digestive pathology lecture 5 - school of medicine...digestive pathology lecture 5 reproduction...
TRANSCRIPT

Digestive Pathology Lecture 5
Reproduction Prohibited
This file contains original text and images as well as materials adapted from copyrighted sources
For use only as a temporary educational aid
Partially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception
for teaching faculty of the U.S. Copyright Law
LSUHSC-New Orleans, 2015
Last updated September 29, 2015
---

The liver II
7. Infectious hepatitis
– Bacterial
– Fungal
– Parasitic
– Liver abscess
– Viral8. Non-infectious hepatitis

Bacterial
Hepatitis
– Systemic infections and sepsis
– Some infections are particularly prone to involve the liver (typhoid and paratyphoid)
Pyogenic abscess
Granulomas and granuloma-like lesions
– Tuberculosis, leprosy, syphilis
Peliosis hepatis
– Focal sinusoidal rupture, blood filled cystic spaces
– Bartonella infections (bacillary peliosis), in children, HIV-infected, other immunosuppressed individuals

Peliosis hepatis
Scheuer’s Liver Biopsy Interpretation

Fungal
Mostly in immunocompromised patients
– Candida (the most common)

Parasitic
Malaria
Trematodes– Opisthorchiasis
– Clonorchiasis
– Fascioliasis
– other
Echinococcosis– Cystic (hydatid cyst, Echinococcus granularis)
– Alveolar (Echinococcus multilocularis)
Amebiasis

Liver flukes1. Opisthorchis viverrini
2. Clonorchis sinensis
3. Fasciola hepaticaAC=acetabulum (ventral sucker), CE=cecum, CL=collar, CS=cirrus sac, EB=excretory bladder, EG=eggs (within uterus), ES=esophagus, IN=intestine, OS=oral sucker, OV=ovary, PH=pharynx, SR=seminal receptacle, TE=testes, UT=uterus, VT=vitellaria

Fasciola hepatica
Adult liver flukes, released on incision of the main bile duct in an infected sheep’s liver during a post-mortem examination, www.afbini.gov.uk

Echinococcus granulosusHydatid cyst with daughter cysts

Echinococcus multilocularisAlveolar echinococcosis
www.parasite-diagnosis.ch

Abscesses, etiology
Pyogenic (enterobacteriaceae)
Fungal (C. albicans)
Parasitic (amebic)
Mixed

Liver abscess, routes
Biliary tract (ascending cholangitis), the most common
Hepatic artery (sepsis)
Portal vein (pylephlebitis)
Direct extension (neighboring tissues)
Penetrating injuries

Liver abscess, multiplicity
Solitary abscess: direct extension, penetrating injury
Multiple, small abscesses: biliary, arterial, portal

Pyogenic abscesses, ascending cholangitis

Amebic abscess
Anchovy paste-like necrotic contents with nuclear debris and few inflammatory cells; organisms present at the advancing edge. Odze, Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas

Amebic Liver AbscessPortal route, solitary
CT scan demonstrating a large abscess in the right hepatic lobe. Wells, Christopher D.; Arguedas, Miguel. Southern Medical Journal. 97(7):673-682, July 2004

Liver abscess, complications
Rupture into the abdominal cavity: peritonitis, peritoneal abscesses
Rupture into the thoracic cavity: empyema, lung abscesses
Rupture into the pericardial cavity
High mortality
Viral hepatitis
Systemic infections (secondary /non-hepatotropic)
– Yellow fever, in tropical regions
– Mononucleosis (Epstein-Barr Virus)
– In children and immunosuppressed:
• Cytomegalovirus
• Herpesvirus
• Adenovirus
• Other
Primary /hepatotropic viruses

Hepatotropic viruses
Hepatitis A, B, C, D, E
Enveloped and un-enveloped

Enveloped viruses (B, C and D)
Wrap themselves with a lipid bilayer that they adopt from infected cells

Enveloped viruses (B, C and D)
Sensitive to desiccation, detergents
Susceptible to emulsification by bile acids
Do not survive in feces
Not specialized in fecal-oral transmission
Transmission by contact with body fluids– Percutaneous
– Mucosal, sexual
– Vertical (mother to fetus, perinatal)
Long incubations, persistent viremia

