eosinophilic digestive diseases: eosinophilic esophagitis ... · pdf filethe pathophysiology...
TRANSCRIPT
834 J Formos Med Assoc | 2009 • Vol 108 • No 11
REVIEW ARTICLE
Eosinophilic digestive diseases (EDD), including
eosinophilic esophagitis, eosinophilic gastroen-
teritis, and eosinophilic colitis, are relatively rare
gastrointestinal disorders. However, these condi-
tions are becoming increasingly recognized and an
area of increasing interest of research. Although
clinical presentation of the disorders varies widely,
the pathophysiology underlying all three is sus-
pected to be hypersensitivity related. Unfortu-
nately, there are no large, randomized, controlled
trials to guide treatment in EDD, and current man-
agement is extrapolated from therapies for other
atopic conditions. The mainstay of therapy is
corticosteroids and avoidance of food antigens.
Pathophysiology of EDD
Under normal, non-pathologic conditions, the gas-
trointestinal tract is the only non-hematopoietic
organ to contain eosinophils,1 with the cecal and
appendiceal region having the highest concen-
trations.2 Under normal conditions, the majority
of gastrointestinal eosinophils reside in the
lamina propria.3 The role of eosinophilia in par-
asitic infections of the gastrointestinal tract has
long been recognized. However, emerging evi-
dence suggests that eosinophils may play a role
in several other conditions, including EDD. The
pathogenesis of eosinophilic gastrointestinal dis-
eases is not clearly understood. But, given the
high correlation with other atopic conditions, a
hypersensitivity response is strongly suspected.
It is postulated that exposure of the gastrointesti-
nal mucosa to antigens promotes a Th-2 mediated
immune response. Th-2 cells produce interleukin
(IL)-4, IL-5 and IL-13, and promote the produc-
tion of eosinophils as well as IgE.4–6 Allergic
conditions, including asthma and allergic rhini-
tis, are also found to have a Th-2 mediated
©2009 Elsevier & Formosan Medical Association. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1Division of Gastroenterology-Hepatology, Department of Medicine, and 2Department of Pathology, University ofConnecticut Health Center, Farmington, Connecticut, USA.
Received: August 28, 2009Revised: September 24, 2009Accepted: October 2, 2009
*Correspondence to: Professor George Y. Wu, Division of Gastroenterology-Hepatology, Department of Medicine, University of Connecticut Health Center,Farmington, CT 06030, USA.E-mail: [email protected]
Eosinophilic Digestive Diseases: EosinophilicEsophagitis, Gastroenteritis, and ColitisAllison Shifflet,1 Faripour Forouhar,2 George Y. Wu1*
Eosinophilic digestive diseases (EDD) are relatively rare disorders associated with increased gastrointesti-nal eosinophilic infiltrates without any underlying primary etiology. The pathophysiology of EDD is un-clear, but is suspected to be related to a hypersensitivity reaction given its correlation with other atopicdisorders and clinical response to corticosteroid therapy. Given the overall relative increase of variousatopic conditions, it is important for clinicians to understand the presentation and diagnosis and treat-ment options available. We present here a review of EDD, including the proposed pathophysiology, diag-nosis and current treatment options for these disorders. [J Formos Med Assoc 2009;108(11):834–843]
Key Words: atopy, colitis, eosinophils, esophagitis, gastritis
response, which suggests that EDD should
be included within the spectrum of atopic
diseases.
Eosinophilic Esophagitis
Eosinophilic esophagitis is the most commonly
recognized EDD. Patients often present with
symptoms similar to gastroesophageal reflux dis-
ease; however, they are not responsive to tradi-
tional antireflux therapy. In fact, there is
emerging data to suggest that use of acid-sup-
pressive medications may predispose patients to
the development of eosinophilic esophagitis.7
The alteration of gastric pH caused by antisecre-
tory medications has been shown to affect pro-
tein digestion, allowing a larger percentage of
ingested protein to be absorbed in larger frag-
ments, potentially inducing an immunologic re-
sponse.8 Additionally, recent studies by Mullin
et al demonstrated increased permeability in the
mucosa of the upper gastrointestinal tract in pa-
tients taking acid-suppressive medications.9,10
This increased permeability may allow poten-
tially allergenic digestion products to permeate
gastric mucosa and induce an immunologic
reaction.
EpidemiologyEosinophilic esophagitis is more common in
Caucasians and males.11–13 The reported incidence
is approximately six per 100,000.14 However, in-
creased awareness of the disease over the past
several years has led to an increasing number of
cases identified. A higher incidence of eosino-
philic esophagitis is noted in patients with other
atopic conditions.11–14
Clinical presentationThe main presenting complaints of eosinophilic
esophagitis are similar to those of gastroesoph-
ageal reflux disease, including epigastric burning
and pain, regurgitation, nausea and vomiting.
