dietary therapy for eosinophilic esophagitis: elimination ... · dietary therapy for eosinophilic...
TRANSCRIPT

Dietary Therapy for Eosinophilic Esophagitis:Elimination and Reintroduction
Kara L. Kliewer1 & Alison M. Cassin2 & Carina Venter3
# Springer Science+Business Media, LLC, part of Springer Nature 2017
AbstractEosinophilic esophagitis (EoE) is a food antigen-mediated disorder of the esophagus characterized by eosinophil predominantinflammation and symptoms of esophageal dysfunction. Dietary antigen elimination induces clinical and histological remissionin patients with EoE. The most restrictive of elimination diets (the elemental diet) removes all possible food antigens whileempiric elimination diets remove all (or a subset) of food antigens most commonly reported to cause esophageal eosinophilia andfood allergies (milk, egg, wheat, soy, peanuts, tree nuts, fish, or legumes). Elimination diets are effective treatments for EoE butpose psychosocial and financial challenges to patients and consequently may impair quality of life. Foods that are commonlyeliminated, especially milk, are also nutrient-dense and therefore their elimination may result in inadequate nutrient intake ordeficiencies without careful diet planning to include nutritionally comparable and safe food substitutes. After remission isachieved with elimination diets, foods can be reintroduced sequentially to identify specific food triggers, but this reintroductionis not standardized. Food elimination and food reintroductions should consider the patient’s lifestyle, nutrition needs, and skillsand ideally be managed by a team with knowledge of eosinophilic gastrointestinal disorders and nutrition.
Keywords Eosinophilic esophagitis . Elimination diet . Food reintroduction . Nutrition
Introduction
Eosinophilic esophagitis (EoE) is an immune-mediated disordercharacterized by eosinophil infiltration of the esophageal epithe-lium and symptoms of esophageal dysfunction (dysphagia, pain,reflux, and vomiting). EoE is diagnosed if an esophageal biopsyshows 15 or more eosinophils per high power field (eos/hpf)while on proton pump inhibitor (PPI) therapy [1]. In 1995,Kelly et al. found that children diagnosed with EoE who weretreated exclusively with amino acid-based elemental formula(i.e., formula free of intact or hydrolyzed proteins) experienced
resolution of both symptoms and esophageal eosinophilia. Foodreintroductions in this study identified cow’s milk, wheat, egg,soy, and peanuts as food Btriggers^—foods that caused a recur-rence of symptoms and esophageal damage [2]. This seminalstudy demonstrated that EoE is, in part, a food antigen-mediateddisease. Kagalwalla et al. subsequently tested the effects of elim-inating six foods most commonly reported to cause food allergyand esophageal eosinophilia (milk, egg, wheat, soy, seafood, andnuts) and found the majority following the diet responded bothclinically and histologically [3]. Since this study, variations ofempiric and other elimination diets have been evaluated in nu-merous studies. Here, we discuss the efficacy of elimination dietsin the treatment of EoE, the practicalities of following elimina-tion diets and reintroducing foods to accurately identify foodtriggers, and the nutritional risks posed by elimination diets.
Elimination Diets: Efficacies
Following the initial success of the elemental and six foodelimination diets in achieving clinical and histological remis-sions in EoE [2, 3], clinicians and researchers beganexperimenting with variations of these elimination diets in
* Kara L. [email protected]
1 Division of Allergy and Immunology, Cincinnati Children’s HospitalMedical Center, MLC 2010, 3333 Burnet Avenue,Cincinnati, OH 45229, USA
2 Division of Nutrition Therapy, Cincinnati Children’s HospitalMedical Center, Cincinnati, OH, USA
3 Section of Allergy and Immunology, University of Colorado DenverSchool of Medicine, Colorado Children’s Hospital, Aurora, CO,USA
Clinical Reviews in Allergy & Immunologyhttps://doi.org/10.1007/s12016-017-8660-1

an attempt to maximize remission rates while minimizing pa-tient burden. Consequently, there are now three broad catego-ries of elimination diets used in the management of EoE—elemental diets, empiric elimination diets, and test-directedelimination diets—with several strategies within each catego-ry that attempt to balance efficacy with tolerability.
Elemental Diets The exclusive use of an amino acid-basedformula that is free of intact or hydrolyzed proteins (allergens)has been shown to be the most effective dietary therapy for EoE[4]. In adults, remission rates are 71 and 72% (94%, if currentguidelines are used [4]) in short-term studies of elemental diets,but dropout rates with this therapy are high (19 and 38%) [5, 6].Interestingly, symptoms may not improve quickly with theelemental diet in adults [5]. In pediatric patients, response ratesrange from 75 to 100% in studies of children following exclu-sive elemental diets [3, 7–10] or elemental formula in combi-nation with a few fruits, vegetables, or fruit juices [2, 11].Symptom improvement is marked in children following ele-mental diets [2, 3, 9] (see Tables 1 and 2 for a summary ofelemental diets in adults and children with EoE).
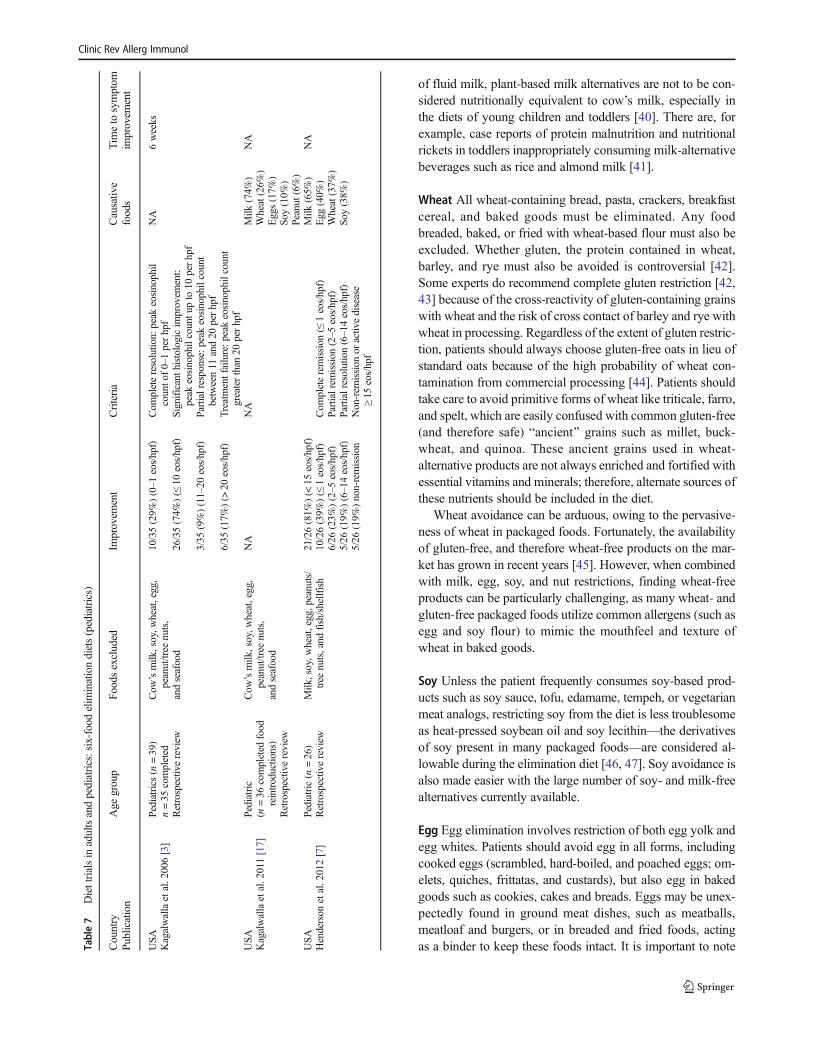
Empiric Elimination Diets Diets that eliminate common aller-gens (i.e., a limited number of foods) are successful at achiev-ing histological and symptom resolution and yet more palat-able for patients to follow than the elemental diet. The six foodelimination diet (SFED), which, depending on the populationstudied, excludes milk, soy and/or legumes, eggs, wheat and/or grains, peanuts/tree nuts, and fish/shellfish [3, 12–17], ishighly effective with histological response rates of 52–74% inadults [12–16] and 74–81% in children [3, 7, 17]. A four foodelimination diet which excludes milk, egg, wheat/gluten, andsoy and/or legumes [18, 19] is slightly less effective than theSFEDwith 54% histological remission rates in adults [18] and64% remission rates in children [19]. However, a two food(milk and wheat) elimination diet is about half as effective as aSFED with a 43% response rate in adult and pediatric patients[20]. Unexpectedly, a one food (milk) elimination diet [10, 21]in children achieved an approximately 65% remission rate intwo separate studies [10, 21]. A 30% dropout rate and con-comitant PPI therapy may have confounded interpretation ofresults in one study [21] (see Tables 3, 4, 5, 6, 7 for a summaryof empiric elimination diets in adults and children with EoE).It is noteworthy that none of these elimination diets have beenrigorously tested in randomized clinical trials.
Test-Directed Elimination DietsA test-directed elimination di-et removes specific foods based on the results of allergy skinprick, blood specific IgE, and/or atopy patch testing [7, 22].The overall success rate for this Btargeted^ approach has beenquite low in both children (48%) and adults (32%) [4]. Thepoor efficacy observed in test-directed elimination diets utiliz-ing IgE-mediated allergy testing (skin prick or blood specific Ta
ble1
Diettrialsin
adultsandpediatrics:Elementald
iets(adults)
Country
Publication
Age
group
Diettherapy
Improvem
ent(%)
Criteria
Causativ
efoods
Timeto
symptom
improvem
ent
USA
Peterson
etal.
2013
[5]
Adults
(n=29)
18completed
thetrial
EleCare
AbbottN
utrition,Abbott
Laboratories,Colum
bus,OH
9(50%
)completehistologic
response
(≤5eos/hpf)
Com
pletehistologicresponse
(≤5eos/hpf)
NA
Noim
provem
ent
Prospectivenon-
random
ized
clinicaltrial
4(22%
)nearly
completeresponse
(6–10eos/hpf)
Nearlycompletehistologic
response
(6–10eos/hpf)
4(22%
)partialresponse
(>10
eos/hpfbut<
half
pretreatmenteos/hpf)
Partialhistologicresponse
(>10
eos/hpfbut<
half
theim
mediatepretreatment
eosinophilcontent)
1(6%)no
response
Netherlands
Warnersetal.
2017
[6]
Adults
(n=21)
17completed
thetrial
Neocate
Nutricia,U
trecht,theNetherlands
12(71%
)completehistological
response
(<15
eos/hpf)
Com
pletehistological
response
(<15
eos/hpf)
NA
4weeks
Prospectivenon-
random
ized
clinicaltrial
Water,black/green
teawith
out
sugar,andsugar-free
chew
ing
gum
perm
itted
4(24%
)partialhistologicalresponse
(≥15
eos/hpfb
ut≥50%
reduction
ofpre-dieteosinophilcount)
Partialhistologicalresponse
(≥15
eos/hpfb
ut≥50%
reduction
ofpre-dieteosinophilcount)
Clinic Rev Allerg Immunol
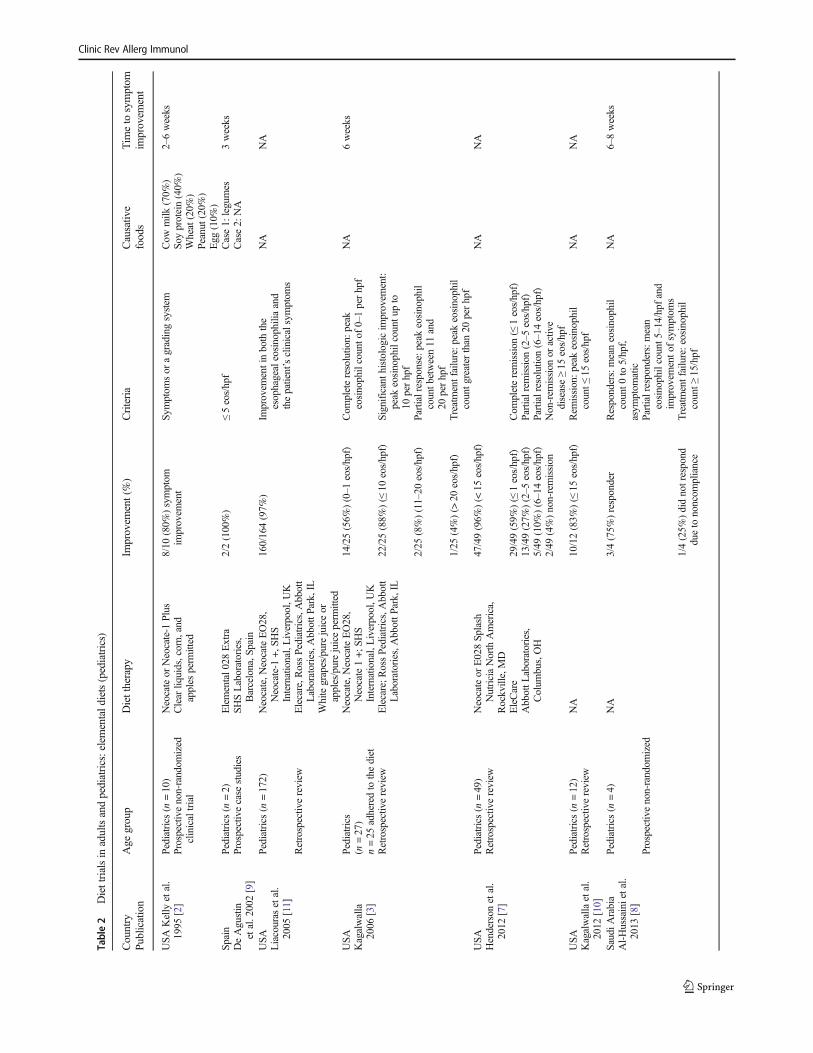
Table2
Diettrialsin
adultsandpediatrics:elementald
iets(pediatrics)
Country
Publication
Age
group
Diettherapy
Improvem
ent(%)
Criteria
Causativ
efoods
Timeto
symptom
improvem
ent
USA
Kelly
etal.
1995
[2]
Pediatrics(n
=10)
Neocateor
Neocate-1
Plus
8/10
(80%
)symptom
improvem
ent
Symptom
sor
agradingsystem
Cow
milk
(70%
)So
yprotein(40%
)Wheat(20%
)Peanut
(20%
)Egg
(10%
)
2–6weeks
Prospectivenon-random
ized
clinicaltrial
Clear
liquids,corn,and
apples
perm
itted
Spain
DeAgustin
etal.2002[9]
Pediatrics(n
=2)
Prospectivecase
studies
Elemental0
28Extra
SHSLaboratories,
Barcelona,S
pain
2/2(100%)
≤5eos/hpf
Case1:
legumes
Case2:
NA
3weeks
USA
Liacouras
etal.
2005
[11]
Pediatrics(n
=172)
Neocate,N
eocateEO28,
Neocate-1
+,SH
SInternational,Liverpool,U
K
160/164(97%
)Im
provem
entinboth
the
esophagealeosinophiliaand
thepatient’sclinicalsymptom
s
NA
NA
Retrospectiv
ereview
Elecare,R
ossPediatrics,Abbott
Laboratories,AbbottP
ark,IL
Whitegrapes/purejuiceor
apples/purejuiceperm
itted
USA
Kagalwalla
2006
[3]
Pediatrics
(n=27)
n=25
adheredto
thediet
Neocate,N
eocateEO28,
Neocate1+;
SHS
International,Liverpool,U
K
14/25(56%
)(0–1
eos/hpf)
Com
pleteresolution:
peak
eosinophilcounto
f0–1perhpf
NA
6weeks
Retrospectiv
ereview
Elecare;R
ossPediatrics,Abbott
Laboratories,AbbottP
ark,IL
22/25(88%
)(≤
10eos/hpf)
Significant
histologicim
provem
ent:
peak
eosinophilcountu
pto
10perhpf
2/25
(8%)(11–20
eos/hpf)
Partialresponse:p
eakeosinophil
countb
etween11
and
20perhpf
1/25
(4%)(>
20eos/hpf)
Treatm
entfailure:p
eakeosinophil
countg
reater
than
20perhpf
USA
Henderson
etal.
2012
[7]
Pediatrics(n
=49)
Retrospectivereview
Neocateor
E028Sp
lash
NutriciaNorth
America,
Rockville,MD
47/49(96%
)(<
15eos/hpf)
NA
NA
EleCare
AbbottL
aboratories,
Colum
bus,OH
29/49(59%
)(≤
1eos/hpf)
Com
pleteremission
(≤1eos/hpf)
13/49(27%
)(2–5
eos/hpf)
Partialremission
(2–5
eos/hpf)
5/49
(10%
)(6–14eos/hpf)
Partialresolution(6–14eos/hpf)
2/49
(4%)non-remission
Non-rem
ission
oractive
disease≥15
eos/hpf
USA
Kagalwallaetal.
2012
[10]
Pediatrics(n
=12)
Retrospectivereview
NA
10/12(83%
)(≤
15eos/hpf)
Rem
ission:p
eakeosinophil
count≤
15eos/hpf
NA
NA
SaudiA
rabia
Al-H
ussainietal.
2013
[8]
Pediatrics(n
=4)
NA
3/4(75%
)responder
Responders:meaneosinophil
count0
to5/hpf,
asym
ptom
atic
NA
6–8weeks
Prospectivenon-random
ized
Partialresponders:m
ean
eosinophilcount5
–14/hpfand
improvem
ento
fsymptom
s1/4(25%
)didnotrespond
dueto
noncom
pliance
Treatm
entfailure:eosinophil
count≥
15/hpf
Clinic Rev Allerg Immunol

