best practices for the management of foot ulcers in people...
TRANSCRIPT
Best Practices for the Management of FootUlcers in People with Diabetes
C M E1 AMA PRACategory 1 CreditTM
ANCC3.0 Contact Hours
Kevin Y. Woo, PhD, RN & Assistant Professor & School of Nursing Queen’s University & Kingston, Ontario, Canada & WoundCare Consultant &West Park Health Centre & Toronto, Ontario, Canada &Web Clinical Editor & Advances in Skin &Wound Care
Mariam Botros, DCh & Chiropodist & Women’s College Hospital & Toronto, Ontario, Canada
Janet Kuhnke, RN, MSc ET & PhD Student & University of Ottawa & Ottawa, Ontario, Canada
Robyn Evans, MD, MSc & Director of Wound Clinic & Women’s College Hospital & Toronto, Ontario, Canada
Afsaneh Alavi, MD & Lecturer & Toronto Dermatology Clinic & Toronto, Ontario, Canada
All faculty, staff, and planners, including spouses/partners (if any), in any position to control the content of this CME activity have disclosed that they have no financial relationships with, orfinancial interests in, any commercial companies pertaining to this educational activity.
To earn CME credit, you must read the CME article and complete the quiz and evaluation on the enclosed answer form, answering at least 13 of the 18 questions correctly.
This continuing educational activity will expire for physicians on November 30, 2014.
PURPOSE:
To enhance the learner’s competence with information about best practices in management of foot ulcers in people
with diabetes.
TARGET AUDIENCE:
This continuing education activity is intended for physicians and nurses with an interest in skin and wound care.
OBJECTIVES:
After participating in this educational activity, the participant should be better able to:
1. Identify assessment parameters to discern causes and risk factors for foot ulcers.
2. Apply evidence-based practices to case scenarios for the prevention and management of diabetic foot ulcers.
NOVEMBER 2013
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 512 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

ABSTRACT
The care of persons with diabetic foot ulcers requires asystematic approach following the wound bed preparationparadigm and the existing best practice recommendations. Thepurpose of this article is to summarize key evidence andrecommendations regarding prevention and management ofdiabetic foot ulcers that can be translated into practice.KEYWORDS: diabetic foot ulcer, evidence-based practice
ADV SKIN WOUND CARE 2013;26:512-24, quiz 525-6.
Diabetes is one of the leading chronic diseases that has
become an epidemic worldwide.1 According to the Inter-
nationalDiabetes Federation, the global number of people
with diabetes will increase from 246 million or 5.9% in 2007 to
380millionor 7.1%by2025.1Ofpersonswithdiabetes (PWDs), 2%
to 3%will develop a foot ulcer annually, whereas the lifetime risk of
developing a foot ulcer is as high as 25%, primarily because of
neuropathy and potential coexisting vascular disease.2 Following
patients with diabetes and neuropathy for 1 year, it was estimated
that 7.2% of this population would develop their first foot ulcer.3
More than 80% of all nontraumatic amputations in diabetes are
preceded by foot ulcers that should be considered as one of the
prognostic indicators for advanced diabetes.4 In most countries,
the healthcare system costs of diabetic foot ulcers are exorbitant
and include a high likelihood of hospitalizations. In the United
States, the care of diabetes-related foot ulcers constitutes 25% to
50% of the total costs associated with diabetic care.1 Despite
these staggering statistics, foot ulcers and related adverse sequelae
in PWDs are deemed highly preventable.5
For optimal patient outcomes, the care of people with diabetic
foot ulcers requires a systematic approach following the wound
bed preparation paradigm and the existing best practice rec-
ommendations.6–9 Integral to the recommended best practices is
the primary emphasis on addressing patient concerns and the
causative factors prior to instituting local wound care. Foot ulcers
are often precipitated by neuropathy and complicated by vas-
cular insufficiency that necessitates thorough evaluation and
specific intervention to promote healing. Local wound care of
wounds with healing potential usually involves 3 core compo-
nents:Debridement of nonviable tissue, Infection management,
and Moisture balance (DIM).10 By applying the principles to
optimal wound healing, it has been demonstrated that 50%
surface area reduction at week 4 is predictive of complete wound
closure at week 12.11 If the wound is not healing at the expected
rate, advanced therapies may be considered. If the wound cause
cannot be corrected, compromisinghealingpotential, localwound
care should focus onmaintenance to prevent secondary infection
and further deterioration.10 This article summarizes key evidence
and recommendations regarding theprevention andmanagement
of diabetic foot ulcers that clinicians can translate into practice.
RECOMMENDATIONS FOR THEPREVENTION AND MANAGEMENT OFDIABETIC FOOT ULCERS
1. Evaluate diabetes management and conduct a systematic
assessment of the PWD including A1c, blood pressure,
cholesterol, diet, exercise, and smoking history.
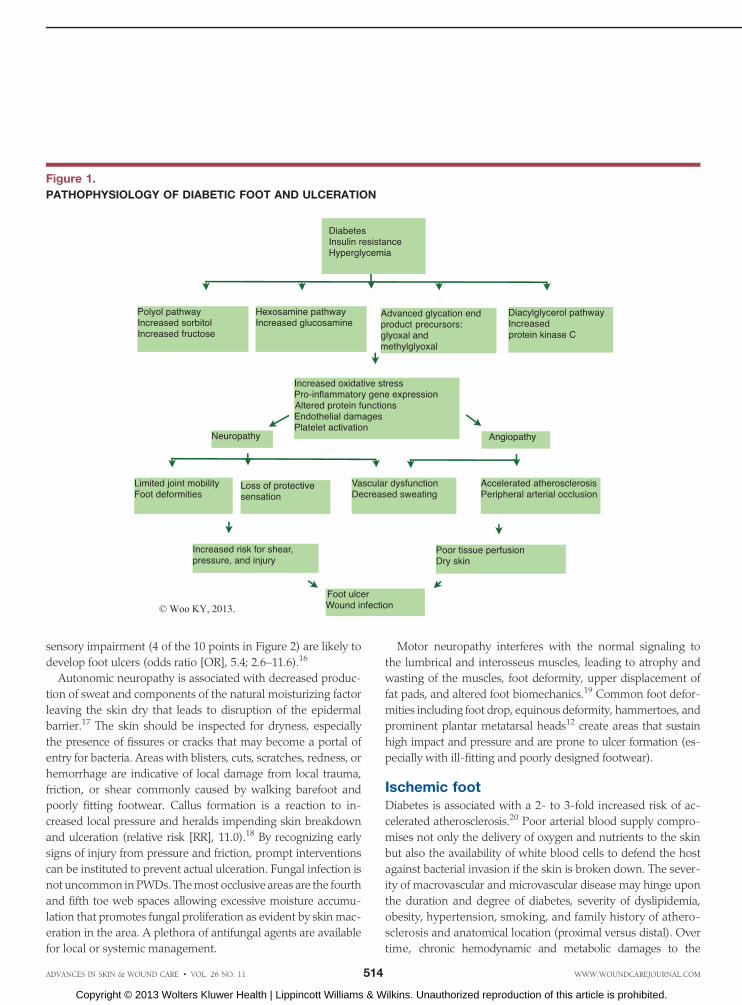
Inadequate management of diabetes can put individuals at
risk for a number of serious complications including foot ul-
ceration. Hyperglycemia triggers a constellation of metabolic
events leading to excessive production of advanced glycation
end-products and overproduction of oxygen free radicals that
can delay healing of foot ulcers12 (Figure 1).
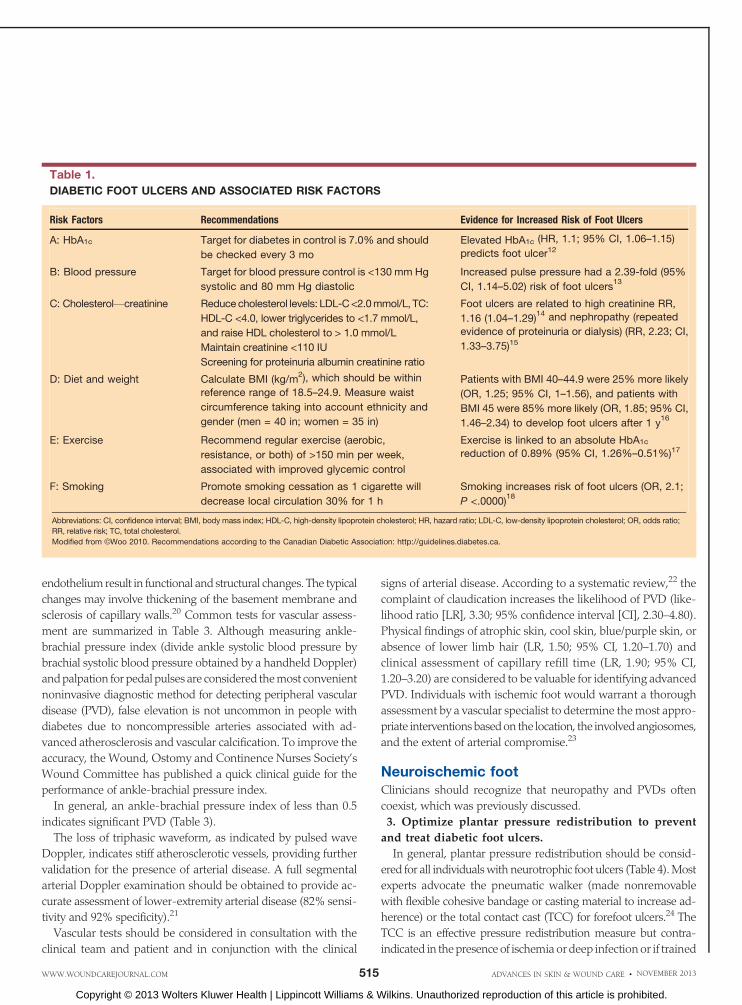
Recognizing the multifaceted nature of diabetes management
and risk factors for foot ulcers,12 several salient factors should
always be part of a careful patient history, and their associated
risks for foot ulceration are summarized in Table 1. Practitioners
may consider close monitoring, early referral to specialists, and
intensive treatment based on the risk profile.
