
pertinent data

49
● Despite all of your interventions, wounds do happen
● Make sure that your documentation supports rationale for “failure” to maintain skin integrity
● Assessment of new or re-admissions to document evidence of wound
● Don’t stage non-pressure areas● Always search for and document etiology

50
Pressure Ulcer Treatment Program
● Standard◆ Ensure that residents who enter the facility having
pressure sores receive necessary treatment and services to promote healing, prevent infection and prevent new sores from developing
◆ Develop a plan of care that systematically assesses and outlines approaches to care of skin breakdown
◆ Appropriately evaluate outcome of treatment program
51
Take five minutes to discuss and
list the barriers to the pressure ulcer treatment program
in your facility

52
Objectives of program
● Assessment◆ Comprehensive H & P◆ Comprehensive wound assessment◆ Assess physical and psychosocial status◆ Determine potential for healing and complications
● Treatment ◆ Utilize specific treatment modalities◆ Protection against adverse effects of external
mechanical forces of pressure, friction and shear
● Management of bacterial colonization and infection
● Staff education and quality improvement

53
Wound Assessment tools
● Use a good tool that the staff understands
● Promote uniform documentation
● Appoint a person to be “in charge” of wound assessment program
● Allow time for – without excuse – for weekly review by interdisciplinary team
54
Skin Changes Due to Aging
● Flattening of the epidermal/dermal junction
● Slower circulation, transport of nutrients and oxygen and elimination of wastes
● Decreased sebacaceous and sweat production
● Decreased cellular growth rate
● Degeneration of collagen and elastic tissue
55
Total Wound Assessment
● Location● Dimensions● Depth● Exudate● Wound Base● Wound Edges
● Undermining● Tunneling● Necrotic Tissue● Epithelial Tissue● Granulation Tissue● Periwound Skin● Signs/Symptoms of
Infection● Staging the wound
◆ Do not stage in the presence of eschar
◆PUSH tool (demonstrates progress)
56
CMS Criteria for Daily Monitoring of a Dressing
● Should include the following:◆ Evaluate the status of the dressing: intact,
without leakage◆ Evaluate the status of the peri-ulcer area◆ Evaluate the wound for the presence of
possible complications: Induration, infection, increasing ulceration
◆ Evaluate the patient for pain: Is it present? Is it controlled?

57
● Evaluate progress at least weekly
● If signs of ulcer deterioration are observed sooner, steps to reverse deterioration should be taken sooner

58
CMS Criteria for Pressure Ulcer Documentation
● Minimal documentation must include:◆ Location and stage◆ Size◆ Exudate◆ Pain◆ Color and type of wound bed tissue◆ Description of the wound edges and the
surrounding tissue
59
Example of wound assessment tool
60
Location
● Below the knee ◆ Venous – knee to ankle◆ Arterial – distal areas◆ Diabetic – plantar ◆ Neuropathic – along nerve pathway
● Over bony prominences (pressure)
● Moist areas

61
62
Definition
● A pressure ulcer is any lesion caused by unrelieved pressure resulting in underlying tissue damage – soft tissue is compressed between a bony prominence and an external surface for a prolonged period of time

