health cooperation in post-conflict setting
TRANSCRIPT

Health cooperation in post-conflict setting
July 16, 2013Hideaki NAKAJIMA
254th IDEC Asia Seminar
254th IDEC Asia Seminar
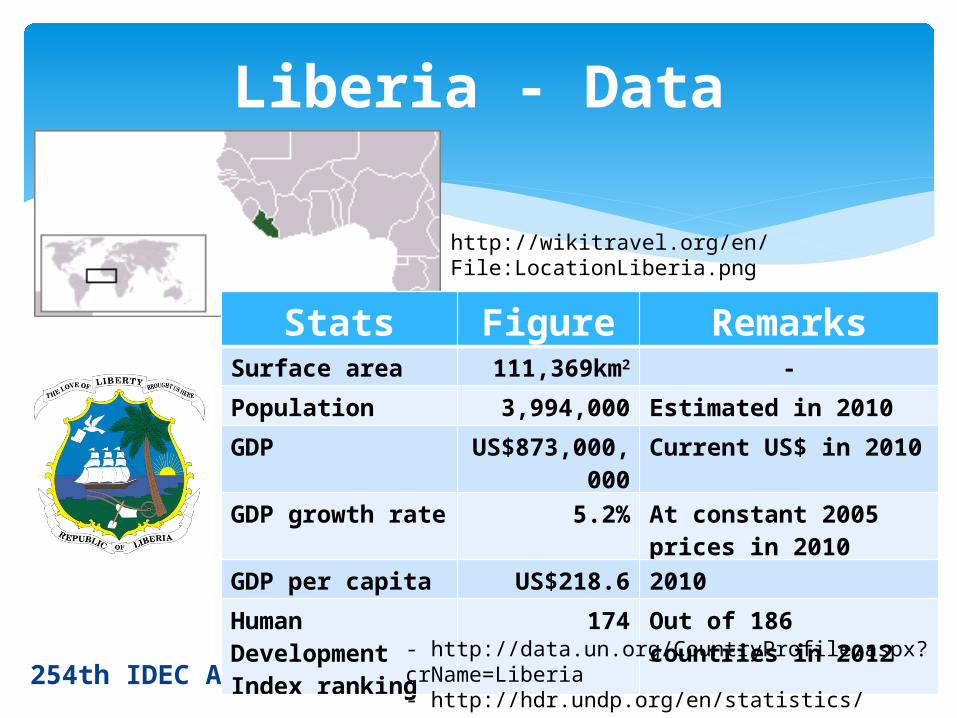
Liberia - Data
http://wikitravel.org/en/File:LocationLiberia.png
Stats Figure RemarksSurface area 111,369km2 -
Population 3,994,000 Estimated in 2010
GDP US$873,000,000
Current US$ in 2010
GDP growth rate
5.2% At constant 2005 prices in 2010
GDP per capita US$218.6 2010
Human Development Index ranking
174 Out of 186 countries in 2012- http://data.un.org/CountryProfile.aspx?
crName=Liberia- http://hdr.undp.org/en/statistics/
1822: Freed American slave settlers arrived 1847: Independence (first republic in Africa)→ Only “Americo-Liberians” had civil rights and politically and economically ruled Liberia 1980: Coup d’etat by Samuel Doe (indigenous
