by leah craft, md, and joseph a. prahlow, md fecal...
TRANSCRIPT
A woman in her 70s with diagnoses of Alzhei-mer’s disease, multiinfarct dementia, depres-sion, anxiety, and hypertension arrived at a hospital ED from the nursing home where
she had been a resident for several months. Although her speech was very limited, the nursing home staff had suspected severe abdominal pain and called an ambulance. (This case is based on a real patient; some details have been changed to protect her identity.)
HOURS
Continuing Education2.1
By Leah Craft, MD, and Joseph A. Prahlow, MD
Overview: The authors present the case of
an elderly, nonverbal nursing home resident
with dementia who developed fecal impaction,
despite interventions such as enema. Subse-
quent stercoral perforation of the sigmoid colon
resulted in peritonitis, sepsis, and death. The
authors discuss colon perforation as a result
of fecal impaction, as well as the difficulties of
pain assessment and communication in pa-
tients with dementia.
Keywords: Alzheimer’s disease, colon perfo-
ration, dementia, enema, fecal impaction, pain
assessment, stercoral perforation
A case of constipation in a patient with dementia leads to death.
The notes from the nursing home showed that in previous months the patient’s dementia had progressed, making her incontinent of bowel and bladder and in need of assistance with all activities of daily living. Ac-cording to her last psychiatric evaluation she was “un-able to even complete sentences.” When in pain she would moan and point to the area of her body that was hurting. Among the medications she was taking were escitalopram (Lexapro) and quetiapine (Sero-quel).
Four days before her hospitalization she had fallen and sustained bruises on her face, arms, and sacral re-gion, but had no other acute symptoms. Two days prior to admission she had moaned and pointed to her back when getting up from a chair. The morning of admis-sion she again moaned and pointed to her back, as well as her stomach; she also vomited. A rectal examination at that time revealed soft fecal material, and she yelled when touched. A disposable saline enema (Fleet) was given, during which she moaned and tried to push away the nursing staff. Three hours later she had a small bow el movement, and staff noted that her abdomen was “very hard.” She had no fever, respirations were shal low and rapid, and her blood pressure was 90/60 mmHg. She refused to stand and continued to moan and hold her abdomen. At that time she was trans-ported to the ED for evaluation.
At the ED she was unresponsive except to painful stimuli. She was afebrile, with a heart rate of 117 beats per minute, respiratory rate of 28 breaths per minute, blood pressure of 88/52 mmHg, and an oxygen sat-uration level in the mid-80s on room air. She never regained consciousness and died within an hour. In
38 AJN ▼ August 2011 ▼ Vol. 111, No. 8 ajnonline.com
From Fecal Impaction to Colon Perforation
impaction are the sigmoid and rectosigmoid colon,1, 11 because here much of the water has already been re-absorbed from the feces, which can then develop into hardened masses known as scybala.1 In addition, the distal colon, particularly along the antimesenteric bor-der, has a relatively poor blood supply, making it more susceptible to pressure necrosis from scybala. Finally, because these areas of the colon have the narrowest di-ameter, they allow the formation of higher intralumi-nal pressure in the event of fecal impaction.
Enemas. Cleansing enema–induced perforations are less commonly reported than are iatrogenic perfo-rations from colonoscopy or barium enemas.4 But their true incidence is difficult to establish, in part because nursing home personnel who refer a patient for treat-ment may provide false or misleading information in order to avoid future litigation.12 In one study, of 10 pa tients presenting with perforation after receiving a retrograde irrigation enema at a nursing home, the relevant information linking the enema to the patient’s condition was given for only 20% of patients. For the others, “the information was vague and sometimes misleading.”12 Therefore, when evaluating a nursing home resident with symptoms concordant with per-foration, clinicians should consider the possibility of enema-induced perforation. Requesting copies of re-cent nursing notes may help to address such concerns.
accordance with a do-not-resuscitate order, no resus-citative efforts were performed. Her family requested an autopsy.