2. Conduct a lower-leg and foot assessment to differentiate
neuropathic, neuroischemic, and ischemic diseases (ulcers).
A thorough foot examination should be conducted at least
on an annual basis to identify risk factors that can lead to foot
ulcers in order to institute early intervention. Only half of the
individuals with diabetes, however, receive routine foot exam-
inations by their healthcare providers.13 To help identify the key
and relevant risk factors, Inlow et al14 developed a 60-second
diabetic foot screening tool that allows clinicians to quickly assess
for skin, nail, foot deformity, footwear, temperature (hot and
cold), range ofmotion, loss of sensation, pedal pulses, dependent
rubor, and erythema. The key elements and supporting evidence
are summarized in Table 2. The interrater reliability of Inlow’s
60-second foot screening tool has been supported by high
intraclass correlation coefficients ranged from0.83 to 0.93.15 There
is a need to explore if the PWD understands the implications of
various risk factors and the importance of self-care practices in
diabetic foot ulcer prevention.
Neuropathic FootDiabetic neuropathy is present in almost 60%of diabetic patients
with foot ulcers5; associated nerve dysfunctionmay be described
as sensory, autonomic, ormotor. Sensory neuropathy removes the
protective sensation rendering the individual to be less aware of
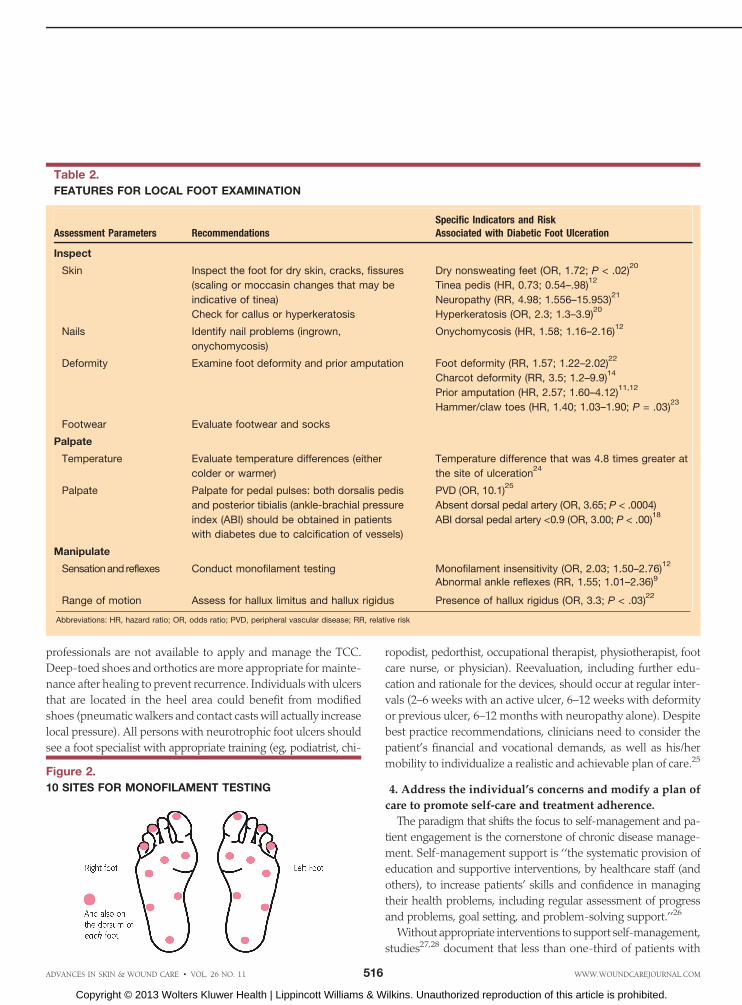
potential or actual trauma to his or her skin. To screen for indi-
vidualswith sensoryneuropathy, the 5.07 (10 g) Semmes-Weinstein
monofilament test is recommended. Individuals with significant
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013513WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
sensory impairment (4 of the 10 points in Figure 2) are likely to
develop foot ulcers (odds ratio [OR], 5.4; 2.6–11.6).16
Autonomic neuropathy is associated with decreased produc-
tion of sweat and components of the natural moisturizing factor
leaving the skin dry that leads to disruption of the epidermal
barrier.17 The skin should be inspected for dryness, especially
the presence of fissures or cracks that may become a portal of
entry for bacteria. Areas with blisters, cuts, scratches, redness, or
hemorrhage are indicative of local damage from local trauma,
friction, or shear commonly caused by walking barefoot and
poorly fitting footwear. Callus formation is a reaction to in-
creased local pressure and heralds impending skin breakdown
and ulceration (relative risk [RR], 11.0).18 By recognizing early
signs of injury from pressure and friction, prompt interventions
can be instituted to prevent actual ulceration. Fungal infection is
not uncommon inPWDs. Themost occlusive areas are the fourth
and fifth toe web spaces allowing excessive moisture accumu-
lation that promotes fungal proliferation as evident by skin mac-
eration in the area. A plethora of antifungal agents are available
for local or systemic management.
Motor neuropathy interferes with the normal signaling to
the lumbrical and interosseus muscles, leading to atrophy and
wasting of the muscles, foot deformity, upper displacement of
fat pads, and altered foot biomechanics.19 Common foot defor-
mities including foot drop, equinous deformity, hammertoes, and
prominent plantar metatarsal heads12 create areas that sustain
high impact and pressure and are prone to ulcer formation (es-
pecially with ill-fitting and poorly designed footwear).
Ischemic footDiabetes is associated with a 2- to 3-fold increased risk of ac-
celerated atherosclerosis.20 Poor arterial blood supply compro-
mises not only the delivery of oxygen and nutrients to the skin
but also the availability of white blood cells to defend the host
against bacterial invasion if the skin is broken down. The sever-
ity of macrovascular and microvascular disease may hinge upon
the duration and degree of diabetes, severity of dyslipidemia,
obesity, hypertension, smoking, and family history of athero-
sclerosis and anatomical location (proximal versus distal). Over
time, chronic hemodynamic and metabolic damages to the
Figure 1.
PATHOPHYSIOLOGY OF DIABETIC FOOT AND ULCERATION
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 514 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
endothelium result in functional and structural changes. The typical
changes may involve thickening of the basement membrane and
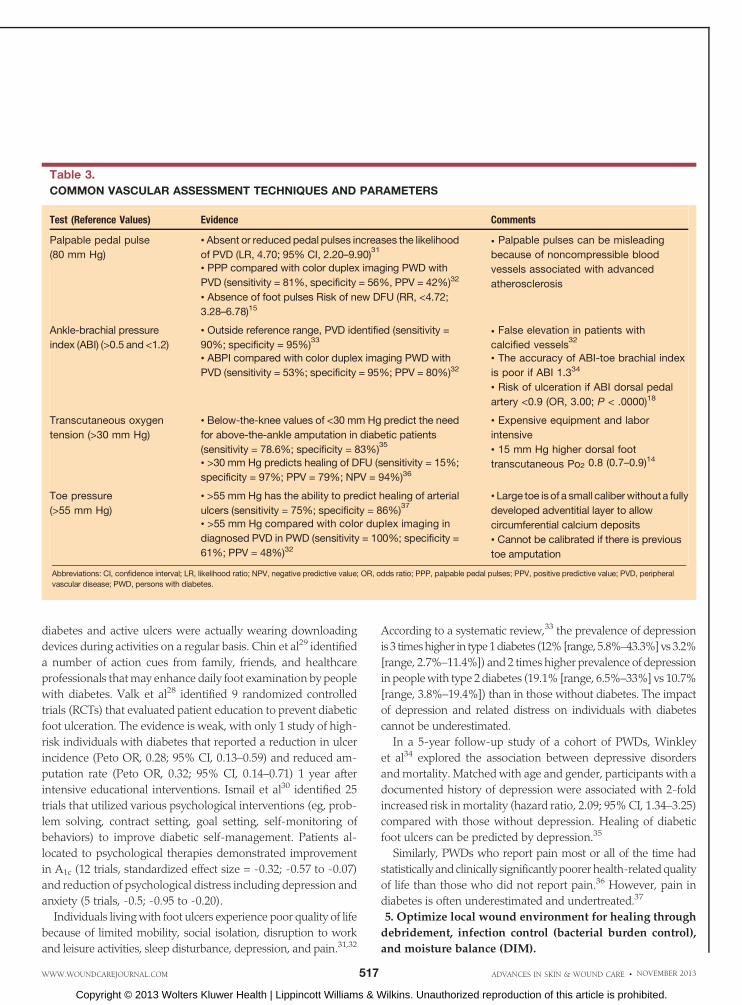
sclerosis of capillary walls.20 Common tests for vascular assess-
ment are summarized in Table 3. Although measuring ankle-
brachial pressure index (divide ankle systolic blood pressure by
brachial systolic blood pressure obtained by a handheld Doppler)
andpalpation for pedal pulses are considered themost convenient
noninvasive diagnostic method for detecting peripheral vascular
disease (PVD), false elevation is not uncommon in people with
diabetes due to noncompressible arteries associated with ad-
vanced atherosclerosis and vascular calcification. To improve the
accuracy, the Wound, Ostomy and Continence Nurses Society’s
Wound Committee has published a quick clinical guide for the
performance of ankle-brachial pressure index.