origin) 1989: Rebel by Charles Taylor→ Civil conflict 2003: Accra Peace Accord 2006: Inauguration of first democratically elected female president in Africa (Ellen Johnson- Sirleaf)
254th IDEC Asia Seminar
Liberia - History
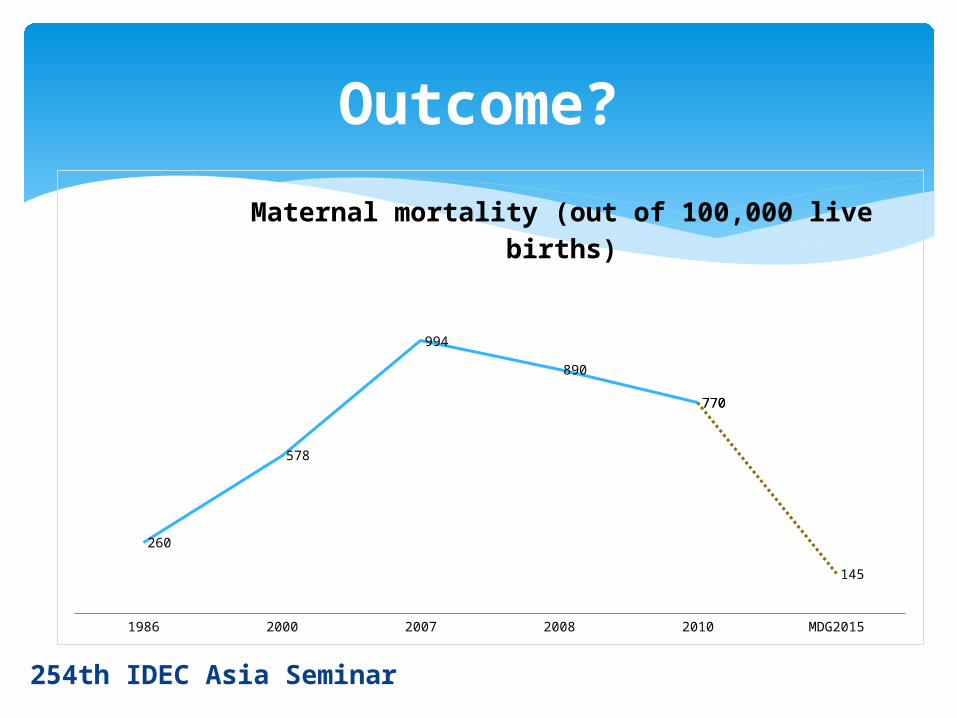
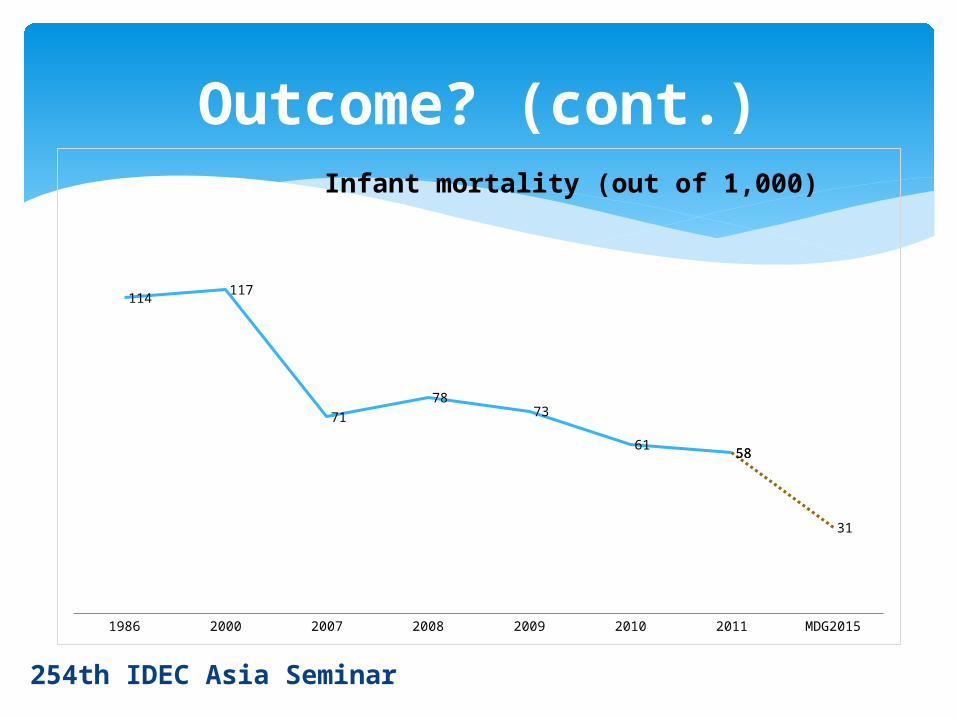
No. of health facilities: 550 before conflict → 354High maternal mortality rate: 770/100,000 (2010) (7th highest in world) (*Japan: 6/100,000)Infant & under 5 mortality rates are also still high: 58/1,000 (2011) (*Japan: 2/1,000) & 78/1,000 (2011) (*Japan: 3/1,000)Infectious disease (malaria) prevalentNeglected tropical disease (NTD: lymphatic
filariasis, etc.)Non-communicable diseases (diabetes,
cardiovascular disease, etc.)Basic care such as eyes, nose & throat (ENT) is
also still to be improved
254th IDEC Asia Seminar
Situation in health in Liberia
BPHS:Introduced into post-conflict setting (e.g.
