iron overload in thalassemia major and sickle cell disease · pdf fileiron overload in...
TRANSCRIPT

Iron overload in thalassemia major
and sickle cell disease
Dr Fleur Samantha Benghiat
Brussels, Belgium
21.11.2015

DISCLOSURES
None

THIS TALK IS APPLICABLE FOR :
Definite Probable
Thalassemia’s X
Sickle cell disease X
Membrane disorders (e.g. sferocytosis)
Enzym defects (e.g. PKD, G6PD)
PNH
Other forms of hemolytic disease

LEARNING OBJECTIVES
1. Red blood cells (RBC)
Life of a RBC
Hemoglobin
Sickle cell disease
Thalassemia Major
Chronic blood transfusion
2. Iron
Distribution of iron
Iron overload
Iron toxicity
Associated complications
Diagnosis
Treatment: Iron chelators

RED BLOOD CELLS
BONE MARROW ERYTHROPOIESIS
Red blood cells =
Erythrocytes
O2 RBC FUNCTION
= Oxygen transportation

HEMOGLOBIN
O2
O2 O2
O2
Oxygen binds to iron on the hemoglobin molecule
Each red blood cell contains several thousand hemoglobin molecules
b-chain
b-chain a-chain
a-chain

THALASSEMIA MAJOR : NO b-CHAIN PRODUCTION
BONE MARROW INEFFECTIVE ERYTHROPOIESIS
SEVERE ANEMIA
IRON OVERLOAD
IRON ABSORPTION +++ MARROW EXPANSION
b-chain a-chain

SICKLE CELL DISEASE : MUTATION ON THE b-CHAIN
SICKLE CELL
RBC Destruction
ANEMIA
Vaso-occlusion
Chronic Organ Damage
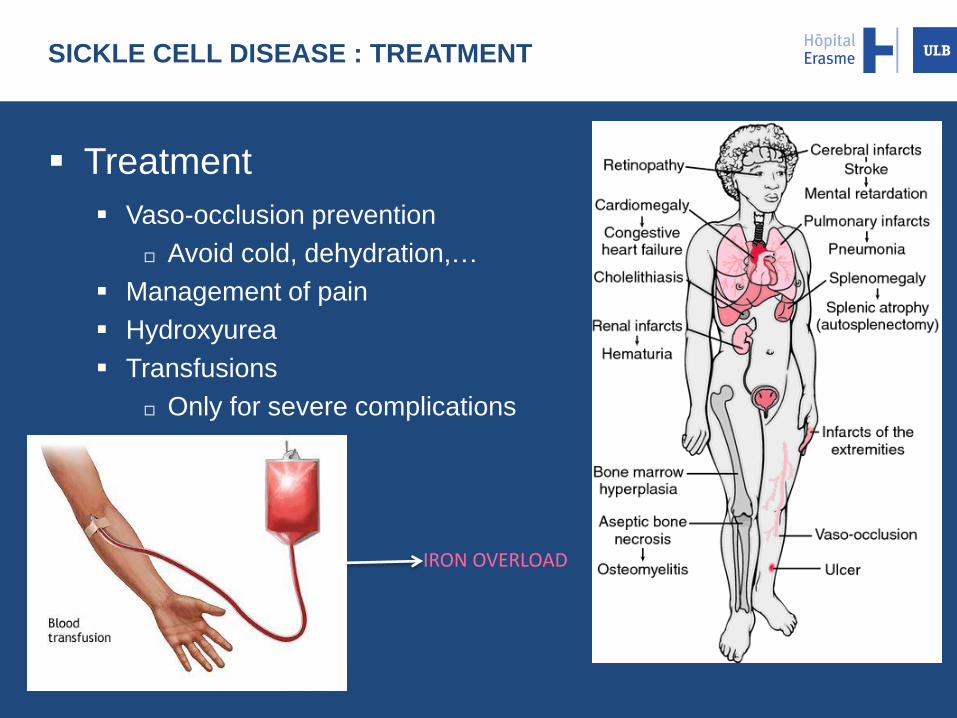
SICKLE CELL DISEASE : TREATMENT
Treatment
Vaso-occlusion prevention
Avoid cold, dehydration,…
Management of pain
Hydroxyurea
Transfusions
Only for severe complications
IRON OVERLOAD

LEARNING OBJECTIVES
1. Red blood cells (RBC)
Life of a RBC
Hemoglobin
Sickle cell disease
Thalassemia Major
Chronic blood transfusion
2. Iron
Distribution of iron
Iron overload
Iron toxicity
Associated complications
Diagnosis
Treatment: Iron chelators