However, symptoms are not responsive to stan-
dard antireflux therapy. Additionally, patients
may present with symptoms of dysphagia and
possible food impaction symptoms.15
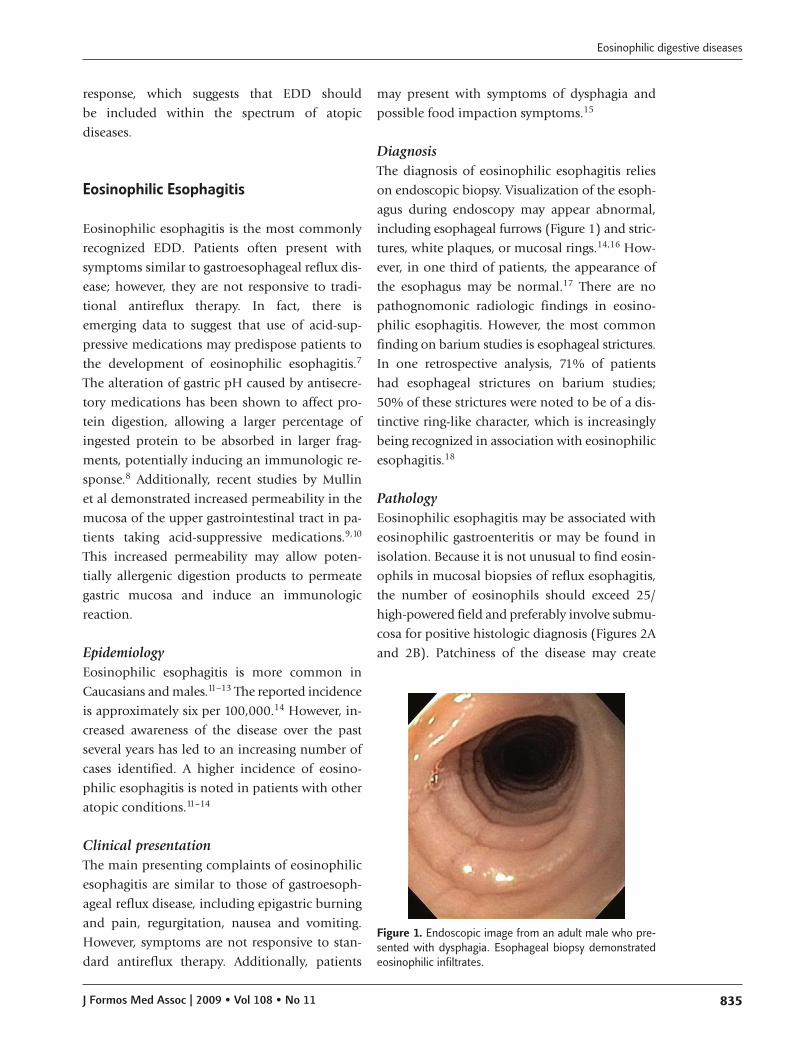
DiagnosisThe diagnosis of eosinophilic esophagitis relies
on endoscopic biopsy. Visualization of the esoph-
agus during endoscopy may appear abnormal,
including esophageal furrows (Figure 1) and stric-
tures, white plaques, or mucosal rings.14,16 How-
ever, in one third of patients, the appearance of
the esophagus may be normal.17 There are no
pathognomonic radiologic findings in eosino-
philic esophagitis. However, the most common
finding on barium studies is esophageal strictures.
In one retrospective analysis, 71% of patients
had esophageal strictures on barium studies;
50% of these strictures were noted to be of a dis-
tinctive ring-like character, which is increasingly
being recognized in association with eosinophilic
esophagitis.18
PathologyEosinophilic esophagitis may be associated with
eosinophilic gastroenteritis or may be found in
isolation. Because it is not unusual to find eosin-
ophils in mucosal biopsies of reflux esophagitis,
the number of eosinophils should exceed 25/
high-powered field and preferably involve submu-
cosa for positive histologic diagnosis (Figures 2A
and 2B). Patchiness of the disease may create
Eosinophilic digestive diseases
J Formos Med Assoc | 2009 • Vol 108 • No 11 835
Figure 1. Endoscopic image from an adult male who pre-sented with dysphagia. Esophageal biopsy demonstratedeosinophilic infiltrates.
