continuing education atrial fibrillation: updated...
TRANSCRIPT
3HOURSContinuing EducationCE
26 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
CE
Atrial fibrillation, the most common chronic cardiac arrhythmia,1 is frequently associated with advancing age, structural cardiac dys-
function, and preexisting comorbidities.2 It’s esti-mated that between 2.7 and 6.1 million Americans currently live with this condition,2, 3 with nearly 75% of cases reportedly occurring in people over 65 years of age.4 According to results from the Framingham Heart Study, the lifetime risk of de-veloping atrial fibrillation is one in four.5 Given the aging of the U.S. population, the incidence is
expected to more than double over the next 50 years.3, 6
Atrial fibrillation has significant financial implica-tions for our health care system. Atrial fibrillation–related expenses alone add an estimated $6 billion to U.S. health care costs annually; when other associ-ated cardiovascular and noncardiovascular care costs are factored in, this figure jumps to $26 billion.7 An analysis of 2001 data found that in the United States, atrial fibrillation accounted for about 350,000 hospi-talizations, 5 million office visits, 276,000 ED visits,
OVERVIEW: Atrial fibrillation, the most common chronic cardiac arrhythmia, adversely affects the quality of life of millions of people. The condition is frequently associated with advancing age, structural cardiac dys-function, and preexisting comorbidities. The most common complications, stroke and heart failure, result in significant morbidity and mortality. Indeed, atrial fibrillation is responsible for over 450,000 hospitalizations and 99,000 deaths annually and adds up to $26 billion to U.S. health care costs each year. Given the aging of the U.S. population, the incidence of atrial fibrillation is expected to double within the next 50 years. There is evidence that nursing intervention in patient education and transition of care coordination can improve ad-herence to treatment plans and patient outcomes.
This article reviews the recently updated guideline for the management of atrial fibrillation, issued jointly by the American Heart Association, the American College of Cardiology, and the Heart Rhythm Society. It focuses on the prevention of thromboembolism and on symptom control, and stresses the importance of patient adherence to treatment plans in order to ensure better outcomes.
Keywords: arrhythmia, atrial fibrillation, care coordination, older adults, patient education, stroke prevention, treatment guidelines
The focus is on symptom control, stroke prevention, and patient adherence.
Atrial Fibrillation: Updated Management Guidelines and Nursing Implications

[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 27
with the sinoatrial node for control of cardiac activity. Normal atrial contractions are replaced by rapid quivering movements, and the atria stop contracting effectively.
This lack of coordinated atrial contractions can result in two of the most common complications of atrial fibrillation—thrombi formation and heart fail-ure. The formation of thrombi on the atrial walls and within the left atrial appendage (LAA) occurs when ineffective emptying allows blood to pool in these chambers. Commonly referred to as mural thrombi, these clots can dislodge and cause strokes and other systemic thromboemboli. The lack of coordinated atrial contractions can also result in less blood enter-ing and leaving the left ventricle. The loss of what is often called “atrial kick” can decrease cardiac output by as much as 30%.17 If normal cardiac output can-not be maintained, heart failure and pulmonary con-gestion will result.
Atrial fibrillation often occurs in patients with comorbidities and with structural cardiac defects. As January and colleagues note in the current AHA/ACC/HRS guideline, structural abnormalities such as fibrosis and hypertrophy “occur most commonly in the setting of underlying heart disease associated with hypertension, coronary artery disease, valvular heart disease, cardiomyopathies, and [heart failure],” and these conditions “tend to increase [left atrial] pressure, cause atrial dilation, and alter wall stress.”2 Comorbidities such as obesity, diabetes mellitus, and hyperthyroidism; alcohol or drug use; and systemic influences such as excessive autonomic nervous sys-tem stimulation (causing catecholamine imbalances) and excessive renin–angiotensin–aldosterone activa-tion (causing sodium retention and hypertension) can also cause abnormalities.2
An analysis of 2011 data from the Centers for Medicare and Medicaid Services serves to illustrate the incidence of various chronic comorbidities in two groups of beneficiaries with atrial fibrillation: those younger than 65 years and those ages 65 and older.2 In both groups, more than 80% had hypertension and more than 50% had ischemic heart disease, hy-perlipidemia, or heart failure. Other common comor-bidities included anemia, arthritis, diabetes mellitus, and chronic kidney disease. (It’s also worth noting the difference in the numbers of beneficiaries in the
By Christine L. Cutugno, PhD, RN
and 234,000 ambulatory care visits annually.8 More recent estimates put the number of hospitalizations with atrial fibrillation as the primary diagnosis at over 450,000 per year.2 As the number of older Americans rises, the costs associated with atrial fibril lation can be expected to increase as well.
Adherence to treatment guidelines for atrial fibril-lation can help to optimize treatment and reduce as-sociated costs.9 Indeed, in general, the importance of patient adherence to the prescribed treatment regimen is well known. Nurses thus have a vital role to play in ensuring that patients (or their caregivers) understand and can follow the plan of care.
This article reviews the recently updated guideline for the management of atrial fibrillation and discusses the nursing implications. The guideline was issued jointly last year by the American Heart Association (AHA), the American College of Cardiology (ACC), and the Heart Rhythm Society (HRS).2 Its recommen-dations constitute the most current evidence-based standard—what the guideline refers to as “guideline-directed medical therapy”—for the management of atrial fibrillation. The primary therapeutic goals are the prevention of thromboembolism and symptom control.
The frequency with which treatment guidelines for atrial fibrillation continue to be updated speaks to both the prevalence and the serious health care impli-cations of the condition. The 2014 AHA/ACC/HRS guideline updates earlier versions published in 2006 and 2011.2 (The European Society of Cardiology has also updated its guidelines, most recently in 2010 and 2012.6, 10) Notable themes in this newest guideline are the importance of patient involvement in and adher-ence to the prescribed plan of care and the value of an individualized treatment plan. (See Table 12, 11-16 for a summary of past and current guideline recommen-dations.)
ATRIAL FIBRILLATION: AN OVERVIEWPathophysiology. Unlike other cells, cardiac cells are capable of self-stimulation. Although this ability is protective if the heart’s conduction system fails, it can also cause ectopic activity in the cardiac cells and re-sult in atrial (or, worse, ventricular) fibrillation. In atrial fibrillation, multiple atrial cells self-stimulate, behaving as individual pacemakers and competing
28 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
two groups: 105,878 in the younger group and 2,426,865 in the older group.)
January and colleagues also point to aging and en-vironmental stress as factors; both have been linked to inflammation and may play a role in the onset of atrial fibrillation.2 Inflammatory mediators (such as C-reactive protein and interleukin-6) have been asso-ciated with such physiologic stressors as pericarditis, cardioversion, and cardiac surgery, and have been implicated in the onset of atrial fibrillation.2 Because of these multiple variables and potential complica-tions, managing atrial fibrillation is challenging.
Disease classification. Atrial fibrillation is charac-terized by the frequency and duration of episodes, and is classified into five categories: paroxysmal, persistent, long-standing persistent, permanent, and nonvalvular. (For detailed descriptions of the five categories, see Table 2.2) A single patient can have both paroxysmal and persistent episodes. Categori-zation has implications for various treatment proce-dures (such as catheter ablation) and therapy decisions, including the medications indicated and the diagnos-tic procedures chosen (such as cardioversion), as dis-cussed later in this article.
Risk factors. The incidence of atrial fibrillation is strongly associated with having one or more risk fac-tors, with one study finding that 57% of patients with atrial fibrillation had one or more risk factors, hyper-tension being the most common.18 Besides advancing age, hypertension, and the aforementioned cardiac diseases, other clinical risk factors include diabetes mellitus; hyperthyroidism; obesity; obstructive sleep apnea; and alcohol, tobacco, or drug use.2 Biomark-ers include increased levels of C-reactive protein and B-type natriuretic peptide.2
CLINICAL ASSESSMENTA diagnosis of atrial fibrillation is confirmed by elec-trocardiography (ECG) and other studies suggested by the patient’s history and physical assessment. These may include chest X-ray, transesophageal echocardiography (TEE), various types of ambula-tory rhythm monitoring (such as by using a Holter monitor or a Zio patch, insertable loop recorder, or event recorder), exercise testing, and electrophysio-logical studies.2 Additional testing may be indicated by the presence of risk factors and associated comor-bidities.