In general, an ankle-brachial pressure index of less than 0.5
indicates significant PVD (Table 3).
The loss of triphasic waveform, as indicated by pulsed wave
Doppler, indicates stiff atherosclerotic vessels, providing further
validation for the presence of arterial disease. A full segmental
arterial Doppler examination should be obtained to provide ac-
curate assessment of lower-extremity arterial disease (82% sensi-
tivity and 92% specificity).21
Vascular tests should be considered in consultation with the
clinical team and patient and in conjunction with the clinical
signs of arterial disease. According to a systematic review,22 the
complaint of claudication increases the likelihood of PVD (like-
lihood ratio [LR], 3.30; 95% confidence interval [CI], 2.30–4.80).
Physical findings of atrophic skin, cool skin, blue/purple skin, or
absence of lower limb hair (LR, 1.50; 95% CI, 1.20–1.70) and
clinical assessment of capillary refill time (LR, 1.90; 95% CI,
1.20–3.20) are considered to be valuable for identifying advanced
PVD. Individuals with ischemic foot would warrant a thorough
assessment by a vascular specialist to determine themost appro-
priate interventionsbasedon the location, the involvedangiosomes,
and the extent of arterial compromise.23
Neuroischemic footClinicians should recognize that neuropathy and PVDs often
coexist, which was previously discussed.
3. Optimize plantar pressure redistribution to prevent
and treat diabetic foot ulcers.
In general, plantar pressure redistribution should be consid-
ered for all individualswith neurotrophic foot ulcers (Table 4).Most
experts advocate the pneumatic walker (made nonremovable
with flexible cohesive bandage or casting material to increase ad-
herence) or the total contact cast (TCC) for forefoot ulcers.24 The
TCC is an effective pressure redistribution measure but contra-
indicated in thepresenceof ischemia or deep infectionor if trained
Table 1.
DIABETIC FOOT ULCERS AND ASSOCIATED RISK FACTORS
Risk Factors Recommendations Evidence for Increased Risk of Foot Ulcers
A: HbA1c Target for diabetes in control is 7.0% and should
be checked every 3 mo
Elevated HbA1c (HR, 1.1; 95% CI, 1.06–1.15)
predicts foot ulcer12
B: Blood pressure Target for blood pressure control is <130 mm Hg
systolic and 80 mm Hg diastolic
Increased pulse pressure had a 2.39-fold (95%
CI, 1.14–5.02) risk of foot ulcers13
C: CholesterolVcreatinine Reducecholesterol levels: LDL-C<2.0mmol/L, TC:
HDL-C <4.0, lower triglycerides to <1.7 mmol/L,
and raise HDL cholesterol to > 1.0 mmol/L
Maintain creatinine <110 IU
Screening for proteinuria albumin creatinine ratio
Foot ulcers are related to high creatinine RR,
1.16 (1.04–1.29)14 and nephropathy (repeated
evidence of proteinuria or dialysis) (RR, 2.23; CI,
1.33–3.75)15
D: Diet and weight Calculate BMI (kg/m2), which should be within
reference range of 18.5–24.9. Measure waist
circumference taking into account ethnicity and
gender (men = 40 in; women = 35 in)
Patients with BMI 40–44.9 were 25% more likely
(OR, 1.25; 95% CI, 1–1.56), and patients with
BMI 45 were 85%more likely (OR, 1.85; 95% CI,
1.46–2.34) to develop foot ulcers after 1 y16
E: Exercise Recommend regular exercise (aerobic,
resistance, or both) of >150 min per week,
associated with improved glycemic control
Exercise is linked to an absolute HbA1c
reduction of 0.89% (95% CI, 1.26%–0.51%)17
F: Smoking Promote smoking cessation as 1 cigarette will
decrease local circulation 30% for 1 h
Smoking increases risk of foot ulcers (OR, 2.1;
P <.0000)18
Abbreviations: CI, confidence interval; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio;
RR, relative risk; TC, total cholesterol.
Modified from BWoo 2010. Recommendations according to the Canadian Diabetic Association: http://guidelines.diabetes.ca.
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013515WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
professionals are not available to apply and manage the TCC.
Deep-toed shoes and orthotics aremore appropriate for mainte-
nance after healing to prevent recurrence. Individuals with ulcers
that are located in the heel area could benefit from modified
shoes (pneumatic walkers and contact casts will actually increase
local pressure). All persons with neurotrophic foot ulcers should
see a foot specialist with appropriate training (eg, podiatrist, chi-
ropodist, pedorthist, occupational therapist, physiotherapist, foot
care nurse, or physician). Reevaluation, including further edu-
cation and rationale for the devices, should occur at regular inter-
vals (2–6 weeks with an active ulcer, 6–12 weeks with deformity
or previous ulcer, 6–12 months with neuropathy alone). Despite
best practice recommendations, clinicians need to consider the
patient’s financial and vocational demands, as well as his/her
mobility to individualize a realistic and achievable plan of care.25
4. Address the individual’s concerns and modify a plan of
care to promote self-care and treatment adherence.
The paradigm that shifts the focus to self-management and pa-
tient engagement is the cornerstone of chronic disease manage-
ment. Self-management support is ‘‘the systematic provision of
education and supportive interventions, by healthcare staff (and
others), to increase patients’ skills and confidence in managing
their health problems, including regular assessment of progress
and problems, goal setting, and problem-solving support.’’26
Without appropriate interventions to support self-management,
studies27,28 document that less than one-third of patients with
Table 2.
FEATURES FOR LOCAL FOOT EXAMINATION
Assessment Parameters RecommendationsSpecific Indicators and RiskAssociated with Diabetic Foot Ulceration
Inspect
Skin Inspect the foot for dry skin, cracks, fissures
(scaling or moccasin changes that may be
indicative of tinea)
Check for callus or hyperkeratosis
Dry nonsweating feet (OR, 1.72; P < .02)20
Tinea pedis (HR, 0.73; 0.54–.98)12
Neuropathy (RR, 4.98; 1.556–15.953)21
Hyperkeratosis (OR, 2.3; 1.3–3.9)20
Nails Identify nail problems (ingrown,
onychomycosis)
Onychomycosis (HR, 1.58; 1.16–2.16)12
Deformity Examine foot deformity and prior amputation Foot deformity (RR, 1.57; 1.22–2.02)22
Charcot deformity (RR, 3.5; 1.2–9.9)14
Prior amputation (HR, 2.57; 1.60–4.12)11,12
Hammer/claw toes (HR, 1.40; 1.03–1.90; P = .03)23
Footwear Evaluate footwear and socks
Palpate
Temperature Evaluate temperature differences (either
colder or warmer)
Temperature difference that was 4.8 times greater at
the site of ulceration24
Palpate Palpate for pedal pulses: both dorsalis pedis
and posterior tibialis (ankle-brachial pressure
index (ABI) should be obtained in patients
with diabetes due to calcification of vessels)
PVD (OR, 10.1)25
Absent dorsal pedal artery (OR, 3.65; P < .0004)
ABI dorsal pedal artery <0.9 (OR, 3.00; P < .00)18
Manipulate
Sensationand reflexes Conduct monofilament testing Monofilament insensitivity (OR, 2.03; 1.50–2.76)12
Abnormal ankle reflexes (RR, 1.55; 1.01–2.36)9
Range of motion Assess for hallux limitus and hallux rigidus Presence of hallux rigidus (OR, 3.3; P < .03)22
Abbreviations: HR, hazard ratio; OR, odds ratio; PVD, peripheral vascular disease; RR, relative risk
Figure 2.
10 SITES FOR MONOFILAMENT TESTING
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 516 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
diabetes and active ulcers were actually wearing downloading
devices during activities on a regular basis. Chin et al29 identified
a number of action cues from family, friends, and healthcare
professionals thatmay enhance daily foot examination by people
with diabetes. Valk et al28 identified 9 randomized controlled
trials (RCTs) that evaluated patient education to prevent diabetic
foot ulceration. The evidence is weak, with only 1 study of high-
risk individuals with diabetes that reported a reduction in ulcer
incidence (Peto OR, 0.28; 95% CI, 0.13–0.59) and reduced am-
putation rate (Peto OR, 0.32; 95% CI, 0.14–0.71) 1 year after
intensive educational interventions. Ismail et al30 identified 25
trials that utilized various psychological interventions (eg, prob-
lem solving, contract setting, goal setting, self-monitoring of
behaviors) to improve diabetic self-management. Patients al-
located to psychological therapies demonstrated improvement
in A1c (12 trials, standardized effect size = -0.32; -0.57 to -0.07)
and reduction of psychological distress including depression and
anxiety (5 trials, -0.5; -0.95 to -0.20).
Individuals livingwith foot ulcers experience poor quality of life
because of limited mobility, social isolation, disruption to work
and leisure activities, sleep disturbance, depression, and pain.31,32
According to a systematic review,33 the prevalence of depression
is3 timeshigher in type1diabetes (12%[range, 5.8%–43.3%]vs3.2%
[range, 2.7%–11.4%]) and 2 times higher prevalence of depression
in peoplewith type 2 diabetes (19.1% [range, 6.5%–33%] vs 10.7%
[range, 3.8%–19.4%]) than in those without diabetes. The impact
of depression and related distress on individuals with diabetes
cannot be underestimated.