Afghanistan other than Liberia)Comprehensive health service package to
“effectively deliver quality health services to the people” (Liberia National Health Policy 2007-2011)
DecentralizationPerformance-based contract with NGOs &
local authority (even aiming at contract with health facilities)254th IDEC Asia Seminar
Basic Package of Health Services (BPHS)

<2007 - 2011>
Maternal & newborn careReproductive & adolescent healthChild healthCommunicable disease controlMental healthEmergency care services
254th IDEC Asia Seminar
BPHS (cont.)
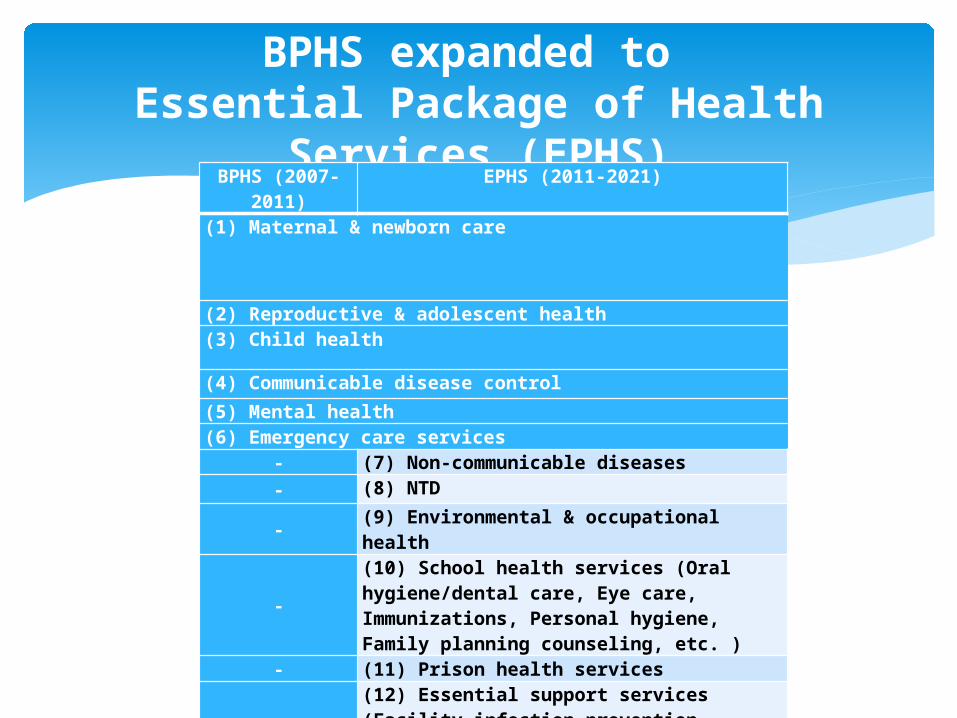
BPHS expanded to Essential Package of Health
Services (EPHS)BPHS (2007-
2011)EPHS (2011-2021)
(1) Maternal & newborn care
(2) Reproductive & adolescent health(3) Child health
(4) Communicable disease control
(5) Mental health(6) Emergency care services
- (7) Non-communicable diseases- (8) NTD
-(9) Environmental & occupational health
-
(10) School health services (Oral hygiene/dental care, Eye care, Immunizations, Personal hygiene, Family planning counseling, etc. )