A. Shifflet, et al
836 J Formos Med Assoc | 2009 • Vol 108 • No 11
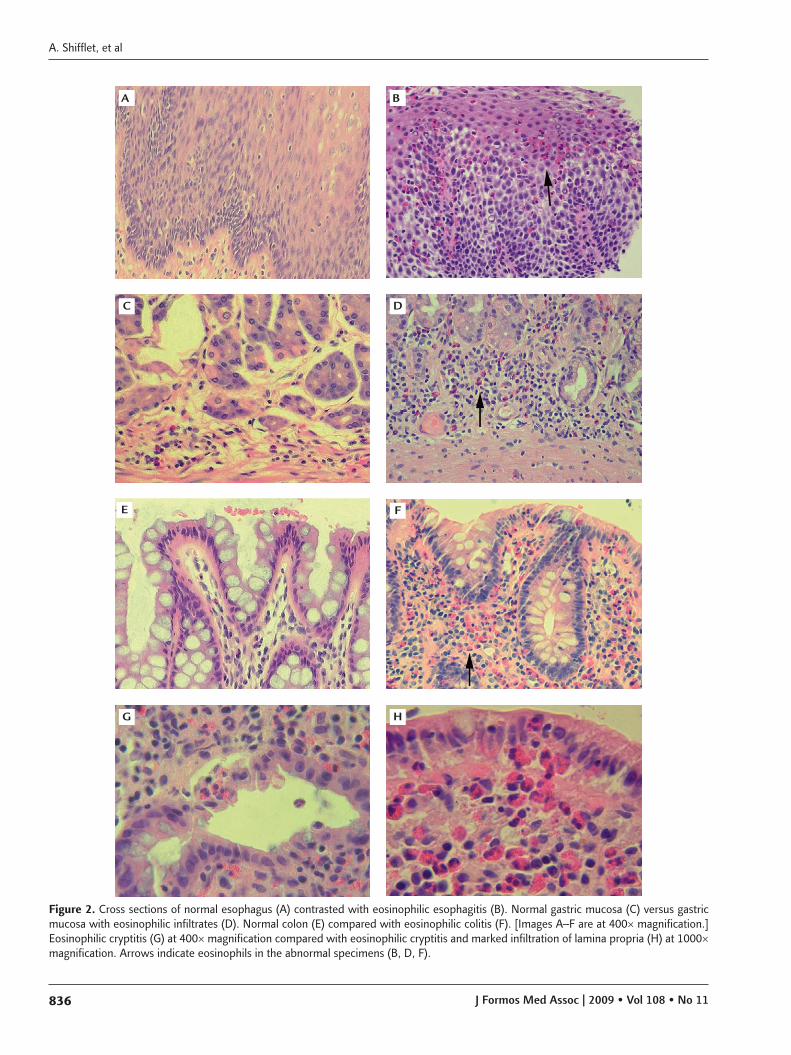
Figure 2. Cross sections of normal esophagus (A) contrasted with eosinophilic esophagitis (B). Normal gastric mucosa (C) versus gastricmucosa with eosinophilic infiltrates (D). Normal colon (E) compared with eosinophilic colitis (F). [Images A–F are at 400× magnification.]Eosinophilic cryptitis (G) at 400× magnification compared with eosinophilic cryptitis and marked infiltration of lamina propria (H) at 1000×magnification. Arrows indicate eosinophils in the abnormal specimens (B, D, F).
A
C
E
G H
F
D
B

false-positive results unless generous multiple
samples are obtained.
Eosinophilic Gastroenteritis
Eosinophilic gastroenteritis is a rare condition
involving eosinophilic infiltrates of gastrointesti-
nal tissue causing a wide array of gastrointestinal
symptoms. The diagnosis of eosinophilic gastro-
enteritis requires a high degree of clinical suspi-
cion, given the relatively nonspecific history and
physical examination findings. Eosinophilic gas-
troenteritis should be considered in the differen-
tial diagnoses of any patient who presents with
abdominal pain or other nonspecific gastroin-
testinal complaints without any clear etiology
on diagnostic evaluation. A definitive diagnosis
can be made by endoscopic biopsy displaying in-
creased eosinophilic infiltrates and exclusion of
any primary etiology causing hypereosinophilia.
EpidemiologyEosinophilic gastroenteritis is a rare disease, with
a peak incidence between the ages of 20 and 50
years.19 While the actual incidence is unknown,
there have been several case reports in the litera-
ture, particularly in the past 30–40 years, with the
initial case report published in 1937.20 Given
the wide variety of presentations in addition to
the relatively nonspecific symptoms of this dis-
ease, the incidence has likely been underreported.
There is an increased incidence of eosinophilic
gastrointestinal disease in patients with other
atopic conditions, such as asthma, allergic rhini-
tis, atopic dermatitis, and food and environmental
allergies. This may relate to the similar underly-
ing reactive processes of these disorders, includ-
ing increased eosinophils, mast cells, IL-4, IL-5,
IL-13 and chemokines.21
Clinical featuresThe clinical features seen in eosinophilic gastro-
enteritis vary based on the region and depth of
the gastrointestinal tract affected by eosinophilic
infiltration.
Mucosal eosinophilic gastroenteritis
Symptoms of mucosal eosinophilic gastroenteritis
include nonspecific complaints such as abdomi-
nal pain, nausea, vomiting and diarrhea as well as
anemia due to fecal occult blood loss and protein
wasting enteropathy.22 Given these nonspecific
symptoms, the diagnosis of mucosal eosinophilic
gastroenteritis requires high clinical suspicion.
The prevalence of mucosal eosinophilic gastroen-
teritis varies widely between studies (25–100%).
However, the higher incidence of this subtype
may be due to the more relative ease of diagnosis
via endoscopic biopsy.23,24
Muscularis eosinophilic gastroenteritis
Muscular eosinophilic gastroenteritis often pres-
ents with signs and symptoms of gastric outlet
and intestinal obstruction, and typically colicky
abdominal pain.25,26 Muscular eosinophilic gas-
troenteritis is the second most common subtype,
found in 13–70% of cases.23
Subserosal eosinophilic gastroenteritis
Subserosal eosinophilic gastroenteritis is the least
common subtype, accounting for only 12–40%
of cases.23 Subserosal eosinophilic gastroenteritis
frequently presents with ascites and bloating,27
and often has a higher level of peripheral eosino-
philia.28 This subset of patients typically has bet-
ter clinical response to steroid treatment, but often
with a more significant number of relapses.28
DiagnosisThe diagnosis of eosinophilic gastroenteritis re-
quires a high index of suspicion, given its wide
array of nonspecific symptoms and relatively low
incidence. A clinical history of other atopic condi-
tions such as asthma, atopic dermatitis, and food
and environmental allergies should heighten sus-
picion for eosinophilic gastroenteritis. Patients
with eosinophilic gastroenteritis may appear chro-
nically ill on physical examination, with signs of
malnutrition due to malabsorption. Suggestive
findings on laboratory data are peripheral eosin-
ophilia. But this finding is extremely variable.19
Radiographic changes in patients with eosinophilic
Eosinophilic digestive diseases
J Formos Med Assoc | 2009 • Vol 108 • No 11 837

gastroenteritis are also variable and are absent in
up to 40% of cases.29 Upper gastrointestinal se-
ries may show an irregular and lacy antral surface
of the stomach or thickening of the circular folds
and wall of the small bowel.30 Additionally, stric-
tures secondary to eosinophilic gastroenteritis may
be evident on imaging. The endoscopic appear-
ance of eosinophilic gastroenteritis is relatively
nonspecific and most notable in the mucosal
subtype. Abnormalities include erythema, ulcer-
ations or focal erosions, and thickening of folds
and friability.31
PathologyDefinitive diagnosis is made by histological
evidence of eosinophilic infiltration on biopsy.
