immunity & abnormal responses pathophysiology. diseases to be discussed: tissue rejection...
TRANSCRIPT

Immunity & Abnormal ResponsesImmunity & Abnormal Responses
PathophysiologyPathophysiology
• Diseases to be discussed:• Tissue rejection
» Includes Organ transplant rejection
• Hypersensitivity reactions» These are hyperactive responses of the
immune system
» Called allergies
• Autoimmune reactions» A misdirected immune response
• Immunodeficiency» A deficient immune response
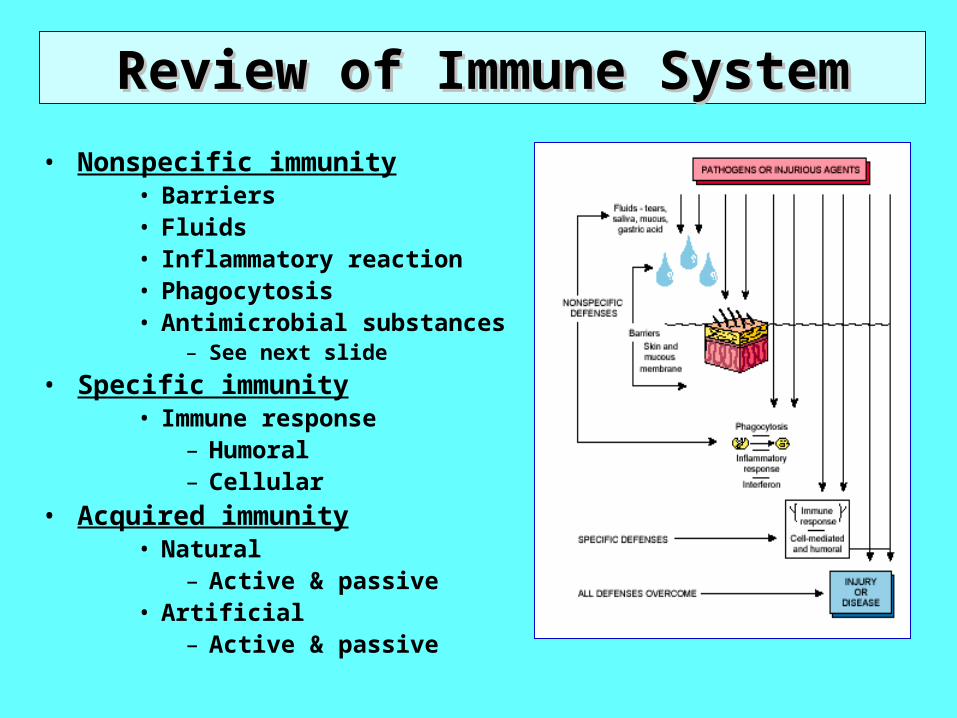
Review of Immune SystemReview of Immune System
• Nonspecific immunity• Barriers• Fluids • Inflammatory reaction• Phagocytosis• Antimicrobial substances
– See next slide
• Specific immunity• Immune response
– Humoral – Cellular
• Acquired immunity• Natural
– Active & passive• Artificial
– Active & passive
Non-specific Immunity System Molecules• Complement system
– Group of inactive plasma proteins, part of non-specific immunity
– Especially active against invading bacteria
– When activated, system compliments action of antibodies by;
– Destruction of target cell membranes
– Attracts phagocytes (chemotaxis)
– Stimulates & enhances phagocytosis
– Stimulates inflammation
– Activation occurs via:
– Compliment binding to IgM or IgG antibody- antigen complex
– Compliment attaching to foreign materials, e.g. bacterial cell wall