63
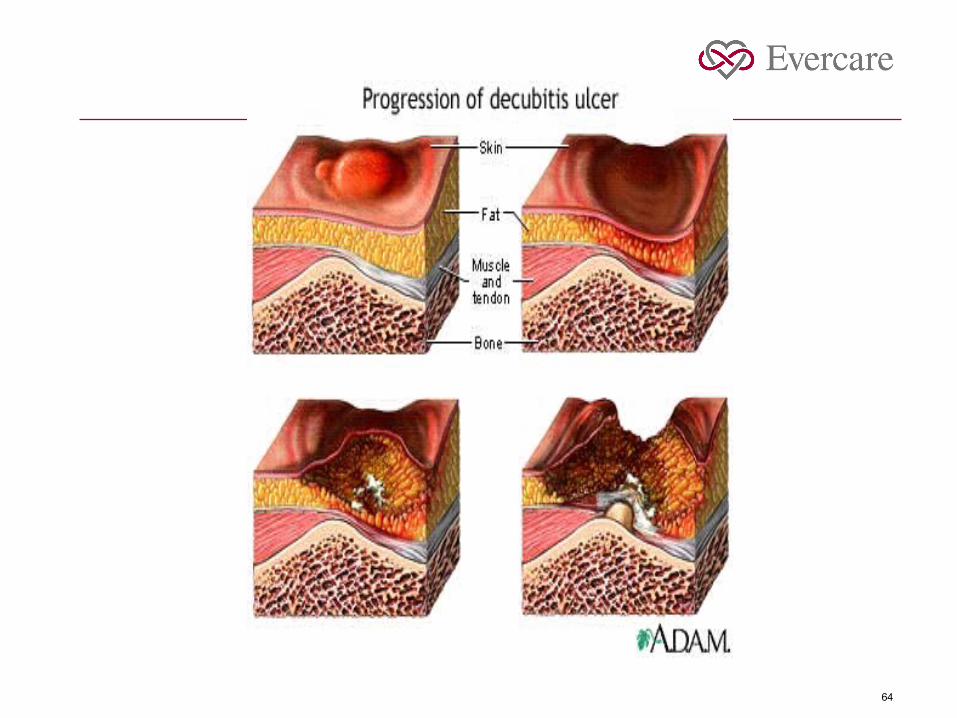
Staging is a recommended system to access the depth of pressure ulcer tissue injury
DO NOT stage in the presence of eschar or slough
DO NOT back stage
Stage ONLY pressure ulcers
64
65
Stage I
Pressure related alteration of intact skin whose indicators as compared to an adjacent or opposite area on the body may include changes in one or more of the following; skin temperature (warmth or coolness), tissue consistency (firm or boggy feel), and/or sensation (pain, itching). Area appears as a defined area of persistent redness in lightly pigmented skin, whereas in darker skin tones, the ulcer may appear with persistent red, blue, or purple hues.

66

67
Partial thickness skin loss involving epidermis, dermis or both.
(The ulcer is superficial and presents as an abrasion, blister or shallow crater)
Stage II

68

69
Stage III
Full thickness skin loss involving damage to or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia.
(The ulcer presents as a deep crater with or without undermining)

70

71
Stage IV
Full thickness skin loss with extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures.

72
73
Unstageable
Can not stage until eschar is removed

74

75
Wound Exudate
● Natural enzymes
● Growth and healing factors
● Dead cells
● Active WBC’s
Serous, Serosanguinous, Fibrinous, Purulent
Universal Precautions

76
Exudate Assessment
● Amount
● Consistency
● Odor
● Distribution in the wound
● Color

77
Exudate
● Too little◆ Desiccates wound◆ Creates non-viable wound bed
● Too much◆ Complicates wound management◆ Can destroy peri-wound
78
DO NOT culture exudate
● Exudate is colonized● Surface contaminants● MRSA
● Systemic symptoms◆ Increase in WBC◆ Change in mental status◆ Tachy◆ Hypotensive◆ Erythema of periwound area◆ Odor◆ Pain◆ Fever is late sign
79
Look at the wound
● Wound base
● Eschar/slough
● Tunneling/undermining
● Wound edges
● Periwound skin

80
Wound base
● Viable◆ Granulation – beefy red◆ Epithelialization – shiny, connecting
● Non-viable◆ Eschar – black, soft or hard, often represents full
thickness tissue destruction◆ Slough – yellow or tan, thin or stringy
81
Tunneling
● Extends into tissue in any direction
● May be more than one present in any wound
● Document number if more than one present
● Document direction of each using face of clock
● Document depth of each if more that one is present
82
Undermining
● Separation of wound edge and wound bed
● Space between the surrounding skin and the wound bed◆ Usually involves significant proportion of wound edges◆ May extend entirely around wound◆ Subcutaneous fat necrosis◆ Usually indicates aerobic and anaerobic bacteria are present
● Shear may be a factor

83
Wound edges
● Irregular
● Crater-like
● Punched-out
● Callus
● Intact, or not intact

84
Periwound skin
● Edema
● Induration
● Erythema
● Periwound pain
● Maceration

85
Documentation of dimensions
● Most wounds are not regular in shape
● Consistency in documentation important
● Document in centimeters
● Length (measure head to toe)
● Width (perpendicular to length)
● Depth (at deepest point)
● Include tunneling/undermining

86
Documentation options
● Flow sheets
● Narrative summary
● Tracing
● Photography

87
Why do I need an accurate, complete assessment??
The only way to successfully treat a wound is through an accurate assessment to determine the
appropriate treatment measures.