WHAT THE AUTOPSY SHOWEDAutopsy revealed a 10-cm rupture on the anterior wall of the mid-to-distal sigmoid colon. The distal sigmoid colon beyond the rupture site and the entire rectum were markedly dilated and impacted with firm feces. Acute peritonitis was identified by both gross and mi-croscopic examination; microscopic assessment also showed necrosis at the site of colon rupture. Gross and microscopic neuropathologic changes associated with Alzheimer’s disease were noted. The cause of death was ruled as acute peritonitis following a ruptured sigmoid colon caused by massive fecal impaction of the recto-sigmoid colon.
COLON PERFORATION Stercoral perforation of the colon is defined as “per-foration of the bowel due to pressure necrosis from fecal masses.”1 A 1996 literature review found only 67 cases of stercoral perforation of the colon since the first reported case in 1894,2 and a more recent paper reported fewer than 90 cases in the literature.3 But the true incidence of stercoral perforation (and colon per-foration in general) may be higher than the reported incidence because while in many cases it may have been the cause of death, an autopsy was never performed to confirm it.
Colon perforation is often fatal.1 Patients usually die of severe peritonitis with resulting sepsis caused by fecal contamination of the peritoneal and extraperi-toneal spaces.4 While diagnosis of colon perforation is sometimes made preoperatively, the exact location and etiology of the perforation are often discovered during either surgery or autopsy.1, 5-8
Two possible causes of colon perforation are fecal impaction and enemas.
Fecal impaction is defined as a “compacted, immov-able mass of feces filling the rectum.”9 It can result in obstipation, the inability to pass stool or gas, but can also present with diarrhea, because liquid stool can pass around the impaction. While a rectal examination may reveal hard stool in the rectal vault, “the absence of stool in the rectum does not rule out fecal impaction.”10 The patient may have had a bowel movement before the ex-amination, and the impacted stool may be higher in the distal colon. In such cases, radiography may be use-ful to differentiate a fecal impaction from other causes of bowel obstruction.10 If untreated, fecal impaction may result in a variety of complications, including ster-coral perforation.
Fecal impaction causes the intraluminal pressure within the colon to increase and exceed the capillary perfusion pressure in the bowel wall, resulting in pres-sure necrosis of the wall and eventually in ulceration and perforation.1, 11 The most common sites of fecal
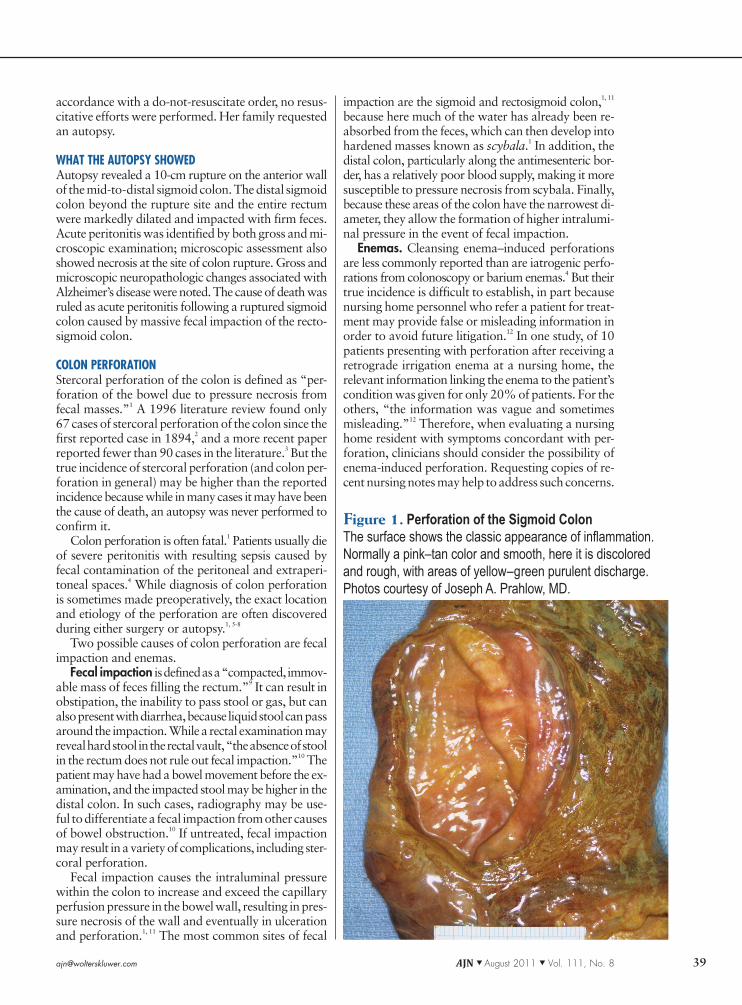
Figure 1. Perforation of the Sigmoid ColonThe surface shows the classic appearance of inflammation. Normally a pink–tan color and smooth, here it is discolored and rough, with areas of yellow–green purulent discharge. Photos courtesy of Joseph A. Prahlow, MD.