The majority of studies have used a definition
of > 20 eosinophils/high-powered field in the
lamina propria for eosinophilic gastroenteritis
(Figures 2C and 2D).19 Involvement of gastric
mucosa is often patchy and multiple biopsies
should be obtained from various regions to im-
prove yield. It involves all layers of the wall and
is typically associated with edema (especially in
the submucosa and muscle), increased vascular-
ity, and fibrosis. Other inflammatory cells are also
increased. In particular, increased number and
degranulation of mast cells have come to atten-
tion more recently. Occasionally, necrotizing gran-
ulomata are noted. Involvement of subserosa
may be associated with eosinophilic ascites and
peritonitis.
Since endoscopic biopsies are typically lim-
ited to mucosa, pathologic findings in this region
carry special significance for everyday diagnosis.
Significant patchy or diffuse eosinophilic infil-
tration of lamina propria is a frequent finding.
However, the number of eosinophils varies con-
siderably in normal mucosa. Thus, other findings
such as epithelial infiltration, eosinophilic cryp-
titis and degranulation, and involvement of mus-
cularis mucosa and submucosa are important to
increase the reliability of histologic diagnosis. In
addition, the frequently patchy nature of the dis-
ease creates high false-negative rate unless gener-
ous and multiple biopsies are obtained.
Once a diagnosis of eosinophilic gastroen-
teritis is made, some clinicians elect to perform
allergy evaluation to determine the inciting anti-
gen. Methods of allergy testing include skin prick
or patch tests and radioallergosorbent tests to
detect IgE antibody formation against various
ingested antigens. This can assist in development
of an elimination diet to avoid antigen exposure.
Eosinophilic Colitis
Eosinophilic colitis is the least common EDD
and varies in clinical presentation depending on
the region and layer of colon affected. Diagnosis
of eosinophilic colitis also relies on biopsy with
pathologic evaluation.
EpidemiologyEosinophilic colitis is the rarest EDD. It mainly
affects neonates and young adults. Eosinophilic
colitis appears to affect both sexes equally.32
Clinical presentationThe clinical symptoms of eosinophilic colitis may
vary depending on the intestinal layer affected,
similar to eosinophilic gastroenteritis. Eosino-
philic colitis affecting the mucosa often presents
with malabsorption, diarrhea, and protein wast-
ing, whereas disease affecting the muscularis
often manifests as intestinal obstruction and
colonic thickening. Eosinophilic colitis affecting
the serosa mainly presents as ascites with fluid
analysis showing the majority of cells to be
eosinophils.33–35
DiagnosisThe mainstay of diagnosis for eosinophilic coli-
tis is biopsy. A small number of eosinophils may
be seen in various regions of the colon under nor-
mal conditions, and at present there is no gen-
eral consensus for differentiating normal versus
abnormal levels of eosinophilia in the colon. Ra-
diologic findings of eosinophilic colitis also de-
pend on the region and layer affected, but may
show strictures or thickening of the bowel wall.33
A. Shifflet, et al
838 J Formos Med Assoc | 2009 • Vol 108 • No 11

PathologyEosinophilic colitis is more problematic to diag-
nose because of marked variability in the num-
ber of eosinophils in the normal population and
in various geographic sites. The concentration
of eosinophils is variable depending on the re-
gion of the colon. Eosinophils are more concen-
trated in the cecum and ascending as compared
to the left colon. Eosinophils comprise up to 3%
of the inflammatory cells in normal colonic mu-
cosa (Figure 2E), and this percentage may in-
crease significantly without any correlating clinical
complaint or disease. Thus, the presence of ede-
ma in the muscularis and submucosa, presence
of eosinophils (Figure 2F) in the epithelium of the
crypts (Figure 2G), degranulation, and involvement
of muscularis mucosa and submucosa (Figure 2H)
are particularly important in formulating a diag-
nosis of eosinophilic colitis. Generous and mul-
tiple biopsy samples are necessary for diagnosis.
Often, eosinophilic cryptitis is observed in asso-
ciation with chronic inflammatory bowel disease,
particularly Crohn’s disease, and this is impor-
tant in the differential diagnosis for eosinophilic
colitis. On rare occasions, eosinophilic colitis or
gastroenteritis manifest themselves as localized
tumor masses and may present with a clinical
picture of obstruction. In such cases, eosinophilic
venulitis may dominate the pathology.