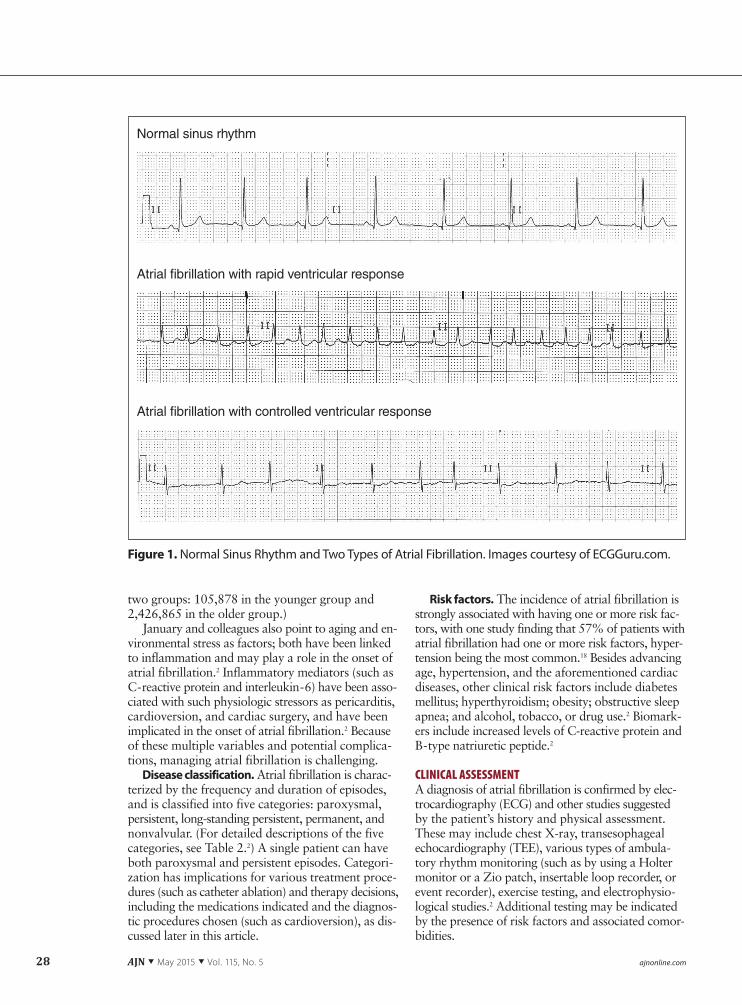
Figure 1. Normal Sinus Rhythm and Two Types of Atrial Fibrillation. Images courtesy of ECGGuru.com.
Normal sinus rhythm
Atrial fibrillation with rapid ventricular response
Atrial fibrillation with controlled ventricular response

[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 29
Signs and symptoms. Atrial fibrillation can be asymptomatic and may go unrecognized. Common symptoms include fatigue, palpitations, dyspnea, hy-potension, and syncope. Less commonly, patients may present with symptoms (such as shortness of breath or evidence of systemic emboli) of serious hemodynamic conditions (such as heart failure or stroke, respectively). One study enrolled 2,580 older adults with hypertension and no history of atrial
fibrillation and monitored them continuously for three months.19 Over the course of the study, the re-searchers found “a substantial incidence of subclini-cal atrial tachyarrhythmias”; the occurrence of such tachyarrhythmias was associated with a significantly higher risk of stroke.
On physical assessment, the heart rate of new on-set or untreated atrial fibrillation is generally rapid, because the ventricles are responding with relatively
AF = atrial fibrillation; ASA = acetylsalicylic acid (aspirin); CHADS2 = congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus, prior stroke or transient ischemic attack (TIA) or thromboembolism (TE) (doubled); CHA2DS2-VASc = congestive heart failure, hypertension, age ≥ 75 years (doubled), diabetes mellitus, prior stroke or TIA or TE (doubled), vascular disease, age 65–74 years, sex category; HAS-BLED = hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile interna-tional normalized ratio, elderly, drugs/alcohol concomitantly; HF = heart failure; HR = heart rate; INR = international normalized ratio.
Table 1. Major Changes in Guideline Recommendations for the Management of Atrial Fibrillation
Category Prior recommendations11-13
Current 2014 recommendations2
Evidence-based support for recommended changes
Recommendedtarget heart rates(remains controversial)
Resting HR < 80 bpm; exercise HR < 110 bpm
HR < 110 bpm at rest for asymptomatic patients without signs of HF
More patients achieved target HR with fewer drugs, lower doses, and fewer provider visits.15
Benefit of rhythm-control vs. rate-control strategies
Rhythm control a long-term goal
Rhythm control indicated for persistent symptoms
No benefits seen for rhythm-control vs. rate-control strategies.2, 12, 14 Lenient rate control did not increase mortality; frequency of hospitalizations and adverse events were similar.15
Risk assessment for stroke and bleeding
CHADS2 used for stroke risk assessment
• CHA2DS2-VASc recommended for stroke risk assessment
• HAS-BLED recommended to evaluate risk of bleeding
• CHA2DS2-VASc adds age, sex differentiation, and vascular disease history to CHADS2
• HAS-BLED evaluates patient based on hyper-tension, abnormal liver or renal function, stroke or bleeding history, labile INRs, elderly (age > 65), drug and alcohol use
Antithromboticagents
Warfarin (Coumadin) • Warfarin still recommended for AF patients with mechanical heart valves
• Newer antithrombotics added for nonvalvular AF: dabigatran (Pradaxa), rivaroxaban (Xarelto), apixaban (Eliquis)
Newer antithrombotics • have a wider therapeutic window than warfarin
• eliminate dietary restrictions and have fewer drug interactions
• are more expensive • do not require blood testing (unlike warfarin)16
Routine use of ASA
Recommended to decrease stroke risk in patients with low cardiovascular risk
Removed as a recommendation owing to lack of supporting evidence
Lack of data linking aspirin use to reduced incidence of strokes
Ablation therapy Not enough available data to determine scope of usefulness
Broader use encouraged for certain symptomatic AF patients refractory to medications and other treatments
Procedure has been demonstrated useful and safe for some AF patients

30 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
little impediment to excessive atrial activity. Patients usually present with tachycardia, with rates often as high as 130 beats per minute (or higher). Atrial fibril-lation can frequently be detected when taking a pulse. The patient’s pulse may be noticeably irregular and vary in strength as a result of irregular ventricular fill-ing times (and thus varying stroke volumes). Atrial fibrillation can be recognized on ECG by its wavy, er-ratic baseline; the absence of discreet and identifiable P waves; and varying R-R intervals (reflecting vary-ing ventricular response.) (See Figure 1 for illustra-tive ECG strips.)
Early evaluation of the effectiveness of cardiac ac-tivity is essential. Sustained tachycardia can result in cardiac ischemia, angina, and heart failure. Coronary arteries are perfused during diastole (or between dias-tole and systole); thus, the faster the heart rate, the less diastolic filling time, limiting such perfusion. Ischemia, seen on ECG as ST-segment and T-wave changes, can be more readily observable during tachycardia.
MANAGEMENT: THE UPDATED GUIDELINESManaging or preventing atrial fibrillation involves addressing modifiable risk factors through lifestyle changes, which might include smoking cessation, ex-ercise, weight management, and treatment for alcohol or drug abuse. Beyond this, treatment centers on pre-venting thromboembolism and controlling heart rate. Because of the effects of atrial fibrillation on cardiac output, even when heart rate is within the normal range, heart failure can occur. If atrial fibrillation remains symptomatic despite rate control, more ag-gressive measures such as ablation may be considered.