IgE) to predict food antigens may be explained by accumulat-ing evidence that esophageal eosinophilic inflammation inEoE is likely independent of IgE [23].
Recently, component resolved diagnostic (CRD) allergytesting, a test measuring sensitization to specific allergenicproteins (e.g., Ara h2 is considered to be a main allergen inpeanut), has been evaluated for predicting EoE food triggers.Unfortunately, a CRD-directed dietary intervention trial foradults with EoE was stopped prematurely when 93% of pa-tients did not improve with the intervention [24] suggestingthe utility of this testing may be low. More recently, esopha-geal and serum IgG4 levels have been considered as possiblepredictors of EoE food triggers for targeted elimination. IgG4levels to foods that are common EoE triggers are increased inpatients with EoE [25] and IgG4 levels to milk allergen com-ponents are unusually high in children with EoE [26] butwhether these measurements can be used to predict food trig-gers is currently unknown.
Food Reintroductions: EoE Triggers
While elimination diets are used to achieve histological andsymptom remission in patients with EoE, they also serve asthe first step in identifying specific food triggers in EoE [27].Once remission is achieved on elimination diets, eliminatedfoods may be sequentially reintroduced to isolate the specificfood triggers among the eliminated foods. In six of the eightstudies where milk, egg, wheat, legumes/soy, seafood, andnuts were reintroduced in patients responding to the SFEDor elemental diet, milk was the most common food triggeridentified [2, 7, 12–17]. In children, 65–74% failed milk rein-troduction [2, 7, 17] while 39–64% of adults had milk as anEoE trigger [12–16]. Wheat was an EoE trigger in approxi-mately 25–40% of adults and children [2, 7, 12, 14–16] with anotable exception of one US study where 60% of adults faileda trial of wheat [13]. There is significant variability in reintro-duction failure rates for egg and soy in studies to date [2, 7,12–17] making it difficult to generalize about responses to eggand soy elimination. In contrast, reintroduction failure ratesfor peanuts/nuts were less variable—accounting as triggersin less than one of five adults and children [12–14, 17] (seeTables 2, 3, 4, 5, 6, 7 for a summary of causative foods iden-tified by food reintroductions in EoE patients responding toelimination diets).
Choosing an Elimination Diet
EoE improves with swallowed topical corticosteroids (tCS)[28–30] and patients treated with tCS often are able to con-sume unrestricted diets. Although swallowed tCS are an ef-fective treatment option when taken correctly, there may beTa
ble3
Diettrialsin
adultsandpediatrics:one-food
elim
inationdiets
Country
Publication
Age
Foodsexcluded
Improvem
ent(%)
Criteria
Timeto
symptom
improvem
ent
USA
Kagalwallaetal.
2012
[10]
Pediatric
(n=17)
Milk
11/17(65%
)(≤
15eos/hpf)
Rem
ission:p
eakeosinophilcount≤
15eos/hpf
NA
Retrospectiv
ereview
7/17
(41%
)(≤
1eos/hpf)
Com
pleteremission:p
eakeosinophilcount≤
1eos/hpf
4/17
(24%
)(2–15eos/hpf)
Significant
improvem
ent:peak
eosinophilcounto
f2–15
eos/hpf
6/17
(35%
)(>
15eos/hpf)
Treatm
entfailure:p
eakeosinophilcount>
15eos/hpf
USA
Kruszew
skietal.
2016
[21]
Pediatric(n
=20)
n=14
completed
Prospective,comparativ
eeffectivenesstrial
Milk
Allpatients
received
PPI
9/14
(64%
)Responders:<15
eos/hpf
6–8weeks
Clinic Rev Allerg Immunol