[email protected] AJN ▼ August 2011 ▼ Vol. 111, No. 8 39

pain, and fever.16 However, it’s important to note that occasionally patients are asymptomatic.4, 17
Prompt diagnosis and surgical intervention are nec-essary to prevent complications including sepsis and multiorgan failure, as well as death. In one study, pa-tients who received a correct diagnosis within 36 hours of perforation survived regardless of age, prior diseases, or operative findings.12 Diagnosis is usually made after taking a history and conducting a physical examina-tion, but radiology can also be used. Plain X-ray may show free air beneath the diaphragm, although this finding isn’t always present. (Free air refers to air that has escaped from the gastrointestinal tract into the peri-toneal cavity; its presence beneath the diaphragm means that the gastrointestinal tract has been perfo-rated.) Computed tomographic scanning is more sen-sitive than plain radiography in detecting free air and can show extraluminal air in the perirectal fat.4
Perforation caused by a cleansing enema has a much higher mortality rate than does that from a barium en-ema or colonoscopy, perhaps because with a barium enema or colonoscopy the colon has been medically prepared, resulting in less fecal contamination when perforation occurs.4
Nurses can play a major role in helping to prevent rectal and colon trauma and perforation caused by enemas. Prior to administration of the enema, it’s im-portant to be aware of any perianal pathology such as fissures or hemorrhoids that can make the procedure more challenging.18 Nurses should also be aware of any colonic pathology such as ulcerative colitis that can in-crease the risk of complications.
After the nozzle has been inserted into the rectum, it should be pointed slightly posteriorly to keep the tip in the middle of the bowel lumen, thus avoiding trauma to the anterior rectal wall.19 It’s also important to pay attention to the patient’s complaints. Discomfort is normal, but pain isn’t. If a patient complains of pain,
it’s best to stop the enema and try again. After admin-istration, any complaints of abdominal pain, rectal pain, or rectal bleeding must be promptly and thor-oughly evaluated.
CHRONIC CONSTIPATIONOne of the most common causes of stercoral colon perforation is chronic constipation, a condition often present in the elderly; its incidence increases on acute geriatric units and in long-term care facilities.20
Enema administration can injure even healthy tissue, particularly the anterior wall of the rectum.13 Because the rectum is insensitive to pain above the dentate line, this area is easily traumatized.14 The patient may not feel any pain until the perforation has occurred and
fecal contents have begun irritating the pain-sensitive peritoneal or perirectal spaces. The enema device itself may cause damage, as can a sudden increase in hydro-static pressure.12 Another possible culprit is chemical irritation or injury, which can result in anaphylaxis, peritonitis, rectal gangrene, or acute colitis.15
Acute abdominal pain, the most common symptom of enema-induced perforation, usually appears soon after the procedure but can occur up to 72 hours later.4 Other symptoms include rectal pain and bleeding, back
40 AJN ▼ August 2011 ▼ Vol. 111, No. 8 ajnonline.com
Prior to administration of the enema, it’s important to be
aware of any perianal pathology such as fissures or
hemorrhoids that can make the procedure more challenging.