88
Phases of wound healingInflammatory, proliferative, maturation
● Inflammatory Phase◆ Vasoconstriction
◆ Platelets begin clot formation
◆ Erythema, edema, heat, pain as neutrophils fight bacteria
◆ Monocytes form macrophages to clear foreign particles
◆ Protein rich fluid enter wound

89
Phases of wound healingInflammatory, proliferative, maturation
● Proliferative phase◆ Granulation – angiogenesis, secretion of growth
factors, collagen deposition
◆ Contraction – fibroblasts convert to myofibroblasts to mediate contraction
◆ Epithelialization – mobilize cells, resurface from wound edges across granulation tissue

90
Phases of wound healingInflammatory, proliferative, maturation
● Maturation phase◆ Begins three weeks after onset
◆ Dissolution of granulation tissue
◆ Reorganization of collagen
◆ Fibroblasts decrease in number
◆ Vascularization decreases
◆ May take up to two years
◆ Chronic wounds regain 50% strength in 2-3 weeks, but will only gain up to 70% strength at best (rationale behind not back-staging)

91
History and physical exam
● Comprehensive● Co-morbid illness will impact healing ability
◆ Peripheral vascular disease◆ Diabetes mellitus◆ Immune deficiencies◆ Collagen vascular diseases◆ Malignancies◆ Psychosis◆ Depression

92
Assessment of Patient
● Health Status● Nutritional Status● Overall physical health● Complicating conditions● Pain● Psychosocial health● Wound etiology
◆ Acute (< 2 weeks)◆ Chronic◆ Surgical

93
Etiology
● Why did this wound form?
● Where is the pressure coming from?
● What are the co-morbid conditions?
● How can I minimize or eliminate the etiology?

94
Nutritional assessment
● Ensure that diet contains nutrients adequate to support wound healing
● Intake must be sufficient to prevent malnutrition● Hydration (30 ml water per kg of body weight per
24 hours)● Weight
◆ Loss of 5% in past month or 10% in past 6 months not good sign
◆ Current body weight below 15% of ideal body weight not good sign
● Dysphagia◆ Assess difficulty swallowing or eating

95
● Nutritional history
◆ Malnutrition◆ Nutrition altering diseases◆ Oral and cutaneous signs of vitamin or mineral
deficiencies● Altered labs
◆ Decreased WBC◆ Decreased serum albumin or prealbumin◆ B12 or folate deficiency
● Address in plan of care◆ Caloric intake◆ Hydration needs◆ Protein needs◆ Vitamin and mineral supplements (A, C, Zinc)

96
Nutritional principles
● Iron, B12, folic acid are needed to enable red blood cells to carry oxygen to healing tissues
● Iron is a cofactor in collagen synthesis● Vitamin C and Zinc are vital to tissue repair● Vitamin A is a cofactor for the stimulation of
collagen cross-linking and epithelialization● Protein is essential to wound healing● Adequate calories are required to fuel wound
healing● Adequate hydration is necessary to carry
nutrients through the blood stream to the wound
97
Nutritional Risk Factors
● Serum Albumin < 3.5 gm/dl◆ Depletion of protein stores
● Serum transferrin < 180 mg/dl◆ Negative nitrogen balance
● Total lymphocyte count < 1800 cells/mm3◆ Malnutrition/impaired immunity
● Hemoglobin < 12mg/dl◆ Deficient iron stores
● Decreased oral intake

98
Pain assessment
● Can be related to the wound or to its treatment● Pain control interventions
◆ Repositioning◆ Covering the wound◆ Systemic analgesia
● Be pro-active● Use drug and non-drug therapies● Frequently reassess ● Always document