In a 5-year follow-up study of a cohort of PWDs, Winkley
et al34 explored the association between depressive disorders
andmortality. Matched with age and gender, participants with a
documented history of depression were associated with 2-fold
increased risk inmortality (hazard ratio, 2.09; 95%CI, 1.34–3.25)
compared with those without depression. Healing of diabetic
foot ulcers can be predicted by depression.35
Similarly, PWDs who report pain most or all of the time had
statistically and clinically significantly poorer health-relatedquality
of life than those who did not report pain.36 However, pain in
diabetes is often underestimated and undertreated.37
5. Optimize local wound environment for healing through
debridement, infection control (bacterial burden control),
and moisture balance (DIM).
Table 3.
COMMON VASCULAR ASSESSMENT TECHNIQUES AND PARAMETERS
Test (Reference Values) Evidence Comments
Palpable pedal pulse
(80 mm Hg)
& Absent or reduced pedal pulses increases the likelihood
of PVD (LR, 4.70; 95% CI, 2.20–9.90)31
& PPP compared with color duplex imaging PWD with
PVD (sensitivity = 81%, specificity = 56%, PPV = 42%)32
& Absence of foot pulses Risk of new DFU (RR, <4.72;
3.28–6.78)15
& Palpable pulses can be misleading
because of noncompressible blood
vessels associated with advanced
atherosclerosis
Ankle-brachial pressure
index (ABI) (>0.5 and <1.2)
& Outside reference range, PVD identified (sensitivity =
90%; specificity = 95%)33
& ABPI compared with color duplex imaging PWD with
PVD (sensitivity = 53%; specificity = 95%; PPV = 80%)32
& False elevation in patients with
calcified vessels32
& The accuracy of ABI-toe brachial index
is poor if ABI 1.334
& Risk of ulceration if ABI dorsal pedal
artery <0.9 (OR, 3.00; P < .0000)18
Transcutaneous oxygen
tension (>30 mm Hg)
& Below-the-knee values of <30 mm Hg predict the need
for above-the-ankle amputation in diabetic patients
(sensitivity = 78.6%; specificity = 83%)35
& >30 mm Hg predicts healing of DFU (sensitivity = 15%;
specificity = 97%; PPV = 79%; NPV = 94%)36
& Expensive equipment and labor
intensive
& 15 mm Hg higher dorsal foot
transcutaneous Po2 0.8 (0.7–0.9)14
Toe pressure
(>55 mm Hg)
& >55 mm Hg has the ability to predict healing of arterial
ulcers (sensitivity = 75%; specificity = 86%)37
& >55 mm Hg compared with color duplex imaging in
diagnosed PVD in PWD (sensitivity = 100%; specificity =
61%; PPV = 48%)32
& Large toe isof a small caliberwithout a fully
developed adventitial layer to allow
circumferential calcium deposits
& Cannot be calibrated if there is previous
toe amputation
Abbreviations: CI, confidence interval; LR, likelihood ratio; NPV, negative predictive value; OR, odds ratio; PPP, palpable pedal pulses; PPV, positive predictive value; PVD, peripheral
vascular disease; PWD, persons with diabetes.
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013517WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
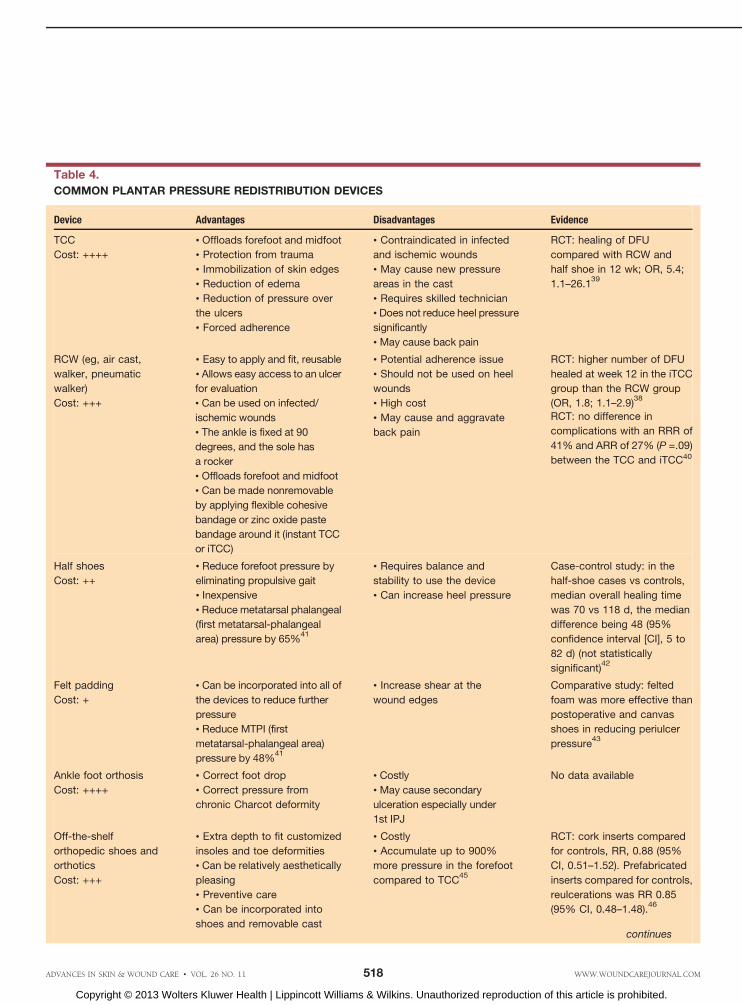
Table 4.
COMMON PLANTAR PRESSURE REDISTRIBUTION DEVICES
Device Advantages Disadvantages Evidence
TCC
Cost: ++++
& Offloads forefoot and midfoot
& Protection from trauma
& Immobilization of skin edges
& Reduction of edema
& Reduction of pressure over
the ulcers
& Forced adherence
& Contraindicated in infected
and ischemic wounds
& May cause new pressure
areas in the cast
& Requires skilled technician
& Does not reduce heel pressure
significantly
& May cause back pain
RCT: healing of DFU
compared with RCW and
half shoe in 12 wk; OR, 5.4;
1.1–26.139
RCW (eg, air cast,
walker, pneumatic
walker)
Cost: +++
& Easy to apply and fit, reusable
& Allows easy access to an ulcer
for evaluation
& Can be used on infected/
ischemic wounds
& The ankle is fixed at 90
degrees, and the sole has
a rocker
& Offloads forefoot and midfoot
& Can be made nonremovable
by applying flexible cohesive
bandage or zinc oxide paste
bandage around it (instant TCC
or iTCC)
& Potential adherence issue
& Should not be used on heel
wounds
& High cost
& May cause and aggravate
back pain
RCT: higher number of DFU
healed at week 12 in the iTCC
group than the RCW group
(OR, 1.8; 1.1–2.9)38
RCT: no difference in
complications with an RRR of
41% and ARR of 27% (P =.09)
between the TCC and iTCC40
Half shoes
Cost: ++
& Reduce forefoot pressure by
eliminating propulsive gait
& Inexpensive
& Reduce metatarsal phalangeal
(first metatarsal-phalangeal
area) pressure by 65%41
& Requires balance and
stability to use the device
& Can increase heel pressure
Case-control study: in the
half-shoe cases vs controls,
median overall healing time
was 70 vs 118 d, the median
difference being 48 (95%
confidence interval [CI], 5 to
82 d) (not statistically
significant)42
Felt padding
Cost: +
& Can be incorporated into all of
the devices to reduce further
pressure
& Reduce MTPI (first
metatarsal-phalangeal area)
pressure by 48%41
& Increase shear at the
wound edges
Comparative study: felted
foam was more effective than
postoperative and canvas
shoes in reducing periulcer
pressure43
Ankle foot orthosis
Cost: ++++
& Correct foot drop
& Correct pressure from
chronic Charcot deformity
& Costly
& May cause secondary
ulceration especially under
1st IPJ
No data available
Off-the-shelf
orthopedic shoes and
orthotics
Cost: +++
& Extra depth to fit customized
insoles and toe deformities
& Can be relatively aesthetically
pleasing
& Preventive care
& Can be incorporated into
shoes and removable cast
& Costly
& Accumulate up to 900%
more pressure in the forefoot
compared to TCC45
RCT: cork inserts compared
for controls, RR, 0.88 (95%
CI, 0.51–1.52). Prefabricated
inserts compared for controls,
reulcerations was RR 0.85
(95% CI, 0.48–1.48).46
continues
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 518 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
DebridementNonviable tissue including eschar or soft slough promotes bac-
teria growth and creates a proinflammatory environment that
inhibits healing.38 However, not all wounds need and benefit
from debridement. The decision to perform debridement should
take into consideration whether complete wound closure is re-
alistic and achievable. For wounds with the ability to heal, sur-
gical debridement of callus and abnormal surface granulation
with a curette, scissors, or scalpel blade has been considered to
be the most effective way to destroy the biofilm structure and
reduce the number of senescent cells that impede healing.39 In a
143-patient study by Saap and Falanga,40 wound closure of
diabetic foot ulcers was predicted by whether the ulcers were
adequately debrided (OR, 2.4; 95% CI, 1.0–5.6). Removal of hy-
perkeratosis and callus has been shown to reduce the risk of
diabetic foot ulcers by lowering overall peak plantar pressure by
29%.41 Edwards and Stapley42 reviewed RCTs pertaining to
debridement of diabetic foot ulcers. Combining results from
3 RCTs suggests hydrogels are superior to gauze or standard
ulcer care to assist tissue autolytic debridement and healing in
diabetic foot ulcers (RR, 1.84; 95% CI, 1.3–2.61). For wounds
that do not have the potential for healing, debridement is con-
traindicated.Without adequate blood supply and immunedefense,
debridement can increase the risk of infection (especially when
moisture is donated into the wound) and create a larger and
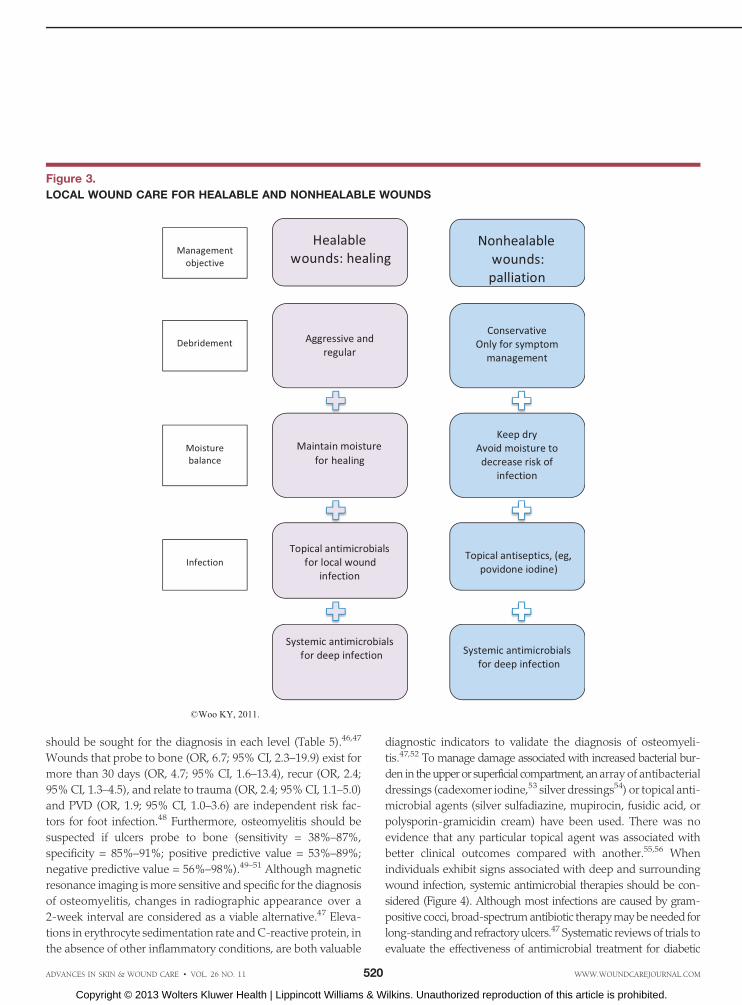
deeper wound that does not heal. It is recommended that non-
healable wounds be kept dry and only loose-hanging slough be
removed under judicious consideration (Figure 3).