risks associated with their long-term use. Recent studies oftCS use in children with EoE demonstrate a possible risk ofadrenal suppression [31, 32]. Data from studies in childrenusing the same medications for asthma treatment suggest thatlong-term steroid use may have adverse effects on lineargrowth and bone mineral density [33, 34], although goodquality data in children with EoE is still lacking. Aside frompotential side effects, tCS may simply not achieve remissionin some patients, [35] and young children may be incapable oftaking tCS correctly or refuse to swallow them entirely.Dietary elimination therapy is a feasible alternative formedication-free disease management.
Choice of dietary therapy should be negotiated with thepatient or family, considering disease severity, response (orlack of response) to previous therapies, family dynamics, fi-nancial resources, and most notably the patient’s quality of lifeand nutritional status. In children with significant feeding dys-function, or older patients with stricturing or narrow caliperesophagus, it may be prudent to treat EoE with tCS in order toachieve remission quickly without the learning curve associ-ated with diet therapy.
For patients embarking on an elimination diet, consultationwith a registered dietitian, ideally with knowledge of eosino-philic gastrointestinal diseases, is strongly recommended [1].EoE specialists may recommend a step-down approach todietary elimination; that is, removing all allergens simulta-neously and confirming disease remission beforereintroducing foods. When compared to a step-up approach,where foods are removed in an accumulative fashion, a step-
down elimination may lessen the psychological weight ofprogressive and, in some cases, prolonged diet elimination.
Empiric Elimination: Foods CustomarilyExcluded
Cow’s Milk Restriction of cow’s milk from the diet includesfluid milk, cheese, yogurt, ice cream, and butter. Because heatdestroys conformational isotopes in cow’s milk, it has beenhypothesized that EoE patients may tolerate cow’s milk inextensively heated (baked) goods. Data from a small cohortof adults supports this idea [36]; however, until more data isavailable, complete cow’s milk elimination, including avoid-ance of milk in baked goods, is recommended [37]. Owing tothe cross-reactivity of cow’s milk with other mammalianmilks in IgE-mediated food allergy [38], such products, likegoat milk and sheep cheese, should also be avoided during anempiric elimination diet.
Cow’s milk avoidance is especially difficult when soy isconcurrently restricted in the empiric elimination diet becausemany cow’s milk substitutes are soy-based. However, appro-priate plant-based milk alternatives, such as rice, coconut,hemp, potato, flax, and pea, and for patients following theFFED, almond and cashew beverages are widely available.These alternative beverages are often enriched with calcium,vitamin D, and sometimes vitamin A, B vitamins, and phos-phorus, but are poor sources of dietary fat and protein [39].While useful in baking and other cooking applications in place
Table 5 Diet trials in adults and pediatrics: four-food elimination diets
CountryPublication
Age group Foods excluded Improvement (%) Criteria Causativefoods
Time to symptomimprovement
SpainMolina-Infante
et al. 2014 [18]
Adults (n = 52)Prospective non-
randomizedclinical trial
Mammalian milk,wheat/gluten-containing grains,eggs, andsoy/legumes.
28/52 (54%) Clinical (50% decreasein symptom score) andhistologic (< 15 eos/hpf)remission
Milk (50%)Egg (36%)Wheat (31%)Legumes (18%)
6 weeks
USA Kagalwallaet al. 2017 [19]
Pediatrics (n = 78)Prospective non-
randomizedclinical trial
Milk, egg, wheat, soy 50/78 (64%) < 15 eos/hpf Milk (85%)Egg (35%)Wheat (33%)Soy (19%)
8 weeks
Table 4 Diet trials in adults and pediatrics: two-food elimination diets
CountryPublication
Age Foods excluded Improvement(%)
Criteria Causative foods Time to symptomimprovement
SpainMolina-Infante
2017 [20]
Adults and pediatric(n = 130)
105 adults, 25 pediatricProspective
non-randomizedclinical trial
Animal milks andgluten-containingcereals
56/130 (43%) Symptom improvementand < 15 eos/hpf
Milk (52%)Gluten containing
cereals (16%)Both (28%)
NA
Clinic Rev Allerg Immunol
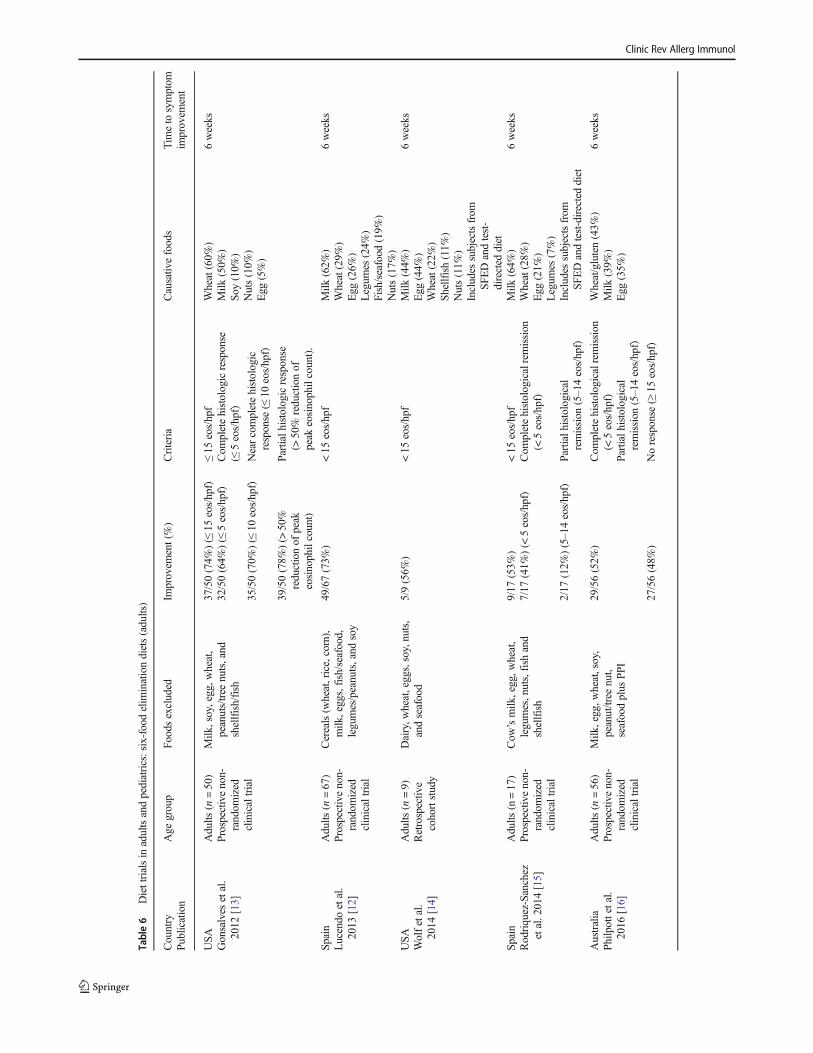
Table6
Diettrialsin
adultsandpediatrics:six-foodelim
inationdiets(adults)
Country
Publication
Age
group
Foodsexcluded
Improvem
ent(%)
Criteria
Causativ
efoods
Timeto
symptom
improvem
ent
USA
Gonsalves
etal.
2012
[13]
Adults
(n=50)
Prospectivenon-
random
ized
clinicaltrial
Milk
,soy,egg,w
heat,
peanuts/treenuts,and
shellfish/fish
37/50(74%
)(≤15
eos/hpf)
≤15
eos/hpf
Wheat(60%
)Milk
(50%
)So
y(10%
)Nuts(10%
)Egg
(5%)
6weeks
32/50(64%
)(≤5eos/hpf)
Com
pletehistologicresponse
(≤5eos/hpf)
35/50(70%
)(≤10
eos/hpf)
Nearcompletehistologic
response
(≤10
eos/hpf)
39/50(78%
)(>50%
reductionof
peak
eosinophilcount)
Partialhistologicresponse
(>50%
reductionof
peak
eosinophilcount).
Spain
Lucendo
etal.
2013
[12]
Adults
(n=67)
Prospectivenon-
random
ized
clinicaltrial
Cereals(w
heat,rice,corn),
milk
,eggs,fish/seafood,
legumes/peanuts,and
soy
49/67(73%
)<15
eos/hpf
Milk
(62%
)Wheat(29%
)Egg
(26%
)Legum
es(24%
)Fish/seafood
(19%
)Nuts(17%
)
6weeks
USA
Wolfetal.
2014
[14]
Adults
(n=9)
Retrospectiv
ecohortstudy
Dairy,w
heat,eggs,soy,nuts,
andseafood
5/9(56%
)<15
eos/hpf
Milk
(44%
)Egg
(44%
)Wheat(22%
)Sh
ellfish
(11%
)Nuts(11%
)Includes
subjectsfrom
SFEDandtest-
directed
diet
6weeks
Spain
Rodriq
uez-Sanchez
etal.2014[15]
Adults
(n=17)
Prospectivenon-
random
ized
clinicaltrial
Cow
’smilk
,egg,w
heat,
legumes,nuts,fishand
shellfish
9/17
(53%
)<15
eos/hpf
Milk
(64%
)Wheat(28%
)Egg
(21%
)Legum
es(7%)
6weeks
7/17
(41%
)(<
5eos/hpf)
Com
pletehistologicalremission
(<5eos/hpf)
2/17
(12%
)(5–14eos/hpf)
Partialhistological
remission
(5–14eos/hpf)
Includes
subjectsfrom
SFEDandtest-directed
diet
Australia
Philp
ottetal.
2016
[16]
Adults
(n=56)
Prospectivenon-
random
ized
clinicaltrial
Milk
,egg,w
heat,soy,
peanut/tree
nut,
seafoodplus
PPI
29/56(52%
)Com
pletehistologicalremission
(<5eos/hpf)
Wheat/gluten(43%
)Milk
(39%
)Egg
(35%
)
6weeks
Partialh
istological
remission
(5–14eos/hpf)
27/56(48%
)Noresponse
(≥15
eos/hpf)
Clinic Rev Allerg Immunol
of fluid milk, plant-based milk alternatives are not to be con-sidered nutritionally equivalent to cow’s milk, especially inthe diets of young children and toddlers [40]. There are, forexample, case reports of protein malnutrition and nutritionalrickets in toddlers inappropriately consuming milk-alternativebeverages such as rice and almond milk [41].
Wheat All wheat-containing bread, pasta, crackers, breakfastcereal, and baked goods must be eliminated. Any foodbreaded, baked, or fried with wheat-based flour must also beexcluded. Whether gluten, the protein contained in wheat,barley, and rye must also be avoided is controversial [42].Some experts do recommend complete gluten restriction [42,43] because of the cross-reactivity of gluten-containing grainswith wheat and the risk of cross contact of barley and rye withwheat in processing. Regardless of the extent of gluten restric-tion, patients should always choose gluten-free oats in lieu ofstandard oats because of the high probability of wheat con-tamination from commercial processing [44]. Patients shouldtake care to avoid primitive forms of wheat like triticale, farro,and spelt, which are easily confused with common gluten-free(and therefore safe) Bancient^ grains such as millet, buck-wheat, and quinoa. These ancient grains used in wheat-alternative products are not always enriched and fortified withessential vitamins and minerals; therefore, alternate sources ofthese nutrients should be included in the diet.
Wheat avoidance can be arduous, owing to the pervasive-ness of wheat in packaged foods. Fortunately, the availabilityof gluten-free, and therefore wheat-free products on the mar-ket has grown in recent years [45]. However, when combinedwith milk, egg, soy, and nut restrictions, finding wheat-freeproducts can be particularly challenging, as many wheat- andgluten-free packaged foods utilize common allergens (such asegg and soy flour) to mimic the mouthfeel and texture ofwheat in baked goods.
Soy Unless the patient frequently consumes soy-based prod-ucts such as soy sauce, tofu, edamame, tempeh, or vegetarianmeat analogs, restricting soy from the diet is less troublesomeas heat-pressed soybean oil and soy lecithin—the derivativesof soy present in many packaged foods—are considered al-lowable during the elimination diet [46, 47]. Soy avoidance isalso made easier with the large number of soy- and milk-freealternatives currently available.
Egg Egg elimination involves restriction of both egg yolk andegg whites. Patients should avoid egg in all forms, includingcooked eggs (scrambled, hard-boiled, and poached eggs; om-elets, quiches, frittatas, and custards), but also egg in bakedgoods such as cookies, cakes and breads. Eggs may be unex-pectedly found in ground meat dishes, such as meatballs,meatloaf and burgers, or in breaded and fried foods, actingas a binder to keep these foods intact. It is important to noteTa
ble7
Diettrialsin
adultsandpediatrics:six-foodelim
inationdiets(pediatrics)
Country
Publication
Age
group
Foodsexcluded
Improvem
ent
Criteria
Causativ
efoods
Timeto
symptom
improvem
ent
USA
Kagalwallaetal.2006[3]
Pediatrics(n
=39)
n=35
completed
Retrospectiv
ereview
Cow
’smilk,soy,w
heat,egg,
peanut/tree
nuts,
andseafood
10/35(29%
)(0–1
eos/hpf)
Com
pleteresolutio
n:peak
eosinophil
counto
f0–1perhpf
NA
6weeks
26/35(74%
)(≤
10eos/hpf)
Significant
histologicim
provem
ent:
peak
eosinophilcountu
pto
10perhpf
3/35
(9%)(11–20
eos/hpf)
Partialresponse:p
eakeosinophilcount
between11
and20
perhpf
6/35
(17%
)(>
20eos/hpf)
Treatm
entfailure:p
eakeosinophilcount
greaterthan
20perhpf
USA
Kagalwallaetal.2011[17]
Pediatric
(n=36
completed
food
reintro
ductions)
Retrospectiv
ereview
Cow
’smilk,soy,w
heat,egg,
peanut/tree
nuts,
andseafood
NA
NA
Milk
(74%
)Wheat(26%
)Eggs(17%
)So
y(10%
)Peanut
(6%)
NA
USA
Henderson
etal.2012[7]
Pediatric
(n=26)
Retrospectiv
ereview
Milk
,soy,w
heat,egg,peanuts/
treenuts,and
fish/shellfish
21/26(81%
)(<
15eos/hpf)
Milk
(65%
)Egg
(40%
)Wheat(37%
)So
y(38%
)
NA
10/26(39%
)(≤
1eos/hpf)
Com
pleteremission
(≤1eos/hpf)
6/26
(23%
)(2–5
eos/hpf)
Partialremission
(2–5
eos/hpf)
5/26
(19%
)(6–14eos/hpf)
Partialresolution(6–14eos/hpf)
5/26
(19%
)non-remission
Non-rem
ission
oractivedisease
≥15
eos/hpf
Clinic Rev Allerg Immunol

that traditional mayonnaise contains emulsified egg, and eggBsubstitutes^ (e.g., Egg Beaters) are simply egg whites andshould also be avoided. A number of allergen-free optionsexist for replacing eggs in baking, such as flax meal or chiaseeds mixed with water, tapioca starch, fruit purees, and gar-banzo Baquafaba^ [48]. Although some patients with IgE-mediated egg allergymay tolerate baked egg, this has not beensystematically investigated in EoE [49].
Peanut and Tree Nut Some patients with EoE avoid peanutsand/or tree nuts due to IgE-mediated allergy [50]. Seeds andseed butters, such as sunflower and pumpkin, are good re-placements nutritionally and practically, as they can be usedin the same culinary applications as peanut and tree nut coun-terparts. Trail mix, granola, and cereal bars often contain nuts,but due to the increasing popularity of Mediterranean, vegan,and Paleolithic style diets, nuts appear unexpectedly in somespecialty items, like certain Bcheeses^ and dips created fromsoaked cashews and baked goods containing nut flour.
Highly refined peanut oil is safe for consumption during anelimination diet [47]; however, cold- and expeller-pressed nutoils retain allergenic protein and therefore should be avoided[51]. Despite its designation as a declared allergen by theFDA, coconut is often well-tolerated by individuals with pea-nut and tree nut allergies [52] and is not a common allergen.Because it is not considered a tree nut, coconut and coconutmilk-based beverages, yogurt, and ice creams are useful cow’smilk alternatives.
Fish and ShellfishDepending on geographic location and fam-ily preferences, seafood may or may not be a major contribu-tor to the diet. Certain condiments, like Worcestershire sauceand Caesar salad dressing, often contain fish or anchovies.Fish oil supplements should be avoided, as well as health-foods enriched with fish-derived omega-3 fatty acids includ-ing EPA and DHA [53]. Algal oils contain both EPA andDHA and are therefore a suitable alternative to fish/krill oil.
Educating Patients
Reading Labels Foods in their whole-state are often easy toidentify: a block of cheese, a bag of peanuts, a scrambled egg.But, in modern society, most individuals consume an assort-ment of whole and processed foods. Allergen content may notbe visually obvious in processed and packaged foods; thus,proficient label reading is an essential skill when following anelimination diet. The Food Labeling and Consumer ProtectionAct of 2004 (FALCPA) requires disclosure of the top 8 com-mon allergens in the USA (cow’s milk, soy, egg, wheat, pea-nut, tree nuts, fish, crustacean shellfish) [54]. The allergenmust be clearly disclosed using its common name within theingredient list. FALCPA applies to all domestic and imported
packaged food products and dietary supplements regulated bythe Food and Drug Administration (FDA). Food labeling lawsvary across the globe; consequently, allergen declarations varyby country [55].
Some food packages bear advisory statements, complicatinga consumer’s discernment of its allergen content. Such declara-tions include statements that a product was Bprocessed in thesame facility^ or Bmanufactured on shared equipment^ with aparticular allergen. These statements are not mandatory and theverbiage does not imply degree of risk. For example, a foodbearing the statement Bmay contain^ is not more likely to in-clude the named allergen than a food label stating Bprocessed ina shared facility^ [56]. Although most foods with advisorystatements do not contain detectible levels of the stated allergen,it is important for highly allergic individuals to proceed withcaution. Certain foods are considered Bhigh risk^: dark choco-late, candies, cereal bars, and other confections have been foundto be more likely to contain traces of milk and nuts than areother foods bearing advisory statements [57]. This is a crucialdetail not only for persons with IgE-mediated allergies, but alsofor patients following an empiric elimination diets, as it is un-known what amount of an antigen has the ability to induceeosinophilic inflammation. As a precaution, patients maychoose to avoid foods bearing allergen advisory statements.However, if a suitable alternative is not available, then suchfoods may be permissible to allow variety in the diet [47].
For patients following test-directed diets, identifyingprohibited foods within ingredient lists can be problematic.Often times, the foods eliciting positive test results are notcommon allergens (such as corn, pea, and apple) and thereforedo not require explicit identification on food labels accordingto FALCPA. On the surface, restricting these foods may notseem burdensome, but foods such as corn, other grains, le-gumes, fruits, and vegetables can be difficult to recognize iningredient lists, as they may be hidden in vague ingredientterms, such as Bnatural flavors^ or Bspices^ [37]. In suchcases, the patient may need to contact the manufacturer toclarify the source of ingredients; otherwise, the food shouldbe excluded from the diet altogether. The additional burdenassociated with this type of label-reading should beunderscored, considering the stress that already accompaniesdaily living with EoE [58].
Preventing Cross Contact Cross contact occurs when non-allergenic foods are unintentionally tainted with allergens.This can happen in the home when other family membersshare the patient’s restricted foods. Common sources of crosscontact in the home include shared condiments (for example,as when double-dipping a knife transfers wheat crumbs into ajelly jar) as well as utensils that are hard to clean, such ascolanders, slotted spatulas, and toaster appliances. Cross con-tact can occur in other settings, such as restaurants if staffmembers are not properly trained or inattentive to consumer
Clinic Rev Allerg Immunol