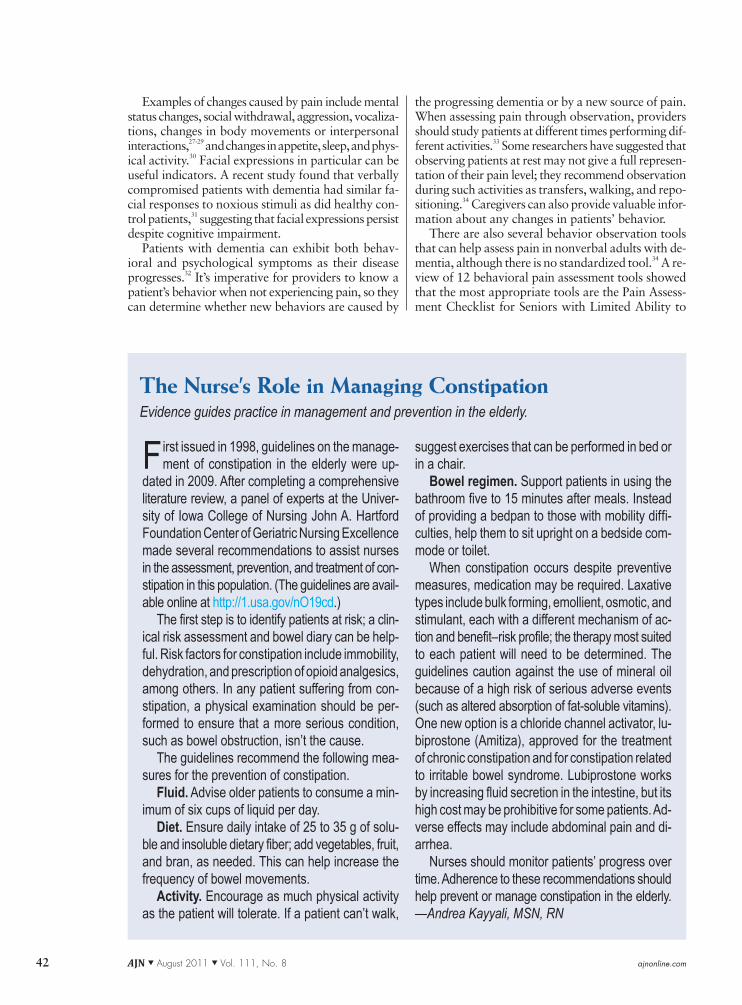
Figure 2. Autopsy Photograph of the Peritoneal CavityThe photograph reveals markedly discolored and feces-stained small and large intestines, indicative of a bowel perforation and associated inflammation (peritonitis).
ignore the urge to defecate, thus increasing the likeli-hood of fecal impaction.10 Immobility, common in this population, also leads to constipation. And patients with dementia are often unaware they have constipa-tion, or if aware, they’re unable to adequately commu-nicate their pain and discomfort to caregivers.
Evaluating pain in patients with dementia. Self- reports have long been considered the gold standard in pain assessment, but they can be difficult for pa-tients who can’t speak and for those with advanced dementia.