99
Myths
● Leave it open to the air● The more often you change the dressing the
better● If the wound is draining, it is infected● Swab cultures are adequate diagnostic tools for
infections● Need to keep wound sterile
100
Ideal wound environment
● Moist● Free from excess exudate● Free from necrotic tissue● Free from trauma (pressure)● Warm● Protected from bacterial invasion● Acidic● Oxygen sensitive
101
Hypoxia
● Decreases fibroblast mitosis and collagen synthesis
● Inhibits epithelial migration
● Leads to cell death

102
Temperature
● Decreased wound temperature reduces mitotic and phagocytic activity
● Dressing changes can reduce wound temperature
● May take up to 3 hours to return to preferred wound temperature each time dressing is changed

103
Desiccation
● Scab delays wound healing
● Results in scaring
● Epidermal cell movement slows due to collagen fibers at the interface of eschar and dermis
● Slows healing by as much as 40%

104
Maceration
● Breakdown of surrounding skin from excessive exudate

105
Debris
● Necrotic tissue, slough – non-viable
● Sutures, dirt, gauze, glass, cotton
● Prolongs inflammatory phase
● Predisposes to infection

106
Medications
● Immunosuppressives, chemotherapy, anticoagulants, anti-inflammatory agents, etc.
● May increase tissue susceptibility and delay wound healing

107
Infection
● Prolongs inflammatory phase
● Increases tissue destruction
● Delays collagen synthesis
● Prevents epithelialization

108
Clinical signs and symptoms of infection
● Friable, bright red granulation tissue● Exuberant granulation tissue● Increased discharge● Increasing pain● Delayed healing● Foul odor
109
Prepare the wound bed
● Determine if wound is acute or chronic
● Assess bacterial burden
● Assess wound etiology
● Assess eschar
● Consider debridement options
● Look for established granulation
110
Bacterial Burden
● Can result in localized ischemia
● Can cause premature wound closure
● Contamination vs. infection◆ Pain, erythema, increased exudate, odor are signs of
heavy colonization and possible infection◆ With heavy colonization, start thinking about topical
antibiotic treatment for 2 weeks■ Pseudomonas – silvidine■ Triple antibiotic ointment, bactroban
111
Wound Infection
● Cultures◆ Never routinely culture◆ Quantitative tissue culture preferred
● Must eliminate infection
● Overuse of antibiotics◆ Reduces normal flora◆ Superinfections◆ Toxicity◆ Resistance

112
Management of bacterial colonization and infection
● Protect from fecal and urinary contamination
● Cleanse and debride
● 2 week trial of topical antibiotic
● Diagnose soft tissue infection vs. osteomyelitis
● Systemic antibiotics for systemic infection only
● Sepsis requires urgent medical attention

113
Management of bacterial colonization and infection (con’t)
● Consider:◆ Silver Sulfadiazine◆ Triple antibiotic◆ Polysporin◆ Mupivocin◆ Metronidazole◆ Bactroban
● Consider only time limited and/or not at all
◆ Povidone iodine◆ Iodophor◆ Dakin’s solution◆ Hydrogen peroxide◆ Acetic acid

114
Systemic infection
● Soft tissue infection
◆ Keflex
◆ Augmentin
● Osteomyelitis
◆ IV vancomycin

115
About 25 % of non-healing wounds have underlying
osteomyeletis
●Systemic antibiotic therapy (long term)
●Review goals of care
●Review advance care planning issues

116
Debridement
● Enhance wound assessment● Promote better wound hygiene● Establish earlier wound bed coverage● Options
◆ Enzymatic◆ Autolytic◆ Mechanical◆ Surgical

117
Autolytic Debridement
● Uses body’s natural enzymes to breakdown necrotic tissue
● Achieved with semi or semi-occlusive dressings● Easy to perform● Little or no discomfort● Takes longer than other methods● Contraindicated in the presence of infection

118
Mechanical Debridement
● Wet to dry dressings, Hydrotherapy, Wound irrigation
● Non-selective
● Time consuming
● Trauma to capillaries may cause bleeding
● Maceration may occur
● Can be painful