Differential Diagnosis
Eosinophilic infiltration of the gastrointestinal
mucosa can be seen secondary to a variety of
other conditions. It is important to evaluate pa-
tients for secondary causes prior to diagnosis of
primary EDD. The classic association is in the
setting of parasitic infections, such as Ascaris,
Anisakis, Trichuris, schistosomiasis, Ancylostoma
caninum (hook worm), and Enterobius vermicularis
(pinworm).36–41 Case reports of Toxocara canis
and Strongyloides causing eosinophilic ascites have
been reported as well.42,43 Evaluation of stool for
ova and parasites or larvae identified on biopsy
confirms primary parasitic infection as the etiology
for eosinophilic infiltration in these cases. Addi-
tionally, several medications have been implicated
in eosinophilic infiltration of gastric mucosa.
The more commonly utilized medications that
have been implicated include azathioprine, gem-
fibrozil, enalapril, and carbamazepine.44–47 Other
causes of secondary gastrointestinal eosinophilia
include connective tissue diseases and vasculi-
tis.48,49 Occasionally, inflammatory bowel disease
may be associated with gastrointestinal eosino-
philic infiltrates as well as peripheral eosinophilia,
as a component of the inflammatory response in
inflammatory bowel disease.50 Hypereosinophilia
syndrome may also be a secondary cause of
eosinophilic gastroenteritis. Hypereosinophilia
syndrome is a rare condition with significant
peripheral eosinophilia for an extended period
of time (> 6 months) and associated infiltration
and end-organ damage related to hypereosino-
philia.51 Clinically, patients with eosinophilic
esophagitis present with complaints similar to
gastroesophageal reflux disease. A recent study by
Sayej et al revealed that high-dose proton pump
inhibitor therapy may be useful in differentiating
patients with eosinophilic esophagitis from those
with non-eosinophilic esophagitis.52 An addi-
tional study by Dellon et al identified a variety of
clinical, endoscopic and histologic findings that
may aid in distinguishing eosinophilic esophagi-
tis from gastroesophageal reflux disease. They
retrospectively reviewed 377 patients with either
gastroesophageal reflux disease or eosinophilic
esophagitis and found that younger age, symp-
toms of dysphagia, history of food allergies,
endoscopic evidence of esophageal rings, linear
furrows, white plaques or exudates, and absence
of hiatal hernia, as well as pathologic evidence of
higher maximum eosinophil count and presence
of eosinophil degranulation independently pre-
dicted eosinophilic esophagitis.53
Treatment of EDD
At present, there are no large, randomized, con-
trolled trials to guide treatment in eosinophilic
Eosinophilic digestive diseases
J Formos Med Assoc | 2009 • Vol 108 • No 11 839

gastroenteritis. The majority of data is from
smaller case series or extrapolated from the man-
agement of other atopic conditions. Cortico-
steroid therapy plays a large role in the treatment
of this condition. Given the suspected inflamma-
tory and hypersensitivity pathology of EDD,
steroids are a reasonable treatment option. Sev-
eral small, uncontrolled studies have evaluated
the efficacy of steroids in the various types of
EDD and shown significant improvement in
symptom management. However, no histologic
correlation has been shown.27,54,55 The optimal
duration of corticosteroid therapy has not yet
been established. Often, a dosing strategy similar
to that used in inflammatory bowel disease has
been utilized (1–2 mg/kg/day for 8 weeks fol-
lowed by a gradual taper).23 Topical corticoste-
roid treatment has also been utilized in patients
with eosinophilic esophagitis. A small study of
21 adult patients evaluated the effects of a 12-
month course of oral fluticasone propionate.56
All patients in this trial had complete resolution
of their dysphagia symptoms per assessment at
4 months post-completion of therapy. However,
a second study that evaluated patients who had
received oral fluticasone treatment approximately
3 years after completion of therapy found that
91% of patients had experienced recurrence of
their dysphagia symptoms.57
Alternative immune-modifying medications,
including mast cell inhibitors (sodium cromo-
glycate, 200 mg four times daily)58 and leukotriene
receptor antagonists have also been evaluated in
this condition. These studies are largely observa-
tional and the medications were often evaluated in
combination with other treatment modalities.59–61
In one case report by Urek et al, montelukast
10 mg/day provided symptom improvement in
an adolescent male with eosinophilic gastroen-
teritis.62 Additional case reports also demonstrated
symptom improvement.63,64 However there are
no large randomized trials evaluating efficacy or
correlating histologic improvement. Leukotriene
receptor antagonists have been shown in multi-
ple case reports to improve symptoms and pro-
vide an alternative to corticosteroids for chronic
maintenance therapy. The majority of case reports
involved children with eosinophilic gastroenteri-
tis or eosinophilic esophagitis and used dosages
of montelukast ranging from 10 mg daily to
40 mg daily.64–66 Additionally, Friesen et al re-
ported a double-blinded, randomized, controlled
study evaluating the efficacy of montelukast
(10 mg daily) in 40 children and adolescents
with eosinophilic duodenitis. Their results showed
significant symptom improvement in the mon-
telukast arm (62%) versus the placebo arm
(32%).67
As mentioned above, it is postulated that EDD
are triggered by food antigen exposure. Allergy
testing can aid in the identification of specific
antigens and development of an elimination diet.