Stroke prevention: stroke and bleeding risk strat-ification. People with untreated or undertreated atrial fibrillation are at high risk for thromboembolism;
to lower that risk, anticoagulation therapy is recom-mended.11 But this increases the risk of bleeding com-plications and a potentially devastating outcome. Risk stratification for both stroke and bleeding can help guide informed decision making.20
Stroke risk stratification tools include the CHADS2 score (the acronym stands for congestive heart failure, hypertension, age 75 years or older, diabetes mellitus, prior stroke or transient ischemic attack or thrombo-embolism [doubled]) and the more recently developed CHA2DS2-VASc score (the acronym stands for con-gestive heart failure, hypertension, age 75 years or older [doubled], diabetes mellitus, prior stroke or transient ischemic attack or thromboembolism [dou-bled], vascular disease, age 65 to 74 years, sex cate-gory). As the acronym shows, the latter tool considers additional risk factors such as female sex and the pres-ence of vascular disease; it also allows for some dif-ferentiation by age, which is important because stroke risk increases with every year over the age of 65.20 The 2014 AHA/ACC/HRS guideline discusses the broader use of CHA2DS2-VASc for assessing stroke risk in pa-tients with nonvalvular atrial fibrillation. Using the rec-ommended CHA2DS2-VASc tool, adjusted stroke rate scores have been found to range from 0% to 15.2% per year.21 (See Table 3 at http://links.lww.com/AJN/A67.2, 21)
Bleeding risk stratification scoring systems such as HAS-BLED (the acronym stands for hypertension, abnormal renal or liver function, stroke, bleeding his-tory or predisposition, labile international normalized ratio [INR], elderly, drugs or alcohol concomitantly) evaluate bleeding risk based on several salient factors. As the acronym suggests, the HAS-BLED system con-siders hypertension, history of stroke or bleeding, labile INRs, age over 65 years, use of drugs that promote
Table 2. Classification of Atrial Fibrillation
AF = atrial fibrillation.Reprinted with permission from January CT, et al. The 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. Circulation 2014;130(23):e199-e267.2
Paroxysmal AF • AF that terminates spontaneously or with intervention within 7 days of onset. • Episodes may recur with variable frequency.
Persistent AF • Continuous AF that is sustained >7 days.
Long-standing persistent AF
• Continuous AF of > 12 months’ duration.
Permanent AF • Permanent AF is used when there has been a joint decision by the patient and clinician to cease further attempts to restore and/or maintain sinus rhythm.
• Acceptance of AF represents a therapeutic attitude on the part of the patient and clinician rather than an inherent pathophysiological attribute of the AF.
• Acceptance of AF may change as symptoms, the efficacy of therapeutic interventions, and patient and clinician preferences evolve.
Nonvalvular AF • AF in the absence of rheumatic mitral stenosis, a mechanical or bioprosthetic heart valve, or mitral valve repair.

[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 31
bleeding or alcohol use (or both), and renal and liver function.2, 22 (See Table 4 at http://links.lww.com/AJN/A68.22)
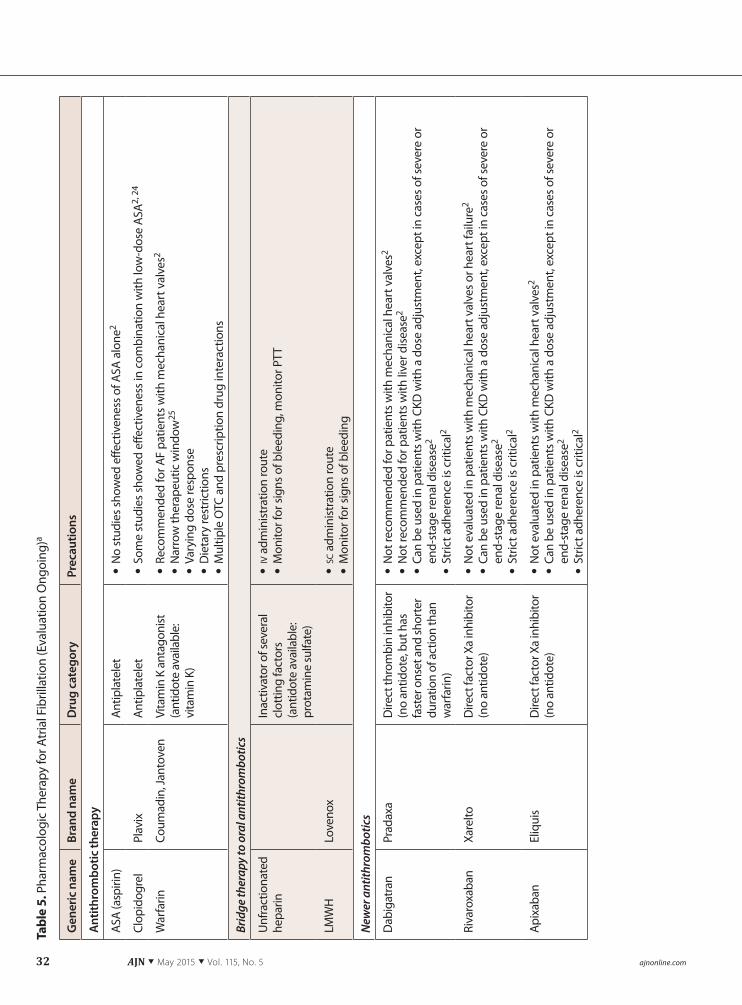
Stroke prevention: antithrombotic agents. An-tithrombotic agents currently used to treat atrial fi-brillation include established anticoagulants such as warfarin (Coumadin, Jantoven), unfractionated hepa-rin, and low-molecular-weight heparin; newer throm-bin and factor Xa inhibitors; and antiplatelet drugs such as clopidogrel (Plavix). Aspirin alone is no lon-ger recommended as data of effectiveness are lacking.2 The U.S. Food and Drug Administration has recently approved several newer antithrombotics, including dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis), and these may be considered in certain cases.2 Like warfarin, these newer drugs re-quire strict adherence in order to be effective. More-over, they have not been tested for use in patients with mechanical heart valves or hemodynamically significant mitral stenosis; these patients should be treated with warfarin.2
The choice of agent will be based on an assessment of the patient’s clinical status, ability to adhere to the medication regimen, and bleeding risk; the drug’s elim-ination route; potential drug–drug interactions; pro-vider preference; and cost considerations. Although warfarin is an established and effective antithrom-botic, it has several disadvantages, including the need for dietary restrictions, its potential for multiple drug interactions, and the need for frequent INR testing to determine adequate therapeutic levels. A recently pub-lished meta-analysis of eight trials of patients on war-farin found that, on average, patients spent only 55% to 68% of the trial period in the therapeutic INR range.23 Warfarin has the advantage of having a re-versal agent, vitamin K; but the other an tithrombotics have much shorter half-lives. Aspirin alone has not been found effective for preventing stroke in patients with atrial fibrillation.2 For more on pharmacologic therapy for atrial fibrillation, see Table 5.2. 24, 25
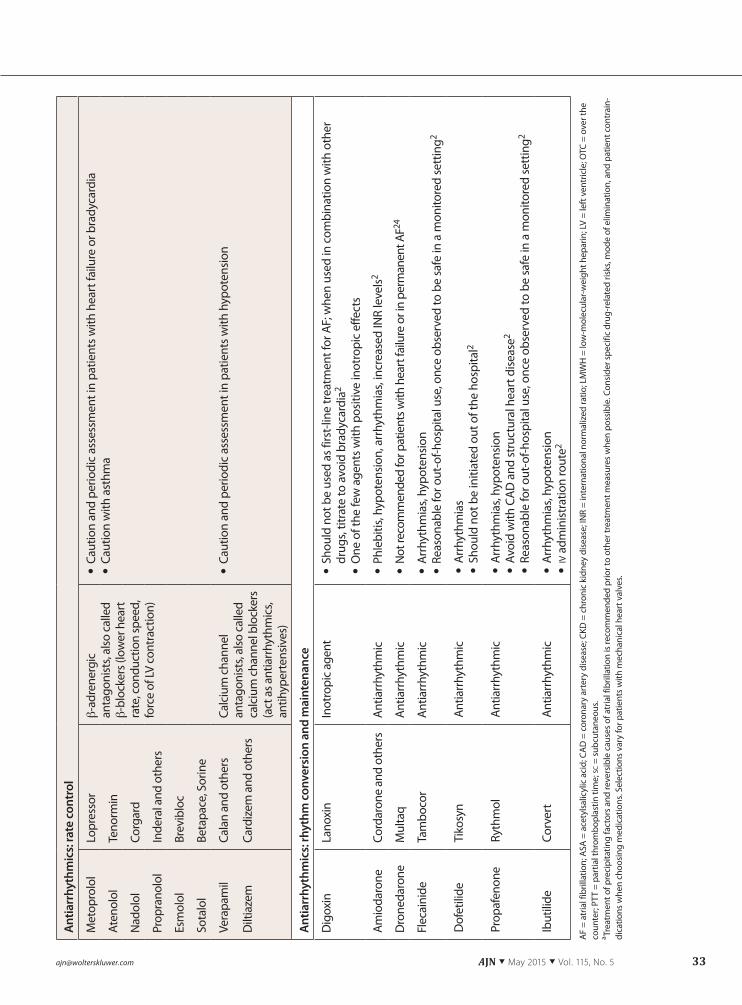
Rate control. For patients who are asymptomatic and show no signs of heart failure, the 2014 AHA/ACC/HRS guideline recommends a resting heart rate of less than 110 beats per minute.2 This relatively le-nient target allows patients to achieve the target rate with fewer drugs, lower doses, and fewer provider vis-its. But for symptomatic patients, the recommended heart rate target is less than 80 beats per minute; and when patients have underlying cardiac disease or other comorbidities, the target rate must be individualized. Rate control reduces the morbidity associated with sustained tachycardia (such as cardiomyopathy) and decreases the distressing cardiac and hemodynamic symptoms associated with rapid heart rates.
