improving maternity care quality for minnesota...
TRANSCRIPT

Improving maternity care quality for Minnesota mothers
Katy B. Kozhimannil, PhD, MPA University of Minnesota School of Public Health
MN Health Action Group
August 8, 2013
Overview
• Background on childbirth in the U.S.
• A new focus: variability
• Key findings from recent research
– Cesarean rates
– Differences by payer
– Rural/urban differences
– Doula care (continuous labor support)
• Next steps: how to incentivize change
Childbirth care in the U.S.
• Childbirth is the most common reason for hospitalization in the U.S.
• Cesarean delivery is the most common operating room procedure in the U.S.
• Recent changes in care (in 2009) – Cesarean rate of 32.9% (5.5% in 1970)
– Induction rate of 23.1% (9.5% in 1990)
Sources of information about birth
• Valuable sources of information – Maternity care provider was most valuable source for both
first time (76%) and experienced (82%) mothers – Other sources identified as very valuable by at least 50% of
moms who used them were childbirth education classes and pregnancy/ childbirth websites
– Apps were rated more highly by first-time mothers (56% “very valuable”) than experienced mothers (47%)
• Trustworthiness of sources of information – 47% identified maternity care providers as “completely
trustworthy” and an additional 33% as “very trustworthy.” – Childbirth education classes, one’s health plan, and
general medical or health websites received the next highest ratings of trustworthiness
Choosing a maternity care provider • Percent listing these as a “major
factor”: – accepting their insurance (85%)
– good match for what I value and want (69%)
– attended births at a hospital I like (68%)
– provided prenatal care in previous pregnancy (62%, asked of experienced mothers only)
– provided well-woman care (60%)

Types of clinicians who care for women during pregnancy and birth
• Primary birth attendant 2011/2012: – Obstetricians (70%)
– midwives (10%)
– family physicians (6%)
– doctor of unknown specialty (7%).
• Doulas supported 6% of women during childbirth
• Women report their delivery attendant was someone she had either met briefly (12%) or had never met (21%)
• More than 60% of all women reported care from more than one type of clinician during pregnancy (2010)

Where women give birth in the U.S.
• Hospital (99%)
• Out of hospital settings (1%)
– Licensed birth center (1/3 of non-hospital births)
– Home birth (2/3 of non-hospital births)

Changes in delivery mode in the U.S.
• Cesarean delivery is the most frequently performed inpatient surgical procedure in U.S. hospitals
• Commonly named reasons:
– Increase in conditions that may necessitate cesarean delivery
– women requesting elective cesareans
– concerns about liability and malpractice
Cesarean: clinical benefits and risks • Cesarean delivery is an important, potentially lifesaving
surgery with demonstrated capacity to improve patient outcomes.
• Cesarean-related risks: – Intrapartum maternal risks (increased risk of
infection, surgical injury, blood clots, and emergency hysterectomy.)
– Immediate postpartum risks (higher rates of rehospitalization following childbirth, breastfeeding challenges, pain)
– Longer term maternal risks (future pregnancies - placenta previa, placenta accreta, placental abruption, and uterine rupture)
– Potential neonatal risks (increased rates of asphyxia, respiratory distress, and other pulmonary disorders)

Cesarean delivery in a systems context
• Total costs (maternal and neonatal) – Commercial $18,328 (vaginal), $27,866 (cs) – Medicaid $9131 (vaginal), $13590 (cs)
• Hospital charges for maternal and neonatal conditions exceed those for all other conditions • Nearly half of all births in the U.S. are covered by public
health insurance (Medicaid) – $3 billion for cesarean delivery in 2009
• Healthy People 2020: 10% reduction in both primary and repeat cesarean rates – from 26.5 to 23.9% and 90.8 to 81.7%, respectively

The “relentless rise”
• Increases over time – rising 60% from 1996 to 2009
• Since 2009, the cesarean rate has not increased
Vaginal Birth After Cesarean Delivery: A Common-Sense Approach. Scott, James Obstetrics & Gynecology. 118(2, Part 1):342-350, August 2011. DOI: 10.1097/AOG.0b013e3182245b39



Variation in procedure rates
• Variation in procedure rates is an important indicator of quality – potential underuse or overuse of service, which
may be both clinically harmful and costly
• Most prior research on variation in care in the U.S. focuses on the Medicare population – conditions affecting older adults
– does not commonly include women of reproductive age

Shifting the focus to variability
• Some potential sources of variability
– Hospital
– Payer
– Geography
– Support