• Interferon– Especially active against viruses
– Small proteins released by lymphocytes & macrophages (primarily T-lymphocytes) when these cells activated by viral antigens
– Interferons do 2 basic things– Bind to normal body cell with virus & via second messenger stimulate the
production of antiviral proteins in cytoplasm which stop viral replication
– Act as cytokines to stimulate production of more macrophages & lymphocytes
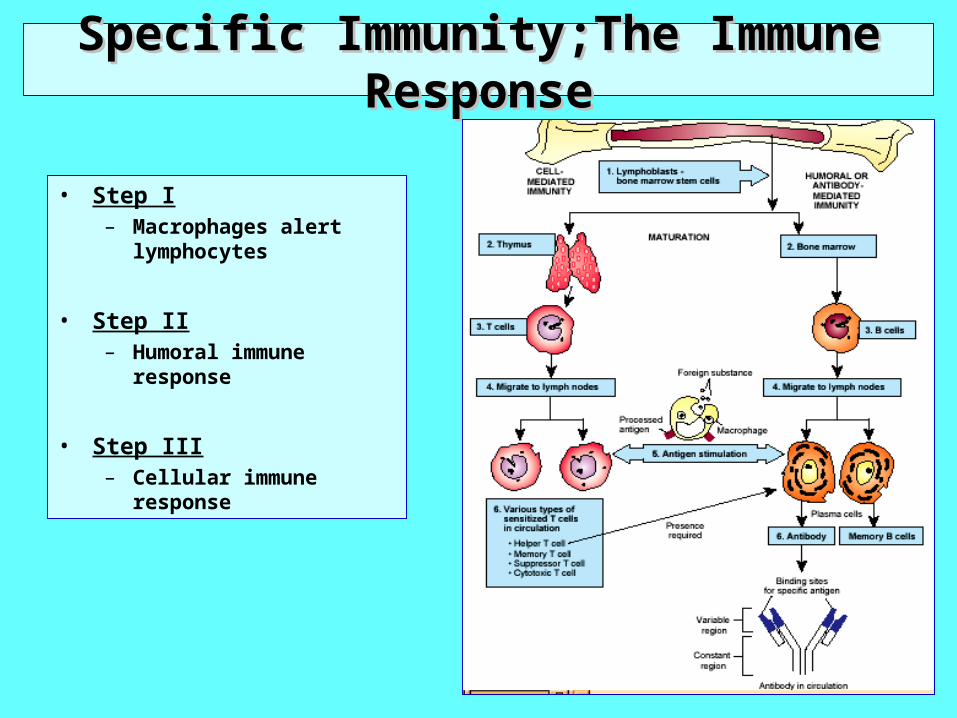
Specific Immunity;The Immune ResponseSpecific Immunity;The Immune Response
• Step I– Macrophages alert
lymphocytes
• Step II– Humoral immune response
• Step III– Cellular immune response
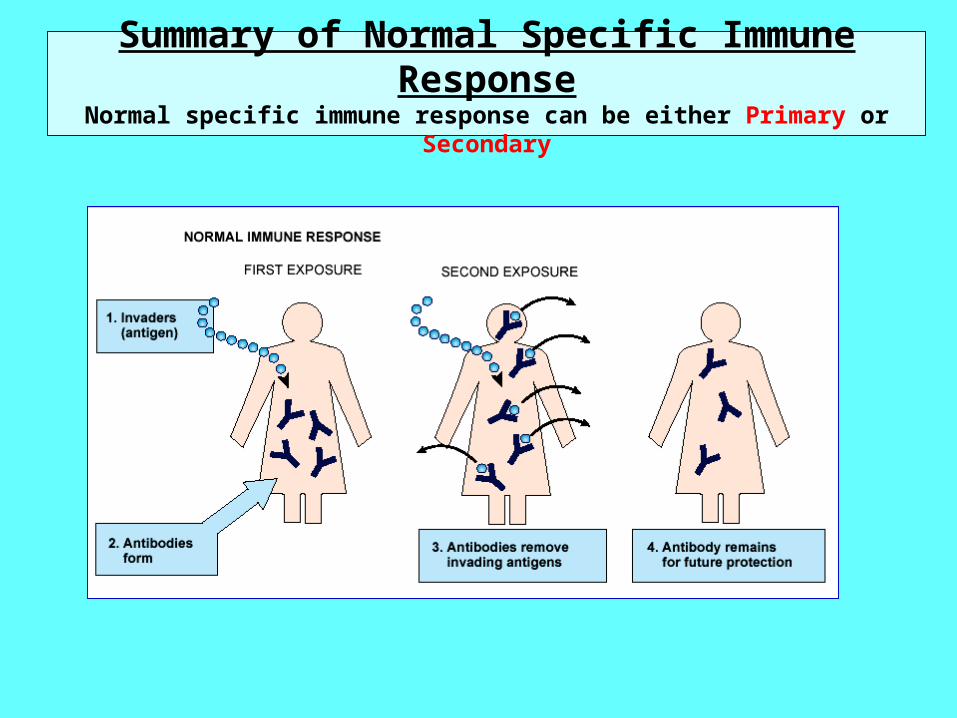
Summary of Normal Specific Immune ResponseNormal specific immune response can be either Primary or Secondary
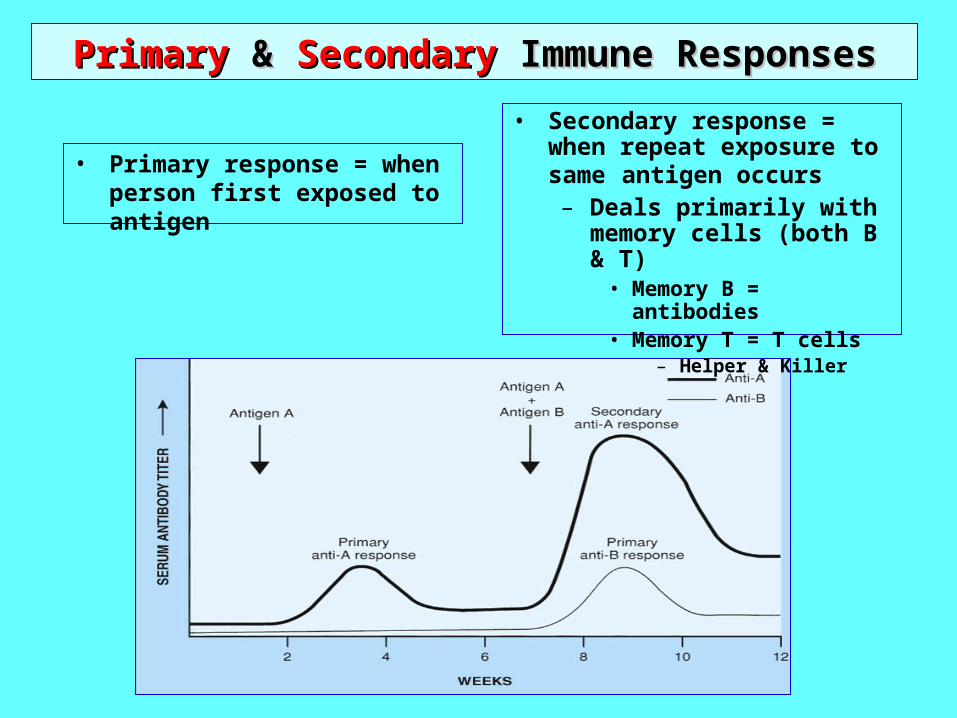
PrimaryPrimary & & SecondarySecondary Immune Responses Immune Responses
• Secondary response = when repeat exposure to same antigen occurs– Deals primarily with
memory cells (both B & T)• Memory B = antibodies• Memory T = T cells
– Helper & Killer
• Primary response = when person first exposed to antigen

• Antibodies ---- Immunoglobulins– General structure = “Y”; 2 light chains & 2 heavy chains
• Variable region--- binds to antigen
• Constant region --- attaches to macrophage– 5 different types of “constant regions”