Recommended and commonly used drugs for rate control include β-adrenergic antagonists (also called β-blockers) and calcium channel antagonists (also called calcium channel blockers); digoxin (Lan-
oxin) and amiodarone (Cordarone and others) may be indicated in particular clinical situations. The Atrial Fibrillation Follow-Up Investigation of Rhythm Man-agement (AFFIRM) study evaluated the effectiveness of such drugs in controlling heart rate in 2,027 pa-tients.26 Heart rate control was achieved in 70% of patients receiving β-blockers (alone or with digoxin), in 54% of those receiving calcium channel blockers (alone or with digoxin), and in 58% of those receiv-ing digoxin alone.
With any drug, the potential for unwanted side effects must be considered relative to (or bal-anced against) the patient’s clinical condition. Both β-blockers and calcium channel blockers can cause arrhythmias, heart failure, and hypotension. Heart failure can result from the negative inotropic effects of these drugs; and hypotension can result from their blocking of the vasoconstrictive effects of the sym-pathetic nervous system. Patients with asthma may be at higher risk for bronchospasm; the use of cardio-selective β-blockers will mitigate this risk. In acutely ill patients, iv administration of these medications is indicated. Patients must be closely monitored for unwanted side effects. Since some of these medica-tions can cause sustained bradycardia, in cases of long-term use prophylactic pacemaker insertion may be indicated.
Rhythm control. The conversion of atrial fibril-lation to normal sinus rhythm has been shown to decrease symptoms.2 Rhythm control is most often used in patients with new-onset atrial fibrillation; in younger patients; and in patients whose symp-toms remain unresponsive to, or who are intolerant of, rate-control medications. Atrial fibrillation of long duration is much more difficult to convert. Rhythm control may involve the use of antiarrhythmics, electri-cal cardioversion, ablation, or a combination of these. Treatment choices vary depending on the patient’s age, the patient’s clinical presentation, and the du-ration and classification of the atrial fibrillation. No benefits for rhythm-control versus rate-control strate-gies have been found; and neither approach has shown superiority in decreasing mortality.2, 12, 14
Pharmacologic cardioversion. Several antiar-rhythmic agents (amiodarone, dofetilide [Tikosyn], flecainide [Tambocor], propafenone [Rythmol], and ibutilide iv [Corvert]) have demonstrated effective-ness in converting atrial fibrillation.2 But most have contraindications and will not be appropriate for all patients. Moreover, each has significant and life-threatening adverse effects that require some duration of ECG assessment for bradycardia or prolongation of the QT interval.2
A meta-analysis of 39 randomized controlled trials found that amiodarone was the most effective drug for maintaining normal sinus rhythm once atrial fibrilla-tion had been converted; but it was also associated with the highest rate of adverse events.27 Dronedarone
32 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
Gen
eric
nam
eBr
and
nam
eD
rug
cate
gory
Prec
autio
ns
Ant
ithro
mbo
tic th
erap
y
ASA
(asp
irin)
Antip
late
let
• N
o st
udie
s sho
wed
effe
ctiv
enes
s of A
SA a
lone
2
Clop
idog
rel
Plav
ixAn
tipla
tele
t • So
me
stud
ies s
how
ed e
ffect
iven
ess i
n co
mbi
natio
n w
ith lo
w-d
ose
ASA2,
24
War
farin
Coum
adin
, Jan
tove
nVi
tam
in K
ant
agon
ist
(ant
idot
e av
aila
ble:
vi
tam
in K
)
• Re
com
men
ded
for A
F pa
tient
s with
mec
hani
cal h
eart
val
ves2
• N
arro
w th
erap
eutic
win
dow
25
• Va
ryin
g do
se re
spon
se • D
ieta
ry re
stric
tions
• M
ultip
le O
TC a
nd p
resc
riptio
n dr
ug in
tera
ctio
ns
Brid
ge th
erap
y to
ora
l ant
ithro
mbo
tics
Unf
ract
iona
ted
hepa
rinIn
activ
ator
of s
ever
al
clot
ting
fact
ors
(ant
idot
e av
aila
ble:
pr
otam
ine
sulfa
te)
• iv
adm
inist
ratio
n ro
ute
• M
onito
r for
sign
s of b
leed
ing,
mon
itor P
TT
LMW
HLo
veno
x • sc
adm
inist
ratio
n ro
ute
• M
onito
r for
sign
s of b
leed
ing
New
er a
ntith
rom
botic
s
Dab
igat
ran
Prad
axa
Dire
ct th
rom
bin
inhi
bito
r(n
o an
tidot
e, b
ut h
as
fast
er o
nset
and
shor
ter
dura
tion
of a
ctio
n th
an
war
farin
)
• N
ot re
com
men
ded
for p
atie
nts w
ith m
echa
nica
l hea
rt v
alve
s2 • N
ot re
com
men
ded
for p
atie
nts w
ith li
ver d
iseas
e2
• Ca
n be
use
d in
pat
ient
s with
CKD
with
a d
ose
adju
stm
ent,
exce
pt in
cas
es o
f sev
ere
or
end-
stag
e re
nal d
iseas
e2
• St
rict a
dher
ence
is c
ritic
al2
Riva
roxa
ban
Xare
ltoD
irect
fact
or X
a in
hibi
tor
(no
antid
ote)
• N
ot e
valu
ated
in p
atie
nts w
ith m
echa
nica
l hea
rt v
alve
s or h
eart
failu
re2
• Ca
n be
use
d in
pat
ient
s with
CKD
with
a d
ose
adju
stm
ent,
exce
pt in
cas
es o
f sev
ere
or
end-
stag
e re
nal d
iseas
e2
• St
rict a
dher
ence
is c
ritic
al2
Apix
aban
Eliq
uis
Dire
ct fa
ctor
Xa
inhi
bito
r (n
o an
tidot
e) • N
ot e
valu
ated
in p
atie
nts w
ith m
echa
nica
l hea
rt v
alve
s2
• Ca
n be
use
d in
pat
ient
s with
CKD
with
a d
ose
adju
stm
ent,
exce
pt in
cas
es o
f sev
ere
or
end-
stag
e re
nal d
iseas
e2
• St
rict a
dher
ence
is c
ritic
al2
Tabl
e 5.
