dal sospetto diagnostico alle complicanze acute - anmco€¦ · dal sospetto diagnostico alle...
TRANSCRIPT

Dal sospetto diagnostico alle complicanze acute
Dott. Cosimo A. GrecoU.O.C. Cardiochirurgia
Ospedale V. Fazzi di Lecce


TIPICALCLINICALSCENARIO



PRESENTAZIONE CLINICA
1. Dolore toracico a riposo, simile a SCA:
nel 33-71% dei casi
2. Dispnea
3. Profonda astenia
4. Sincope

ECG

Initial presentation
1. STE in precord fino all’80% se pres precoce
2. Onde T negative profonde: fino al 40%
3. Alteraz. ripolar. non specifiche: 5%
4. Onde Q patologiche: 6-31%
5. ECG normale







ECG: Subacute phase
Initial ST elevation
Days 1-3Deep T wave inversionsProminent QT prolongation> 500 ms
1-2 monthsnormal

BIOMARKERS
1. Peak troponin levels are modest
(60x the ULN as opposed to >400x ULN for STEMI)
2. BNP levels higher in TTC than in STEMI
(BNP/Troponin may diff TTC from STEMI)

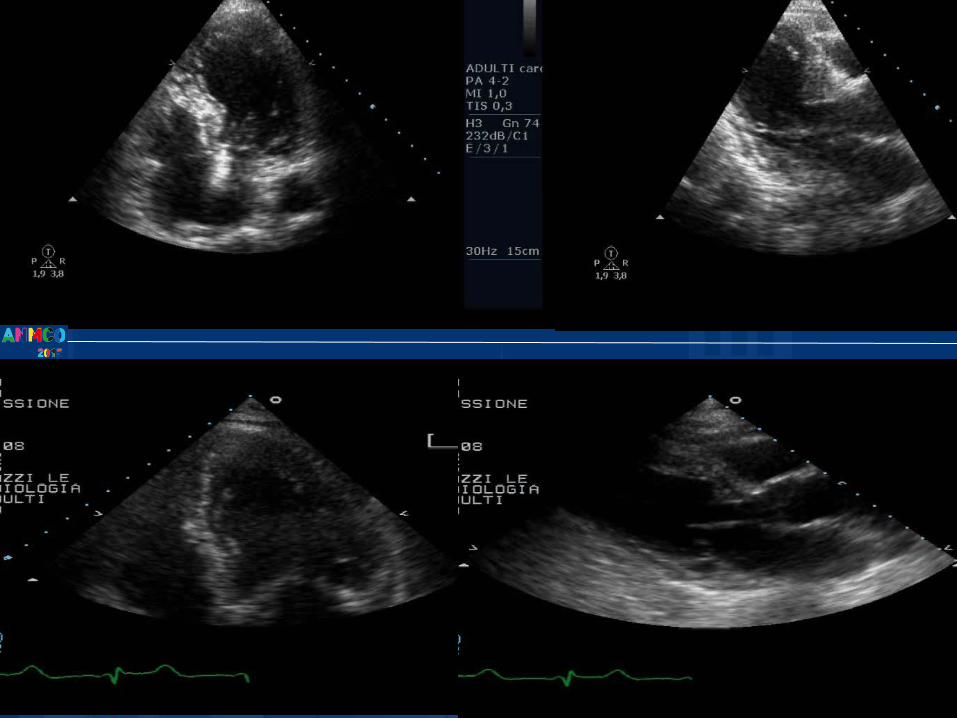
IMAGING

ECOCARDIOGRAFIA

ECHOCARDIOGRAPHY
1. Area of dysfunctional myocardium extended beyond the territory
distrib of single coron art: regional abnormalities extending into the
Anterior, inferior and lateral walls
2. RV involvement (14,5%)
3. LVOT obstruction (<20%), MR, LV thrombus, ventricular rupture
4. To confirm recovery of LV function at follow-up

DIAGNOSTIC PATTERN
1. Classic pattern: akinesis of the apical and
mid-ventric segments EXTENDING
BEYOND A SINGLE EPICARDIAL CORON
DISTRIBUTION
2. Mid-ventricular variant: apical preserved
3. Inverted TTC: mid and apical preserved


LV segmental systolic dysfunctionaccording to cor art distribution in TT vs STEMI

ECHOCARDIOGRAPHY
1. Area of dysfunctional myocardium extended beyond the territory
distrib of single coron art: regional abnormalities extending into the
Anterior, inferior and lateral walls
2. RV involvement (14,5%)
3. LVOT obstruction (<20%), MR, LV thrombus, ventricular rupture
4. To confirm recovery of LV function at follow-up

RV INVOLVEMENT: biventricularballooning, reverse Mc Connel’s sign
- RV apical akinesis and basalhyperkinesis- TAPSE e TDI anello tricuspidalico non mostrano segni di disfunzione VD

DIAGNOSTIC PATTERN
1. Classic pattern: akinesis of the apical and
mid-ventric segments EXTENDING
BEYOND A SINGLE EPICARDIAL CORON
DISTRIBUTION
2. Mid-ventricular variant: apical preserved
3. Inverted (basal ballooning) TTC: mid and apical
preserved


ECHOCARDIOGRAPHY
1. Area of dysfunctional myocardium extended beyond the territory
distrib of single coron art: regional abnormalities extending into the
Anterior, inferior and lateral walls
2. RV involvement (14,5%)
3. LVOT obstruction (<20%), MR, LV thrombus, ventricular rupture
4. To confirm recovery of LV function at follow-up

SAM
OstruzioneEfflussoLVOT

Ostruzione efflusso LVOT
InsufficienzaMitralicada SAM
ESORDIO

LVOT dopoqualche giorno

CORONARYANGIOGRAPHY

CORONARY ANGIOGRAPHY
1. In the acute phase necessary for dif diagnosis
2. Absence of: - stenosi ostruttiva (> 50%)- rottura acuta di placca ATS
3. TIMI frame count e TIMI myocardialperfusion grade prolungati
4.



Diagnostic workup



Cardiac M. R. I.

RISONANZA CARDIACA
1. Non molti studi, assenza di accumulo tardivo
di gadolinio (late enhancement) tipico dell’IMA
2. Assenza di miocardite: edema in acuto e la sua scomparsa tardiva, zone di DE sottoepicard.patchy
3. Molto utile x la diagnosi differenziale

sistole diastole

Complications

Complications


IMPLICATIONS
EARLY IDENTIFICATION OF ANY
POTENTIAL COMPLICATIONS
is CRUCIAL
FOR THE MANAGEMENT,
RISK STRATIFICATION
AND FOLLOW-UP


1 morte x SCC2 riospedalizzazioni:
1 x dolore toracico senza alteraz ECG e labor. 1 x polmonite
92% 69%


GRAZIE PER
L’ATTENZIONE