Data issues
Data problems – Linked data (mom and baby) – Gestational age, medical codes, charting, midwifery,
doulas….
Data used – Nationwide Inpatient Sample (NIS) of the Healthcare
Cost and Utilization Project (HCUP) • All discharge records for a 20% sample of hospitals
– Birth certificate data from the CDC’s National Center for Health Statistics (NCHS)
– Listening to Mothers Surveys – Community data, provider data

Key findings from recent studies
• Hospitals: 15-fold variation in low-risk cesarean rates
• Payers: Cesarean rates increasing more rapidly among private vs. publicly insured births
• Location: Rising rates of low-risk cesarean and low VBAC rates are problematic in both rural and urban areas
• Support: Doula-supported births are associated with lower cesarean rates
Key findings – hospital variation
• Hospital cesarean rates vary substantially across the U.S. Hospital cesarean rates varied 10-fold across the U.S., from 7% to 70%.
• In 2009, low-risk hospital cesarean delivery rates varied 15-fold across facilities with at least 100 deliveries.
• Large variations around increasing cesarean rates indicate that differences in practice patterns may be driving costly potential overuse of cesarean in many U.S. hospitals.
Kozhimannil KB, Law MR, Virnig BA. Cesarean delivery rates vary 10-fold among US hospitals; reducing variation may address quality and cost issues. Health Affairs. 2013;32(3)527-535
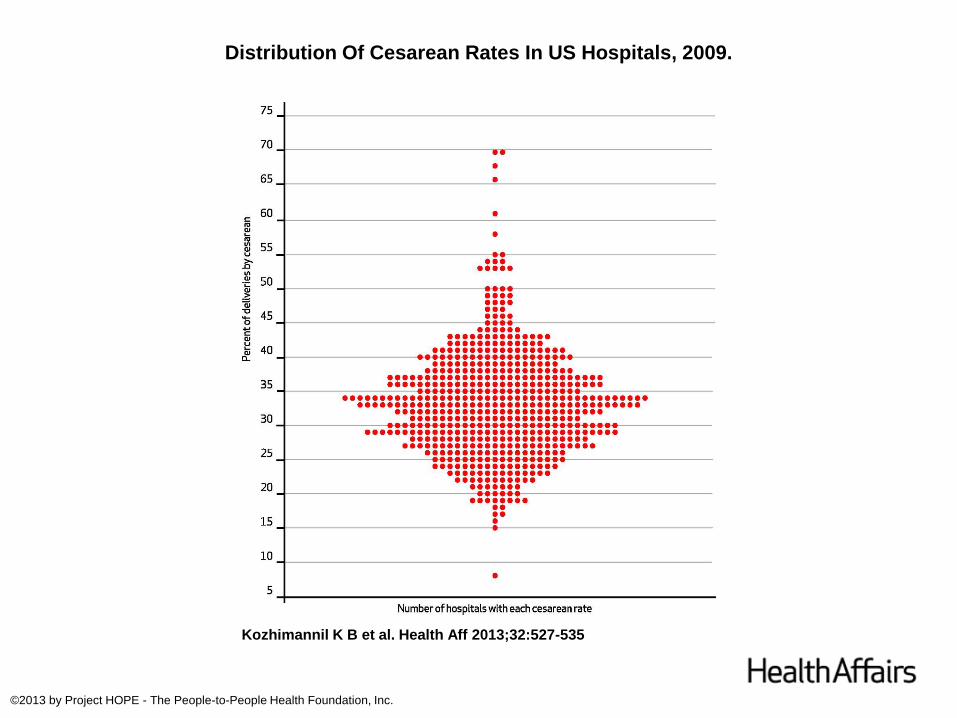
Distribution Of Cesarean Rates In US Hospitals, 2009.
Kozhimannil K B et al. Health Aff 2013;32:527-535
©2013 by Project HOPE - The People-to-People Health Foundation, Inc.

Distribution Of Cesarean Rates In US Hospitals Among Lower-Risk Pregnancies, 2009.
Kozhimannil K B et al. Health Aff 2013;32:527-535
©2013 by Project HOPE - The People-to-People Health Foundation, Inc.

Key findings – who pays? From 2002 to 2009:
• Obstetric intervention rates increased over time for all births, regardless of payer.
• Presence and type of health insurance affected hospital-based childbirth care; births covered by private insurance had higher rates of obstetric intervention compared with Medicaid-funded births.
• Controlling for individual and hospital-level factors, the cesarean delivery rate increased more rapidly for births covered by private insurance, compared with Medicaid.
In Minnesota, Medicaid 20.9% c/s rate; private ins 27%.
Kozhimannil KB, Shippee TP, Adegoke O, Virnig BA. Trends in hospital-based childbirth care: the role of health insurance. American Journal of Managed Care, 2013;19(4):e125-e132.