- (11) Prison health services
-
(12) Essential support services (Facility infection prevention, control & health waste management, pharmaceutical services, Health management information systems, Laboratory services, Health promotion/IEC/BCC)
254th IDEC Asia Seminar
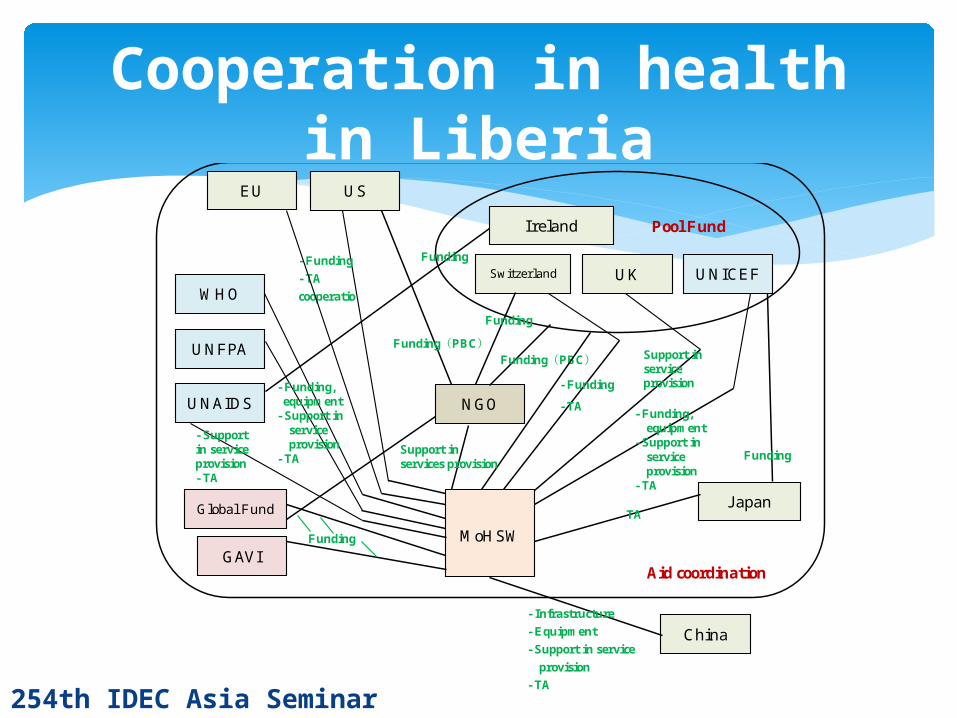
Cooperation in health in Liberia
MoHSW
NGO
GAVI
Global Fund J apan
China
Ireland
Switzerland UK
EU US
WHO UNICEF
UNAIDS
UNFPA
Pool Fund
Aid coordination
Funding(PBC)
Support in services provision
TA
Funding(PBC)
- Funding
- TA
cooperatio
Support in service provision - Funding
- TA
Funding
- Funding, equipment
- Support in service provision
- TA
Funding
Funding
- Funding, equipment
- Support in service provision
- TA
- Support in service provision - TA
Funding
- Infrastructure
- Equipment
- Support in service
provision
- TA
254th IDEC Asia Seminar
Outcome?
1986 2000 2007 2008 2010 MDG2015
260
578
994
890
770770
145
Maternal mortality (out of 100,000 live births)
254th IDEC Asia Seminar
Outcome? (cont.)