requests. French fried potatoes cooked in the same fryers asbreaded foods are contaminated with wheat and should beavoided. Grills, marinades, cutting boards are all potentialtransferors of allergens. At supermarkets, the deli slicers, bulkbins, and salad bars all pose risk of cross contact.
Other Dietary Considerations
Prolonged Meal Times Children and adults may adapt feedingbehaviors to avoid odynophagia and dysphagia by excessivelychewing and Bwashing down^ each bite of food with fluids.This behavior can prolong meal times and limit the sum ofcalories consumed at each meal [59]. In schools where lunch-time is hurried, childrenmay not have enough time to eat a fullmeal.
Feeding Problems Infancy and toddlerhood provide a criticalwindow for oral motor skill development. Maturation of skillsoccurs between birth and 24months of age [60]. When infantsand toddlers associate eating with discomfort during thisphase, they may develop an immature diet, consuming onlyliquids and purees in favor of highly textured foods [61]. Intoddlers and young children with EoE, this learned behavior isthe most common cause of feeding dysfunction [61]. Thechild, experiencing discomfort with each eating encounter,then associates food with discomfort and adapts feeding be-havior as a result. Poor intake can be exacerbated by well-intentioned caregivers who repeatedly and anxiously offerfoods, especially when the child struggles to gain weight ap-propriately [59]. Undergoing feeding therapy before the pa-tient has achieved remission can be counterproductive, asfeeding may incite pain and thus exacerbate apprehensiontowards eating. Although dietary elimination and tCS are ef-fective treatments and resolve eosinophilic inflammation,feeding issues often persist despite remission [62].
Pollen Food Allergy Syndrome Fresh fruits and vegetables arethe foundation of a nutrient-dense, balanced diet and are im-portant components of an empiric elimination diet. However,adolescents and adults with EoE may be prone to tree (e.g.,birch) or grass pollen sensitization, and therefore the symp-toms (oral swelling and itching) of pollen food allergy syn-drome (PFAS) when consuming raw fruits and vegetables[63]. In one study, nearly half of adults with EoE reportedPFAS [64]. Ram et al. [65] found that children with EoE andallergic rhinitis may have exacerbations of esophageal eosin-ophilia during pollen seasons suggesting aero-allergen andcross-reacting food allergens may play a role in eosinophilicinflammation. While there is still some uncertainty whetherthese cross-reactions affect eosinophilic inflammation, theoral discomfort associated with intake of certain fresh fruitsor vegetables may reduce variety in patients’ diets further.
Microbiome The gut microbiota plays a significant role inimmune system maturity and function. Early life dysbiosismay in f luence food a l l e rgy pa thogenes i s [66] .Environmental factors such as a low-fiber, high fat diet, anti-biotic use, cesarean delivery, and lack of breastfeeding caninduce gut microbiota dysbiosis, and have been associatedwith the occurrence of food allergy [67]. A very recent studyindicates the following risk factors for the development ofEoE: preterm labor, maternal fever, cesarean delivery, anduse of antibiotic or acid suppressants during infancy [68]which may also affect gut microbiota. Studies on the micro-biota in EoE, however, focus on the esophageal microbiome[69, 70], and it is unknown to what degree diet modifies mi-crobiota at this site in the gastrointestinal tract. Future studiesmay address how the diet elimination alters gut microbiotaand perhaps precursors of esophageal inflammation.
The Elemental Diet
The elemental diet has been shown to be an extremely effec-tive treatment for EoE [2, 7, 71]. Despite its efficacy, theelemental diet is often reserved for patients with refractorydisease for whom empiric elimination diets and/or tCS areineffective. Because of the psychosocial upset associated withcomplete food elimination and the financial burden associatedwith cost of elemental formula, the elemental diet is typicallynot the first method of dietary therapy [72].
The elemental diet involves complete avoidance of all die-tary antigens, thus all foods and naturally derived ingredients(although some studies deviate by allowing fruit/vegetable/juices) [2, 11]. Although costly and socially challenging, theelemental diet does not cause nutritional deficiencies, as ami-no acid-based formulas fulfill macro- and micronutrient re-quirements. However, a prolonged elemental diet coursemay lead to coenzyme Q10 deficiency, as this nutrient is notpresent in formulas [73]. Whether extensively hydrolyzed ca-sein formula, marketed as hypoallergenic and often toleratedby patients with other forms cow’s milk allergy, should beused during the elemental diet phase of treatment in patientswith EoE is uncertain [1]. One adult trial from Spain did show88% (15/17) of adults with milk-driven EoE tolerated an ex-tensively hydrolyzed formula [74], but studies in children arelacking. Amino acid-based formulas are now available in avariety of flavors and ready-to-feed preparations, but it re-mains challenging for patients to orally consume the requiredvolume to deliver complete nutrition. Administration via gas-tronomy or nasogastric tube may be necessary [71].
Because the patient avoids all foods, maintaining and pro-moting oral skills should be a priority for the duration of theelemental diet, especially in children under the age of 2 andolder children with established feeding dysfunction. When allsolid foods are absent from the diet, children, especially
Clinic Rev Allerg Immunol

infants and toddlers, are at risk for delayed oral-motor skilldevelopment [75]. Food products lacking of antigenic foodprotein, such as artificially flavored candies, popsicles, anddrinks, may be permissible to provide solid food for oral stim-ulation during the elemental diet [72]. Semi-solid, amino acid-based medical food (Neocate Nutra) is also a safe, construc-tive tool to use for skill development during this time. Oralintake should be monitored in conjunction with speech andoccupational therapists, especially in children with preexistingfeeding dysfunction.
Food Reintroduction Trials
Post-empiric Elimination After the preliminary phase of dietelimination, typically 8–12 weeks, a follow-up endoscopywith biopsies is performed to assess the state of esophagealmucosa and confirm disease remission.
If the empiric elimination diet is successful in achievingsymptomatic and histologic remission, single food groupsare thereafter added sequentially, with endoscopic and histo-logic evaluation between reintroduction of each separate aller-gen. Trialed foods should be offered most days of the week(5–7 days/week), with an age-appropriate serving size con-sumed at each interval. If the patient develops symptoms with-in the trial period, the food should be removed, with a 6-weekwash-out [43] before either reattempting the same food toconfirm failure, or abandoning the food and moving to thenext. Absence of symptoms does not imply that EoE remainsinactive, as symptoms poorly correlate with histology, there-fore endoscopic and histologic evaluation is required [62].This process of reintroduction may vary among clinicians asthere are no standardized protocols for food reintroductions(number of foods to introduce in a trial, length of the food trial,and length of wash-out) [27].
Because cow’s milk, wheat, and egg are the most commontriggers of EoE in both children and adults, it may be judiciousto reintroduce less provocative foods such as seafood, nuts,and soy earlier in the food trial process following the SFED[76]. Each food is trialed, except for those with IgE-mediatedallergy, until the offending food(s) are identified and the leastrestrictive diet is achieved.
Post-elemental DietOnce EoE remission is achieved and con-firmed by endoscopy, single-ingredient foods are individuallyreintroduced, followed by endoscopic evaluation after a trialof each food or group of foods to gradually rebuild the diet.Duration of food trials and number of foods introduced be-tween endoscopies vary between medical centers and physi-cians. Adding one new single-ingredient food every 2 weeks,with follow-up endoscopies every 12 weeks to evaluate dis-ease activity is common practice. Another approach is to ad-vance foods in order of increasing allergenicity, beginning
with fruits and vegetables, followed by the addition ofwheat-free grains, and eventually animal meats and legumes[72].
It is also necessary to consider the patient’s individualneeds and preferences when planning food reintroductions.Certain single-ingredient foods provide variety in texture, fla-vor, and culinary application and are good choices for prelim-inary food trials. For example, corn is available in manyforms, from corn on the cob, puffed corn cereal, corn noo-dles/pasta, air-popped popcorn and kettle corn, and grits/po-lenta. Choosing nutrient- and calorically dense foods maymoderate the reliance on amino acid-based formulas for nutri-tion and hasten the transition to a solid food diet withoutformula supplementation.
During this phase of food reintroduction, health care pro-viders may adjust the formula prescription as food trials prog-ress. Children may experience fatigue as a consequence of themonotony of limited diet choices and may not regularly con-sume Bsafe^ foods. In some cases, formula intake may need tobe increased to compensate for decreased oral food intakedespite progression of variety of allowable foods in the diet.Conversely, excessive weight gain can occur if formula vol-ume is maintained despite the addition of several caloricallydense foods. As formula is weaned and the diet variety in-creases, vitamin andmineral supplementationmay be requiredto ensure adequate intake. Achieving a nutritionally completediet may take several months to several years [7].
Nutritional Implications of Elimination Diets
Growth andWeightAt diagnosis, patients with EoEmay haveexisting nutritional deficits including impaired growth orweight. More than 15% of children, for example, presentedwith failure to thrive at the time of EoE diagnosis in one USstudy [77]. In France, a downward shift in the distribution ofweight-for-height was also observed in children at EoE diag-nosis [78]. IgE-mediated food allergy, a comorbid conditioncommonly found in children with EoE [77], may also reducegrowth [79–83] and weight [79–82, 84]. Pediatric EoE pa-tients with comorbid Bcow’s milk allergy^ may be at highestrisk of impaired growth [83, 85] at the time of EoE diagnosis.
Excluding foods from the diet that significantly contributeto energy, protein, andmicronutrient intake could theoreticallyresult in (or exacerbate) negative anthropometric profiles inchildren and adults with EoE. However, in the few studies thathave examined the impact of therapeutic elimination diets inpatients with EoE, growth and/or weight were not negativelyaffected. Colson et al. found that short-term elimination dietsdid not worsen weight-for-height z-scores in children withEoE [78]. Moreover, in a US observational study, childrenwho were underweight before initiating an elimination dietfor EoE experienced an increase in weight after starting the
Clinic Rev Allerg Immunol