» MADGE = all monomers, but M = pentamer & A = dimer
– The constant regions have no effect on the specificity of the antibody
• 5 types of immunoglobulins produced by plasma cells– IgM
– First secreted after arrival of antigen
– In monomer form, can act as receptor on cell membrane
– Usually in pentamer form, thus large & can cause agglutination
– Activates compliment
– Present early in the course of infection & then falls as IgG levels rise
– IgG
– Most numerous of circulating antibodies (75%)
– Called gamma globulin
– Effective against all pathogens & most toxins
– Can cross placenta
– Is key antibody in primary & secondary immune response
– Can activate compliment
– IgA
– In epithelium, thus in secretions (mucus, tears, saliva, colostrum, etc.)
– Prevents attachment of viruses & bacteria to epithelial surfaces
• 5 types of immunoglobulins produced by plasma cells
– IgE
– Attached to basophils & mast cells
– When antigen attaches, these cells release histamine
» Thus, they involved in allergic reactions (hypersensitivity rx)
» Called “troublemaker antibody” since they cause allergic reactions when exposed to antigen
– IgD
– Always attached to B lymphocyte
– Can activate B lymphocyte
– May be important in causing B cell to become either plasma cell or memory cell
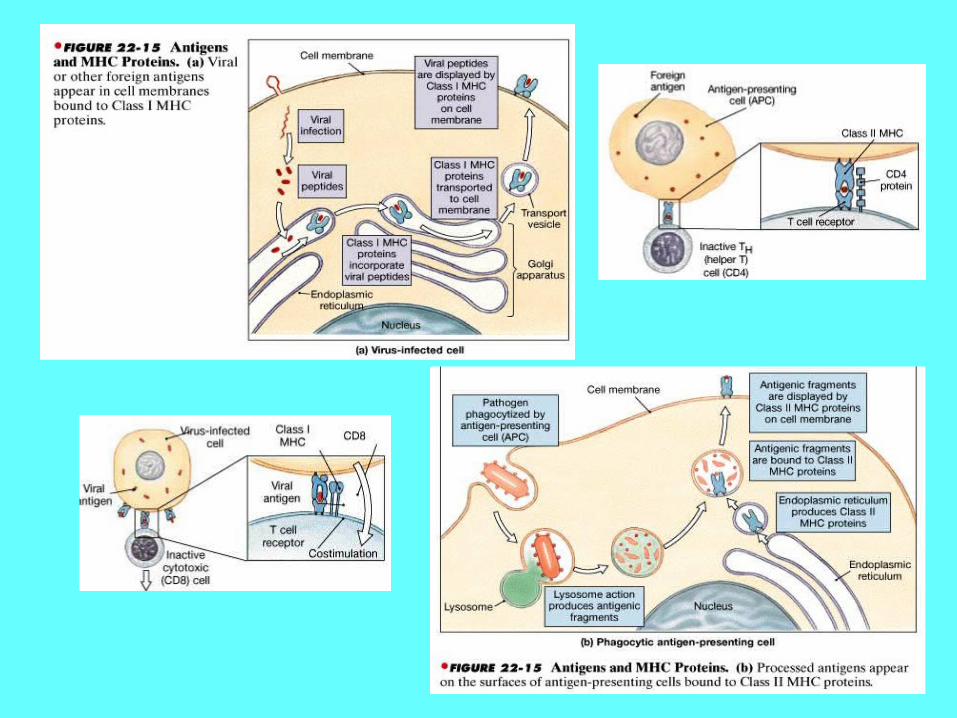