IRON : NORMAL DISTRIBUTION
STORAGE = 1000mg
Skin Gut
Menstruation Pregnancy
Pietrangelo A. NEJM 2004; 350:2383-2397
Total body iron = 4000 mg
Transferrin

IRON OVERLOAD
21.11.2015
Iron In
200mg/unit
STORAGE
No mechanism to excrete excess iron
CIRRHOSIS
Iron Chelator
Iron Out
Total body iron = 4000 mg
3U/month = 600mg/month 7,2 g/year

Pituitary → impaired growth, infertility
Thyroid → hypothyroidism
Heart → cardiomyopathy, heart failure
Liver → hepatic cirrhosis, cancer
Pancreas → diabetes mellitus
Gonads → hypogonadism
COMPLICATIONS OF IRON OVERLOAD
In the absence of treatment
Damages are inevitable
Lethal complications

IRON OVERLOAD MEASUREMENT
v
v
v American association for cancer research
v
v v
v
v v
↑ Ferritin ≠ ↑ Iron burden
BUT
↓ Ferritin = ↓ Iron burden
Liver Iron Concentration (LIC)
• LVEF measurement v
Liver and cardiac MRI (Magnetic Resonance Imaging)

MAGNETIC RESONANCE IMAGING (MRI)
= GOLD STANDARD
Heart
Liver
Before treatment After treatment

TREATMENT : WHAT IS CHELATION THERAPY?
Chelate
Chelator Iron Chelator
Toxic
Excretion Iron
With the courtesy of Dr Axelle Gilles

IRON CHELATION THERAPY IMPROVES
SURVIVAL IN THALASSAEMIA
Olivieri NF, et al. N Engl J Med. 1994;331:574-8
Well treated Ferritin < 2500
Poorly treated Ferritin > 2500

TREATMENT : AIM? WHEN TO START?
Prior transfusions
Evidence of chronic
iron overload
OR OR
After 120 mL/kg pRBC
(~ After 10-20 units)
Serum ferritin > 800 - 1000 μg/L1,2
(constantly)
OR
LIC ≥ 5 - 7 mg Fe/g dw1,2
Therapeutic
Goal3
• PREVENTION • Remove transfused iron
• RESCUE • Reduce the existing iron burden
• Slow, less efficient
• Damages often irreversible
1. Treating iron overload in patients with non-transfusion-dependent thalassemia. Taher AT et al. Am J Hematol. 88 : 409-415, 2013 2. Consequences and management of iron overload in sickle cell disease. Porter J, Garbowski M. Hematology Am Soc Hematol Educ Program. 2013:447-56 3. Porter J., Viprakasit V. Iron overload and chelation - Guidelines for the Management of Transfusion Dependent Thalassaemia, 3rd Edition (2014)
When to start chelation:

Property Deferoxamine Deferiprone Deferasirox
Usual dose
(mg/kg/day) 25–50 75–100 20–40
Route
sc, iv
(8–12 hours,
5 days/week)
Oral
3 times daily
Oral
Once daily
Half-life 20–30 minutes 3–4 hours 12–16 hours
Excretion Urinary, fecal Urinary Fecal
Adverse
effects
Local reactions,
Auditory,
Ocular,
Growth retardation,
Allergy
GI,
agranulocytosis,
neutropenia,
Arthralgia,
Liver enzymes ↑
GI,
rash,
creatinine level ↑
Indication Transfusional iron
overload
Iron overload in TM
when DFO is CI or
inadequate
Transfusional iron
overload
SCD: if DFO inadequate
TREATMENT : IRON CHELATING AGENTS
Adapted from Brittenham GM. N Engl J Med 2011;364:146

Side effect Frequency Management Recommendations
Nausea, vomiting Abdominal pain
15-26% Transient Evening, with or after food Divide dose / ↓ dose then ↑
• Renal and hepatic functions
1x/week (1st month) 1x/month • Urinanalysis 1x/month • Auditory and
ophtalmic testing 1x/year
Diarrhea (! Lactose) 5 – 20% Lactase / Loperamide /↓ dose
Rash 7-11% Transient Short course corticoids STOP - Start lower dose
Creatinine ↑ >33% 38% ↓ dose by 10mg/kg / STOP
Proteinuria 19% ↓ dose or STOP if >1mg/g creat
Liver enzyme ↑ 2 – 8% STOP - Start lower dose
Teratogenic in animals STOP before pregnancy
SIDE EFFECTS MANAGEMENT : DEFERASIROX
Transfusional iron overload and iron chelation therapy in thalassemia major and sickle cell disease. Marsella M et al. Hematol Oncol Clin North Am. 2014 Aug;28(4):703-27