Enveloped viruses (B, C, D)
Cause carrier state– Persistent infection with no signs or
symptoms of disease
Cause chronic hepatitis– Evidence of disease > 6 months
Linked to cirrhosis, hepatocellular carcinoma
Immune complex deposition– Arthralgias, vasculitis, glomerulonephritis

Unenveloped viruses (A and E)
Not wrapped in lipid bilayer
Survive exposure to bile
Specialized in fecal-oral transmission
Short incubation periods
Short-lasting viremia
Rare bloodborne transmission
No chronic hepatitis, no carrier state in immunocompetent individuals
Not linked to hepatocellular carcinoma

Hepatitis A Single stranded RNA
Incubation 2-6 weeks
Prodromal (pre-icteric) state
Icteric state
May be anicteric
May be subclinical, particularly in young children
May be fulminant
Shed in feces 2-3 w before to 1 w after jaundice
Shellfish concentrate the virus
Contaminated agricultural products cause outbreaks

Hepatitis A Sexual transmission may occur
Bloodborne transmission may occur
May follow a prolonged course
May relapse
Rare reports of chronic hepatitis

Hepatitis A
Diagnosis:
– Acute hepatitis:
• IgM anti-HAV, blood
• HAV RNA, feces
– Previous exposure: IgG (total) anti-HAV, protective immunity
Vaccine available since 1995

Hepatitis A incidenceVaccine licensed in 1995

Hepatitis A incidence
Rate per 100,000 population by county before and after widespread use of vaccination. National Notifiable Disease Surveillance System

Hepatitis E
Single-stranded RNA
Incubation 2-9 weeks
Enzootic/zoonotic (cows, pigs, sheep, goats, rodents, deer, wild boars…)
In developing countries:– Genotypes 1 and 2
– Mostly young and middle age adults
– May be subclinical in children
– Pregnant women, third trimester, mortality 20-30%

Geographic distribution of hepatitis E

Chronic hepatitis E
Chronic infection that may progress to cirrhosis has been reported in:
– Immunosuppressed patients (particularly organ transplant recipients)
– HIV-infected individuals

Hepatitis E
Diagnosis:
– Acute hepatitis
• IgM anti-HEV, blood
• HEV RNA, feces
– Previous exposure: IgG anti-HEV, loss of antibodies over time, re-infections may occur
Vaccine is available since 2012 (China)

Hepatitis E indigenous to developed countries
Genotypes 3 and 4
Among healthy individuals seroprevalence 5-20%
Clinical disease in middle age and older individuals
Severity increases with age
Pet ownership or occupational exposure to pigs
Uncooked, undercooked meat or viscera: pigs, deer, boars

New Microbiologica, 36, 331-344, 2013
Hepatitis E, genotypes

Tatsuo Miyamura. Hepatitis E virus infection in developed countries. Virus Research Volume 161, Issue 1 2011 40 – 46. http://dx.doi.org/10.1016/j.virusres.2011.03.006
Food source of infection of domestic hepatitis E cases, Japan, 2009

Hepatitis B
Double stranded DNA virus
Incubation 4-26 weeks
Acute illness may be subclinical or have symptoms similar to hepatitis A– Jaundice occurs less often
May be fulminant
May resolve completely
May become chronic:– Asymptomatic (carrier state)
– Symptomatic

Hepatitis B outcome
Hepatitis B, risk factors
Sex with an infected partner, sexual promiscuity
Injection drug use sharing needles, syringes
Birth to an infected mother
Contact with blood or fluids of an infected person
Needle sticks or sharp instrument exposures
Sharing razors or toothbrushes
Tattooing, body piercing
Inmates, institutional overcrowding

Hepatitis B, risk of chronicity Newborn (vertical transmission), 90% < 1, 70-90% 2-3, 40-70% 4-6, 10-40% >7, 6-10% Immunocompetent adult, <5% Immunocompromised adult, >50% Dominant cause of viral persistence:
– Weak immune response– Tolerance

Recombinant vaccine

HBV virion (Dane particle)
– Surface antigen, envelope, HBsAg
– “Core" antigen, nucleocapsid, HBcAg
– Non-structural "e" antigen, HBeAg
– HBx protein (replication, trans-activate host genes)
– DNA polymerase
– HVB DNA