diet. Height and weight were also not negatively altered in theremaining patients who were treated with diet therapy overvarious lengths of follow-up [11]. In a study of adults withEoE treated with the six food elimination diet, body weightalso did not significantly change after the intervention [12]. Itis likely, however, that close monitoring and/or dietarycounseling in each of these studies contributed to the favor-able anthropometric outcomes [79, 84].
While these studies of medically supervised eliminationdiets for EoE are reassuring, other studies do suggest growthand weight could be negatively affected when multiple foodsare excluded from the diet. Adults excluding all foods (fol-lowing an elemental diet) to manage EoE lost significantweight during a short-term trial [5]. A UK observational studyof IgE- and non-IgE-mediated food allergies, for example,found children who eliminated ≥ 3 foods were at the highestrisk for lower weight [80]. Other studies of children avoidingfoods due to IgE-mediated food allergy have also showngrowth negatively correlates with the number of foodsavoided [81, 86]. While factors related to IgE-mediated foodallergy and atopic comorbidities (e.g., increased intestinal per-meability) [87] may explain these growth deficits, inadequateintake cannot be dismissed as causal [88]. Patients with EoEeliminating multiple foods may face similar risks.
Although impaired growth and low weight predominate asconcerns when foods are excluded from the diet, excessiveweight gain can occur—even when multiple foods are elimi-nated. Indeed, a significant proportion (12%) of children withIgE- and non-IgE-mediated food allergies who were exclud-ing ≥ 3 foods were obese [80]. In a large retrospective study ofadults eliminating gluten to manage celiac disease, 16% ofpatients with low or normal BMI class moved into the over-weight BMI class when following a gluten-free diet [89].While improved absorption may have played a role in thelatter study, poor food selection [90, 91] and/or improvedappetite (due to reduced symptoms when following the elim-ination diet) [92] may contribute to excess weight gain—bothof which can occur in patients with EoE.
Given the aforementioned risks, anthropometric measure-ments (height, weight, and body mass index) should beassessed in adults and children prior to initiating any therapeu-tic elimination diet for EoE and then be monitored for excessloss and gains after diet commencement. Children with EoEand comorbid IgE-mediated food allergy should be mostclosely monitored to mitigate risk of faltering growth.
Macronutrients Elimination diets to manage EoE often re-move common sources of fats (milk, egg, fish, nuts), protein(milk, egg, soy, fish, nuts, legumes), and complex carbohy-drates (wheat) from the diet thereby placing patients that fol-low these diets at risk for macronutrient intake inadequacies orimbalances.
Dietary fats include saturated, monounsaturated, and poly-unsaturated fatty acids, the latter of which include omega-3and omega-6 fatty acids. Omega-6 fatty acids are found innuts, seeds, poultry, eggs, and whole-grains while goodsources of omega-3 fatty acids include cold-water oily fish,nuts, eggs, and milk from grass-fed cows. Patients with EoEwho eliminate milk, egg, fish, and nuts may therefore be atrisk of insufficient or imbalanced polyunsaturated fatty acids(PUFA) intake—fats important to brain development [93] andoptimal health [94]. Indeed, children eliminating major foodallergens (e.g., milk, egg, fish) to manage IgE-mediated foodallergy or atopic dermatitis were found to have lower plasmaomega-3 polyunsaturated fatty acid levels compared to theirpeers [95] and failed to meet omega-3 and omega-6 intakerequirements [96]. Moreover, insufficient essential fatty acid(linoleic acid, ω6 and alpha linolenic acid, ω3) levels wereevident in a significant proportion of pediatric patients onelimination diets to manage food allergies [95, 97].Consequently, nutritional recommendations for EoE patientseliminating milk, nuts, and fish (common polyunsaturated fat-ty acid sources) should include food substitutes with linolenicand linoleic acids (e.g., algae, hemp, flax, and chia seeds) and/or vegetable oils (e.g., olive, safflower, corn, or canola oils).
While elimination diets for EoE may negatively impact fatintake, protein intake may be less affected. Children excludingone or more of the top food allergens to manage IgE- and non-IgE-mediated food allergies met or exceeded protein intakerecommendations [81, 98]. Even children on milk-free dietsexceeded minimum protein intake recommendations by 2–3-fold in one study [83]. In adults in the USA, only 16% of totalprotein intake comes from dairy [99]; consequently, dairy ex-clusion may have little effect on overall protein intake. Infantsand toddlers, however, may be more affected by milk exclu-sion as milk often comprises a significant portion of their diet.For these children or children with feeding dysfunction or oralmotor skill deficits, intake of animal protein may not be suf-ficient to recoup protein averted from milk avoidance.Therefore, the panel on the Diagnosis and Rationale forAction against Cow’s Milk Allergy (DRACMA) recommendschildren with cow’s milk allergy (or in the case of EoE, cow’smilk avoidance) be prescribed a substitute formula until age 2[40]. Plant-based milk alternatives should not be used in in-fants and toddlers as a primary source of nutrition.
While total protein intake may be minimally affected, pro-tein Bquality^ may be affected with some elimination diets.Limited research suggests, for example, that animal proteinsmay stimulate a more robust skeletal muscle protein syntheticresponse than isonitrogenous plant proteins due to differencesin digestibility, amino acid composition, and/or amino acidkinetics [100]. Additionally, newmethods of assessing proteinquality (based on the digestibility of individual amino acids)suggests that compared to wheat and peas, proteins like milkand soy provide far more digestible amino acids than
Clinic Rev Allerg Immunol

previously understood [101]. Thus, when milk and soy areexcluded from the diet, nutrition advice in these cases shouldinclude recommendations to include other animal proteinsources when possible, combinations of plant-based proteinsor protein powders (rice, pea, and seed) to create a completeamino acid profile [100], or amino acid-based formulas toensure sufficient amino acid diversity.
When wheat, gluten, and/or legumes are excluded from thediet to manage EoE, soluble and insoluble fiber intake couldbe reduced. Many gluten-free grains, especially rice and corn,are lower in fiber than gluten-containing grains [102]. Gluten-free products may be made with starches (e.g., tapioca) orrefined flours (e.g., rice) with low content in fiber [103]. Notsurprisingly, low intake of fiber has been found in adults [91,104] and children [90] following gluten-free diets to manageceliac disease. Patients with EoE excluding wheat and glutenmay have similar risks. Happily, more recent analyses ofgluten-free packaged products have shown several productscontain the same (and occasionally more) fiber than gluten-containing foods [105–107]. Increased use of pseudo grains(e.g., quinoa, millet, amaranth) containing more fiber and useof hydrocolloids and gums may have contributed to this im-provement [102, 103]. Because higher fiber diets are associ-ated with reduced risk of colon cancer, coronary heart disease,and diabetes [108], EoE patients excluding wheat, gluten, orlegumes from the diet should be encouraged to select gluten-free pseudo andwhole grains (quinoa, buckwheat, oats, brownrice, amaranth, and millet) and products made with thesegrains or gums.
Micronutrients Patients with EoE who eliminate all (or a sub-set) of the major food allergens effectively eliminate commonsources of calcium (milk) and vitamin D (milk, egg, fatty fish),zinc/copper/selenium (nuts, fish, shellfish), B vitamins (milk,wheat, egg), and iodine (milk, shellfish). In the absence ofclose monitoring, these patients may fail to meet intake rec-ommendations for a number of micronutrients important tobone health (calcium, vitamin D) [109], immunomodulation(vitamin D, zinc) [110, 111], and neurological health (B vita-mins, iodine) [112].
While there are no studies of micronutrient intake in EoEpatients, studies of children with food allergies have foundthat excluding milk reduces calcium [81, 85, 113] and vitaminB2 [113] intake; excluding eggs reduces vitamin A and vita-min B2 intake [113]; and excluding wheat and soybeans re-duces intake of zinc, vitamin B2, vitamin B6, and niacin com-pared with intakes in non-allergic children [113]. Likewise, asignificant proportion of children with food allergies fail tomeet vitamin D intake recommendations while avoiding ma-jor food allergens [114, 115] as do the majority of children andadults in the general population in the USA [116, 117].Additionally, infants avoiding milk have been shown to havehigh rates of iodine insufficiency [82]. As expected, the more
foods that are eliminated, the more micronutrient deficienciesmay be observed [113]. EoE patients excluding the majorallergens could have similar nutritional insufficiencies.Nutrition advice should therefore include recommendationsof allergen-free food substi tutes that replace themicronutrients eliminated, supplemented formulas, and/or vi-tamin and mineral supplements [47]. Pre-existing nutritionaldeficiencies should be addressed prior to starting eliminationdiets and re-assessed regularly as intake and needs are likely tochange over time.
While inadequate intake of micronutrients may be a con-cern for EoE patients following elimination diets, micronutri-ent absorption may also be affected in some patients. High-dose proton pump inhibitor (PPI) therapy is used to excludeGERD-associated esophageal eosinophilia and PPI-responsive esophageal eosinophilia when diagnosing EoE[1]. Proton pump inhibitor therapymay also be continued afterdiagnosis to manage symptoms of EoE [118]. Consequently, asignificant proportion of EoE patients may use PPI. Becausemineral salts and protein-bound vitamin B12 require an acidicenvironment for digestion, decreased stomach acid as a resultof PPI therapy could theoretically result in poor absorptionand consequently micronutrient deficiencies. Evidence forcalcium, iron, and magnesium deficiencies with PPI use isinconsistent, but some studies do suggest an increased riskof vitamin B12 deficiency with PPI therapy [119]. However,the overall quality of evidence supporting any of these possi-ble adverse effects is low or very low [120]. Consequently,b e s t p r a c t i c e g u i d e l i n e s f r om t h e Ame r i c a nGastroenterological Association do not recommend micronu-trient supplementation beyond the recommended daily intakesfor patients on PPI [120]. Patients, however, should be closelymonitored to ensure recommended intakes are met.
In addition to the risk of deficient intake of micronutrientswhen following elimination diets to manage EoE, excess in-take of non-essential heavy metals may also be a concern.Gluten-free products are often made with rice [121]—one ofthe primary sources of inorganic arsenic in the US diet [122].In recent population studies, persons consuming a gluten-freediet were found to have high levels of urinary arsenic [123,124], blood methylmercury [123, 124], and blood cadmiumand lead [124]. These heavy metals are known carcinogensand toxicants that can cause numerous adverse health effectsin humans that are dose dependent [125] . Patients avoidingwheat or gluten should be advised to select products madewith a variety of grains and starches and avoid solely depend-ing on any one grain. Patients avoiding cow’s milk shouldsimilarly select a variety of milk substitutes and avoid excessconsumption of rice milk. Moreover, the American Academyof Pediatrics and the European Food Standards Agency do notrecommend giving rice milk to young children.
When children and adults exclude major food allergens,care should be taken to recommend food substitutes that
Clinic Rev Allerg Immunol

increase essential micronutrient intake while minimizing in-take of non-essential heavy metals.
Barriers and Facilitators of Diet Adherence
Adherence to medical or lifestyle interventions to manage anychronic disease is generally poor with non-adherence rates indeveloped countries estimated to be approximately 50%[126]. Very little, however, is known about adherence ratesto diet therapies to manage EoE. In one of the few studiesexamining adherence to elimination diets in children with eo-sinophilic gastrointestinal disorders, 33% of the children re-ported at least one food allergen exposure over a 2-week pe-riod [127]. In a second study, non-adherence to diet restric-tions appeared to be more common in teenagers than in youngchildren [128]. In adults following the most restrictive of elim-ination diets—the elemental diet—the dropout and non-adherence rate was also high (38%) [5].
There are a number of factors that may make followingelimination diets difficult. In studies of patients prescribedrestrictive dietary interventions for other chronic diseases, fac-tors identified as barriers to following the diets included finan-cial and logistical costs [129, 130], limited availability or va-riety of appropriate foods [129–131], lack of knowledge ofappropriate foods [132], interference with socialization [132,133], and lack of support from family or friends [134]. EoEpatients following elimination diets may have similar barriers.In one focus group study, parents and children with EoEexpressed the most concern about the social impact of elimi-nation diets—Bnot being able to eat what their peers and fam-ily members could eat^ [128]. In a small study of EoE patientsthat were current or former followers of the SFED, former dietfollowers had more anxiety and social challenges with theSFED than those that were currently following the diet. Themajority also found the diet too restrictive [135]. Like otherpatients with chronic diseases following dietary interventions,EoE patients following the SFED may also incur significantfinancial costs. A recent study of shopping costs found thefinancial cost of SFED (for one person) to be $650 per yearmore than the cost of an unrestricted diet when shopping at astandard grocery store in the USA [136]. Moreover, there maybe substantial logistical costs (e.g., additional shopping bur-den) to elimination diets [136].
Fortunately, several of these barriers can be diminished bytrained professionals—ideally a multi-disciplinary team thatincludes gastroenterologists, allergists, nurses, dietitians, andpsychologists. Lack of knowledge of appropriate foods can beaddressed with a well-developed dietary educationBcurriculum^ that includes instruction on label reading, diningout, food substitutions and risks of cross contact with foodallergens while following an elimination diet as describedabove. Practical guidance on educating patients about
elimination diets is masterfully summarized in two recent pub-lications by Groetch et al. and Doerfler et al. [43, 47]. Studiessuggest such dietary education can improve both adherence[129, 132, 137] and the nutritional quality of elimination diets[84, 138]. A skilled dietitian can also increase the palatabilityand variety of an elimination diet despite the restrictions [47]. Aspecialized psychologist can provide support to manage psy-chosocial effects of dietary interventions and EoE itself [139].
Webb and Byrd-Bredbenner suggested that dietary guid-ance to consumers should be Brealistic, consistent, positive,easy-to-understand, actionable, personalized advice that fitswithin their time, money, and skill constraints^ [140]. Thisadvice is equally (if not more) germane to dietary guidancethat is provided to patients following elimination diets.Healthcare professionals should actively engage the patientwhen choosing diet interventions as patient engagement maypromote adherence and therefore diet efficacy [141]. Mostimportantly, dietary guidance should stress optimal health,growth, and development rather than focusing on allergenavoidance alone.
Conclusion
Elimination diets are medication-free option for patients withEoE—effectively reducing both symptoms and esophagealinflammation. Each variation of elimination diet is associatedwith nutritional and social risks, but with proper education andindividualization, elimination diets can be nutritionally com-plete, socially appropriate, and successful in achieving remis-sion. Randomized trials of dietary interventions and foodreintroductions would likely improve our understanding ofelimination diet efficacies and consequently improve care forall patients.
Funding There is no funding source for this review.
Compliance with Ethical Standards
Conflict of Interest KK declares no conflicts of interest. AC has re-ceived honoraria from Nutricia and Abbott Nutrition. CV has receivedhonoraria from Danone, Nestle, Mead Johnson, and DBV Technologies.
Ethical Approval and Informed Consent This article does not containany studies with human participants or animals performed by any of theauthors. The present article is a review; therefore, no informed consentwas required.
References
1. Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, BonisPA et al (2011) Eosinophilic esophagitis: updated consensus rec-ommendations for children and adults. J Allergy Clin Immunol128(1):3–20 e6; quiz 1-2
Clinic Rev Allerg Immunol

2. Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA,Sampson HA (1995) Eosinophilic esophagitis attributed to gastro-esophageal reflux: improvement with an amino acid-based formu-la. Gastroenterology 109(5):1503–1512
3. Kagalwalla AF, Sentongo TA, Ritz S, Hess T, Nelson SP, EmerickKM et al (2006) Effect of six-food elimination diet on clinical andhistologic outcomes in eosinophilic esophagitis. ClinGastroenterol Hepatol 4(9):1097–1102
4. Arias A, Gonzalez-Cervera J, Tenias JM, Lucendo AJ (2014)Efficacy of dietary interventions for inducing histologic remissionin patients with eosinophilic esophagitis: a systematic review andmeta-analysis. Gastroenterology 146(7):1639–1648
5. Peterson KA, Byrne KR, Vinson LA, Ying J, Boynton KK, FangJC, Gleich GJ, Adler DG, Clayton F (2013) Elemental diet in-duces histologic response in adult eosinophilic esophagitis. Am JGastroenterol 108(5):759–766. https://doi.org/10.1038/ajg.2012.468
6. Warners MJ, Vlieg-Boerstra BJ, Verheij J, van Rhijn BD, VanAmpting MT, Harthoorn LF et al (2017) Elemental diet decreasesinflammation and improves symptoms in adult eosinophilicoesophagitis patients. Aliment Pharmacol Ther 45(6):777–787.https://doi.org/10.1111/apt.13953
7. Henderson CJ, Abonia JP, King EC, Putnam PE, Collins MH,Franciosi JP, Rothenberg ME (2012) Comparative dietary therapyeffectiveness in remission of pediatric eosinophilic esophagitis. JAllergy Clin Immunol 129(6):1570–1578. https://doi.org/10.1016/j.jaci.2012.03.023
8. Al-Hussaini A, Al-Idressi E, Al-Zahrani M (2013) The role ofallergy evaluation in children with eosinophilic esophagitis. JGastroenterol 48(11):1205–1212
9. DeAgustin JC, SanzN, CanalsMJ, Alvarez E,Morales JL, Soler Jet al (2002) Successful medical treatment of two patients witheosinophilic oesophagitis. J Pediatr Surg 37(2):207–213
10. Kagalwalla AF, Amsden K, Shah A, Ritz S, Manuel-Rubio M,Dunne K, Nelson SP, Wershil BK, Melin-Aldana H (2012)Cow’s milk elimination: a novel dietary approach to treat eosino-philic esophagitis. J Pediatr Gastroenterol Nutr 55(6):711–716.https://doi.org/10.1097/MPG.0b013e318268da40
11. Liacouras CA, Spergel JM, Ruchelli E, Verma R, Mascarenhas M,Semeao E, Flick J, Kelly J, Brown–Whitehorn T, Mamula P,Markowitz JE (2005) Eosinophilic esophagitis: a 10-year experi-ence in 381 children. Clin Gastroenterol Hepatol 3(12):1198–1206. https://doi.org/10.1016/S1542-3565(05)00885-2
12. Lucendo AJ, Arias A, Gonzalez-Cervera J, Yague-Compadre JL,Guagnozzi D, Angueira T et al (2013) Empiric 6-food eliminationdiet induced and maintained prolonged remission in patients withadult eosinophilic esophagitis: a prospective study on the foodcause of the disease. J Allergy Clin Immunol 131(3):797–804.https://doi.org/10.1016/j.jaci.2012.12.664
13. Gonsalves N, Yang GY, Doerfler B, Ritz S, Ditto AM, Hirano I(2012) Elimination diet effectively treats eosinophilic esophagitisin adults; food reintroduction identifies causative factors.Gastroenterology 142(7):1451–9 e1 quiz e14–5
14. Wolf WA, Jerath MR, Sperry SL, Shaheen NJ, Dellon ES (2014)Dietary elimination therapy is an effective option for adults witheosinophilic esophagitis. Clin Gastroenterol Hepatol 12(8):1272–1279. https://doi.org/10.1016/j.cgh.2013.12.034
15. Rodriguez-Sanchez J, Gomez Torrijos E, Lopez Viedma B, de laSanta Belda E, Martin Davila F, Garcia Rodriguez C et al (2014)Efficacy of IgE-targeted vs empiric six-food elimination diets foradult eosinophilic oesophagitis. Allergy 69(7):936–942. https://doi.org/10.1111/all.12420
16. Philpott H, Nandurkar S, Royce SG, Thien F, Gibson PR (2016) Aprospective open clinical trial of a proton pump inhibitor, elimi-nation diet and/or budesonide for eosinophilic oesophagitis.
Aliment Pharmacol Ther 43(9):985–993. https://doi.org/10.1111/apt.13576
17. Kagalwalla AF, Shah A, Li BU, Sentongo TA, Ritz S, Manuel-Rubio M et al (2011) Identification of specific foods responsiblefor inflammation in children with eosinophilic esophagitis suc-cessfully treated with empiric elimination diet. J PediatrGastroenterol Nutr 53(2):145–149. https://doi.org/10.1097/MPG.0b013e31821cf503
18. Molina-Infante J, Arias A, Barrio J, Rodriguez-Sanchez J,Sanchez-Cazalilla M, Lucendo AJ (2014) Four-food group elim-ination diet for adult eosinophilic esophagitis: a prospective mul-ticenter study. J Allergy Clin Immunol 134(5):1093–1099 e1
19. Kagalwalla AF,Wechsler JB, Amsden K, Schwartz S, MakhijaM,Olive A, Davis CM, Manuel-Rubio M, Marcus S, Shaykin R,Sulkowski M, Johnson K, Ross JN, Riffle ME, Groetch M,Melin-Aldana H, Schady D, Palac H, Kim KYA, Wershil BK,Collins MH, Chehade M (2017) Efficacy of a 4-food eliminationdiet for children with eosinophilic esophagitis. Clin GastroenterolHepatol 15(11):1698–1707.e7. https://doi.org/10.1016/j.cgh.2017.05.048
20. Molina-Infante J, Arias A, Alcedo J, Garcia-Romero R, Casabona-Frances S, Prieto-Garcia A, Modolell I, Gonzalez-Cordero PL,Perez-Martinez I, Martin-Lorente JL, Guarner-Argente C,Masiques ML, Vila-Miravet V, Garcia-Puig R, Savarino E,Sanchez-Vegazo CT, Santander C, Lucendo AJ (2017) Step-upempiric elimination diet for pediatric and adult eosinophilic esoph-agitis: the 2-4-6 study. J Allergy Clin Immunol. https://doi.org/10.1016/j.jaci.2017.08.038
21. Kruszewski PG, Russo JM, Franciosi JP, Varni JW, Platts-MillsTA, Erwin EA (2016) Prospective, comparative effectiveness trialof cow’s milk elimination and swallowed fluticasone for pediatriceosinophilic esophagitis. Dis Esophagus 29(4):377–384. https://doi.org/10.1111/dote.12339
22. Spergel JM, Beausoleil JL, Mascarenhas M, Liacouras CA (2002)The use of skin prick tests and patch tests to identify causativefoods in eosinophilic esophagitis. J Allergy Clin Immunol 109(2):363–368. https://doi.org/10.1067/mai.2002.121458
23. Simon D, Cianferoni A, Spergel JM, Aceves S, Holbreich M,Venter C, Rothenberg ME, Terreehorst I, Muraro A, LucendoAJ, Schoepfer A, Straumann A, Simon HU (2016) Eosinophilicesophagitis is characterized by a non-IgE-mediated food hyper-sensitivity. Allergy 71(5):611–620. https://doi.org/10.1111/all.12846
24. van Rhijn BD, Vlieg-Boerstra BJ, Versteeg SA, Akkerdaas JH,van Ree R, Terreehorst I, Sprikkelman AB, Verheij J, SmoutAJPM, Bredenoord AJ (2015) Evaluation of allergen-microarray-guided dietary intervention as treatment of eosinophil-ic esophagitis. J Allergy Clin Immunol 136(4):1095–1097 e3.https://doi.org/10.1016/j.jaci.2015.02.038
25. Clayton F, Fang JC, Gleich GJ, Lucendo AJ, Olalla JM, VinsonLA, Lowichik A, Chen X, Emerson L, Cox K, O’Gorman MA,Peterson KA (2014) Eosinophilic esophagitis in adults is associ-ated with IgG4 and not mediated by IgE. Gastroenterology 147(3):602–609. https://doi.org/10.1053/j.gastro.2014.05.036
26. Wilson JM, Schuyler AJ, Tripathi A, Erwin EA, Commins SP,Platts-Mills TAE (2016) IgG4 component allergens are preferen-tially increased in eosinophilic esophagitis as compared to patientswith milk anaphylaxis or galactose-alpha-1,3-galactose allergy. JAllergy Clin Immunol. Presented AAAAI 2016
27. Venter C, Fleischer DM (2016) Diets for diagnosis and manage-ment of food allergy: the role of the dietitian in eosinophilic esoph-agitis in adults and children. Ann Allergy Asthma Immunol117(5):468–471. https://doi.org/10.1016/j.anai.2016.08.003
28. Liacouras CA, Wenner WJ, Brown K, Ruchelli E (1998) Primaryeosinophilic esophagitis in children: successful treatment with oralcorticosteroids. J Pediatr Gastroenterol Nutr 26(4):380–385
Clinic Rev Allerg Immunol