Side effect Frequency Management Recommendations
Nausea, abd pain, diarrhea
3 – 25% 3%
Transient If not, Loperamide, ↓ dose
• Neutrophil count 1x/week
• Avoid other
neutropenia-inducing drugs
• Hepatic and renal functions
Neutropenia (500-1500/mm³)
7% STOP Neutro count 1x/d (> 1500) Re-Start with caution
Agranulocytosis (< 500/mm³)
2% STOP definitely, AB if infection G-CSF
Liver test ↑ 8% Transient If not, ↓ dose then ↑
Teratogenic in animals Contraception Stop before pregnancy
SIDE EFFECTS MANAGEMENT : DEFERIPRONE
Transfusional iron overload and iron chelation therapy in thalassemia major and sickle cell disease. Marsella M et al. Hematol Oncol Clin North Am. 2014 Aug;28(4):703-27
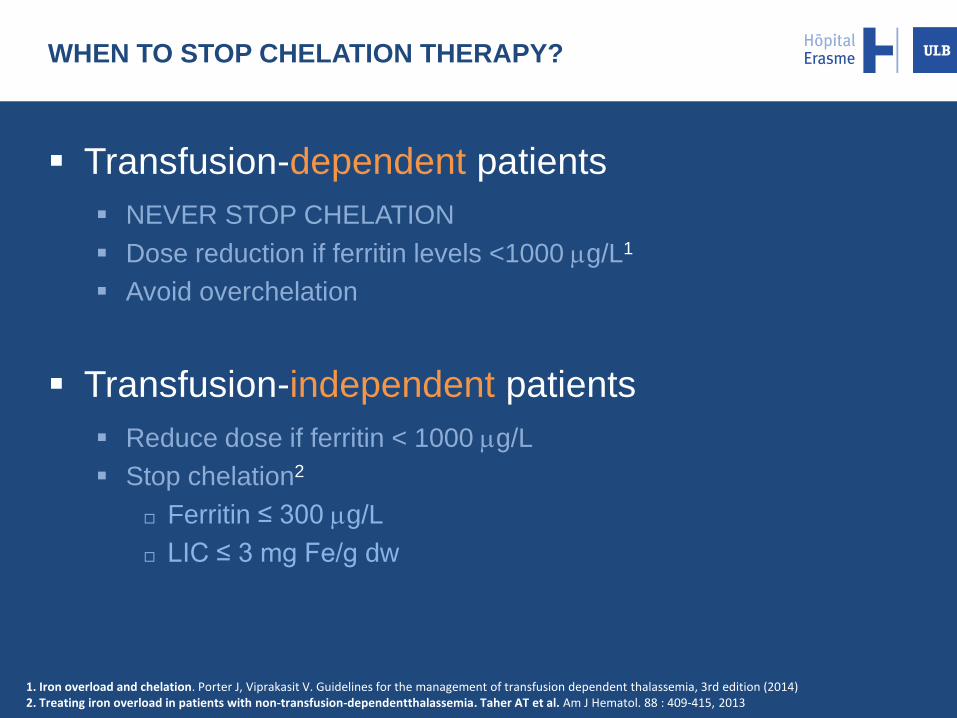
WHEN TO STOP CHELATION THERAPY?
Transfusion-dependent patients
NEVER STOP CHELATION
Dose reduction if ferritin levels <1000 mg/L1
Avoid overchelation
Transfusion-independent patients
Reduce dose if ferritin < 1000 mg/L
Stop chelation2
Ferritin ≤ 300 mg/L
LIC ≤ 3 mg Fe/g dw
1. Iron overload and chelation. Porter J, Viprakasit V. Guidelines for the management of transfusion dependent thalassemia, 3rd edition (2014) 2. Treating iron overload in patients with non-transfusion-dependentthalassemia. Taher AT et al. Am J Hematol. 88 : 409-415, 2013

CONCLUSION : ADHERENCE TO CHELATION THERAPY
Adherence = Success
Therapeutic alliance Doctor + Patient
Involvement of patients in decisions self-management
Reviews of results (MRI, ferritin levels…)
Administration
prefer oral
Side effects
Strict control
Monitoring Prevention
Dose adjustment
Transfusional iron overload and iron chelation therapy in thalassemia major and sickle cell disease. Marsella M et al. Hematol Oncol Clin North Am. 2014 Aug;28(4):703-27