Pha
rmac
olog
ic T
hera
py fo
r Atr
ial F
ibril
latio
n (E
valu
atio
n O
ngoi
ng)a
[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 33
Ant
iarr
hyth
mic
s: ra
te c
ontr
ol
Met
opro
lol
Lopr
esso
rβ-
adre
nerg
ic
anta
goni
sts,
also
cal
led
β-bl
ocke
rs (l
ower
hea
rt
rate
, con
duct
ion
spee
d,
forc
e of
LV c
ontr
actio
n)
• Ca
utio
n an
d pe
riodi
c as
sess
men
t in
patie
nts w
ith h
eart
failu
re o
r bra
dyca
rdia
• Ca
utio
n w
ith a
sthm
aAt
enol
olTe
norm
in
Nad
olol
Corg
ard
Prop
rano
lol
Inde
ral a
nd o
ther
s
Esm
olol
Brev
iblo
c
Sota
lol
Beta
pace
, Sor
ine
Vera
pam
il
Dilt
iaze
m
Cala
n an
d ot
hers
Card
izem
and
oth
ers
Calc
ium
cha
nnel
an
tago
nist
s, al
so c
alle
d ca
lciu
m c
hann
el b
lock
ers
(act
as a
ntia
rrhy
thm
ics,
antih
yper
tens
ives
)
• Ca
utio
n an
d pe
riodi
c as
sess
men
t in
patie
nts w
ith h
ypot
ensio
n
Ant
iarr
hyth
mic
s: rh
ythm
con
vers
ion
and
mai
nten
ance
Dig
oxin
Lano
xin
Inot
ropi
c ag
ent
• Sh
ould
not
be
used
as f
irst-
line
trea
tmen
t for
AF;
whe
n us
ed in
com
bina
tion
with
oth
er
drug
s, tit
rate
to a
void
bra
dyca
rdia
2
• O
ne o
f the
few
age
nts w
ith p
ositi
ve in
otro
pic
effe
cts
Amio
daro
neCo
rdar
one
and
othe
rsAn
tiarr
hyth
mic
• Ph
lebi
tis, h
ypot
ensio
n, a
rrhy
thm
ias,
incr
ease
d IN
R le
vels
2
Dro
neda
rone
Mul
taq
Antia
rrhy
thm
ic • N
ot re
com
men
ded
for p
atie
nts w
ith h
eart
failu
re o
r in
perm
anen
t AF24
Flec
aini
deTa
mbo
cor
Antia
rrhy
thm
ic • Ar
rhyt
hmia
s, hy
pote
nsio
n • Re
ason
able
for o
ut-o
f-hos
pita
l use
, onc
e ob
serv
ed to
be
safe
in a
mon
itore
d se
ttin
g2
Dof
etili
deTi
kosy
nAn
tiarr
hyth
mic
• Ar
rhyt
hmia
s • Sh
ould
not
be
initi
ated
out
of t
he h
ospi
tal2
Prop
afen
one
Ryth
mol
Antia
rrhy
thm
ic • Ar
rhyt
hmia
s, hy
pote
nsio
n • Av
oid
with
CAD
and
stru
ctur
al h
eart
dise
ase2
• Re
ason
able
for o
ut-o
f-hos
pita
l use
, onc
e ob
serv
ed to
be
safe
in a
mon
itore
d se
ttin
g2
Ibut
ilide
Corv
ert
Antia
rrhy
thm
ic • Ar
rhyt
hmia
s, hy
pote
nsio
n • iv
adm
inist
ratio
n ro
ute2
AF
= at
rial f
ibril
latio
n; A
SA =
ace
tyls
alic
ylic
aci
d; C
AD
= c
oron
ary
arte
ry d
isea
se; C
KD =
chr
onic
kid
ney
dise
ase;
INR
= in
tern
atio
nal n
orm
aliz
ed ra
tio; L
MW
H =
low
-mol
ecul
ar-w
eigh
t hep
arin
; LV
= le
ft v
entr
icle
; OTC
= o
ver t
he
coun
ter;
PTT
= pa
rtia
l thr
ombo
plas
tin ti
me;
sc =
sub
cuta
neou
s.a Tr
eatm
ent o
f pre
cipi
tatin
g fa
ctor
s an
d re
vers
ible
cau
ses
of a
tria
l fib
rilla
tion
is re
com
men
ded
prio
r to
othe
r tre
atm
ent m
easu
res
whe
n po
ssib
le. C
onsi
der s
peci
fic d
rug-
rela
ted
risks
, mod
e of
elim
inat
ion,
and
pat
ient
con
trai
n-di
catio
ns w
hen
choo
sing
med
icat
ions
. Sel
ectio
ns v
ary
for p
atie
nts
with
mec
hani
cal h
eart
val
ves.
34 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
(Multaq) was associated with the lowest rate of ad-verse events. Other drugs shown to be effective in maintaining normal sinus rhythm following cardio-version include dofetilide, flecainide, propafenone, and sotalol (Betapace, Sorine).2, 27
Electrical cardioversion. The purpose of electrical cardioversion is to depolarize all of the cardiac cells si-multaneously in an effort to prompt a normal cardiac rhythm. This involves delivering an electrical shock synchronized to the QRS complex (in order to avoid delivering current during the T wave, which could cause ventricular fibrillation). Cardioversion is per-formed under moderate sedation with ECG moni-toring; advanced cardiac life support (ACLS)–trained staff should be present and resuscitation equipment available. The standard of care for hemodynamically unstable patients remains immediate electrical cardio-version.2
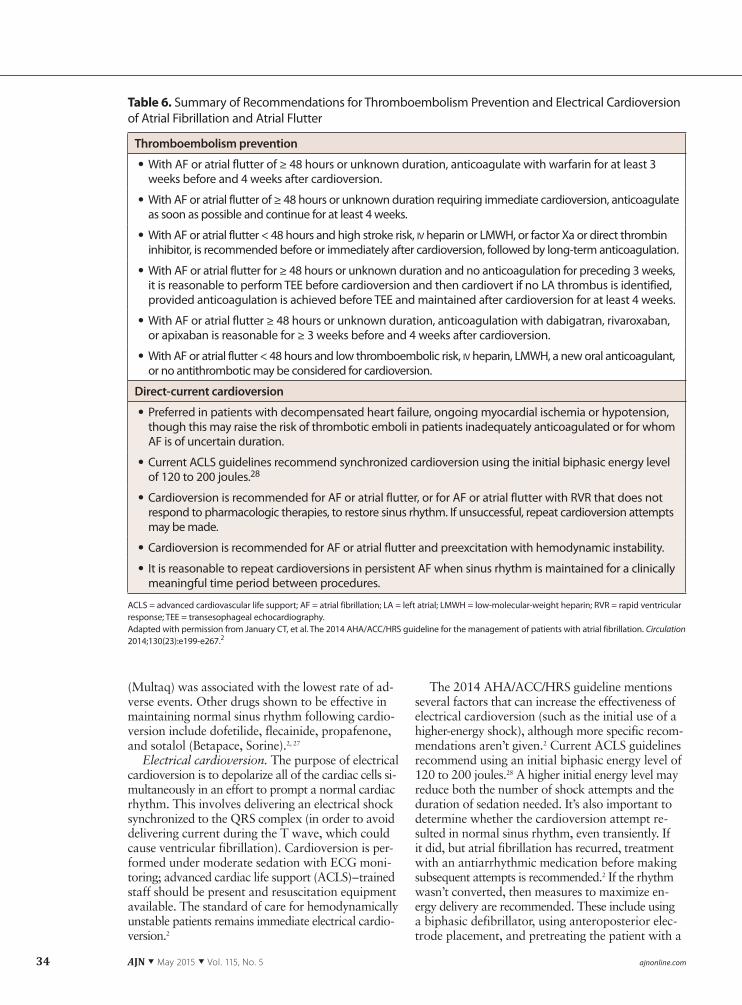
The 2014 AHA/ACC/HRS guideline mentions several factors that can increase the effectiveness of electrical cardioversion (such as the initial use of a higher-energy shock), although more specific recom-mendations aren’t given.2 Current ACLS guidelines recommend using an initial biphasic energy level of 120 to 200 joules.28 A higher initial energy level may reduce both the number of shock attempts and the duration of sedation needed. It’s also important to determine whether the cardioversion attempt re-sulted in normal sinus rhythm, even transiently. If it did, but atrial fibrillation has recurred, treatment with an antiarrhythmic medication before making subsequent attempts is recommended.2 If the rhythm wasn’t converted, then measures to maximize en-ergy delivery are recommended. These include using a biphasic defibrillator, using anteroposterior elec-trode placement, and pretreating the patient with a
ACLS = advanced cardiovascular life support; AF = atrial fibrillation; LA = left atrial; LMWH = low-molecular-weight heparin; RVR = rapid ventricular response; TEE = transesophageal echocardiography.Adapted with permission from January CT, et al. The 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. Circulation 2014;130(23):e199-e267.2
Thromboembolism prevention
• With AF or atrial flutter of ≥ 48 hours or unknown duration, anticoagulate with warfarin for at least 3 weeks before and 4 weeks after cardioversion.