The American Geriatrics Society (AGS) recom-mends that pain assessment in patients with mild-to-moderate dementia be attempted by directly asking about pain.25 Providers need to be patient when asking questions, use a variety of terms to describe pain, repeat questions, give patients enough time to respond, and use the present tense.26 In patients with moderate-to-severe dementia or those who are nonverbal, the AGS recommends that pain be assessed by noting changes in behavior through direct observation or by obtain-ing a history from caregivers.25
The best way to prevent stercoral perforation is to prevent constipation. Nurses and physicians need to be aware of how often patients are having bowel move-ments and do what they can to prevent constipation from occurring. While some patients have idiopathic constipation, many others suffer from iatrogenic con-stipation as an adverse effect of medications, includ-ing opioid analgesics, antidepressants, aluminum-based antacids, calcium carbonate, nonsteroidal antiinflam-matory drugs, steroids, anticholinergics, calcium chan-nel blockers, antihypertensives, pseudoephedrine, and iron. These patients may benefit from a stool softener (at the least) and close monitoring of bowel habits. (For a list of medications that treat constipation, see Table 1.21-24)
AN ADDED CHALLENGE: DEMENTIA People with cognitive impairment have an increased risk of fecal impaction and stercoral perforation. They are more likely to develop chronic constipation because they have a decreased awareness of thirst. In addition, their cognitive disabilities may cause them to regularly
[email protected] AJN ▼ August 2011 ▼ Vol. 111, No. 8 41
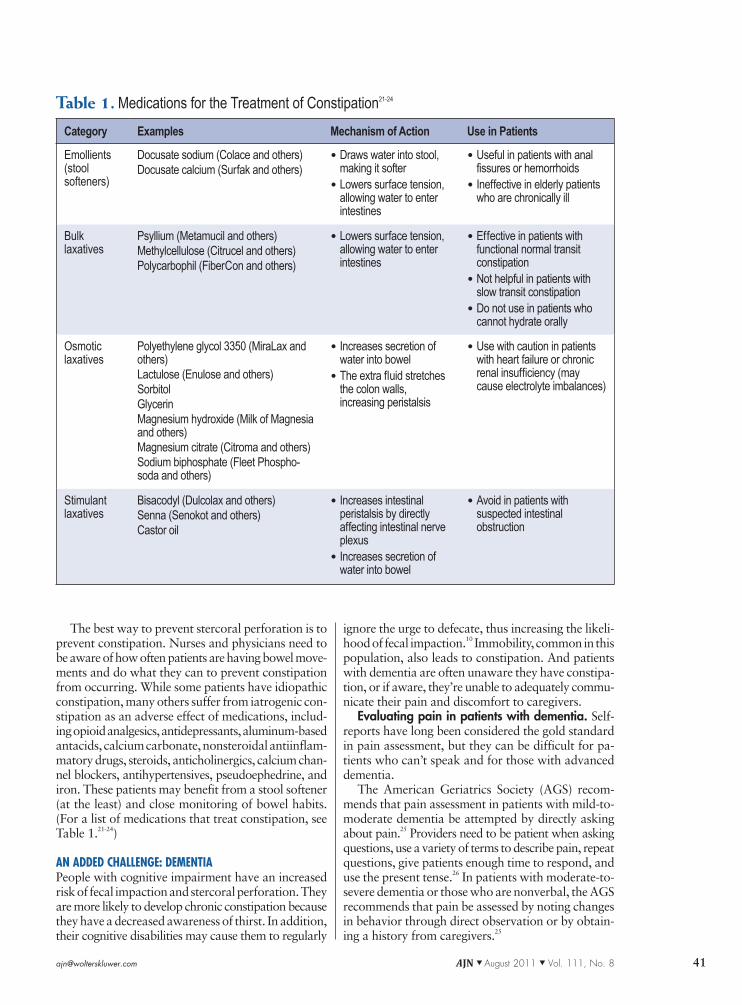
Table 1. Medications for the Treatment of Constipation21-24
Category Examples Mechanism of Action Use in Patients
Emollients (stool softeners)
Docusate sodium (Colace and others) Docusate calcium (Surfak and others)
• Draws water into stool, making it softer
• Lowers surface tension, allowing water to enter intestines
• Useful in patients with anal fissures or hemorrhoids
• Ineffective in elderly patients who are chronically ill
Bulk laxatives
Psyllium (Metamucil and others)Methylcellulose (Citrucel and others)Polycarbophil (FiberCon and others)
• Lowers surface tension, allowing water to enter intestines
• Effective in patients with functional normal transit constipation
• Not helpful in patients with slow transit constipation
• Do not use in patients who cannot hydrate orally
Osmotic laxatives
Polyethylene glycol 3350 (MiraLax and others)Lactulose (Enulose and others) SorbitolGlycerinMagnesium hydroxide (Milk of Magnesia and others)Magnesium citrate (Citroma and others) Sodium biphosphate (Fleet Phospho-soda and others)
• Increases secretion of water into bowel
• The extra fluid stretches the colon walls, increasing peristalsis
• Use with caution in patients with heart failure or chronic renal insufficiency (may cause electrolyte imbalances)
Stimulant laxatives
Bisacodyl (Dulcolax and others)Senna (Senokot and others)Castor oil
• Increases intestinal peristalsis by directly affecting intestinal nerve plexus
• Increases secretion of water into bowel
• Avoid in patients with suspected intestinal obstruction