Hepatitis B, surface antigen
Hepatitis Web StudyUniversity of Washington

Hepatitis B, phases
Proliferative (episomal)
– Formation of complete virions
Integrated
– Virus integrated into the host’s DNA
– Cessation of viral replication
– Continuous production of HBsAg

Hepatitis B, pathogenesis
Expression of HBsAg and HBcAg on hepatocytes activates cytotoxic T lymphocytes, responsible for the cell damage
Immunosuppressed individuals suffer less cell damage but are more likely to develop chronicity
Chronic cell injury, inflammatory and regenerative responses promote carcinogenesis

Hepatitis B, diagnosis Acute infection
– HBsAg
– IgM anti-HBcAg
Active viral replication, infectivity– HBeAg
– HBV DNA
Chronic infection:– > 6 months: HBsAg
– IgM anti-HBcAg has been replaced by IgG anti-HBcAg
Hepatitis B, prior infection, vaccine
Resolution, prior infection
– HBsAg, HBV DNA and HBeAg disappear
– IgG Anti-HBsAg appear and persist
Vaccination effect:
– Anti-HBsAg present without anti-HBcAg
– Vaccine is made of recombinant HBsAg

Hepatitis D (Delta agent)
Very small, single-stranded RNA virus
Replication defective, requires HBsAg
Coinfection– Fulminant disease more likely
– Chronicity <5%
Superinfection of HBV carrier– Fulminant hepatitis less likely
– Chronicity: 80%
In the US mostly restricted to– Drug addicts
– Hemophiliacs
– Their sexual contacts
Prophylaxis: vaccination for HBV, no vaccine for HDV

Wedemeyer, H. & Manns, M. P. (2010) Epidemiology, pathogenesis and management of hepatitis D: update and
challenges ahead. Nat. Rev. Gastroenterol. Hepatol. doi:10.1038/nrgastro.2009.205
Prevalence of HDV infection, viral genotype

Hepatitis D, diagnosis IgM anti-HDV
Coinfection with HBV:
– IgM anti-HDV with HBsAg and IgM anti-HBcAg
Superinfection
– IgM anti-HDV, with HBsAg, without IgM anti-HBcAg
HDV RNA
Immunohistochemistry

Hepatitis C
Single-stranded RNA virus
Classified into six major genotypes
Genotypes 1a and 1b cause 70% of all infections in the US

Hepatitis C, evolutionary treeAmerican Association for the study of liver diseases, 2005

Hepatitis C
Incubation 2 to 26 weeks
Acute infection commonly subclinical
No fulminant presentation
High rate of chronicity, 55-85%
High rate of progression to cirrhosis
High rate of progression to HCC

Natural history of HCV infection
100 People
Resolve (15)
15%
Chronic (85)
85%
Cirrhosis (17)Stable (68)
80%
75%
Stable (13)
Mortality (4)
25%
20%

Hepatitis C, risk factors
Reported risk factors in the US:
– Intravenous drug abuse, 60%
• Highly efficient mode of transmission
– Sexual, < 20%
• Rare between long-term sex partners (1.5-3%)
– Perinatal transmission is low
– Health care workers
• Risk after needle stick accident: (1.8-10%)
– No recognized source of infection 10%

Hepatitis C
HCV genome is unstable• Emergence of mutated strains (quasispecies)
cause recurrences
• Variability hampers development of vaccine
• IgG anti-HCV does not confer protection
• Rapid variation may cause resistance to therapy
– New antiviral therapies promise cure rates >90%
Hepatitis C
Diagnosis:– Antibodies anti-HCV
• Enzyme immunoassay (EIA)
• Recombinant immunoblot assay (RIBA)
• Only total antibodies are measured, IgM anti-HCV is not used (does not indicate acute infection)
• Detectable 7 weeks after exposure, remain positive for life
• Indicate exposure to the virus not current infection