InfectionIndividuals with diabetes are susceptible to wound infection
as a result of immunodeficiency, neuropathy, and arteriopathy.
Mowat et al43 documented an in vitro leukocyte chemotaxis
defect in PWDs. Phagocytosis and bactericidal capacity were
significantly reduced in thepresenceofhyperglycemia.Galkowska
et al44 compared ulcer margin of foot biopsies in PWDs (n = 12)
to normal controls (n = 5) and found no increased ratio of theCD4
andCD8 T lymphocytes indicating a relative lymphocyte response
defect. Loots et al45 examined the cellular infiltrate patterns of
punch biopsies from acute and chronic wounds including PWDs
and foot ulcers. The CD4/CD8 ratio in all chronic wounds was
significantly lower (P < .0027) compared with acute wounds. In
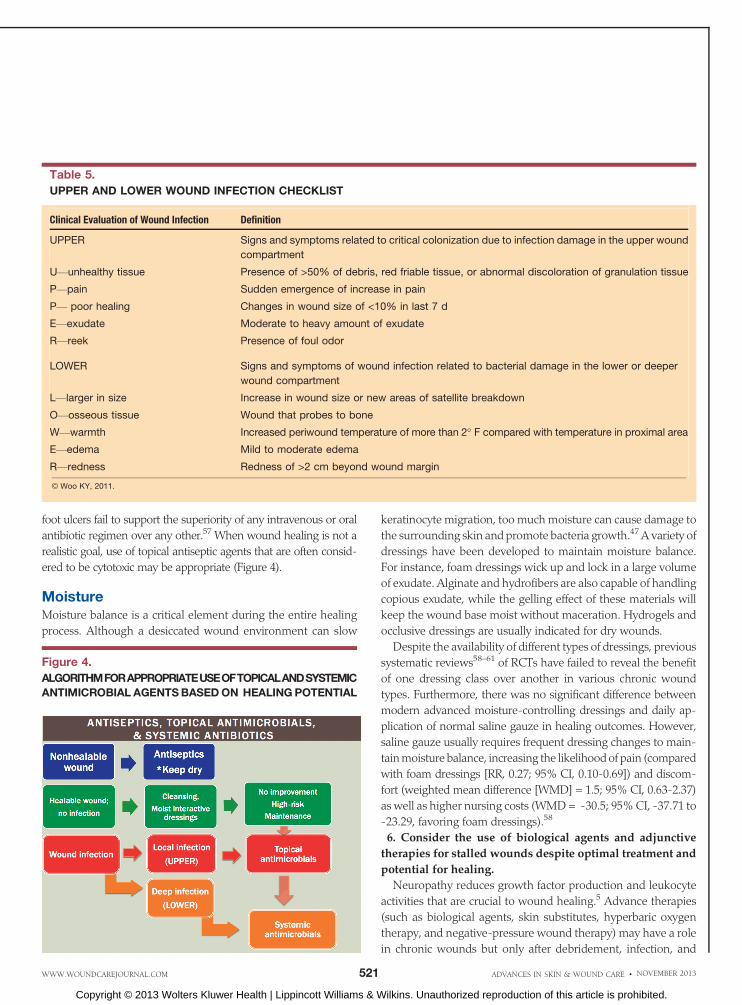
light of the ubiquitous presence of microbes, proposed clinical
presentations (Table 5) may help to distinguish whether sig-
nificant bacterial damage occurs in the upper superficial or ex-
tends to the lower deep compartments.46 Early assessment and
prompt treatment may help to prevent untoward outcomes.
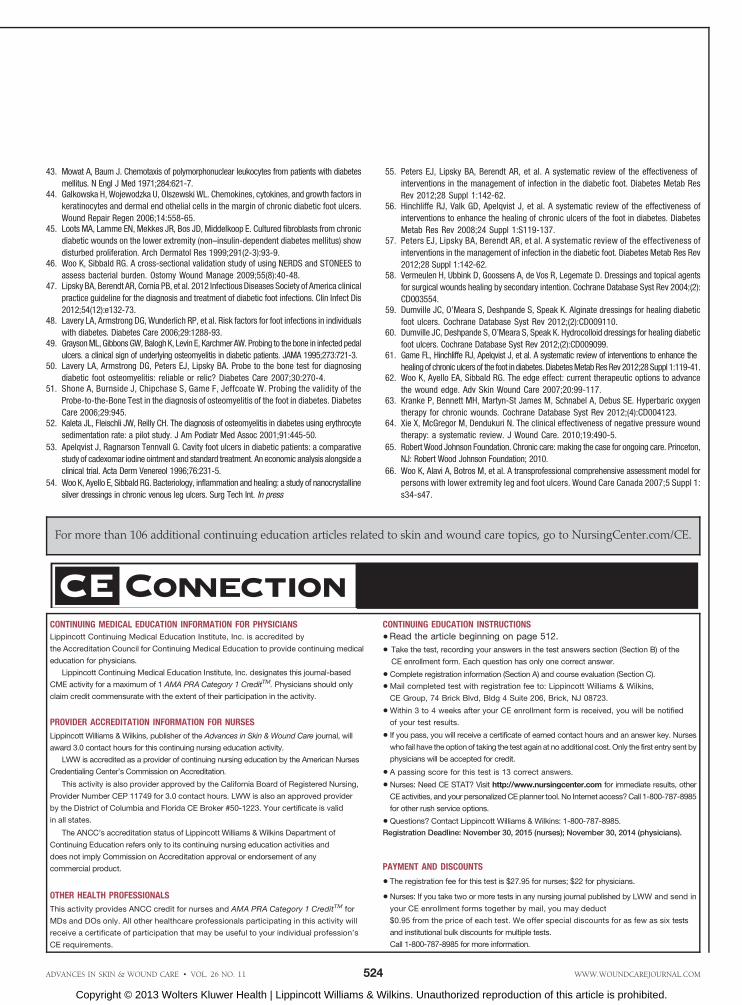
Increased surface bacterial burdenmay be treated with topical
antimicrobials, whereas systemic treatment is required for lower
compartment involvement (Figure 4). There is no one individ-
ual sign or symptom that will accurately confirm the diagnosis
of wound infection, but a combination of 2 or more indicators
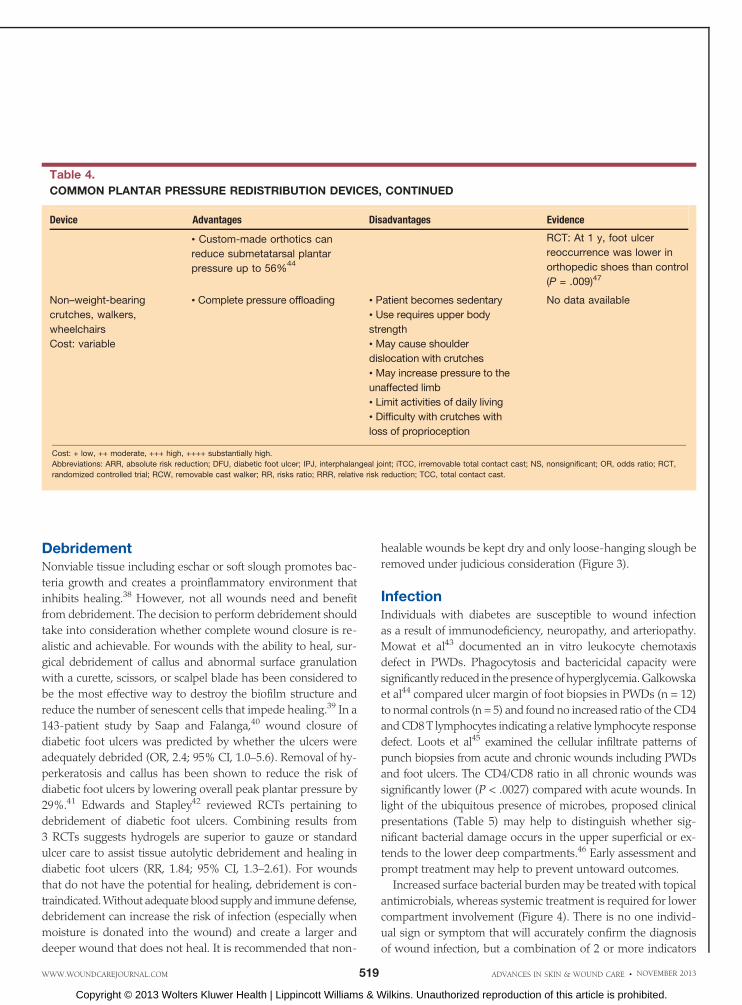
& Custom-made orthotics can
reduce submetatarsal plantar
pressure up to 56%44
RCT: At 1 y, foot ulcer
reoccurrence was lower in
orthopedic shoes than control
(P = .009)47
Non–weight-bearing
crutches, walkers,
wheelchairs
Cost: variable
& Complete pressure offloading & Patient becomes sedentary
& Use requires upper body
strength
& May cause shoulder
dislocation with crutches
& May increase pressure to the
unaffected limb
& Limit activities of daily living
& Difficulty with crutches with
loss of proprioception
No data available
Cost: + low, ++ moderate, +++ high, ++++ substantially high.