the progressing dementia or by a new source of pain. When assessing pain through observation, providers should study patients at different times performing dif-ferent activities.33 Some researchers have suggested that observing patients at rest may not give a full represen-tation of their pain level; they recommend observation during such activities as transfers, walking, and repo-sitioning.34 Caregivers can also provide valuable infor-mation about any changes in patients’ behavior.
There are also several behavior observation tools that can help assess pain in nonverbal adults with de-mentia, although there is no standardized tool.34 A re-view of 12 behavioral pain assessment tools showed that the most appropriate tools are the Pain Assess-ment Checklist for Seniors with Limited Ability to
Examples of changes caused by pain include mental status changes, social withdrawal, aggression, vocaliza-tions, changes in body movements or interpersonal interactions,27-29 and changes in appetite, sleep, and phys-ical activity.30 Facial expressions in particular can be useful indicators. A recent study found that verbally compromised patients with dementia had similar fa-cial responses to noxious stimuli as did healthy con-trol patients,31 suggesting that facial expressions persist despite cognitive impairment.
Patients with dementia can exhibit both behav-ioral and psychological symptoms as their disease progresses.32 It’s imperative for providers to know a patient’s behavior when not experiencing pain, so they can determine whether new behaviors are caused by
42 AJN ▼ August 2011 ▼ Vol. 111, No. 8 ajnonline.com
First issued in 1998, guidelines on the manage-ment of constipation in the elderly were up-
dated in 2009. After completing a comprehensive literature review, a panel of experts at the Univer-sity of Iowa College of Nursing John A. Hartford Foundation Center of Geriatric Nursing Excellence made several recommendations to assist nurses in the assessment, prevention, and treatment of con-stipation in this population. (The guidelines are avail-able online at http://1.usa.gov/nO19cd.)
The first step is to identify patients at risk; a clin-ical risk assessment and bowel diary can be help-ful. Risk factors for constipation include immobility, dehydration, and prescription of opioid analgesics, among others. In any patient suffering from con-stipation, a physical examination should be per-formed to ensure that a more serious condition, such as bowel obstruction, isn’t the cause.
The guidelines recommend the following mea-sures for the prevention of constipation.
Fluid. Advise older patients to consume a min-imum of six cups of liquid per day.
Diet. Ensure daily intake of 25 to 35 g of solu-ble and insoluble dietary fiber; add vegetables, fruit, and bran, as needed. This can help increase the frequency of bowel movements.
Activity. Encourage as much physical activity as the patient will tolerate. If a patient can’t walk,
suggest exercises that can be performed in bed or in a chair.
Bowel regimen. Support patients in using the bathroom five to 15 minutes after meals. Instead of providing a bedpan to those with mobility diffi-culties, help them to sit upright on a bedside com-mode or toilet.