• With AF or atrial flutter of ≥ 48 hours or unknown duration requiring immediate cardioversion, anticoagulate as soon as possible and continue for at least 4 weeks.
• With AF or atrial flutter < 48 hours and high stroke risk, iv heparin or LMWH, or factor Xa or direct thrombin inhibitor, is recommended before or immediately after cardioversion, followed by long-term anticoagulation.
• With AF or atrial flutter for ≥ 48 hours or unknown duration and no anticoagulation for preceding 3 weeks, it is reasonable to perform TEE before cardioversion and then cardiovert if no LA thrombus is identified, provided anticoagulation is achieved before TEE and maintained after cardioversion for at least 4 weeks.
• With AF or atrial flutter ≥ 48 hours or unknown duration, anticoagulation with dabigatran, rivaroxaban, or apixaban is reasonable for ≥ 3 weeks before and 4 weeks after cardioversion.
• With AF or atrial flutter < 48 hours and low thromboembolic risk, iv heparin, LMWH, a new oral anticoagulant, or no antithrombotic may be considered for cardioversion.
Direct-current cardioversion
• Preferred in patients with decompensated heart failure, ongoing myocardial ischemia or hypotension, though this may raise the risk of thrombotic emboli in patients inadequately anticoagulated or for whom AF is of uncertain duration.
• Current ACLS guidelines recommend synchronized cardioversion using the initial biphasic energy level of 120 to 200 joules.28
• Cardioversion is recommended for AF or atrial flutter, or for AF or atrial flutter with RVR that does not respond to pharmacologic therapies, to restore sinus rhythm. If unsuccessful, repeat cardioversion attempts may be made.
• Cardioversion is recommended for AF or atrial flutter and preexcitation with hemodynamic instability.
• It is reasonable to repeat cardioversions in persistent AF when sinus rhythm is maintained for a clinically meaningful time period between procedures.
Table 6. Summary of Recommendations for Thromboembolism Prevention and Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter

[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 35
medication that lowers the defibrillation threshold (such as ibutilide).
Under nonemergent conditions, and depending on the patient’s clinical presentation, anticoagula-tion pretreatment for at least three weeks may be recommended before either pharmacologic or elec-trical cardioversion.2, 29 When emergency cardiover-sion is performed, antithrombotics should be started before or during the procedure, if possible, and con-tinued afterward; regardless, emergency cardioversion should not be delayed.29 When cardioversion is elec-tive, TEE can provide an alternative to anticoagulation pretreatment.2, 29 TEE allows visualization of the inner chambers of the atria and can help in the detection of mural thrombi. If the atrial fibrillation has lasted 48 hours or less, neither TEE nor antithrombotic pre-treatment is generally indicated, but antithrombotics should be given “at full venous thromboembolism treatment doses” during and after cardioversion.29 If the atrial fibrillation has lasted longer than 48 hours, or if the duration is unknown, evaluation with TEE and antithrombotic pretreatment are recommended.2, 29 Anticoagulation treatment should continue for at least four weeks after cardioversion.
For a summary of current AHA/ACC/HRS recom-mendations for cardioversion, see Table 6.2, 28
Supplemental treatment modalities include the following.
Occlusion of the LAA. The LAA is “the primary source” of thromboembolism in patients with nonval-vular atrial fibrillation.2, 30 It can be excluded as such a source either with devices inserted percutaneously or during cardiac surgery. The percutaneously inserted devices, which occlude or tie off the opening of the LAA, are still under investigation, but may be consid-ered for use in patients who don’t respond to pharma-cologic anticoagulation. There is a lack of consensus regarding the use of surgical procedures to exclude the LAA during concomitant cardiac surgery. Removal has yielded “inconsistent results”; and the data reveal “highly variable rates of successful LAA occlusion.”2
Radiofrequency catheter ablation and the Cox maze procedure. The 2014 AHA/ACC/HRS guideline recommends radiofrequency catheter ablation for symptomatic patients who are refractory to or can-not tolerate other treatments.2 The procedure involves inserting catheters to locate areas of atrial tissue that are causing fibrillation and then scarring the pulmo-nary veins in those areas to prevent the conduction of ectopic stimuli.31 In a study of 323 patients treated with catheter ablation and followed for two years, 72% maintained normal sinus rhythm without anti-arrhythmics; an additional 15% maintained it with antiarrhythmics.32 Improvement in atrial fibrillation–related symptoms and quality of life were also noted. A recent literature review concluded that catheter ablation appears to be safe for use in appropriately screened elderly patients, with one study reportedly
finding an average complication rate of 4.5%.33 And a large study of adults who had undergone an initial ablation procedure found that 5% had serious peri-procedural complications, including perforation, cardiac tamponade, and stroke.34 Other potential complications include atrial-esophageal fistula, myo-cardial infarction, pericarditis, pulmonary vein steno-sis, vascular complications, and death.
Early versions of the Cox maze procedure (often called simply “the maze procedure”) required sur-geons to surgically ablate atrial tissue using “cut and sew” methods. Of these, the Cox maze III is still some-times performed. In the most recent version, known as the Cox maze IV, surgeons use radiofrequency ab-lation or cryoablation techniques to achieve the same end. The Cox maze procedure may be appropriate for select patients undergoing concomitant cardiac surgery for other reasons or for highly symptomatic patients whose atrial fibrillation isn’t well managed.2 In a study of 112 patients undergoing the most recent procedure, 50% to 87% of patients were free from atrial fibril-lation at six months’ follow-up.35 (The range reflects variation according to the duration of atrial fibrilla-tion and whether patients required continuing treat-ment with antiarrhythmics.) The overall complication rate was 10%.
Pacemakers and nodal ablation. Pacemakers are indicated primarily for patients who develop symp-tomatic bradycardia as a result of pharmacotherapy for atrial fibrillation.2 (These patients often have underlying sick sinus syndrome.) Pacemakers are also used in patients with refractory atrial fibrilla-tion who have been treated with nodal ablation.2 In nodal ablation, radiofrequency catheter ablation is used to obliterate the atrioventricular node, thus pre-venting the atria’s rapid, irregular impulses from reach-ing the ventricles.