Abbreviations: ARR, absolute risk reduction; DFU, diabetic foot ulcer; IPJ, interphalangeal joint; iTCC, irremovable total contact cast; NS, nonsignificant; OR, odds ratio; RCT,
randomized controlled trial; RCW, removable cast walker; RR, risks ratio; RRR, relative risk reduction; TCC, total contact cast.
Table 4.
COMMON PLANTAR PRESSURE REDISTRIBUTION DEVICES, CONTINUED
Device Advantages Disadvantages Evidence
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013519WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
should be sought for the diagnosis in each level (Table 5).46,47
Wounds that probe to bone (OR, 6.7; 95% CI, 2.3–19.9) exist for
more than 30 days (OR, 4.7; 95% CI, 1.6–13.4), recur (OR, 2.4;
95%CI, 1.3–4.5), and relate to trauma (OR, 2.4; 95%CI, 1.1–5.0)
and PVD (OR, 1.9; 95% CI, 1.0–3.6) are independent risk fac-
tors for foot infection.48 Furthermore, osteomyelitis should be
suspected if ulcers probe to bone (sensitivity = 38%–87%,
specificity = 85%–91%; positive predictive value = 53%–89%;
negative predictive value = 56%–98%).49–51 Although magnetic
resonance imaging ismore sensitive and specific for the diagnosis
of osteomyelitis, changes in radiographic appearance over a
2-week interval are considered as a viable alternative.47 Eleva-
tions in erythrocyte sedimentation rate andC-reactive protein, in
the absence of other inflammatory conditions, are both valuable
diagnostic indicators to validate the diagnosis of osteomyeli-
tis.47,52 To manage damage associated with increased bacterial bur-
den in theupperor superficial compartment, anarray of antibacterial
dressings (cadexomer iodine,53 silver dressings54) or topical anti-
microbial agents (silver sulfadiazine, mupirocin, fusidic acid, or
polysporin-gramicidin cream) have been used. There was no
evidence that any particular topical agent was associated with
better clinical outcomes compared with another.55,56 When
individuals exhibit signs associated with deep and surrounding
wound infection, systemic antimicrobial therapies should be con-
sidered (Figure 4). Although most infections are caused by gram-
positive cocci, broad-spectrumantibiotic therapymaybeneeded for
long-standing and refractory ulcers.47 Systematic reviews of trials to
evaluate the effectiveness of antimicrobial treatment for diabetic
Figure 3.
LOCAL WOUND CARE FOR HEALABLE AND NONHEALABLE WOUNDS
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 520 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
foot ulcers fail to support the superiority of any intravenous or oral
antibiotic regimen over any other.57 When wound healing is not a
realistic goal, use of topical antiseptic agents that are often consid-
ered to be cytotoxic may be appropriate (Figure 4).
MoistureMoisture balance is a critical element during the entire healing
process. Although a desiccated wound environment can slow
keratinocyte migration, too muchmoisture can cause damage to
the surrounding skin and promote bacteria growth.47A variety of
dressings have been developed to maintain moisture balance.
For instance, foam dressings wick up and lock in a large volume
of exudate. Alginate and hydrofibers are also capable of handling
copious exudate, while the gelling effect of these materials will
keep the wound base moist without maceration. Hydrogels and
occlusive dressings are usually indicated for dry wounds.
Despite the availability of different types of dressings, previous
systematic reviews58–61 of RCTs have failed to reveal the benefit
of one dressing class over another in various chronic wound
types. Furthermore, there was no significant difference between
modern advanced moisture-controlling dressings and daily ap-
plication of normal saline gauze in healing outcomes. However,
saline gauze usually requires frequent dressing changes to main-
tainmoisture balance, increasing the likelihoodof pain (compared
with foam dressings [RR, 0.27; 95% CI, 0.10-0.69]) and discom-
fort (weighted mean difference [WMD] = 1.5; 95% CI, 0.63-2.37)
as well as higher nursing costs (WMD= -30.5; 95%CI, -37.71 to
-23.29, favoring foam dressings).58
6. Consider the use of biological agents and adjunctive
therapies for stalled wounds despite optimal treatment and
potential for healing.
Neuropathy reduces growth factor production and leukocyte
activities that are crucial to wound healing.5 Advance therapies
(such as biological agents, skin substitutes, hyperbaric oxygen
therapy, and negative-pressure wound therapy) may have a role
in chronic wounds but only after debridement, infection, and
Table 5.
UPPER AND LOWER WOUND INFECTION CHECKLIST
Clinical Evaluation of Wound Infection Definition
UPPER Signs and symptoms related to critical colonization due to infection damage in the upper wound
compartment
UVunhealthy tissue Presence of >50% of debris, red friable tissue, or abnormal discoloration of granulation tissue
PVpain Sudden emergence of increase in pain
PV poor healing Changes in wound size of <10% in last 7 d
EVexudate Moderate to heavy amount of exudate
RVreek Presence of foul odor
LOWER Signs and symptoms of wound infection related to bacterial damage in the lower or deeper
wound compartment
LVlarger in size Increase in wound size or new areas of satellite breakdown
OVosseous tissue Wound that probes to bone
WVwarmth Increased periwound temperature of more than 2- F compared with temperature in proximal area
EVedema Mild to moderate edema
RVredness Redness of >2 cm beyond wound margin
B Woo KY, 2011.
Figure 4.
ALGORITHMFORAPPROPRIATEUSEOFTOPICALANDSYSTEMIC
ANTIMICROBIAL AGENTSBASEDON HEALINGPOTENTIAL
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013521WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

moisture balance are addressed.62 Clinicians ask if there is suf-
ficient evidence to support advanced therapies. Analysis of
pooled data from 3 RCTs of 140 people with a diabetic foot ulcer
demonstrated an increase in the rate of ulcer healing (RR, 5.20;
95%CI, 1.25–21.66; P = .02) in favor of hyperbaric oxygen therapy
at 6 weeks, but long-term benefits remained unequivocal. There
was no difference in major amputation rate according to results
from 5 trials with 312 participants (RR, 0.36; 95% CI, 0.11–1.18).63
Negative-pressure wound therapy has been widely used. In a
recent review of 7 RCTs involving 580 patients with diabetic foot
ulcers, 5 studies documented acceleratedwoundhealingwith the
treatment of negative-pressure wound therapy.64
7. Establish and empower an interprofessional team to
improve care of PWDs and foot ulcers
The optimal care of individualswith chronic leg and foot ulcers
is complex and time-consuming and requires the support of an
interprofessional team. Management of these ulcers involves a
detailed examination and discussion with patients to adequately
address their concerns. The management of a chronic wound
may be further complicated by the fragmentation of communi-
cation and services between acute, chronic, and home care.65
An interprofessional team approach that draws on the re-
quired expertise from a number of healthcare professionals,
including diabetic education, medicine, nursing, infection con-
trol, chiropody, rehabilitation, andnutrition, is required to address
the complexity of diabetic foot ulcer care.66 A patient education
sample handout is illustrated in Table 6.
SummaryPeople with diabetes are at risk for foot problems, including skin
ulcerations. This article highlighted the need to complete a com-
prehensive and holistic assessment to include laboratory evalu-
ation, physical examination, lifestyle modifications, and patients’
perception and readiness to participate in self-management of the
disease. Lower leg and foot assessment should be part of routine
practice at each patient encounter to identify risks and needs for
early intervention. Although debridement, infection manage-
ment, and moisture balance are the key elements to optimize
local wound environment for healing, clinicians must consider all
available options to redistribute plantar pressure. The care of an
active foot ulcer would necessitate involvement of an inter-
professional team and ongoing psychosocial support.