• “Antigen presenting proteins” & the processing of the antigen – Those proteins made by the cell that are incorporated into the cell membrane &
hold or present foreign antigenic material that has gotten into the cell– These are usually glycoproteins & everybody has different ones
• Controlled by genes on chromosome 6 in region called MHC» MHC = major histocompatability complex
• Antigen presenting proteins also called MHC proteins» Used to be called HLA (human leukocyte antigens)
– In immune system key cell is macrophage --- it is an “antigen presenting cell”– 2 classes of MHC proteins
– (1) MHC class I --- made continuously by all nucleated cells» For viral antigens & normal peptides made by cell
– (2) MHC class II --- made only by macrophages & lymphocytes when cell is processing antigens
» For antigenic fragments produced by lysosome
• Activation of lymphocytes– Antigen presenting proteins + foreign antigen -------- fit into receptor proteins in
cell membrane of cell that needs activation
• Recognition proteins– Those in cell membrane that are unique to that individual, thus “name tags”– These are the same as MHC proteins
Tissue & Organ Transplant RejectionTissue & Organ Transplant Rejection
• When the immune system of the individual responds to the HLAs in foreign tissue
• Remember that HLAs = MHC proteins
• Mechanism = – type IV cell-mediated hypersensitivity reaction
– Humoral response (antibody production)
• To decrease risk:– HLA match is excellent
– Donor is living
– Use of immunosuppressive drugs
» Side effects --- opportunistic infections
Hypersensitivity ReactionsHypersensitivity Reactions • Types
– Type I hypersensitivity---- allergy• Mech = IgE bound to mast cell & release of histamine and chemical mediators
– Person exposed to allergen causes B cells to make IgE antibodies
– These IgE attach to mast cells & make them sensitized
– Upon re-exposure get An + IgE & mast cell releases chemical mediators
• Sx = depend on where the sensitized mast cells located– Hay fever (allergic rhinitis)
– Food allergies
– Atopic dermatitis(eczema)
» Atopic means runs in families, thus genetic component
– Asthma
• Anaphylaxis = severe allergic reaction– Mech = large amounts of chemical mediators released from mast cells
– Can get C-V collapse & severe bronco-constriction
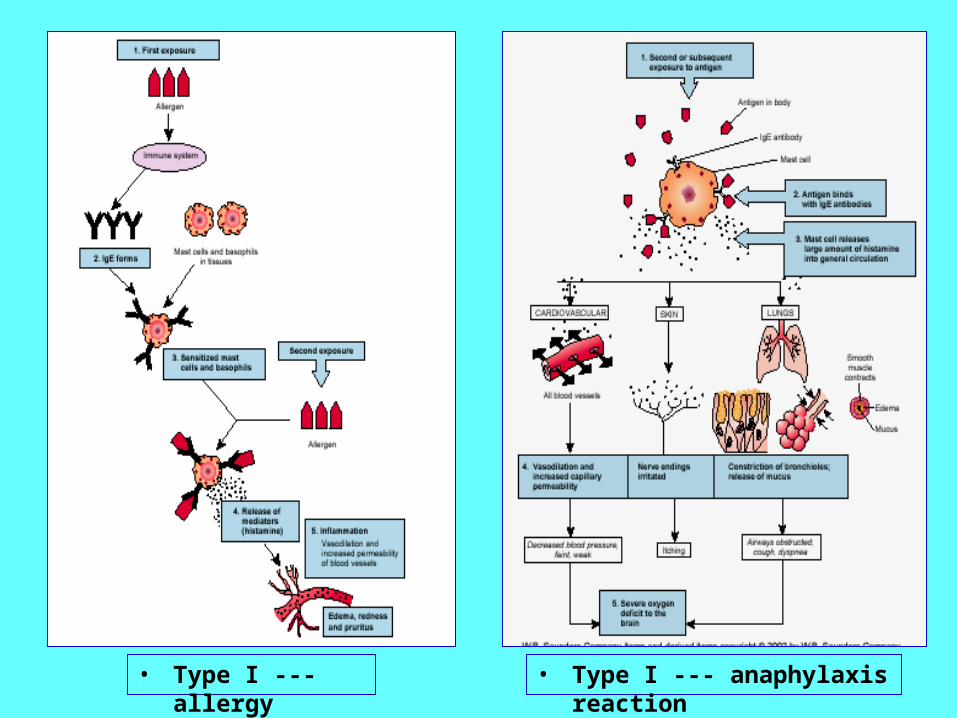
• Type I --- allergy • Type I --- anaphylaxis reaction
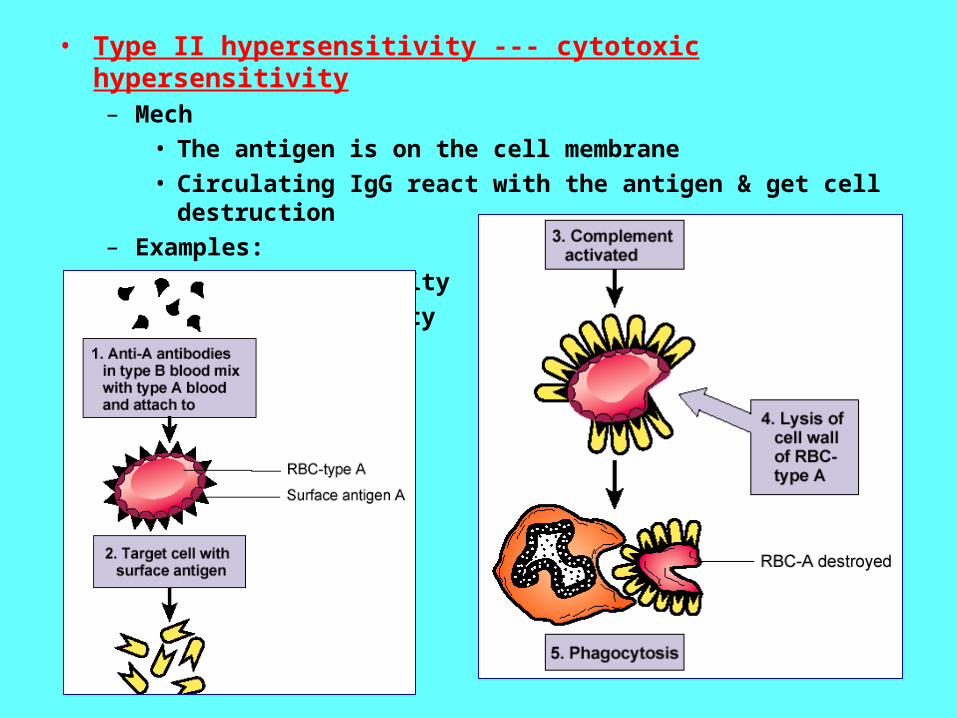
• Type II hypersensitivity --- cytotoxic hypersensitivity– Mech
• The antigen is on the cell membrane
• Circulating IgG react with the antigen & get cell destruction
– Examples:
• ABO incompatibility
• Rh incompatibility

• Type III --- immune complex hypersensitivity– Mech
• Antigen-antibody complex deposits in tissue