The majority of data evaluating diet modifica-
tion have been obtained from the pediatric pop-
ulation. In a large study, specific elimination diets
based on food sensitivities resulted in improve-
ment in symptoms and esophageal biopsy in 75%
of patients.68 However, allergy testing has low
sensitivity and specificity with high false-positive
rates and should be cautiously interpreted. Other
studies have evaluated the effect of a trial of em-
piric elimination diet, with removal of the six most
common food allergens (milk, soy, egg, wheat,
nuts and seafood). In a small study of 35 patients
who were placed on an empiric elimination diet
for a 6-week trial, 74% showed improvement on
esophageal biopsy.69
Given the relative lack of data at this time,
there is no definitive treatment regimen for pa-
tients with EDD. However, it is reasonable to
consider a course of corticosteroid treatment
(1–2 mg/kg/day for 8 weeks followed by a gradual
taper) for the management of acute symptoms in
the appropriate clinical setting. Topical steroids,
including oral fluticasone (fluticasone inhaler
220 mmol/puff, two puffs twice daily), may also
be considered as a treatment option. Some pa-
tients may require chronic maintenance therapy
and steroid-sparing options, including mast cell
inhibitors (sodium cromoglycate, 200 mg four
times daily) and leukotriene receptor antago-
nists (montelukast 10–40 mg daily). Empiric diet
A. Shifflet, et al
840 J Formos Med Assoc | 2009 • Vol 108 • No 11

modification or allergy testing with specific diet
modifications may be an alternative option in
motivated patients.
Conclusion
EDD, including eosinophilic esophagitis, eo-
sinophilic gastroenteritis and eosinophilic coli-
tis, are rare conditions involving gastrointestinal
eosinophilic infiltrates and associated gastroin-
testinal symptoms without a primary etiology
for hypereosinophilic infiltrates. The pathophys-
iology of this condition is not well understood,
but a hypersensitivity mechanism is suspected
given its increased association with other atopic
conditions and clinical improvement with corti-
costeroids. The definitive diagnosis of EDD is
made with endoscopic biopsy displaying increased
eosinophilic infiltrates and the absence of any
primary disorders that may cause secondary
eosinophilic infiltrates. At this time, there is min-
imal data to guide EDD treatment. Treatment reg-
imens are extrapolated from therapies for other
atopic disorders and current evidence for efficacy
is limited to case reports and smaller studies.
Based on this data, it is reasonable to use corti-
costeroids in the acute setting and, if necessary,
mast cell inhibitors, leukotriene receptor antago-
nists and diet modification for chronic mainte-
nance. Additional studies are needed to further
delineate the pathophysiology of EDD, and
larger randomized, controlled studies are needed
to determine optimal treatment regimens.
References
1. Kato M, Kephart GM, Talley NJ, et al. Eosinophil infiltra-
tion and degranulation in normal human tissue. Anat Rec
1998;252:418–25.
2. Lowichik A, Weinberg AG. A quantitative evaluation of
mucosal eosinophils in the pediatric gastrointestinal tract.
Mod Pathol 1996;9:110–4.
3. Mishra A, Hoga SP, Lee JJ, et al. Fundamental signals that
regulate eosinophil homing to the gastrointestinal tract.
J Clin Invest 1999;103:1719–27.
4. Rankin SM, Conroy DM, Williams TJ. Eotaxin andeosinophil recruitment: implications for human disease.Mol Med Today 2000;6:20–7.
5. Hogan SP, Rothenberg ME, Forbes E, et al. Chemokines in eosinophil-associated gastrointestinal disorders. CurrAllergy Asthma Rep 2004;4:74–82.
6. Bieber T. Atopic dermatitis. N Engl J Med 2008;358:1483–94.
7. Merwat SN, Spechler SJ. Might the use of acid-suppressivemedications predispose to the development of eosinophilicesophagitis? Am J Gastroenterol 2009;104:1897–902.
8. Untersmayr E, Jensen-Jarolim E. The role of protein digestibility and antacids on food allergy outcomes. J Allergy Clin Immunol 2008;121:1301–8.
9. Mullin JM, Valenzano MC, Whitby M, et al. Esomeprazoleinduces upper gastrointestinal tract transmucosal perme-ability increase. Aliment Pharmacol Ther 2008;28:1317–25.
10. Mullin JM, Valenzano MC, Trembeth S, et al. Transepithe-lial leak in Barrett’s esophagus. Dig Dis Sci 2006;51:2326–36.
11. Blanchard C, Wang N, Rothenberg ME. Eosinophilicesophagitis: pathogenesis, genetics, and therapy. J AllergyClin Immunol 2006;118:1054–9.
12. Heltzer ML, Franciosi JP, Shuker M, et al. Demographic information of patients with eosinophilic esophagitis. J Allergy Clin Immunol 2007;119:S111.
13. Brown-Whitehorn T, Liacouras CA. Eosinophilic esopha-gitis. Curr Opin Pediatr 2007;19:575–80.
14. Straumann A, Spichtin HP, Grize L, et al. Natural history ofprimary eosinophilic esophagitis: a follow-up of 30 adultpatients for up to 11.5 years. Gastroenterology 2003;125:1660–9.