Table 6.
PATIENT HANDOUTYou need to ensure that your feet last a lifetime. The care of your feet can be summarized with the 12 words beginning
with the letter ‘‘S’’ in the chart below. You can prevent foot complications: Act to protect your own feet.
Things to Consider Take Action
Sugar & Take care of your diabetes; check your blood glucose regularly and have your doctor check your
long-term glucose control with a test called the hemoglobin A1c every 3 months.
Smoking & Stop smoking. Every cigarette will decrease the circulation in your legs by 30% for an hour.
Sores (blisters, cuts,
open skin)
& Check for sores on your feet every day. The skin breaks down because of a loss of protective sensation
and the silent trauma of rubbing or increased pressure points during walking. Seek help!
Scale and callus & Check for scale and callus on your feet every day. Scale because of dry skin or a fungus infection and
callus because of too much local pressure. Seek help!
See the bottom of your
feet daily
&Make sure you can see and check the bottom of your feet. You may want to have someone else to help
check your feet if your vision is poor.
Socks & Socks should have no seams and should not bunch up in the shoes creating new areas of increased
pressure. Wear socks at night if your feet are cold.
Shoes & Wear proper-fitting deep-toed shoes with orthotics. Avoid pointed toes and sandals. Have your shoes
fitted at the end of the day by a professional shoe fitter. You will often choose shoes that are too tight.
Steps: & Wear your shoes all the time with each step, inside and outside of your home (including going to the
bathroom at night). Do not walk barefoot or in socks or with slippers that have no support.
Shower and wash & Shower and wash your feet every day.
Soaks & Never soak your feet!
Safe nail care & Cut nails straight across and see your foot care specialist.
Skin care & Avoid adhesive tape and chemical treatments, such as wart removers. Use moisturizers to keep your
skin soft. Do not put oil or cream between the toes.
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 522 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

REFERENCES1. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic
foot disease. Lancet 2005;366(9498):719-24.2. Brem H, Sheehan P, Rosenberg H, Schneider JS, Boulton AJ. Evidence-based protocol
for diabetic foot ulcers. Plast Reconstr Surg 2006;117(Suppl 7):193S-209S.3. Abbott CA, Carrington AL, Ashe H, et al. The North-West Diabetes Foot Care Study: incidence
of, and risk factors for, new diabetic foot ulceration in a community-based patient-cohort.
Diabet Med 2002;19:377-84.4. Adler AI, Boyko EJ, Ahroni JH, Smith DG. Lower extremity amputation in diabetes. The
independent effects of peripheral vascular disease, sensory neuropathy, and foot ulcers.
Diabetes Care 1999;22:1029-35.5. Bakker K, Apelqvist J, Schaper NC. Practical guidelines on the management and prevention
of the diabetic foot 2011. Diabet Metab Res Rev 2012;28(Suppl 1):225-31.6. Sibbald GR, Woo KY. The biology of chronic foot ulcers in persons with diabetes. Diabetes
Metab Res Rev 2008;24(Suppl 1):S25-30.7. Orsted HL, Searles G, Trowell H, Shapera L, Miller M, Rahman J. Best practice recommen-
dations for the prevention, diagnosis, and treatment of diabetic foot ulcers: update 2006. Adv
Skin Wound Care 2007;20:655-69.8. Centre for Clinical Practice at NICE (UK). Diabetic Foot Problems: Inpatient Management of
Diabetic Foot Problems. London, UK: National Institute for Health and Clinical Excellence; 2011.9. Bakker K, Apelqvist J, Schaper NC; , International Working Group on Diabetic Foot Editorial
Board. Practical guidelines on the management and prevention of the diabetic foot 2011.
Diabetes Metab Res Rev 2012;28 Suppl 1:225-31.10. Sibbald RG, Goodman L, Woo KY, et al. Special considerations in wound bed preparation
2011: an update. Adv Skin Wound Care 2011;24:415-36.11. Warriner RA, Snyder RJ, Cardinal MH. Differentiating diabetic foot ulcers that are unlikely to
heal by 12 weeks following achieving 50% percent area reduction at 4 weeks. Int Wound J
2011;8:632-7.
12. Monteiro-Soares M, Boyko E, Ribeiro J, Ribeiro I, Dinis-Ribeiro M. Predictive factors for
diabetic foot ulceration: a systematic review. Diabetes Metab Res Rev 2012;28:574-600.
13. Boyko EJ, Ahroni JH, Cohen V, Nelson KM, Heagerty PJ. Prediction of diabetic foot ulcer
occurrence using the commonly available clinical information: the Seattle Diabetic Foot
Study. Diabetes Care 2006;29:1202-07.
14. Inlow S, Orsted H, Sibbald RG. Best practices for the prevention, diagnosis and treatment of
diabetic foot ulcers. Ostomy Wound Manage 2000;46(11):55-68.
15. Murphy CA, Laforet K, DaRosa P, Tabamo F, Woodbury MG. Reliability and predictive
validity of Inlow’s 60-Second Diabetic Foot Screen Tool. Adv Skin Wound Care 2012;25:
261-6.
16. Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques
to identify people at high risk for diabetic foot ulceration; a prospective multicenter trial.
Diabetes Care 2000;23:606-11.
17. Crawford F, Inkster M, Kleijnen J, Fahey T. Predicting foot ulcers in patients with diabetes: a
systematic review and meta-analysis. Q J Med 2007;100:65-86.
18. Murray HJ, Young MJ, Hollis S, Boulton AJM. The association between callus formation,
high pressures and neuropathy in diabetic foot ulceration. Diabetic Med 1996;13:979-82.
19. Cowley MS, Boyko EJ, Shofer JB, Ahroni JH, Ledoux WR. Foot ulcer risk and location in
relation to prospective clinical assessment of foot shape and mobility among persons
with diabetes. Diabetes Res Clin Pract 2008;82:226-32.
20. Khan NA, Rahim SA, Anand SA, Simel DL, Panju A. Does the clinical examination predict
lower extremity peripheral arterial disease? JAMA 2006;295:536-46.
21. Williams DT, Harding KG, Price P. An evaluation of the efficacy of methods used in screening
for lower-limb arterial disease in diabetes. Diabetes Care 2005;28:2206-10.
22. Crique MH, Fronek A, Klauber MR, Barrett-Connor E, Gabriel S. The sensitivity, specificity
and predictive value of traditional clinical evaluation of peripheral arterial disease: results
from non-invasive testing in a defined population. Circulation 1985;71:516-522.
23. Alexandrescu V, Sderstrm M, Vermano M. Angiosome theory: fact or fiction? Scand J
Surg 2012;101:125-31.
24. Katz IA, Harlan A, Miranda-Palma B, et al. A randomized trial of two irremovable off-loading
devices in the management of plantar neuropathic diabetic foot ulcers. Diabetes Care
2005;28:555-9.
25. Gale L, Vedhara K, Searle A, Kemple T, Campbell R. Patients’ perspective on foot complications
in type 2 diabetes: a qualitative study. Br J Gen Pract 2008;58:555-63.
26. Health Council of Canada. Self-management support for Canadians with chronic health
conditions. Toronto, ON, Canada: Health Council of Canada; 2012.
27. Knowles EA, Boulton AJ. Do people with diabetes wear their prescribed footwear? Diabet
Med 1996;13:1064-8.
28. Valk GD, Kriegsman DM, Assendelft WJ. Patient education for preventing diabetic foot
ulceration. Cochrane Database Syst Rev 2001;(4):CD001488.
29. Chin YF, Huang TT, Hsu BR. Impact of action cues, self-efficacy and perceived barriers on
daily foot exam practice in type 2 diabetes mellitus patients with peripheral neuropathy.
J Clin Nurs 2013;22(1-2):61-8.
30. Ismail K, Winkley K, Rabe-Hesketh S. Systematic review and meta-analysis of randomized
controlled trials of psychological interventions to improve glycemic control in patients with
type II diabetes. Lancet 2004;363(9421):1589-97.
31. Egede LE, Ellis C. Diabetes and depression: global perspectives. Diabetes Res Clin
Pract 2010;87(3):302-12.
32. Gask L, Macdonald W, Bower P. What is the relationship between diabetes and depression?
A qualitative metasynthesis of patient experience of co-morbidity. Chronic Illn 2011;7(3):
239-52.
33. Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect
Disord 2012;142 Suppl:S8-21.
34. Winkley K, Sallis H, Kariyawasam D, et al. Five-year follow-up of a cohort of people with
their first diabetic foot ulcer: the persistent effect of depression on mortality. Diabetologia
2012;55:303-10.
35. Vedhara K, Miles JN, Wetherell MA, et al. Coping style and depression influence the healing of
diabetic foot ulcers: observational and mechanistic evidence. Diabetologia 2010;53:1590-8.
36. Ribu L, Rusten T, Birkeland K, Hanestad BR, Paul SM, Miaskowski C. The prevalence
and occurrence of diabetic foot ulcer pain and its impact on health-related quality of
life. J Pain 2006;7:290-9.
37. Bengtsson L, Jonsson M, Apelqvist J. Wound-related pain is underestimated in patients
with diabetic foot ulcers. J Wound Care 2008;17:433-5.
38. Kirshen C, Woo K, Ayello EA, Sibbald RG. Debridement: a vital component of wound bed
preparation. Adv Skin Wound Care 2006;19:506-17.
39. Wolcott RD, Rumbaugh KP, James G, et al. Biofilm maturity studies indicate sharp debridement
opens a time- dependent therapeutic window. J Wound Care 2010;19:320-8.