• Tissue is frequently blood vessel walls
• Complement is activated
– Sx = inflammation & tissue destruction
– Examples• Glomerulonephritis
• Rheumatoid arthritis
• Arthus reaction = localized inflammation & tissue necrosis– Seen in “valley fever”in humans
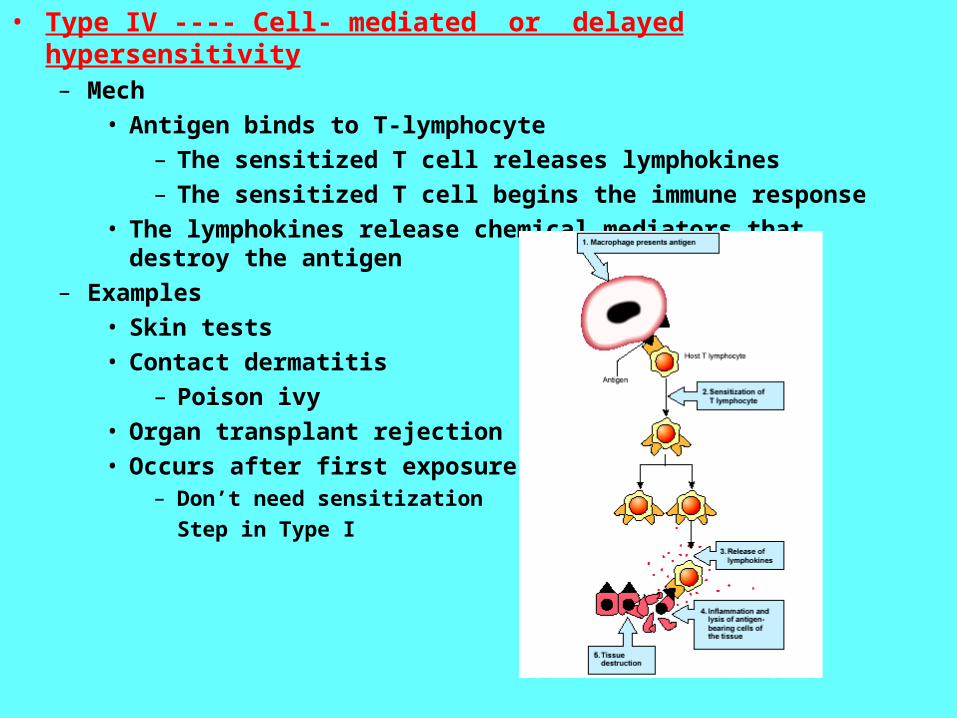
• Type IV ---- Cell- mediated or delayed hypersensitivity– Mech
• Antigen binds to T-lymphocyte
– The sensitized T cell releases lymphokines
– The sensitized T cell begins the immune response
• The lymphokines release chemical mediators that destroy the antigen
– Examples
• Skin tests
• Contact dermatitis
– Poison ivy
• Organ transplant rejection
• Occurs after first exposure– Don’t need sensitization
Step in Type I
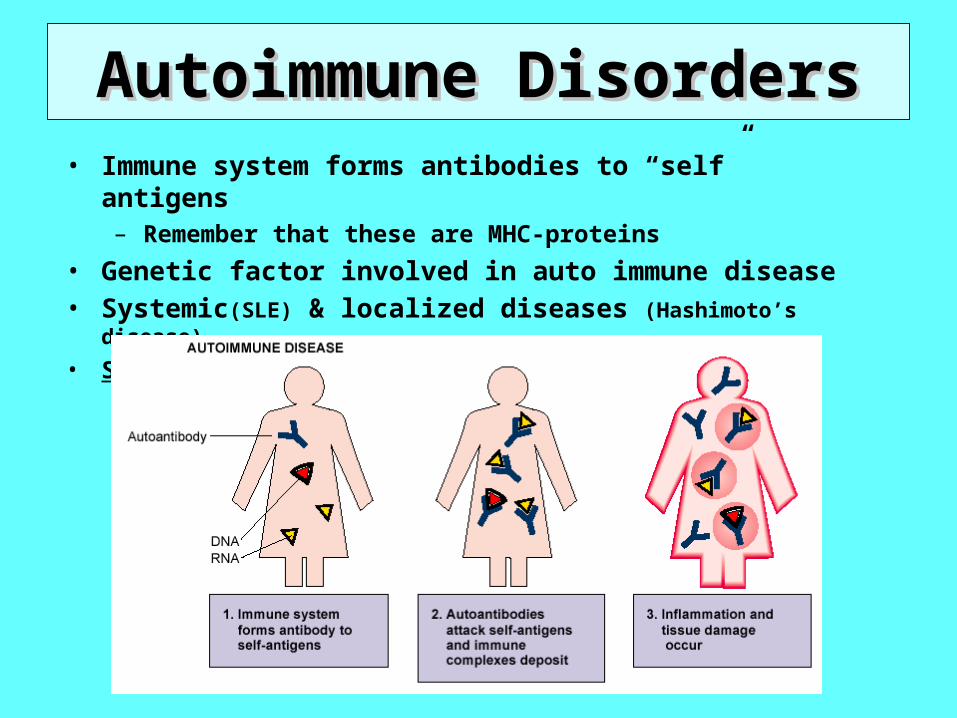
Autoimmune DisordersAutoimmune Disorders• Immune system forms antibodies to “self” antigens
– Remember that these are MHC-proteins
• Genetic factor involved in auto immune disease• Systemic(SLE) & localized diseases (Hashimoto’s disease)
• Systemic Lupus Erythematosus
• SLE– General
• Primarily women; age 20-40
• Butterfly rash; face of wolf (lupo)
• Course = remissions & exacerbations
– Pathophys
• Get circulating anti-DNA antibodies [anti-nuclear antibodies(ANA)]
• Immune complexes deposited in connective tissue anywhere in body
– Get inflammation & necrosis
• Vasculitis gives ischemia
– Sx