15. Desai TK, Stecevic V, Chang CH, et al. Association ofeosinophilic inflammation with esophageal food impactionin adults. Gastrointestinal Endosc 2005;61:795–801.
16. Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilicesophagitis: a 10 year experience in 381 children. ClinGastroenterol Hepatol 2005;3:1198–206.
17. Siafakas CG, Ryan CK, Brown MR, et al. Multiple esoph-ageal rings: an association with eosinophilic esophagitis.Am J Gastroenterol 2000;95:1572–5.
18. Zimmerman S, Levine M, Rubesin S, et al. Idiopathic eosinophilic esophagitis in adults: the ringed esophagus.Radiology 2005;236:159–65.
19. Talley NJ, Shorter RG, Philips SF, et al. Eosinophilic gas-troenteritis: a clinicopathological study of patients withdisease of the mucosa, muscle layer and subserosal tissues.Gut 1990;31:54–5.
20. Kaijser R. Zur kenntnis der allergischen affectionen desverdauungskanals vom standpunkt des chirurgen aus.Arch Klin Chir 1937;188:36–64. [In German]
21. Jyonouchi S, Brown-Whitehorn T, Spergel JM. Associationof eosinophilic gastrointestinal disorders with other atopicdisorders. Immunol Allergy Clin North Am 2009;29:85–97.
Eosinophilic digestive diseases
J Formos Med Assoc | 2009 • Vol 108 • No 11 841

22. Kalantar SJ, Marks R, Lambert JR et al. Dyspepsia due to eosinophilic gastroenteritis. Dig Dis Sci 1997;42:2327–32.
23. Khan S. Eosinophilic gastroenteritis. Best Pract Res ClinGastroenterol 2005;19:177–98.
24. Daneshjoo R, Daneshjoo J, Talley N. Eosinophilic gas-troenteritis. Curr Gastroenterol Rep 2002;4:366–72.
25. Steffen RM, Wyllie R, Petras RE, et al. The spectrum ofeosinophilic gastroenteritis. Report of six pediatric casesand review of the literature. Clin Pediatr (Phil) 1991;30:404–11.
26. Zora JA, O’Connelll EJ, Sachs MI, et al. Eosinophilic gas-troenteritis: a case report and review of the literature. AnnAllergy 1984;53:45–7.
27. Falley NJ, Shorter RG, Phillips SF, et al. Eosinophilic gas-troenteritis: a clinicopathological study of patients withdisease of the mucosa, muscle layer and subserosal tissues. Gut 1990;31:54–8.
28. Fenoglio LM, Benedetti V, Rossi C, et al. Eosinophilic gas-troenteritis with ascites: a case report and review of theliterature. Dig Dis Sci 2003;48:1013–20.
29. Baig MA, Qadir A, Rasheed J. A review of eosinophilicgastroenteritis. J Natl Med Assoc 2006;98:1616–9.
30. Teele RL, Katz AJ, Goldman H, et al. Radiographic featuresof eosinophilic gastroenteritis (allergic gastroenteropathy)of childhood. AJR Am J Roentgenol 1979;132:575–80.
31. Katsumi N, Yamaguchi Y, Yamato T, et al. Multiple ulcera-tive lesions of the stomach: a rare case of eosinophilic gas-troenteritis. Gastrointest Endosc 2002;56:762–4.
32. Rothenberg ME. Eosinophilic gastrointestinal disorders(EGID). J Allergy Clin Immunol 2004;113:11–28.
33. Velchuru VR, Khan MA, Hellquist HB, et al. Eosinophiliccolitis. J Gastrointest Surg 2007;11:1373–5.
34. Clouse RE, Alpers DH, Hockenbery DM, et al. Pericrypt eosin-ophilic enterocolitis and chronic diarrhea. Gastroenterology1992;103:168–76.
35. Okpara N, Aswad B, Baffy G. Eosinophilic colitis. World JGastroenterol 2009;15:2975–9.
36. Takeyama Y, Kamimura S, Suzumiya J, et al. Case report:eosinophilic colitis with high antibody titre against Ascarissuum. J Gastroenterol Hepatol 1997;12:204–6.
37. Esteve C, Resano A, Diaz-Tejeiro P, et al. Eosinophilic gastri-tis due to Anisakis: a case report. Allergol Immunopathol(Madr) 2000;28:21–3.
38. Hong ST, Lim HS, Kim DS, et al. A case of gastroenteritisassociated with gastric tricuriasis. J Korean Med Sci 2003;18:429–32.
39. Bogers J, Moreels T, De Man J, et al. Schistosoma mansoni infection causing diffuse enteric inflammationand damage of the enteric nervous system in the mousesmall intestine. Neurogastroenterol Motil 2000;12:431–40.
40. Walker NI, Croese J, Clouston AD, et al. Eosinophilic en-teritis in northeastern Australia. Pathology, associationwith Ancylostoma caninum, and implications. Am J SurgPathol 1995;19:328–37.
41. Macedo T, MacCarty RL. Eosinophilic ileocolitis secondaryto Enterobius vermicularis: a case report. Abdom Imaging2000;25:530–2.
42. Van Laethem JL, Jacobs F, Braude P, et al. Toxocara canisinfection presenting as eosinophilic ascites and gastroen-teritis. Dig Dis Sci 1994;39:1370–2.