1986 2000 2007 2008 2009 2010 2011 MDG2015
114117
71
7873
615858
31
Infant mortality (out of 1,000)
254th IDEC Asia Seminar
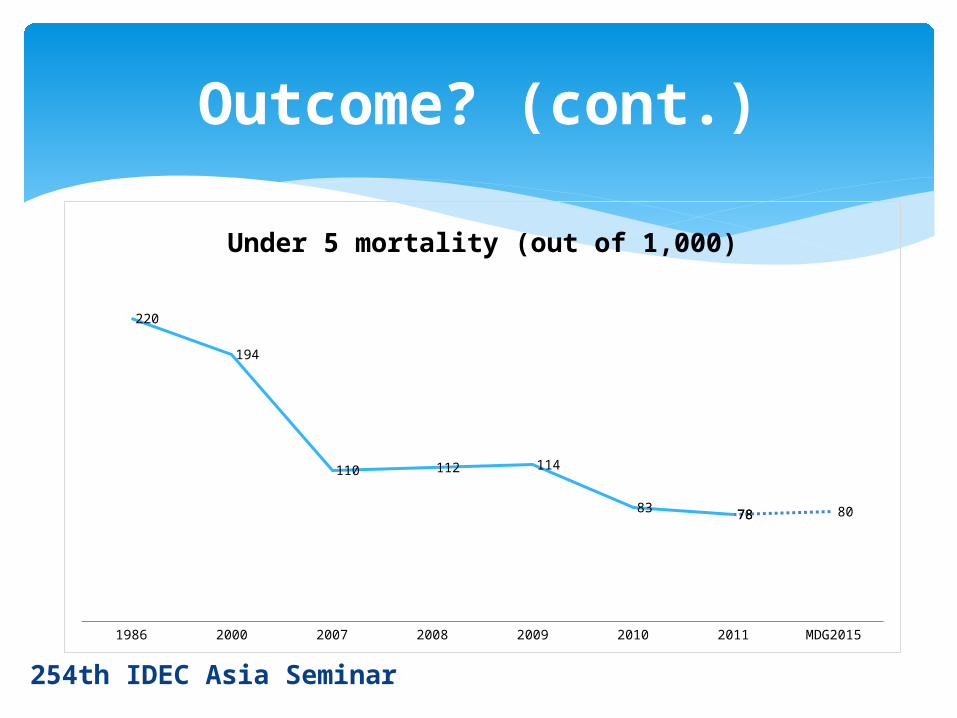
Outcome? (cont.)
1986 2000 2007 2008 2009 2010 2011 MDG2015
220
194
110 112 114
83 7878 80
Under 5 mortality (out of 1,000)
254th IDEC Asia Seminar
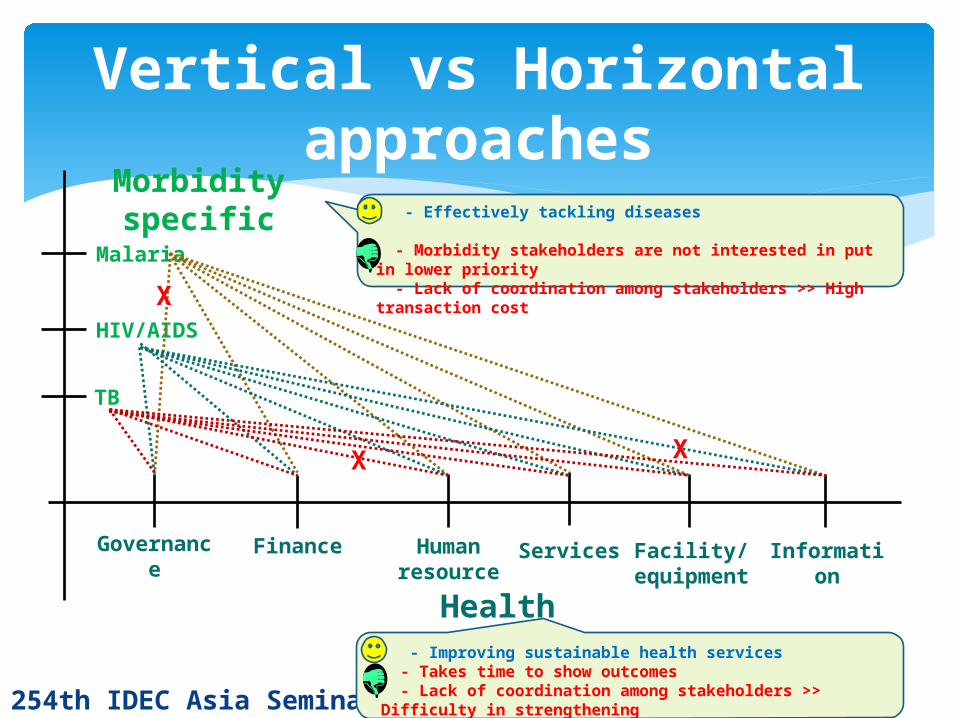
Vertical vs Horizontal approaches
Health systems
Governance
Finance Human resource
Services Facility/equipme
nt
Information
Malaria
Morbidity specific
HIV/AIDS
TB
- Effectively tackling diseases
- Morbidity stakeholders are not interested in put in lower priority - Lack of coordination among stakeholders >> High transaction cost
- Improving sustainable health services - Takes time to show outcomes - Lack of coordination among stakeholders >> Difficulty in strengthening all components in balance
X
XX

Policies/strategies made in the course of state reconstruction (sometimes in donors’ interest?)