29. Aceves SS, Dohil R, Newbury RO, Bastian JF (2005) Topicalviscous budesonide suspension for treatment of eosinophilicesophagitis. J Allergy Clin Immunol 116(3):705–706
30. Konikoff MR, Noel RJ, Blanchard C, Kirby C, Jameson SC,Buckmeier BK, Akers R, Cohen MB, Collins MH, Assa’ad AH,Aceves SS, Putnam PE, Rothenberg ME (2006) A randomized,double-blind, placebo-controlled trial of fluticasone propionate forpediatric eosinophilic esophagitis. Gastroenterology 131(5):1381–1391. https://doi.org/10.1053/j.gastro.2006.08.033
31. Ahmet A, Benchimol EI, Goldbloom EB, Barkey JL (2016)Adrenal suppression in children treated with swallowedfluticasone and oral viscous budesonide for eosinophilic esopha-gitis. Allergy Asthma Clin Immunol 12:49
32. Golekoh MC, Hornung LN, Mukkada VA, Khoury JC, PutnamPE, Backeljauw PF (2016) Adrenal insufficiency after chronicswallowed glucocorticoid therapy for eosinophilic esophagitis. JPediatr 170:240–245. https://doi.org/10.1016/j.jpeds.2015.11.026
33. Turpeinen M, Pelkonen AS, Nikander K, Sorva R, Selroos O,Juntunen-Backman K, Haahtela T (2010) Bone mineral densityin children treated with daily or periodical inhaled budesonide: theHelsinki early intervention childhood asthma study. Pediatr Res68(2):169–173. https://doi.org/10.1203/PDR.0b013e3181e69e36
34. Pedersen S (2006) Clinical safety of inhaled corticosteroids forasthma in children: an update of long-term trials. Drug Saf29(7):599–612
35. WolfWA, Cotton CC, Green DJ, Hughes JT,Woosley JT, ShaheenNJ, Dellon ES (2015) Predictors of response to steroid therapy foreosinophilic esophagitis and treatment of steroid-refractory pa-tients. Clin Gastroenterol Hepatol 13(3):452–458. https://doi.org/10.1016/j.cgh.2014.07.034
36. Leung J, Hundal NV, Katz AJ, Shreffler WG, Yuan Q,Butterworth CA et al (2013) Tolerance of baked milk in patientswith cow’s milk-mediated eosinophilic esophagitis. J Allergy ClinImmunol 132(5):1215–1216 e1
37. GroetchM, HenryM, FeulingMB, Kim J (2013) Guidance for thenutrition management of gastrointestinal allergy in pediatrics. JAllergy Clin Immunol Pract 1(4):323–331. https://doi.org/10.1016/j.jaip.2013.05.002
38. Burks AW, Jones SM, Boyce JA, Sicherer SH,Wood RA, Assa’adA et al (2011) NIAID-sponsored 2010 guidelines for managingfood allergy: applications in the pediatric population. Pediatrics128(5):955–965
39. Singhal S, Baker RD, Baker SS (2017) A comparison of the nu-tritional value of cow’s milk and nondairy beverages. J PediatrGastroenterol Nutr 64(5):799–805. https://doi.org/10.1097/MPG.0000000000001380
40. Fiocchi A, Schunemann HJ, Brozek J, Restani P, Beyer K,Troncone R et al (2010) Diagnosis and Rationale for ActionAgainst Cow’s Milk Allergy (DRACMA): a summary report. JAllergy Clin Immunol 126(6):1119–1128 e12
41. Carvalho NF, Kenney RD, Carrington PH, Hall DE (2001) Severenutritional deficiencies in toddlers resulting from health food milkalternatives. Pediatrics 107(4):E46
42. Kliewer KL, Venter C, Cassin AM, Abonia JP, Aceves SS, BonisPA et al (2016) Should wheat, barley, rye, and/or gluten beavoided in a 6-food elimination diet? J Allergy Clin Immunol137(4):1011–1014
43. Doerfler B, Bryce P, Hirano I, Gonsalves N (2015) Practical ap-proach to implementing dietary therapy in adults with eosinophilicesophagitis: the Chicago experience. Dis Esophagus 28(1):42–58
44. Hernando A, Mujico JR, Mena MC, Lombardia M, Mendez E(2008) Measurement of wheat gluten and barley hordeins in con-taminated oats from Europe, the United States and Canada bySandwich R5 ELISA. Eur J Gastroenterol Hepatol 20(6):545–554. https://doi.org/10.1097/MEG.0b013e3282f46597
45. Marketsandmarkets.com. Gluten-free products market by type,sales channel and geography: global trends and forecasts to2018. Available at http://www.marketsandmarkets.com/MarketReports/gluten-free-products-market-738.html2013
46. Awazuhara H, Kawai H, Baba M, Matsui T, Komiyama A (1998)Antigenicity of the proteins in soy lecithin and soy oil in soybeanallergy. Clin Exp Allergy 28(12):1559–1564. https://doi.org/10.1046/j.1365-2222.1998.00431.x
47. Groetch M, Venter C, Skypala I, Vlieg-Boerstra B, Grimshaw K,Durban R, Cassin A, Henry M, Kliewer K, Kabbash L, Atkins D,Nowak-Węgrzyn A, Holbreich M, Chehade M, EosinophilicGastrointestinal Disorders Committee of the American Academyof Allergy, Asthma and Immunology (2017) Dietary therapy andnutrition management of eosinophilic esophagitis: a work groupreport of the American Academy of Allergy, Asthma, andImmunology. J Allergy Clin Immunol Pract 5(2):312–324 e29 .https://doi.org/10.1016/j.jaip.2016.12.026
48. Borneo R, Aguirre A, Leon AE (2010) Chia (Salvia hispanica L)gel can be used as egg or oil replacer in cake formulations. J AmDiet Assoc 110(6):946–949
49. Leonard SA,Nowak-WegrzynAH (2016) Bakedmilk and egg dietsfor milk and egg allergy management. Immunol Allergy Clin NAm36(1):147–159. https://doi.org/10.1016/j.iac.2015.08.013
50. Assa'ad AH, Putnam PE, Collins MH, Akers RM, Jameson SC,Kirby CL et al (2007) Pediatric patients with eosinophilic esoph-agitis: an 8-year follow-up. J Allergy Clin Immunol 119(3):731–738
51. Teuber SS, Brown RL, Haapanen LA (1997) Allergenicity ofgourmet nut oils processed by different methods. J Allergy ClinImmunol 99(4):502–507
52. Stutius LM, Sheehan WJ, Rangsithienchai P, Bharmanee A, ScottJE, YoungMC, Dioun AF, Schneider LC, Phipatanakul W (2010)Characterizing the relationship between sesame, coconut, and nutallergy in children. Pediatr Allergy Immunol 21(8):1114–1118.https://doi.org/10.1111/j.1399-3038.2010.00997.x
53. Fiocchi A, Bouygue GR, Sarratud T, Terracciano L, Martelli A,Restani P (2004) Clinical tolerance of processed foods. AnnAllergy Asthma Immunol 93(5 Suppl 3):S38–S46. https://doi.org/10.1016/S1081-1206(10)61731-0
54. United States Food and Drug Administration CfFSaAN. FoodAllergen Labeling and Consumer Protection Act of 2004 (TitleII of Public Law 108e282). August 2004 ed2004
55. Allen KJ, Turner PJ, Pawankar R, Taylor S, Sicherer S, Lack G,Rosario N, Ebisawa M, Wong G, Mills EN, Beyer K, Fiocchi A,Sampson HA (2014) Precautionary labelling of foods for allergencontent: are we ready for a global framework? World AllergyOrgan J 7(1):10. https://doi.org/10.1186/1939-4551-7-10
56. Turner PJ, Kemp AS, Campbell DE (2011) Advisory food labels:consumers with allergies need more than Btraces^ of information.BMJ 343(oct13 2):d6180. https://doi.org/10.1136/bmj.d6180
57. Ford LS, Taylor SL, Pacenza R, Niemann LM, Lambrecht DM,Sicherer SH (2010) Food allergen advisory labeling and productcontaminationwith egg,milk, and peanut. J Allergy Clin Immunol126(2):384–385. https://doi.org/10.1016/j.jaci.2010.05.034
58. Taft TH, Ballou S, Keefer L (2012) Preliminary evaluation ofmaternal caregiver stress in pediatric eosinophilic gastrointestinaldisorders. J Pediatr Psychol 37(5):523–532
59. Menard-Katcher C, Henry M, Furuta GT, Atkins D, Maune NC,Haas AM (2014) Significance of feeding dysfunction in eosino-philic esophagitis. World J Gastroenterol 20(31):11019–11022
60. Haas AM, Maune NC (2009) Clinical presentation of feedingdysfunction in children with eosinophilic gastrointestinal disease.Immunol Allergy Clin N Am 29(1):65–75 ix
61. Mukkada VA, Haas A, Maune NC, Capocelli KE, Henry M,Gilman N et al (2010) Feeding dysfunction in children with eo-sinophilic gastrointestinal diseases. Pediatrics 126(3):e672–e677
Clinic Rev Allerg Immunol

62. Pentiuk S, Putnam PE, Collins MH, Rothenberg ME (2009)Dissociation between symptoms and histological severity in pedi-atric eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 48(2):152–160. https://doi.org/10.1097/MPG.0b013e31817f0197
63. van Rhijn BD, van Ree R, Versteeg SA, Vlieg-Boerstra BJ,Sprikkelman AB, Terreehorst I, Smout AJPM, Bredenoord AJ(2013) Birch pollen sensitization with cross-reactivity to food al-lergens predominates in adults with eosinophilic esophagitis.Allergy 68(11):1475–1481. https://doi.org/10.1111/all.12257
64. Mahdavinia M, Bishehsari F, Hayat W, Elhassan A, Tobin MC,Ditto AM (2017) Association of eosinophilic esophagitis and foodpollen allergy syndrome. Ann Allergy Asthma Immunol 118(1):116–117. https://doi.org/10.1016/j.anai.2016.10.012
65. RamG, Lee J, Ott M, Brown-Whitehorn TF, Cianferoni A, ShukerM, Wang ML, Verma R, Liacouras CA, Spergel JM (2015)Seasonal exacerbation of esophageal eosinophilia in children witheosinophilic esophagitis and allergic rhinitis. Ann Allergy AsthmaImmunol 115(3):224–228 e1 . https://doi.org/10.1016/j.anai.2015.07.004
66. Broussard JL, Devkota S (2016) The changing microbial land-scape of Western society: diet, dwellings and discordance. MolMetab 5(9):737–742. https://doi.org/10.1016/j.molmet.2016.07.007
67. Tamburini S, Shen N, HC W, Clemente JC (2016) Themicrobiome in early life: implications for health outcomes. NatMed 22(7):713–722
68. Jensen ET, Kuhl JT, Martin LJ, RothenbergME, Dellon ES (2017)Prenatal, intrapartum, and postnatal factors are associated withpediatric eosinophilic esophagitis. J Allergy Clin Immunol
69. Benitez AJ, Hoffmann C, Muir AB, Dods KK, Spergel JM,Bushman FD, Wang ML (2015) Inflammation-associated micro-biota in pediatric eosinophilic esophagitis. Microbiome 3(1):23.https://doi.org/10.1186/s40168-015-0085-6
70. Harris JK, Fang R,Wagner BD, Choe HN, Kelly CJ, Schroeder S,Moore W, Stevens MJ, Yeckes A, Amsden K, Kagalwalla AF,Zalewski A, Hirano I, Gonsalves N, Henry LN, Masterson JC,Robertson CE, Leung DY, Pace NR, Ackerman SJ, Furuta GT,Fillon SA (2015) Esophageal microbiome in eosinophilic esoph-agitis. PLoSOne 10(5):e0128346. https://doi.org/10.1371/journal.pone.0128346
71. Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA (2003)Elemental diet is an effective treatment for eosinophilic esophagi-tis in children and adolescents. Am J Gastroenterol 98(4):777–782
72. Wechsler JB, Schwartz S, Amsden K, Kagalwalla AF (2014)Elimination diets in the management of eosinophilic esophagitis.J Asthma Allergy 7:85–94. https://doi.org/10.2147/JAA.S47243
73. Miles MV, Putnam PE, Miles L, Tang PH, DeGrauw AJ, WongBL, Horn PS, Foote HL, Rothenberg ME (2011) Acquired coen-zyme Q10 deficiency in children with recurrent food intoleranceand allergies. Mitochondrion 11(1):127–135. https://doi.org/10.1016/j.mito.2010.08.010
74. Lucendo AJ, Arias A, Gonzalez-Cervera J, Mota-Huertas T,Yague-Compadre JL (2013) Tolerance of a cow’s milk-based hy-drolyzed formula in patients with eosinophilic esophagitis trig-gered by milk. Allergy 68(8):1065–1072
75. Delaney AL, Arvedson JC (2008) Development of swallowingand feeding: prenatal through first year of life. Dev Disabil ResRev 14(2):105–117. https://doi.org/10.1002/ddrr.16
76. Davis BP, Rothenberg ME (2013) Emerging concepts of dietarytherapy for pediatric and adult eosinophilic esophagitis. ExpertRev Clin Immunol 9(4):285–287
77. Pelz BJ, Wechsler JB, Amsden K, Johnson K, Singh AM,WershilBK, Kagalwalla AF, Bryce PJ (2016) IgE-associated food allergyalters the presentation of paediatric eosinophilic esophagitis. ClinExp Allergy 46(11):1431–1440. https://doi.org/10.1111/cea.12776
78. Colson D, Kalach N, Soulaines P, Vannerom Y, Campeotto F,Talbotec C, Chatenoud L, Hankard R, Dupont C (2014) The im-pact of dietary therapy on clinical and biologic parameters of pe-diatric patients with eosinophilic esophagitis. J Allergy ClinImmunol Pract 2(5):587–593. https://doi.org/10.1016/j.jaip.2014.05.012
79. BerryMJ, Adams J, VoutilainenH, Feustel PJ, Celestin J, JarvinenKM (2015) Impact of elimination diets on growth and nutritionalstatus in children with multiple food allergies. Pediatr AllergyImmunol 26(2):133–138
80. Meyer R, De Koker C, Dziubak R, Venter C, Dominguez-OrtegaG, Cutts R, Yerlett N, Skrapak AK, Fox AT, Shah N (2014)Malnutrition in children with food allergies in the UK. J HumNutr Diet 27(3):227–235. https://doi.org/10.1111/jhn.12149
81. Flammarion S, Santos C, Guimber D, Jouannic L, Thumerelle C,Gottrand F et al (2011) Diet and nutritional status of children withfood allergies. Pediatr Allergy Immunol 22(2):161–165
82. Thomassen RA, Kvammen JA, Eskerud MB, Juliusson PB,Henriksen C, Rugtveit J (2017) Iodine status and growth in 0-2-year-old infants with cow’s milk protein allergy. J PediatrGastroenterol Nutr 64(5):806–811. https://doi.org/10.1097/MPG.0000000000001434
83. Tuokkola J, Luukkainen P, Nevalainen J, Ahonen S, Toppari J,Ilonen J, Veijola R, Knip M, Virtanen SM, Kaila M (2017)Eliminating cows' milk, but not wheat, barley or rye, increasesthe risk of growth deceleration and nutritional inadequacies.Acta Paediatr 106(7):1142–1149. https://doi.org/10.1111/apa.13846
84. Berni Canani R, Leone L, D'Auria E, Riva E, Nocerino R, RuotoloS et al (2014) The effects of dietary counseling on children withfood allergy: a prospective, multicenter intervention study. J AcadNutr Diet 114(9):1432–1439
85. Robbins KA, Wood RA, Keet CA (2014) Milk allergy is associ-ated with decreased growth in US children. J Allergy ClinImmunol 134(6):1466–1468 e6 . https://doi.org/10.1016/j.jaci.2014.08.037
86. Christie L, Hine RJ, Parker JG, Burks W (2002) Food allergies inchildren affect nutrient intake and growth. J Am Diet Assoc102(11):1648–1651
87. Jarvinen KM, Konstantinou GN, Pilapil M, Arrieta MC, Noone S,Sampson HA et al (2013) Intestinal permeability in children withfood allergy on specific elimination diets. Pediatr AllergyImmunol 24(6):589–595. https://doi.org/10.1111/pai.12106
88. Sova C, Feuling MB, Baumler M, Gleason L, Tam JS, Zafra Het al (2013) Systematic review of nutrient intake and growth inchildren with multiple IgE-mediated food allergies. Nutr ClinPract 28(6):669–675
89. Kabbani TA, Goldberg A, Kelly CP, Pallav K, Tariq S, Peer A et al(2012) Body mass index and the risk of obesity in coeliac diseasetreated with the gluten-free diet. Aliment Pharmacol Ther 35(6):723–729
90. Ohlund K, Olsson C, Hernell O, Ohlund I (2010) Dietary short-comings in children on a gluten-free diet. J Hum Nutr Diet 23(3):294–300. https://doi.org/10.1111/j.1365-277X.2010.01060.x
91. Wild D, Robins GG, Burley VJ, Howdle PD (2010) Evidence ofhigh sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment Pharmacol Ther 32(4):573–581. https://doi.org/10.1111/j.1365-2036.2010.04386.x
92. Murray JA, Watson T, Clearman B, Mitros F (2004) Effect of agluten-free diet on gastrointestinal symptoms in celiac disease.Am J Clin Nutr 79(4):669–673
93. Innis SM (2008) Dietary omega 3 fatty acids and the developingbrain. Brain Res 1237:35–43
94. De Caterina R (2011) N-3 fatty acids in cardiovascular disease. NEngl J Med 364(25):2439–2450. https://doi.org/10.1056/NEJMra1008153
Clinic Rev Allerg Immunol