Kozhimannil KB, Shippee TP, Adegoke O, Virnig BA. Trends in hospital-based childbirth care: the role of health insurance. American Journal of Managed Care, 2013;19(4):e125-e132.
Key findings – rural/urban differences
• Rising cesarean rates for low-risk pregnancies and limited VBAC access are problematic for both rural and urban hospitals. – Low risk cesarean rates ~16% in 2010 (both rural and
urban hospitals) – VBAC rates 10% urban, 5% rural in 2010
• Rates of non-indicated labor induction rose overall, but increased more rapidly in rural vs. urban hospitals. – 16.5% of women with no indication had labor induced
in rural hospitals in 2010
Kozhimannil KB, Hung P, Prasad S, Casey M, Moscovice IS. Geographic variation in obstetric care trends, 2002-2010. Under review.

The role of doula support • RCT evidence shows continuous labor support is
associated with positive birth outcomes
• Women with continuous labor support have: – higher rates of spontaneous vaginal birth
– lower odds of cesarean delivery
– lower rates of regional anesthesia (i.e. epidural)
– lower rates of instrument-assisted delivery (i.e. forceps and vacuum)
– shorter labors
– higher levels of satisfaction
Key findings – doula support
• The cesarean rate was 22.3% among doula-supported births and 31.5% among Medicaid beneficiaries nationally.
• After control for clinical and sociodemographic factors, odds of cesarean delivery were 40.9% lower for doula-supported births
• Potential cost savings to Medicaid programs associated with such cesarean rate reductions are substantial but depend on states’ reimbursement rates, birth volume, and current cesarean rates.
Kozhimannil KB, Hardeman R, Attanasio L, Blauer-Peterson C, O’Brien M. Doula care and birth outcomes: the potential for improving care and reducing costs for diverse, low-income women. American Journal of Public Health, 2013;103(4): e113–e121.

Minnesota statute change
Sec. 11. Minnesota Statutes 2012, section 256B.0625, is amended by adding a subdivision to read: Subd. 28b. Doula services. Medical assistance covers doula services provided by a certified doula as defined in section 148.995, subdivision 2, of the mother's choice. For purposes of this section, "doula services" means childbirth education and support services, including emotional and physical support provided during pregnancy, labor, birth, and postpartum. EFFECTIVE DATE. This section is effective July 1, 2014, or upon federal approval, whichever is later, and applies to services provided on or after the effective date.
• Birth is a cultural process
• Cultural concordance in medical care is associated with improved outcomes
• In order to recruit doulas from diverse communities,
– Insurers should pay
– Improve feasibility of a doula care business model for a wider range of women
– Trainings need to be accessible/available
In addition to financial access, cultural access

Implications • Efforts to decrease variation are warranted
and may focus on:
– improving access to evidence-based care
– quality measurement and public reporting
– management practices in hospitals
– patient-centered decision-making
Maternity care measurement
• NICHD/ACOG/SMFM recommendations (Spong 2012) – Rate of nonmedically indicated cesarean delivery – Rate of nonmedically indicated induction – Rate of labor arrest or failed induction diagnosed without
meeting accepted criteria – Rate of cesarean deliveries for nonreassuring fetal heart
rate by NICHD category • Note lack of standards for these measures
• Joint Commission – Perinatal Care Core measures (5)
• NQF – Endorsed measures list
How should rates be reported
• Hospital rates (NY example)
– New York State Public Health Law: § 2803-j. Information for Maternity Patients
– http://www.health.ny.gov/statistics/facilities/hospital/maternity/
• Provider group rates (MNCM example)
– 2012 Health Care Quality Report
• Individual providers?

Ways to incentivize change
• Structural changes – Coding, payment systems (e.g. doulas) or
structures (e.g. bundled payments, blended rates)
• Political changes – Potential resistance/concerns from clinicians,
patients, or employees
• See: Catalyst for Payment Reform Action Brief (http://www.catalyzepaymentreform.org/images/documents/maternity)

Discussion points
• What do we (employers, health plans, providers, patients) want for pregnant women and their families?
– Good quality measures that focus on outcomes we care about
– Coordination of care across settings and providers
– Shared decision-making and engaged patients
• How to get there from here?
Acknowledgments
• Collaborators – University of Minnesota Medical School – University of British Columbia – Minnesota Population Center – University of Minnesota Rural Health Research Center – Everyday Miracles
• Funding – University of Minnesota’s Building Interdisciplinary
Research Careers in Women’s Health (BIRCWH) Program (5K12HD055887), funded by NICHD and NIA, administered by ORWH