When constipation occurs despite preventive measures, medication may be required. Laxative types include bulk forming, emollient, osmotic, and stimulant, each with a different mechanism of ac-tion and benefit–risk profile; the therapy most suited to each patient will need to be determined. The guidelines caution against the use of mineral oil because of a high risk of serious adverse events (such as altered absorption of fat-soluble vitamins). One new option is a chloride channel activator, lu-biprostone (Amitiza), approved for the treatment of chronic constipation and for constipation related to irritable bowel syndrome. Lubiprostone works by increasing fluid secretion in the intestine, but its high cost may be prohibitive for some patients. Ad-verse effects may include abdominal pain and di-arrhea.
Nurses should monitor patients’ progress over time. Adherence to these recommendations should help prevent or manage constipation in the elderly. —Andrea Kayyali, MSN, RN
The Nurse’s Role in Managing ConstipationEvidence guides practice in management and prevention in the elderly.

7. Heffernan C, et al. Stercoral colitis leading to fatal peritonitis: CT findings. AJR Am J Roentgenol 2005;184(4):1189-93.
8. Murakami S, et al. Stercoraceous perforation of the sigmoid colon: report of two cases. Surg Today 1992;22(5):461-3.
9. Annells M, Koch T. Faecal impaction: older people’s experi-ences and nursing practice. Br J Community Nurs 2002;7(3):118-26.
10. Wright BA, Staats DO. The geriatric implications of fecal impaction. Nurse Pract 1986;11(10):53-66.
11. Haddad R, et al. Stercoral perforation of the sigmoid colon. ANZ J Surg 2005;75(4):244-6.
12. Paran H, et al. Enema-induced perforation of the rectum in chronically constipated patients. Dis Colon Rectum 1999;42(12):1609-12.
13. Fielding JF, Lumsden K. Large-bowel perforations in patients undergoing sigmoidoscopy and barium enema. Br Med J 1973;1(5851):471-3.
14. de Feiter PW, et al. Rectal perforations after barium enema: a review. Dis Colon Rectum 2006;49(2):261-71.
15. Pietsch JB, et al. Injury by hypertonic phosphate enema. Can Med Assoc J 1977;116(10):1169-70.
16. Bobba RK, Arsura EL. Septic shock in an elderly patient on dialysis: enema-induced rectal injury confusing the clinical picture. J Am Geriatr Soc 2004;52(12):2144.
17. Gedebou TM, et al. Clinical presentation and management of iatrogenic colon perforations. Am J Surg 1996;172(5):454-8.
18. Saltzstein RJ, et al. Anorectal injuries incident to enema ad-ministration. A recurring avoidable problem. Am J Phys Med Rehabil 1988;67(4):186-8.
19. Tanswell IJ, et al. Rectal perforation in ulcerative colitis: com-plication of an enema tip. Gastrointest Endosc. 2009;69(2):344.
20. De Lillo AR, Rose S. Functional bowel disorders in the geri-atric patient: constipation, fecal impaction, and fecal inconti-nence. Am J Gastroenterol 2000;95(4):901-5.
21. Hsieh C. Treatment of constipation in older adults. Am Fam Physician 2005;72(11):2277-84.
22. Bosshard W, et al. The treatment of chronic constipation in elderly people: an update. Drugs Aging 2004;21(14):911-30.
23. Spinzi GC. Bowel care in the elderly. Dig Dis 2007;25(2):160-5.
24. Venable SJ. Gastrointestinal system drugs. In: Aschenbrenner DS, Venable SJ, editors. Drug therapy in nursing. 3rd ed. Phil-adelphia: Lippincott Williams and Wilkins; 2009. p. 991-1050.
25. AGS Panel on Persistent Pain in Older Persons. The manage-ment of persistent pain in older persons. J Am Geriatr Soc 2002;50(6 Suppl):S205-S224.
26. Tsai PF, Chang JY. Assessment of pain in elders with demen-tia. Medsurg Nurs 2004;13(6):364-9, 390.
27. Molony SL, et al. Assessing pain as a fifth vital sign in long-term care facilities: recommendations from the field. J Geron-tol Nurs 2005;31(3):16-24.