119
Sharp Debridement
● Use of scalpel or scissors to remove devitalized tissue
● Mostly selective● Requires technical skill● Fast● Not recommended in severely compromised
patient or those with bleeding disorders● Painful – medication required● Antibiotics recommended

120
Enzymatic Debridement
● Topical use of chemical agents to devitalized tissue
● Not as traumatizing to wound● Patient discomfort minimal● Easy to use● Selective to devitalized tissue● Should not be used in presence of infection● Recommended type of debridement by AHCPR
guidelines

121
DO NOT DEBRIDE
● Dry, non-fluctuating eschar on heels
“Stable heel ulcers with a protective eschar covering are considered an exception to the recommendation that all eschar be debrided….a wound is stable if it is clean, dry, nontender, nonfluctuant, nonerythematous, and nonsuppurative. The eschar provides a natural protective cover. If any signs of complications appear, however, debridement is usually mandatory.” AHCPR Guidelines

122
Odor control
● Increase dressing changes, more aggressive cleansing
● Minimize necrotic tissue● Contain drainage● Antibiotics and antifungal agents i.e.,
metronidazole (metrogel), dakin’s solution● Charcoal dressings● Remember: Hydrocolloid dressings have a
natural odor

123
When a wound does not heal
● Inadequate circulation/perfusion● Unrelieved mechanical stress (pressure)● Systemic disease● Non-compliance● Edema● Infection/osteomyelitis● Cytotoxicity● Malnutrition
124
Dressing, dressing, which dressing????
What makes the ideal dressing??● Keep the wound moist, keep the skin dry● Free of toxic materials and fibers● Maintains warm, constant temperature● Prevents bacterial invasion● Prevents trauma on removal● Maintains pH● Allows gaseous exchange

125
No easy choice…..
There are well over 3500 products on
the market

126
Deciding the treatment…..
● This really is the hard part● Understand properties of wound care products● Differentiate various treatment options for
specific wound environments● Everyone needs to look at the wound the same
way● Everyone needs to understand the basic
principles of wound healing● Everyone needs to understand which products
are appropriate for each wound

127
Personal recommendations● Develop a formulary
◆ Get a group together, examine the products and decide which are best for your facility – choose company with multiple choices in size and style of dressing material
◆ Clean out your storage areas ◆ Get rid of inappropriate supplies
● Develop protocols and stick to them● Work with your Part B supplier or find one that
will work with you◆ Products can be reimbursed◆ Can develop systems to ensure right product is
delivered for right resident and billed to right account

128
If the wound is dry, moisten it
If the wound is wet, absorb it
“Since wounds and dressing techniques vary so much, it is impossible to specify the ideal dressing for all eventualities.”
George Winter

129
Dressing considerations● What does the wound bed look like?
● Is there non-viable tissue?
● Is there tunneling or undermining?
● How much exudate can you expect?
● How deep is the wound?
● What is the condition of the surrounding skin?
● How often should the dressing be changed?

130
Gauze
Disadvantages●Frequent dressings costly●Minimal absorption●Painful removal●Difficult to maintain moist wound bed●No barrier to contamination to wound bed
Indications●Primary dressing●Secondary dressing●Filler for dead space●Cleansing material●Mechanical debridement●Carrier for medication
Types●All purpose●Impregnated●Nonadherant●Packing material●Debriding material●Rolls for wrapping

131
Hydrogel
Indications●Partial or full thickness wounds●Dry to minimal exudate●Abrasions, minor burns or minor wounds●Autolytic debridement of necrotic / sloughing wound by increasing moisture content
Characteristics ●Available in gels, sheets, impregnated in gauze●Water or glycerin base●Non-adhesive●Limited absorptive ability●Hydrating effect softens eschar and promotes autolysis●Maintains or provides moist wound environment

132
Hydrogel (con’t)
Disadvantages●Requires a second dressing●May cause maceration if exudate increases●Difficult to keep in place on superficial wound
Advantages●Soothing, covers nerve endings●No residue in sounds●Easy to apply and remove●Easy to use, requires no mixing●Conformable