Aside from such cases, neither pacemakers nor im-plantable cardioverter–defibrillators have been shown to be effective in preventing or treating atrial fibrilla-tion, and are not recommended.2
NURSING IMPLICATIONSThe importance of nursing interventions to improv-ing patient care outcomes has been well documented. With any illness, patient education and care coordina-tion are vital to effective disease management. Multi-ple studies have evaluated nursing interventions used in the management of atrial fibrillation or of compli-cations often associated with atrial fibrillation (such as heart failure), and found numerous benefits.36-40
For example, in an Australian study by Inglis and colleagues of 152 patients with atrial fibrillation and with or without concurrent heart failure, patients re-ceived either a nurse-led, multidisciplinary home-based intervention or usual postdischarge care.40 Those in the intervention group had fewer readmissions, shorter hospital stays, and fewer fatal events than those in the

36 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
control group, although significance varied. Gillis and colleagues looked at data for Canadian patients who were referred to a nurse clinician–based atrial fibrilla-tion clinic and found they had “markedly shorter” wait times to see a specialist than were usual for that region.37 In a Dutch study, a nurse-driven, guideline-based, integrated chronic care program was imple-mented for 111 patients with atrial fibrillation.39 Guideline adherence for patients in the program was 96%, compared with 70% for controls.
In a study by Benatar and colleagues, conducted among 216 patients with heart failure, patients re-ceived either home nurse visits from cardiac nurses or interdisciplinary home telemanagement implemented by an advanced practice nurse.36 After three months, the researchers found that compared with patients managed through traditional home care, those man-aged by home telemanagement had signif icantly fewer hospital readmissions (13 versus 24), shorter readmis-sion lengths of stay (49.5 versus 105 days), and lower hospital charges ($65,023 versus $177,365). And in a study by Cowan and colleagues conducted among 1,207 hospitalized general medicine patients, patients received either usual care management or an inter-vention that included the involvement of an NP dur-ing hospitalization and for 30 days after discharge.41 The results showed that compared with controls,
patients in the intervention group had shorter hospital stays and associated cost reductions. Further studies investigating the financial impact of implementing more nursing interventions and adding more nursing hours in order to improve outcomes and prevent re-admissions are warranted.
Managing atrial fibrillation has traditionally been challenging for both providers and patients. A quantitative study by Aliot and colleagues involv-ing 825 patients with atrial fibrillation and 810 car-diologists in 11 European countries found that the patients (who often had associated diseases) visited a physician an average of nine times per year, and that the physicians considered atrial fibrillation difficult and time consuming to manage.1 Achieving adequate anticoagulation offers a prime example of such dif-ficulty. Strict adherence to the medication regimen is essential and may require frequent blood tests and dietary restrictions (as is the case for patients on war-farin). Inadequate anticoagulation of high-risk atrial fibrillation patients has been found to be associated with a significantly worse cardiovascular prognosis over the course of one year.42
All chronic diseases are known to affect quality of life, and this can influence patients’ desire or ability to follow prescribed treatment plans. Aliot and col-leagues found that 24% of patients rated their ability
ASA = acetylsalicylic acid (aspirin); NSAIDs = nonsteroidal antiinflammatory drugs.
Table 7. Patient Education for Atrial Fibrillation Patients: Content to Cover45
Topic Content
Atrial fibrillation Causes, risks if untreated, complications, signs and symptoms
Treatment plan • Goals of treatment • For each medication: purpose, dosage, time of day it should be taken, normal and adverse effects, importance of monitoring and therapeutic range, frequency of laboratory tests, signs and symptoms to report (for example, with anticoagulation agents, signs of bleeding), importance of not stopping medications
• Follow-up care: treatments, how often to schedule laboratory tests and provider visits
Dietary and activity restrictions
Dietary restrictions and medication interactions, permitted and restricted activities, pulse taking
Risk factor modifications
Smoking cessation, exercise, weight and cholesterol management, alcohol and drug use
Stroke symptoms Headache, blurred or double vision, face droop, one-sided weakness, dizziness
Safety precautions to prevent injury
• Home safety-check elements: loose floor rugs, poor lighting • Personal elements: assistive devices, vision and hearing checks, well-fitting shoes, gait testing
Important information to report
• Signs and symptoms such as palpitations, syncope, weight gain, shortness of breath, fatigue, edema, signs of bleeding (bruising, bleeding gums, blood in urine, black stools)
• Use of supplements (such as St. John’s wort, ginseng) and of over-the-counter drugs (especially NSAIDs, ASA, and any medication containing ASA, such as Alka-Seltzer)
[email protected] AJN ▼ May 2015 ▼ Vol. 115, No. 5 37
to explain atrial fibrillation as poor and more than one-third were worried or fearful about the disease.1 Another study involving 101 patients with atrial fi-brillation and 97 controls with hypertension found that about one-third of the atrial fibrillation patients had elevated levels of depression and anxiety, which persisted at six months.43 Depressive symptoms were found to be the strongest independent predictor of their future quality of life.
Care coordination and guideline adherence. The care of patients with atrial fibrillation is complex and can be confusing even for health care providers. Care coordination among providers is essential, as is ad-herence by patients and providers to both guideline recommendations and individual treatment plans. As the 2014 AHA/ACC/HRS guideline makes a point of noting, “Prescribed courses of treatment . . . are effec-tive only if followed.”2
A systematic review of seven studies utilizing care pathway management for 3,690 patients with heart failure found that the use of care pathways decreased mortality and readmission rates.44 In another study, Hendricks and colleagues randomized 712 patients with atrial fibrillation to either a nurse-led care group or a usual care group; the nurse-led care group was guideline based and included more detailed patient education and the use of dedicated decision-making software.38 The researchers found that compared with patients in the usual care group, patients in the nurse-led care group were better informed and adherence to guideline recommendations by providers and patients was markedly improved.
Patient education. Since patient education is a common regulatory requirement, most patient health records document this. But providing information doesn’t guarantee understanding. The content that pa-tients with atrial fibrillation need to be taught about the condition and their treatment plan is generally rec-ognized (for a summary, see Table 745). Ensuring that patients understand this content is more difficult and requires more than a cursory discussion.
It’s well known that patients need time to access information and to clarify with providers anything they don’t fully understand. Indeed, it’s an accepted principle in education that repeating what one has been taught improves comprehension and retention.
But time is a scarce resource in busy, often under-staffed, hospitals.
The effectiveness of evidence-based, RN-led, follow-up care plans has also been demonstrated.36, 38, 40, 41 Yet such plans usually require more nurses and nursing hours, and unfortunately predominate only in the lit-erature. It’s my observation, based on nearly 40 years in hospital nursing, that the usual discharge instruc-tions typically delivered just once by a harried staff nurse or medical resident don’t begin to meet patient education needs. And follow-up care must consist of more than scheduling a follow-up appointment with a provider. Sustained follow-up by an outpatient or home care nurse can provide opportunities for pa-tients to have their questions answered and can rein-force the goals of treatment.
Given that U.S. expenditures for the treatment of atrial fibrillation and associated conditions stand at $26 billion annually,7 and with nearly 75% of these costs associated with inpatient care,8 it also makes financial sense to make sure that patients are well-informed and understand their treatment plans. Fo-cused efforts to prepare patients for care transitions may prevent unnecessary—and often unreimbursed—readmissions.
LOOKING AHEADThe 2014 AHA/ACC/HRS guideline invites a recom-mitment to the effective management of patients with atrial fibrillation. Its recommendations, which are based on the most recent evidence available, focus particularly on measures to prevent thromboembo-lism and control symptoms. The guideline also stresses the importance of patient adherence to treatment plans in achieving improved outcomes. And there is evidence that nursing interventions in patient education and in care coordination, particularly at transition points, can also improve patient outcomes and decrease costs. More resources must be dedicated if these goals are to be realized. ▼
Christine L. Cutugno is an assistant professor of nursing and graduate coordinator for the Adult-Gerontology Clinical Nurse Specialist Program at the Hunter-Bellevue School of Nursing in New York City. A critical care nurse for over 30 years, she was most recently the director of the Critical Care Division at St. Joseph’s Regional Medical Center in Paterson, NJ, from 2003 to 2009, and at Jacobi Medical Center, Bronx, NY, from 1999 to 2003. Contact author: [email protected]. The au-thor and planners have disclosed no potential conflicts of in-terest, financial or otherwise.