95. Aldamiz-Echevarria L, Bilbao A, Andrade F, Elorz J, Prieto JA,Rodriguez-Soriano J (2008) Fatty acid deficiency profile in chil-dren with food allergy managed with elimination diets. ActaPaediatr 97(11):1572–1576
96. Kim SH, Lee JH, Ly SY (2016) Children with atopic dermatitis inDaejeon, Korea: individualized nutrition intervention for diseaseseverity and nutritional status. Asia Pac J Clin Nutr 25(4):716–728. https://doi.org/10.6133/apjcn.092015.31
97. Paassilta M, Kuusela E, Korppi M, Lemponen R, Kaila M,Nikkari ST (2014) Food allergy in small children carries a riskof essential fatty acid deficiency, as detected by elevated serummead acid proportion of total fatty acids. Lipids Health Dis 13(1):180. https://doi.org/10.1186/1476-511X-13-180
98. Meyer R, DeKoker C, Dziubak R,Godwin H, Dominguez-OrtegaG, Chebar Lozinsky A, Skrapac AK, Gholmie Y, Reeve K, ShahN (2016) The impact of the elimination diet on growth and nutri-ent intake in children with food protein induced gastrointestinalallergies. Clin Transl Allergy. 6(1):25. https://doi.org/10.1186/s13601-016-0115-x
99. Pasiakos SM, Agarwal S, Lieberman HR, Fulgoni VL 3rd (2015)Sources and amounts of animal, dairy, and plant protein intake ofUS adults in 2007-2010. Nutrients 7(8):7058–7069
100. van Vliet S, Burd NA, van Loon LJ (2015) The skeletal muscleanabolic response to plant- versus animal-based protein consump-tion. J Nutr 145(9):1981–1991
101. Dietary protein quality evaluation in human nutrition (2013).Report of an FAQ Expert Consultation. FAO Food Nutr Pap 92:1–66
102. Saturni L, Ferretti G, Bacchetti T (2010) The gluten-free diet:safety and nutritional quality. Nutrients 2(1):16–34
103. Pellegrini N, Agostoni C (2015) Nutritional aspects of gluten-freeproducts. J Sci Food Agric 95(12):2380–2385. https://doi.org/10.1002/jsfa.7101
104. Martin J, Geisel T, Maresch C, Krieger K, Stein J (2013)Inadequate nutrient intake in patients with celiac disease: resultsfrom a German dietary survey. Digestion 87(4):240–246
105. Missbach B, Schwingshackl L, Billmann A, Mystek A,Hickelsberger M, Bauer G, König J (2015) Gluten-free food da-tabase: the nutritional quality and cost of packaged gluten-freefoods. PeerJ 3:e1337. https://doi.org/10.7717/peerj.1337
106. JH W, Neal B, Trevena H, Crino M, Stuart-Smith W, Faulkner-Hogg K et al (2015) Are gluten-free foods healthier than non-gluten-free foods? An evaluation of supermarket products inAustralia. Br J Nutr 114(3):448–454
107. Miranda J, Lasa A, Bustamante MA, Churruca I, Simon E (2014)Nutritional differences between a gluten-free diet and a diet con-taining equivalent products with gluten. Plant Foods Hum Nutr69(2):182–187. https://doi.org/10.1007/s11130-014-0410-4
108. Anderson JW, Baird P, Davis RH Jr, Ferreri S, Knudtson M,Koraym A et al (2009) Health benefits of dietary fiber. Nutr Rev67(4):188–205. https://doi.org/10.1111/j.1753-4887.2009.00189.x
109. Golden NH, Abrams SA (2014) Committee on N. Optimizingbone health in children and adolescents. Pediatrics 134(4):e1229–e1243. https://doi.org/10.1542/peds.2014-2173
110. Pludowski P, HolickMF, Pilz S,Wagner CL, Hollis BW,GrantWB,Shoenfeld Y, Lerchbaum E, Llewellyn DJ, Kienreich K, Soni M(2013) Vitamin D effects on musculoskeletal health, immunity, au-toimmunity, cardiovascular disease, cancer, fertility, pregnancy, de-mentia and mortality—a review of recent evidence. AutoimmunRev 12(10):976–989. https://doi.org/10.1016/j.autrev.2013.02.004
111. Prasad AS (2008) Zinc in human health: effect of zinc on immunecells. Mol Med 14(5–6):353–357. https://doi.org/10.2119/2008-00033.Prasad
112. Prado EL, Dewey KG (2014) Nutrition and brain development inearly life. Nutr Rev 72(4):267–284. https://doi.org/10.1111/nure.12102
113. Kim J, Kwon J, Noh G, Lee SS (2013) The effects of eliminationdiet on nutritional status in subjects with atopic dermatitis. NutrRes Pract 7(6):488–494. https://doi.org/10.4162/nrp.2013.7.6.488
114. Meyer R, DeKoker C, DziubakR, Skrapac AK,GodwinH, ReeveK, Chebar-Lozinsky A, Shah N (2015) A practical approach tovitamin and mineral supplementation in food allergic children.Clin Transl Allergy 5(1):11. https://doi.org/10.1186/s13601-015-0054-y
115. Meyer R, De Koker C, Dziubak R, Godwin H, Dominguez-OrtegaG, Shah N (2014) Dietary elimination of children with food pro-tein induced gastrointestinal allergy—micronutrient adequacywith and without a hypoallergenic formula? Clin Transl Allergy4(1):31
116. Moore CE, Radcliffe JD, Liu Y, Vitamin D (2014) Intakes ofchildren differ by race/ethnicity, sex, age, and income in theUnited States, 2007 to 2010. Nutr Res 34(6):499–506. https://doi.org/10.1016/j.nutres.2014.06.002
117. Bailey RL, Dodd KW, Goldman JA, Gahche JJ, Dwyer JT,Moshfegh AJ, Sempos CT, Picciano MF (2010) Estimation oftotal usual calcium and vitamin D intakes in the United States. JNutr 140(4):817–822. https://doi.org/10.3945/jn.109.118539
118. Molina-Infante J, Katzka DA, Gisbert JP (2013) Review article:proton pump inhibitor therapy for suspected eosinophilicoesophagitis. Aliment Pharmacol Ther 37(12):1157–1164
119. Jung SB, Nagaraja V, Kapur A, Eslick GD (2015) Associationbetween vitamin B12 deficiency and long-term use of acid-lowering agents: a systematic review and meta-analysis. InternMed J 45(4):409–416
120. Freedberg DE, Kim LS, Yang YX (2017) The risks and benefits oflong-term use of proton pump inhibitors: expert review and bestpractice advice from the American GastroenterologicalAssociation. Gastroenterology 152(4):706–715. https://doi.org/10.1053/j.gastro.2017.01.031
121. do Nascimento AB, Fiates GM, Dos Anjos A, Teixeira E (2013)Analysis of ingredient lists of commercially available gluten-freeand gluten-containing food products using the text mining tech-nique. Int J Food Sci Nutr 64(2):217–222. https://doi.org/10.3109/09637486.2012.718744
122. deCastro BR, Caldwell KL, Jones RL, Blount BC, Pan Y,Ward C,Mortensen ME (2014) Dietary sources of methylated arsenic spe-cies in urine of the United States population, NHANES 2003-2010. PLoS One 9(9):e108098. https://doi.org/10.1371/journal.pone.0108098
123. Bulka CM, Davis MA, Karagas MR, Ahsan H, Argos M (2017)The unintended consequences of a gluten-free diet. Epidemiology28(3):e24–ee5. https://doi.org/10.1097/EDE.0000000000000640
124. Raehsler SL, Choung RS, Marietta EV, Murray JA (2017)Accumulation of heavy metals in people on a gluten-free diet.Clin Gastroenterol Hepatol. https://doi.org/10.1016/j.cgh.2017.01.034
125. Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ (2012)Heavy metal toxicity and the environment. EXS 101:133–164.https://doi.org/10.1007/978-3-7643-8340-4_6
126. De Geest S, Sabate E (2003) Adherence to long-term therapies:evidence for action. Eur J Cardiovasc Nurs 2(4):323. https://doi.org/10.1016/S1474-5151(03)00091-4
127. Hommel KA, Franciosi JP, Hente EA, Ahrens A, Rothenberg ME(2012) Treatment adherence in pediatric eosinophilic gastrointes-tinal disorders. J Pediatr Psychol 37(5):533–542
128. Franciosi JP, Hommel KA, Greenberg AB, DeBrosse CW, GreenlerAJ, Abonia JP, Rothenberg ME, Varni JW (2012) Development ofthe pediatric quality of life inventory eosinophilic esophagitis mod-ule items: qualitative methods. BMC Gastroenterol 12(1):135.https://doi.org/10.1186/1471-230X-12-135
129. Leffler DA, Edwards-George J, Dennis M, Schuppan D, Cook F,Franko DL et al (2008) Factors that influence adherence to a
Clinic Rev Allerg Immunol

gluten-free diet in adults with celiac disease. Dig Dis Sci 53(6):1573–1581
130. MacCulloch K, Rashid M (2014) Factors affecting adherence to agluten-free diet in children with celiac disease. Paediatr ChildHealth 19(6):305–309. https://doi.org/10.1093/pch/19.6.305
131. Singh J, Whelan K (2011) Limited availability and higher cost ofgluten-free foods. J HumNutr Diet 24(5):479–486. https://doi.org/10.1111/j.1365-277X.2011.01160.x
132. McMahon EJ, Campbell KL, Mudge DW, Bauer JD (2012)Achieving salt restriction in chronic kidney disease. Int JNephrol 2012:720429
133. Whitaker JK, West J, Holmes GK, Logan RF (2009) Patient per-ceptions of the burden of coeliac disease and its treatment in theUK. Aliment Pharmacol Ther 29(10):1131–1136. https://doi.org/10.1111/j.1365-2036.2009.03983.x
134. Schulman-Green D, Jaser SS, Park C, Whittemore R (2016) Ametasynthesis of factors affecting self-management of chronic ill-ness. J Adv Nurs 72(7):1469–1489
135. Wang R, Hirano I, Doerfler B, Zalewski A, Gonsalves N, Taft T(2017) Assessing adherence and barriers to long term dietary elim-ination therapy in patients with eosinophilic esophagitis (EOE).Gastroenterology 152(5):S864
136. AsherWolf W, Huang KZ, Durban R, Iqbal ZJ, Robey BS, KhalidFJ et al (2016) The six-food elimination diet for eosinophilic
esophagitis increases grocery shopping cost and complexity.Dysphagia 31(6):765–770
137. Roma E, Roubani A, Kolia E, Panayiotou J, ZellosA, SyriopoulouVP (2010) Dietary compliance and life style of children with coe-liac disease. J Hum Nutr Diet 23(2):176–182. https://doi.org/10.1111/j.1365-277X.2009.01036.x
138. Giovannini M, D'Auria E, Caffarelli C, Verduci E, Barberi S,Indinnimeo L, Iacono I, Martelli A, Riva E, Bernardini R (2014)Nutritional management and follow up of infants and childrenwith food allergy: Italian Society of Pediatric Nutrition/ItalianSociety of Pediatric Allergy and Immunology Task ForcePosition Statement. Ital J Pediatr 40(1):1. https://doi.org/10.1186/1824-7288-40-1
139. Harris RF, Menard-Katcher C, Atkins D, Furuta GT, Klinnert MD(2013) Psychosocial dysfunction in children and adolescents witheosinophilic esophagitis. J Pediatr Gastroenterol Nutr 57(4):500–505. https://doi.org/10.1097/MPG.0b013e31829ce5ad
140. Webb D, Byrd-Bredbenner C (2015) Overcoming consumer iner-tia to dietary guidance. Adv Nutr 6(4):391–396
141. Henry ML, Atkins D, Fleischer D, Pan Z, Ruybal J, Furuta GT(2012) Factors contributing to adherence to dietary treatment ofeosinophilic gastrointestinal diseases. J Pediatr Gastroenterol Nutr54(3):430–432. https://doi.org/10.1097/MPG.0b013e3182407aee
Clinic Rev Allerg Immunol