133
Indications●Superficial wounds with no or minimal drainage●Protect from friction and shear●Occlusion may reduce wound pain●Protect newly epithelialized area●Soften necrotic area
Characteristics●Polyurethane or copolyester composition with adhesive layer●Waterproof, protect from external contamination●Gas and oxygen permeable●Promotes autolysis of necrotic wounds●Maintains moist wound environment
Transparent dressing

134
Disadvantages●Can not use when signs of infection are present●Can tear healthy skin if removed improperly●Does not absorb – may macerate skin●Contraindicated with cavity wounds, undermining or tunneling
Advantages●Conformable●Transparent nature allows visualization of wound●Waterproof covering●May be left in place for several days
Transparent Dressing Con’t

135
Hydrocolloid Indications●Partial thickness (not full thickness) wounds with small to moderate exudate●Small full thickness wounds if absorptive filler used●Moisture may soothe nerves to reduce pain●Autolytic debridement by keeping moisture in contact with eschar●Not indicated for diabetic ulcers
Characteristics●Wafers, granules, pastes, powders●Absorbent components: gelatin, peptin, carboxymethly cellulose●Occlusive and adhesive●Reacts with wound fluid to form a gel that maintains a moist wound environment●Promotes autolytic debridement
Hydrocolloid

136
Hydrocolloid (con’t)Disadvantages●Melts down●Odor present when removed●Risk of hypergranulation●Impermeable to oxygen●Can not be used with infected wounds●May damage fragile periwound skin●Use for wounds with undermining, tunneling or cavity only with absorptive filler
Advantages●Waterproof●Prevents contamination●Easy to apply●Long wear time (3-5 days)●Variety of thickness – use thicker for higher amounts of exudate
Hydrocolloid Con’t
137
Alginate Indications
Partial or full thickness wound with moderate to heavy exudate
Non-healing surgical wounds, leg ulcers
Able to pack wound
Can use with contaminated or infected wound
Can use with bleeding surface wound
Provides autolytic debridement of moist, necrotic wounds
Characteristics
Non-woven fiber, cellulose-like polysaccharide, derived from seaweed
Absorbs up to 20 times weight
Pads, ropes
Interacts with wound fluid to form a moisture-vapor permeable gel creating a moist wound environment
Alginate

138
Alginate (con’t)Disadvantages●Will dry wound base if used in wounds with low volume of exudate●Always requires a secondary dressing
Advantages●Easy to apply●High capacity for absorption●May be used under compression●Useful for packing exudating wounds
Alginate con’t

139
Foam
Indications
Partial and full thickness wound with moderate to heavy exudate
Can be used with contaminated or infected wounds
Can be used as dead space filler in deep wounds
May control hypergranulation
Characteristics
Made of hydrophilic polyurethane foam
Semi-occlusive
Non-adherent to wound bed
Some have film backing on outer surface
Adhesive or non-adhesive sheets, pillows, wafers
Maintains moist wound environment
Foam

140
Disadvantages●Will dry wound base if used in wounds with low volume of exudate●Always requires a secondary dressing
Advantages●Easy to apply●High capacity for absorption●May be used under compression●Useful for packing exudating wounds
Foam Con’t

141
Other wound fillers/absorbers
● Various compositions such as gels, strands, beads, powders, granules and pastes
● Varying levels of absorption
● May fill in dead space
● May promote autolytic debridement
142
Composite dressing
Characteristics● Incorporates features of multiple
products into one
● Available as waterproof, with gauze, as tape, etc.
● Comes in multiple sizes and shapes
Indications● Acute wounds
● Abrasions and lacerations
● IV sites
● Surgical incisions
● Skin tears
● Primary or secondary dressing

143
Other methods
● Electric stimulation
● Ultrasound
● Laser
● Growth factors
● Hyperbaric oxygen

144
Review Dressing considerations
What does the wound bed look like? Is there non-viable tissue? Is there tunneling or undermining? How much exudate can you expect? How deep is the wound? What is the condition of the surrounding skin? How often should the dressing be changed?