REFERENCES1. Aliot E, et al. An international survey of physician and patient
understanding, perception, and attitudes to atrial fibrillation
The 2014 guideline invites a
recommitment to the effective
management of patients with
atrial fibrillation.
For more than 60 additional continuing nursing education activities on cardiovascular topics, go to www.nursingcenter.com/ce.
38 AJN ▼ May 2015 ▼ Vol. 115, No. 5 ajnonline.com
and its contribution to cardiovascular disease morbidity and mortality. Europace 2010;12(5):626-33.
2. January CT, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Soci-ety. Circulation 2014;130(23):e199-e267.
3. Naccarelli GV, et al. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol 2009;104(11): 1534-9.
4. Kazemian P, et al. Atrial fibrillation and heart failure in the elderly. Heart Fail Rev 2012;17(4-5):597-613.
5. Lloyd-Jones DM, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation 2004; 110(9):1042-6.
6. European Heart Rhythm Association, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010;31(19):2369-429.
7. Kim MH, et al. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes 2011;4(3):313-20.
8. Coyne KS, et al. Assessing the direct costs of treating non-valvular atrial fibrillation in the United States. Value Health 2006;9(5):348-56.
9. Singh SN. Costs and clinical consequences of suboptimal atrial fibrillation management. Clinicoecon Outcomes Res 2012;4: 79-90.
10. Camm AJ, et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. De-veloped with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012;33(21):2719-47.
11. Wann LS, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Car-diology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;57(2):223-42.
12. Curtis AB. Practice implications of the atrial fibrillation guide-lines. Am J Cardiol 2013;111(11):1660-70.
13. Prasun MA. Providing best practice in the management of atrial fibrillation in the United States. J Cardiovasc Nurs 2012; 27(5):445-56.
14. Van Gelder IC, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med 2002;347(23):1834-40.
15. Van Gelder IC, et al. Lenient versus strict rate control in pa-tients with atrial fibrillation. N Engl J Med 2010;362(15): 1363-73.
16. Rosanio S, et al. Pharmacology, benefits, unaddressed ques-tions, and pragmatic issues of the newer oral anticoagulants for stroke prophylaxis in non-valvular atrial fibrillation and proposal of a management algorithm. Int J Cardiol 2014; 174(3):471-83.
17. Morton PG, Fontaine DK, eds. Critical care nursing: a holis-tic approach. 9th ed. Philadelphia: Wolters Kluwer/Lippincott Williams and Wilkins; 2009.
18. Huxley RR, et al. Absolute and attributable risks of atrial fi-brillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study. Cir-culation 2011;123(14):1501-8.
19. Healey JS, et al. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med 2012;366(2):120-9.
20. Berra K. Antithrombotics for stroke prevention in non-valvular atrial fibrillation: an update. Eur J Cardiovasc Nurs 2014; 13(1):32-40.
21. Lip GY, et al. Atrial fibrillation. Lancet 2012;379(9816):648-61. 22. Lip GY, et al. Comparative validation of a novel risk score for
predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol 2011;57(2):173-80.
23. Agarwal S, et al. Current trial-associated outcomes with war-farin in prevention of stroke in patients with nonvalvular atrial
fibrillation: a meta-analysis. Arch Intern Med 2012;172(8): 623-31; discussion 631-33.
24. Danelich IM, et al. Clinical update on the management of atrial fibrillation. Pharmacotherapy 2013;33(4):422-46.
25. Verheugt FW. The new oral anticoagulants in atrial fibrilla-tion: an update. Neth Heart J 2013;21(11):480-4.
26. Olshansky B, et al. The Atrial Fibrillation Follow-up Investi-gation of Rhythm Management (AFFIRM) study: approaches to control rate in atrial fibrillation. J Am Coll Cardiol 2004; 43(7):1201-8.
27. Freemantle N, et al. Mixed treatment comparison of drone-darone, amiodarone, sotalol, flecainide, and propafenone for the management of atrial fibrillation. Europace 2011;13(3): 329-45.
28. Field JM, et al. Part 1: executive summary: 2010 American Heart Association guidelines for cardiopulmonary resuscita-tion and emergency cardiovascular care. Circulation 2010; 122(18 Suppl 3):S640-S656.
29. You JJ, et al. Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141(2 Suppl):e531S-e575S.
30. Reddy VY, et al. Percutaneous left atrial appendage closure for stroke prophylaxis in patients with atrial fibrillation: 2.3-year follow-up of the PROTECT AF (Watchman Left Atrial Appendage System for Embolic Protection in Patients with Atrial Fibrillation) trial. Circulation 2013;127(6):720-9.
31. Johnson TW, et al. Atrial fibrillation ablation. Am J Nurs 2011;111(2):58-61.
32. Wokhlu A, et al. Long-term quality of life after ablation of atrial fibrillation: the impact of recurrence, symptom relief, and placebo effect. J Am Coll Cardiol 2010;55(21):2308-16.
33. Kennedy R, Oral H. Catheter ablation of atrial fibrillation in the elderly: does the benefit outweigh the risk? Expert Rev Cardiovasc Ther 2013;11(6):697-704.
34. Shah RU, et al. Procedural complications, rehospitalizations, and repeat procedures after catheter ablation for atrial fibril-lation. J Am Coll Cardiol 2012;59(2):143-9.
35. Edgerton JR, et al. Minimally invasive surgical ablation of atrial fibrillation: six-month results. J Thorac Cardiovasc Surg 2009;138(1):109-13; discussion 114.
36. Benatar D, et al. Outcomes of chronic heart failure. Arch In-tern Med 2003;163(3):347-52.
37. Gillis AM, et al. Treating the right patient at the right time: an innovative approach to the management of atrial fibrilla-tion. Can J Cardiol 2008;24(3):195-8.
38. Hendriks JM, et al. Nurse-led care vs. usual care for patients with atrial fibrillation: results of a randomized trial of inte-grated chronic care vs. routine clinical care in ambulatory pa-tients with atrial fibrillation. Eur Heart J 2012;33(21):2692-9.
39. Hendriks JM, et al. An integrated chronic care program for patients with atrial fibrillation: study protocol and methodol-ogy for an ongoing prospective randomised controlled trial. Int J Nurs Stud 2010;47(10):1310-6.
40. Inglis S, et al. A new solution for an old problem? Effects of a nurse-led, multidisciplinary, home-based intervention on re-admission and mortality in patients with chronic atrial fibril-lation. J Cardiovasc Nurs 2004;19(2):118-27.
41. Cowan MJ, et al. The effect of a multidisciplinary hospitalist/physician and advanced practice nurse collaboration on hos-pital costs. J Nurs Adm 2006;36(2):79-85.
42. Nieuwlaat R, et al. Guideline-adherent antithrombotic treat-ment is associated with improved outcomes compared with undertreatment in high-risk patients with atrial fibrillation. The Euro Heart Survey on Atrial Fibrillation. Am Heart J 2007;153(6):1006-12.
43. Thrall G, et al. Depression, anxiety, and quality of life in pa-tients with atrial fibrillation. Chest 2007;132(4):1259-64.
44. Kul S, et al. Effects of care pathways on the in-hospital treat-ment of heart failure: a systematic review. BMC Cardiovasc Disord 2012;12:81.
45. McCabe PJ. Spheres of clinical nurse specialist practice influ-ence evidence-based care for patients with atrial fibrillation. Clin Nurse Spec 2005;19(6):308-17.