• Initially; skin rash, joint inflammation(polyarthritis)
• Pleuritis
• Carditis
• Raynauld’s phenomenon
• Glomerulonephritis
– Dx
• LE prep
• ANA
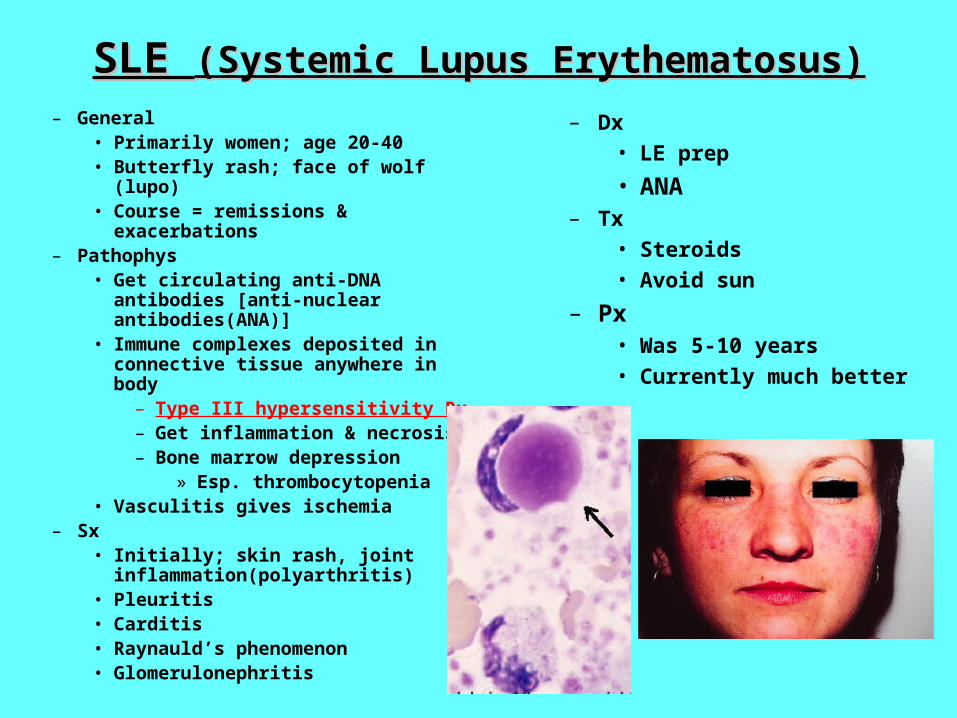
SLE SLE (Systemic Lupus Erythematosus)(Systemic Lupus Erythematosus)
– General• Primarily women; age 20-40• Butterfly rash; face of wolf (lupo)• Course = remissions & exacerbations
– Pathophys• Get circulating anti-DNA antibodies
[anti-nuclear antibodies(ANA)]• Immune complexes deposited in
connective tissue anywhere in body– Type III hypersensitivity Rx– Get inflammation & necrosis– Bone marrow depression
» Esp. thrombocytopenia • Vasculitis gives ischemia
– Sx• Initially; skin rash, joint
inflammation(polyarthritis)• Pleuritis• Carditis • Raynauld’s phenomenon• Glomerulonephritis
– Dx
• LE prep
• ANA– Tx
• Steroids
• Avoid sun
– Px• Was 5-10 years
• Currently much better
ImmunodeficiencyImmunodeficiency
• Primary immunodeficiency disorders = congenital and/or genetic
• Secondary immunodeficiency disorders = those acquired – Causes
• Immunosuppressive therapy
• Chemo & radiation cancer treatment
• HIV infection
• Use of corticosteroids
• Effects• Opportunistic infections
• Increase of certain cancers, especially non-Hodgkin’s lymphoma
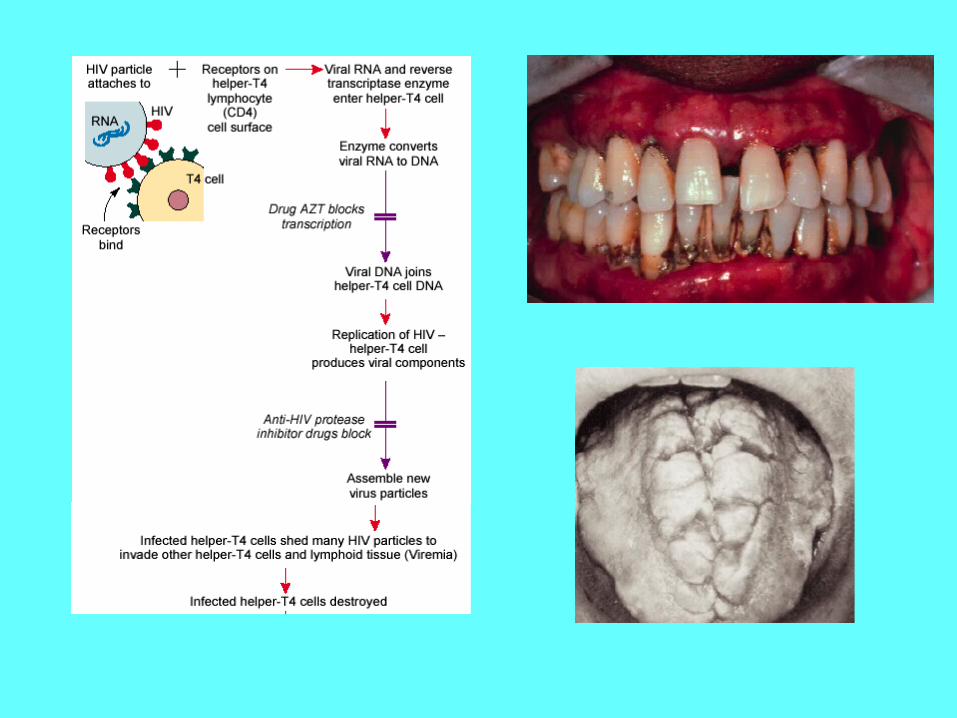
• Etiology = HIV virus– Retrovirus (RNA)– Antibodies appear after initial