145
Recipes
● Ensure consistency● Limit choices ● Limit confusion● Right product for the right wound● Easier order writing● Easier transcription● Add your favorite brands (by team decision)● Work with vendors to secure best price● Educate staff to “sing out the the same book”

146
Step one
Always clean the wound before dressing it
147
Wound Cleansing
● Remove surface contaminants◆ Bacteria◆ Excess exudate◆ purulence
● Methods◆ Normal Saline◆ Wound cleansers
● Cleanse initially and at each dressing change● Use enough irrigation pressure to enhance
wound cleansing without causing trauma

148
Wound Cleansing (con’t)
● “Saline irrigation is a safe and appropriate method of wound cleansing for most ulcers” AHCPR Guidelines
● Other cleansers◆ Antimicrobial◆ Non-irritating◆ No-rinse
● Always cleanse gently

149
Stage I● Assess and eliminate etiology
◆ Pressure ■ Pressure reduction surface■ Turn/reposition at least q2 hours; positioning devices■ Do not massage area■ Limit out-of-bed time
◆ Moisture■ If due to wound exudate, protect intact skin with zinc based cream■ If due to feces or urine, apply protective barrier cream
◆ Friction ■ Apply moisturizer (non-alcohol) to dry areas■ Apply film dressing to cover high friction area
◆ Shear■ Maintain head of bed below 30 degrees■ Use draw sheet for repositioning

150
Stage II
Film with or without hydrogel to soften, create autolytic debride
Wound bed: slough/necrotic
Exudate: minimal
Thick hydrocolloid or foam for moist wound bed and to absorb exudate
Wound bed: clean
Exudate: moderate/heavy
Thin hydrocolloid for moist wound bed and exudate absorb
Wound bed: clean
Exudate: minimal
Film dressing for moist wound bed maintenance
Wound bed: clean
Exudate: none
Options Assessment
151
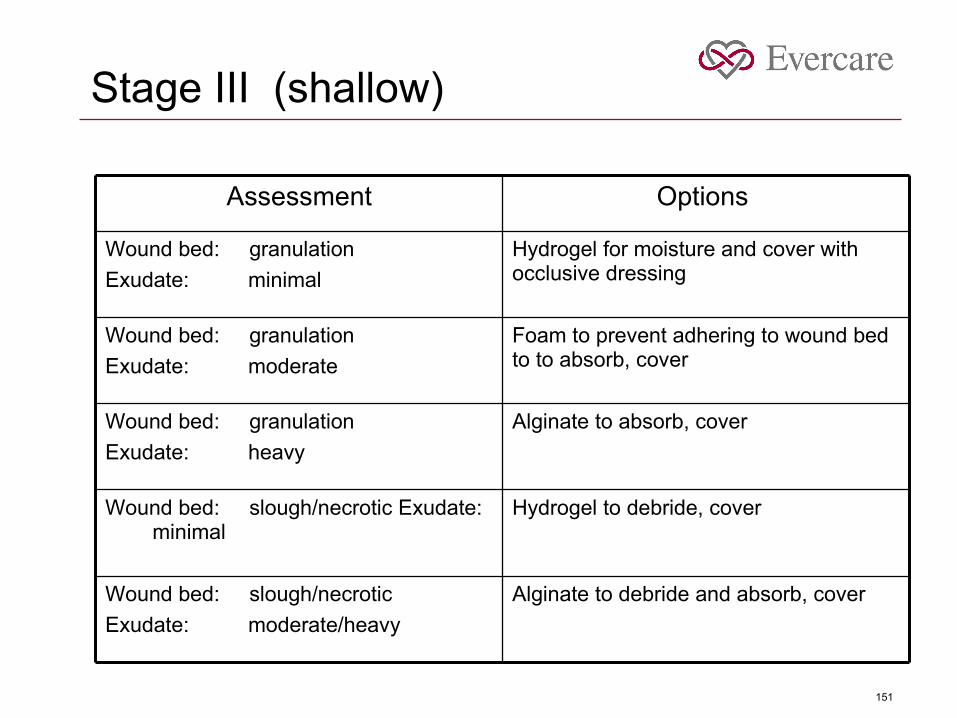
e III (
Alginate to absorb, coverWound bed: granulation
Exudate: heavy
Alginate to debride and absorb, coverWound bed: slough/necrotic
Exudate: moderate/heavy
Hydrogel to debride, coverWound bed: slough/necrotic Exudate: minimal
Foam to prevent adhering to wound bed to to absorb, cover
Wound bed: granulation
Exudate: moderate
Hydrogel for moisture and cover with occlusive dressing
Wound bed: granulation
Exudate: minimal
Options Assessment
Stage III (shallow)