Hepatitis C
Diagnosis:– HCV RNA
• Qualitative
• Quantitative
• Detectable 2 weeks after exposure
Hepatitis G
GB virus type C (GBV-C)
RNA virus, flavivirus, same family as hepatitis C, yellow fever and West Nile viruses
Parenteral, sexual, vertical transmission
Transmission by transfusion documented
Lymphotropic, no hepatotropic
Pathogenic capacity questioned
Coinfection with HIV and GBV-C associated with a BETTER outcome for the HIV infection
Acute hepatitis, morphology Centered in the lobules (lobular, lobulocentric)
– More severe in zone 3 than in portal/periportal areas
Inflammation
– May be mostly lymphocytic
Hepatocyte injury
– Ballooning
– Apoptosis
– Necrosis (focal, bridging, submassive or massive)
Hepatocyte regeneration
– Variation in size
– Disarray of liver plates

Acute viral hepatitis
Hepatocytes in the perivenular area in the center of the field are swollen and the area is infiltrated by inflammatory cells. Scheuer’s Liver Biopsy Interpretation.

Chronic hepatitis, histology
Centered in the portal/periportal area
Grade, determined by the extent of:
– Portal/periportal inflammation
– Hepatocyte injury (ballooning, apoptosis, necrosis)
Stage, determined by the extent of fibrosis
– Portal
– Periportal
– Bridging
– Cirrhosis

Chronic hepatitis, grading (interface hepatitis)

Chronic hepatitis, grading (lytic necrosis)

Chronic hepatitis, staging (fibrosis)

HBV, ground-glass hepatocytes

HBV, surface antigen, immunoperoxidase

HVB, sanded nuclei

HBV, core antigen, immunoperoxidase

The liver II7. Infectious hepatitis
Non-infectious hepatitis
8. Autoimmune hepatitis
9. Drug induced
10. Alcoholic and non-alcoholic steatohepatitis
11. Inborn errors of metabolism
• Wilson disease
• Alpha1-antitrypsin deficiency
• Primary biliary cirrhosis

8. Autoimmune hepatitis T-cell mediated injury
Genetic predisposition
May be triggered by viral infections, drugs
Female predominance, >70%
Concurrent autoimmune diseases
Morphologically similar to viral hepatitis– Prominent plasma cell infiltrate
– Tends to be the more severe• Acute presentation is common, may be fulminant
• May progress rapidly to cirrhosis
Responds to immunosuppressive therapy

Autoimmune hepatitisProminent plasma cell infiltration, severe

Autoimmune hepatitis
Elevated serum gamma-globulin
Autoantibodies:
– Type 1, most common
• Anti-nuclear (ANA)
• Anti-smooth muscle (ASMA)
– Type 2, rare, mostly children
• Anti-liver/kidney microsome 1 (LKM1)
• Anti-liver cytosol-1 (ALC1)
Biopsy

9. Drug and toxic liver injury
Direct toxicity
Indirect toxicity, hepatic conversion
Immune injury, usually as a hapten– Small molecule elicits immune response
when attached to a large carrier

Predictable and unpredictable injury
Predictable (intrinsic)– Occur in anyone, at sufficient dose
(acetaminophen)
Unpredictable (idiosyncratic)– Immune response (halothane)
– Slow metabolism (isoniazid)