40. Saap LJ, Falanga V. Debridement performance index and its correlation with complete
closure of diabetic foot ulcers. Wound Repair Regen 2002;10:354-9.
41. Slater RA, Hershkowitz I, Ramot Y, Buchs A, Rapoport MJ. Reduction of digital plantar
pressure by debridement and silicone orthosis. Diab Res Clin Pract 2006;74:263-6.
42. Edwards J, Stapley S. Debridement of diabetic foot ulcers. Cochrane Database Syst Rev
2010;(1):CD003556.
This article focuses on the current state of care recommenda-
tions for persons living with diabetic foot ulcers. These include
the following:
& Perform a comprehensive clinical assessment that includes
A1c, blood pressure, cholesterol, diet, exercise, and smoking
history.
& Conduct a lower-leg and foot assessment to differentiate
neuropathic from neuroischemic diseases (ulcers).
&Optimize plantar pressure redistribution to prevent and
treat diabetic foot ulcers.
& Address the individual’s concerns and modify plan of care
to promote self-care and treatment adherence.
&Optimize local wound environment for healing through
debridement, infection control (bacterial burden control),
and moisture balance (DIM).
& Consider the use of biological agents and adjunctive ther-
apies for stalled wounds despite optimal treatment and po-
tential for healing.
& Establish and empower an interprofessional team to im-
prove the care of persons with diabetes and foot ulcers.
PRACTICE PEARLS
ADVANCES IN SKIN & WOUND CARE & NOVEMBER 2013523WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
43. Mowat A, Baum J. Chemotaxis of polymorphonuclear leukocytes from patients with diabetes
mellitus. N Engl J Med 1971;284:621-7.44. Galkowska H, Wojewodzka U, Olszewski WL. Chemokines, cytokines, and growth factors in
keratinocytes and dermal end othelial cells in the margin of chronic diabetic foot ulcers.
Wound Repair Regen 2006;14:558-65.45. Loots MA, Lamme EN, Mekkes JR, Bos JD, Middelkoop E. Cultured fibroblasts from chronic
diabetic wounds on the lower extremity (non–insulin-dependent diabetes mellitus) show
disturbed proliferation. Arch Dermatol Res 1999;291(2-3):93-9.46. Woo K, Sibbald RG. A cross-sectional validation study of using NERDS and STONEES to
assess bacterial burden. Ostomy Wound Manage 2009;55(8):40-48.47. Lipsky BA, Berendt AR, Cornia PB, et al. 2012 Infectious Diseases Society of America clinical
practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis
2012;54(12):e132-73.48. Lavery LA, Armstrong DG, Wunderlich RP, et al. Risk factors for foot infections in individuals
with diabetes. Diabetes Care 2006;29:1288-93.49. Grayson ML, Gibbons GW, Balogh K, Levin E, Karchmer AW. Probing to the bone in infected pedal
ulcers. a clinical sign of underlying osteomyelitis in diabetic patients. JAMA 1995;273:721-3.50. Lavery LA, Armstrong DG, Peters EJ, Lipsky BA. Probe to the bone test for diagnosing
diabetic foot osteomyelitis: reliable or relic? Diabetes Care 2007;30:270-4.51. Shone A, Burnside J, Chipchase S, Game F, Jeffcoate W. Probing the validity of the
Probe-to-the-Bone Test in the diagnosis of osteomyelitis of the foot in diabetes. Diabetes
Care 2006;29:945.52. Kaleta JL, Fleischli JW, Reilly CH. The diagnosis of osteomyelitis in diabetes using erythrocyte
sedimentation rate: a pilot study. J Am Podiatr Med Assoc 2001;91:445-50.
53. Apelqvist J, Ragnarson Tennvall G. Cavity foot ulcers in diabetic patients: a comparative
study of cadexomar iodine ointment and standard treatment. An economic analysis alongside a
clinical trial. Acta Derm Venereol 1996;76:231-5.
54. Woo K, Ayello E, Sibbald RG. Bacteriology, inflammation and healing: a study of nanocrystalline
silver dressings in chronic venous leg ulcers. Surg Tech Int. In press
55. Peters EJ, Lipsky BA, Berendt AR, et al. A systematic review of the effectiveness of
interventions in the management of infection in the diabetic foot. Diabetes Metab Res
Rev 2012;28 Suppl 1:142-62.56. Hinchliffe RJ, Valk GD, Apelqvist J, et al. A systematic review of the effectiveness of
interventions to enhance the healing of chronic ulcers of the foot in diabetes. Diabetes
Metab Res Rev 2008;24 Suppl 1:S119-137.57. Peters EJ, Lipsky BA, Berendt AR, et al. A systematic review of the effectiveness of
interventions in the management of infection in the diabetic foot. Diabetes Metab Res Rev
2012;28 Suppl 1:142-62.58. Vermeulen H, Ubbink D, Goossens A, de Vos R, Legemate D. Dressings and topical agents
for surgical wounds healing by secondary intention. Cochrane Database Syst Rev 2004;(2):
CD003554.59. Dumville JC, O’Meara S, Deshpande S, Speak K. Alginate dressings for healing diabetic
foot ulcers. Cochrane Database Syst Rev 2012;(2):CD009110.60. Dumville JC, Deshpande S, O’Meara S, Speak K. Hydrocolloid dressings for healing diabetic
foot ulcers. Cochrane Database Syst Rev 2012;(2):CD009099.61. Game FL, Hinchliffe RJ, Apelqvist J, et al. A systematic review of interventions to enhance the
healing of chronic ulcers of the foot in diabetes. Diabetes Metab Res Rev 2012;28 Suppl 1:119-41.62. Woo K, Ayello EA, Sibbald RG. The edge effect: current therapeutic options to advance
the wound edge. Adv Skin Wound Care 2007;20:99-117.63. Kranke P, Bennett MH, Martyn-St James M, Schnabel A, Debus SE. Hyperbaric oxygen
therapy for chronic wounds. Cochrane Database Syst Rev 2012;(4):CD004123.64. Xie X, McGregor M, Dendukuri N. The clinical effectiveness of negative pressure wound
therapy: a systematic review. J Wound Care. 2010;19:490-5.
65. Robert Wood Johnson Foundation. Chronic care: making the case for ongoing care. Princeton,
NJ: Robert Wood Johnson Foundation; 2010.
66. Woo K, Alavi A, Botros M, et al. A transprofessional comprehensive assessment model for
persons with lower extremity leg and foot ulcers. Wound Care Canada 2007;5 Suppl 1:
s34-s47.
For more than 106 additional continuing education articles related to skin and wound care topics, go to NursingCenter.com/CE.
CONTINUING MEDICAL EDUCATION INFORMATION FOR PHYSICIANSLippincott Continuing Medical Education Institute, Inc. is accredited by
the Accreditation Council for Continuing Medical Education to provide continuing medical
education for physicians.
Lippincott Continuing Medical Education Institute, Inc. designates this journal-based
CME activity for a maximum of 1 AMA PRA Category 1 CreditTM. Physicians should only
claim credit commensurate with the extent of their participation in the activity.
PROVIDER ACCREDITATION INFORMATION FOR NURSES
Lippincott Williams & Wilkins, publisher of the Advances in Skin & Wound Care journal, will
award 3.0 contact hours for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing education by the American Nurses
Credentialing Center’s Commission on Accreditation.
This activity is also provider approved by the California Board of Registered Nursing,
Provider Number CEP 11749 for 3.0 contact hours. LWW is also an approved provider
by the District of Columbia and Florida CE Broker #50-1223. Your certificate is valid
in all states.
The ANCC’s accreditation status of Lippincott Williams & Wilkins Department of
Continuing Education refers only to its continuing nursing education activities and
does not imply Commission on Accreditation approval or endorsement of any
commercial product.
OTHER HEALTH PROFESSIONALS
This activity provides ANCC credit for nurses and AMA PRA Category 1 CreditTM for
MDs and DOs only. All other healthcare professionals participating in this activity will
receive a certificate of participation that may be useful to your individual profession’s
CE requirements.
CONTINUING EDUCATION INSTRUCTIONS
&Read the article beginning on page 512.
& Take the test, recording your answers in the test answers section (Section B) of the
CE enrollment form. Each question has only one correct answer.
&Complete registration information (Section A) and course evaluation (Section C).
&Mail completed test with registration fee to: Lippincott Williams & Wilkins,
CE Group, 74 Brick Blvd, Bldg 4 Suite 206, Brick, NJ 08723.
&Within 3 to 4 weeks after your CE enrollment form is received, you will be notified
of your test results.
& If you pass, you will receive a certificate of earned contact hours and an answer key. Nurses
who fail have the optionof taking the test again at no additional cost.Only the first entry sent by
physicians will be accepted for credit.
& A passing score for this test is 13 correct answers.
&Nurses: Need CE STAT? Visit http://www.nursingcenter.com for immediate results, other
CEactivities, andyour personalizedCEplanner tool. No Internet access?Call 1-800-787-8985
for other rush service options.
&Questions? Contact Lippincott Williams & Wilkins: 1-800-787-8985.
Registration Deadline: November 30, 2015 (nurses); November 30, 2014 (physicians).
PAYMENT AND DISCOUNTS
& The registration fee for this test is $27.95 for nurses; $22 for physicians.
&Nurses: If you take two or more tests in any nursing journal published by LWW and send in
your CE enrollment forms together by mail, you may deduct
$0.95 from the price of each test. We offer special discounts for as few as six tests
and institutional bulk discounts for multiple tests.
Call 1-800-787-8985 for more information.
ADVANCES IN SKIN & WOUND CARE & VOL. 26 NO. 11 524 WWW.WOUNDCAREJOURNAL.COM
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.