SICKLE CELL DISEASE : TRANSFUSION THERAPY
Acute: simple transfusion Chronic: transfusion program
• Surgery (selected cases)
• Severe symptomatic anemia
Splenic sequestration
Severe or long-lasting aplastic crises
• Severe complications
Acute CNS stroke
Acute chest syndrome
Multiple-organ failure syndrome
• Prevention of severe complications
Prophylaxis against recurrent stroke
Prevention of 1st episode of stroke in high-risk
pediatric patients
• Hydroxyurea non-responders
• Severe chronic complications
Chronic pulmonary hypertension
Heart failure
Adapted from Stuart MJ et al. Lancet 2004;364:1343–1360; Vichinsky E. Semin Hematol 2001;38:2–4
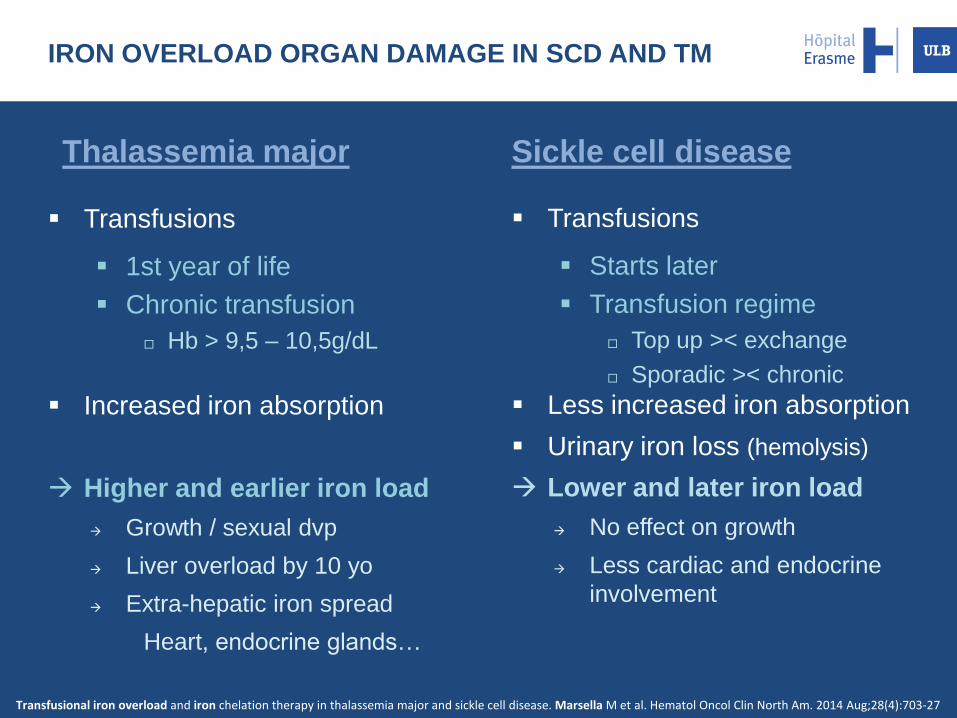
Sickle cell disease
Transfusions
Starts later
Transfusion regime
Top up >< exchange
Sporadic >< chronic
Less increased iron absorption
Urinary iron loss (hemolysis)
Lower and later iron load
No effect on growth
Less cardiac and endocrine
involvement
Thalassemia major
Transfusions
1st year of life
Chronic transfusion
Hb > 9,5 – 10,5g/dL
Increased iron absorption
Higher and earlier iron load
Growth / sexual dvp
Liver overload by 10 yo
Extra-hepatic iron spread
Heart, endocrine glands…
IRON OVERLOAD ORGAN DAMAGE IN SCD AND TM
Transfusional iron overload and iron chelation therapy in thalassemia major and sickle cell disease. Marsella M et al. Hematol Oncol Clin North Am. 2014 Aug;28(4):703-27

IRON TOXICITY
FREE RADICALS OXIDATIVE DAMAGE
TISSUES IRON OVERLOAD
Loss of mitochondrial membrane potential
Loss of respiratory enzyme activities
Apoptosis Lipid peroxidation
Increased lysosomal fragility CELL DEATH – FIBROSIS
With the courtesy of Dr Axelle Gilles
INFECTIONS CANCER

Pituitary → LH, FSH, GH, ACTH
Para/Thyroid → TSH, T3, T4 – PTH, D-Vit, Ca, P
Heart → MRI T2*, LVEF, EKG
Liver → MRI T2*, abdominal echography
Pancreas → Glycemia, Oral Glucose Tolerance Test
Gonads → Estradiol, Progesteron, Testosteron
IRON OVERLOAD – WORK UP