28. Davies E, et al. Pain assessment and cognitive impairment: part 1. Nurs Stand 2004;19(12):39-42.
29. Murdoch J, Larsen D. Assessing pain in cognitively impaired older adults. Nurs Stand 2004;18(38):33-9.
30. Zwakhalen SM, et al. Pain in elderly people with severe de-mentia: a systematic review of behavioural pain assessment tools. BMC Geriatr 2006;6:3.
31. Kunz M, et al. The facial expression of pain in patients with dementia. Pain 2007;133(1-3):221-8.
32. Boustani M, et al. Characteristics associated with behavioral symptoms related to dementia in long-term care residents. Gerontologist 2005;45 Spec No 1(1):56-61.
33. Wheeler MS. Pain assessment and management in the pa-tient with mild to moderate cognitive impairment. Home Healthc Nurse 2006;24(6):354-9.
34. Herr K, et al. Tools for assessment of pain in nonverbal older adults with dementia: a state-of-the-science review. J Pain Symptom Manage 2006;31(2):170-92.
Commu nicate (PACSLAC, which helps detect subtle changes in behavior) and Doloplus-2 (which has the most clinical utility).30 Another useful tool is the Pain Assessment in Advanced Dementia (PAINAD) scale.30 (See “Pain Assessment in People with Dementia,” July 2008, for more on the use of pain scales in this pop-ulation.)
COULD THIS DEATH HAVE BEEN PREVENTED?If the nursing home staff had recognized that the pa-tient’s changes in behavior—her increased moaning and pointing to her back—were caused by pain, and if they’d been aware that constipation was a possibil-ity, they might have referred her to the hospital sooner and she might still be alive today.
What about the enema she received in the nursing home on the morning of her admission to the ED? Had that played a role? Hydrostatic pressure changes that occur with enema administration may have in-creased the intraluminal pressure enough to perforate the bowel wall. But since the perforation was sigmoid and not rectal, and since the bowel distal to the sig-moid perforation was impacted with feces, it’s un-likely that the enema tip caused the perforation. In addition, perforation would most likely not have oc-curred if the massive fecal impaction had not already caused pressure necrosis of the bowel wall. There-fore, even though the cleansing enema may have con-tributed to the perforation, the massive fecal impaction and stercoral ulceration were the primary causes. ▼
Leah Craft is a resident in family medicine at the Memorial Hos-pital of South Bend, South Bend, IN. Joseph A. Prahlow is a pa-thology professor at Indiana University School of Medicine on the South Bend campus and a forensic pathologist at the South Bend Medical Foundation. Contact author: Leah Craft, [email protected]. The authors have disclosed no significant ties, fi-nancial or otherwise, to any company that might have an interest in the publication of this educational activity.
REFERENCES
1. Serpell JW, Nicholls RJ. Stercoral perforation of the colon. Br J Surg 1990;77(12):1325-9.
2. Dubinsky I. Stercoral perforation of the colon: case report and review of the literature. J Emerg Med 1996;14(3):323-5.
3. Patel VG, et al. Stercoral perforation of the sigmoid colon: report of a rare case and its possible association with non-steroidal anti-inflammatory drugs. Am Surg 2002;68(1):62-4.
4. Gayer G, et al. Perforations of the rectosigmoid colon induced by cleansing enema: CT findings in 14 patients. Abdom Im-aging 2002;27(4):453-7.
5. Yano T, et al. A stercoral perforation of the colon with an obvious faecal mass diagnosed by computed tomography. ANZ J Surg 2008;78(3):214-5.
6. Hecht PG, et al. Fatal fecaloma. N Y State J Med 1976;76(2):264-7.
[email protected] AJN ▼ August 2011 ▼ Vol. 111, No. 8 43
For more than 70 additional articles on geriatric topics, go to www.nursingcenter.com/ce.