infection• Avg time = 4-8 wks• May take as long as 6 months
• Transmission– Via blood & body fluids
• Exception = saliva• Virus is fragile & cannot live
outside body– Not by casual contact
• Tests– ELISA(enzyme-linked
immunoassay)– Western blot– CD4 counts
• Pathophys
– Virus has predilection for:• Helper T lymphocytes
• Macrophages
• CNS cells
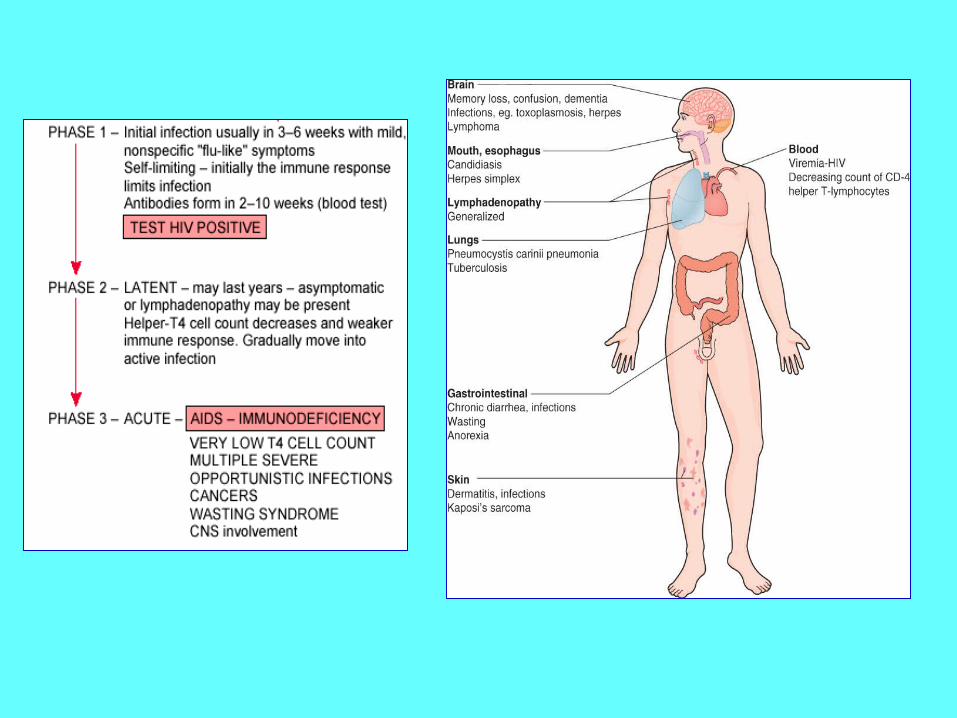
• Course of HIV infection (see next slide)
– Initial phase – like URI• May last longer than usual cold
– Latent phase – up to 10 years
– Active disease --- AIDS
• Usually begins with generalized lymphadenopathy
• G-I effects – esp diarrhea with cachexia
• Opportunistic infections
• HIV encephalopathy
• Cancers
AIDS (Acquired Immunodeficiency Syndrome)
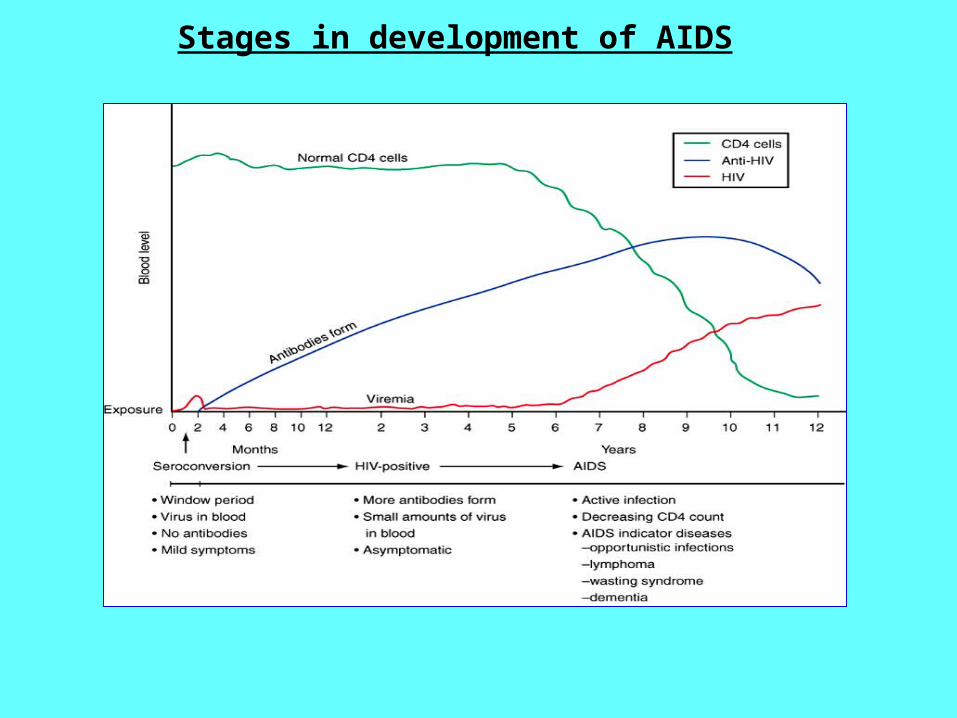
Stages in development of AIDS
• Opportunistic infections
– TB
– PCP(pneumocystis carinii pneumonia) – fungus
• Frequent cause of death in AIDS
– Toxoplasmosis
– Candidiasis
– Herpes
– Varicella
– Cytomegalovirus retinitis
– Necrotizing periodontal disease
• Opportunistic cancers
– Kaposi’s sarcoma
– Non-Hodgkins lymphoma
• HIV encephalopathy
– Called AIDS dementia
– Can end with seizures & coma
• Women with HIV
– AZT & pregnancy
• Tx
– Reverse transcriptase inhibitors
– Protease inhibitors
– Viral integrase inhibitors
– Tx opportunistic infections
AIDS (Acquired Immunodeficiency Syndrome)