152
Stage III (deep) / Stage IV
Foam or alginate to fill, debride and absorb, cover
Wound bed: slough/necrotic
Exudate: moderate/heavy
Hydrogel, non-adhesive filler to debride, cover
Wound bed: slough/necrotic
Exudate: minimal
Foam or alginate to fill and absorb, cover
Wound bed: granulation
Exudate: moderate/heavy
Hydrogel, non-adhesive filler, coverWound bed: granulation
Exudate: minimal
Options Assessment
Stage III (deep) / Stage IV

153
Suggestions ● Assess the wound before you determine the
product(s) you need – always monitor for infection
● Read your product inserts to determine the product recommendations for use
● Limit the number of products in use by facility to lessen confusion and reduce cost
● Be consistent. If wound worsens after two weeks, re-assess product
● Be clear when writing orders so all understand what the recipe is
● Have your Medical Director sign off on protocols● Send copy to all MD’s on staff with cover letter
from Medical Director

154
Writing / transcribing orders
● Make labels (see sample) for each wound stage ◆ Be very specific, include product name
● Store in file separated by stage (portable file box)◆ Pre-printed care plan◆ Pre-printed order sheet for vendor◆ Bring file box to weekly wound meeting for re-fill
● Use one label for physician’s order page● Could use a label for Telephone order sheet (if
facility uses them)● Use one label for treatment sheet (add date)

155
Sample treatment order
Use two entries, one for the dressing and one for the monitoring
● Box 1:
Wash wound (specify site) with normal saline, pat dry with 4X4. Prep skin surrounding wound with Skin Prep and allow to dry for 20 seconds. Apply Alevyn Adhesive to (specify site) extending at least two inches beyond wound edges. Frame with dressing tape. Replace and reassess every five days or sooner if soiled, wrinkled or loose.
● Box 2:
Monitor dressing (specify site) every shift.

156
Work with your Part B vendor
● See order form● Specify size of wound and location and let the
vendor send you the appropriate dressing material
◆ Vendor can place in zip lock bag with resident name which can be stored in treatment cart
● Have an “emergency kit” ready to start treatments – same principles as emergency med kit for tracking/billing
● Instruct vendor to bill by resident● Facility billing office can bill Part B for dressing
supplies

157
OR…..
● Set up your own central supply system
● Consider increasing your buying power by “grouping” with other facilities/organizations
◆ Dressing products◆ Specialty beds / chair cushions◆ Positioning devices
● Work with a product manufacturer

158
Forms
● Repositioning/Turn schedule form● Braden● Weekly skin assessment● Care Plans● Weekly Pressure Ulcer Summary
● Add to your Nursing Assistant documentation record – preventative measures, i.e., barrier cream application after incontinent care, use of adaptive equipment, etc.

159
Facility Education Programs
● Structured● Organized● Comprehensive
● Stress roles of Dietician, PT, OT, Assistants

160
Comprehensive education
● Etiology and risk factors● Risk assessment and contributing factors● Skin assessment● Selection and/or use of support surfaces● Development and implementation of an
individualized program of skin care● Demonstration of positioning to decrease risk of
tissue breakdown● Instruction on accurate documentation of
resident care

161
● Instruction on accurate documentation of
pertinent data● Information on pain, discomfort, possible
outcomes and treatment strategies● Assessment of tissue damage● Pathology of pressure ulcers● Risk factors● Staging terminology● Principles of wound healing● Principles of nutritional support● Principles of cleansing and infection control● Product selection● Documentation principles

162
● Case studies