43. Corsetti M, Basilisco G, Pometta R, et al. Mistaken diag-nosis of eosinophilic colitis. Ital J Gastroenterol Hepatol1999;31:607–9.
44. Riedel RR, Schmitt A, de Jonge JP, et al. Gastrointestinaltype 1 hypersensitivity to azathioprine. Klin Wochenschr1990;68:50–2.
45. Lee JY, Medellin MV, Tumpkin C. Allergic reaction to gemfibrozil manifesting as eosinophilic gastroenteritis.South Med J 2000;93:807–8.
46. Barak N, Hart J, Sitrin MD. Enalapril-induced eosinophilicgastroenteritis. J Clin Gastroenterol 2001;33:157–8.
47. Shakeer VK, Devi SR, Chettupuzha AP, et al. Carbamazepine-induced eosinophilic enteritis. Indian J Gastroenterol2002:21:114–5.
48. DeSchryver-Kecskemeti K, Clouse RE. A previously unrec-ognized subgroup of “eosinophilic gastroenteritis”. Associ-ation with connective tissue diseases. Am J Surg Pathol1984;8:171–80.
49. Solans R, Bosch JA, Perez-Bocanegra C, et al. Churg–Strausssyndrome: outcome and long-term follow-up of 32 pa-tients. Rheumatology 2001;40:763–71.
50. Levy AM, Gleich GJ, Sandborn WJ, et al. Increased eosin-ophil granule proteins in gut lavage fluid from patientswith inflammatory bowel disease. Mayo Clin Proc 1997;72:117–23.
51. Roufosse F, Cogan E, Goldman M. Recent advances inpathogenesis and management in hypereosinophilic syndromes. Allergy 2004;59:673–89.
52. Sayej WN, Patel R, Baker R, et al. Treatment with high-dose proton pump inhibitors helps distinguish eosinophilicesophagitis from noneosinophilic esophagitis. J PediatrGastroenterol Nutr 2009 Jul 21 [Epub ahead of print]
53. Dellon ES, Gibbs WB, Fritchie KJ, et al. Clinical, endo-scopic, and histologic findings distinguish eosinophilicesophagitis from gastroesophageal reflux disease. ClinGastroenterol Hepatol 2009 Sep 2 [Epub ahead of print]
54. Naylor AR. Eosinophilic gastroenteritis. Scott Med J 1990;35:163–5.
55. Lee CM, Changchien CS, Chen PC, et al. Eosinophilic gas-troenteritis: 10 years experience. Am J Gastroentrol 1993;88:70–4.
56. Arora AS, Perrault J, Smyrk TC. Topical corticosteroidtreatment of dysphagia due to eosinophilic esophagitis inadults. Mayo Clin Proc 2003;78:830–5.
57. Helou EF, Simonson J, Arora AS. 3-yr-follow-up of topicalcorticosteroid treatment for eosinophilic esophagitis inadults. Am J Gastroenterol 2008;103:2194–9.
58. Di Gioacchino M, Pizzicannella G, Fini N, et al. Sodiumcromoglycate in the treatment of eosinophilic gastroen-teritis. Allergy 1990;45:161–6.
A. Shifflet, et al
842 J Formos Med Assoc | 2009 • Vol 108 • No 11

59. Perez-Millan A, Martin Lorente JL, Lopez-Morante A, et al. Subserosal eosinophilic gastroenteritis treated effi-caciously with sodium cromoglycate. Dig Dis Sci 1997;42:342–4.
60. Neustrom MR, Friesen C. Treatment of eosinophilic gas-troenteritis with montelukast. J Allergy Clin Immunol 1999;104:506.
61. Melamed I, Feanny SJ, Sherman PM, et al. Benefit of ke-totifen in patients with eosinophilic gastroenteritis. Am JMed 1991;90:310–4.
62. Urek MC, Kujundzic M, Banic M. Leukotriene receptorantagonists as potential steroid sparing agents in a patientwith serosal eosinophilic gastroenteritis. Gut 2006;55:1363–4.
63. Katsinelos P, Pilpilidis I, Xiarchos P, et al. Oral administra-tion of ketotifen in a patient with eosinophilic colitis andsevere osteoporosis. Am J Gastroenterol 2002;97:1072–4.
64. Vanderhoof JA, Young RJ, Hanner TL, et al. Montelukast:use in pediatric patients with eosinophilic gastrointestinal
disease. J Pediatr Gastroenterol Nutr 2003;36:293–4.
65. Attwood SE, Lewis CJ, Bronder CS, et al. Eosinophilic oe-sophagitis: a novel treatment using montelukast. Gut2003;52:181–5.
66. Schwartz DA, Pardi DS, Murray JA. Use of montelukast assteroid-sparing agent for recurrent eosinophilic gastroen-teritis. Dig Dis Sci 2001;46:1787–90.
67. Friesen CA, Kearns GL, Andre L, et al. Clinical efficacy andpharmacokinetics of montelukast in dyspeptic childrenwith duodenal eosinophilia. J Pediatr Gastroenterol Nutr2004;38:343–51.
68. Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilicesophagitis: a 10-year experience in 381 children. ClinGastroenterol Hepatol 2005;3:1198–206.
69. Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomesin eosinophilic esophagitis. Clin Gastroenterol Hepatol2006;4:1097–102.
Eosinophilic digestive diseases
J Formos Med Assoc | 2009 • Vol 108 • No 11 843