Macrovesicular steatosis, methotrexate
Ethanol, amiodarone

Microvesicular steatosis, tetracycline
Salicylates (Reye syndrome)
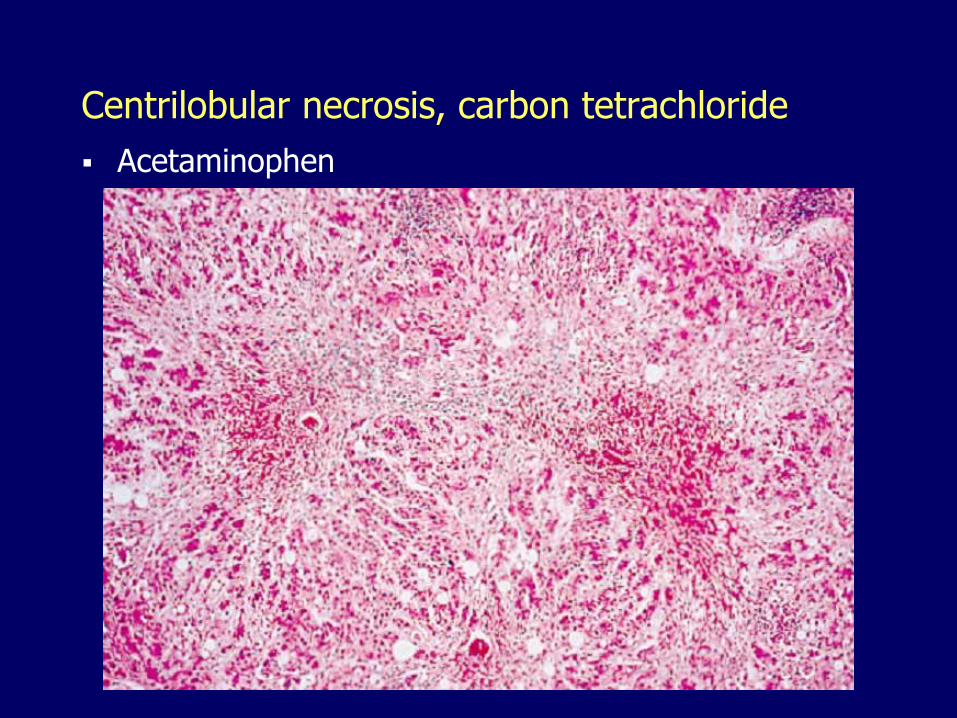
Centrilobular necrosis, carbon tetrachloride
Acetaminophen

Massive necrosis, isoniazid
Acetaminophen, halothane, Amanita phalloides

Chronic hepatitis, nitrofurantoin
Methyldopa, isoniazid, phenytoin, oxyphenisatin

Granulomatous hepatitis, phenylbutazone
Sulfonamides, hydralazine, allopurinol, quinidine

Cholestasis, erythromycin estolate
Chlorpromazine, anabolic steroids, contraceptives

Acetaminophen
Metabolism
– Small amount metabolized by cytochrome P-450 to form toxic oxidative metabolites (particularly N-acetyl-p-benzoquinone imine NAPQI)
– Toxic metabolites are inactivated by glutathione

Acetaminophen toxicity, treatment
Inactivation of toxic metabolites overwhelmed by overdose
Alcohol potentiation
– Induces cytochrome P-450
– Depletes glutathione
Treatment:
– N-acetyl cysteine, restores glutathione

Reye syndrome
Children given aspirin for virus-induced fever (respiratory infections, varicella)
Defect in mitochondrial fatty acid oxidation
Fatty acids accumulate in the SER– Extensive microvesicular steatosis
Liver failure
Hepatic encephalopathy
Potentially fatal

Reye syndrome

10. Steatohepatitis
Alcoholic
Non-alcoholic

Alcoholic liver disease
Leading cause of liver disease
Fifth leading cause of death
25-30% of hospitalized patients
Spectrum of injury:
– Steatosis
– Steatohepatitis
– Established cirrhosis

Alcoholic steatohepatitis, individual susceptibility
Men, significant toxicity at >80 gm/day
Increased susceptibility:– Women
– Asians (slow aldehyde dehydrogenase)
– African Americans
Concomitant iron overload, HBV or HCV infections and other comorbid conditions
Only 10% of alcoholics develop cirrhosis

Ethanol, metabolism
Ethanol
Acetaldehyde
Acetate
NAD
NADH + H
NAD
NADH + H
Alcohol dehydrogenase
Aldehyde dehydrogenase

Alcoholic steatohepatitis, etiology
Induction of cytochrome P-450 (increase in toxic metabolites)
Depletion of glutathione
Generation of free radicals
Acetaldehyde causes lipid peroxidation and protein adduct formation
Release of bacterial endotoxin from the gut
Malnutrition– Alcohol constitutes the major calorie source
– Impaired digestive function
– Pancreatitis

Alcoholic steatohepatitis, etiology
Steatosis
– Shunt metabolism toward lipid biosynthesis
• Alcohol dehydrogenase, aldehyde dehydrogenase generate excess NADH
– Increased peripheral catabolism of fat
– Impaired assembly and secretion of lipoproteins

Alcoholic steatohepatitis
Steatosis, centrilobular
Cell injury
– Ballooning
– Mallory bodies
– Necrosis, apoptosis
Inflammation
Fibrosis, initially centrilobular
Cirrhosis (Laennec)