Essential, BUT… Gap between what is written and what
is actually implemented
254th IDEC Asia Seminar
Liberal peacebuilding/development?
Midwives & nurses always scold me at clinic. Drugs are sometimes out of stock and so I have to buy ones myself. And, clinic is far! I don’t want to go to clinic…
So many people come and I’m busy and tired… No pay increase, and payment sometimes delays! I want to get new skills, to be respected. I don’t want to stay in rural area…!
Decentralization?Wait a minute…
Weak enforcement of systems, weak governance, lack of authority…
- Government and donors/NGOs are working on strengthening gov’t governance…
- But no good coordination among them…
254th IDEC Asia Seminar
Liberal peacekeeping/development? (cont.)

HumanitarianismHuman securityEquity/justiceNational interestsGlobal public goods
254th IDEC Asia Seminar
Why aid?
?
?
Public goods: Non-excludable & non-rivalrous in consumption (e.g. lighthouse, peace & security, law & order)
In this rapidly globalizing world, health GPGis…
- Health R&D- Communicable disease control(Smith R.D. & MacKellar L. (2007))254th IDEC Asia Seminar
Global public goods (GPG)

WHO’s recent report:“Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence”
254th IDEC Asia Seminar
GPG (cont.)
<Sexually transmitted infections (STIs)>
Women who experience physical/sexual partner violence are 1.5 times more likely to acquire STIs including HIV.

The politically/economically/socially disadvantaged (women) are physically (and mentally) abused and suffer from morbidity… Society, whose structure keeps the vulnerable (women as well as children) as they are, is itself vulnerable in that it is prone to conflict, isn’t it? And there is no peace, if those people are still vulnerable, in post-conflict situation.
254th IDEC Asia Seminar
GPG (cont.)

254th IDEC Asia Seminar
How health cooperation works in post-conflict setting?
1. Evoking and extending altruism generates positive feelings among parties
2. Identifying and replacing rumors with facts rebuilds mutual confidence
3. Redefining the prevalent norms changes the terms of the debate and opens new space for discussion
4. Regenerating a sense of shared identity5. Personal solidarity actions by healthcare
professionals, especially respected doctors, can have a demonstrably powerful effect(Mukesh Kapila, Healing Broken Societies: Can Aid Buy Love
and Peace?)

Capacity development Synergy between the dual approaches: top-down
(system/rule making/strengthening) & bottom-up Stakeholder coordination/collaboration Rights approach (e.g. right to health; universal health
coverage) Cross-cutting approaches (e.g. education & health;
economic development that gives people hope for future, which does not indulge people in desperate health damaging abuse)
AND… Respect for people: think & try hard to help people get
motivated, esteemed and rewarded as we wanted if we were them!
254th IDEC Asia Seminar
How health cooperation works in post-conflict setting? (cont.)
Takes time to achieve goals (sometimes three steps forward & two steps back…), but we can do it!

254th IDEC Asia Seminar
Thank you!!