Alcohol, ballooning, Mallory bodies

Mallory body, satellitosis

Alcohol, perivenular fibrosis, steatosis
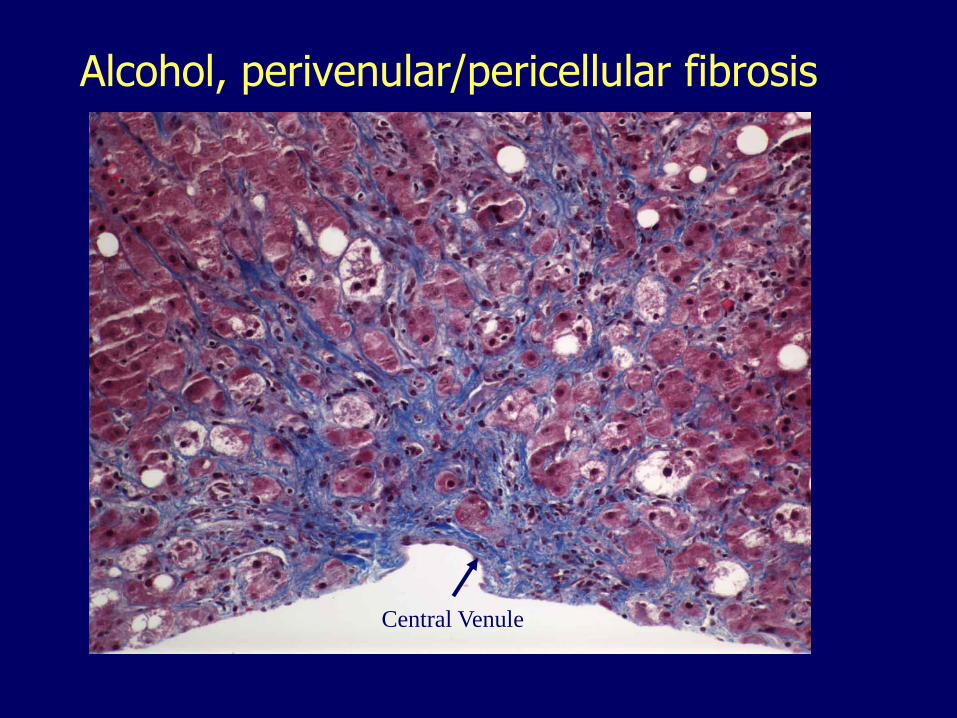
Central Venule
Alcohol, perivenular/pericellular fibrosis

Alcohol, perivenular, portal, bridging fibrosis
Non-alcoholic fatty liver disease (NAFLD)
Continuum of steatosis, hepatocyte injury, inflammation, fibrosis and cirrhosis
The designation of non-alcoholic steatohepatitis (NASH) applied when there is evidence of significant hepatocellular injury and inflammation

Non-alcoholic fatty liver disease (NAFLD)
Major risk factors:– Central obesity (visceral adiposity)– Insulin resistance (glucose intolerance)/type 2
diabetes, – Hypertriglyceridemia
Prevalence and severity increase with age Affects between 17 and 30% of Americans Prevalence is highest among Hispanics
Non-alcoholic steatohepatitis (NASH)
Morphologically similar but less severe than alcoholic steatohepatitis
Asymptomatic elevation of aminotransferases
Likelihood of progression to cirrhosis

Pathogenesis of NASH, lipotoxicity
Increased dietary fat and insulin resistance cause an increased influx of FFAs into the liver
FFAs should undergo β-oxidation or must be stored as triglycerides (steatosis)
Oxidation is compromised with insulin resistance
Individuals who develop NASH may have a reduced capacity to store FFAs as triglycerides
When the storage of FFAs is overwhelmed, FFAs generate toxic lipid metabolites that act as ROS resulting in oxidative injury and inflammation

Current concept of steatohepatitis
Insulin resistance; excessive peripheral lipolysis; increased influx of free fatty acids; lipotoxicity, oxidative stress, inflammation, fibrosis in patients who fail to adequately incorporate FFAs into triglycerides; good fat storers have a benign outcome unless additional hepatic injury (second hit) occurs